Back to Journals » HIV/AIDS - Research and Palliative Care » Volume 12
Risky Sexual Practice, Sexually Transmitted Infection and Associated Factors Among Newly Diagnosed HIV-positive People in Northwest Ethiopia
Authors Moges NA ![]() , Adesina OA
, Adesina OA ![]() , Okunlola MA, Berhane Y
, Okunlola MA, Berhane Y ![]() , Akinyemi JO
, Akinyemi JO ![]()
Received 11 June 2020
Accepted for publication 13 August 2020
Published 18 September 2020 Volume 2020:12 Pages 431—439
DOI https://doi.org/10.2147/HIV.S267215
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Bassel Sawaya
Nurilign Abebe Moges,1,2 Olubukola Adeponle Adesina,3,4 Michael A Okunlola,3,4 Yemane Berhane,5 Joshua Odunayo Akinyemi6
1Department of Public Health, College of Health Sciences, Debre Markos University, Debre Markos, Ethiopia; 2Pan African University Life and Earth Sciences Institute, University of Ibadan, Ibadan, Nigeria; 3Department of Obstetrics and Gynecology, College of Medicine, University of Ibadan, Ibadan, Nigeria; 4Department of Obstetrics and Gynecology, University College Hospital, Ibadan, Nigeria; 5Department of Epidemiology, Addis Continental Institute of Public Health, Addis Ababa, Ethiopia; 6Department of Epidemiology and Medical Statistics, Faculty of Public Health, College of Medicine, University of Ibadan, Ibadan, Nigeria
Correspondence: Nurilign Abebe Moges Tel +251910106295
Email [email protected]
Purpose: Risky sexual practice expose for the acquisition of sexually transmitted infection (STI) including human immunodeficiency virus (HIV). This study was conducted to fill the knowledge gap on the prevalence of risky sexual practice, STIs and associated factors among newly diagnosed HIV-positive people in northwest Ethiopia.
Patients and Methods: This study was a cross-sectional study design which was conducted on 745 newly diagnosed HIV patients. An interviewer-administered questionnaire was used to interview patients within seven days of HIV diagnosis using client exit interview approach. Data were entered to EpiData and exported to SPSS version 24 for analysis. Binary logistic regression analysis was employed to select factors for multivariate logistic regression at p-value of less than 0.25. Two separate logistic regression models were used for risky sexual practice and STI as dependent variables. The strength of statistical association was quantified using an adjusted odds ratio (AOR) with a 95% confidence level.
Results: The prevalence of risky sexual practices and STIs among newly diagnosed HIV-positive people were 15.8% (95%CI: 13.1– 18.4) and 6.6% (95%CI: 4.8– 8.5), respectively. Although there were no statistically significant factors associated with STI, having two or more lifetime sexual partners (AOR=3.19; 95%CI: 1.57– 6.49) and frequent use of alcohol (AOR=3.10; 95%CI: 1.34– 7.19) were the factors associated with risky sexual practice.
Conclusion: Risky sexual practice and STI were found to be low among newly identified HIV patients. Factors associated with risky sexual practice failed to explain STI diagnosis using the syndromic approach. Therefore, revisiting the definition of risky sexual practice is necessary for the universal test and treat approach since sustained viral suppression may leave the need for consistent use of condoms among HIV patients who are on ART especially with regular sexual partners. Further study is also recommended to measure changes in sexual practice after initiating antiretroviral therapy.
Keywords: risky sexual behavior, newly diagnosed HIV patients, STI, Ethiopia
Introduction
Personality and physiology play significant role in determining a person’s sexual practice.1 Risky sexual practice and sexually transmitted infections (STIs) including human immunodeficiency virus (HIV) are often related to each other.2 The two are associated because an acute STI may enhance the transmission of and susceptibility to HIV,1 while HIV, can modify the natural history of STI by causing immunosuppression.3,4 Antiretroviral therapy (ARV) that achieves virologic suppression reduces risk of horizontal transmission to HIV uninfected partners5 lending hope that “treatment as prevention” (TasP) may result in sex without a condom is becoming more frequent, and anxiety about HIV acquisition risk can be considerably lessened.6 Therefore, a study on risky sexual practice during the TasP era of HIV prevention and treatment approach is essential.
Though several studies reported a high prevalence of risky sexual practice among the general population and HIV-positive people who were on ART7–10 in particular, there are very few studies on the sexual behavior of newly HIV diagnosed people. In addition, findings from HIV treatment-experienced individuals may not be generalized to those patients who were newly enrolled in care. This is because counseling interventions delivered during routine clinical care reduces risky sexual practices.11
The definition of sexual practice as “risky” varies across culture, gender, age, and the threshold.12 The definition can also take several forms which range from having a large number of sexual partners, having unprotected sex, starting sex at an earlier age, to sexual intercourse under the influence of substances such as alcohol or cocaine.13–16 Many previous studies defined risky sexual practice when one or more of the following happen: having multiple sexual partners (more than one sexual partner), early initiation of sex (sexual debut at the age <18 years old), inconsistent use of condoms (inconsistent/failure to use condoms at least once during sexual intercourse) and sex with commercial sex workers.7,14,17–19 In this study, we adopted the definitions of risky sexual practice as having unprotected sexual intercourse as the most recent sexual activity among those who had sex with a nonregular sexual partner.20 This would avoid overestimation of risky sexual practice in line with the study population.
The expansion of ART treatments to all individuals as recommended by the new WHO guidelines21 has the potential to increase the prevalence of risky sexual practice because individuals are aware that ART increases life expectancy.22 Indeed, some studies have reported that using ART as prevention may change peoples’ sexual practice to “risky” due to perceived “lower HIV threat”,23 and some works have reported no significant change in the level of sexual behavior24 and persistence of risky sexual practice after enrollment in care.9 These findings are similar to those in studies that reported persistent risky sexual practice among patients on ART15,25 while patients in the early and standard ART groups reported no change in sexual practice in Côte d’Ivoire.26
Factors associated with risky sexual practice in various studies include being educated, being wealthy and young,27 substance abuse, peer pressure, and watching pornography.16,17,28–30 Other factors are living in urban areas,27 being single and married compared to widowed,19 having HIV-positive sexual partner, nondisclosure of HIV-positive status, having experienced HIV-related stigma,31 history of suicide attempt and sexual assault.29
A study conducted in South Africa noted that there is a high level of risky sexual practice among HIV-positive individuals on and about to start ART.32 This is because people with higher risky sexual practice were also less likely to know their HIV-positive status.33 Previous separately undertaken studies for risky sexual practice and STIs have identified the same factors for both issues. For this reason, risky sexual practice is often identified through the diagnosis of an STI.13 Hence, we aimed to identify similar factors for risky sexual practice and STI in separate models. Moreover, there is recommendation from previous study to combine both outcomes at a time since self-reported risky sexual practice may not necessarily be a good measure of exposure to STIs.1 Furthermore, there is a paucity of evidence on risky sexual practices, STIs and associated factors among newly diagnosed HIV-positive people in regard to risky sexual practice, STI, and associated factors. Therefore, this study was conducted to fill the knowledge gap on the prevalence of risky sexual practice, STIs, and associated factors among newly diagnosed HIV-positive people. Moreover, we have tested the hypothesis that factors associated with risky sexual practice can explain the diagnosis of STIs using syndromic approach.
Patients and Methods
Study Settings and Period
The study was conducted in three administrative zones of Amhara regional state, northwest Ethiopia. These were East Gojjam Zone, West Gojjam Zone and Bahir Dar city administration. There are five hospitals and six health centers in East Gojjam Zone. These are Debre Markos Referral Hospital, Motta Primary Hospital, Lumame Primary Hospital, Yejube Primary Hospital, and Bichena Primary Hospital. Health Centers found in this zone are Debre Markos Health Center, Hidasie Health Center, Lumame Health Center, Dejen Health Center, Debre Work Health Center, and Bichena Health Center. Two hospitals and six health centers are found in the West Gojjam Zone. These are Finote Selam Primary Hospital, Asrade Memorial Primary Hospital, Burie Health Center, Mankusa Health Center, Finote Selam Health Center, Jiga Health Center, Dembecha Health Center and Durbete Health Center. From Bahir Dar city administration two hospitals and three health centers were selected. These are Felege Hiwot Referral Hospital, Addis Alem Primary Hospital, Abay Health center, Bahrdar Health Center and Han Health Center. The study was conducted between December 1, 2018 and July 30, 2019.
Study Design
A cross-sectional study design was conducted to determine the prevalence of risky sexual practice and STIs with possible associated factors among newly diagnosed HIV-positive people.
Population and Eligibility Criteria
All newly diagnosed HIV-positive individuals during the study period were the source population. Whereas, the study population were those patients who were within a week of HIV diagnosis from selected health facilities and those who fulfilled the inclusion criteria.
The inclusion criteria for health facilities was having an adequate patient flow (three to five patients per month) so as to ensure efficient utilization of available resources. All adults (≥18 years) who were newly diagnosed as HIV positive in the selected health facilities were included. Patients who interrupted their treatment and re-initiated ART within the study period were excluded from the study. A total of 745 patients to determine both risky sexual practice, STIs, and associated factors were included in this study.
Sample Size and Sampling Technique
There are 72 public health facilities rendering ART services in the three zones. Based on an adequate patient flow, we included 24 health facilities with an average case flow of three to five new cases per month. Health facilities involved in the study were 11 form East Gojjam, eight from West Gojjam and five from Bahir Dar city administrative zones. All adult HIV-positive people were enrolled in the study after securing their consent.
Data Collection Tools, Procedure and Quality Assurance
Data collection tools were used to obtain sociodemographic, clinical, behavioral, and psychological characteristics of the patients. The tools were developed by reviewing similar literature in the field.4,6,12,17,20,30,31,34 The tools were used in similar settings including Ethiopia. An interviewer-administered questionnaire was used at exit to interview the newly diagnosed HIV-positive people. Nurses working in the ART clinic conducted the client exit interview in a separate and quiet room. The interviews were undertaken within the week in which patients know their HIV status depending on the patient’s readiness. To ensure the quality of data, we trained data collectors, arranged pretest among 5% of the total sample (40 individuals) in Wuseta health center. But this was not included in the final data collection. Furthermore, close supervision of the data collection process was undertaken by the principal investigator and trained supervisors.
Study Variables and Operational Definitions
The dependent variables were risky sexual practice and sexually transmitted infection. Risky sexual practice included any of the following: having had sex in the last year with a nonregular partner, and not using a condom on the last occasion with that partner.12,35 STIs were ascertained by using syndrome approach of STI management. Syndromic management is based on the identification of a group of symptoms and easily recognized signs associated with infection of well-defined pathogens.36 Treatment for each syndrome is directed against the main organisms within that geographical setting responsible for the syndrome.36 The independent variables for both outcomes were sociodemographic characteristics, baseline clinical characteristics, behavioral characteristics, and psychological characteristics identified using perceived stigma and psychological distress. In addition, community and health facility level variables were also examined. These included patient residence (rural, urban), zones (East Gojjam, West Gojjam and Bahir Dar City Administration), health facility type (health center or hospital), and distance from health facility.
Data Processing and Analysis
Data were entered into EpiData version 3.5 and were exported to SPSS version 24 for further analysis. Data were cleaned and descriptive analysis carried out using SPSS. Bivariate and multivariate logistic regression analyses were carried out. Separate logistic regression models were fitted for risky sexual behavior and STI. In the bivariate analysis, we assessed the association between each independent variable and the outcome variable (risky sexual practice and STI). Variables with a p-value less than 0.25 on bivariate logistic regression analysis were then included in the multivariate logistic regression model. Finally, statistical associations were quantified using adjusted odds ratio (AOR) with 95%CI.
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki. The proposal was approved by the joint University of Ibadan/University College Hospital, Ibadan Institutional Review Board (IRB) of the University College Hospital (UCH), University of Ibadan, Nigeria (reference number UI/EC/18/0463). It was also approved by IRB at Debre Markos University (reference number HSC/30/02/2011). Permission was obtained from Amhara Public Health Institute. Moreover, we obtained written informed consent from each study subject. Collected data were treated with utmost confidentiality.
Results
Sociodemographic Characteristics
A total of 745 HIV-positive patients participated in the study giving a response rate of 98%. More than half of the study participants (57.9%) were females. Almost half (347, 46.6%) were in the age group of 25–34 years and the mean age of study participants was 33.25 years (SD ±9 years). The majority (94.6%) were Ethiopian Orthodox Christians by religion. Four hundred and ninety-three (66.2%) were employed and 166 (22.3%) were among the poorest wealth quartiles (Table 1).
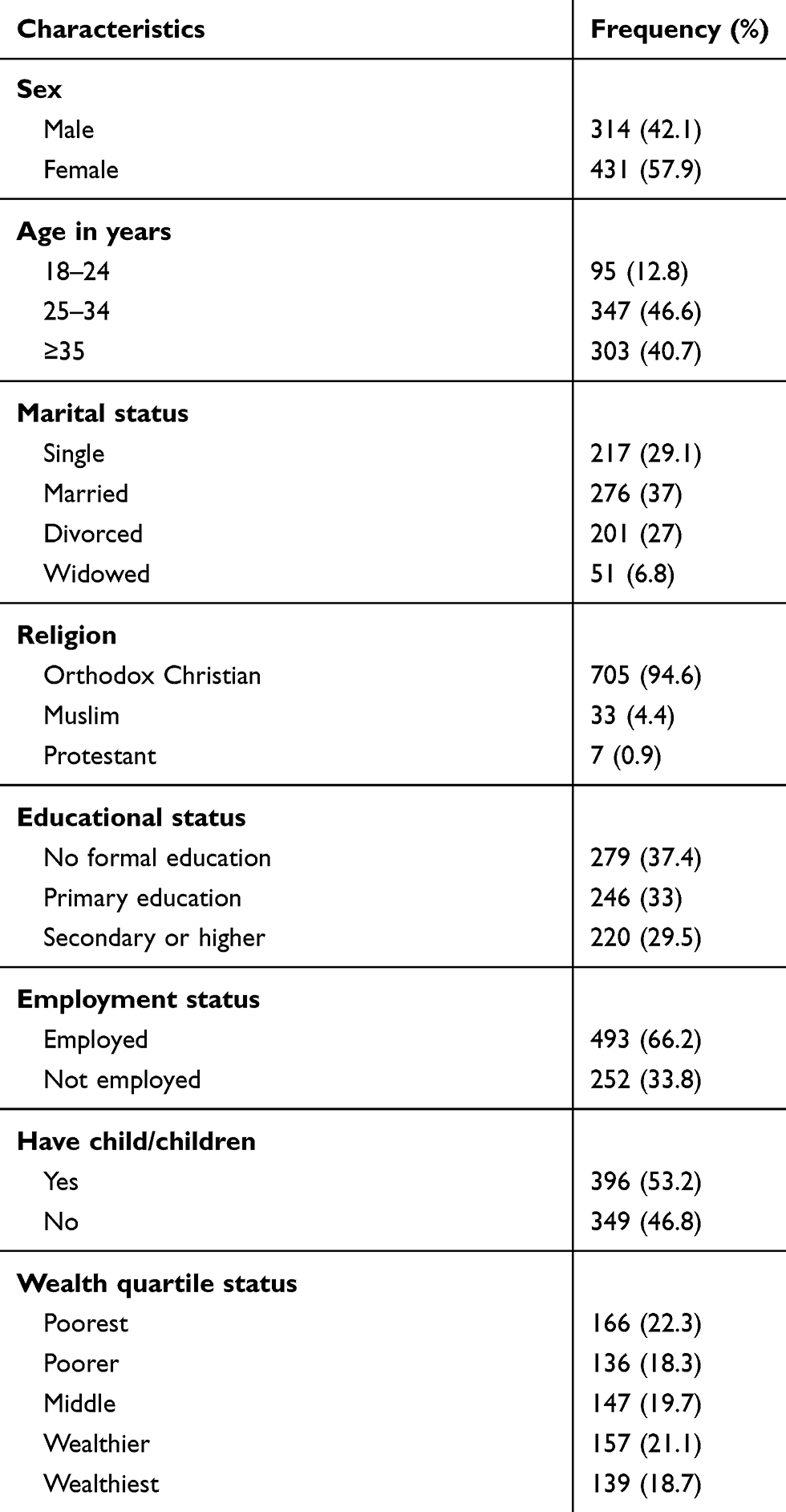 |
Table 1 Socio-Demographic Characteristics of Newly HIV-diagnosed People in Northwest Ethiopia, 2019 |
Health Facility and Community-related Characteristics
The majority of the patients (328, 44%) were from the East Gojjam Zone followed by patients from Bahir Dar City (250, 33.6%) and West Gojjam Zone (167, 22.4%) administrations. About half (373, 50.1%) of the patients were from hospitals. Meanwhile, majority (565, 75.8%) were urban residents. The majority of the patients 573 (76.9%) were diagnosed with their HIV status in the same health facility in which they were enrolled for ART services whereas the rest (172, 23.1%) were referred from another health facility.
Clinical Characteristics of Study Participants
Most of the patients (564, 75.7%) were WHO clinical stage I/II while 181 (24.3%) were WHO stage III/IV. Four hundred and seventy-eight (64.2%) presented to care with no symptoms while 267 (35.8%) had various symptoms. Similarly, 647 (86.8%) were at working functional status and 98 (13.2%) were either in ambulatory or bedridden functional status. Four hundred and ninety-nine (74%) were normal in their nutritional status while 139 (20.6%) and 36 (5.3%) were mildly and severely malnourished, respectively. The majority of patients (501, 67.2%) were tested due to health-care providers’ initiation while 244 (32.8%) were from voluntary HIV testing and counseling service.
Risky Sexual Practice, STI and Other Behavioral Characteristics
The magnitude of risky sexual practice was 118 (15.8%, 95%CI: 13.1–18.4%). The percentage of patients who presented for HIV care with STI was 49 (6.6%) at (95%CI: 4.8–8.5). The majority (75.3%) had disclosed their HIV status to somebody. More than half (57.4%) of the study participants did not know the serostatus of their sexual partner (Table 2).
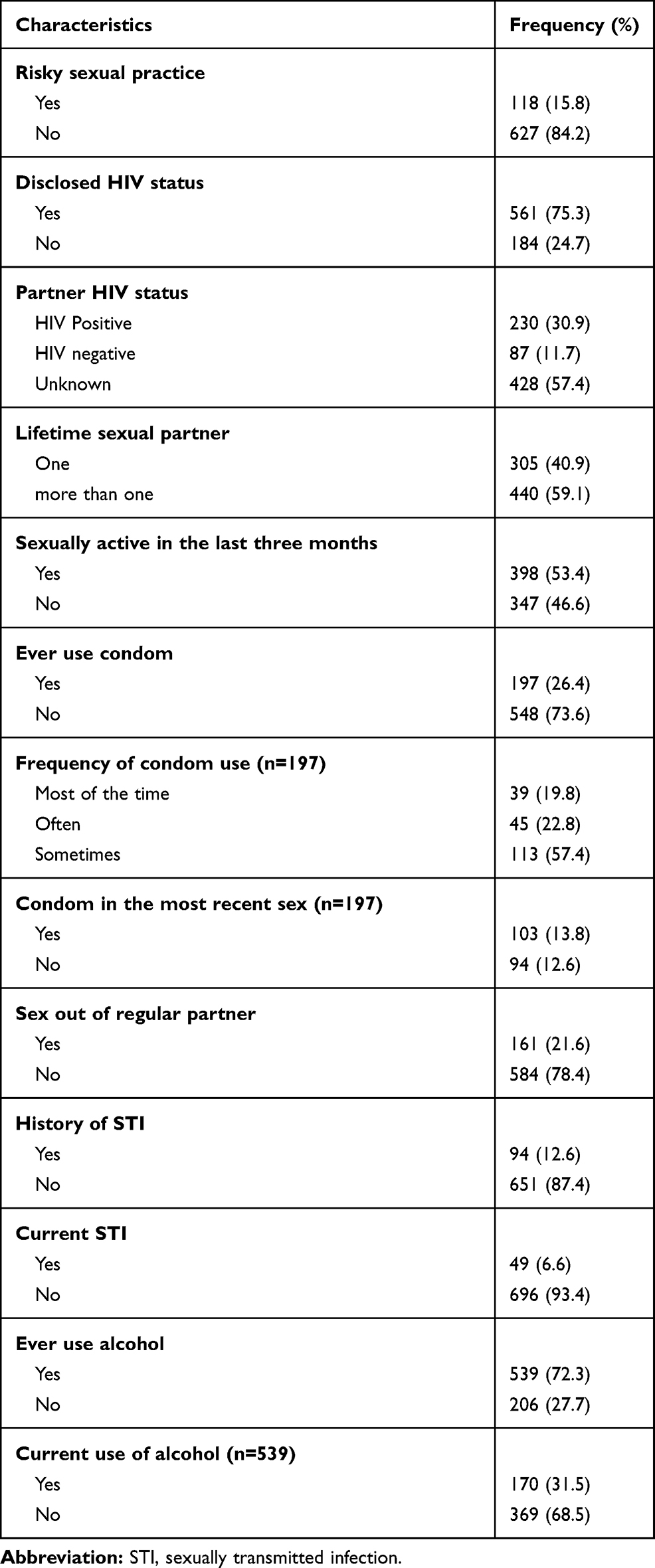 |
Table 2 Behavioral Characteristics of Newly HIV-diagnosed People in Northwest Ethiopia, 2019 |
Factors Associated with Risky Sexual Practices
In the bivariate analysis, several independent variables were associated with risky sexual practice at a p-value less than 0.25. These include being male, having no child, HIV test via PICT, two or more lifetime sexual partners, history of STI and history of alcohol use. In the final multivariate logistic regression model, only two variables were statistically associated with the outcome variable. These were, having two or more lifetime sexual partners (AOR=3.19; 95%CI: 1.57–6.49) and ever use of alcohol (AOR=3.10; 95%CI: 1.34–7.19) (Table 3).
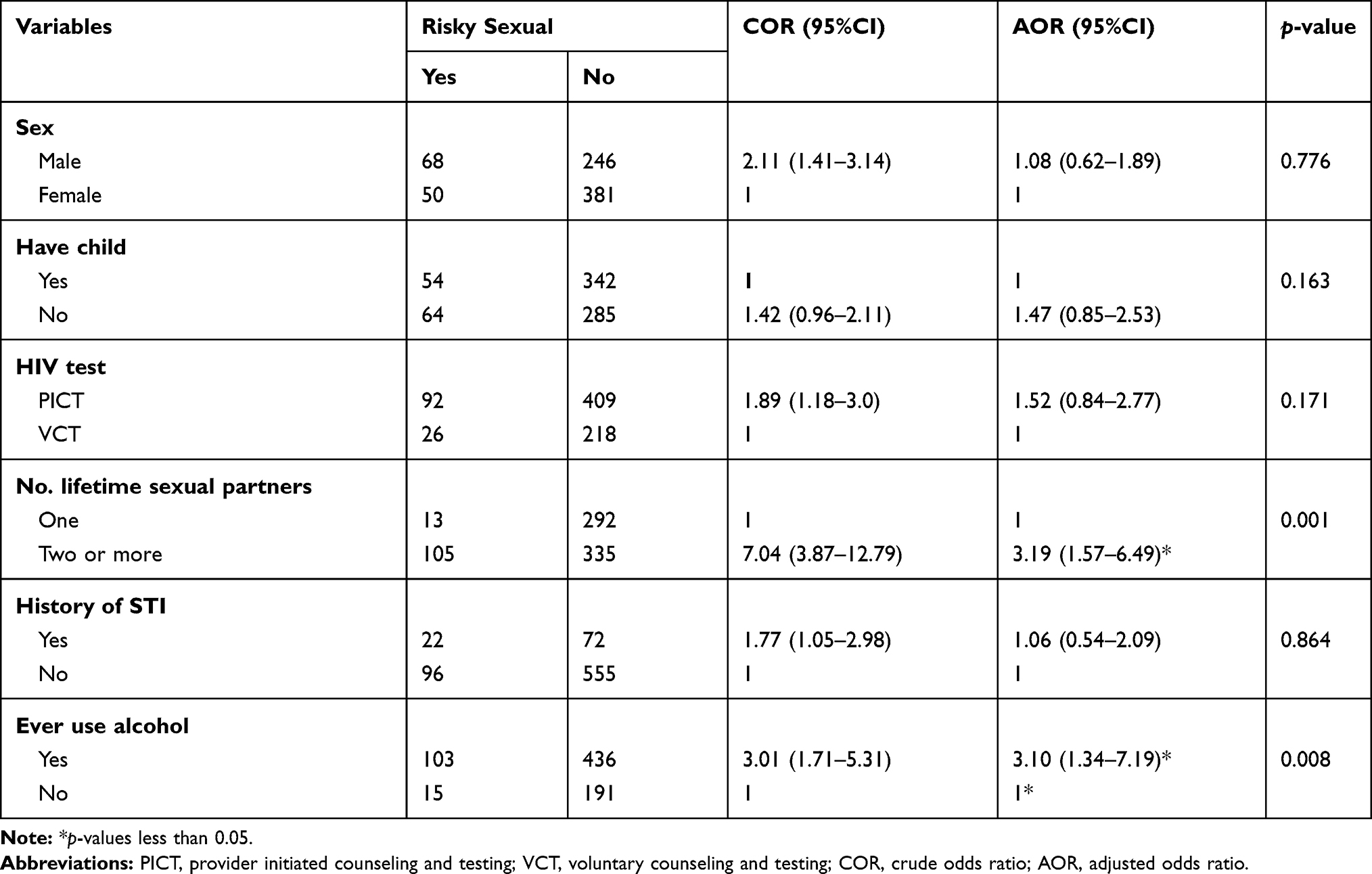 |
Table 3 Factors Associated with Risky Sexual Behavior Among Newly HIV-diagnosed People in Northwest Ethiopia, 2019 |
Factors Associated with STI
In the bivariate analysis, many independent variables were associated with the dependent variable of having an STI. From health facility-related variables, patients who resided in the East Gojjam Zone and the West Gojjam Zone were more likely to have an STI compared to patients who resided in the regional city (Bahir Dar). A number of socioeconomic variables were associated with presentation with STIs. These included being a merchant and unemployed compared to farmers. Age group of 25–34 years and medium wealth status were associated with STIs compared to >34 years of age and the poorest. Furthermore, patients who lived in a rented house were less likely to present with STI compared to patients who were living in their own house. Similarly, several behavioral-related independent variables were associated with presenting with STI. These were never testing for HIV, nondisclosure of HIV status, having more than one lifetime sexual partner and never using condoms. However, in the multivariate logistic regression model, none of the independent variables were statistically associated with STI.
Discussion
This study examined the prevalence of risky sexual practice, STI and associated factors among newly diagnosed HIV positive people in northwest Ethiopia. The findings revealed that relatively lower prevalence of risky sexual practice (15.8%) and STI (6.6%) among newly diagnosed HIV-positive people in Ethiopia. Factors associated with risky sexual practice were having two or more lifetime sexual partners and frequent use of alcohol while no statistically significant factors were associated with STIs.
The prevalence of risky sexual practice among newly diagnosed HIV-positive people in the study area was lower (15.8%) compared to findings from different studies in other parts of Ethiopia. Risky sexual practices among preparatory school students was 19.6% in Aksum northern Ethiopia,17 41.62% among university and college students across Ethiopia,30 42.8% in the general population of Ethiopia28 and 22.4% among preparatory school students in Arba Minch town, southern Ethiopia.16 The differences of the findings may be due to the different characteristics of the study participants. Most of the previous studies were undertaken among young students in whom risky sexual practices were documented to be high.37–39 Similarly, risky sexual practices among HIV-positive people who are on ART were documented to be high in Ethiopia and elsewhere in Africa.10,19 Such cases include study reports from Nekemte Referral Hospital in western Ethiopia 32.9%,31 Gondar University Referral Hospital in northwest Ethiopia 38%,19 Nairobi in Kenya 44.4%,10 Dar Es Salaam, in Tanzania 40%,8 Cape Town in South Africa 44–46%25,32 and the Regional Hospital of Sokodé, in Togo 34.6%.7 The discrepancies between the current findings and the previous studies could be different definitions of risky sexual practices which ranges from having a large number of sexual partners, having unprotected sex, starting sex in earlier age, to sexual intercourse under the influence of substances such as alcohol or cocaine.13–16
Failure to abide by the strong recommendations of consistent condom use among HIV-positive people40 may raise the magnitude of risky sexual practice among HIV positive people who were on ART. Though consistent and correct use of condoms reduces the risk of heterosexual HIV transmission, in the new approach of ART treatment as prevention21,41 that reported undetectable viral load is effectively zero of HIV transmission.42,43 Therefore, it is time to redefine the risky sexual practices among HIV patients on ART in line with the current findings stating that persons living with HIV who achieve sustained viral suppression with ART can avoid sexual transmission of HIV without using condoms.5,6 However, the risky sexual practices in the current study was higher than a in study in France which is 9.5%.29 The difference could be due to differences in study population and broader definitions of risky sexual practices since the later study included failure to use a condom at first intercourse with a new partner as risky sexual behavior.29
Newly diagnosed HIV-positive people with a history of two or more lifetime sexual partners were more likely to practice risky sex compared to those who have had only one lifetime sexual partner. This finding was supported by similar evidence in Tanzania8 and Uganda.2 Similarly, patients with history of alcohol use were related to the likelihood of practicing risky sex. Such findings were in line with studies in Togo,7 Kenya10 and Tanzania.8 The reason for the associations of alcohol consumption and risky sexual practice can be explained that alcohol consumption prior to sex may affect the decision made to practice safer or unsafe sex.
This study also found a low (6.6%) prevalence of sexually transmitted infections among newly diagnosed HIV-positive people in Ethiopia. The value was lower than a study report in Gondar (18.20%), northwest Ethiopia,44 in Asella (26.6%), central Ethiopia,45 Addis Ababa46 and national antenatal sentinel surveillances.34 The reason can be explained by the fact that the previous three studies34,45,46 employed a serological test showing exposure to specific STI pathogens among pregnant women, while the current study utilized only syndromic approach to diagnose STI.
Although previous evidence showed different factors associated with STI were previous history of STI, multiple sexual partners in life and not using condoms during sexual intercourse,44 in the current study, no variable was identified as a factor associated with STI. This may suggest that the study participants in our study were homogeneous study population in the current study in terms of included variables (risk factors for STI), and therefore, failed to discriminate on the basis of STI and its contributing factors among the study participants. The study participants in this study differed from the previous in the field as all of them had sexual experience and all were HIV positive. This implied that exposures for HIV can explain risky sexual behavior that causes STI in a similar way. Such findings were further supported by the fact that the prevalence of HIV is largely driven by heterosexual sex that assumed other STIs are also the result of unsafe sex.1 Further study is recommended to gauge the variability of risky sexual practice, STI and associated factors after initiation of lifelong ART.
Though the study was the first to determine the prevalence of risky sexual practice, STI and associated factors among newly diagnosed HIV-positive people in Ethiopia, there were limitations in the study due to the nature of the study design and methods of data collection. These included recall bias of participants in the use of condoms with nonregular sexual partners and the use of self-reported assessment of STI instead of serological test exposures for specific STI pathogens.
Conclusion
Risky sexual practices and STIs were low among newly diagnosed people living with HIV in northwest Ethiopia. Thus, revisiting the definition of risky sexual practice among HIV-positive patients is necessary in the universal test and treat approach since sustained viral suppression may remove the need for consistent condom use among HIV patients who are on ART especially with regular sexual partners. Factors associated with risky sexual practices failed to explain STI diagnosis using syndromic approach. Moreover, it reinforced that risky sexual practice was the base for the acquisition of HIV and other STIs.
Acknowledgments
This study was supported by the Pan African University (PAU), a continental initiative of the African Union Commission (AU), Addis Ababa, Ethiopia, as part of the PhD program in Reproductive Health Sciences. NAM received the funding from PAU. The University had no role in the study design and decision to publish, or preparation of the manuscript. Moreover, we want to extend our appreciation to Dr Sualih Mussa for his language editing assistance.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ezzati M, Lopez AD, Rodgers AA, et al. Comparative quantification of health risks: global and regional burden of disease attributable to selected major risk factors. 2004.
2. Rutaremwa G, Agaba P, Nansubuga E, Nankinga O. Association between risky sexual behaviour and having STIs or HIV among young persons aged 15–24 years in Uganda. 2016.
3. Mayaud P, McCormick D. Interventions against sexually transmitted infections (STI) to prevent HIV infection. Br Med Bull. 2001;58(1):129–153. doi:10.1093/bmb/58.1.129
4. Okoboi S, Castelnuovo B, Moore DM, et al. Incidence rate of sexually transmitted infections among HIV infected patients on long-term ART in an urban and a rural clinic in Uganda. BMC Public Health. 2019;19(1):87. doi:10.1186/s12889-019-6417-x
5. Cohen MS, Chen YQ, McCauley M, et al. Antiretroviral therapy for the prevention of HIV-1 transmission. N Engl J Med. 2016;375(9):830–839. doi:10.1056/NEJMoa1600693
6. Marrazzo JM, Dombrowski JC, Mayer KH. Sexually transmitted infections in the era of antiretroviral-based HIV prevention: priorities for discovery research, implementation science, and community involvement. PLoS Med. 2018;15(1):e1002485. doi:10.1371/journal.pmed.1002485
7. Yaya I, Saka B, Landoh DE, et al. Sexual risk behavior among people living with HIV and AIDS on antiretroviral therapy at the regional hospital of Sokodé, Togo. BMC Public Health. 2014;14(1):636. doi:10.1186/1471-2458-14-636
8. Mhalu A, Leyna GH, Mmbaga EJ. Risky behaviours among young people living with HIV attending care and treatment clinics in Dar Es Salaam, Tanzania: implications for prevention with a positive approach. J Int AIDS Soc. 2013;16(1):17342. doi:10.7448/IAS.16.1.17342
9. Braunstein SL, Umulisa -M-M, Veldhuijzen NJ, et al. HIV diagnosis, linkage to HIV care, and HIV risk behaviors among newly diagnosed HIV-positive female sex workers in Kigali, Rwanda. J Acquir Immune Defic Syndr. 2011;57(4):e70–e76. doi:10.1097/QAI.0b013e3182170fd3
10. Muturi N, Kikuvi G, Gichuki R, et al. Factors associated with risky sexual behavior among HIV negative partners in HIV discordant relationships in Nairobi, Kenya. Afr J Health Sci. 2013;26(4):324–336.
11. Fisher JD, Cornman DH, Shuper PA, et al. HIV prevention counseling intervention delivered during routine clinical care reduces HIV risk behavior in HIV-infected South Africans receiving antiretroviral therapy: the Izindlela Zokuphila/Options for Health randomized trial. JAIDS. 2014;67(5):499. doi:10.1097/QAI.0000000000000348
12. Chawla N, Sarkar S. Defining “high-risk sexual behavior” in the context of substance use. J Psychosexual Health. 2019;1(1):26–31. doi:10.1177/2631831818822015
13. Glen-Spyron C. Risky Sexual Behavior in Adolescence. Namibia: Belia Vida Centre; 2015.
14. Rockwell JA. Association between HIV/AIDS education and reduced risky sexual behaviors amongst African American adolescents living in the United States in 2013. 2016.
15. George G, Beckett S, Cawood C, et al. Impact of HIV testing and treatment services on risky sexual behaviour in the uMgungundlovu District, KwaZulu-Natal, South Africa: a cross-sectional study. AIDS Res Ther. 2019;16(1):20. doi:10.1186/s12981-019-0237-z
16. Abera M, Kedir T, Rasha D, et al. Risky sexual behaviors and associated factors among preparatory school students in Arba Minch town, Southern Ethiopia. J Public Health Epidemiol. 2018;10(12):429–442. doi:10.5897/JPHE2018.1073
17. Girmay A, Mariye T. Risky sexual behavior practice and associated factors among secondary and preparatory school students of Aksum town, northern Ethiopia, 2018. BMC Res Notes. 2019;12(1):698. doi:10.1186/s13104-019-4714-1
18. Uchudi J, Magadi M, Mostazir M. A multilevel analysis of the determinants of high risk sexual behavior (multiple sexual partners) in sub-Saharan Africa.
19. Molla AA, Gelagay AA, Ciccozzi M. Risky sexual practice and associated factors among HIV positive adults attending anti-retroviral treatment clinic at Gondar University Referral Hospital, Northwest Ethiopia. PLoS One. 2017;12(3):e0174267. doi:10.1371/journal.pone.0174267
20. Gómez F, Barrientos J, Cárdenas M. Relation between HIV status, risky sexual behavior, and mental health in an MSM sample from three Chilean cities. Revista Panamericana de Salud Pública. 2017;41:e4.
21. WHO. Guidelines for managing advanced HIV disease and rapid initiation of antiretroviral therapy, July 2017. 2017.
22. Delavande A, Kohler H-P. HIV/AIDS-related expectations and risky sexual behaviour in Malawi. Rev Econ Stud. 2016;83(1):118–164. doi:10.1093/restud/rdv028
23. Stolte IG, Dukers NH, Geskus RB, et al. Homosexual men change to risky sex when perceiving less threat of HIV/AIDS since availability of highly active antiretroviral therapy: a longitudinal study. Aids. 2004;18(2):303–309. doi:10.1097/00002030-200401230-00021
24. Ko N-Y, Liu H-Y, Lee H-C, et al. One-year follow-up of relapse to risky behaviors and incidence of syphilis among patients enrolled in the HIV case management program. AIDS Behav. 2011;15(5):1067–1074. doi:10.1007/s10461-010-9841-6
25. Eisele TP, Mathews C, Chopra M, et al. Changes in risk behavior among HIV-positive patients during their first year of antiretroviral therapy in Cape Town South Africa. AIDS Behav. 2009;13(6):1097. doi:10.1007/s10461-008-9473-2
26. Jean K, Gabillard D, Moh R, et al. Effect of early antiretroviral therapy on sexual behaviors and HIV-1 transmission risk among adults with diverse heterosexual partnership statuses in Cote d’Ivoire. J Infect Dis. 2013;209(3):431–440. doi:10.1093/infdis/jit470
27. Berhan Y, Berhan A. A meta-analysis of risky sexual behaviour among male youth in developing countries. AIDS Res Treat. 2015;2015:1–9. doi:10.1155/2015/580961
28. Muche AA, Kassa GM, Berhe AK, et al. Prevalence and determinants of risky sexual practice in Ethiopia: systematic review and meta-analysis. Reprod Health. 2017;14(1):113. doi:10.1186/s12978-017-0376-4
29. Sicard S, Mayet A, Duron S, et al. Factor associated with risky sexual behaviors among the French general population. J Public Health. 2017;39(3):523–529. doi:10.1093/pubmed/fdw049
30. Amare T, Yeneabat T, Amare Y. A systematic review and meta-analysis of epidemiology of risky sexual behaviors in college and university students in Ethiopia, 2018. J Environ Public Health. 2019;2019:1–8. doi:10.1155/2019/4852130
31. Mosisa G, Woldemichael K, Ayalew F. Risky sexual behavior and associated factors among antiretroviral therapy attendees in Nekemte referral hospital, Western Ethiopia: a cross-sectional study. HIV/AIDS. 2018;10:125.
32. Eisele TP, Mathews C, Chopra M, et al. High levels of risk behavior among people living with HIV Initiating and waiting to start antiretroviral therapy in Cape Town South Africa. AIDS Behav. 2008;12(4):570–577. doi:10.1007/s10461-007-9279-7
33. Huerga H, Venables E, Ben-Farhat J, et al. Higher risk sexual behaviour is associated with unawareness of hiv-positivity and lack of viral suppression–implications for treatment as prevention. Sci Rep. 2017;7(1):1–7. doi:10.1038/s41598-017-16382-6
34. Kassa D, Gebremichael G, Tilahun T, et al. Prevalence of sexually transmitted infections (HIV, hepatitis B virus, herpes simplex virus type 2, and syphilis) in pregnant women in Ethiopia: trends over 10 years (2005–2014). Int J Infect Dis. 2019;79:50–57. doi:10.1016/j.ijid.2018.11.009
35. CSACE I. Ethiopia Demographic and Health Survey 2016. Addis Ababa, Ethiopia, and Rockville, Maryland, USA: CSA and ICF; 2016.
36. National AIDS Commission. National guidelines for the management of sexually transmitted infections using syndromic approach. Addis Ababa, Ethiopia; 2015.
37. Tarkang E, Pencille L, Amu H, et al. Risky sexual behaviours among young people in sub-Saharan Africa: how can parents use the Ottawa Charter for Health Promotion for change? SAHARA-J: J Social Aspects HIV/AIDS. 2019;16(1):77–80. doi:10.1080/17290376.2019.1636710
38. Ssewanyana D, Mwangala PN, Van Baar A, et al. Health risk behaviour among adolescents living with HIV in sub-Saharan Africa: a systematic review and meta-analysis. Biomed Res Int. 2018;2018:1–18. doi:10.1155/2018/7375831
39. Malga PF, Setlalentoa BM, Oduaran C, et al. Factors influencing HIV/AIDS and risky sexual behaviour among learners in South Africa. Glob J Health Sci. 2018;10(5):197. doi:10.5539/gjhs.v10n5p197
40. Frehiwot N, Mizan K, Seble M et al. National guidelines for comprehensive HIV prevention, care and treatment. Addis Ababa: Ministry of Health; 2014.
41. Ford N, Migone C, Calmy A, et al. Benefits and risks of rapid initiation of antiretroviral therapy. AIDS. 2018;32(1):17. doi:10.1097/QAD.0000000000001671
42. Patel RR, Curoe KA, Chan PA. Undetectable equals untransmittable: a game changer for HIV prevention. Clin Chem. 2020;66(3):406–407. doi:10.1093/clinchem/hvz010
43. Rodger AJ, Cambiano V, Bruun T, et al. Risk of HIV transmission through condomless sex in serodifferent gay couples with the HIV-positive partner taking suppressive antiretroviral therapy (PARTNER): final results of a multicentre, prospective, observational study. Lancet. 2019;393(10189):2428–2438. doi:10.1016/S0140-6736(19)30418-0
44. Kassie BA, Yenus H, Berhe R, Kassahun EA. Prevalence of sexually transmitted infections and associated factors among the University of Gondar students, Northwest Ethiopia: a cross-sectional study. BMC Reprod Health. 2019;16:163. doi:10.1186/s12978-019-0815-5
45. Schönfeld A, Feldt T, Tufa TB, et al. Prevalence and impact of sexually transmitted infections in pregnant women in central Ethiopia. Int STD & AIDS. 2017;29:251–258. doi:10.1177/0956462417723545
46. Duncan ME, Tibaus G, Pelzer A, et al. Prevalence and significance of sexually transmitted diseases among Ethiopian women attending antenatal clinics in Addis Ababa. Ethiop J Health Dev. 1995;9(1):31–40.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.