")
Back to Journals » Research and Reports in Urology » Volume 15
Robot-assisted Surgery in the Field of Urology: The Most Pioneering Approaches 2015–2023
Authors Franco A, Ditonno F, Manfredi C, Johnson AD, Mamgain A, Feldman-Schultz O, Feng CL, Pellegrino AA, Mir MC, Porpiglia F, Crivellaro S, De Nunzio C, Chow AK, Autorino R
Received 27 July 2023
Accepted for publication 30 September 2023
Published 9 October 2023 Volume 2023:15 Pages 453—470
DOI https://doi.org/10.2147/RRU.S386025
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Panagiotis J Vlachostergios
Antonio Franco,1,2 Francesco Ditonno,1,3 Celeste Manfredi,1,4 Andrew D Johnson,1 Avinash Mamgain,1 Oren Feldman-Schultz,1 Carol L Feng,1 Antony A Pellegrino,5,6 Maria Carmen Mir,7 Francesco Porpiglia,8 Simone Crivellaro,5 Cosimo De Nunzio,2 Alexander K Chow,1 Riccardo Autorino1
1Department of Urology, Rush University, Chicago, IL, USA; 2Department of Urology, Sant’Andrea Hospital, Sapienza University, Rome, Italy; 3Department of Urology, University of Verona, Verona, Italy; 4Urology Unit, “Luigi Vanvitelli” University, Naples, Italy; 5Department of Urology, University of Illinois at Chicago, Chicago, Illinois, USA; 6Unit of Urology/Division of Oncology, IRCCS San Raffaele Scientific Institute, Milan, Italy; 7Department of Urology, Hospital Universitario La Ribera, Valencia, Spain; 8Department of Oncology, Division of Urology, University of Turin, San Luigi Gonzaga Hospital, Orbassano, Italy
Correspondence: Riccardo Autorino, Professor of Urology, Director of Surgical Innovation & Clinical Research, Department of Urology, Rush University Medical Center, 1725 W Harrison St Professional Building – Suite 970, Chicago, IL, 60612, USA, Email [email protected]; [email protected]
Abstract: Robot-assisted surgery has emerged as a transformative technology, revolutionizing surgical approaches and techniques that decades ago could barely be imagined. The field of urology has taken charge in pioneering a new era of minimally invasive surgery with the ascent of robotic systems which offer enhanced visualization, precision, dexterity, and enabling surgeons to perform intricate maneuvers with improved accuracy. This has led to improved surgical outcomes, including reduced blood loss, lower complication rates, and faster patient recovery. The aim of our review is to present an evidence-based critical analysis on the most pioneering robotic urologic approaches described over the last eight years (2015– 2023).
Keywords: robotic urologic surgery, robot-assisted, minimally invasive, image-guided surgery, single port robot
Introduction
Over the past decade, there has been a significant surge in the adoption of robotic surgery. Publications on robotic surgery in urology alone imply a four-fold increase in the number of robot-assisted procedures performed.1 The main advantages of standard laparoscopy over open surgery were mostly related to lower surgical morbidity including decreased blood loss, shorter length of hospital stay, and fewer complications.2,3 The popularity of robot-assisted surgery over conventional laparoscopy can be attributed to its enhanced surgical precision, higher magnification and easier wrist manipulation.4 From the first Da Vinci™ robotic surgical system’s (Intuitive Surgical, Sunnyvale, CA, USA) release in 2000 to the latest single-port (SP) platform recently approved by FDA in 2018, many advances have been made. Several pioneering approaches have been introduced, also fostered by technological innovations, such as augmented reality, artificial intelligence, and the new multiport robotic surgical systems.
The aim of the present review is to summarize the most recent advances in robot-assisted surgery in the field of urology, highlighting their potential benefits and limitations.
Evidence Acquisition
A nonsystematic literature review was performed using PubMed and Scopus to retrieve publications related to robotic surgery in urology from 2015 to 2023. In the free-text protocol, the following terms were applied: robotic urologic surgery; robotic prostate surgery; robotic kidney surgery; robotic ureteral surgery; robotic bladder surgery; robotic lymphadenectomy; robotic urology. Review articles, editorials, commentaries, and letters to the editor were included only if considered relevant to the topic. References from selected articles were also assessed for inclusion. An evidence-based critical analysis was conducted by focusing on the latest innovative approaches described in the literature. A summary of the most pioneering techniques between 2015 and 2023 is provided in Figure 1.
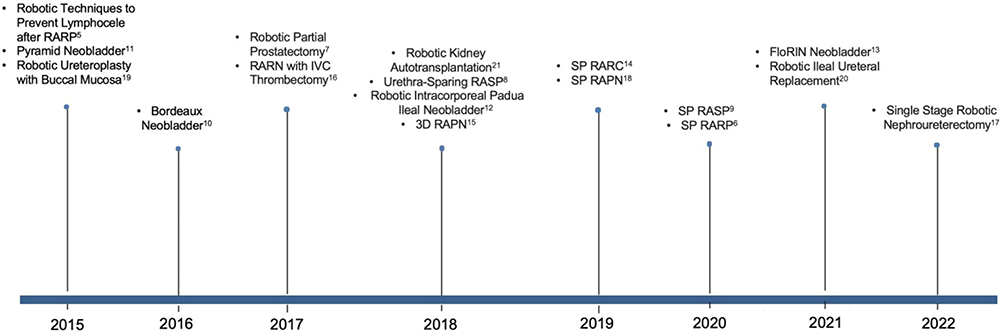 |
Figure 1 Summary of the most pioneering techniques between 2015 and 2023. Abbreviations: RARP, robot-assisted radical prostatectomy; RARN, robot-assisted radical nephrectomy; IVC, inferior vena cava; RASP, robot-assisted single prostatectomy; RAPN, robot-assisted partial nephrectomy; RARC, robot-assisted radical cystectomy. Note: Data from these studies.5–21 |
Robot-assisted Radical Prostatectomy
Robot-assisted radical prostatectomy (RARP) was first described in 2000.22 Since then, several techniques have been described as this procedure has become de facto the new gold standard in prostate cancer surgery. When looking at last 8 years, advances in the field of RARP have been made in the direction of maximizing the functional outcomes of the procedure, minimizing the risk of lymphocele formation, exploring new approaches to the prostate, and testing the feasibility of a “partial” prostatectomy.
Techniques to Improve Functional Outcomes
Techniques to Improve Urinary Continence
Bahler et al23 reported a randomized trial on the use of a small intestinal submucosa bladder neck sling to expedite return to continence after RARP. While there were no increasing obstructive symptoms, the sling failed to show a significant improvement at 1 month postoperatively. In contrast, Canvasser et al24 found a beneficial effect of a posterior urethral suspension on objective measures of urinary control in the early weeks after RARP.24 Nguyen et al failed to demonstrate a benefit in using an autologous urethral sling placement on early return of continence at 6 months.25
A team at Mount Sinai Hospital developed the “Hood” technique to optimize urinary continence after RARP. The technique is based on the concept of preserving the contents of the space of Retzius by using an anterior approach, thus sparing the pouch of Douglas. Preserved tissue after prostate removal has the appearance of a “hood” comprising the detrusor apron, arcus tendinous, puboprostatic ligament complex, endopelvic fascia, and anterior vessels, and some fibers of the detrusor muscle (Figure 2). This hood surrounds and safeguards the membranous urethra, external sphincter, and supportive structures that remain untouched. In their initial series, a continence rate (defined as completely pad free) was achieved in 83%, 91% and 95% of patients at 1, 3, and 12 months, respectively.26 Furthermore, a study from Shimmura et al compared a modified Hood technique-RARP to standard and umbilical ligament preservation RARP, suggesting a complete (100%) continence recovery at 6 months follow-up.27
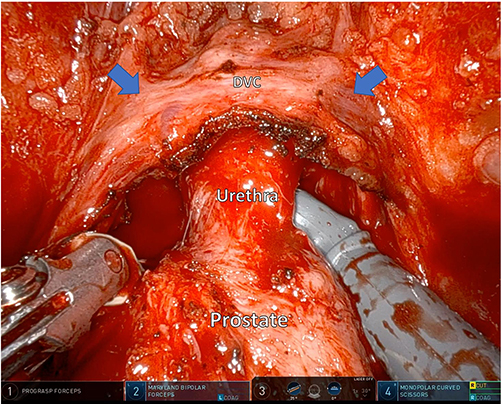 |
Figure 2 Hood Technique. Blue arrows indicate the “hood” containing the detrusor apron, arcus tendineus, puboprostatic ligament, anterior vessels, and some fibers of the detrusor muscle. Abbreviation: DVC, deep vein complex. |
Techniques to Improve Sexual Potency
First described by the Martini Clinic group,28 the neurovascular structure-adjacent frozen-section examination (NeuroSAFE) technique aims to achieve the best possible oncological outcomes while preserving erectile function in the setting of nerve-sparing RARP. Once the prostate is dissected and removed, the specimen is then painted on the surface of where the neurovascular bundles (NVBs) are dissected and sprayed with an ink aid, to better examine the presence of tumor foci on histopathology analysis. If tumor is present, the ipsilateral NVB is completely dissected. Despite the short follow-up, several series have adopted this approach with encouraging results, showing higher potency rates while maintaining lower PSM rate at the same time.29–31
De Carvalho et al32 proposed a technical modification for the nerve sparing RARP to allow maximal preservation of sexual potency. Their technical modification consisted in the release of the neurovascular bundle by starting at the level of the bladder neck, developing an avascular plane underneath the dorsal venous complex, without opening the endopelvic fascia. Potency was achieved in 53% and 86% of patients at 1 month and 1 year follow-up. Overall oncological outcomes were in line with standard techniques.32
Techniques to Prevent Lymphocele Formation
Lymphocele is the most frequent complication after radical prostatectomy and its incidence has been reported between 0% to 8%, with controversial results regarding the adopted template (extended vs standard) or the considered approach (transperitoneal vs extraperitoneal).33 Some recent studies have proposed new intriguing robot-assisted techniques using peritoneal reconstruction as an intervention to prevent the formation of lymphocele5,34–42 (Table 1). Overall, all these studies suggest that the use of a peritoneal flap translates into a reduced risk of lymphocele formation. Moreover, a randomized controlled phase-3 trial (PELYCAN) was published later this year, suggesting the role of bilateral peritoneal reconfiguration as a standard procedure associated to RARP to prevent lymphocele formation.43
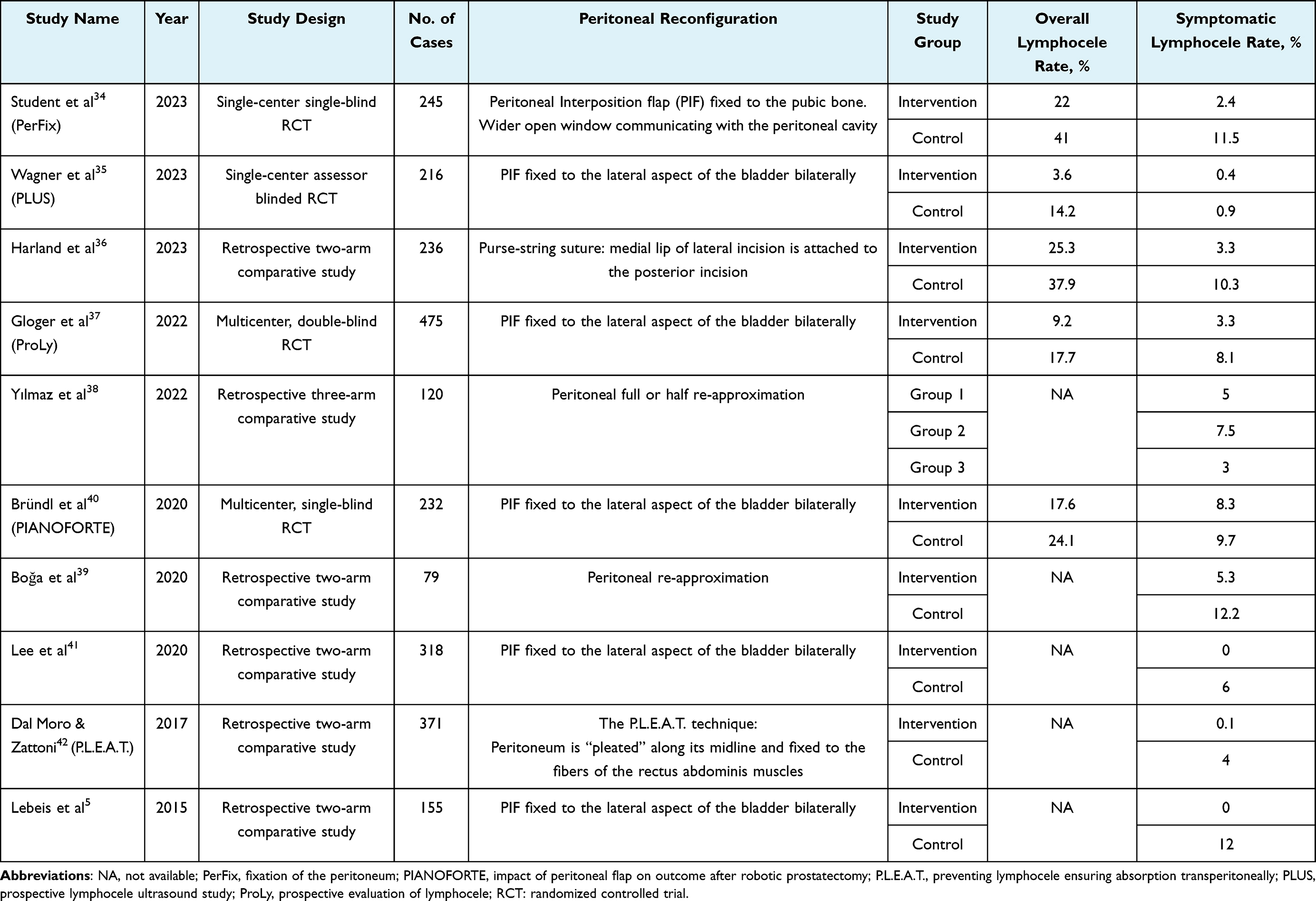 |
Table 1 Main Characteristics of Lymphocele Prevention Techniques |
Single Port Approaches to RARP
In 2018, the Da Vinci Single Port (SP) system was approved by the FDA for urologic surgery. This novel platform accommodates all the robotic instruments and camera through a single multichannel 2.5 cm port inserted through a single skin incision. Although current available literature on SP is limited,44,45 the adoption of this technology is progressively increasing in the United States. The implementation of the SP platform to the RARP procedure paved the way to the “rediscovery” of old surgical approaches (extraperitoneal, transperineal) and the exploration of novel ones (transvesical).
Extraperitoneal SP RARP
Extraperitoneal RARP has regained popularity with the advent of SP platform,46 which features minimization of instrument clashing and workspace maximization within the patient, all peculiarities that makes it perfectly fit for extraperitoneal space. First description of the extraperitoneal SP RALP was reported by Kaouk et al, who described the feasibility of the technique and compared its outcomes with those of standard multiport transperitoneal RARP. They found superior pain control, early recovery of bowel function and decreased hospital stay.6,47
Transvesical SP RALP
A transvesical approach was first described by Desai et al48 in a cadaver model back in 2008. More recently, Zhou et al49 shared their initial clinical experience using the using the Da Vinci Si/Xi system. Robotic ports are placed directly into the urinary bladder in a W standard configuration; bladder incision is performed on the posterosuperior aspect of the bladder and usually suspension stitches are passed through the lateral abdominal wall to allow optimal exposure.49 The procedure is then carried out similarly to the transverse circular anterior dissection, moving posteriorly. Similarly, this access can be performed using the transperitoneal approach by making an incision in the bladder and entering it, essentially creating a hybrid extraperitoneal/intraperitoneal technique.50
Given the advantage of transvesical approach in preserving the Retzius’ space, this technique was first performed to obtain better urinary continence recovery.51 Indeed, Deng et al52 showed an increased very early continence rate compared to the standard transperitoneal approach, but the significant difference between the two groups in UC recovery appeared to disappear at last follow-up. No significant differences were noticed in terms of postoperative complications and oncological outcomes.
Recently Kaouk et al described the transvesical approach utilizing the SP robotic platform with the first 100 cases performed with single incision.53 This approach allowed same day discharge, improved pain control without use of opioids, and 75% with early continence at 48 h following catheter removal.
Retzius-Sparing SP RARP
The Retzius-sparing (RS-RARP) approach was first described by Bocciardi et al in Milan in 2010.54 This technique keeps the bladder suspended in its native anatomical position, sparing Santorini’s plexus, endopelvic fascia, puboprostatic ligaments, and the other anterior compartment structures. However, adoptees of this approach must acknowledge the risk of positive surgical margins, particularly for anterior lesions and high-grade disease. To overcome these limitations, Dell’Oglio et al analyzed a large series of RS-RARP in high-risk prostate cancer patients, performing a modified RS approach where substantially parts of the Denonvillier’s fascia (DVF) and of the perirectal fat are left attached to the seminal vesicles and removed with the specimen, gaining optimal outcomes.55
SP Retzius-sparing radical prostatectomy’ (SP-rsRARP) initial experience has been also described.56,57 Balasubramanian et al described the largest cohort of SP-rsRARP, comparing this approach to the extraperitoneal and transperitoneal ones. Faster and improved returns of both continence and erection were recorded with this technique.58 However, a steep learning curve and potential complications still make this surgical procedure demanding.56
Transperineal SP RARP
Although perineal radical prostatectomy was the most common access for surgical treatment of prostate cancer for almost seven decades, this technique became less favored due to technical complexity and the narrow operative space.59 Moreover, this approach also did not allow access for pelvic lymph node dissection. The use of robotic assistance, especially with the introduction of the SP platform, has led to a renewed interest in transperineal radical prostatectomy,60,61 however its feasibility is still confined to selected centers with high expertise on this technique.
Access for transperineal RARP is obtained by making a transverse incision in the perineum on a semicircumferential line connecting the ischial tuberosity. Then, the recto-urethralis muscle is divided, the external urethral sphincter is retracted, and the pubococcygeus branches of the levator ani are divided. The Xi robot is docked, and the prostate is identified. The Denonvilliers fascia is dissected, and the prostate is freed toward the vasa deferentia and seminal vesicles. The dissection then moves laterally and the NVBs are dissected. The apical dissection is then performed, and the anterior prostatic dissection in a caudocranial fashion finally completes the procedure.62 The feasibility of pelvic lymph node dissection and nerve sparing approach was shown using Da Vinci Xi System on a single Gel-port platform.63,64
The Cleveland Clinic group reported the only clinical series on SP transperineal RARP.65 The steps resemble the multiport approach, including a bilateral pelvic lymphadenectomy with SP platform. Equivalent functional and oncological outcomes at 12 months were noted when comparing SP perineal to the multiport transperitoneal RARP, but at cost of higher complication and positive surgical margin rates (38.5% vs 7.7%, p<0.01).65 In summary, minimally invasive perineal approach may represent a valid option in patients with previous abdominal surgery, also offering the chance to perform bilateral lymphadenectomy without another access, as previously reported during open perineal radical prostatectomy.66
SP Robotic Partial Prostatectomy
Focal therapy has emerged as a promising approach for the management of localized prostate cancer, aiming to balance cancer control and preservation of quality of life.67 However, limitations such as accurate lesion identification, potential undertreatment of multifocal tumors, long-term oncological outcomes, and patient selection still need to be addressed, especially regarding intermediate-risk disease.68,69 Based on the same rationale of focal therapy, initial subtotal or partial RARP techniques have been explored.
A team at Vattikuti Institute described their novel technique of “precision” prostatectomy, a form of surgical focal therapy that allows radical excision of the index lesion along with >90% prostatic tissue extirpation, while preserving the prostatic capsule and seminal vesicle/vas deferens complex on the side contralateral to the dominant cancer lesion. Overall, 88 patients were prospectively enrolled and up to 90% of them were totally continent, potent and free from clinically significant residual cancer, without need for any further type of treatment.70
Villers et al proposed an “anterior” partial prostatectomy for anterior cancers originating also from the transitional zone of the prostate in 17 patients with a median follow-up of 30 (IQR 25–70) months. Due to a possible damage to the external sphincter with thermal energy delivering the authors developed en bloc excision of the anterior part of the prostate including the anterior fibromuscular stroma, the bladder neck, prostate adenoma along with the proximal prostate urethra, the apical anterior horns, anterior aspect of the distal urethra, and anterior bladder neck. Despite the feasibility of the procedure and satisfying functional outcomes, initially the sample size was limited and 24% of patients recurred, undergoing a complete radical prostatectomy.7 Later this year, the same group published an updated series of 28 patients with a median follow-up of 7 (IQR 4.2–8) years, where 62.7% (35.0–81.3%) of patients were free of recurrence after 7 years.71
With the advent of SP platform, Kaouk et al pioneer a “partial” prostatectomy in nine patients with low-volume, localized, low- to intermediate-risk prostate cancer by a transvesical approach: once the access to the prostate was gained through a 2 cm vertical midline cystotomy, an ultrasound-MRI fusion software (Koelis, Princeton, NJ) was used to identify and target the lesion. Again, although results appear encouraging with no complications were reported and acceptable functional and oncological outcomes, sample was very limited.72
New Multiport Robotic Surgical Systems for RARP
Several novel multiport robotic surgical systems have been developed over the past decade, and some have recently been introduced into clinical practice.73 In June 2022 Fan et al74 published the first series of RARP by using the KangDuo Surgical Robot-01 (KD-SR-01). This new platform consists of a surgeon control console, a 3-arm patient cart, a high-definition vision cart and reusable endoscopic instruments, allowing a more comfort posture and good ergonomics overall. Sixteen patients successfully underwent extraperitoneal RARP. Median docking time, console time and urethrovesical anastomosis time were 5.9, 87, and 14.4 min, respectively. A positive surgical margin was recorded in 25% of the cohort.74
In 2017 the Senhance® robotic system (Asensus Surgical, Durham, NC, USA) was approved in the US. In contrast to Da Vinci system, the Senhance robot is designed to be compatible with traditional laparoscopic trocars and mimics laparoscopic style handle, owing to its open console and four separate arms. Kastelan et al described an initial series of 40 cases performed through the extraperitoneal approach.75 The largest series published so far was conducted by Venckus et al, who performed a prospective analysis of 127 patients undergoing RARP. Among these patients, a pelvic lymph node dissection was carried out in 16.5% of cases, and nerve-sparing surgery was performed on at least one side in 29.1% of cases. The positive surgical margin rate in this series was a bit higher (33.9%) than what is reported in the literature.76
Rocco et al reported the first successful use of the Versius robotic system (CMR, Cambridge, UK) performing a radical prostatectomy in 2023.77 As a major difference from the Da Vinci system, the device controls are exclusively hand controlled and the console is wide open. Reeves et al reported 10 cases performed in the UK, including four radical prostatectomies: no incidences of conversion or major complications were reported and only one patient experienced a urine leak requiring delayed catheter removal.78
Not yet approved by FDA in the United States, the Hugo RAS™ system (Medtronic, Minneapolis, MN, USA) is gaining momentum among the urologist robotic surgeons in Europe. Four independent arm carts and an open console with two arm-controllers characterized this novel platform. First series of RARP were described79,80 with no conversion nor system failure reported. More recently, a nonrandomized study comparing radical prostatectomy outcomes between the Hugo RAS and the Da Vinci system showed no significant disparities in terms of total operative time or console time. To note, although the docking process took more time with the Hugo RAS, the presence of independent arms provided enhanced flexibility and increased working space for the bedside assistant.81
Robot Assisted Simple Prostatectomy
In recent years, robot assisted simple prostatectomy (RASP) has become one the minimally invasive techniques for the surgical treatment of severe lower urinary tract symptoms due to benign prostatic enlargement.82 It is primarily recommended for patients with large prostate glands (>80–100 mL) as an alternative to currently available and rapidly evolving transurethral enucleation techniques.83,84
Although robotic simple prostatectomy has been traditionally performed following Freyer85 and Millin86 techniques, new approaches has been recently explored.
Urethra-Sparing (Madigan) RASP
The urethra-sparing (usRASP) technique was first proposed8 to preserve anterograde ejaculation. Dissection is meticulously performed in an antegrade fashion, ensuring the avoidance of urethral injuries as the apex is approached. Following the dissection of the apex, the prostatic lobe is excised to enhance exposure of the contralateral lobe, which is subsequently dissected and removed. To assess urethral integrity, the bladder is filled with 100–150 mL of saline while carefully examining the urethra for any signs of perforation.
A modification of this approach was proposed later87 using near-infrared fluorescence imaging to better identify the proximal urethra filled with 50 mL of indocyanine green. Results appeared encouraging, ensuring satisfactory anterograde ejaculation in 66% of the cohort analyzed and avoidance of continuous bladder irrigation.87 Porpiglia et al compared their series of usRASP with a standard Millin RASP cohort: interestingly, 81% of usRASP patients maintained anterograde ejaculation at 1 year of follow-up; same perioperative and urinary functional outcomes were reported between the two groups, but with an improvement in terms of sexual function, especially for the ejaculation for the usRASP technique.88
To note, the presence of large lateral lobes and/or medium lobe protruding into the bladder neck is a contraindication to this approach, increasing the risk of missing the proper dissection plane, and thus leading to an incomplete resection with a potential risk of BPH recurrence.87
SP RASP
The idea of performing a RASP through a transvesical (percutaneous) single incision approach was initially explored by Cleveland Clinic group in 2012 using the multiport Da Vinci robot. Despite being feasible and providing adequate relief of LUTS, the procedure carried high risk of complications, likely because of lack of adequate instrumentation.89 With the introduction of the SP system, this idea could be revisited, as first reported.9 Direct access to the bladder was achieved through a 3 cm midline suprapubic skin incision over a needle guide puncture, after filling the bladder with saline. Dissection is carried on through the abdominal wall into the bladder. A Gelpoint port was placed, and robot was docked; dissection of the prostate adenoma was performed using the prostate capsule as a landmark. Benefits of this technique were the total extraperitoneal access, no bowel manipulation and fast access to the adenoma. Furthermore, concomitant bladder disease such as bladder stones or bladder diverticula can be managed simultaneously. Limitations include difficulties in handling very large adenoma and a limited traction of the instruments when dissecting the adenoma.90 Having achieved these promising results, a few studies started to compare SP RASP vs Multi-Port RASP, assessing both perioperative outcomes and complications rate, which appear to be comparable between the two platforms. More in detail, SP RASP required a shorter hospital stay, less use of opioids, and a shorter Foley catheter duration.91,92
On April 28, 2023, the FDA recognized the safety and efficacy of this approach using the SP Platform and approved its use for simple prostatectomy. SP RASP is being adopted at many Institutions across the US, including Rush University Medical Center. Key points of transvesical technique – as described by Crivellaro at UIC (personal communication) – are: 3–4 cm midline transverse incision 3–4 fingerbreadths above the pubic symphysis with patient in the supine position; identification of the bladder dome under cystoscopic guidance with use of CO2 insufflation; use of the Access port (Intuitive Surgical, Sunnyvale, CA, US) with the Alexis internal ring into the bladder; optional additional transvesical 5 mm port under digital guidance); incision of the bladder mucosa overlying the middle lobe starting from its posterior aspect (Figure 3); enucleation of prostate adenoma from the base towards the apex; retrigonization.
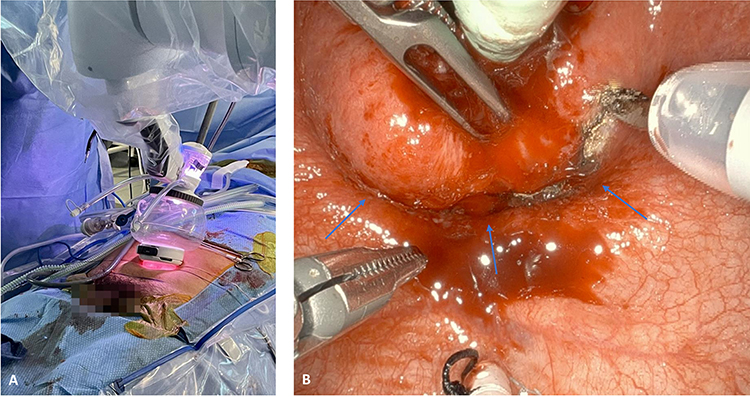 |
Figure 3 SP RASP. (A) Robot docking through SP access port (Intuitive Surgical, Sunnyvale, California, United States) (B) Intraoperative view of transvesical SP RASP. Blue arrows delimit the adenoma incision’s plane. Abbreviation: SP RASP, single port robot-assisted simple prostatectomy. |
Robotic Assisted Radical Cystectomy
Sexual-sparing RARC
As experience with robotic assisted radical cystectomy (RARC) matures, there has been an effort to optimize functional outcomes whenever possible. Therefore, different groups have looked at “sexual sparing” techniques during RARC. A team from Bordeaux10 described their technique of nerve and seminal vesicle sparing robot-assisted radical cystectomy. Attention was given to anatomical and functional intactness of proximal neurovascular plate; neurovascular tissue’s detachment from lateral prostate-vesicular angle and subsequent intrafascial dissection of periprostatic nerves to membranous urethra guarantee overall preservation of parasympathetic nerve supply to the corpora cavernosa. Sexual function was preserved in 72% of patients.
Pacchetti et al showed different approaches for sexual-sparing RARC in women. In this technique the anterior vaginal wall is preserved, as well as the vaginal pedicles. A modification of this approach can be indicated in case of young women with no pathological uterine and ovarian findings, by performing a fully sexual-sparing RARC where the vesicovaginal plan is gained without dissecting the vaginal dome and leaving internal genitalia intact. The vesicovaginal plan can also be developed after opening the vaginal dome. In doing so, the cervix may be subsequently dissected, and the vaginal pedicles with the anterior vaginal wall are preserved.93
Orthotopic Neobladder
A variety of orthotopic neobladder (ONB) techniques are currently used, and they do differ in the type of intestinal segment used, segment length, surgical approaches, and the folding construction of the reservoir.94 Several techniques have been explored during the last eight years, seeking either oncological radicality and functional outcomes11–13,95,96 (Table 2).
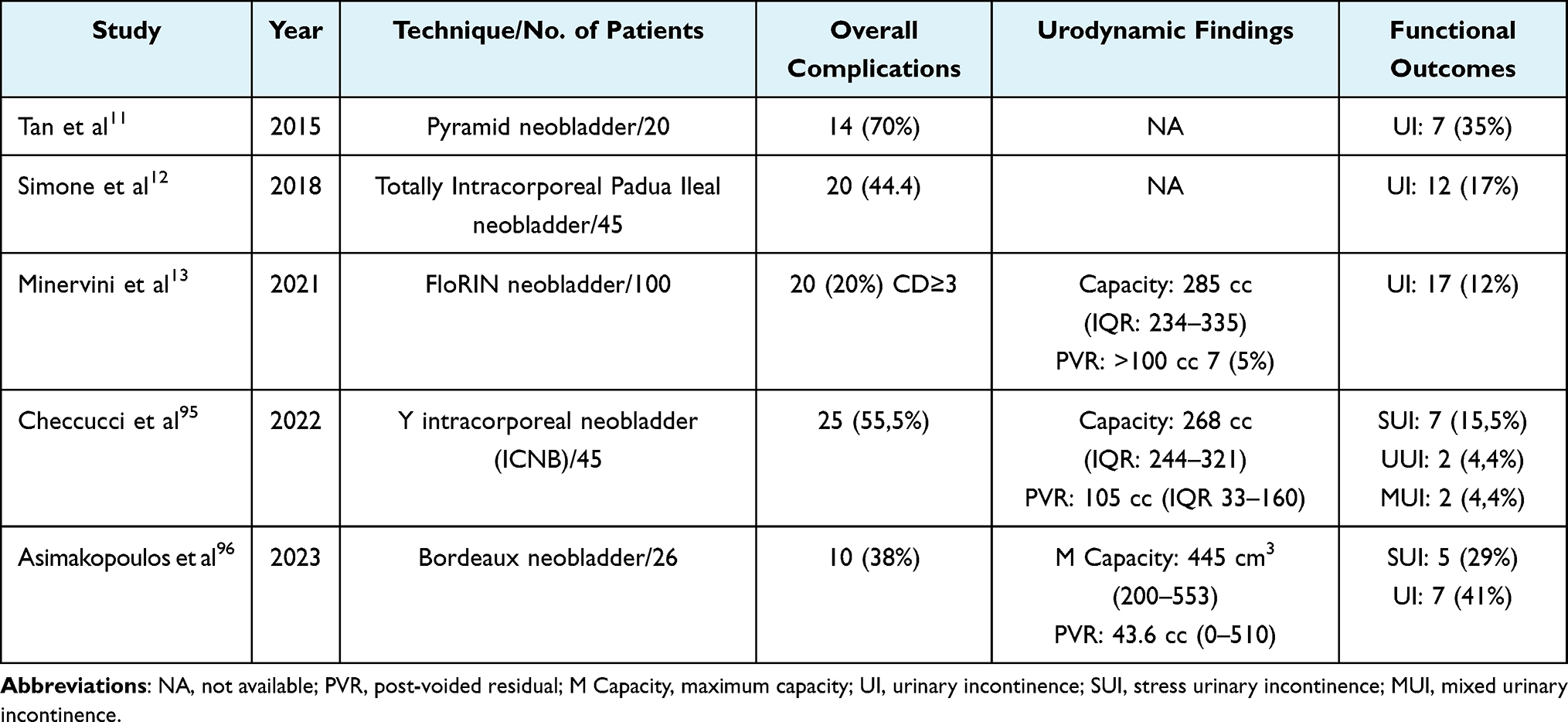 |
Table 2 Overall Complications and Functional Outcomes of Most Recent Orthotopic Neobladder Techniques (2015–2023) |
SP RARC
Preliminary outcomes are promising in the utilization of Da Vinci SP for RARC with intracorporeal ileal conduit urinary diversion. However, the current literature on this remains weak, consisting in few single-center studies with small sample sizes.14,97,98
Robotic Assisted Kidney Surgery
Hyperaccuracy 3D Model and Augmented Reality Assisted Robotic Partial Nephrectomy
Advantages of 3D models in robotic partial nephrectomy include enhancing visualization of renal masses ex vivo, thereby assisting in surgical planning, physician education and training, as well as patient counseling prior to the resection procedure.15 Augmented reality (AR) merges elements taken from the virtual 3D model with the surgeon’s real vision on the 3D vision in robot-assisted laparoscopy; the use of AR has historically required constant remapping of the Hyperaccuracy 3D model (HA3D) models to the anatomy itself. In 2021, Amparore et al99 attempted, for the first time, to remove this barrier by identifying landmarks on the kidney and linking the virtual model to the kidney, thus reducing operator’s dependence throughout the procedure, and confirming potential for application across all surgical specialties. In 2023, the same research group tested a new algorithm tool to estimate kidney perfusion regions and its role in assisting surgeons to perform safe and effective selective clamping during surgery. Results showed no differences between planning and surgery in terms of the number or order of arteries clamped or the perfusion regions that underwent ischemia.100 Overall, patients whose surgical planning involved 3D AR models proved to have longer operative time, but shorter warm ischemia time, lower transfusion rate, lower major complications, lower conversion rate to open, shorter length of stay, and lower rate of clampless procedures.101
Robot Assisted Radical Nephrectomy with IVC Thrombectomy
IVC thrombus occurs in up to 10% of RCC tumors.102 Recently, several groups shared their experience with minimally invasive approaches for IVC thrombectomy, describing promising results despite technical difficulties.16,103 As robotic approaches have evolved, there have been continued challenges due to anatomy barriers (SMA crossing left renal vein), IVC control, and contralateral renal clamping. As such, access to both sides of the retroperitoneum is required.104
In 2015, Gill et al from USC presented the initial series of completely intracorporeal robotic level III inferior vena cava tumor thrombectomy, describing a “IVC-first, kidney-last” technique where manipulation of the kidney is strictly reduced and only after thrombus extraction, to prevent thrombus dislodgment and subsequent pulmonary embolism. However, when a left side thrombus occurs, repositioning of the patient and robot re-docking is needed.105
In a recent technique report, Zhang et al106 demonstrated a hybrid method of both open and robotic approaches in the same surgery. Surgeons were able to approach the dissection of the renal mass and hilum utilizing the robot. A midline incision was performed to help with IVC thrombectomy and specimen removal. This open incision also allowed improved control of great vessels and contralateral renal hilum while avoiding unnecessary complications commonly seen with subcostal incisions.
Robot-assisted Bilateral Nephrectomy
Bilateral native nephrectomies have been recognized as necessary treatment in end stage renal disease (ESRD) patients waiting for renal transplantation.107 Gurung et al108 described the first robot-assisted bilateral synchronous nephrectomy (RABSN) for polycystic kidney disease in 2021. Due to often prior abdominal surgery/transplant, an open cut-down access to place a 12 mm assistant port approximately 10 cm below the umbilicus is conducted, eventually used for extraction of the specimens at the end of the procedure; four robotic ports are then placed in a fan-like distribution along the umbilical. In case of enormous cysts, puncture is allowed, as far as any malignancies suspicion is ruled out. Nephrectomies are then performed in the usual fashion, redocking and repositioning the patient to the desired side. Seven patients successfully completed the procedure reporting only two Clavien-1 events overall and resulting alive at 3.8 years of follow-up.108 Alternatively, Pan et al proposed a single-access bilateral nephrectomy (r-SABN), where the patient is placed in a supine position with slight degree rotation to the target side, thus only requiring robot redocking but no patient repositioning. To note, only Xi robotic platform can guarantee this type of approach.109
Robotic Nephroureterectomy
Robot-assisted nephroureterectomy (RANU) for upper tract disease was reported for the first time in 2006.110 The primary challenge in performing a RANU procedure has been the necessity to address two distinct anatomical regions, requiring modifications to the technique to overcome this hurdle. In the past, patient repositioning and re-docking were often required with the Da Vinci Si system. Advancements have been made, such as the straight-line port placement described by Zargar et al,111 enabling a single-stage procedure without the need for repositioning or redocking. The introduction of the Da Vinci® Xi system has revolutionized RANU by minimizing arm clashing through a thinner and more accessible patient cart and longer instruments, facilitating the transition between the bladder and kidney regions.112
Veccia et al17 in 2022 described Xi single stage robotic nephroureterectomy in 148 patients through the ROBUUST multicenter collaborative group. Ports are placed on the same oblique straight line along with the lateral rectus abdominis, with the two assistant ports just above the umbilicus line; robot is docked only once, usually perpendicular to the table, in order to gain access to the pelvic quadrant to perform bladder cuff excision. Median operative time and estimated blood loss were 215.5 min and 100 mL, respectively. Postoperative complications were 26 (17.7%), with four major (2.7%), while bladder cuff excision and lymph node dissection were performed in 96% and 38.1% of the procedures, respectively.17
Sparwasser et al instead, published the first completely retroperitoneal RANU in five patients, with a mean operative time of 189.2 min and EBL of 150 (100–250). Only one patient reported a Clavien-2 complication and lymphadenectomy was performed in three/five patients. Ports placement starts from the Petit’s triangle and then follows a line above the iliac crest; to note, in this approach redocking for the distal ureter’s management is needed.113
SP Robotic Kidney Surgery
SP Robotic Partial Nephrectomy
Several groups proved SP robotic partial nephrectomy (SP RAPN) to be a safe and acceptable alternative to multiport robotic partial nephrectomy, providing comparable perioperative and postoperative outcomes while reducing inpatient opioid use.18,114 Moreover, SP RAPN can be performed effectively and safely regardless of the approach. In fact, transperitoneal and retroperitoneal approaches offer similar perioperative and postoperative outcomes for T1 RCC.115
A novel approach named SARA (Supine Anterior Retroperitoneal access) for either partial, radical nephrectomy, nephroureterectomy or pyeloplasty was recently described by Pellegrino et al116 in order to gain access to the retroperitoneum anteriorly: with the patient in a supine position, a 3-cm incision is made at the McBurney point, 3 cm medial and 3 cm caudal to the anterior superior iliac spine, and the abdominal muscles are dissected in order to develop the retroperitoneal space for the Da Vinci SP access port. Careful finger dissection can be conducted to gently separate the peritoneum’s anterior reflection from the transversus abdominis muscle; in doing so, adequate space for the placement of the robotic access port is provided. Advantages of this techniques are mainly represented by fast access to anterior mass and renal hilum, and easier dissection of the ureter during nephroureterectomy; concerning perioperative outcomes, high same-day discharge rate and no narcotic use were noted, suggesting ulterior benefits of this approach, along with less anesthesiologic issues due to the supine position.
SP Robotic Nephroureterectomy
Further innovation in Da Vinci platform leads to the pioneering single-Pprt robotic nephroureterectomy: to date only a few studies116,117 have reported this technique, where distal ureter dissection and bladder cuff resection were performed before completion of nephrectomy and all the procedure was performed without the change of patient position or re-docking of the robot system.
In 2021 Garden et al reported the first experience performing single-port robot-assisted donor nephrectomy (RADN) using the Da Vinci SP® surgical system. Access is gained through a 60 mm Pfannenstiel incision, in which the GelPOINT® advanced access platform is placed; a separate, paraumbilical 12 mm port is inserted for suction and/or stapler assistance. Overall, seven patients successfully underwent RADN, no major complications were reported, and mean hospitalization day was 2.1 days.118
Robot-assisted Inguinal Lymph Node Dissection for Penile Cancer
Radical inguinal lymph node dissection (ILND) remains the standard of care for palpable resectable nodes or clinical negative node with intermediate and high-risk penile cancer.119
Considering the significant complications associated with open inguinal lymph node dissection,120 minimally invasive techniques have been explored as alternatives.121 In small series, (robot-assisted) videoendoscopic inguinal lymphadenectomy (VEIL or RAVEIL) has shown feasibility, utilizing ports placed in the Scarpa triangle apex or in the hypogastrium. While the operative time is longer, VEIL or RAVEIL can yield similar lymph node counts as open ILND, with lower rates of lymphedema. In addition, patients who underwent VEIL or RAVEIL had shorter hospital stays, reduced drainage indwelling time, lower wound complication rates, although lymphocele and readmission rates were comparable.122,123 Minimally invasive ILND procedures also demonstrated a higher likelihood of sparing the saphenous vein compared to open ILND.124
Very initial series have documented feasibility of inguinal lymph node dissection with SP platform for penile cancer.125 Advantages of SP platform such as minimization of instrument clashing and workspace maximization certainly make this system perfectly fit for a narrow operating space such as the femoral triangle.
Robotic Reconstructive Urologic Surgery
Bladder Neck Reconstruction
Since the introduction of robotic surgery, rates of bladder neck contractures (BNC) postprostatectomy have declined but it remains a challenging complication for patients with various comorbidities.126 Patients often present with BNC six to twelve months after surgery with obstructive voiding issues.127 While most presentations can be partially managed with endoscopic incision, scar modulation, and open reconstruction, robotic bladder neck reconstruction (RBNR) has recently been revealed to be a promising avenue.128
In 2018, Kirshenbaum et al129 treated 12 patients with RBNR which allowed for a dissection above the level of the sphincter and prevention of pubectomy due to improved visualization and reach provided by robot assistance. While technique varied by surgeon, access and port placement was like that of RALP. The space of Retzius was developed and a urethral catheter was placed to determine location, and extent of the stenosis. The bladder neck was freed and mobilized from surgical adhesions and the catheter helped maintain patency until adequate healing occurred.
A Y-V plasty was described by Kropfl et al:130 briefly, a Y-incision is performed through all tissue layers of the bladder neck, creating a well-vascularized anterior bladder wall V-flap; interrupted sutures are then placed in a way that the apex of the V-flap is brought to the base of the Y-incision, thus creating a wide bladder neck. Results showed 75% achieved success determined by passage of a 17 Fr cystoscope into the bladder or a flow rate >15 mL/second. Only 18% of patients had incontinence after reconstruction which is a drastic improvement from the near inevitable incontinence seen with perineal dissection.130 Despite being preliminary and limited by small sample size, these series suggest that RBNR is a safe and effective treatment for BNC.
Ureteral Surgery
Complex proximal and mid-ureteral strictures are difficult to repair and have limited surgical options.131,132 Robotic assistance has definitively widened the options for ureteral strictures management.
Ureteroplasty with Buccal Mucosal Graft
Robotic ureteroplasty with buccal mucosa graft (RU-BMG) is a technique for ureteral reconstruction that avoids the morbidity of previous open techniques.133
RU-BMG was first reported in 2015, and since then the technique has been increasingly adopted at multiple centers.19 Currently, the largest study on intermediate-term outcomes of RU-BMG is a multi-institutional study conducted by Lee Z et al.134 In this study, RU-BMG was performed utilizing either an onlay graft after incising the stricture, or an augmented anastomotic repair in which the ureter was transected and anastomosed primarily on one side, and the graft on the other side. Outcomes from this multicenter study showed RBU is associated with low perioperative morbidity and excellent intermediate-term out. At a median follow-up of 27.5 months, 47 of 54 (87.0%) cases were surgically successful.134 Overall, available literature suggests RU-BMG is an effective treatment option for the management of complex mid and proximal ureteral strictures. In addition, indocyanine green can be utilized intraoperatively to offer real-time contrast to assist with ureteral identification and assessment of ureteral perfusion.135
The feasibility and safety of this kind of procedure performed with Da Vinci SP platform has been described by Lee et al;136 however, further studies with larger sample and longer follow-up are needed.
Ileal Ureteral Replacement
Long segment ureteral disease can rarely occur during endoscopic procedures, pelvic surgeries but also following malignant disease or retroperitoneal fibrosis.137
In 2021 Grosso et al20 reported three cases of totally intracorporeal robotic ileal ureter replacement (RA-IUR) for long ureteral defects. A flank position was used when using the Xi system, a supine position with the Si when approaching ileovesical anastomosis. Once isolated, a 20 cm ileal segment is first anastomosed proximally with the renal pelvis in an isoperistaltic fashion and, after redocking, ileovesical anastomosis is performed at the level of the bladder’s dome. All the procedures were successfully completed without complications, with a median operative time of 270 min.20
Yang et al138 enrolled 15 patients who underwent totally intracorporeal robotic ileal ureter replacement, eight of whom received bilateral replacement. The authors proposed two different docking approaches: a standard double-docking technique, where the robot is replaced to perform the distal ileovesical anastomosis; a single docking approach where robot is docked between the bladder and kidney directions, maintaining 2–3 cm distance between robotic trocars and the camera. Regarding bilateral RA-IUR, port placements and docking were the same as a standard RARC. Premeasured ileal segment was then prepared and anastomosed with the upper and distal ureter tract respectively. Remarkably, for bilateral RA-IUR, the upper anastomosis included an end-to-end anastomosis on one side and an end-to-side anastomosis on the other side. Results showed that this technique can be performed safely and efficiently with acceptable minor complications and a high success rate.138
Kidney Autotransplantation
Kidney autotransplantation (KAT) has been used as the ultimate resource to salvage kidneys with complex renovascular, ureteral, or malignant pathologies.139
Decaestecker et al reported the first series of robotic assisted kidney autotransplantation (RAKAT), describing both extracorporeal bench surgery and totally intracorporeal technique: after heparin administration, transection and a transfixing ligation of the vessels stump are performed; exteriorization of the kidney is gained with a GelPOINT access. During transplantation phase, the robot is redocked and RAKT is performed following the Vattikuti Urology Institute-Medanta technique. Results showed that RAKAT is feasible, safe, and provides good performance of the autotransplant in selected patients.21
To overcome limitations of RAKAT, such as patient’s repositioning or multiple docking, in 2023 Kaouk et al successfully performed eight cases of RAKAT using the SP system, with no perioperative complications nor need of conversion and operative time ranging from 366 to 701 min; postoperative renal function essentially remained stable in all the patients.140
Conclusions
Over the last eight years a tremendous number of intriguing and sophisticated robotic techniques and procedures have been successfully described both for oncologic and nononcologic indications. Some of these will play a major role in the urologic surgery armamentarium, and it can be expected to be implemented at larger scale. Overall, the adoption of robotic technology allowed us to aim at minimizing surgical morbidity while maximizing functional preservation. The flourishing of these techniques and procedures have also been fostered by the introduction of novel robotic systems, especially the SP platform. With maturing surgical experience and evolving technology, the use of these novel platforms is likely to facilitate future advances in the field of robotic urologic surgery.
Disclosure
Dr Simone Crivellaro is a consultant for Intuitive. The authors report no other conflicts of interest in this work.
References
1. Mottrie A, Larcher A, Patel V. The Past, the Present, and the Future of Robotic Urology: robot-assisted Surgery and Human-assisted Robots. Eur Urol Focus. 2018;4(5):629–631. doi:10.1016/j.euf.2018.10.002
2. Ilic D, Evans SM, Allan CA, Jung JH, Murphy D, Frydenberg M. Laparoscopic and robotic-assisted versus open radical prostatectomy for the treatment of localised prostate cancer. Cochrane Database Systematic Rev. 2017;2017(9). doi:10.1002/14651858.CD009625.pub2
3. Rassweiler J. Open vs.Laparoscopic Radical Prostatectomy. and Laparoscopy is Better! Eur Urol. 2006;50(1):26–28. doi:10.1016/j.eururo.2006.03.009
4. Singh I. Robotics in urological surgery: review of current status and maneuverability, and comparison of robot-assisted and traditional laparoscopy. Computer Aided Surgery. 2011;16(1):38–45. doi:10.3109/10929088.2010.541620
5. Lebeis C, Canes D, Sorcini A, Moinzadeh A. Novel technique prevents lymphoceles after transperitoneal robotic-assisted pelvic lymph node dissection: peritoneal flap interposition. Urology. 2015;85(6):1505–1509. doi:10.1016/j.urology.2015.02.034
6. Kaouk J, Valero R, Sawczyn G, Garisto J. Extraperitoneal single-port robot-assisted radical prostatectomy: initial experience and description of technique. BJU Int. 2020;125(1):182–189. doi:10.1111/bju.14885
7. Villers A, Puech P, Flamand V, et al. Partial Prostatectomy for Anterior Cancer: short-term Oncologic and Functional Outcomes. Eur Urol. 2017;72(3):333–342. doi:10.1016/j.eururo.2016.08.057
8. Wang P, Xia D, Ye S, et al. Robotic-assisted Urethra-sparing Simple Prostatectomy Via an Extraperitoneal Approach. Urology. 2018;119:85–90. doi:10.1016/j.urology.2018.06.005
9. Kaouk J, Sawczyn G, Wilson C, et al. Single-Port Percutaneous Transvesical Simple Prostatectomy Using the SP Robotic System: initial Clinical Experience. Urology. 2020;141:173–177. doi:10.1016/j.urology.2020.02.024
10. Asimakopoulos AD, Campagna A, Gakis G, et al. Nerve Sparing, Robot-Assisted Radical Cystectomy with Intracorporeal Bladder Substitution in the Male. J Urol. 2016;196(5):1549–1557. doi:10.1016/j.juro.2016.04.114
11. Tan WS, Sridhar A, Goldstraw M, et al. Robot-assisted intracorporeal pyramid neobladder. BJU Int. 2015;116(5):771–779. doi:10.1111/bju.13189
12. Simone G, Papalia R, Misuraca L, et al. Robotic Intracorporeal Padua Ileal Bladder: surgical Technique, Perioperative, Oncologic and Functional Outcomes. Eur Urol. 2018;73(6):934–940. doi:10.1016/j.eururo.2016.10.018
13. Minervini A, Di Maida F, Tasso G, et al. Robot assisted radical cystectomy with Florence robotic intracorporeal neobladder (FloRIN): analysis of survival and functional outcomes after first 100 consecutive patients upon accomplishment of Phase 3 IDEAL framework. Eur J Surgical Oncol. 2021;47(10):2651–2657. doi:10.1016/j.ejso.2021.05.007
14. Kaouk J, Garisto J, Eltemamy M, Bertolo R. Single-port Robotic Intracorporeal Ileal Conduit Urinary Diversion During Radical Cystectomy Using the SP Surgical System: step-by-step Technique. Urology. 2019;130. doi:10.1016/j.urology.2019.03.023
15. Wake N, Bjurlin MA, Rostami P, Chandarana H, Huang WC. Three-dimensional Printing and Augmented Reality: enhanced Precision for Robotic Assisted Partial Nephrectomy. Urology. 2018;116. doi:10.1016/j.urology.2017.12.038
16. Chopra S, Simone G, Metcalfe C, et al. Robot-assisted Level II–III Inferior Vena Cava Tumor Thrombectomy: step-by-Step Technique and 1-Year Outcomes. Eur Urol. 2017;72(2):267–274. doi:10.1016/j.eururo.2016.08.066
17. Veccia A, Carbonara U, Derweesh I, et al. Single-stage Xi® robotic radical nephroureterectomy for upper tract urothelial carcinoma: surgical technique and outcomes. Minerva Urol Nephrol. 2022;74(2). doi:10.23736/S2724-6051.21.04247-8
18. Kaouk J, Garisto J, Eltemamy M, Bertolo R. Pure Single-Site Robot-Assisted Partial Nephrectomy Using the SP Surgical System: initial Clinical Experience. Urology. 2019;124. doi:10.1016/j.urology.2018.11.024
19. Zhao LC, Yamaguchi Y, Bryk DJ, Adelstein SA, Stifelman MD. Robot-Assisted Ureteral Reconstruction Using Buccal Mucosa. Urology. 2015;86(3):634–638. doi:10.1016/j.urology.2015.06.006
20. Grosso AA, Di Maida F, Mari A, et al. Totally intracorporeal robotic ileal ureter replacement: focus on surgical technique and outcomes. Minerva Urol Nephrol. 2021;73(4). doi:10.23736/S2724-6051.20.04191-0
21. Decaestecker K, Van Parys B, Van Besien J, et al. Robot-assisted Kidney Autotransplantation: a Minimally Invasive Way to Salvage Kidneys. Eur Urol Focus. 2018;4(2). doi:10.1016/j.euf.2018.07.019
22. Abbou CC, Hoznek A, Salomon L, et al. Laparoscopic radical prostatectomy with a remote controlled robot. J Urol. 2001;165(6 I):1964–1966. doi:10.1097/00005392-200106000-00027
23. B CD, S CP, K N, et al. A Parallel Randomized Clinical Trial Examining the Return of Urinary Continence after Robot-Assisted Radical Prostatectomy with or without a Small Intestinal Submucosa Bladder Neck Sling. J Urol. 2016;196(1):565.
24. Canvasser NE, Lay AH, Koseoglu E, Morgan MSC, Cadeddu JA. Posterior Urethral Suspension during Robot-Assisted Radical Prostatectomy Improves Early Urinary Control: a Prospective Cohort Study. J Endourol. 2016;30(10):1089–1094. doi:10.1089/end.2016.0220
25. Nguyen HG, Punnen S, Cowan JE, et al. A Randomized Study of Intraoperative Autologous Retropubic Urethral Sling on Urinary Control after Robotic Assisted Radical Prostatectomy. J Urol. 2017;197(2):369–375. doi:10.1016/j.juro.2016.08.122
26. Wagaskar VG, Mittal A, Sobotka S, et al. Hood Technique for Robotic Radical Prostatectomy—Preserving Periurethral Anatomical Structures in the Space of Retzius and Sparing the Pouch of Douglas, Enabling Early Return of Continence Without Compromising Surgical Margin Rates. Eur Urol. 2021;80(2):213–221. doi:10.1016/j.eururo.2020.09.044
27. Shimmura H, Banno T, Nakamura K, et al. A single‐center retrospective comparative analysis of urinary continence in robotic prostatectomy with a combination of umbilical ligament preservation and Hood technique. Int J Urol. 2023. doi:10.1111/iju.15227
28. Beyer B, Schlomm T, Tennstedt P, et al. A feasible and time-efficient adaptation of NeuroSAFE for da Vinci robot-assisted radical prostatectomy. Eur Urol. 2014;66(1):138–144. doi:10.1016/j.eururo.2013.12.014
29. Mirmilstein G, Rai BP, Gbolahan O, et al. The neurovascular structure-adjacent frozen-section examination (Neuro SAFE) approach to nerve sparing in robot-assisted laparoscopic radical prostatectomy in a British setting – a prospective observational comparative study. BJU Int. 2018;121(6):854–862. doi:10.1111/bju.14078
30. van der Slot MA, den Bakker MA, Tan TSC, et al. NeuroSAFE in radical prostatectomy increases the rate of nerve-sparing surgery without affecting oncological outcome. BJU Int. 2022;130(5):628–636. doi:10.1111/bju.15771
31. Noël J, Spencer NH, Lodia S, et al. Neurovascular structure-adjacent frozen-section examination robotic-assisted radical prostatectomy: outcomes from 500 consecutive cases in the UK. J Robot Surg. 2022;16(4). doi:10.1007/s11701-021-01324-2
32. de Carvalho PA, Barbosa JABA, Guglielmetti GB, et al. Retrograde Release of the Neurovascular Bundle with Preservation of Dorsal Venous Complex During Robot-assisted Radical Prostatectomy: optimizing Functional Outcomes. Eur Urol. 2020;77(5):628–635. doi:10.1016/j.eururo.2018.07.003
33. Ploussard G, Briganti A, De La Taille A, et al. Pelvic lymph node dissection during robot-assisted radical prostatectomy: efficacy, limitations, and complications - A systematic review of the literature. Eur Urol. 2014;65(1):7–16. doi:10.1016/j.eururo.2013.03.057
34. Student V, Tudos Z, Studentova Z, et al. Effect of Peritoneal Fixation (PerFix) on Lymphocele Formation in Robot-assisted Radical Prostatectomy with Pelvic Lymphadenectomy: results of a Randomized Prospective Trial. Eur Urol. 2023;83(2):154–162. doi:10.1016/j.eururo.2022.07.027
35. Wagner J, McLaughlin T, Pinto K, Tortora J, Gangakhedkar A, Staff I. The Effect of a Peritoneal Iliac Flap on Lymphocele Formation After Robotic Radical Prostatectomy: results From the PLUS Trial. Urology. 2023;178:173. doi:10.1016/j.urology.2022.12.002
36. Harland N, Alfarra M, Erne E, et al. A Peritoneal Purse-String Suture Prevents Symptomatic Lymphoceles in Retzius-Sparing Robot-Assisted Radical Prostatectomy. J Clin Med. 2023;12(3):791. doi:10.3390/jcm12030791
37. Gloger S, Ubrig B, Boy A, et al. Bilateral Peritoneal Flaps Reduce Incidence and Complications of Lymphoceles after Robotic Radical Prostatectomy with Pelvic Lymph Node Dissection - Results of the Prospective Randomized Multicenter Trial ProLy. J Urol. 2022;208(2):333–340. doi:10.1097/JU.0000000000002693
38. Yılmaz K, Ölçücü MT, Arı Ö, et al. The Results of Peritoneal Re-Approximation Methods on Symptomatic Lymphocele Formation in Robot-Assisted Laparoscopic Radical Prostatectomy and Extended Pelvic Lymphadenectomy. Arch Esp Urol. 2022;75(5):447. doi:10.56434/j.arch.esp.urol.20227505.65
39. Boğa MS, Sönmez MG, Karamik K, Yilmaz K, Savaş M, Ateş M. The effect of peritoneal re-approximation on lymphocele formation in transperitoneal robot-assisted radical prostatectomy and extended pelvic lymphadenectomy. Turk J Urol. 2020;46(6). doi:10.5152/tud.2020.20255
40. Bründl J, Lenart S, Stojanoski G, et al. Peritoneal Flap in Robot-Assisted Radical Prostatectomy. Dtsch Arztebl Int. 2020;117(14):243–250. doi:10.3238/arztebl.2020.0243
41. Lee M, Lee Z, Eun DD. Utilization of a Peritoneal Interposition Flap to Prevent Symptomatic Lymphoceles after Robotic Radical Prostatectomy and Bilateral Pelvic Lymph Node Dissection. J Endourol. 2020;34(8):821–827. doi:10.1089/end.2020.0073
42. Dal Moro F, Zattoni F. P.L.E.A.T.—Preventing Lymphocele Ensuring Absorption Transperitoneally: a Robotic Technique. Urology. 2017;110. doi:10.1016/j.urology.2017.05.031
43. Neuberger M, Kowalewski KF, Simon V, et al. Peritoneal Flap for Lymphocele Prophylaxis Following Robotic-assisted Radical Prostatectomy with Lymph Node Dissection: the Randomised Controlled Phase 3 PELYCAN Trial. Eur Urol Oncol. 2023. doi:10.1016/j.euo.2023.07.009
44. Garbens A, Morgan T, Cadeddu JA. Single Port Robotic Surgery in Urology. Curr Urol Rep. 2021;22(4). doi:10.1007/s11934-021-01040-2
45. Kaouk JH, Haber GP, Autorino R, et al. A Novel Robotic System for Single-port Urologic Surgery: first Clinical Investigation. Eur Urol. 2014;66(6):1033–1043. doi:10.1016/J.EURURO.2014.06.039
46. Crivellaro S. In Favor of Extraperitoneal Robotic Radical Prostatectomy: back to the Future through a Single-Port Approach. J Endourol. 2021;35(8):1121–1122. doi:10.1089/end.2021.0294
47. Kaouk J, Aminsharifi A, Wilson CA, et al. Extraperitoneal versus Transperitoneal Single Port Robotic Radical Prostatectomy: a Comparative Analysis of Perioperative Outcomes. J Urol. 2020;203(6):1135–1140. doi:10.1097/JU.0000000000000700
48. Desai MM, Aron M, Berger A, et al. Transvesical robotic radical prostatectomy. BJU Int. 2008;102(11):1666–1669. doi:10.1111/j.1464-410X.2008.08004.x
49. Zhou X, Fu B, Zhang C, et al. Transvesical robot-assisted radical prostatectomy: initial experience and surgical outcomes. BJU Int. 2020;126(2):300–308. doi:10.1111/bju.15111
50. Martini A, Falagario UG, Villers A, et al. Contemporary Techniques of Prostate Dissection for Robot-assisted Prostatectomy. Eur Urol. 2020;78(4):583–591. doi:10.1016/j.eururo.2020.07.017
51. Deng W, Jiang H, Liu X, et al. Transvesical Retzius-Sparing Versus Standard Robot-Assisted Radical Prostatectomy: a Retrospective Propensity Score-Adjusted Analysis. Front Oncol. 2021:11. doi:10.3389/fonc.2021.687010
52. Deng W, Zhang C, Jiang H, et al. Transvesical Versus Posterior Approach to Retzius-Sparing Robot-Assisted Radical Prostatectomy: a Retrospective Comparison With a 12-Month Follow-Up. Front Oncol. 2021:11. doi:10.3389/fonc.2021.641887
53. Ramos-Carpinteyro R, Ferguson EL, Chavali JS, Geskin A, Soputro N, Kaouk J. Single-port Transvesical Robot-assisted Radical Prostatectomy: the Surgical Learning Curve of the First 100 Cases. Urology. 2023;178:76–82. doi:10.1016/j.urology.2023.05.027
54. Galfano A, Ascione A, Grimaldi S, Petralia G, Strada E, Bocciardi AM. A new anatomic approach for robot-assisted laparoscopic prostatectomy: a feasibility study for completely intrafascial surgery. Eur Urol. 2010;58(3):457–461. doi:10.1016/j.eururo.2010.06.008
55. Dell’Oglio P, Tappero S, Longoni M, et al. Retzius-sparing Robot-assisted Radical Prostatectomy in High-risk Prostate Cancer Patients: results from a Large Single-institution Series. Eur Urol Open Sci. 2022:38. doi:10.1016/j.euros.2022.02.007
56. Bassett JC, Salibian S, Crivellaro S. Single-Port Retzius-Sparing Robot-Assisted Radical Prostatectomy: feasibility and Early Outcomes. J Endourol. 2021;36(5):620–625. doi:10.1089/end.2021.0542
57. Koukourikis P, Alqahtani AA, Han WK, Rha KH. Pure single‐port retzius‐sparing robot‐assisted radical prostatectomy with the da Vinci SP: initial experience and technique description. BJUI Compass. 2022;3(3):251–256. doi:10.1002/bco2.131
58. Balasubramanian S, Shiang A, Vetter JM, Henning GM, Figenshau RS, Kim EH. Comparison of Three Approaches to Single-Port Robot-Assisted Radical Prostatectomy: our Institution’s Initial Experience. J Endourol. 2022;36(12):1551–1558. doi:10.1089/end.2022.0330
59. Laydner H, Akça O, Autorino R, et al. Third prize: perineal robot-assisted laparoscopic radical prostatectomy: feasibility study in the cadaver model. J Endourol. 2014. doi:10.1089/end.2014.0244
60. Janoff DM, Parra RO. Contemporary appraisal of radical perineal prostatectomy. J Urol. 2005;173(6):1863–1870. doi:10.1097/01.ju.0000161483.65619.b3
61. Garisto J, Bertolo R, Wilson CA, Kaouk J. The evolution and resurgence of perineal prostatectomy in the robotic surgical era. World J Urol. 2020;38(4):821–828. doi:10.1007/s00345-019-03004-1
62. Kaouk JH, Akca O, Zargar H, et al. Descriptive Technique and Initial Results for Robotic Radical Perineal Prostatectomy. Urology. 2016;94:129–138. doi:10.1016/j.urology.2016.02.063
63. Tuğcu V, Akça O, Şimşek A, et al. Robotic perineal radical prostatectomy and robotic pelvic lymph node dissection via a perineal approach: the Tugcu Bakirkoy Technique. Turk J Urol. 2018;44(2). doi:10.5152/tud.2018.24603
64. Carbonara U, Minafra P, Papapicco G, et al. Xi Nerve-sparing Robotic Radical Perineal Prostatectomy: European Single-center Technique and Outcomes. Eur Urol Open Sci. 2022:41. doi:10.1016/j.euros.2022.04.014
65. Lenfant L, Garisto J, Sawczyn G, et al. Robot-assisted Radical Prostatectomy Using Single-port Perineal Approach: technique and Single-surgeon Matched-paired Comparative Outcomes. Eur Urol. 2021;79(3):384–392. doi:10.1016/j.eururo.2020.12.013
66. Sullivan LD, Weir MJ, Kinahan JF, Taylor DL. A comparison of the relative merits of radical perineal and radical retropubic prostatectomy. BJU Int. 2000;85(1):95–100. doi:10.1046/j.1464-410X.2000.00405.x
67. Ahmed HU, Hindley RG, Dickinson L, et al. Focal therapy for localised unifocal and multifocal prostate cancer: a prospective development study. Lancet Oncol. 2012;13(6):622–632. doi:10.1016/S1470-2045(12)70121-3
68. Bass R, Fleshner N, Finelli A, Barkin J, Zhang L, Klotz L. Oncologic and functional outcomes of partial gland ablation with high intensity focused ultrasound for localized prostate cancer. J Urol. 2019;201(1):113–119. doi:10.1016/j.juro.2018.07.040
69. Golan R, Bernstein AN, McClure TD, et al. Partial Gland Treatment of Prostate Cancer Using High-Intensity Focused Ultrasound in the Primary and Salvage Settings: a Systematic Review. J Urol. 2017;198(5):1000–1009. doi:10.1016/j.juro.2017.03.137
70. Sood A, Jeong W, Palma-Zamora I, et al. Description of Surgical Technique and Oncologic and Functional Outcomes of the Precision Prostatectomy Procedure (IDEAL Stage 1–2b Study). Eur Urol. 2022;81(4):396–406. doi:10.1016/j.eururo.2021.10.017
71. Villers A, Seguier D, Puech P, et al. Robot Partial Prostatectomy for Anterior Cancer: long-term Functional and Oncological Outcomes at 7 Years. Eur Urol Open Sci. 2023:55. doi:10.1016/j.euros.2023.07.001
72. Kaouk JH. Single-port Robotic Transvesical Partial Prostatectomy for Localized Prostate Cancer: initial Series and Description of Technique. Eur Urol. 2022;82(5):551.
73. Salkowski M, Checcucci E, Chow AK, et al. New multiport robotic surgical systems: a comprehensive literature review of clinical outcomes in urology. Ther Adv Urol. 2023;15:175628722311777. doi:10.1177/17562872231177781
74. Fan S, Zhang Z, Wang J, et al. Robot-Assisted Radical Prostatectomy Using the KangDuo Surgical Robot-01 System: a Prospective, Single-Center, Single-Arm Clinical Study. J Urol. 2022;208(1):119–127. doi:10.1097/JU.0000000000002498
75. Kastelan Z, Hudolin T, Kulis T, et al. Extraperitoneal Radical Prostatectomy with the Senhance Robotic Platform: first 40 Cases. Eur Urol. 2020;78(6):932–934. doi:10.1016/j.eururo.2020.07.012
76. Venckus R, Jasenas M, Telksnys T, et al. Robotic-assisted radical prostatectomy with the Senhance® robotic platform: single center experience. World J Urol. 2021;39(12):4305–4310. doi:10.1007/s00345-021-03792-5
77. Rocco B, Turri F, Sangalli M, et al. Robot-assisted Radical Prostatectomy with the Versius Robotic Surgical System: first Description of a Clinical Case. Eur Urol Open Sci. 2023;47:48. doi:10.1016/j.euros.2022.11.019
78. Reeves F, Challacombe B, Ribbits A, Ourselin S, Dasgupta P. Idea, Development, Exploration, Assessment, Long-term follow-up study (IDEAL) Stage 1/2a evaluation of urological procedures with the Versius robot. BJU Int. 2022;130(4):441–443. doi:10.1111/bju.15829
79. Bravi CA, Paciotti M, Sarchi L, et al. Robot-assisted Radical Prostatectomy with the Novel Hugo Robotic System: initial Experience and Optimal Surgical Set-up at a Tertiary Referral Robotic Center. Eur Urol. 2022;82(2):233–237. doi:10.1016/j.eururo.2022.04.029
80. Totaro A, Campetella M, Bientinesi R, et al. The new surgical robotic platform HUGO TM RAS: system description and docking settings for robot-assisted radical prostatectomy. Urologia J. 2022;89(4):603–609. doi:10.1177/03915603221107855
81. Ragavan N, Bharathkumar S, Chirravur P, Sankaran S. Robot-Assisted Laparoscopic Radical Prostatectomy Utilizing Hugo RAS Platform: initial Experience. J Endourol. 2023;37(2):147–150. doi:10.1089/end.2022.0461
82. Autorino R, Zargar H, Mariano MB, et al. Perioperative outcomes of robotic and laparoscopic simple prostatectomy: a European-American multi-institutional analysis. Eur Urol. 2015;68(1):86–94. doi:10.1016/j.eururo.2014.11.044
83. Oelke M, Bachmann A, Descazeaud A, et al. EAU guidelines on the treatment and follow-up of non-neurogenic male lower urinary tract symptoms including benign prostatic obstruction. Eur Urol. 2013;64(1):118–140. doi:10.1016/j.eururo.2013.03.004
84. McVary KT, Roehrborn CG, Avins AL, et al. Update on AUA Guideline on the Management of Benign Prostatic Hyperplasia. J Urol. 2011;185(5):1793–1803. doi:10.1016/j.juro.2011.01.074
85. Sotelo R, Clavijo R, Carmona O, et al. Robotic Simple Prostatectomy. J Urol. 2008;179(2):513–515. doi:10.1016/j.juro.2007.09.065
86. Yuh B, Laungani R, Perlmutter A, et al. Robot-assisted Millin’s retropubic prostatectomy: case series. Can J Urol. 2008;15(3):4101–4105.
87. Simone G, Misuraca L, Anceschi U, et al. Urethra and Ejaculation Preserving Robot-assisted Simple Prostatectomy: near-infrared Fluorescence Imaging-guided Madigan Technique. Eur Urol. 2019;75(3):492–497. doi:10.1016/j.eururo.2018.11.051
88. Porpiglia F, Checcucci E, Amparore D, et al. Urethral-sparing Robot-assisted Simple Prostatectomy: an Innovative Technique to Preserve Ejaculatory Function Overcoming the Limitation of the Standard Millin Approach. Eur Urol. 2021;80(2):222–233. doi:10.1016/j.eururo.2020.09.028
89. Fareed K, Zaytoun OM, Autorino R, et al. Robotic single port suprapubic transvesical enucleation of the prostate (R-STEP): initial experience. BJU Int. 2012;110(5):732–737. doi:10.1111/j.1464-410X.2012.10954.x
90. Abou Zeinab M, Kaviani A, Ferguson E, et al. Single-port transvesical versus open simple prostatectomy: a perioperative comparative study. Prostate Cancer Prostatic Dis. 2022;26(3):538–542. doi:10.1038/s41391-022-00566-x
91. Khalil MI, Chase A, Joseph JV, Ghazi A. Standard Multiport vs Single-Port Robot-Assisted Simple Prostatectomy: a Single-Center Initial Experience. J Endourol. 2022;36(8):1057–1062. doi:10.1089/end.2021.0510
92. Abou Zeinab M, Ramos R, Ferguson EL, et al. Single Port Versus Multiport Robot-assisted Simple Prostatectomy: a Multi-institutional Study From the Single-port Advanced Research Consortium (SPARC). Urology. 2023;176:94–101. doi:10.1016/j.urology.2023.03.022
93. Pacchetti A, Pignot G, Le Quellec A, et al. Sexual-Sparing Robot Assisted Radical Cystectomy in Female: a Step-By-Step Guide. Urology. 2021:156. doi:10.1016/j.urology.2021.06.002
94. Chopra S, de Castro Abreu AL, Berger AK, et al. Evolution of robot-assisted orthotopic ileal neobladder formation: a step-by-step update to the University of Southern California (USC) technique. BJU Int. 2017;119(1):185–191. doi:10.1111/bju.13611
95. Checcucci E, Manfredi M, Sica M, et al. Robot-assisted-radical-cystectomy with total intracorporeal Y neobladder: analysis of postoperative complications and functional outcomes with urodynamics findings. Eur J Surgical Oncol. 2022;48(3):694–702. doi:10.1016/j.ejso.2021.12.014
96. Asimakopoulos AD, Gubbiotti M, Agrò EF, et al. “Bordeaux Neobladder”: first Evaluation of the Urodynamic Outcomes. Eur Urol Open Sci. 2023;47:102–109. doi:10.1016/j.euros.2022.11.010
97. Chen G, Crivellaro S. Single-port robotic radical cystectomy with ileal conduit urinary diversion: technique and review of the early outcomes in literature. Mini-Invasive Surgery. 2021;5. doi:10.20517/2574-1225.2021.69
98. Zhang M, Thomas D, Salama G, Ahmed M. Single port robotic radical cystectomy with intracorporeal urinary diversion: a case series and review. Transl Androl Urol. 2020;9(2):925–930. doi:10.21037/tau.2020.01.19
99. Amparore D, Checcucci E, Piazzolla P, et al. Indocyanine Green Drives Computer Vision Based 3D Augmented Reality Robot Assisted Partial Nephrectomy: the Beginning of “Automatic” Overlapping Era. Urology. 2022:164. doi:10.1016/j.urology.2021.10.053
100. Amparore D, Piramide F, Checcucci E, et al. Three-dimensional Virtual Models of the Kidney with Colored Perfusion Regions: a New Algorithm-based Tool for Optimizing the Clamping Strategy During Robot-assisted Partial Nephrectomy. Eur Urol. 2023;84(4):418–425. doi:10.1016/j.eururo.2023.04.005
101. Michiels C, Khene ZE, Prudhomme T, et al. 3D-Image guided robotic-assisted partial nephrectomy: a multi-institutional propensity score-matched analysis (UroCCR study 51). World J Urol. 2023;41(2). doi:10.1007/s00345-021-03645-1
102. Margulis V, Master VA, Cost NG, et al. International consultation on urologic diseases and the European Association of Urology international consultation on locally advanced renal cell carcinoma. Eur Urol. 2011;60(4):673–683. doi:10.1016/j.eururo.2011.06.042
103. Abaza R. Technical considerations in robotic nephrectomy with vena caval tumor thrombectomy. Indian J Urol. 2014;30(3):283. doi:10.4103/0970-1591.134252
104. Nelson RJ, Maurice MJ, Kaouk JH. Robotic Radical Left Nephrectomy With Inferior Vena Cava Level III Thrombectomy. Urology. 2017;107. doi:10.1016/j.urology.2017.04.043
105. Gill IS, Metcalfe C, Abreu A, et al. Robotic level III inferior vena cava tumor thrombectomy: initial series. J Urol. 2015;194(4):929–938. doi:10.1016/j.juro.2015.03.119
106. Zhang JH, Zeinab MA, Ferguson EL, et al. Minimally-Invasive Radical Nephrectomy and Left-Sided Level II Caval Thrombectomy: a New Combined Technique. Urology. 2023:172. doi:10.1016/j.urology.2022.10.028
107. Darby CR, Cranston D, Raine AEG, Morris PJ. Bilateral nephrectomy before transplantation: indications, surgical approach, morbidity and mortality. Br J Surgery. 1991;78(3):305–307. doi:10.1002/bjs.1800780313
108. Gurung PMS, Frye TP, Rashid HH, Joseph JV, Wu G. Robot-assisted Synchronous Bilateral Nephrectomy for Autosomal Dominant Polycystic Kidney Disease: a Stepwise Description of Technique. Urology. 2021;153. doi:10.1016/j.urology.2020.05.069
109. Pan G, Campsen J, Kim RD, Rofaiel G. Efficacy and utility of robotic single-access bilateral nephrectomy (r-SABN) in end-stage renal disease patients. J Robot Surg. 2021;15(4):511–518. doi:10.1007/s11701-020-01137-9
110. Nanigian DK, Smith W, Ellison LM. Robot-assisted laparoscopic nephroureterectomy. J Endourol. 2006;20(7):463–466. doi:10.1089/end.2006.20.463
111. Zargar H, Krishnan J, Autorino R, et al. Robotic nephroureterectomy: a simplified approach requiring no patient repositioning or robot redocking. Eur Urol. 2014;66(4):769–777. doi:10.1016/j.eururo.2014.02.060
112. Argun OB, Mourmouris P, Tufek I, et al. Radical Nephroureterectomy Without Patient or Port Repositioning Using the da Vinci Xi Robotic System: initial Experience. Urology. 2016:92. doi:10.1016/j.urology.2016.02.047
113. Sparwasser P, Epple S, Thomas A, et al. First completely robot-assisted retroperitoneal nephroureterectomy with bladder cuff: a step-by-step technique. World J Urol. 2022;40(4):1019–1026. doi:10.1007/s00345-021-03920-1
114. Francavilla S, Abern MR, Dobbs RW, et al. Single-port robot assisted partial nephrectomy: initial experience and technique with the da Vinci Single-port platform (ideal Phase 1). Minerva Urol Nephrol. 2022;74(22). doi:10.23736/S2724-6051.21.03919-9
115. Bang S, Shin D, Hyung Woo M, et al. Comparison of transperitoneal and retroperitoneal partial nephrectomy with single port robot. J Endourol. 2023;37(5):551–556. doi:10.1089/end.2022.0730
116. Pellegrino AA, Chen G, Morgantini L, Calvo RS, Crivellaro S. Simplifying Retroperitoneal Robotic Single-port Surgery: novel Supine Anterior Retroperitoneal Access. Eur Urol. 2023;84(2):223–228. doi:10.1016/j.eururo.2023.05.006
117. Kim KH, Ahn HK, Kim M, Yoon H. Technique and perioperative outcomes of single-port robotic surgery using the da Vinci SP platform in urology. Asian J Surg. 2023;46(1):472–477. doi:10.1016/j.asjsur.2022.05.128
118. Garden EB, Al-Alao O, Razdan S, Mullen GR, Florman S, Palese MA. Robotic single-port donor nephrectomy with the da Vinci SP® surgical system. J Society Laparoendoscopic Surgeons. 2021;25(4). doi:10.4293/JSLS.2021.00062
119. Hakenberg OW, Compérat EM, Minhas S, Necchi A, Protzel C, Watkin N. EAU guidelines on penile cancer: 2014 update. Eur Urol. 2015;67(1):142–150. doi:10.1016/j.eururo.2014.10.017
120. Bevan-Thomas R, Slaton JW, Pettaway CA. Contemporary morbidity from lymphadenectomy for penile squamous cell carcinoma: the M.D. Anderson cancer center experience. J Urol. 2002;167(4):1638–1642. doi:10.1016/s0022-5347(05)65169-5
121. Russell CM, Salami SS, Niemann A, et al. Minimally Invasive Inguinal Lymphadenectomy in the Management of Penile Carcinoma. Urology. 2017;106:113–118. doi:10.1016/j.urology.2017.04.022
122. Singh A, Jaipuria J, Goel A, et al. Comparing Outcomes of Robotic and Open Inguinal Lymph Node Dissection in Patients with Carcinoma of the Penis. J Urol. 2018;199(6):1518–1525. doi:10.1016/j.juro.2017.12.061
123. Kumar V, Sethia KK. Prospective study comparing video-endoscopic radical inguinal lymph node dissection (VEILND) with open radical ILND (OILND) for penile cancer over an 8-year period. BJU Int. 2017;119(4):530–534. doi:10.1111/bju.13660
124. Fankhauser CD, Lee EWC, Issa A, et al. Saphenous-sparing Ascending Video Endoscopic Inguinal Lymph Node Dissection Using a Leg Approach: surgical Technique and Perioperative and Pathological Outcomes. Eur Urol Open Sci. 2022;35:9–13. doi:10.1016/j.euros.2021.10.004
125. Abdullatif VA, Davis J, Cavayero C, Toenniessen A, Nelson RJ. Single-Port Robotic Inguinal Lymph Node Dissection for Penile Cancer. Urology. 2022;161. doi:10.1016/j.urology.2021.12.007
126. Modig KK, Godtman RA, Bjartell A, et al. Vesicourethral Anastomotic Stenosis After Open or Robot-assisted Laparoscopic Retropubic Prostatectomy—Results from the Laparoscopic Prostatectomy Robot Open Trial. Eur Urol Focus. 2021;7(2):317–324. doi:10.1016/j.euf.2019.10.012
127. Parihar JS, Ha YS, Kim IY. Bladder neck contracture-incidence and management following contemporary robot assisted radical prostatectomy technique. Prostate Int. 2014;2(1):12–18. doi:10.12954/pi.13034
128. Branche B, Crocerossa F, Carbonara U, et al. Management of Bladder Neck Contracture in the Age of Robotic Prostatectomy: an Evidence-based Guide. Eur Urol Focus. 2022;8(1):297–301. doi:10.1016/j.euf.2021.01.007
129. Kirshenbaum EJ, Zhao LC, Myers JB, et al. Patency and Incontinence Rates After Robotic Bladder Neck Reconstruction for Vesicourethral Anastomotic Stenosis and Recalcitrant Bladder Neck Contractures: the Trauma and Urologic Reconstructive Network of Surgeons Experience. Urology. 2018:118. doi:10.1016/j.urology.2018.05.007
130. Kröpfl D, Musch M, Hohenhorst JL, Pailliart A, Loewen H, Krege S. Robot-assisted laparoscopic YV-plasty in 12 patients with refractory bladder neck contracture. Eur Urol Supplements. 2016;15(7):360. doi:10.1016/s1569-9056(16)15313-8
131. Boxer RJ, Fritzsche P, Skinner DG, et al. Replacement of the ureter by small intestine: clinical application and results of the ileal ureter in 89 patients. J Urol. 1979;121(6):728–731. doi:10.1016/S0022-5347(17)56972-4
132. Chung BI, Hamawy KJ, Zinman LN, Libertino JA. The use of bowel for ureteral replacement for complex ureteral reconstruction: long-term results. J Urol. 2006;175(1):179–83; discussion 183–4. doi:10.1016/S0022-5347(05)00061-3
133. Lee Z, Waldorf BT, Cho EY, Liu JC, Metro MJ, Eun DD. Robotic ureteroplasty with buccal mucosa graft for the management of complex ureteral strictures. J Urol. 2017;198(6):1430–1435. doi:10.1016/j.juro.2017.06.097
134. Lee Z, Lee M, Koster H, et al. A Multi-Institutional Experience With Robotic Ureteroplasty With Buccal Mucosa Graft: an Updated Analysis of Intermediate-Term Outcomes. Urology. 2021:147. doi:10.1016/j.urology.2020.08.003
135. Lee Z, Moore B, Giusto L, Eun DD. Use of indocyanine green during robot-Assisted ureteral reconstructions. Eur Urol. 2015;67(2):291–298. doi:10.1016/j.eururo.2014.08.057
136. Liu W, Shakir N, Zhao LC. Single-Port Robotic Posterior Urethroplasty Using Buccal Mucosa Grafts: technique and Outcomes. Urology. 2022;159. doi:10.1016/j.urology.2021.07.049
137. Cindolo L, Castellan P, Primiceri G, et al. Life-Threatening complications after ureteroscopy for urinary stones: survey and systematic literature review. Minerva Urologica e Nefrologica. 2017;69(5). doi:10.23736/S0393-2249.17.02787-4
138. Yang K, Wang X, Xu C, et al. Totally Intracorporeal Robot-assisted Unilateral or Bilateral Ileal Ureter Replacement for the Treatment of Ureteral Strictures: technique and Outcomes from a Single Center. Eur Urol. 2023. doi:10.1016/j.eururo.2023.04.022
139. Azhar B, Patel S, Chadha P, Hakim N. Indications for renal autotransplant: an overview. Exp Clin Transplantation. 2015;13(2). doi:10.6002/ect.2014.0238
140. Kaouk J, Chavali JS, Ferguson E, et al. Single Port Robotic Kidney Autotransplantation: initial Case Series and Description of Technique. Urology. 2023;176:87–93. doi:10.1016/j.urology.2023.02.030
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.