")
Back to Journals » Clinical Interventions in Aging » Volume 16
Risk Factors of Emergency Room Visits for Bleeding Complications Following Transurethral Procedures in the Treatment of Benign Prostatic Hyperplasia: A Retrospective Cohort Study
Authors Teng TC , Shao IH, Hsu YC, Chen Y, Tsao SH , Kang YT, Hsieh ML
Received 19 July 2021
Accepted for publication 15 September 2021
Published 29 September 2021 Volume 2021:16 Pages 1747—1756
DOI https://doi.org/10.2147/CIA.S329468
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Nandu Goswami
Tzu-Chi Teng,1,2 I-Hung Shao,1,2 Yu-Chao Hsu,1,2 Yu Chen,1,2 Shu-Han Tsao,1,2 Yen-Te Kang,1,2 Ming-Li Hsieh1,2
1Division of Urology, Department of Surgery, Linkou Chang Gung Memorial Hospital, Taoyuan City, 33302, Taiwan; 2College of Medicine, Chang Gung University, Taoyuan City, 33302, Taiwan
Correspondence: Ming-Li Hsieh; I-Hung Shao
Division of Urology, Department of Surgery, Linkou Chang Gung Memorial Hospital, No. 5, Fuxing Street, Guishan District, Taoyuan City, 333423, Taiwan
Tel +886 975 365 568
; +886 975 361311
Fax +886-3-3274541
Email [email protected]; [email protected]
Purpose: Transurethral procedures, including transurethral resection of the prostate (TURP) and laser prostatectomy, are often linked to emergency room (ER) visits for postoperative bleeding. Although some studies have been conducted, the risk factors associated with these ER visits are not completely understood. This retrospective cohort study identified potential risk factors associated with ER visits for postoperative bleeding.
Patients and Methods: Preoperative assessment data and operational and postoperational parameters recorded at Chang Gung Memorial Hospital, Taiwan between December 2015 and January 2017 for patients who underwent elective transurethral procedures were analyzed to identify potential risk factors. The primary endpoint was ER visits for gross hematuria within three months following operation, and the secondary endpoint was ER visits for blood clot-induced urinary retention (clot retention) within three months following operation.
Results: A total of 665 patients who underwent elective transurethral procedures were enrolled. The transurethral procedures included monopolar transurethral resection of the prostate (M-TURP), bipolar TURP (B-TURP), greenlight photoselective vaporization of the prostate (PVP), thulium laser enucleation of the prostate (ThuLEP) and thulium laser transurethral vaporesection of the prostate (ThuVARP). Regarding ER visits for clot retention within three months, multivariable logistic regression revealed significantly lower rates of clot retention in patients who received B-TURP than in those who underwent ThuVARP (AOR, 0.18; 95% confidence interval [CI], 0.04– 0.82, p = 0.027). Moreover, significantly higher clot retention was observed in patients who underwent two or more rounds of manual irrigation (AOR, 9.51; 95% CI, 1.66– 54.43, p = 0.011).
Conclusion: Multiple manual irrigations shortly after operation can be considered a novel predictor of postoperative clot retention-related ER visits. Among the transurethral procedures, ThuVARP was associated with a higher risk of clot retention-related ER visits than was B-TURP.
Keywords: transurethral resection of prostate, laser prostatectomy, hematuria, clot retention
Introduction
Prevalence rates of benign prostatic hyperplasia (BPH) in patients with lower urinary tract symptoms (LUTS) are 50% to 75% among men over the age of 50 years and 80% among men over the age of 70 years. Overall incidence rates were reported to be 8.5 to 41 cases per 1000 people/year.1 In the past 20 years, the gold standard technique for BPH/LUTS surgical treatment has been TURP.2 However, TURP has risks of complications such as bleeding.
TURP is undertaken according to one of two methods, namely M-TURP and B-TURP. Postoperative hematuria is reported in 3.5% to 15.7% of patients who undergo M-TURP and 1% who undergo B-TURP. Clot retention is reported in 4.9% to 7.2% of patients who undergo M-TURP and 2.7% to 7.9% who undergo B-TURP.3–6 Through the use of laser technology, several therapies have been developed that can potentially surpass the efficacy of TURP methods and lead to fewer complications.7 Studies have reported that PVP,8 ThuLEP,9 and ThuVARP10 have lower risks of bleeding than that of TURP. Zorn and Liberman introduced the use of a 532-nm laser with GL 180-W XPS for performing PVP.11 ThuLEP was first described by Herrmann et al and consists of creating an incision through the surgical capsule with a thulium laser and blunt enucleation of the prostatic adenoma into the bladder.12 The ThuVARP method comprises resection of the prostatic tissue with a thulium laser (similar to TURP).13
The complication of bleeding may be associated with Foley catheter changing, manual irrigation, transfusion, ER visits, or readmission and may ultimately lead to increases in medical costs. In our clinic, despite excellent urologist training and thorough patient screening, some patients return to the ER with postoperative bleeding. Research into the risk factors associated with ER visits and bleeding complications is lacking. This study identified the potential risk factors of ER visits for bleeding after transurethral procedures in the treatment of BPH/LUTS.
Materials and Methods
This was a retrospective cohort study of patients who underwent elective transurethral procedures for the treatment of BPH/LUTS at a single tertiary center (Chang Gung Memorial Hospital, Taiwan). The data were collected between December 30, 2015, and January 4, 2017 (Ethics Committee approval: 201900001B0C102). Patients diagnosed as having genitourinary tract cancer, neurogenic LUTS, bladder neck contracture, or urethral stricture were excluded from the study. Preoperative assessment of age, Charlson Comorbidity Index (CCI) score, International Prostate Symptom Score (IPSS), prostate-specific antigen level (PSA), prostate volume, platelet count, international normalized ratio (INR), activated partial thromboplastin time (aPTT), length of hospital stay, and catheterization time was performed. Prostate volume was measured through transrectal ultrasonography (TRUS). Medication history, including the use of platelet aggregation inhibitors (PAIs), anticoagulants, and 5α-reductase inhibitors (5-ARIs), was collected. Operative- and postoperative-related parameters, including the seniority of the urologist, timing of operation (eg, first operation of the day, afternoon operation), weight and percentage of resected prostate, the use of Foley traction immediately after operation, repeated Foley traction after release, and the number of rounds of manual irrigation were recorded. The percentage of resected prostate was defined as the weight of the resected prostate divided by the prostate volume (as measured through TRUS). The percentage of resected prostate following PVP was not included in the analysis because no specimens were collected. The primary endpoint was defined as an ER visit for gross hematuria within three months following operation. The secondary endpoint was defined as an ER visit for urinary retention as a result of a blood clot within three months following operation.
Transurethral procedures included ThuVARP, ThuLEP, PVP, M-TURP, and B-TURP, and all operations were performed by experienced urological physicians. The patients on anticoagulants would stop the medication three days before surgery and restart before discharge from the hospital. Patients on PAIs were instructed to cease taking the medication 7 days prior to the operation and be resumed before discharge. Empiric antibiotics with cefazolin were prescribed if urinary tract infection was noted before surgery. Foley traction with balloon compression was performed on patients with all nonlaser procedures. All patients received continuous postoperative irrigation with a 22- or 24-Fr three-way Foley catheter for at least 8 h until the urine was sufficiently clear. Manual irrigation was arranged if a clot-related obstruction was noted. The Foley catheters were removed before the patients were discharged, and outpatient department (OPD) follow-ups were arranged.
Univariate and multivariable analyses were conducted through logistic regression. The parameters with p value less than 0.1 in univariable analysis were selected in the multivariable analysis. Subgroup analysis between methods was conducted with a chi-squared test. All tests were two-tailed, and p < 0.05 was considered statistically significant. Data analyses were conducted using SPSS v. 25 (IBM, Armonk, NY, USA).
Results
Of the 665 patients who underwent transurethral procedures, the percentage of patients who returned to our ER for gross hematuria in the first, second, and third month following operation was 5.3%, 5.7%, and 5.9%, respectively. The percentage of patients who returned to our ER for clot retention in the first, second, and third month following operation was 3.2%, 3.3%, and 3.3%, respectively (Figure 1). Thulium prostatectomy was performed on 43.5% of patients, 17.7% received ThuLEP, and 25.7% received ThuVARP. Manual irrigation was performed more than twice on 1.4% of patients (Table 1).
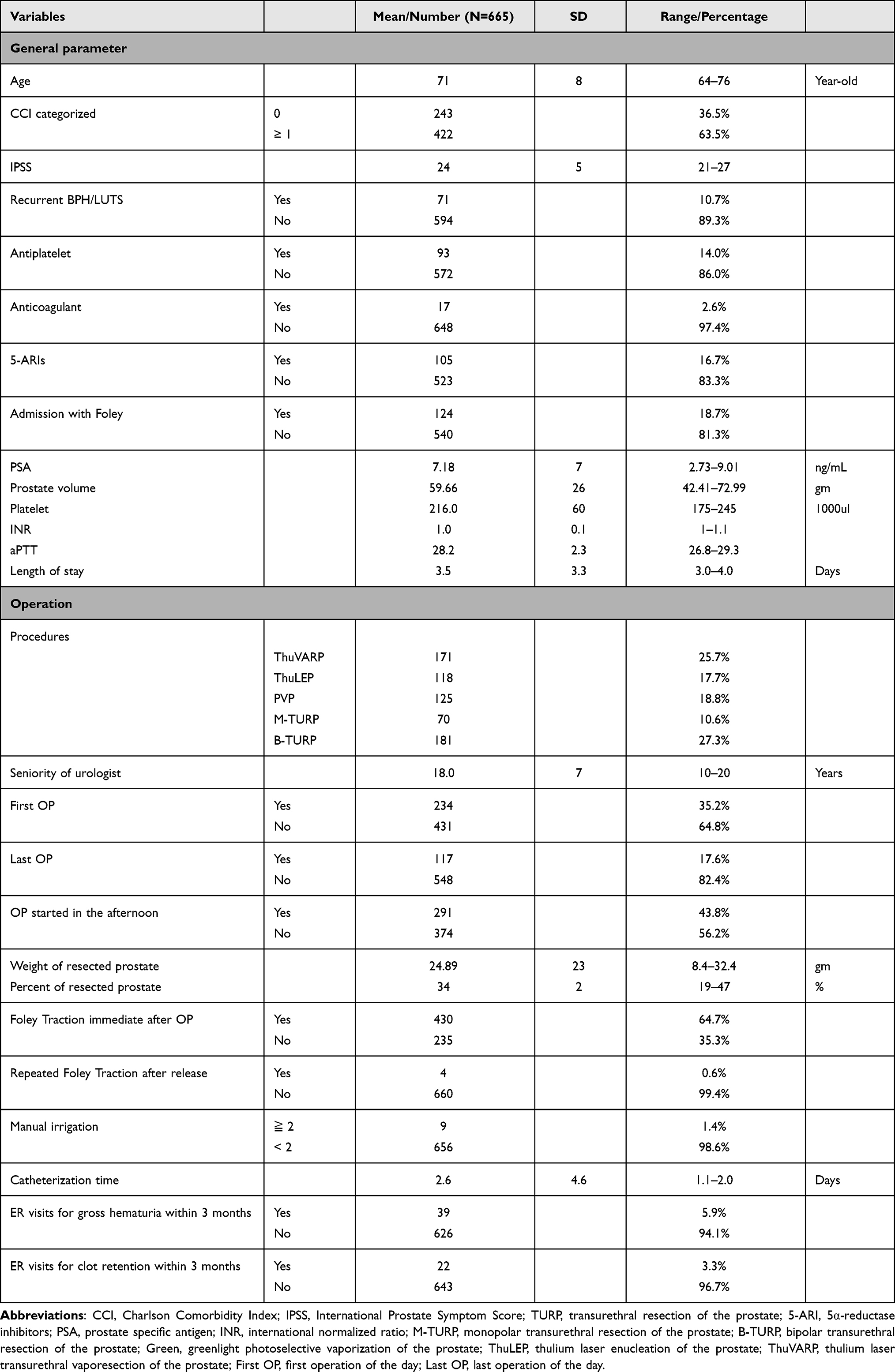 |
Table 1 Patient Characteristics |
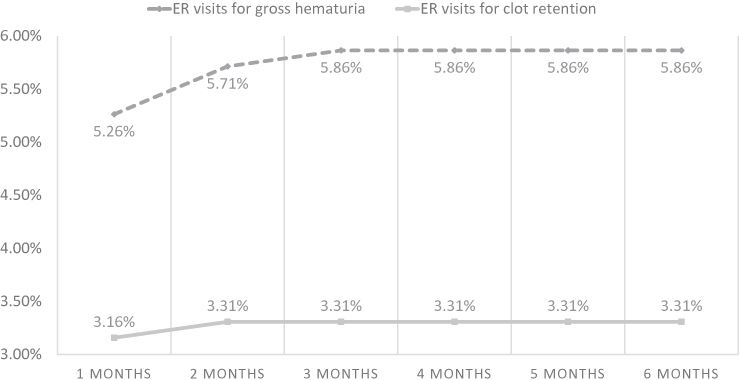 |
Figure 1 Trend of ER visits for hematuria and clot retention within six months following operation. |
Regarding ER visits for gross hematuria within three months, the odds ratio (OR) was significantly lower for PVP than for ThuVARP procedures (0.24; 95% confidence interval [CI], 0.07–0.84, p = 0.025). However, multivariable logistic regression revealed no significant difference in the adjusted odds ratios (AORs; Table 2). In the subgroup analysis of the different methods, significantly higher levels of gross hematuria were noted for ThuVARP than for PVP (p = 0.016; Figure 2).
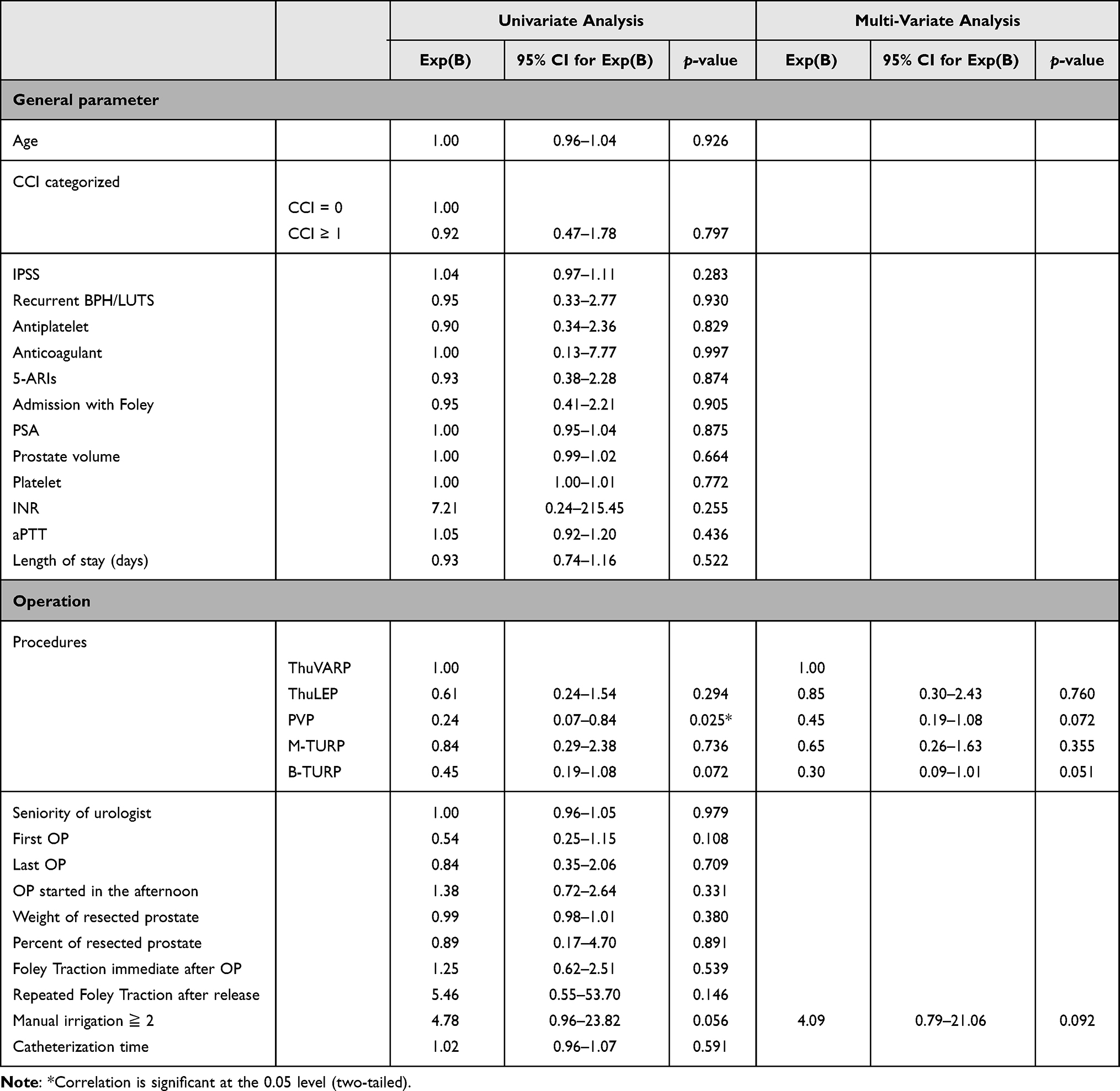 |
Table 2 Analysis of Predictors of ER Visits for Gross Hematuria Within Three Months |
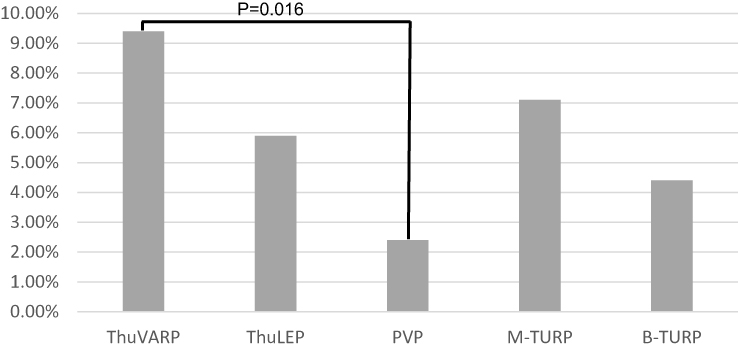 |
Figure 2 Incidence of ER visits for hematuria within three months for different methods. |
Regarding ER visits for clot retention within three months, the OR was significantly lower for B-TURP than for ThuVARP procedures (OR, 0.18; 95% CI, 0.04–0.83, p = 0.028). Additionally, repeated Foley traction after release (OR, 10.143; 95% CI, 1.01–101.63, p = 0.049) and two or more rounds of manual irrigation (OR, 9.086; 95% CI, 1.77–46.53, p = 0.008) were associated with a significantly increased risk of clot retention. Multivariable logistic regression revealed significantly lower rates of clot retention in patients who underwent B-TURP than in those who underwent ThuVARP (AOR, 0.18; 95% CI, 0.04–0.82, p = 0.027) and significantly higher rates of clot retention in patients who received two or more rounds of manual irrigation (AOR, 9.51; 95% CI, 1.66–54.43, p = 0.011; Table 3). In the subgroup analysis of different methods, significantly higher rates of clot retention were noted in patients who underwent ThuVARP than in those who underwent B-TURP (p = 0.014; Figure 3).
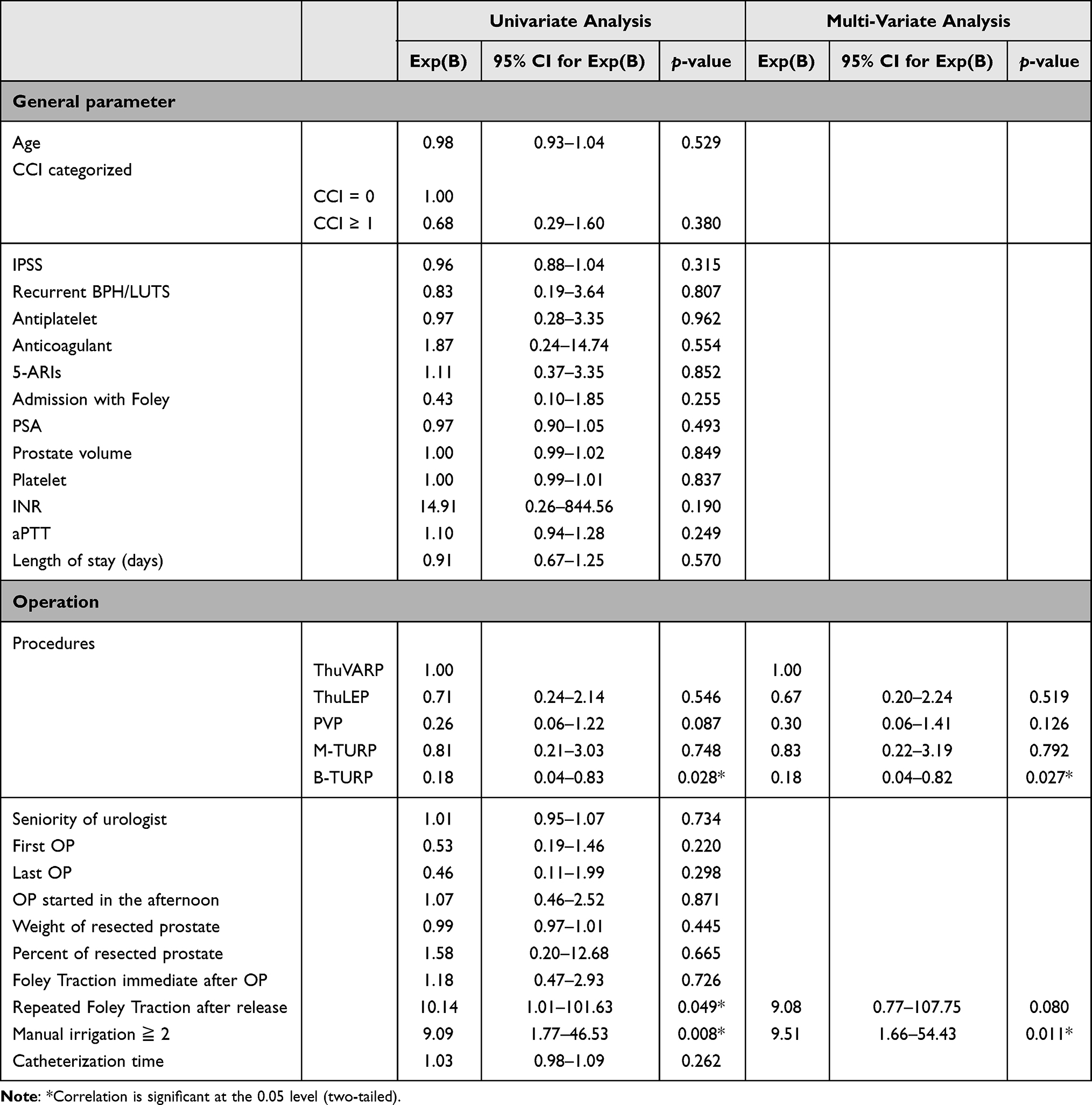 |
Table 3 Analysis of Predictors of ER Visits for Clot Retention Within Three Months |
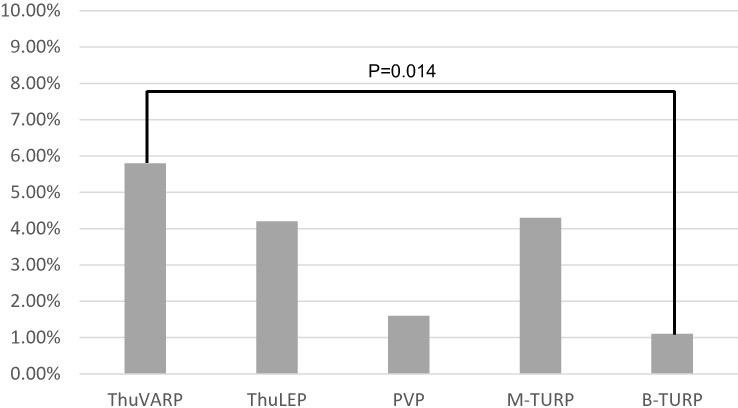 |
Figure 3 Incidence of ER visits for clot retention within three months for different methods. |
No significant differences were noted between both end points with respect to age; CCI score; the use of antiplatelets, anticoagulants, or 5-ARIs; prostate volume; length of hospital stay; timing of operation; percentage of resected prostate; or catheterization time.
Table 4 shows the early postoperative complications within 30-day. Gross hematuria and urge urinary incontinence found in 208 and 76 patients. All patients recovered spontaneously under conservative treatment. Urinary tract infection was noted in 201 patients and improved after antibiotics and hydration. 50 patients were diagnosed with acute urinary retention, who needed catheterization either Foley or cystostomy. All of them achieved catheter-free status within 3 months follow-up. 21 patients with clot retention went to our ER. All of them received Foley insertion with manual and continuous irrigation. 6 of them received cystoscopy for transurethral coagulation. There was no patient suffered from stroke or acute myocardial infarction in our clinical practice.
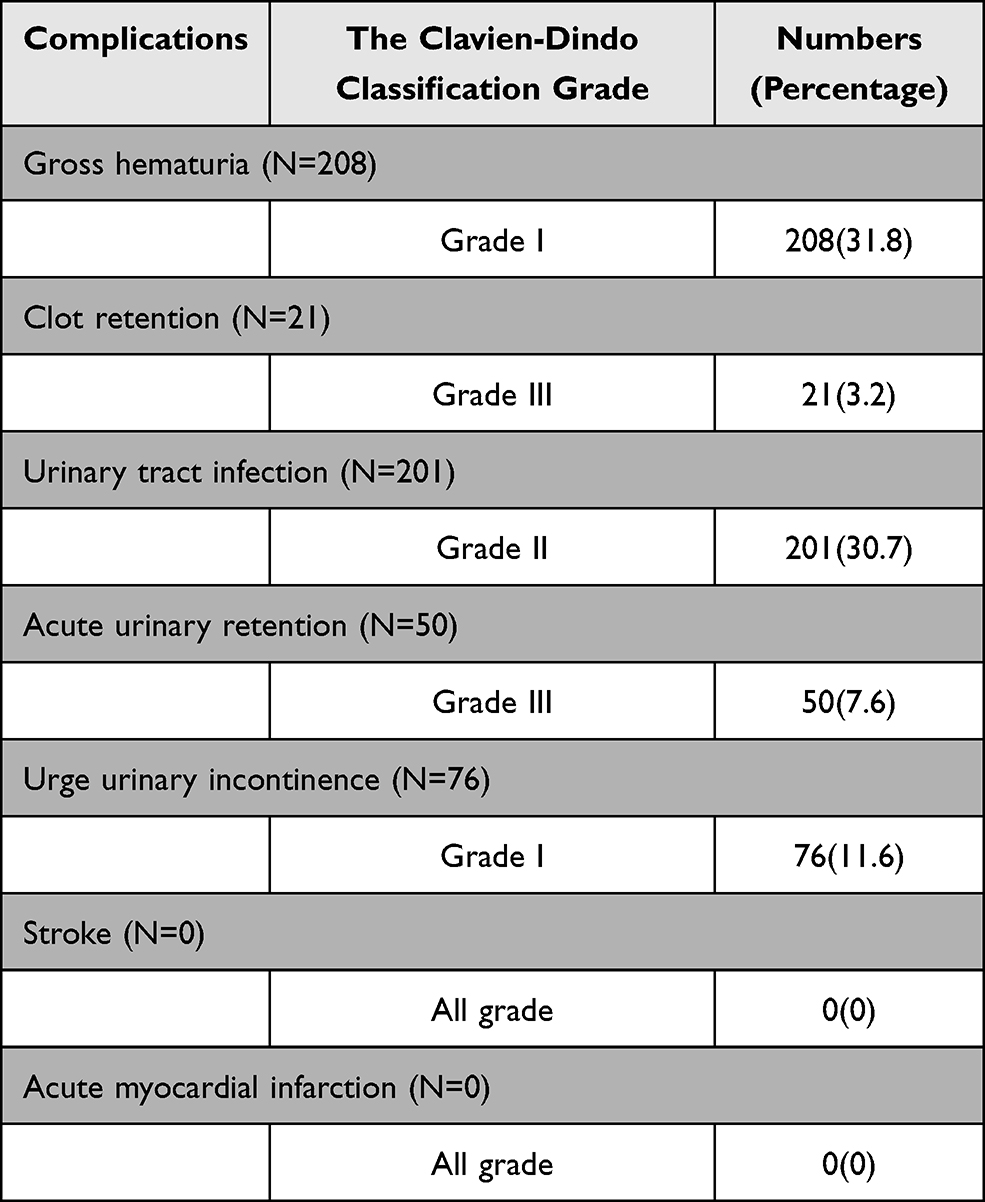 |
Table 4 Early Postoperative Complications Within 30-Day |
Discussion
To our knowledge, this is the first study to compare five transurethral procedures performed in the treatment of BPH/LUTS and investigate postoperative bleeding associated with ER visits. Our study results indicate that the need for two or more rounds of manual irrigation during the hospital stay is a potential indicator of clot retention within 3 months following operation. No previous study has reported on this topic. A possible explanation for this finding is that the first round of manual irrigation may be related to residual blood clots or small prostate fragments after the operation instead of active bleeding events; thus, a single round of manual irrigation is sufficient. However, the need for additional manual irrigation may be an indicator of active bleeding and is a potential risk factor for postoperative bleeding–related ER visits. The results indicate that a second look surgery with transurethral procedure to check bleeding is optimal treatment rather than manual or continuous irrigation only for a patient requiring multiple postoperative manual irrigation for blood clots retention.
Notably, the multivariable logistic regression and subgroup analysis in our study indicated that postoperative clot retention–related ER visits occurred more frequently among patients who received ThuVARP than among those who received B-TURP. This may be attributable to the exposure of some uncoagulated microvascular during visual resection of prostatic tissue, which may lead to further clot retention–related ER visits. The findings of a randomized prospective trial conducted in China by Xia et al13 and the European Association of Urology guidelines on laser technologies10 indicate that ThuVARP has shorter catheterization and hospitalization times and lower transfusion rates than those of TURP. However, a randomized controlled trial conducted in the United Kingdom did not corroborate these findings of shorter hospital stays and lower rates of postoperative hemorrhage among patients undergoing ThuVARP compared with among those undergoing TURP, and ThuVARP was reported to be inferior in terms of maximum urinary flow rate.14 Our results indicate that ThuVARP has a higher bleeding risk, which warrants further study.
Early postoperative bleeding is considered to occur within one month after surgery.15 In a pilot study of TURP by Olapade-Olaopa et al, at the end of the first, second, third, and fourth weeks, gross hematuria stopped in 47%, 73%, 96%, and 97% of patients, respectively.16 However, in a study on the healing response of the prostatic urethra following TURP, complete wound sealing and re-epithelialization was not observed within the first three months postoperatively.17 Additionally, a population-based cohort study conducted in Canada by Shamout et al reported that 15.4% of patients visited the ER with gross hematuria within 90 days after TURP.18 In our study, the number of ER visits related to gross hematuria stabilized in the third month, and the number of patients with clot retention stabilized in the second month during six months of postoperative follow-up. The incidence of postoperative bleeding–related ER visits was lower in the present study than in other studies, which may be related to longer hospital stays in Taiwan compared with in western countries.
Delayed hematuria following PVP during an average follow-up of 33 months was reported by Jackson et al. They suggested anticoagulation, larger prostate size and longer follow-up were associated with delayed gross hematuria. On the other hand, the use of 5-ARI and older age were protective factor.19 In our study, we did not see the difference in those parameters between bleeding–related ER visits or not within 3 months. A long-term follow-up after five transurethral procedures is needed.
Following TURP, 5-ARI was considered a suitable preventor of postoperative bleeding. In a randomized controlled study conducted by Ozdal et al, a 4-week prescription of finasteride used before TURP reduced perioperative bleeding.20 In a prospective, randomized, double-blind placebo-controlled trial conducted by Bansal and Arora, 4-week administration of 5-ARIs prior to the operation was associated with lower rates of perioperative bleeding for TURP, indicating that it may reduce the risk of perioperative bleeding complications.21 By contrast, a population-based cohort study indicated that the use of 5-ARIs before TURP was not related to rates of postoperative blood transfusion, clot retention, or subsequent ER visits.22 In our study, 5-ARIs did not affect the rate of postoperative bleeding–related ER visits. It can be reasoned that our study included the patients used of 5‑ARIs within 4 weeks.
The relationship between PAIs and postoperative bleeding was studied by Yee et al, who reported that ceasing consumption of PAIs 5 days before operation was associated with early postoperative bleeding.23 However, a European single-center study revealed that B-TURPs can be performed under ongoing administration of PAIs with acetylsalicylic acid and do not increase the risk of bleeding complications. However, ongoing intake of clopidogrel may increase the risks of bleeding complications and need for blood transfusions.24 We did not distinguish between acetylsalicylic acid and clopidogrel groups in our study. In addition, we routinely cease patients’ PAI intake 7 days before operation. No significant difference in rate of postoperative bleeding–related ER visits was noted between patients who used PAIs and those who did not.
A single-center study proposed that age and comorbidities should be considered indicators of the likelihood of postoperative ER visits,25 and a population-based cohort study offered similar conclusions.18 However, these studies assessed patients with ER visits related to all types of complications and urgent surgery. In our study, age and comorbidities were not determined to be indicators of the likelihood of postoperative bleeding–related ER visits following elective transurethral procedures.
Strengths and Limitations
A key strength of our study is that we enrolled all patients who underwent elective surgery, with approximately 10% repeated surgery, which is reflective of general clinical practice. We also compared five transurethral procedures in a single center, which potentially reduced the systemic bias between centers.
This study had some limitations. First, this was a retrospective study with a relatively small sample size. Second, urological and cost-effective outcomes were not evaluated. A third potential limitation is the diverse experience of the surgeons performing the different methods evaluated. Further studies with larger sample sizes and a randomized controlled design are necessary to confirm our findings.
Conclusion
Multiple manual irrigations shortly after operations can be considered a novel predictor for postoperative clot retention–related ER visits and is an indicator for a second look surgery with transurethral procedure to check bleeding. Among the transurethral procedures, compared with B-TURP, ThuVARP was associated with a higher risk of clot retention–related ER visits.
Ethical Approval
This research was approved by the Chang Gung Medical Foundation Institutional Review Board. Informed consent was waived due to the retrospective study design. This study has been conducted in accordance with the ethical principles mentioned in the Declaration of Helsinski (2013).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Egan KB. The epidemiology of benign prostatic hyperplasia associated with lower urinary tract symptoms: prevalence and incident rates. Urol Clin North Am. 2016;43(3):289–297.
2. Teo JS, Lee YM, Ho HSS. An update on transurethral surgery for benign prostatic obstruction. Asian J Urol. 2017;4(3):195–198.
3. Cornu JN, Ahyai S, Bachmann A, et al. A systematic review and meta-analysis of functional outcomes and complications following transurethral procedures for lower urinary tract symptoms resulting from benign prostatic obstruction: an update. Eur Urol. 2015;67(6):1066–1096.
4. Mayer EK, Kroeze SG, Chopra S, Bottle A, Patel A. Examining the ‘gold standard’: a comparative critical analysis of three consecutive decades of monopolar transurethral resection of the prostate (TURP) outcomes. BJU Int. 2012;110(11):1595–1601.
5. Ahyai SA, Gilling P, Kaplan SA, et al. Meta-analysis of functional outcomes and complications following transurethral procedures for lower urinary tract symptoms resulting from benign prostatic enlargement. Eur Urol. 2010;58(3):384–397.
6. Issa MM. Technological advances in transurethral resection of the prostate: bipolar versus monopolar TURP. J Endourol. 2008;22(8):1587–1595.
7. Nair SM, Pimentel MA, Gilling PJ. A review of laser treatment for symptomatic BPH (Benign Prostatic Hyperplasia). Curr Urol Rep. 2016;17(6):45.
8. Olcese SP, Derosa R, Kern SQ, Lustik MB, Sterbis JR, McMann LP. Comparison of outcomes after TURP versus photoselective vaporization of the prostate with respect to trainee involvement utilizing ACS NSQIP. Prostate Cancer Prostatic Dis. 2014;17(3):227–232.
9. Bozzini G, Seveso M, Melegari S, et al. Thulium laser enucleation (ThuLEP) versus transurethral resection of the prostate in saline (TURis): a randomized prospective trial to compare intra and early postoperative outcomes. Actas Urológicas Españolas. 2017;41(5):309–315.
10. Herrmann TR, Liatsikos EN, Nagele U, Traxer O, Merseburger AS. Eau Guidelines Panel on Lasers T. EAU guidelines on laser technologies. Eur Urol. 2012;61(4):783–795.
11. Zorn KC, Liberman D. GreenLight 180W XPS photovaporization of the prostate: how I do it. Can J Urol. 2011;18(5):5918–5926.
12. Herrmann TR, Bach T, Imkamp F, et al. Thulium laser enucleation of the prostate (ThuLEP): transurethral anatomical prostatectomy with laser support. Introduction of a novel technique for the treatment of benign prostatic obstruction. World J Urol. 2010;28(1):45–51.
13. Xia SJ, Zhuo J, Sun XW, Han BM, Shao Y, Zhang YN. Thulium laser versus standard transurethral resection of the prostate: a randomized prospective trial. Eur Urol. 2008;53(2):382–389.
14. Hashim H, Worthington J, Abrams P, et al. Thulium laser transurethral vaporesection of the prostate versus transurethral resection of the prostate for men with lower urinary tract symptoms or urinary retention (UNBLOCS): a randomised controlled trial. Lancet. 2020;396(10243):50–61.
15. Cornu JN, Herrmann T, Traxer O, Matlaga B. Prevention and management following complications from endourology procedures. Eur Urol Focus. 2016;2(1):49–59.
16. Olapade-Olaopa EO, Solomon LZ, Carter CJ, Ahiaku EK, Chiverton SG. Haematuria and clot retention after transurethral resection of the prostate: a pilot study. Br J Urol. 1998;82(5):624–627.
17. Orihuela E, Pow-Sang M, Motamedi M, Cowan DF, Warren MM. Mechanism of healing of the human prostatic urethra following thermal injury. Urology. 1996;48(4):600–608.
18. Shamout S, Carlson K, Brotherhood HL, Crump T, Baverstock R. Incidence and predictors of early and late hospital readmission after transurethral resection of the prostate: a population-based cohort study. BJU Int. 2020;127:238–246.
19. Jackson RE, Casanova NF, Wallner LP, et al. Risk factors for delayed hematuria following photoselective vaporization of the prostate. J Urol. 2013;190(3):903–908.
20. Ozdal OL, Ozden C, Benli K, Gokkaya S, Bulut S, Memis A. Effect of short-term finasteride therapy on peroperative bleeding in patients who were candidates for transurethral resection of the prostate (TUR-P): a randomized controlled study. Prostate Cancer Prostatic Dis. 2005;8(3):215–218.
21. Bansal A, Arora A. Transurethral resection of prostate and bleeding: a prospective, randomized, double-blind placebo-controlled trial to see the efficacy of short-term use of finasteride and dutasteride on operative blood loss and prostatic microvessel density. J Endourol. 2017;31(9):910–917.
22. Yang TY, Chen M, Lin WR, et al. Preoperative treatment with 5alpha-reductase inhibitors and the risk of hemorrhagic events in patients undergoing transurethral resection of the prostate - A population-based cohort study. Clinics. 2018;73:e264.
23. Yee CH, Wong JH, Chiu PK, et al. Secondary hemorrhage after bipolar transurethral resection and vaporization of prostate. Urol Ann. 2016;8(4):458–463.
24. Ruhle A, Blarer J, Oehme F, et al. Safety and effectiveness of bipolar transurethral resection of the prostate in patients under ongoing oral anticoagulation with coumarins or antiplatelet drug therapy compared to patients without anticoagulation/antiplatelet therapy. J Endourol. 2019;33(6):455–462.
25. Palmisano F, Boeri L, Fontana M, et al. Incidence and predictors of readmission within 30 days of transurethral resection of the prostate: a single center European experience. Sci Rep. 2018;8(1):6575.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.