Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Robotic-Assisted Bronchoscopy for Volume Reduction of Giant Emphysematous Bulla: A Case Report
Authors Li Y ![]() , You M, Chen E
, You M, Chen E ![]() , Zhang J
, Zhang J
Received 11 July 2025
Accepted for publication 13 December 2025
Published 22 December 2025 Volume 2025:20 Pages 4083—4089
DOI https://doi.org/10.2147/COPD.S552360
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Vanesa Bellou
Yalun Li,1,2,* Mengzhen You,1,2,* Enguo Chen,1 Jisong Zhang1
1Department of Pulmonary and Critical Care Medicine, Regional Medical Center for National Institute of Respiratory Disease, Sir Run Run Shaw Hospital, School of Medicine, Zhejiang University, Hangzhou, People’s Republic of China; 2School of Medicine, Zhejiang University, Hangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jisong Zhang, Department of Pulmonary and Critical Care Medicine, Regional Medical Center for National Institute of Respiratory Disease, Sir Run Run Shaw Hospital, School of Medicine, Zhejiang University, No. 3 Qingchun East Road, Hangzhou, 310016, People’s Republic of China, Email [email protected]
Abstract: We report the first successful case of volume reduction of a giant emphysematous bulla (GEB) using the latest shape-sensing robotic-assisted bronchoscopy (ssRAB). The patient was a 70-year-old male with chronic obstructive pulmonary disease (COPD) who developed GEB. He had previously undergone endobronchial valve (EBV) removal due to pneumonia caused by long-term implantation of EBVs for bulla volume reduction after a left emphysematous bulla rupture and subsequent pneumothorax. The patient visited our hospital for gradually worsening shortness of breath over two months. Chest radiography and computed tomography (CT) showed a GEB compressing 60% of the right lung volume, with the largest part filling the entire cross-section of the right lower lung. Under general anesthesia and with the assistance of ssRAB, we precisely punctured the bulla, safely aspirated the gas within the bulla, and injected medical adhesive to close the bulla. Postoperatively, the patient’s shortness of breath improved significantly, and a CT follow-up six months later showed that the bulla had reduced to about half of its original size. Our experience indicates the feasibility and potential benefits of the novel ssRAB for volume reduction of GEB. The long-term efficacy and safety of using ssRAB to reduce GEB need to be evaluated by larger-scale studies.
Keywords: pulmonary bulla, chronic obstructive pulmonary disease, robotic-assisted bronchoscopy, lung volume reduction
Introduction
The occurrence of pulmonary bulla is closely related to the progression of chronic obstructive pulmonary disease (COPD). The thin-walled, air-containing cysts with a diameter of more than 1 cm formed thereby are called emphysematous bulla. There is a definition that when a bulla occupies more than 30% of hemithorax, it is called a giant emphysematous bulla (GEB).1 The age-standardized incidence of GEB is very low, at 0.21 per 100,000 per year.2 However, due to the significant impact on gas exchange in the surrounding normal lung parenchyma, patients with GEB may experience severe dyspnea, and even life-threatening conditions such as secondary pneumothorax or infection. We report a case of successful volume reduction of a GEB by precisely aspirating the gas within the bulla and injecting adhesive under the assistance of the latest shape-sensing robotic-assisted bronchoscopy (ssRAB).
Case Presentation
A 70-year-old male presented with progressive shortness of breath after activity over two months. He was admitted to the hospital in December 2024. The patient was a long-term smoker and had a 20-year history of COPD, which was maintained with inhaled bronchodilators and lack of regular follow-up chest imaging. In 2016, he experienced a sudden pneumothorax, which was found to be caused by the rupture of an emphysematous bulla in the left lung. A therapy of bronchoscopic lung volume reduction with endobronchial valve was successfully performed on the left lower lobe in a previous hospital. However, the two implanted endobronchial valves (EBVs) were removed in June 2024 due to repeated acute exacerbations of COPD and difficult-to-control infections.
Post-Admission Assessment
Physical examination after admission revealed reduced breath sounds in both lungs, with hyperresonance in the right lower lung. Blood gas analysis showed a partial pressure of carbon dioxide of 47.2 mmHg. Chest radiography showed no lung-markings in the right lower lung, occupying 60% of the entire right lung (Figure 1A); computed tomography (CT) images showed typical signs of chronic bronchitis and emphysema, with a GEB on the right lung and adjacent lung tissue atelectasis. The largest part of the bulla filled the entire cross-section of the lower lung (Figure 2A). The patient has a GEB in the right lung, which causes shortness of breath. Given the patient’s history of bulla rupture leading to pneumothorax, pulmonary function tests that require the patient to actively exhale forcefully were not conducted.
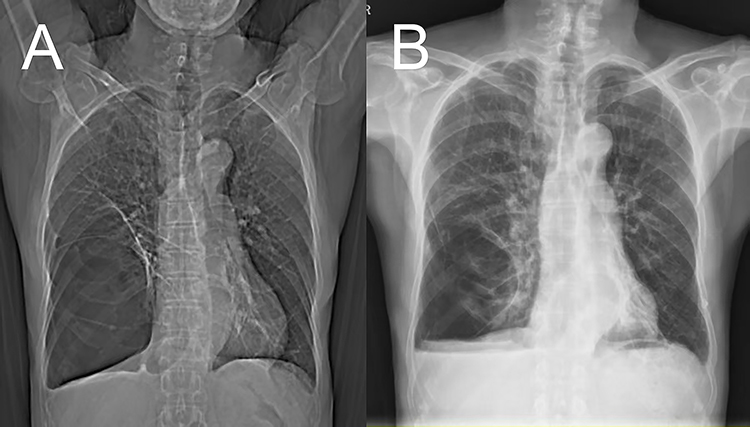 |
Figure 1 Comparison of preoperative and postoperative chest radiography images. (A) Preoperatively, the chest radiography shows that a giant bulla compressed approximately 60% of the entire right lung. (B) Postoperative chest radiography within 24 hours shows that the space compressed by the bulla in the entire right lung has decreased to 30%. |
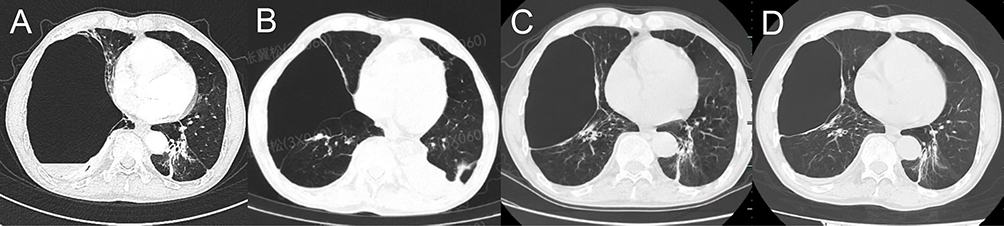 |
Figure 2 Comparison of preoperative, postoperative and follow-up CT images. (A) Preoperative CT image reveals that the largest part of the bulla in the right lung filled the entire cross-section of the lower lung. (B) Postoperative CT image within 24 hours shows a reduction in the size of the bulla with re-expansion of the previously compressed pulmonary parenchyma. (C) Postoperative CT image at the 3-month follow-up shows that the bulla in the right lung has significantly decreased compared to before. (D) Postoperative CT image at the 6-month follow-up shows that the bulla remained stable and had slightly shrunk in size again. |
After admission, in combination with the patient’s elevated PaCO2, the history of sudden rupture of bulla and pneumothorax in 2016, and the need to improve tolerance for daily activities, we conducted a multidisciplinary assessment of the possible therapies that the patient could benefit from and provided a detailed explanation to the patient of the procedures and risks associated with treating GEB. The patient and his family members declined the surgical lung volume reduction and expressed a clear expectation for safer, minimally invasive therapeutic alternatives. Ultimately, we chose the robotic bronchoscopy system renowned for its exceptional stability and precision, which we deemed essential for safely accessing and managing GEB.
Procedure for GEB Volume Reduction
The operation was performed under general anesthesia with endotracheal intubation and mechanical ventilation. The anesthesiologist precisely set the ventilator and adopted a protective lung ventilation strategy to avoid excessive pressure within the lungs, thereby reducing the risk of bulla rupture. A multidisciplinary emergency response team remains on standby at all times. It was carried out by a doctor who was proficient in the technique of robotic bronchoscopy. The Ion robotic bronchoscopy system (Intuitive Surgical Co., Ltd., Sunnyvale, California, The United States of America) was used, which is a shape-sensing robotic platform equipped with an ultra-thin 3.5 mm articulating catheter. A 3D bronchial tree model was created based on preoperative CT data, and appropriate puncture points that were conducive to aspiration and avoided blood vessels were preset. The bronchoscopist controlled the robotic arm through the control panel and inserted the sheath through the endotracheal tube. Under direct endoscopic observation, it was noted that the mucosa at the left lower opening was slightly swollen, thickened and narrowed, and the right middle and lower lobe bronchial lumens were compressed and narrowed. During the operation, the guiding sheath was sent along the path planned by the navigation system to reach the target point in the right lower anterior basal segment. Cone beam CT (CBCT) was used during the operation to confirm the correct position of the sheath. A 18G puncture needle (Length: 1.4m, Broncus Co., Ltd., China) was then inserted (Figure 3). After confirming the positions of the sheath and the puncture needle with CBCT again (Figure 4), the needle was advanced under fluoroscopy until it reached the cavity of the bulla. The endoscopist connected a negative pressure syringe with the puncture needle and began to aspirate under fluoroscopy. If air aspiration proves difficult, CBCT should be utilized to verify whether adjustment of the needle’s position and angle is required. The decision to discontinue air aspiration is guided by three key indicators: changes in bulla size, characteristics of drainage fluid, and stability of physiological parameters. With stable vital signs and oxygen saturation, and in the absence of blood-tinged fluid aspiration and alveolar wall rupture, CBCT monitoring demonstrated a significant reduction of the GEB, which stabilized in size without further regression. A total of 1920 mL of air was extracted. Subsequently, 4 mL of a mixture of human serum albumin solution and succinimidyl succinate-PEG-succinimidyl succinate (SS-PEG-SS) was injected into the bulla cavity. After reconfirming that the bulla and the patient’s indicators are both stable, the endoscope was then withdrawn.
 |
Figure 3 The operating doctor is puncturing the bulla through the bronchoscope with the help of 3D modeling. |
 |
Figure 4 Intraoperative CBCT images showed that the puncture needle was located within the bulla. |
Postoperative Performance and Therapeutic Outcome
The operation was carried out smoothly as planned, with no complications such as pneumothorax or bleeding. The patient exhibited no significant postoperative discomfort. Postoperative chest radiography within 24 hours showed that the space compressed by the GEB had shrunk to approximately 30% of the entire right lung (Figure 1B), the CT image shows a reduced bulla with re-expansion of the previously compressed pulmonary parenchyma (Figure 2B). The patient was able to get out of bed and walk around the ward the next day. At discharge, the general condition and shortness of breath had improved significantly. Postoperative CT image at the 3-month follow-up showed that the bulla had significantly decreased compared to before (Figure 2C). Postoperative CT image at the 6-month follow-up shows that the bulla remained stable and had slightly shrunk in size again (Figure 2D). No infectious exacerbation occurred. The patient reported that his shortness of breath had improved significantly and he could complete daily activities, such as housework and feeding poultry, without difficulty.
Discussion
Our patient had a long history of COPD and had previously experienced a left emphysematous bulla rupture leading to secondary pneumothorax. After implantation of EBVs for improving symptoms, the valves were removed due to secondary pneumonia. The patient was admitted to our hospital due to progressive shortness of breath over 2 months, and a GEB occupying almost the entire right lower lung was found on the opposite side of the previous bulla. The corresponding volume reduction procedure for GEB can be summarized as: precisely puncturing, aspirating the gas within the bulla and injecting adhesive under the assistance of ssRAB. The follow-up results indicated more than 50% effective volume reduction and significant improvement in symptoms. To our knowledge, this is the first report of the use of ssRAB for volume reduction of such a GEB.
GEB often remains at the stage of imaging discovery and is considered difficult to reverse, with few receiving active and successful interventions. GEB refractory to pharmacological intervention is conventionally treated with lung volume reduction surgery, but the surgical risks always need to be carefully considered. Previous studies have found that when preoperative forced expiratory volume at 1 second over vital capacity is less than 35%, accompanied by hypoxemia and hypercapnia, the benefits and risks of surgical reduction are disproportionate, and the postoperative mortality rate significantly increases.3 In recent years, significant advancements have been made in surgical techniques and postoperative care, while minimally invasive respiratory interventions have also evolved rapidly. A recent meta-analysis systematically evaluated lung volume reduction surgery and bronchoscopic techniques (such as EBV) in adults with severe emphysema, revealing that lung volume reduction surgery offers the greatest efficacy benefits but carries the highest risks (early mortality of 4.1% and overall mortality of 21.5%).4 Our patient is not contraindicated for surgery; however, considering the presence of hypercapnia, a history of pneumothorax, and the patient’s limited inclination toward surgical intervention, we have prioritized bronchoscopic intervention of the GEB. In recent years, minimally invasive respiratory interventional techniques have developed rapidly and have become another common choice. The mainstream interventional procedures volume reduction via the bronchus include the previously mentioned EBV and biologic lung volume reduction,5–7 etc. This patient had previously received bronchoscopic lung volume reduction with EBVs, a technique that allows air to be expelled from the distal lung segments during exhalation but prevents air from entering during inhalation, achieving “one-way deflation” of the bullae. The application of EBV in emphysema has become relatively mature,8,9 but early pneumothorax remains a common adverse event, with an incidence rate ranging from 4% to 23%,10,11 The prerequisite for successful EBV treatment is the integrity of the interlobar fissure and the absence of bypass ventilation, which often requires determination through high-resolution CT or even on-site bronchoscopy.12 In addition, long-term implantation of EBV may lead to pneumonia and hemoptysis, and some patients may require valve removal,13 as experienced by this patient. These factors prompted us to choose a more minimally invasive and precise approach, namely, using ssRAB to reduce the volume of bulla.
The strategy of “puncturing a bulla, aspirating gas, and injecting adhesives” that we have adopted enables the preservation of potential lung parenchyma by avoiding resection. This bronchoscopic technique of intrabullous aspiration and/or sclerotherapy is not a novel approach. Previous case series have preliminarily indicated its clinical efficacy: under fluoroscopic guidance, direct endoscopic instillation of autologous blood into bullae can induce an inflammatory response, leading to scar formation, fibrosis, and eventual reduction in bulla volume, with significant improvements in lung function, exercise capacity, and quality of life observed at three months after volume reduction.14 Other sclerosing agents have similar effects. A study used bronchoscopic lung volume reduction with autologous blood and thrombin in three patients with very severe COPD, showing sustained improvements in exercise capacity and St. George’s Respiratory Questionnaire scores for at least 12 months during follow-up.15 Besides, the injection of human serum albumin solution and SS-PEG-SS can induce fibrosis of the bulla wall and can be regarded as a type of biologic lung volume reduction.16 A small-sample prospective study has preliminarily verified the safety and effectiveness of a similar principle using fibrinogen and thrombin for lung volume reduction.17 In this case, a large amount of gas within the bulla was aspirated before the injection of adhesives, which could reduce the pressure of the bulla, induce fibrosis of the bulla wall and prevent re-expansion. In addition, the techniques used to approach the target bulla are constantly being updated. Navigation bronchoscopy and O-arm CT technology have been employed to more accurately access and aspirate air as well as inject sclerosing agents,18 suggesting the need for improved techniques to precisely reach the bullae. The novelty of our case lies in the first application of the robotic bronchoscopy system to access and reduce the GEB. As the latest bronchoscopy technology, ssRAB combines the flexibility of robotic arms with the technology of optical fiber shape sensing and localization, and its advantages in the early diagnosis and interventional treatment of lung cancer have been continuously confirmed by multiple studies.12,19,20 The characteristics of high precision, minimally invasiveness and integrated diagnosis and treatment make it show great potential for effectiveness and a solid foundation for safety in the diagnosis and treatment of other respiratory diseases. However, clinical researches in these domains have yet to be initiated. Our intervention indicated that ssRAB is enable to effectively treat GEB without obvious complications, and the application in the volume reduction of GEB can serve as a reference for clinical decision for similar patients.
The primary therapeutic objective for GEB is volume reduction, which can increase the proportion of normal lung parenchyma and thereby improve symptoms. This case report documents successful single-session robotic bronchoscopy intervention that achieved appreciable symptomatic improvement. However, follow-up imaging revealed residual capacity for further bulla volume reduction. A planned second aspiration may yield additional volume reduction, warranting consideration in future practice. Currently, evidence regarding staged bulla aspiration combined with sclerotherapy remains limited, with even scarcer data available on secondary aspiration. The minimally invasive nature and procedural reproducibility of robotic bronchoscopy render staged therapeutic interventions a promising research avenue that warrants broader validation. On the other hand, GEB volume reduction can also prevent pneumothorax caused by rupture. It is worth noting that more than 50% of patients with primary spontaneous pneumothorax have contralateral bullae, and about 1/4 will develop contralateral pneumothorax.21 Studies have shown that preemptive video-assisted thoracic surgery for contralateral bullae can effectively prevent contralateral bullae from developing into pneumothorax,22 demonstrating the value of preventive intervention. Whether patients with a history of bulla rupture and secondary pneumothorax need preventive volume reduction for contralateral bullae is a question that deserves further exploration in more cases. In the future, for the preventive reduction of bullae-induced pneumothorax, the safe and minimally invasive ssRAB may be a better choice.
Our study has several limitations: 1) The patient did not receive adequate examinations and follow-up. Given that the pulmonary function test requires the patient to exhale forcefully and actively, and considering the patient’s history of pneumothorax due to bulla rupture and his personal preference, the test was not carried out. Postoperatively, the patient reported significant symptomatic improvement and expressed no intention to undergo pulmonary function follow-up. However, multi-timepoint pulmonary function and CT data serve as critical objective indicators for efficacy assessment. A similar study using the “aspiration” technique for bullae volume reduction suggested that the majority of effectively reduced bullae remained stable or even continued to shrink during the follow-up period of more than six months, with only a few showing an increase in volume.23 Whether the bulla volume of our case will increase again remains to be observed. We will endeavor to obtain these metrics in subsequent studies where feasible. 2) The procedures and strategies for volume reduction need to be improved. As a preliminary attempt at robotic bronchoscopic volume reduction for GEB, the most appropriate patient characteristics, aspiration strategies, and the selection of sclerosing agents all remain to be explored. The increasing sample data will gradually answer these questions in the near future.
Conclusion
This study represents the first report on the short-term efficacy and safety of ssRAB-assisted volume reduction in patients with GEB. Six-month follow-up demonstrates symptomatic relief and reduction in bulla volume; however, long-term functional outcomes and the potential for pneumothorax prevention require further investigation. Extended follow-up studies involving a larger patient cohort will be continued. The subsequent phase of research should focus on multi-center clinical trials to verify the safety in the particular population and obtain effectiveness data, while further exploring the procedures and strategies for volume reduction.
Abbreviations
COPD, chronic obstructive pulmonary disease; GEB, giant emphysematous bulla; ssRAB, shape-sensing robotic-assisted bronchoscopy; EBV, endobronchial valve; CT, computed tomography; Co., Ltd., company limited; CBCT, cone beam CT; SS-PEG-SS, succinimidyl succinate-PEG-succinimidyl succinate.
Ethics Approval and Informed Consent
The written informed consent was obtained from the patient for the publication of the case details. According to the ethic committee of the affiliated institution, the ethic approval is required to publish the case details. Ethical approval has been obtained from the Ethics Committee of Sir Run Run Shaw Hospital, Zhejiang University School of Medicine, with the license number: Sir Run Run Shaw Hospital Ethics Review 2025 Research No. 1109.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Schipper PH, Meyers BF, Battafarano RJ, Guthrie TJ, Patterson GA, Cooper JD. Outcomes after resection of giant emphysematous bullae. Ann Thorac Surg. 2004;78(3):976–982. doi:10.1016/j.athoracsur.2004.04.005
2. Gunnarsson SI, Johannesson KB, Gudjonsdottir M, Magnusson B, Jonsson S, Gudbjartsson T. Incidence and outcomes of surgical resection for giant pulmonary bullae--a population-based study. Scand J Surg. 2012;101(3):166–169. doi:10.1177/145749691210100305
3. Nakahara K, Nakaoka K, Ohno K, et al. Functional indications for bullectomy of giant bulla. Ann Thorac Surg. 1983;35(5):480–487. doi:10.1016/s0003-4975(10)60419-5
4. Bo L, He X, Chen Y, Shi L, Li C. Lung volume reduction therapies in patients with emphysema: a systematic review and network meta-analysis. COPD. 2025;22(1):2567022. doi:10.1080/15412555.2025.2567022
5. Buttery SC, Banya W, Bilancia R, et al. Lung volume reduction surgery versus endobronchial valves: a randomised controlled trial. Eur Respir J. 2023;61(4):2202063. doi:10.1183/13993003.02063-2022
6. Cheng TL, Fan Y. The real-world safety of endobronchial valve: what we need to know. Chest. 2025;167(2):307–308. doi:10.1016/j.chest.2024.10.030
7. Refaely Y, Dransfield M, Kramer MR, et al. Biologic lung volume reduction therapy for advanced homogeneous emphysema. Eur Respir J. 2010;36(1):20–27. doi:10.1183/09031936.00106009
8. Sciurba FC, Ernst A, Herth FJ, et al. A randomized study of endobronchial valves for advanced emphysema. N Engl J Med. 2010;363(13):1233–1244. doi:10.1056/NEJMoa0900928
9. Klooster K, Ten Hacken NH, Hartman JE, Kerstjens HA, Van Rikxoort EM, Slebos DJ. Endobronchial valves for emphysema without interlobar collateral ventilation. N Engl J Med. 2015;373(24):2325–2335. doi:10.1056/NEJMoa1507807
10. Herth FJ, Eberhardt R, Gompelmann D, et al. Radiological and clinical outcomes of using Chartis™ to plan endobronchial valve treatment. Eur Respir J. 2013;41(2):302–308. doi:10.1183/09031936.00015312
11. Gompelmann D, Eberhardt R, Herth F. Endoscopic volume reduction in COPD- a critical review. Dtsch Arztebl Int. 2014;111(49):827–833. doi:10.3238/arztebl.2014.0827
12. Low SW, Lentz RJ, Chen H, et al. Shape-sensing robotic-assisted bronchoscopy vs digital tomosynthesis-corrected electromagnetic navigation bronchoscopy: a comparative cohort study of diagnostic performance. Chest. 2023;163(4):977–984. doi:10.1016/j.chest.2022.10.019
13. Choi M, Lee WS, Lee M, et al. Effectiveness of bronchoscopic lung volume reduction using unilateral endobronchial valve: a systematic review and meta-analysis. Int J Chron Obstruct Pulmon Dis. 2015;10(10):703–710. doi:10.2147/copd.S75314
14. Zoumot Z, Kemp SV, Caneja C, Singh S, Shah PL. Bronchoscopic intrabullous autologous blood instillation: a novel approach for the treatment of giant bullae. Ann Thorac Surg. 2013;96(4):1488–1491. doi:10.1016/j.athoracsur.2013.03.108
15. Mizumori Y, Mochiduki Y, Nakahara Y, et al. Effects of bronchoscopic lung volume reduction using transbronchial infusion of autologous blood and thrombin in patients with severe chronic obstructive pulmonary disease. J Thorac Dis. 2015;7(3):413–421. doi:10.3978/j.issn.2072-1439.2015.01.10
16. Reilly J, Washko G, Pinto-Plata V, et al. Biological lung volume reduction: a new bronchoscopic therapy for advanced emphysema. Chest. 2007;131(4):1108–1113. doi:10.1378/chest.06-1754
17. El Gohary D, Eltomey MA, Mohamed AS, Farahat A, Abd El Zaher AH. Bronchoscopic lung volume reduction by instillation of fibrinogen and thrombin in COPD patients with homogenous emphysema. BMC Pulm Med. 2024;24(1):86. doi:10.1186/s12890-024-02883-4
18. Zhu J, Xu X, Wang R, Li Z, Wang Y, Hu Y. A case of pulmonary bulla volume reduction by transbronchial puncture under electromagnetic navigation platform combined with O-Arm CT guidance. Int J Chron Obstruct Pulmon Dis. 2025;Volume 20(20):451–455. doi:10.2147/copd.S493818
19. Kalchiem-Dekel O, Connolly JG, Lin IH, et al. Shape-sensing robotic-assisted bronchoscopy in the diagnosis of pulmonary parenchymal lesions. Chest. 2022;161(2):572–582. doi:10.1016/j.chest.2021.07.2169
20. Fernandez-Bussy S, Yu Lee-Mateus A, Barrios-Ruiz A, et al. Diagnostic performance of shape-sensing robotic-assisted bronchoscopy for pleural-based and fissure-based pulmonary lesions. Thorax. 2025;80(3):150–158. doi:10.1136/thorax-2024-222502
21. Sihoe AD, Yim AP, Lee TW, et al. Can CT scanning be used to select patients with unilateral primary spontaneous pneumothorax for bilateral surgery? Chest. 2000;118(2):380–383. doi:10.1378/chest.118.2.380
22. Chou SH, Li HP, Lee JY, et al. Is prophylactic treatment of contralateral blebs in patients with primary spontaneous pneumothorax indicated? J Thorac Cardiovasc Surg. 2010;139(5):1241–1245. doi:10.1016/j.jtcvs.2009.07.047
23. Wang Z, Liu Z, Zhang W, et al. A novel percutaneous volume reduction technique for giant emphysematous bullae: combined percutaneous erythromycin sclerotherapy with bronchoscopic occlusion. Int J Chron Obstruct Pulmon Dis. 2025;Volume 20(20):641–657. doi:10.2147/copd.S495903
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.