")
Back to Journals » Patient Preference and Adherence » Volume 17
Role of Health Literacy, Social Support, Patient-Physician Relationship, and Health-Related Quality of Life in Predicting Medication Adherence in Cardiovascular Diseases in Oman
Authors Al-Noumani H , Al Omari O, Al-Naamani Z
Received 15 December 2022
Accepted for publication 25 February 2023
Published 13 March 2023 Volume 2023:17 Pages 643—652
DOI https://doi.org/10.2147/PPA.S401666
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Huda Al-Noumani,1 Omar Al Omari,2 Zakariya Al-Naamani3
1Adult Health and Critical Care Department, College of Nursing, Sultan Qaboos University, Muscat, Oman; 2Fundamental and Administration Department, College of Nursing, Sultan Qaboos University, Muscat, Oman; 3Armed Forces Medical Services, Ministry of Defense, Muscat, Oman
Correspondence: Huda Al-Noumani, Adult Health and Critical Care Department, College of Nursing, Sultan Qaboos University, P.O.Box 66, P.C. 123, Alkhoud, Muscat, Oman, Tel +968 2414 5400, Fax +968 2441 3536, Email [email protected]
Purpose: Cardiovascular diseases (CVDs) remain a global health threat, and medication adherence remains low. Medication adherence is a complex phenomenon and is affected by many factors that require investigation. Oman has limited literature examining medication adherence and influencing factors among patients with CVDs. This study examined the influence of health literacy, social support, the patient-physician relationship, and health-related quality of life on medication adherence among patients with cardiovascular diseases.
Patients and Methods: This cross-sectional study used a correlation design. The study included 360 participants with CVDs. Descriptive statistics, independent t-test, one-way ANOVA, and multiple regression analysis were utilized for data analyses.
Results: Findings revealed that higher social support (B=0.117; p=0.033), good patient-physician relationship (B=0.124; p < 0.01), better mental health (B=0.045; p < 0.01), more bodily pain (B=0.030; p < 0.01), and unemployment (B=1.297; p < 0.01) were predictors of higher adherence. High school education and above predicted lower medication adherence (B= − 1.255; p= 0.019), while health literacy was not a significant predictor of medication adherence (B= 0.061; p= 0.289).
Conclusion: To improve medication adherence, healthcare providers and researchers should consider improving patients’ social support, mental health, and the patient-physician relationship. In addition, patients’ socioeconomic status should always be considered and examined as an influencing factor of medication adherence.
Keywords: social support, health literacy, adherence, physician-patient relations, cardiovascular diseases
Introduction
Cardiovascular diseases (CVDs) are considered one of the leading causes of death globally, taking approximately 18.6 million lives in 2019.1 In Oman, the burden of CVDs is relatively high and, on the rise, mainly due to the rapid socioeconomic development and unhealthy lifestyle, accounting for 33% of all total death.2 Although pharmacological interventions can significantly decrease CVDs morbidity and mortality rate, adherence to the prescribed medications remains a remarkable problem that causes deterioration in patients’ condition and health outcomes.3 For example, a recent systematic review found that 45% of hypertensive patients in Asia have not adhered to their prescribed medications.4 Similarly, in Oman, medication non-adherence is also high, and 64.5% of patients have either low or medium adherence.5
Medication adherence means the extent to which the individual behaves about taking the prescribed medications upon the agreed amount, frequency, and time from their healthcare providers.6,7 However, adherence to prescribed cardiac medications is a multifactorial phenomenon. Based on the World Health Organization (WHO) multidimensional adherence model, non-adherence influencing factors can be classified into five main categories, including (1) social/economic related-factors (eg, poor health literacy, low level of education, unemployment, and limited social support), (2) patient related-factors in terms of their knowledge, resources, behaviors, and beliefs about the importance of taking prescribed medications, (3) Condition/therapy-related factors, concerning the burden of long-term condition, lifelong therapy with multiple daily doses and associated side effects, and (4 and 5) healthcare team-and system-related factors, including inadequate patient-staff relationship and communication, which can negatively impact taking prescribed medications.8 In addition, several studies highlighted that those domains of health-related quality of life (HRQoL) associated with physical and psychosocial functioning could impact individuals taking their prescribed medications.9,10 Although these factors might influence medication adherence, the evidence is still not conclusive and inconsistent, and further research is required to confirm the relationship among these factors.11 Utilizing a well-designed model developed by WHO can help examine various influencing factors to medication non-adherence.
Thus, for several reasons, further insights into the multi-factors that influence medication adherence are vital, especially in developing countries. First, obtaining such information can help identify contributing factors from patients’ perspectives concerning their socio-cultural and healthcare services status. Second, the data can guide eliminating potential risks of medication non-adherence by developing appropriate strategies tailored to patients’ needs. This study, therefore, aims to determine the impact of various influencing factors concerning health literacy, social support, the patient-physician relationship, and HRQoL domains on medication adherence among Omani patients with CVD.
Materials and Methods
Study Design and Sample
This study is cross-sectional, using a descriptive correlational design. Eligibility criteria were Omani aged 18 years and above, speaking Arabic or English, had been diagnosed with at least one of the following CVDs (ie, HTN, IHD, HF), and taking one or more medication(s) for a minimum of one year. Cognitive impairment, acute illnesses, and refusal to participate were set as criteria for exclusion from participation. A non-probability convenience sampling was used.
Sample Size
The sample size was calculated based on the most sophisticated statistics, the multiple linear regression. The number of variables included in the current study was calculated to estimate the sample size, which is 13 variables (Table 1). As a rule of thumb, we counted 20 participants for each variable plus 50.12 However, to account for possible missing data, we added 50 participants. Accordingly, the needed sample size will be a total of 360 participants.
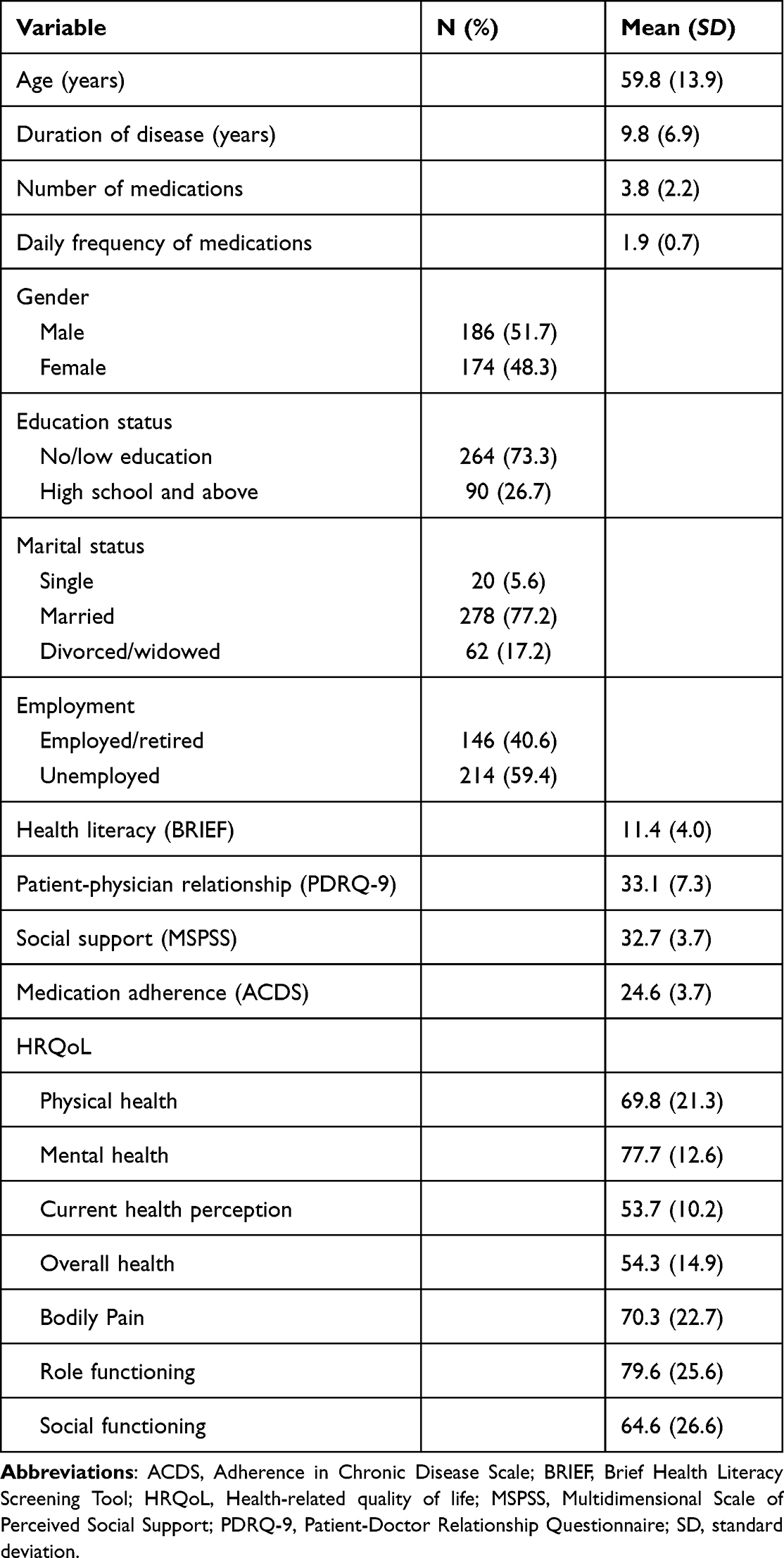 |
Table 1 Sample Characteristics and Variables Descriptive Statistics |
Procedure
The institutional ethical approval for this study was obtained from the Research and Ethical Review and Approval Committee at the Ministry of Health (MOH/DGPS/CSR/PROPOSAL_APPROVED/19/2019). Data were screened, collected, and entered by trained research nurse assistants (RAs). After getting permission from the primary health center’s administration, the RAs screened the medical records to identify the eligible participants. Then with the support of nurses working in the study setting, RAs approached participants, explained the study details, and consented to participate using a written consent form. Participants were requested to complete the self-administered questionnaire that took 15–30 minutes. Confidentiality of information and voluntary participation was ensured and explained to participants before the study commencement. Participants were also informed about their right to withdraw at any time during the study without any harm.
Measures
The Brief Health Literacy Screening Tool (BRIEF) measured the participants’ health literacy.13 The BRIEF tool consisted of four items; items 1, 2, and 3 were rated on a 5-point Likert scale (1=always - 5=never). Item 4 was rated on a Likert scale of 1=not at all, 2=little bit, 3=somewhat, 4=quite a bit, and 5=extremely. The final BRIEF score is the sum of the four non-weighted items that ranged from 4 to 20, with a higher score indicating higher health literacy. A Cronbach’s alpha of 0.680 was reported.13 In this study, Cronbach’s alpha was reported as 0.53.
The Multidimensional Scale of Perceived Social Support (MSPSS) was used to measure social support.14 MSPSS consists of 12 items, and its responses are rated on a 7-point Likert scale (1=very strongly disagree to 7=very strongly agree), with possible total scores ranging between 12 and 84. A higher score represents higher social support 14. This scale has been widely used in different cultures, and a Cronbach’s alpha of 0.75 was reported for the Arabic population.15,16 In this study, the Cronbach’s alpha of the MSPSS was 0.86.
We used the Patient-Doctor Relationship Questionnaire (PDRQ-9) to measure the patient-physician relationship. The PDRQ-9 contains nine items that quantify the therapeutic dimensions of the patient-doctor relationship and is scored using a 5-point Likert scale (1= not at all appropriate to 5=totally appropriate). Possible total scores ranged from 9 to 45, with higher scores representing a more favorable patient-doctor relationship (Van Der Feltz-Cornelis et al, 2004). Good internal consistency was reported among cancer patients with a Cronbach’s alpha of 0.95.17,18 The Cronbach’s alpha of the PDRQ-9 in this study was 0.93.
The HRQoL was assessed using SF −20, which contains six dimensions, three related to functioning (physical, role, and social) and three related to well-being (mental health, health perception, and bodily pain).19 The 20 items of the SF-20 are distributed across the following six dimensions: physical functioning (6 items), role functioning (2 items), social functioning (1 item), mental health (5 items), overall general health perception (1 item), current health perception (4 items), and bodily pain over the last four week (1 item). All scores were transformed linearly to 0–100 scales after the negatively scored items were reversed. Higher scores represent better functioning and well-being, except for pain, where higher scores reflect more pain. In this study, Cronbach’s alpha of the SF-20 was 0.72.
Outcome Variable
The Adherence in Chronic Disease Scale (ACDS) was used to assess medication adherence.20 The ACDS consists of seven questions with five possible responses scored on a Likert scale of 0 to 4 with a possible total score of 28. Questions 1–5 determined patient behavior related to adherence, and questions 6 and 7 assessed the indirect effects of adherence. This scale was reported to have good reliability and internal consistency with a Cronbach’s alpha of 0.74. In this study, the ACDS Cronbach’s alpha was 0.78.
The SF-20, PDRQ-9, ACDS, and BRIEF standardized English questionnaires were translated into Arabic Using the World Health Organization’s translation guidelines.21 Permission to use and translate the tools was obtained from their authors.
Statistical Analysis
Before statistical analysis, data were tested for normal distribution. Multiple linear regression assumptions of normality, variance, and homogeneity were tested. Assumptions of all other inferential statistical analysis were met and not violated. The sample was described using frequencies for categorical data and mean and standard deviation for continuous data. The continuous outcome variable was compared with categorical variables using independent t-test or one-way ANOVA tests. Correlations were tested using the Pearson correlation to test the relationships between the study variables stated in Table 1 and the dependent variable of medication adherence. Variables detected to be significant correlates with adherence in the bivariate and variables commonly described in the literature as predictors of medication adherence were then regressed on medication adherence. All estimates were standardized except for those of model constants. The significance level was set at p < 0.05. Analysis was done using IBM SPSS Statistics version 23.0 (IBM Corp. Released 2017. IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp.)
Results
A total of 360 participants were included in the study, with a mean age of about 60. The majority were male (51.7%), had no/low education (73.3%), were married (77.2%), and were unemployed (59.4%). Participants reported an average of 10 years of illness duration and took four medications twice daily on average (Table 1).
When bivariate analysis between the study variables included in Table 1 and medication adherence, the analyses showed that medication adherence was significantly correlated with age (p=0.028), employment status (p < 0.01), an education level (p < 0.01), PDRQ-9 (p < 0.01), MSPSS (p < 0.01), mental health (p < 0.01), and bodily pain (p < 0.01) (Table 2).
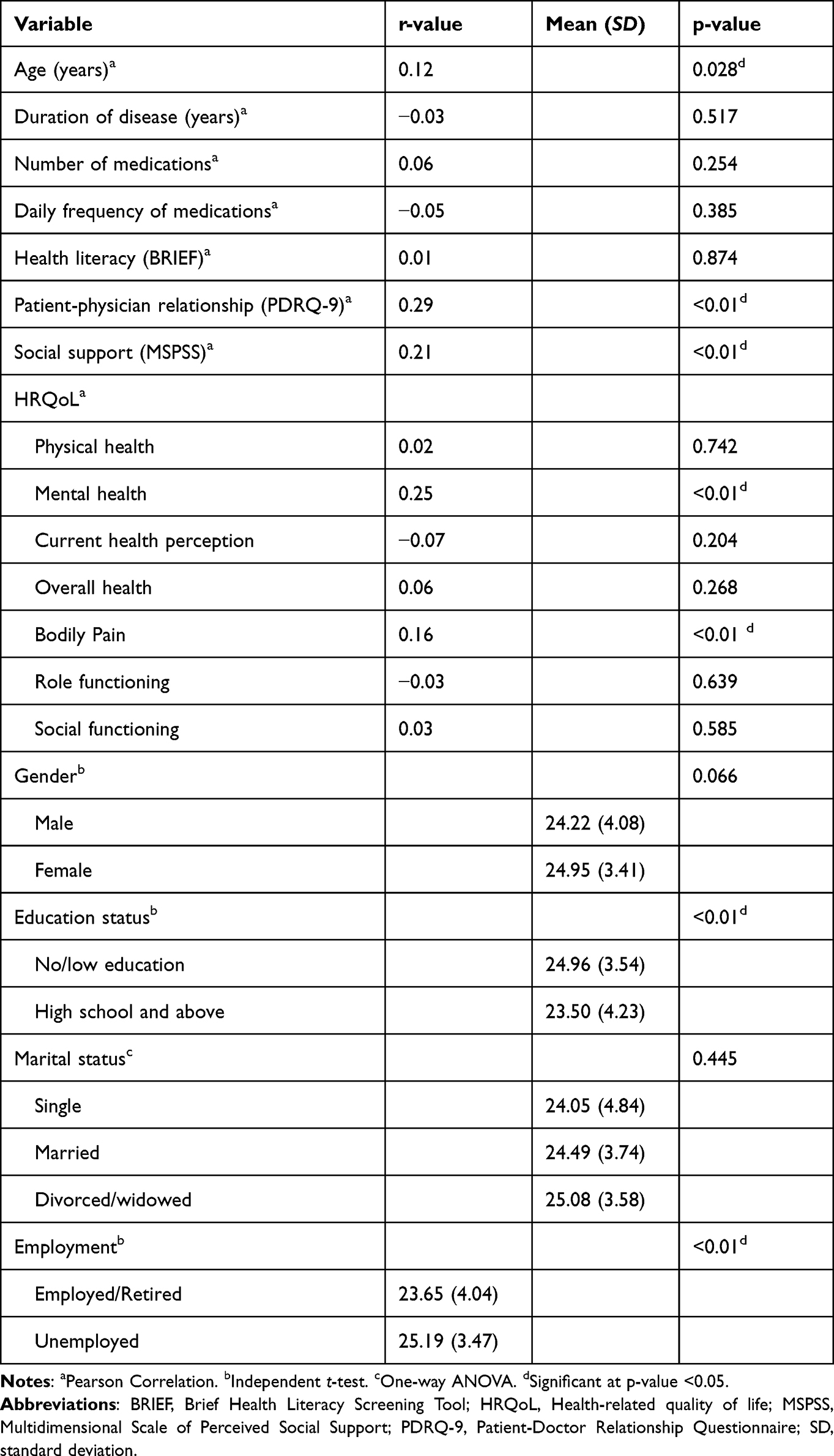 |
Table 2 Bivariate Relationship Between Medication Adherence and Study (n=360) |
All significant variables in the bivariate analyses (Table 2) and variables found significantly correlate with medication adherence in the literature (ie, health literacy (BRIEF) were included in the regression model to examine the independent predictors of medication adherence. The multivariate linear regression model showed that the patient-physician relationship, social support, mental health, bodily pain, employment, and education level significantly predicted medication adherence; these variables explained about 23% of the variation in medication adherence (R2=0.225, F(8349)=12.643; p < 0.000). In specific, participants with higher social support (B=0.117; p=0.033), good patient-physician relationship (B=0.124; p < 0.01), better mental health (B=0.045; p < 0.01), more bodily pain (B=0.030; p < 0.01), and unemployed (B=1.297; p < 0.01) reported higher adherence. On the other hand, participants with high school education and above reported lower medication adherence (B= −1.255; p=0.019). Health literacy was not a significant predictor of medication adherence (B= 0.061; p= 0.289) (Table 3).
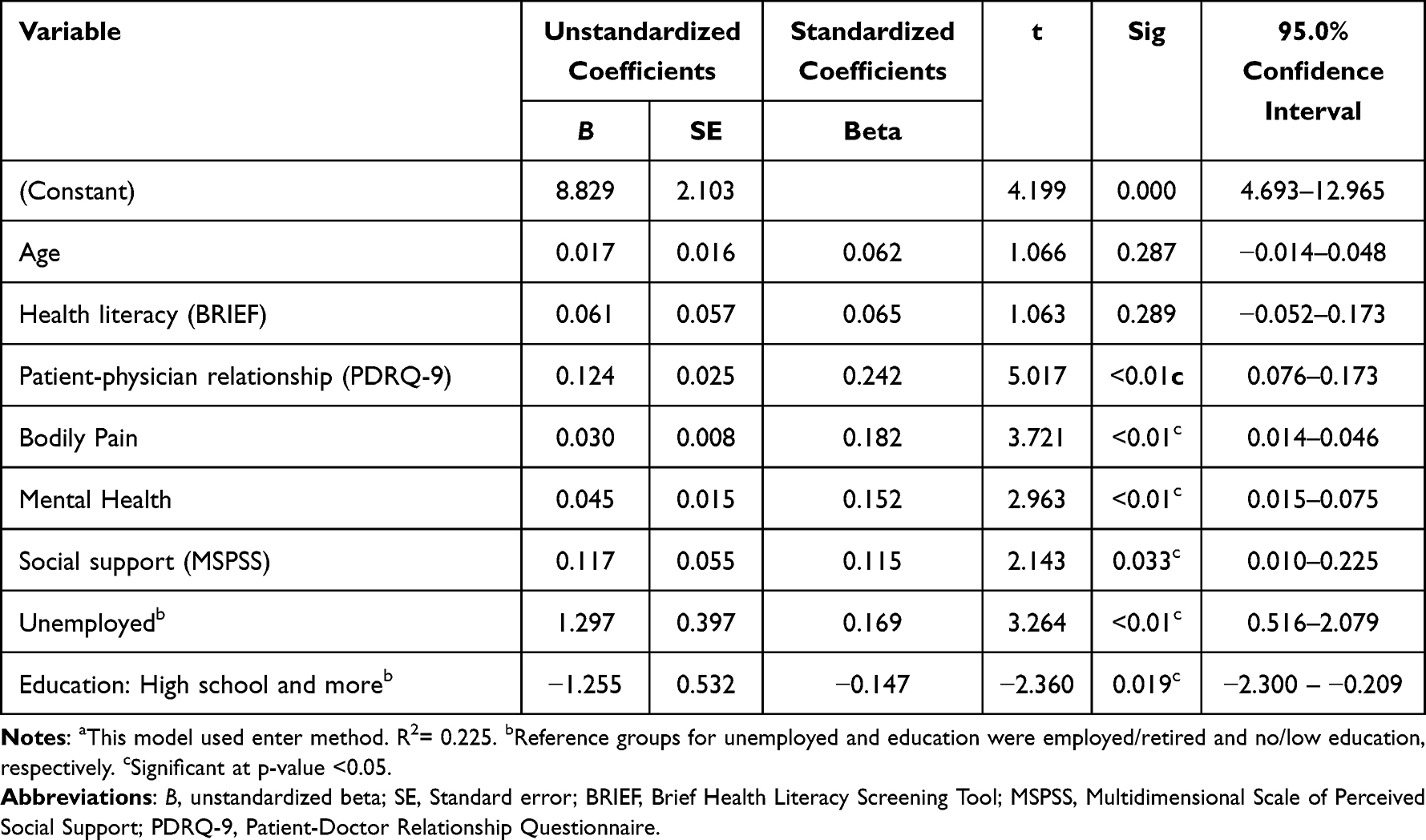 |
Table 3 Predictors of Medication Adherence Using Multiple Linear Regressiona |
Discussion
The current study aimed to determine the impact of various influencing factors concerning health literacy, social support, the patient-physician relationship, and HRQoL domains on medication adherence among Omani patients with CVD.
The average participants score on the adherence scale was 24.6 out of 28, reflecting a good score. In line with the current study finding, a study was conducted in Jordan, which showed patients with hypertension have a good level of adherence.22 However, a previous study conducted in Lebanon23 and Oman5 showed that patients with chronic diseases have a low level of adherence, which was supported by findings of a recent systematic review.4 This variation in adherence level among the literature suggests that the cultural and sociodemographic factors of the patients influence adherence behavior. For example, in the current study, several factors, including patient-physician relationship, bodily pain, mental health, and Social support, were significantly associated with medication adherence among patients with CVD.
Some demographic variables like unemployment and education: high school and more were significant predictors of adherence in the current study. We found that unemployment predicted better adherence while high education predicted less adherence. However, most previous studies results were inconclusive or did not identify demographics as significant predictors of adherence.23,24 The possible explanation for the significant association in the current study is that unemployed participants were not busy with their duties and could remember to take and refill their medication on time. In Oman, unemployment does not affect adherence level because healthcare is free, and participants are not expected to purchase medicine. On the other hand, participants who completed high school or more showed less adherence which means that higher education does not necessarily mean high health literacy. These participants may not correctly understand their chronic conditions and the necessity for their medications. Education on diseases’ nature and medication action will improve and ensure patients’ adherence for extended periods.25 Also, they might be busy with their duties and work, which keeps them engaged from remembering to take medications on schedule. More qualitative research is required to investigate the influence of employment and educational status on patients’ adherence behavior, which could also vary in different populations and cultures.
The patient-physician relationship was the first positive predictor for adherence in the current study; this is in line with previous studies.26–28 A Lebanese study elaborated more on the nature of the relationship and stressed the importance of therapeutic communication between patients and physicians. When the health care providers are sensitive to patients’ needs; provide full instructions about the disease and medication, adherence will increase significantly.23 Furthermore, involving the patients in the decision-making process could enhance the patient-physician relationship and, consequently, adherence.29,30 Conversely, poor communication could lead to non-adherence31 and several medication errors.32 Therefore, more courses should be provided to health care providers to improve their communication and capacity to deal with patients, which reflect positively on patients’ adherence and lead to unnecessary errors.
Social support is another positive significant predictor variable. Previous research reported similar findings.33–35 The explanation for the relationship between social support and health can be found in the work of Cohen and Wills36 and Cohen,37 who provide two popular theories (1) the stress-buffering and (2) primary effect pathways. In this regard, researchers distinguish between structural and functional social support.34 Functional social support is more significant in stressful conditions, and structural social support has been demonstrated to primarily impact health, enhancing adherence.34,38 Structural social support operationally refers to living with someone like a spouse or friend. Functional social support operationally refers to the assistance and motivation the individual receives from his/her social network.34 In Oman’s context, family, friends, and significant others may reinforce the positive health messages that patients with CVD receive, which may result in greater adherence to medication regimens and vice versa is true. That is, there is a bidirectional relationship between both variables. Therefore, healthcare providers should be careful and target the families and friends of patients with CVD in their education plans to improve patients’ adherence to medication. It would also be necessary for healthcare providers to emphasize the significance of structural and functional social support to reduce stress and improve patients’ healthy behavior, such as medication adherence.
Another significant positive predictor is mental health. There is a significant positive relationship between mental health and adherence. A study conducted in Ghana reported similar results.39 A study in Lebanon showed a positive association between depression and/or anxiety and non-adherence.23 Stress was also significantly associated with non-adherence to hypertension medication.39 Several health psychological theories have been used to predict and explain the relationship between health and medication adherence.40 For example, the health belief model,41,42 the theory of reasoned action,43 and the theory of planned behavior44 are the most widely used theories.45,46 The self-regulatory model47 and the transactional model of stress and coping48 have also been used but are less common. Overall there is no physical health without mental health.49 Therefore, healthcare providers must evaluate and promote the patients’ mental health to promote adherence, especially in patients with chronic illnesses. Mental health should be an integral component of any future educational plan. Healthcare providers should be trained to identify signs of poor mental health and ready to refer patients to mental health services to promote their health.
In the current study, bodily pain was another positive predictor of medication adherence, which is inconsistent with Al-Hajje,23 who found a negative association between chronic pain and adherence to medication. This finding may explain that patients with more pain would appreciate the necessity of medicine, which describe their high adherence level compared to patients with less or no pain. Although the current study did not differentiate between acute and chronic pain, which may explain the inconsistencies between the studies’ findings, more research is required to validate the recent results. It is important to note that patients who do not report symptoms or bodily pain, as in HTN, may have less medication adherence compared to other CVD diseases, such as HF or IHD.
Although health literacy is a concept of recent interest, we found no relationship between medication adherence and health literacy. Our finding could be explained by the use of four-items tool that show low reliability. However, our findings are consistent with findings of some studies reported a current systematic review;50 This review showed conflicting findings of the relationship between health literacy and medication adherence and conclude that the relationship maybe is indirect and mediated or moderated by other factors. The review also concluded that variations in tools used to measure health literacy, population demographics, and cultures maybe the reason for this variation.50
This study did not come without limitations; the study’s cross-sectional design did not produce a causal relationship between the study variables. Hence, longitudinal studies are required to establish a causal relationship. Another limitation is the use of convenience sample, which affect the generalizability of the study findings. However, this study is national, using multiple centers and recruited heterogeneous sample representing all governorates across the country. Another limitation is the self-reporting technique which opens the door to recall bias and causes an overrating of some of the study variables, such as medication adherence. Health literacy is a concept of interest nowadays. However, we found no significant relationship between adherence and health literacy; this could be due to the tool used to examine health literacy, which demonstrated a low Cronbach’s alpha (α = 0.53) in the current study. Although BRIEF’s construct validity was established in the original study and correlated with other health literacy tools such as Short Test of Functional Health Literacy in Adults (STOFHLA) and the Rapid Estimate of Adult Literacy (REALM). Future studies should examine BRIEF’s validity and reliability in different population.13 Future studies should review this vital concept concerning adherence to medication and healthy behaviors using different tools. Moreover, future studies should focus on creating interventions to improve social support, mental health, and patient-physician relationship to increase medication adherence; these studies should target patients and healthcare providers. Future studies could examine other factors like side effects of medication and how it influences adherence level.
Conclusion
Participants’ adherence to medication was rated as good. Participants and healthcare providers should be more oriented toward the patient-physician relationship, bodily pain, mental health, and social support as factors that promote their adherence. Health literacy is a factor that need to be considered and examined in light of other factors affecting adherence. Adherence is a multifactorial problem in which patients, families, and health team members play a role. Decision makers need to consider these factors and develop comprehensive educational and interventional programs to improve patients with CVD adherence to medication.
Data Sharing Statement
The dataset used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
The authors acknowledge all patients participated in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by The Research Council (TRC) grant number (RC/RGCON/AHCC/18/01).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Roth GA, Mensah GA, Johnson CO, et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: update from the GBD 2019 study. J Am Coll Cardiol. 2020;76(25):2982–3021. doi:10.1016/J.JACC.2020.11.010
2. Al-Mawali A. Non-communicable diseases: shining a light on cardiovascular disease, Oman’s biggest killer. Oman Med J. 2015;30(4):227–228. doi:10.5001/omj.2015.47
3. Walsh CA, Cahir C, Tecklenborg S, Byrne C, Culbertson MA, Bennett KE. The association between medication non-adherence and adverse health outcomes in ageing populations: a systematic review and meta-analysis. Br J Clin Pharmacol. 2019;85(11):2464–2478. doi:10.1111/bcp.14075
4. Mahmood S, Jalal Z, Hadi MA, Khan TM, Haque MS, Shah KU. Prevalence of non-adherence to antihypertensive medication in Asia: a systematic review and meta-analysis. Int J Clin Pharm. 2021;43(3):486–501. doi:10.1007/S11096-021-01236-Z
5. Al-Noumani H, Al-Harrasi M, Jose J, Al-Naamani Z, Panchatcharam SM. Medication adherence and patients’ characteristics in chronic diseases: a national multi-center study. Clin Nurs Res. 2022;31(3):426–434. doi:10.1177/10547738211033754
6. Simon ST, Kini V, Levy AE, Ho PM. Medication adherence in cardiovascular medicine. BMJ. 2021;374. doi:10.1136/bmj.n1493
7. Cramer JA, Roy A, Burrell A, et al. Medication compliance and persistence: terminology and definitions. Value Health. 2008;11(1):44–47. doi:10.1111/j.1524-4733.2007.00213.x
8. Chaudri NA. Adherence to long-term therapies evidence for action. Ann Saudi Med. 2004;24(3):221. doi:10.5144/0256-4947.2004.221
9. Lee YM, Kim RB, Lee HJ, et al. Relationships among medication adherence, lifestyle modification, and health-related quality of life in patients with acute myocardial infarction: a cross-sectional study. Health Qual Life Outcomes. 2018;16(1). doi:10.1186/s12955-018-0921-z
10. Suhail M, Saeed H, Saleem Z, et al. Association of health literacy and medication adherence with health-related quality of life (HRQoL) in patients with ischemic heart disease. Health Qual Life Outcomes. 2021;19(1):1–13. doi:10.1186/s12955-021-01761-5
11. Gast A, Mathes T. Medication adherence influencing factors - an (updated) overview of systematic reviews. Syst Rev. 2019;8(1):1–17. doi:10.1186/s13643-019-1014-8
12. Bujang MA, Sa’at N, Sidik TMITAB. Determination of minimum sample size requirement for multiple linear regression and analysis of covariance based on experimental and non-experimental studies. Epidemiol Biostat Public Health. 2017. doi:10.2427/12117
13. Haun J, Noland-dodd V, Varnes J, Graham-pole J, Rienzo B, Donaldson P. Testing the brief health literacy screening tool: implications for utilization of a BRIEF health literacy indicator. Fed Pract. 2009;26(12):24–31.
14. Zimet GD, Dahlem NW, Zimet SG, Farley GK. The multidimensional scale of perceived social support. J Pers Assess. 1988;52(1):30–41. doi:10.1207/s15327752jpa5201_2
15. Alzayyat A, Al-Gamal E, Ahmad MM. Psychosocial correlates of internet addiction among Jordanian university students. J Psychosoc Nurs Ment Health Serv. 2015;53(4):43–51. doi:10.3928/02793695-20150309-02
16. Norris AE, Aroian KJ, Nickerson DM. Premigration persecution, postmigration stressors and resources, and postmigration mental health: a study of severely traumatized U.S. Arab immigrant women. J Am Psychiatr Nurses Assoc. 2011;17(14):283–293. doi:10.1177/1078390311408900
17. Calderón C, Lorenzo-Seva U, Ferrando PJ, et al. Psychometric properties of the pdrq-9 in cancer patients: patient-doctor relationship questionnaire. Psicothema. 2021;33(2):304–311. doi:10.7334/psicothema2020.393
18. Zenger M, Schaefert R, Van Der Feltz-Cornelis C, Brähler E, Häuser W. Validation of the patient-doctor-relationship questionnaire (PDRQ-9) in a representative cross-sectional German population survey. PLoS One. 2014;9(3):1–8. doi:10.1371/journal.pone.0091964
19. Carver DJ, Chapman CA, Thomas VS, Stadnyk KJ, Rockwood K. Validity and reliability of the medical outcomes study short form-20 questionnaire as a measure of quality of life in elderly people living at home. Age Ageing. 1999;28(2):169–174. doi:10.1093/ageing/28.2.169
20. Buszko K, Obońska K, Michalski P, et al. The Adherence Scale in Chronic Diseases (ASCD). The power of knowledge: the key to successful patient — health care provider cooperation. Med Res J. 2016;1(1):37–42. doi:10.5603/mrj.2016.0006
21. WHO. Process of translation and adaptation of instruments. World Health Organization; 2009. Available from: http://www.who.int/substance_abuse/research_tools/translation/en.
22. Al-daken LI, Eshah NF. Self-reported adherence to therapeutic regimens among patients with hypertension. Clin Exp Hypertens. 2017;39(3):264–270. doi:10.1080/10641963.2016.1247164
23. Al-Hajje A, Awada S, Rachidi S, et al. Factors affecting medication adherence in Lebanese patients with chronic diseases. Pharm Pract. 2015;13(3):4–12. doi:10.18549/PharmPract.2015.03.590
24. Moore T, Neher JO, Safranek S. FPIN’s clinical inquiries: improving medication adherence in patients with comorbidities. Am Fam Physician. 2011;84(7):1–2.
25. Contreras-Vergara A, Sifuentes-Franco S, Haack S, et al. Impact of pharmaceutical education on medication adherence and its clinical efficacy in patients with type 2 diabetes and systemic arterial hypertension. Patient Prefer Adherence. 2022;16:1999–2007. doi:10.2147/PPA.S370323
26. Greenberg KL, Leiter E, Donchin M, Agbaria N, Karjawally M, Zwas DR. Cardiovascular health literacy and patient–physician communication intervention in women from disadvantaged communities. Eur J Prev Cardiol. 2019;26(16):1762–1770. doi:10.1177/2047487319853900
27. Laufs U, Rettig-Ewen V, Böhm M. Strategies to improve drug adherence. Eur Heart J. 2011;32(3):264–268. doi:10.1093/eurheartj/ehq297
28. Petrovic K, Blank TO. The Andersen–Newman behavioral model of health service use as a conceptual basis for understanding patient behavior within the patient–physician dyad: the influence of trust on adherence to statins in older people living with HIV and cardiovascular disease. Cogent Psychol. 2015;2(1):1038894. doi:10.1080/23311908.2015.1038894
29. Fiorillo A, Barlati S, Bellomo A, et al. The role of shared decision-making in improving adherence to pharmacological treatments in patients with schizophrenia: a clinical review. Ann Gen Psychiatry. 2020;19(1). doi:10.1186/s12991-020-00293-4
30. Schoenthaler A, Rosenthal DM, Butler M, Jacobowitz L. Medication adherence improvement similar for shared decision-making preference or longer patient-provider relationship. J Am Board Fam Med. 2018;31(5):752–760. doi:10.3122/jabfm.2018.05.180009
31. Noble LM. Doctor-patient communication and adherence to treatment. Adherence Treat Med Cond. 2020;51–82. doi:10.1201/9781003072348-5
32. Hassan I. Avoiding medication errors through effective communication in healthcare environment. Mov Health Exerc. 2018;7(1):113–126. doi:10.2139/ssrn.3573437
33. Cavalari E, Nogueira MS, Fava SMCL, Cesarino CB, Martin JFV. Adherence to treatment: study among patients with arterial hypertension in outpatient follow-up. Rev Enferm UERJ. 2012;20(1):67–72.
34. Magrin ME, D’Addario M, Greco A, et al. Social support and adherence to treatment in hypertensive patients: a meta-analysis. Ann Behav Med. 2015;49(3):307–318. doi:10.1007/s12160-014-9663-2
35. Wu JR, Frazier SK, Rayens MK, Lennie TA, Chung ML, Moser DK. Medication adherence, social support, and event-free survival in patients with heart failure. Health Psychol. 2013;32(6):637–646. doi:10.1037/a0028527
36. Cohen S, Wills TA. Stress, social support, and the buffering hypothesis. Psychol Bull. 1985;98(2):310–357. doi:10.1037/0033-2909.98.2.310
37. Cohen S. Social relationships and health. Am Psychol. 2004;59(8):676–684. doi:10.1037/0003-066X.59.8.676
38. Barth J, Schneider S, Von Känel R. Lack of social support in the etiology and the prognosis of coronary heart disease: a systematic review and meta-analysis. Psychosom Med. 2010;72(3):229–238. doi:10.1097/PSY.0b013e3181d01611
39. Kretchy IA, Owusu-Daaku FT, Danquah SA. Mental health in hypertension: assessing symptoms of anxiety, depression and stress on anti-hypertensive medication adherence. Int J Ment Health Syst. 2014;8:1. doi:10.1186/1752-4458-8-25
40. Munro S, Lewin S, Swart T, Volmink J. A review of health behaviour theories: how useful are these for developing interventions to promote long-term medication adherence for TB and HIV/AIDS? BMC Public Health. 2007;7:104. doi:10.1186/1471-2458-7-104
41. Becker MH, Haefner DP, Kasl SV, Kirscht JP, Maiman LA, Rosenstock IM. Selected psychosocial models and correlates of individual health-related behaviors. Med Care. 1977;27–46. doi:10.1097/00005650-197705001-00005
42. Rosenstock IM. The health belief model and preventive health behavior. Health Educ Behav. 1977;2(4):354–386. doi:10.1177/109019817400200405
43. Ajzen I, Fishbein M. The prediction of behavioral intentions in a choice situation. J Exp Soc Psychol. 1969;5(4):400–416. doi:10.1016/0022-1031(69)90033-X
44. Ajzen I. The theory of planned behavior. Organ Behav Hum Decis Process. 1991;50(2):179–211. doi:10.1016/0749-5978(91)90020-T
45. Bandura A, Adams NE. Analysis of self-efficacy theory of behavioral change. Cognit Ther Res. 1977;1(4):287–310. doi:10.1007/BF01663995
46. Bandura A. Social Foundations of Thought and Action: A Social Cognitive Theory. Prentice-Hall, Inc; 1986.
47. Leventhal H, Diefenbach M, Leventhal EA. Illness cognition: using common sense to understand treatment adherence and affect cognition interactions. Cognit Ther Res. 1992;16(2):143–163. doi:10.1007/BF01173486
48. Folkman S. Personal control and stress and coping processes: a theoretical analysis. J Pers Soc Psychol. 1984;46(4):839–852. doi:10.1037/0022-3514.46.4.839
49. Kolappa K, Henderson DC, Kishore SP. No physical health without mental health: lessons unlearned? Bull World Health Organ. 2013;91(1):3. doi:10.2471/BLT.12.115063
50. Hyvert S, Yailian AL, Haesebaert J, et al. Association between health literacy and medication adherence in chronic diseases: a recent systematic review. Int J Clin Pharm. 2022;45(1):38–51. doi:10.1007/s11096-022-01470-z
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.