Back to Journals » Clinical Interventions in Aging » Volume 19
Robot Navigation System Assisted PFNA Fixation of Femoral Intertrochanteric Fractures in the Elderly: A Retrospective Clinical Study
Authors Qi H ![]() , Li Z, Ma T, Jiang Y, Ren C, Xu Y, Huang Q, Zhang K, Lu Y, Li M
, Li Z, Ma T, Jiang Y, Ren C, Xu Y, Huang Q, Zhang K, Lu Y, Li M
Received 25 June 2023
Accepted for publication 1 December 2023
Published 5 January 2024 Volume 2024:19 Pages 11—19
DOI https://doi.org/10.2147/CIA.S412397
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Prof. Dr. Nandu Goswami
Hongfei Qi,1,* Zhong Li,1,* Teng Ma,1 Yangyang Jiang,2,* Cheng Ren,1,* Yibo Xu,1 Qiang Huang,1 Kun Zhang,1 Yao Lu,1 Ming Li1
1Department of Orthopaedics and Trauma, Hong Hui Hospital, Xi’an Jiaotong University College of Medicine, Xi’an, Shaanxi, 710000, People’s Republic of China; 2Xi’an Medical College, Xi’an, Shaanxi, 710000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ming Li; Teng Ma, Email [email protected]; [email protected]
Objective: The incidence of hip fracture in the elderly is increasing. Robot navigation technology has the advantages of minimally invasive and accurate. To explore the difference between the clinical effects of proximal femoral anti-rotation intramedullary nail (PFNA) assisted by robot navigation in the treatment of femoral intertrochanteric fracture and traditional PFNA in the treatment of femoral intertrochanteric fracture in the elderly; analyze the advantages and feasibility of PFNA assisted by robot navigation in the treatment of femoral intertrochanteric fracture in the elderly.
Patients and Methods: From February 2021 to October 2022, the elderly (> 65 years old) with femoral intertrochanteric fracture underwent surgery in our center. Divided the patients included in the study into 2 groups based on the surgical method. The surgical method of robot group was PFNA fixation assisted by robot navigation, while the surgical method of traditional group was classic PFNA fixation, Baseline data (general condition, Evans classification, time from injury to operation, preoperative hemoglobin) and observation indicators (intraoperative bleeding, operation time, the length of incision for mail nail insertion, postoperative hemoglobin drop, blood transfusion rate and the Harris score of hip joint 1 year after operation) of the two groups were collected to compare whether there were differences between the two groups.
Results: There was no statistical difference in baseline data between the two groups (P> 0.05). The intraoperative bleeding in the robot group was 68.17± 10.66 mL, the intraoperative bleeding in the traditional group was 174± 8.11mL (P< 0.001). The operation time in the robot group was 68.81 ± 6.89 min, in the traditional group, the operation time was 76.94 ± 8.18 min (P< 0.001). The length of incision for mail nail insertion in the robot group was 3.53 ± 0.63 cm, the length of the incision for mail nail insertion in the traditional group was 4.23 ± 0.71 cm (P< 0.001). 5 patients (13.9%) in the robot group received blood transfusion treatment, and 13 patients (36.1%) in the traditional group received blood transfusion treatment (P=0.029). The hemoglobin in the robot group decreased by 14.81 ± 3.27 g/l after operation compared with that before operation, while that in the traditional group decreased by 16.69 ± 3.32 g/l (P=0.018). The Harris score of the hip joint of the affected limb in the robot group was excellent in 25 cases, good in 8 cases and poor in 3 cases one year after the operation; In the traditional group, Harris scores were excellent in 18 cases, good in 11 cases and poor in 7 cases (P=0.021).
Conclusion: PFNA fixation of femoral intertrochanteric fracture with robot navigation assistance has the advantages of minimally invasive and accurate, shorter operation time, less bleeding and lower blood transfusion rate than traditional surgical methods, and has certain advantages in reducing postoperative complications of elderly patients.
Keywords: orthopedics robot navigation, femoral fracture, older persons, intramedullary nail fixation
Introduction
Hip fracture is a common fracture in the elderly. With the increase of the elderly population, the incidence of hip fractures is also increasing. In 2050, the global number of hip fractures is expected to reach 6.3 million. For those aged over 65 years who have a hip fracture, if the treatment is not timely, the prognosis is poor.1 Some studies show that the risk of death of patients with hip fractures who are not treated surgically for one year is four times higher than that of patients who are treated surgically.2 Therefore, at present, we believe that the elderly hip fracture should be treated surgically. Femoral intertrochanteric fracture account for about half of hip fractures.3 The surgical treatment methods include intramedullary fixation and extramedullary fixation. Intramedullary fixation has unique advantages for unstable and oblique fracture lines.4–6 As a kind of intramedullary fixation for femoral intertrochanteric fracture, proximal femoral anti-rotation intramedullary nail (PFNA) has gradually become the preferred internal fixation device for the treatment of femoral intertrochanteric fracture due to its advantages of central fixation, less surgical complications, and good curative effect.7
In the operation of PFNA fixation of the femoral intertrochanteric fracture, accurate determination of the insertion point is the key to ensuring a good fixation position and reducing postoperative complications.8,9 In traditional surgery, we use the lateral femoral incision to touch the apex of the greater trochanter of the femur with our fingers to determine the position of the insertion point. However, for patients with poor reduction or obesity, it may be difficult to determine the needle entry point, and it is necessary to extend the surgical incision or repeatedly probe. These operations may prolong the operation time, increase bleeding, over-peel the gluteus medius muscle and aggravate the injury of surrounding tissues. Elderly patients have a higher probability of complications with medical diseases and a higher risk of various complications.10 Reducing trauma and bleeding and shortening the operation time is conducive to a better prognosis for elderly patients.
With the development of minimally invasive surgery and the increasing demand for surgical accuracy, robot navigation technology is increasingly used in spine, joint surgery, and pelvic fracture surgery.11–13 Robot navigation technology has high security and accuracy.14 It can assist surgeons in quickly and accurately determining the needle insertion point during the operation of PFNA fixation, which is of great significance to elderly patients. In our study, a retrospective clinical controlled study was conducted to explore the difference between the clinical efficacy of robot navigation assisted PFNA in the treatment of femoral intertrochanteric fracture and the traditional PFNA in the treatment of femoral intertrochanteric fracture in the elderly; to analyze the advantages and feasibility of PFNA assisted by robot navigation in the treatment of femoral intertrochanteric fracture in the elderly.
Materials and Methods
Inclusion Criteria
Exclusion Criteria
Case Selection
This clinical study was approved by the Ethics Committee of Xi’an Hong Hui Hospital, and the whole research process followed the relevant requirements of the Helsinki Declaration. In strict accordance with the case inclusion and exclusion criteria, patients who received surgical treatment for intertrochanteric fracture of the femur in our center in February 2021 and October 2022 were included. The patients included in the study were divided into a robot group and a traditional group based on surgical methods. The surgical method of the robot group was robot navigation assisted PFNA fixation, while the surgical method of the traditional group was classic PFNA fixation.
Preoperative Preparation
The patients included in the study should complete preoperative examination, and the patients with medical diseases should be evaluated by the anesthesiologists, respiratory physicians, and cardiovascular physicians in a multidisciplinary manner, actively treat the medical complications, eliminate the contraindications of surgery, and evaluate the risk of surgery before surgery.
Surgical Technique
Robot group: The robot navigation system in this study was Tianji Robot (Beijing Tianzhihang Company), and the robot was placed in the appropriate position (Figure 1a). Patients was in supine position, after general anesthesia or epidural anesthesia was satisfied, put both lower limbs on the traction bed, the hip of the affected side was moderately elevated, and closed reduction of fracture by traction of affected limb. After the reduction was satisfied by C-arm X-ray machine detection (Figure 1b, in case of poor reduction, the anterior incision was used for repositioning), disinfected and laid sterile operation sheet. The C-arm X-ray machine took the anteroposterior and lateral X-ray films of the affected hip joint to ensure that the 10 positioning points on the positioning ruler were included in the X-ray image (Figure 1c). Then the acquired anteroposterior and lateral X-ray images of the hip joint were imported into the workstation. Planed the route of inserting the guide pin. The ideal insertion point was at the highest point of the greater trochanter of the femur in the X-ray anteroposterior, at the midpoint of the femur in the X-ray lateral, or at the front 1/3 of the femur, and the direction of the guide pin deviated to the outside along the long axis of the femoral shaft in the X-ray anteroposterior, and was consistent with the long axis of the femoral shaft in the X-ray lateral (Figure 1d). Started the robot arm, moved to the insertion point on the body surface, made an incision, placed the guide pin, confirmed the position of the guide pin with the C-arm X-ray machine, withdrew the robot arm, placed the guide pin again along the long axis of the femur (Figure 1e). After reaming the proximal pulp, inserted the appropriate main screw along the guide pin, and then inserted the proximal spiral blade and the distal locking screw. After the C-arm X-ray machine confirmed that the reduction is good (Figure 1f), closed the wound layer by layer after washed with a large amount of water.
 |
Figure 1 (a) Placement of robot navigation system; (b) The C-arm X-ray machine showed satisfactory fracture reduction; (c) 10 position points were shown in the X-ray image of Hip joint; (d) Planed the ideal guide pin channel; (e) The robot navigation system placed the guide pin along the planned channel; (f) The C-arm X-ray machine showed satisfactory fracture reduction and good internal fixation position. |
Traditional group: Patients in the traditional group and the robot group received the same anesthesia mode and posture. Traction of the affected limb for closed reduction of the fracture (through the anterior incision during the operation in case of poor reduction), the surgical incision was selected as the lateral femoral incision, the tip of the greater trochanter was touched by hand, and the guide pin was inserted. After the position of the guide pin was satisfied, the main screw, the proximal spiral blade and the distal locking screw were inserted in turn. The rest of the operation process was the same as that of the robot group.
Observation Indicators
After admission, record the patient’s detailed medical history, including basic information, combined medical diseases, and oral drug history. Complete preoperative examination and record the patient’s Body Mass Index (BMI), the Evans classification, time from injury to operation, preoperative hemoglobin, and other clinical data. During the operation, the patient’s bleeding volume, operation time, and the length of incision for mail nail insertion were recorded. After the operation, recheck the patient’s hemoglobin, calculate the patient’s hemoglobin drop, and record the blood transfusion during the perioperative period.
The patient’s hip joint function was evaluated by the Harris score,15,16 which included pain, function, deformity and joint range of motion. The higher the score is, the better the function of the hip joint is, and the score between 90 and 100 is excellent; 70–89 is good; Below 70 represents poor hip joint function. All patients were examined and evaluated one year after the operation.
Statistical Analysis
Data analysis was performed using SPSS version 18.0 (SPSS Inc, Chicago, IL, USA). Continuous variables are represented by mean ± standard deviation. Continuous variables are first subjected to a normality test, variables that meet the normal distribution are subjected to two independent sample t-tests, and variables that do not meet the Mann–Whitney U-test. Chi-squared (χ2) test was used to compare the count data between the two groups. P < 0.05, the difference was considered to be statistically significant.
Results
Baseline Data
This study included 72 patients, including 36 in the robot group and 36 in the traditional surgery group. See Figure 2 for the inclusion process. There are 16 males and 20 females in the robot group; There are 18 males and 18 females in the traditional operation group. In terms of age, the age of patients in the robot group was 77.58±9.28 years old, and that in the traditional surgery group was 80.31±9.13 years old. The BMI of patients in the robot group was 20.89±3.04, and that of patients in the traditional surgery group was 21.38±2.85. All patients completed X-ray and CT examination before the operation and carried out AO classification. The Evans classification of fracture in the robot group was: type I: 0, type II: 15, type III: 10, type IV 5:, type V 6:; The fracture types of the traditional operation group were: type I: 0, type II: 22, type III:10, type IV : 3, and type V1. The average time from injury to surgery in the robot group was 3.19±1.53 days; The time from injury to operation in the traditional operation group was 2.92±1.32 days. The preoperative examination showed that the preoperative hemoglobin of patients in the robot group was 96.28 ± 10.66g/l, and that of patients in the traditional operation group was 100.50±9.40g/l. There was no significant difference between the two groups in the above baseline data, P>0.05 (see Table 1).
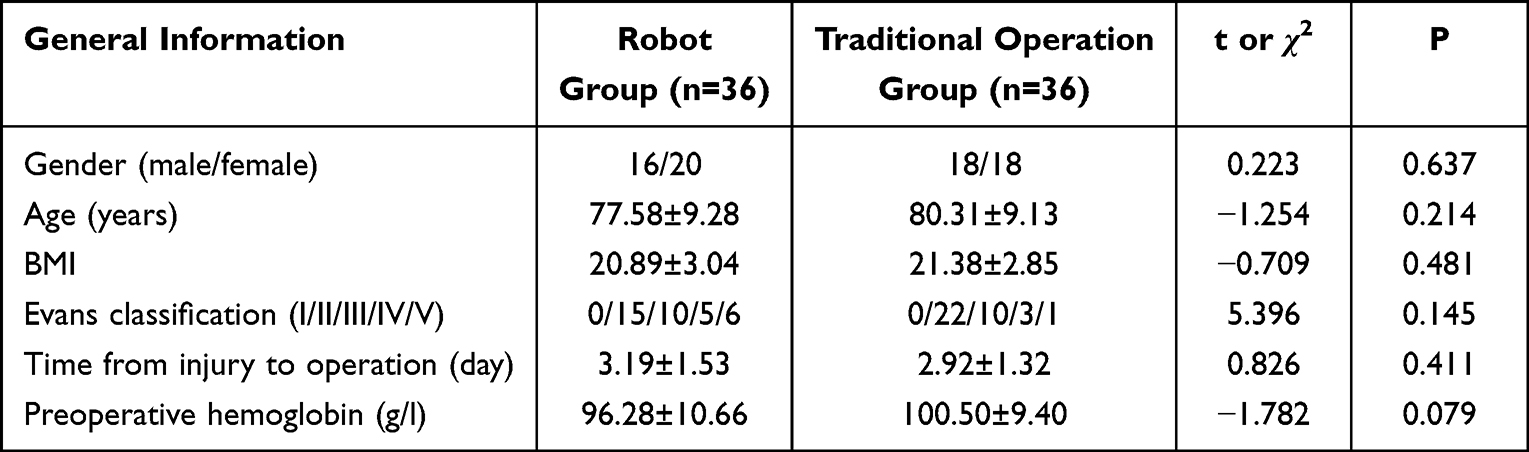 |
Table 1 Comparison of General Conditions and Preoperative Data |
 |
Figure 2 Include in the flow chart. |
All patients’ fractures healed smoothly, and no cases had complications such as deep infection, internal fixation failure, and secondary operation. The following are the specific observation indicators.
Intraoperative Bleeding
The intraoperative bleeding of patients in the robot group was 68.17± 10.66 mL, and that of patients in the traditional surgery group was 174.83±8.11 mL. The intraoperative bleeding of patients in the traditional surgery group was more, and the difference between the two groups was statistically significant P<0.05 (see Table 2).
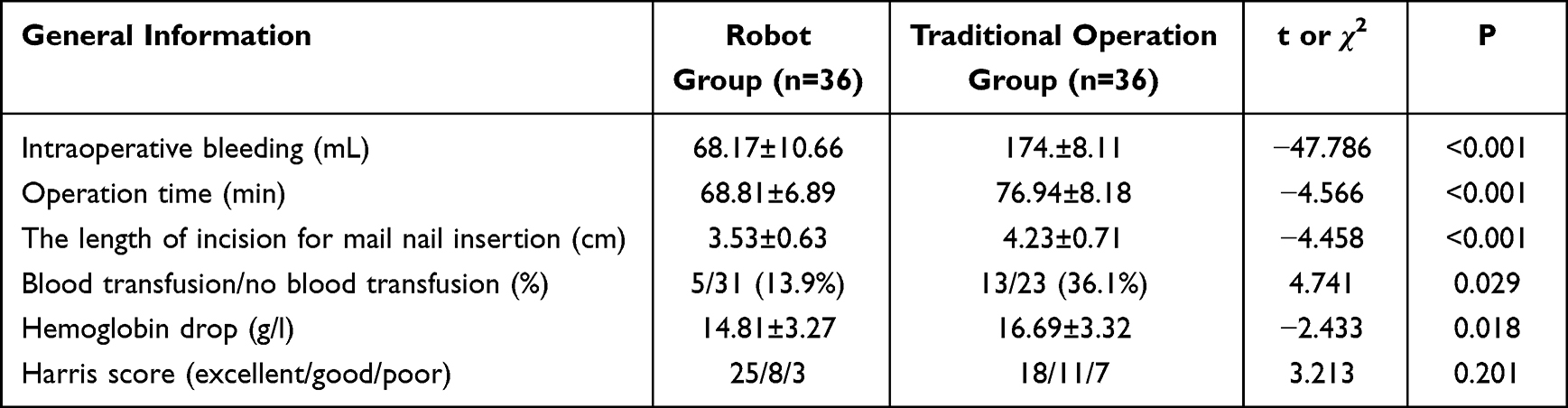 |
Table 2 Comparison of Intraoperative Data and Prognosis Between the Two Groups |
Operation Time
The operation time of the robot group was 68.81 ± 6.89 min, while that of the traditional operation group was 76.94 ± 8.18 min. The operation time of the traditional operation group was longer. The difference between the two groups was statistically significant (see Table 2).
The length of incision for mail nail insertion The length of incision for mail nail insertion in the robot group was 3.5±0.63 cm, the length of incision for mail nail insertion in the traditional operation group was 4.23±0.71 cm, and the length of incision for mail nail insertion in the traditional operation group was longer. The difference between the two groups was statistically significant P<0.05 (see Table 2).
Blood Transfusion Rate
5 patients (13.9%) in the robot group received blood transfusion treatment during the perioperative period, and 13 patients (36.1%) in the traditional operation group received blood transfusion treatment. The blood transfusion rate in the traditional operation group was higher, and the difference between the two groups was statistically significant P<0.05 (see Table 2).
Hemoglobin Drop
The hemoglobin drop of patients in the robot group was 14.81±3.27g/l, and that of patients in the traditional operation group was 16.69±3.32g/l. The hemoglobin drop of patients in the traditional operation group was greater after the operation, and the difference between the two groups was statistically significant (see Table 2).
Harris Score of Hip Function
According to Harris score, the function of the hip joint of the affected limb in the two groups was evaluated 1 year after the operation. The evaluation results showed that in the robot group, there were 25 cases with excellent hip joint function, 8 cases with good hip joint function, and 3 cases with poor hip joint function, and the excellent and good rate was 91.7% (33/36). In the traditional operation group, there were 18 cases with excellent hip joint function, 11 cases with good hip joint function, and 7 cases with poor hip joint function, and the excellent and good rate was 80.6% (29/36). There was no statistically significant difference between the two groups P=0.201 (see Table 2).
Discussion
The incidence of hip fractures in the elderly is increasing year by year.17 The treatment principle for hip fracture in the elderly is to operate as soon as possible, reduce the time patients are in bed, and avoid the occurrence of fracture complications.18 Femoral intertrochanteric fracture is one of the most common hip fractures. PFNA is the most widely used internal fixation for the treatment of femoral intertrochanteric fracture at present. It has the advantages of central fixation, fewer complications, and a good curative effect.19,20 With the development of various technologies and minimally invasive surgery, robot navigation assistant system has been used more and more in surgery because of its advantages of small trauma and high accuracy.21 The purpose of this study is to compare the clinical efficacy of robot navigation assisted PFNA and traditional PFNA in the treatment of femoral intertrochanteric fracture in the elderly through a retrospective clinical controlled study, and analyze the advantages and feasibility of robot navigation assisted PFNA in the treatment of femoral intertrochanteric tendon fracture in the elderly.
The robot navigation assistant system is to analyze and processes the collected patient image data through computer processing and guides doctors to complete the placement of internal fixation quickly and accurately.22,23 When placing pedicle screws in spine surgery, the robot navigation assistant system has been proven to have a better effect and lower complications compared with traditional surgery.12,13 In the operation of pelvic fracture, the insertion of a sacroiliac joint screw has the risk of iatrogenic vascular and nerve injury and requires a long learning curve. The robot navigation assistant system can help doctors to insert sacroiliac joint screws safely and accurately.24,25 For PFNA fixation of the femoral intertrochanteric fracture, the accurate insertion point is one of the important factors that determine the surgical effect.8,9 Traditional surgery determines the position of the insertion point by touching the apex of the greater trochanter of the femur with fingers through the lateral femoral incision. For patients with poor reduction or obesity, it is necessary to extend the incision and repeatedly probe. These operations will prolong the operation time and aggravate the damage to surrounding tissues. Elderly patients have a higher risk of various complications. Reducing trauma and bleeding and shortening operation time is of great significance to the prognosis of patients.1 The robot navigation system can help doctors insert the guide pin of the main nail accurately according to the collected patient image information, avoid excessive stripping of surrounding soft tissue, shorten the operation time, and reduce the incidence of postoperative complications in elderly patients with hip fractures.22
In this study, the intraoperative bleeding, operation time, the length of incision of mail nail insertion, blood transfusion rate, postoperative hemoglobin drop, and Harris score of the hip joint in the two groups were compared. The results showed that the robot group had less intraoperative bleeding, shorter operation time, shorter main nail incision, lower blood transfusion rate, and lower postoperative hemoglobin drop value (P<0.05). The intraoperative blood loss in this study refers to visible blood loss, while hidden blood loss is difficult to accurately observe, so this study did not explore. One study26 has shown that the visible blood loss of PFNA fixation for femoral intertrochanteric fractures was approximately 147.3 ± 81.6mL, which is consistent with the results of the traditional surgical group in our study. The robot navigation system can help surgeons accurately and quickly insert guide pins, which is beneficial for reducing surgical bleeding. There was no statistical difference in Harris score of the hip joint in the first year after operation (P>0.05). In some studies, it is not clear whether the robot planning time is included in the operation time. The robot planning stage has not caused surgical trauma to patients, so the operation time in this study does not include the robot planning time.23 The robot navigation assistant system has small trauma and high accuracy, avoids the repeated stripping of soft tissue around the greater trochanter during the operation, and the process of inserting the guide needle is simpler, so the intraoperative bleeding is less, the operation time is shorter, and the main nail incision is shorter. On the other hand, some elderly patients have anemia and poor nutritional status, while the intertrochanteric part of the femur is mainly cancellous bone. After the fracture, there is much bleeding, which will inevitably cause trauma to the body during the operation process: for example, PFNA needs to be operated in the femoral bone marrow, and some also need to be reamed, these factors will aggravate the blood loss of patients, and may need a blood transfusion to improve the anemia of patients. A blood transfusion will increase the risk of complications such as deliration elderly patients.27–29 The robot navigation assistant system has smaller surgical incisions, more accurate guide needle insertion, and a higher success rate. This will make the operation time shorter, the trauma smaller, less apparent and hidden blood loss, and lower the blood transfusion rate in the perioperative period compared with the traditional operation group. In addition, the robot navigation system has a higher success rate of inserting the guide needle, which can reduce the radiation damage to patients and surgical staff, which is a protection for our surgical staff, and also a major advantage of the robot navigation technology.
In the process of PFNA fixation of femoral intertrochanteric fracture assisted by the robot navigation system, it should be noted that robot navigation assistance does not mean that fracture reduction is not required, and it should be ensured that the fracture is well reduced before inserting the guide pin. For stable fractures, the reduction may be relatively simple, and the robot navigation system can complete the placement of the main nail through smaller trauma; For the femoral intertrochanteric fracture with difficult reduction, it may still need to open reduction, extend the surgical incision and other operations, but the robot navigation technology has great advantages in the success rate of inserting the guide needle, and the corresponding operation time and intraoperative blood loss will be reduced. For elderly patients, it can reduce the occurrence of various complications after the operation, which is conducive to postoperative recovery. In traditional surgery, the position of the apex of the large tuberosity needs to be exposed to judge the position of the needle insertion point. Therefore, unclear exposure, visual differences, and the instability of the unarmed operation may lead to differences between the insertion path of the guide needle and the planned path (ideal path), which requires repeated attempts during the operation. The advantage of the robot navigation system is that it can ensure the completion of the insertion of the guide needle in the planned path at one time, and avoid the trauma caused by the repeated operation. However, the robot navigation is very expensive.30 The cost of most surgical robots is more than US $1 million. The high cost may lead to the failure of robot navigation technology to be widely used.30,31 Robotic navigation technology requires a long learning cycle, which is different from the thinking mode of traditional surgery. Robotic navigation surgery requires more detailed planning before surgery and is familiar with the use of a robot navigation system. In this study, our surgeon has received at least one year of training in robot navigation technology.
Of course, our research also has some limitations. First of all, this is a single-center study with a small sample size, and we are looking forward to a large sample and multi-center study in the future; Secondly, our follow-up time is relatively short. We found no difference between the two groups in the evaluation of the joint function of the patients one year after the operation, and this result may change after a longer follow-up.
Conclusion
Compared with traditional surgical methods, PFNA fixation assisted by a robot navigation system has shorter operation time, less intraoperative bleeding, shorter incision, lower perioperative blood transfusion rate, and lower postoperative hemoglobin drop. The robot navigation system has certain advantages for elderly patients with intertrochanteric fractures of the femur, which is beneficial to the rehabilitation of elderly patients and reduces the occurrence of postoperative complications.
Data Sharing Statement
The data is available from the corresponding author upon the reasonable request.
Ethical Approval and Consent to Participate
This study is a single-center retrospective clinical control, which was approved by the Ethics Committee of Xi’an Hong Hui Hospital. During the study, we strictly followed the relevant requirements and ethical standards of the Helsinki Declaration, and all patients included in the study signed a written informed consent.
Consent for Publication
Informed consent was obtained from all the participants and/or their legal guardian to publish their information.
Acknowledgments
We would like to thank the participants of this study and the members of the Department of Traumatology and Orthopedics of Xi’an Hong Hui Hospital for their strong support.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by a project grant from the Scientific Research Program Funded by Shaanxi Provincial Education Department (Grand No.22JK0541).
Disclosure
The authors have no conflicts of interest to declare in this work.
References
1. Bhandari M, Swiontkowski M, Solomon CG. Management of acute hip fracture. New Engl J Med. 2017;377(21):2053–2062. doi:10.1056/NEJMcp1611090
2. Tay E. Hip fractures in the elderly: operative versus nonoperative management. Singapore Med J. 2016;57(4):178–181. doi:10.11622/smedj.2016071
3. Mingli F, Huiliang S, Guanglei C, et al. A clinical study on arthroplasty for failed internal fixation of hip fractures and review of literature. Pak J Med Sci. 2017;33(4):798–803. doi:10.12669/pjms.334.12459
4. Parker MJ, Bowers TR, Pryor GA. Sliding hip screw versus the targon PF nail in the treatment of trochanteric fractures of the Hip: a randomised trial of 600 fractures. J Bone Joint Surg Br. 2012;94(3):391–397. doi:10.1302/0301-620x.94b3.28406
5. Xu YZ, Geng DC, Mao HQ, et al. A comparison of the proximal femoral nail antirotation device and dynamic hip screw in the treatment of unstable pertrochanteric fracture. J Int Med Res. 2010;38(4):1266–1275. doi:10.1177/147323001003800408
6. Little NJ, Verma V, Fernando C, et al. A prospective trial comparing the Holland nail with the dynamic hip screw in the treatment of intertrochanteric fractures of the Hip. J Bone Joint Surg Br. 2008;90-B(8):1073–1078. doi:10.1302/0301-620x.90b8.20825
7. Bojan AJ, Beimel C, Speitling A, et al. 3066 consecutive gamma nails. 12 years experience at a single centre. BMC Musculoskelet Disord. 2010;11(1). doi:10.1186/1471-2474-11-133
8. Mavrogenis AF, Panagopoulos GN, Megaloikonomos PD, et al. Complications after hip nailing for fractures. Orthopedics. 2016;39(1):e108–e116. doi:10.3928/01477447-20151222-11
9. Ostrum RF, Marcantonio A, Marburger R. A critical analysis of the eccentric starting point for trochanteric intramedullary femoral nailing. J Orthop Trauma. 2005;19(10):681–686. doi:10.1097/01.bot.0000184145.75201.1b
10. Leblanc ES, Hillier TA, Pedula KL, et al. Hip fracture and increased short-term but not long-term mortality in healthy older women. Arch Intern Med. 2011;171(20):1831–1837. doi:10.1001/archinternmed.2011.447
11. Liu HS, Duan SJ, Xin FZ, et al. Robot-assisted minimally-invasive internal fixation of pelvic ring injuries: a single-center experience. Orthop Surg. 2019;11(1):42–51. doi:10.1111/os.12423
12. Karthik K, Colegate-Stone T, Dasgupta P, et al. Robotic surgery in trauma and orthopaedics: a systematic review. Bone Joint J. 2015;97-b(3):292–299. doi:10.1302/0301-620x.97b3.35107
13. Karuppiah K, Sinha J. Robotics in trauma and orthopaedics. Ann R Coll Surg Engl. 2018;100(6_sup):8–15. doi:10.1308/rcsann.supp1.8
14. Digioia AM, Jaramaz B, Colgan BD. Computer assisted orthopaedic surgery. Image guided and robotic assistive technologies. Clin Orthopaedics Related Res. 1998;354:8–16. doi:10.1097/00003086-199809000-00003
15. Li F, Zhu L, Geng Y, et al. Effect of hip replacement surgery on clinical efficacy, VAS score and Harris hip score in patients with femoral head necrosis. Am J Transl Res. 2021;13(4):3851–3855.
16. Weel H, Lindeboom R, Kuipers SE, et al. Comparison between the Harris- and oxford hip score to evaluate outcomes one-year after total hip arthroplasty. Acta Orthop Belg. 2017;83(1):98–109.
17. Han J, Hahn MH. Proximal femoral geometry as fracture risk factor in female patients with osteoporotic hip fracture. J Bone Metab. 2016;23(3):175–182. doi:10.11005/jbm.2016.23.3.175
18. Roberts KC, Brox WT, Jevsevar DS, et al. Management of hip fractures in the elderly. J Am Acad Orthop Surg. 2015;23(2):131–137. doi:10.5435/jaaos-d-14-00432
19. Mu W, Zhou J, Gu C. PFNA-II internal fixation helps hip joint recovery and improves quality of life of patients with lateral-wall dangerous type of intertrochanteric fracture. Biomed Res Int. 2021;2021(5911868):1–6. doi:10.1155/2021/5911868
20. Shen L, Zhang Y, Shen Y, et al. Antirotation proximal femoral nail versus dynamic hip screw for intertrochanteric fractures: a meta-analysis of randomized controlled studies. Orthop Traumatol Surg Res. 2013;99(4):377–383. doi:10.1016/j.otsr.2012.12.019
21. Lanfranco AR, Castellanos AE, Desai JP, et al. Robotic surgery: a current perspective. Ann Surg. 2004;239(1):14–21. doi:10.1097/01.sla.0000103020.19595.7d
22. Lan H, Tan Z, Li K-N, et al. Intramedullary nail fixation assisted by orthopaedic robot navigation for intertrochanteric fractures in elderly patients. Orthop Surg. 2019;11(2):255–262. doi:10.1111/os.12447
23. Schuijt HJ, Hundersmarck D, Smeeing DPJ, et al. Robot-assisted fracture fixation in orthopaedic trauma surgery: a systematic review. OTA Int. 2021;4(4):e153. doi:10.1097/oi9.0000000000000153
24. Liu H-S, Duan S-J, Liu S-D, et al. Robot-assisted percutaneous screw placement combined with pelvic internal fixator for minimally invasive treatment of unstable pelvic ring fractures. Int J Med Robot. 2018;14(5):e1927. doi:10.1002/rcs.1927
25. Wang JQ, Wang Y, Feng Y, et al. Percutaneous sacroiliac screw placement: a prospective randomized comparison of robot-assisted navigation procedures with a conventional technique. Chin Med J. 2017;130(21):2527–2534. doi:10.4103/0366-6999.217080
26. Yang X, Wu Q, Wang X. Investigation of perioperative hidden blood loss of unstable intertrochanteric fracture in the elderly treated with different intramedullary fixations. Injury. 2017;48(8):1848–1852. doi:10.1016/j.injury.2017.06.017
27. Lemaire R. Strategies for blood management in orthopaedic and trauma surgery. J Bone Joint Surg Br. 2008;90(9):1128–1136. doi:10.1302/0301-620x.90b9.21115
28. Hill GE, Frawley WH, Griffith KE, et al. Allogeneic blood transfusion increases the risk of postoperative bacterial infection: a meta-analysis. J Trauma. 2003;54(5):908–914. doi:10.1097/01.ta.0000022460.21283.53
29. Bursi F, Barbieri A, Politi L, et al. Perioperative red blood cell transfusion and outcome in stable patients after elective major vascular surgery. Eur J Vasc Endovasc Surg. 2009;37(3):311–318. doi:10.1016/j.ejvs.2008.12.002
30. Turchetti G, Palla I, Pierotti F, et al. Economic evaluation of da Vinci-assisted robotic surgery: a systematic review. Surg Endosc. 2012;26(3):598–606. doi:10.1007/s00464-011-1936-2
31. Ahmed K, Ibrahim A, Wang TT, et al. Assessing the cost effectiveness of robotics in urological surgery - a systematic review. BJU Int. 2012;110(10):1544–1556. doi:10.1111/j.1464-410X.2012.11015.x
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.