Back to Archived Journals » Robotic Surgery: Research and Reviews » Volume 6
Robotics in Cleft Surgery: Origins, Current Status and Future Directions
Authors Al Omran Y, Abdall-Razak A ![]() , Ghassemi N, Alomran S, Yang D
, Ghassemi N, Alomran S, Yang D ![]() , Ghanem AM
, Ghanem AM
Received 18 July 2019
Accepted for publication 29 November 2019
Published 24 December 2019 Volume 2019:6 Pages 41—46
DOI https://doi.org/10.2147/RSRR.S222675
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Masoud Azodi
Yasser Al Omran,1 Ali Abdall-Razak,2 Nader Ghassemi,3 Samar Alomran,4 Ding Yang,5 Ali M Ghanem6
1Department of Plastic Surgery, Birmingham Women’s and Children’s Hospital NHS Foundation Trust, Birmingham, UK; 2Imperial College of Medicine, London, UK; 3Department of Surgery, University Hospital North Midlands NHS Foundation Trust, Stoke-On-Trent, UK; 4Salmaniya Medical Complex, Manama, Kingdom of Bahrain; 5University Hospital North Midlands NHS Foundation Trust, Stoke-On-Trent, UK; 6Academic Plastic Surgery Group, Barts and the London School of Medicine and Dentistry, London, UK
Correspondence: Yasser Al Omran
Department of Plastic Surgery, Birmingham Women’s and Children’s Hospital NHS Foundation Trust, Birmingham, UK
Email [email protected]
Abstract: The field of robotic surgery is an exciting and growing field that has bolstered its way to become a mainstream application in a number of surgical disciplines. The application of robotic surgery in cleft surgery is novel and has captivated many with the benefit it provides: the slender and small arms with wrist articulation at the instrument tip; motion scaling; tremor elimination; and high fidelity, three-dimensional visualization make the robot a very attractive platform for use in confined spaces with small surgical targets. The story of the origin of robotic surgery in cleft surgery is an interesting one, and one that has arisen from other allied surgical specialities to render robotic cleft surgery as its own specialised field. A field that has coined its own terms and has demonstrated a number of applications for its use. This review details the origins of robotic cleft surgery, its evolution and its current status and elaborates on future directions to enhance its application.
Keywords: cleft lip, cleft palate, robotics
Introduction
The use of robotics in surgery has captivated the imagination of many. It remains a field that is rapidly expanding, with many procedures becoming routinely classed as “robot-assisted.” Cleft surgery is a challenging procedure because of the small boundaries of the infant oral cavity, and the fine dissection and tissue handling warranted for many of these procedures.1–3 The operations performed are challenging for the surgeon as it requires awkward postures, movements and ambidexterity for success.4 Teaching trainees the fine art of this specialist surgery is also difficult because of the limited access and visibility to teach and perform. The use of a surgical robot in the field of cleft surgery offers the advantage of improved access, precision,5 visualization,6 instrument manipulation,7 ergonomics,8 tremor reduction,4 and ambidexterity.9 Therefore, the coupling of robotics and cleft surgery remains a potentially very fruitful avenue that justifies a review. The aim of this review is to explore the background of robotics in cleft surgery, focussing on sentinel studies that have been instrumental in the development of the field. It also brings to the reader’s attention to particular areas that are still in need of improvement and suggests how these may be achieved.
Paediatric Robotic Surgery
The first landmark papers that explored the role of robotic surgery in children occurred in the 1990s when Partin and colleagues and Okada and colleagues first reported on the use of robot assistance for surgery in children in the form of an extracorporeal camera holder.10,11 Technology evolved to more established platforms and in April 2001, Meininger and colleagues published the first cases of robotic surgery in children undergoing endoscopic Nissen fundoplication with a telemanipulatory robot system in two children using this platform.12,13 Shortly afterwards, the first robotic urological procedure in a child was undertaken in March 2002 by Peters and colleagues who performed a pyeloplasty using the da Vinci® Surgical System.14 In fact, the field has developed exponentially and in 2013 Cundy and colleagues published a 10-year review of paediatric robotic surgery.14 They highlight the accelerated rate of publications and reported case volumes in this period.14 This widespread adoption of robotic surgery in paediatric surgery is presumably related to the advantages that robotics may offer patients: faster recovery, less post-operative pain, smaller incisions and scars and a shorter hospital stay.14 In earlier years of development of paediatric robotic surgery, where fundoplication and cholecystectomy cases remained salient, there has been a change in paediatric robotic surgery cases with genitourinary procedures forming a greater percentage of case volumes. Additionally, paediatric robotic surgery has spread far and wide, with a recent review showing that publications of robotic surgery have originated from 18 countries. In total, 52 institutions were represented in the literature.14
Transoral Robotic Surgery (TORS) in Adults
Historically, one of the challenges behind open surgery of the laryngopharyngeal complex for cancer resection remains the balance between providing access, safe resection and preservation of normal structures. Unfortunately, operations in this area produced inconsistent and poor results with consequences including poor speech and swallowing functions, tracheostomy tube dependence, gastrostomy tube dependence, and suboptimal quality of life.15 In pursuit of a balance between survival and post-treatment function, surgeons have continued to develop minimally invasive techniques and approaches to the larynx/hypopharynx. The most rapidly advancing techniques in this domain is Transoral Robotic Surgery (TORS). The principle behind the advent of TORS is to be able to reliably perform state-of-the-art oncological resection of the primary tumour through a minimally invasive transoral approach. This technique affords surgeons exceptional views of the larynx and hypopharynx with great manoeuvrability in difficult to access areas.15 As a result, negative margins and preservation of normal laryngeal structures have become increasingly possible.15
TORS surgery is facilitated by remote-controlled miniaturized surgical instruments and magnified visualization with a high-definition three-dimensional camera. It has proven to be an effective alternative to open surgery, with or without a mandibulotomy approach for oropharyngeal cancer in a large number of studies since its approval by the Food and Drug Administration (FDA) in 2009 for T1 and T2 lesions.16 In a large multicentre study to assess its feasibility, TORS demonstrated decreased rates of postoperative complications, improved functional outcomes, and favourable oncological results.17 In the year following clearance of the da Vinci TORS system, the otolaryngology community has enthusiastically embraced this technology and was adopted across the USA. As in other specialties, we are also beginning to see trends towards market consolidation, and so for a large number of surgeons, it has become a standard-of-care among other treatment modalities in oropharyngeal squamous cell carcinoma staged T1–T2.18–20 With laryngeal cancers, TORS has been explored for minimally invasive surgery of supraglottic and glottic lesions, as well as for total laryngectomy. The role of TORS is continuing to expand to thyroid and sleep surgery with trans-axillary thyroidectomies and lingual tonsillectomy being performed via TORS.21,22
Transoral Robotic Surgery (TORS) in Children
The use of TORS in the paediatric population is in its infancy compared to that of adults, this may be in part due to the inherent challenges that the paediatric patients bring forth towards the surgeon: the smaller-sized anatomy, the narrower working field and the increased risk of causing iatrogenic injury. In a recent study, the use of TORS surgery in the paediatric population was reviewed by Erkul and colleagues.23 The authors report on TORS surgery being performed on 41 patients over a 10-year period.23 The cases included 16 lingual tonsillectomies, 9 base of tongue and lingual tonsillectomies, 2 malignant diseases in the oropharynx (a high-grade undifferentiated sarcoma and a biphasic synovial sarcoma), one tongue base thyroglossal duct cyst, 11 laryngeal cleft cyst, 1 posterior glottic stenosis, and 1 congenital true vocal cord paralysis surgeries.23 In these 41 subjects, 37 TORS procedures were completed successfully and the completion rate was 90.2%, with the other 4 cases needing to be converted to an open approach.23 In another recent case series of TORS in the paediatric population, the authors highlight key components that are essential for success with TORS:
- Having a team of at least two surgeons who have experience in robotic surgery.
- Selecting older and bigger children to enable better access with the surgical instruments, and excluding patients with malignancy and vascular tumours.
- Securing the airway with the appropriate laser-safe endotracheal or tracheostomy tubes.
- Having appropriate exposure.
- Securing surgical access with the robotic arms to allow for unrestricted mobility.
- Having the first assistant seated at the head of the operating table; specifically around the patient’s head and therefore in the best position to protect the airway while assisting the main operating surgeon detect and remedy such problems early in addition to providing assistance in the operative field.24
Most of the instruments designed for TORS are based on general or urological surgeries and so it is necessary for the future innovation and advancement of paediatric robotic airway surgery to have specialized airway instrumentation. As technologies continue to advance with smaller optics, arms and instruments, the potential applications of TORS will continue to expand as the challenges once encountered will become less apparent.24
Transoral Robotic Cleft Surgery (TORCS)
The recent advances in the use of robotic surgical systems in transoral surgery with TORS to grow beyond the domains of traditional laparoscopic applications prompted authors to explore other avenues to deliver other surgical applications. A seminal paper that expanded beyond the role of TORS was initiated in 2013 when a group from Philadelphia evaluated the feasibility of using a robotic surgical telemanipulator system to perform superior-based “Hogan”-style posterior pharyngeal flaps on thee fresh cadaveric human specimens. The flaps in all 3 specimens were performed successfully, the learning curve for using the robot system was steep in part due to the the lack of haptic feedback, which is important not only for delicate handling of tissues, but also for sensing areas of physical interference between the robotic arms. Nevertheless, the operating surgeons report distinct advantages using the robotic system: 1) the system provided great visualisation of the working field; 2) it allowed for greater instrument manoeuvrability and handing and 3) while many surgeons report significant neck fatigue after performing posterior pharyngeal flap surgery, the robot console was ergonomically designed in that minimal neck and torso strain was encountered by the surgeons. Overall, the instrumentation and setup and the overall use of the system were ergonomic, safe and feasible.25
The concept of Transoral robotic cleft surgery (TORCS) was further enhanced by a group from Oxford who realised that the space required to operate combined with the abnormal anatomy can make cleft surgery taxing to the surgeon. Using a paediatric airway manikin, the authors evaluated all possible permutations of patient and robotic instrument configurations with the daVinci Si Surgical System to determine the optimal visualization and surgical access to simulate posterior pharyngeal wall surgery before performing a full robot-assisted cadaveric Hynes pharyngoplasty, whereby two superiorly placed flaps are used to augment the posterior pharyngeal wall in order to bridge the gap in velopharyngeal incompetence. The use of a bedside assistant was used in the setup; this enabled both hands of the surgeon to work via the miniaturized wristed surgical tools afforded by the robotic system as well as the hands of the assistant as well. The use of a more available surgical assistant is perhaps the most significant advantage of robotic-assistant trans-oral approach and the authors draw parallels to that of having an assistant in open surgical approaches, which would not otherwise be possible in transoral approaches.26 The authors note that contact of the ring of the mouth gage when working at the extremes of the operative field was a limitation but was immediately recognised.26 Ultimately, the authors concluded that these findings demonstrate that trans-oral robotic cleft surgery (TORCS) is theoretically feasible for safe intra-oral cleft palate and pharyngeal surgery, especially when smaller 5-mm instruments are used.26
The aforementioned pilot studies that evaluated the use of TORCS occurred in simulated environments involving cadaveric specimens. A key question remains, will this work in true clinical environments? After trialling the da Vinci Surgical Robot on a cadaveric specimen, Nasser Nadjmi, a Professor of Cranio-Maxillofacial surgery from the University of Antwerp and colleagues performed a modified Furlow Palatoplasty in 10 consecutive patients with palatal clefts for a variety of indications; five patients had isolated cleft palate, two patients had complete unilateral cleft lip and palate, two patients had complete bilateral cleft lip and palate, and one patient had submucosal cleft palate. Six of the patients were male, 4 were female and ages ranged from 9 months to 12 months. He completed the nasal and oral mucosal layer of repair without the da Vinci Surgical Robot. The results were compared to controls without the use of the robot.27 In summary, the mean surgical duration was 122 ± 8 mins in patients who underwent the TORCS approach, which included a 35-min docking time compared to 87 ± 6 mins without the robot. No intraoperative complications were noted and in the patients who underwent a TORCS approached had a significantly shorter hospital stay compared to controls.27 The authors highlight that the TORCS approach enabled delicate soft-tissue handling, excellent 3D depth perception, increased freedom of motion, tremor reduction and relatively easy intraoral suturing.27 These findings are encouraging as they demonstrate that TORCS is clinically feasible and with further development may categorically supersede non-robotic cleft surgery repair.
Moving Forward
The previous studies have highlighted that robotic cleft palate surgery repair remains technically and clinically feasible. However, there remain significant hurdles that need to be passed before a “tipping point” can occur whereby clinical application of robotic cleft repair becomes a reality. Some of these challenges are intuitive, such as the high start-up costs, training of staff and ethical considerations; others may be conspicuous such as the lack of haptic feedback and inappropriate contact of the instruments to structures as has been noted in the previous studies. However, one challenge that may not be so conspicuous is the number of possible permutations available. For example, which one of the robotic systems should an institute invest in? What about the size of the instrument? Is one system easier to use than the other? These questions are valid and warrant an answer before limited resources can be invested to enhance the field. In a landmark paper, Podolsky and colleagues have helped clarify some of these answers. The authors developed a high-fidelity cleft palate simulator that allowed for performance of all the critical steps of a cleft palate repair and evaluated the da Vinci Si is system that can accommodate 5-mm instruments, and the newer da Vinci Xi is the new system which can only accommodate 8-mm instruments in performing cleft palate repair on this simulator.4 The authors note that Cleft palate repair with the da Vinci Xi system was superior to the da Vinci Si system with respect to better elimination of arm repositioning, improved instrument excursion in the posterior oral cavity, less severe instrument oral aperture contact, and an ability to use an ideal wrist orientation for most of the surgical steps.4 The difference in performance between the two robotic systems is due to the slimmer robotic arms of the da Vinci Xi system and the more compact articulation and longer length of the 8-mm instruments which allowed for better movement during each surgical step.4 Despite the advantages of the 8-mm instruments with the da Vinci Xi system, their larger size can restrict instrument and endoscope excursion when manipulating the endoscope for close-up viewing.4 At the time, 5-mm instruments cannot be used with da Vinci Xi system and so this permutation was not explored by the authors.
Furthermore, the evaluation of key critical steps in the simulator presented in Podolsky and colleagues articles provide a connotation to competency-based surgical training. Competency-based training is the idea that learners advance based on the quality of the training, rather than the quantity of the training and is a domain that has developed significant traction over recent years.28,29 Methods of assessment have been demonstrated through Hand motion analysis (HMA),30–32 and global rating scales and other surgical-specific outcomes, but their article suggests that this application may be applied to robotic cleft surgery (Figure 1).
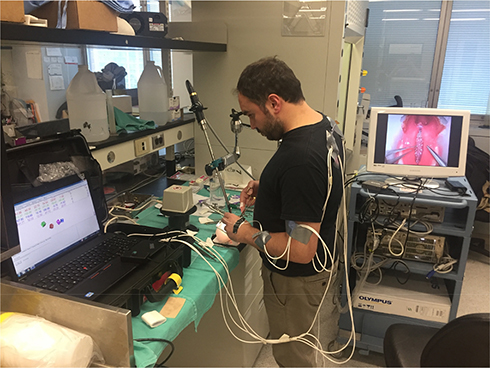 |
Figure 1 Hand motion analysis is used to provide an objective assessment of cleft surgery. |
Furthermore, the authors note important limitations of the robotic systems: First, neither 5- nor 8-mm could be used for soft tissue dissection without interfering with the retractor. Second, the da Vinci Systems lack providing the surgeon with haptic feedback, which is important, as it can prevent excessive tissue damage especially in the smaller confines of an infant’s mouth. The authors additionally advocate for the development of “smart haptics” with the ability to sense impending collisions; setting workspace, force, and speed limits on the instruments; and using protective oral retractors as adding haptics alone would fail to prevent sudden unintended movement of the instruments because of user error or system malfunction that may cause substantial injury and may further improve the safety of the procedure. Ultimately, current instruments that are used in robotic cleft palate surgery require further optimization to fully take advantage of the robot’s capabilities to ensure greater efficacy.
Conclusions
Robotic cleft surgery is a new and exciting field that holds numerous advantages to both patients and surgeons. Previous research in allied health specialities has paved the way to the feasibility studies of robotic cleft surgery. These studies have shown that robotic cleft surgery is feasible and so future research should focus on optimization. Future work is also necessary to develop more suitable instrumentation to safely compare outcomes of a full robotic cleft palate repair to the traditional approach in real patients before widescale implementation can be adopted. Importantly, training and validation of simulators for the purposes of robotic cleft surgery are needed to provide an assessment of surgeons who want to use surgical robots before it becomes more mainstream in cleft surgery.
Finally, the use of surgical robots at present introduces economic challenges to implementation because of increased operative time and high capital and operating costs and it is hoped that over time, costs will reduce and performance will increase as more systems are developed in the future.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Vadodaria S, Watkin N, Thiessen F, Ponniah A. The first cleft palate simulator. Plast Reconstr Surg. 2007;120(1):259–261. doi:10.1097/01.prs.0000264394.27150.0d
2. Nagy K, Mommaerts MY. Advanced s(t)imulator for cleft palate repair techniques. Cleft Palate Craniofac J. 2009;46(1):1–5. doi:10.1597/08-004.1
3. Şentürk S. The simplest cleft palate simulator. J Craniofac Surg. 2013;24(3):1056. doi:10.1097/SCS.0b013e31828f2679
4. Podolsky DJ, Fisher DM, Wong KW, Looi T, Drake JM, Forrest CR. Evaluation and implementation of a high-fidelity cleft palate simulator. Plast Reconstr Surg. 2017;139(1):85e–96e. doi:10.1097/PRS.0000000000002923
5. Selber JC, Baumann DP, Holsinger FC. Robotic latissimus dorsi muscle harvest. Plast Reconstr Surg. 2012;129(6):1305–1312. doi:10.1097/PRS.0b013e31824ecc0b
6. Biffi R. Dealing with robot-assisted surgery for rectal cancer: current status and perspectives. World J Gastroenterol. 2016;22(2):546. doi:10.3748/wjg.v22.i2.546
7. Alrasheed T, Liu J, Hanasono MM, Butler CE, Selber JC. Robotic microsurgery. Plast Reconstr Surg. 2014;134(4):794–803. doi:10.1097/PRS.0000000000000550
8. Maan ZN, Gibbins N, Al-Jabri T, D’Souza AR. The use of robotics in otolaryngology–head and neck surgery: a systematic review. Am J Otolaryngol. 2012;33(1):137–146. doi:10.1016/j.amjoto.2011.04.003
9. Mucksavage P, DC K, JY L. The da Vinci(®) surgical system overcomes innate hand dominance. J Endourol. 2011;25(8):1385–1388. doi:10.1089/end.2011.0093
10. Partin AW, Adams JB, Moore RG, Kavoussi LR. Complete robot-assisted laparoscopic urologic surgery: a preliminary report. J Am Coll Surg. 1995;181(6):552–557.
11. Okada S, Tanaba Y, Yamauchi H, Sato S. Single-surgeon thoracoscopic surgery with a voice-controlled robot. Lancet. 1998;351(9111):1249. doi:10.1016/S0140-6736(98)24017-7
12. Meininger DD, Byhahn C, Heller K, Gutt CN, Westphal K. Totally endoscopic Nissen fundoplication with a robotic system in a child. Surg Endosc. 2001;15(11):1360. doi:10.1007/s00464-001-4200-3
13. Meininger D, Byhahn C, Markus BH, Heller K, Westphal K. Roboterassistierte, endoskopische Fundoplikatio nach Nissen bei Kindern Hämodynamik, Gasaustausch und anästhesiologisches Management [Total endoscopic Nissen fundoplication with the robotic device “da Vinci” in children. Hemodynamics, gas exchange, and anesthetic management]. Anaesthesist. 2001;50(4):271–275. German. doi:10.1007/s001010051001
14. Cundy TP, Shetty K, Clark J, et al. The first decade of robotic surgery in children. J Pediatr Surg. 2013;48(4):858–865. doi:10.1016/j.jpedsurg.2013.01.031
15. Dziegielewski PT, Kang SY, Ozer E. Transoral robotic surgery (TORS) for laryngeal and hypopharyngeal cancers. J Surg Oncol. 2015;112(7):702–706. doi:10.1002/jso.24002
16. Gorphe P. A contemporary review of evidence for transoral robotic surgery in laryngeal cancer. Front Oncol. 2018;8:121. doi:10.3389/fonc.2018.00121
17. Weinstein GS, O’Malley BW, Magnuson JS, et al. Transoral robotic surgery: a multicenter study to assess feasibility, safety, and surgical margins. Laryngoscope. 2012;122(8):1701–1707. doi:10.1002/lary.23294
18. Genden EM, O’Malley BW, Weinstein GS, et al. Transoral robotic surgery: role in the management of upper aerodigestive tract tumors. Eisele DW, ed. Head Neck. 2012;34(6):886–893. doi:10.1002/hed.21752
19. Sload R, Silver N, Jawad BA, Gross ND. The role of transoral robotic surgery in the management of HPV negative oropharyngeal squamous cell carcinoma. Curr Oncol Rep. 2016;18(9):53. doi:10.1007/s11912-016-0541-x
20. Weinstein GS. Transoral robotic surgery and the standard of care. Int J Radiat Oncol. 2017;97(1):4. doi:10.1016/J.IJROBP.2016.09.028
21. Vauterin T, Garas G, Arora A. Transoral robotic surgery for obstructive sleep apnoea-hypopnoea syndrome. ORL. 2018;1–14. doi:10.1159/000489465
22. Tae K, Ji YB, Song CM, Ryu J. Robotic and endoscopic thyroid surgery: evolution and advances. Clin Exp Otorhinolaryngol. 2018. doi:10.21053/ceo.2018.00766
23. Erkul E, Duvvuri U, Mehta D, Aydil U. Transoral robotic surgery for the pediatric head and neck surgeries. Eur Arch Oto-Rhino-Laryngol. 2017;274(3):1747–1750. doi:10.1007/s00405-016-4425-3
24. Zdanski CJ, Austin GK, Walsh JM, et al. Transoral robotic surgery for upper airway pathology in the pediatric population. Laryngoscope. 2017;127(1):247–251. doi:10.1002/lary.26101
25. Smartt JM, Gerety P, Serletti JM, Taylor JA. Application of a robotic telemanipulator to perform posterior pharyngeal flap surgery: a feasibility study. Plast Reconstr Surg. 2013;131(4):841–845. doi:10.1097/PRS.0b013e318282761b
26. Khan K, Dobbs T, Swan MC, Weinstein GS, Goodacre TEE. Trans-oral robotic cleft surgery (TORCS) for palate and posterior pharyngeal wall reconstruction: a feasibility study. J Plast Reconstr Aesthet Surg. 2016;69(1):97–100. doi:10.1016/J.BJPS.2015.08.020
27. Nadjmi N. Transoral robotic cleft palate surgery. Cleft Palate-Craniofacial J. 2016;53(3):326–331. doi:10.1597/14-077
28. Brasel KJ, Klingensmith ME, Englander R, et al. Entrustable professional activities in general surgery: development and implementation. J Surg Educ. 2019;76:1174–1186. doi:10.1016/j.jsurg.2019.04.003
29. Ganesh Kumar N, Marwaha J, Drolet BC. Milestones on the plastic surgery in-service training examination. J Surg Educ. 2019. doi:10.1016/j.jsurg.2019.03.014
30. Zago M, Sforza C, Mariani D, et al. Educational impact of hand motion analysis in the evaluation of FAST examination skills. Eur J Trauma Emerg Surg. 2019. doi:10.1007/s00068-019-01112-6
31. Al Omran Y, Kostusiak M, Myers SR, Ghanem AM. Effects of habitual physical activity on microsurgical performance. Br J Oral Maxillofac Surg. 2016;54(9):1025–1027. doi:10.1016/j.bjoms.2016.01.008
32. Applebaum MA, Doren EL, Ghanem AM, Myers SR, Harrington M, Smith DJ. Microsurgery competency during plastic surgery residency: an objective skills assessment of an integrated residency training program. Eplasty. 2018;18:e25.
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.