Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 12
Risk Factors of Anomalous Cord Insertion Among Singleton Births at the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia: An Institution-Based Cross-Sectional Study
Authors Aragie H ![]() , Asmare Y
, Asmare Y ![]() , Tenaw B
, Tenaw B
Received 11 February 2021
Accepted for publication 8 April 2021
Published 28 April 2021 Volume 2021:12 Pages 205—212
DOI https://doi.org/10.2147/PHMT.S306054
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Roosy Aulakh
Hailu Aragie, Yared Asmare, Bahiru Tenaw
Department of Human Anatomy, School of Medicine, College of Medicine and Health Science, University of Gondar, Gondar, Ethiopia
Correspondence: Hailu Aragie
Department of Human Anatomy, School of Medicine, College of Medicine and Health Science, University of Gondar, PO. Box 196, Gondar, Ethiopia
Email [email protected]
Introduction: Anomalous cord insertion causes bad pregnancy outcomes. Therefore, knowledge on the prevalence and risk factors of anomalous cord insertion will reinforce the prenatal care by health providers in addressing the adverse outcome caused by this abnormality.
Methods and Materials: An institution-based cross-sectional study design was conducted among 421 singleton births at the University of Gondar comprehensive specialized hospital. A systematic random sampling technique was used to select study participants. Data were collected by using a structured questionnaire and checklist and was entered into epi-data version 3.1 and then exported to SPSS version 20 for data cleansing and analysis. Bi-variable and multivariable logistic regression was employed to identify factors associated with anomalous cord insertions. Crude and adjusted odds ratio with a 95% confidence interval was calculated to identify the independent risk factors for anomalous cord insertions.
Results: The prevalence of anomalous cord insertion was 9.0% in singleton pregnancies. Independent risk factors for ACI were advanced maternal age (AOR= 4.77), primiparity (AOR=3.87), maternal chronic hypertension (AOR=3.23), previous caesarian delivery (AOR=3.28), and use of IUCD before pregnancy (AOR=3.91).
Conclusion: Anomalous cord insertion was reported in approximately one-tenth of singleton deliveries in the representative Ethiopian population. Advanced age, primiparity, hypertensive disorder, history of caesarian section, and IUCD usage before pregnancy were associated with increased risk of anomalous cord insertion.
Keywords: prevalence, anomalous cord insertion, singleton births, Gondar, Ethiopia
Introduction
Most of the time, umbilical cord inserts into the central portion of the placenta, well away from the placental edge, ie central insertion or eccentric insertion (insertion of the umbilical cord between the center and 2 cm away from the placental disc edge).1 However, sometimes the umbilical cord may insert within 2 cm from the placental edge, which is considered as marginal cord insertion2 or to the chorioamniotic membranes of the placenta rather than on to the placental mass.3 The last two types are grouped into anomalous cord insertion.
The reason for variations in the site of insertion of the umbilical cord is not well understood. But it is thought to be resulted from a process known as trophotrophism1 in which the chorionic frondosum or the early placenta “migrates” with advancing gestation to ensure a better blood supply from a more richly vascularized area.
The prevalence of anomalous cord insertion is 8.1%.4 This anomaly causes different adverse pregnancy and perinatal outcomes. Intrauterine growth retardation, preterm labor, low birth weight, growth retardation, low APGAR scores, abnormal fetal heart patterns and congenital anomalies like esophageal atresia, obstructive uropathies, congenital hip dislocations, asymmetrical head shape, and spina bifida are some of the complications of anomalous cord insertion.4,5
Even though the burden of anomalous cord insertion is high to this end, there is a clear gap in measuring the prevalence and identifying the risks which lead to ACI in Ethiopia. For this reason, this study aims to measure the magnitude of the problem (prevalence of anomalous cord insertion) and to state the possible predisposing factors that lead to anomalous cord insertion in the University of Gondar comprehensive specialized hospital, northwest Ethiopia.
Methods and Materials
Study Setting
The study was conducted at the University of Gondar Comprehensive Specialized Hospital (UOGCSH), maternity and neonatal ward. This hospital serves a population of seven million across the Amhara region, and averages of 10,140 mothers give birth per year.
Study Design and Period
The institution-based cross-sectional study design was conducted from February 2020 to April 2020.
Population
All singleton births at the University of Gondar comprehensive specialized hospital in the maternity and neonatal ward are the source population, and the study population is all singleton births that met the inclusion criteria within the study period at the UOGCSH maternity and neonatal ward.
Inclusive and Exclusive Criteria
All singleton births were included. Placenta specimens without intact umbilical cord and with externally identifiable pathology, Bifurcated umbilical cord before its insertion, and seriously ill mothers if unable to communicate were excluded.
Sample Size Determination and Sampling Procedure
The sample size was estimated using a single population proportion formula that took into account the following factors: population proportion, p =0.5, a margin of error, d =0.05, and 95% confidence interval. With a 10% non-response rate, the final sample size was estimated to be 422.
The study participants were chosen using a systematic random sampling technique. Six months prior to the data collection period, the client registration book was checked, and the total number of deliveries during the data collection time was calculated (1690 deliveries per two months) The number of units in the population (N) was divided by the optimal sample size to decide the sampling interval (K) (n). N=1690, n=422, k=1690/422= 4. K=N/n, N=1690, n=422, k=1690/422= 4. Starting with the randomly selected (4th) newly born eligible mothers’ placentas and umbilical cords, every 4th mother placenta with the attached umbilical cord was enrolled in the study, proportional to the unit participant numbers (size).
Variables of the Study
Dependent Variable
Anomalous cord insertion (Absence: Central, Eccentric, Presence: velamentous and/or marginal).
Independent Variables
Sociodemographic characteristics: maternal age, residence, income, educational level, marital status.
Obstetrical and pregnancy-related factors: parity, prior termination, infertility, previous caesarian delivery, placenta praevia, vaginal bleeding, previous miscarriage, a female fetus.
Drugs and medicine-related factors: use of IUCD before current pregnancy, smoking cigarette, folic acid supplementation, consumption of alcohol.
Data Collection Procedure and Tools
When the mother gave birth to the placenta in the maternity and neonatal ward, fresh specimens that met the inclusion requirements were collected immediately. The umbilical cord’s course and insertion site were then carefully noted by the data collectors. The distance between the placental edge and the insertion site of the umbilical cord was also measured. A standardized questionnaire and checklist were used to collect information about the mother and the pregnancy. The data collection questionnaire and checklist were written in English first, then translated into Amharic and back to English.
Data Quality Control and Management
Data collecting checklists adapted from various works of literature and updated according to our study objectives were reviewed for clarification, understandability, uniformity, and completeness prior to data collection to ensure data quality. The aims, method of data collection, and standard operating procedure were discussed to data collectors (two BSc. Midwives from the University of Gondar comprehensive specialized hospital) and a supervisor (one MSC midwife lecturer from Gondar University) over the course of two days. At Dembia Primary Hospital, a pretest was conducted on 5% of the sample size before the actual data collection period. Based on the pretest outcome, necessary changes, significant amendments, and a logical flow of ideas were retained. Near supervision was provided by qualified supervisors every day and by the principal investigator every other day. All necessary feedback was offered to data collectors the next morning before data collection and the quality of equipment was also checked to ensure accuracy.
Data Processing and Analysis
The data were manually reviewed for completeness, coded, and entered into Epi Data version 3.1 statistical packages, after which it was exported to SPSS Version 20 for further cleaning and analysis. Inconsistent values were double-checked and corrected as required against the filled data extract format. The effects of categorical variables were represented using frequency, percentage, graphs, and pie charts, while continuous variables were represented using means and standard deviations. The frequency or percentage of study participants was calculated using cross-tabulation. The relationship of independent variables with the dependent variable was determined using bivariate and multivariate logistic regression analyses. By controlling confounders, variables with P-value<0.2 in bivariate analysis were entered into a multivariate logistic regression model to classify the relevant determinants. To determine the existence and strength of associations, odds ratios with 95% confidence were calculated, and statistical significance was declared if P-value<0.05. The Hosmer–Lemeshow goodness-of-fit test was used to validate the final model.
Ethical Considerations
The ethical review committee of the University of Gondar’s School of Medicine, College of Medicine and Health Sciences (Ref. No 1879/02/2020) gave its approval. UOGCSH’s Gynecology and Obstetrics Department got an official note. Finally, after receiving approval from the Maternity and Neonatal Ward supervisor, the mothers from whom the specimens were collected were told about the study’s intent and benefits, as well as the protocol and their right to refuse. Furthermore, the research participants were told that confidentiality would be upheld, and each mother’s informed written consent was obtained at the time of data collection. The University of Gondar Ethical Review Committee also approved participants under the age of 18 years to provide informed consent on their behalf, and the informed consent included the publication of anonymized responses. We can confirm that all procedures were carried out in accordance with the Declaration of Helsinki.
Result
Statistical Descriptions of Socio-Demographic Factors
A total of 421 mothers took part in the study, with a 99.76% response rate. Respondent mothers in this study ranged in age from 16 to 45 years old, with a mean of 27 years and SD of 6.19. The mothers were mostly from urban areas, with 368 (87.4%) hailing from the city and 53 (12.6%) hailing from the countryside. Eighty-nine percent of the respondents were married, and the mothers’ predominant faith was orthodox Christianity. Approximately 10.9% of the respondents were illiterate, while 210 (49.9%) had a diploma or higher. Eighty percent of the mothers who replied were either government employees or stay-at-home moms (Table 1).
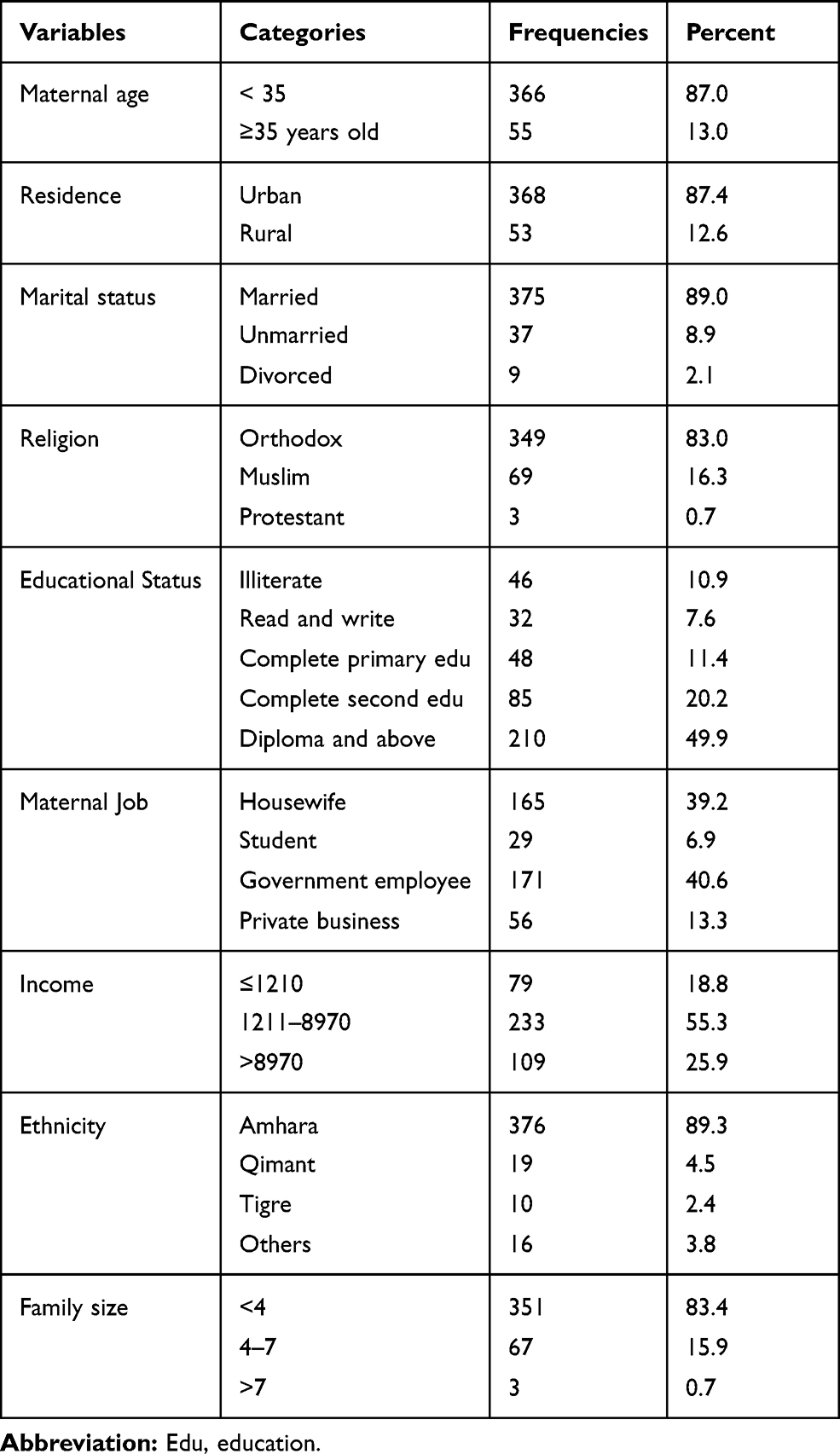 |
Table 1 Descriptive Statistics of Socio-Demographic Characteristics of Mothers in the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia, 2020 |
Statistical Descriptions of Factors Related to ACI
108 (25.7%) of the study participants were primiparous, as shown in Table 2. Thirty-one (9.9%) of the multiparous women had at least one caesarian section delivery. About a quarter of the respondents (13%) had experienced a miscarriage or stillbirth. Fertility-related problems were recorded by 32 (7.6%) of mothers. In this study, approximately 7.8% and 4.0% of the participants had vaginal bleedings and placenta praevia, respectively, during pregnancy. Among all the participants, about half of the mothers had a female fetus, and just 0.5% of the umbilical cords had a single artery.
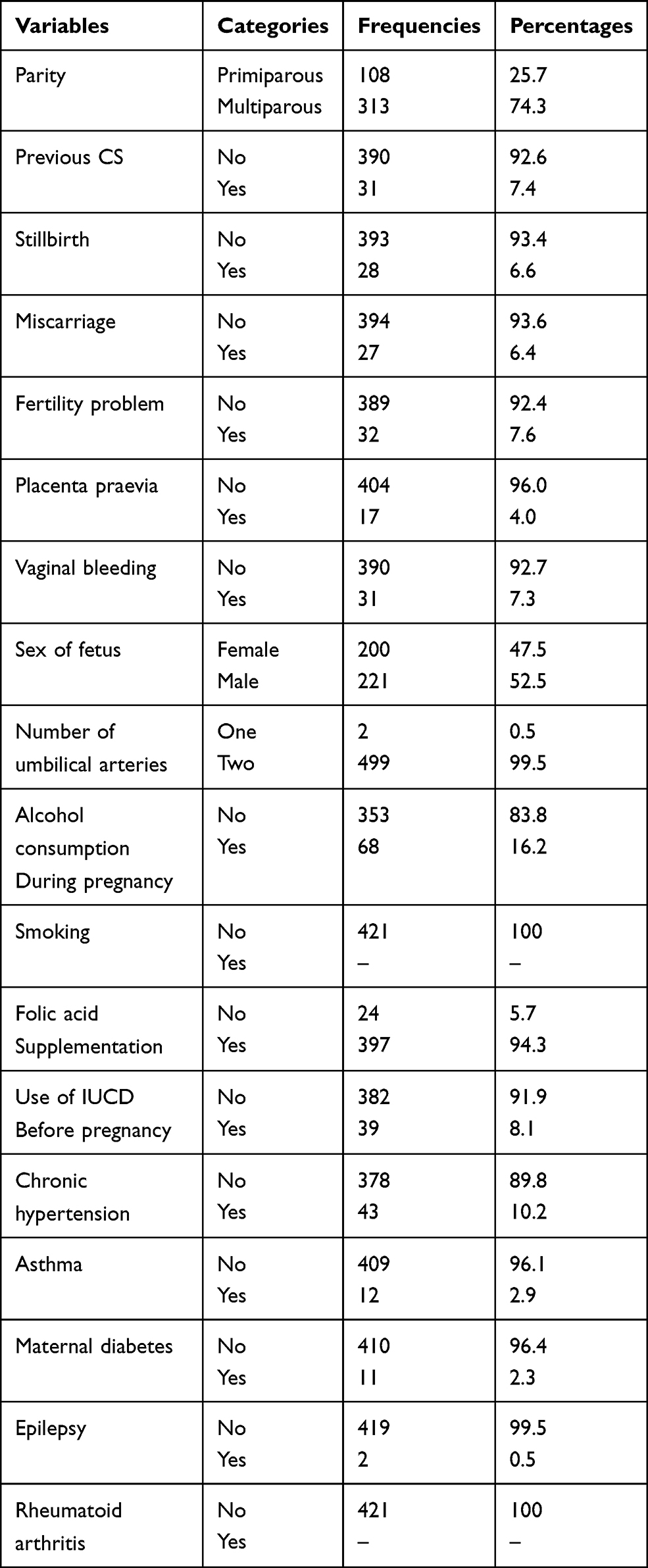 |
Table 2 Descriptive Statistics of Pregnancy and Obstetrical Characteristics of Mothers in the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia, 2020 |
According to Table 2, 68 (16.2%) of mothers had a history of alcohol use during and before pregnancy, but no mother had a history of smoking during and before pregnancy. 397 (94.3%) of all respondent mothers took folic acid supplements during pregnancy, and 34 (8.1%) of the women had a history of IUCD use.
Table 2 also displays descriptive figures for chronic diseases that affect mothers. According to the results, 43 (10.2%) of the participants were hypertensive, while 12 (2.9%), 11 (2.3%), and 2 (0.5%) were asthmatic, diabetic, and epileptic patients, respectively.
Prevalence of ACI
With a 95% confidence interval of 9.0%, the prevalence of anomalous placental cord insertion was 9.0% (6.4–12.0). Furthermore, 91.0% of placentas had regular cord insertion, with 51.3% eccentric and 39.7% central.
Risk Factors Associated with ACI
Advanced maternal age, primiparity, previous caesarian section, use of IUCD before pregnancy, maternal chronic hypertension, placenta praevia, and vaginal bleeding during pregnancy were reported variables for multivariable analysis with a P-value less than 0.2 for anomalous cord insertion in the binary logistic regression analysis (Table 3).
 |
Table 3 Result of Bivariate and Multivariate Logistic Regression for Risks Associated with ACI in the University of Gondar Comprehensive Specialized Hospital, Northwest Ethiopia, 2020 |
Advanced maternal age, previous caesarian section, use of IUCD before birth, maternal chronic hypertension, and primiparity were variables that showed statistically significant association with ACI in multivariable logistic regression analysis.
Therefore, in comparison to their counterparts, primiparous mothers were 3.87 times more likely to have ACI (AOR = 3.87 95% CI=1.77–8.69). ACI was 4.77 times more likely in placentas delivered by mothers over 35 (AOR=4.77, 955 CI=2.05–11.08) than in placentas delivered by mothers under 35 (AOR=4.77, 955 CI=2.05–11.08). A mother who had previously had a caesarian section had a 3.28-fold increased chance of developing ACI.
Women with chronic hypertension had a 3.23 times higher chance of developing anomalous cord insertion than their counterparts (AOR= 3.23, 95% CI = 1.24–8.38). Furthermore, mothers who used IUCD before pregnancy (AOR=3.91, 95% CI =1.36–11.21) were four times more likely than mothers who did not use IUCD to have an ACI (Table 3).
Discussion
The overall prevalence of ACI was found to be 9% (95% CI=0.6.4–12.0) in the current report. This prevalence is consistent with studies conducted in Norway (7.8%) and India (8.9%), (8%t).6–8 But this prevalence was lower than studies in the USA (20.3%) and India (16.45%).4,9 The disparity in ACI prevalence between the current research and the American study is most likely due to methodological variations. Because the American study used sonographic evaluation to assess the outcome, there may have been a false-negative sonogram, placental remodeling, or technical error, resulting in a high prevalence of ACI.9 This might also be due to the absence of multiple gestations and assisted reproductive technology user respondents in our study population.8 Since the Indian study did not use standard outcome measurement parameters, the higher ACI prevalence in the Indian study compared to the current study may be attributed. In contrast, the current study found a higher prevalence of ACI than a study conducted in India (2.0%).10 It is likely that the higher prevalence in the current study compared to the Indian study is due to a disparity in the study participants’ range. The Indian research excluded mothers with chronic illnesses, which may raise the risk of ACI.8 The Indian research, on the other hand, did not involve fetal abnormalities, which may have arisen as a result of ACI.11
We found a statistically important strong positive correlation between maternal age and anomalous cord insertion in the current research. As a result, mothers over 35 years of age may face a nearly five-fold increase in the risk of ACI (Table 3). Interestingly, our findings are backed up by a report performed elsewhere.8 Uterine hypoxia is most likely the cause of ACI in mothers in their forties and fifties (≥35). Since uterine hypoxia is a common phenomenon among mothers in their forties and fifties,12 Trophotropism (the migration of early placental cells from one part of the uterus to another in search of nutrition) is induced, resulting in abnormal cord insertion.
Like other studies done in Norway and Finland,8,13 Primiparity was found to be an important predictor of ACI in our research. As a result, first pregnancies were more likely to result in ACI. Since numerous studies have shown a direct connection between placenta praevia and ACI,13,14 the higher risk of ACI in primiparity relative to multiparity may be explained by the higher occurrence of placenta praevia in primiparity.15 Placenta praevia was found to be present in 7.4% of primiparous women and 2.8% of multiparous women in our research. In this study, placentas delivered by mothers with chronic hypertension had a 3.23 times higher risk of developing ACI than placentas delivered by mothers without chronic hypertension. This finding is consistent with previous research from Israel and Norway.8,15 Jain A. and collaborators stated a strong association between anomalous cord insertion and altered placental shape.16 Since chronic hypertension caused altered placental shape as a result of repeated branching of uteroplacental vascular trees17 our finding of a connection between chronic hypertension and ACI is indirectly supported.
According to the findings of our study, mothers who had previously had a caesarian section had a threefold increased risk of developing ACI compared to mothers who had never had a caesarian section (Table 3). Studies in the Norwegian population found a connection between previous caesarian section delivery experience and ACI.8 This is most likely due to abnormal placentation, which is linked to uterine scarring from previous caesarian sections.18 In our study, we identified that using IUCD before conception increases the mother’s risk of developing ACI by four times as compared to control mothers. The use of IUCD has been related to a progressive thinning of the endometrium in some studies.19 Where the endometrium is not well regenerated, conception of a thin endometrium can result in asymmetrical placental development from the point of cord insertion, with the placenta being less grown.20
Strength and Limitations of the Study
The research is the first of its kind in the study region, as well as Ethiopia. And, as far as we know, the occurrence and risk factors of anomalous cord insertion in Africa have not been investigated. Under the close supervision of the principal investigator, direct measurement of the umbilical cord insertion site was performed to the nearest decimal and reported by well-trained data collectors. There are two drawbacks to this analysis. There are two drawbacks to this analysis. The first is that, due to a lack of evidence, the study did not take into account some possible risk factors, such as preconception BMI and previous pregnancy cord insertion type. The study’s second drawback is that, since it was performed in health facilities, the findings might not apply to the whole population.
Conclusion
The current hospital-based cross-sectional study’s prevalence and most of the risk factors are consistent with previous research. Primiparous women, advanced in age, have chronic hypertension, have used IUCD before birth, or have a mother who has had a prior caesarian section delivery are all at high risk of developing ACI. During antenatal care, prenatal detection of ACI should be done on a regular basis, particularly for those pregnancies with a high risk of cord insertion anomaly. Health professionals should receive relevant training, especially to improve their knowledge of the ACI risk community. Pregnancy and obstetrical history, including the form of cord insertion, must be accurately documented from conception to delivery.
Abbreviations
ACI, anomalous cord insertion; CI, cord insertion; IUCD, intrauterine contraceptive device; ORD, odds ratio; UoGCSH, University of Gondar comprehensive specialized hospital; VCI, velamentous cord insertion.
Data Sharing Statements
All data and materials of this study are available and can be accessed with a reasonable request from the corresponding author with the email address of “[email protected]”.
Acknowledgments
Our heartfelt thanks goes to the University of Gondar for funding this research. The authors are also thankful to all data collectors, supervisors, and study participants for their co-operation during data collection.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they do not have any conflict of interest for this work.
References
1. Robinson LK, Jones KL, Benirschke K. The nature of structural defects associated with velamentous and marginal insertion of the umbilical cord. Am J Obstet Gynecol. 1983;146(2):191–193. doi:10.1016/0002-9378(83)91052-9
2. Pretorius DH, Chau C, Poeltler DM, Mendoza A, Catanzarite VA, Hollenbach KA. Placental cord insertion visualization with prenatal ultrasonography. J Ultrasound Med. 1996;15(8):585–593. doi:10.7863/jum.1996.15.8.585
3. Bjøro K
4. Reddy VM, Geetha SP, Nim VK. Variations in placental attachment of umbilical cord. J Anat Soc India. 2012;61(1):1–4. doi:10.1016/S0003-2778(12)80002-5
5. Bjøro K
6. Jeyasingh T, Vimala V. Variations in the placental attachment of umbilical cord and its embryological significance. J Dent Med Sci. 2016;15(3):101–103.
7. Shrivastava S. Variation of human placental attachment of umbilical cord. Int J Sci Stud. 2018;6(1):17–20.
8. Ebbing C, Kiserud T, Johnsen SL, Albrechtsen S, Rasmussen S, Sahasrabuddhe V. Prevalence, risk factors and outcomes of velamentous and marginal cord insertions: a population-based study of 634,741 pregnancies. PLoS One. 2013;8(7):e70380. doi:10.1371/journal.pone.0070380
9. Salvo D, Benson C, Laing F, Brown D, Frates M, Doubilet P. Sonographic evaluation of the placental cord insertion site. AJR Am J Roentgenol. 1998;170:1295–1298. doi:10.2214/ajr.170.5.9574605
10. Gupta A, Musharaf S, Singh G, Gupta A. Morphological changes in placenta in cases of oligohydramnios. Int J Reprod Contracept Obstet Gynecol. 2018;7(4):1519. doi:10.18203/2320-1770.ijrcog20181347
11. Ismail KI, Hannigan A, Kelehan P, O’Donoghue K, Cotter A. Abnormal placental cord insertion and adverse pregnancy outcomes: results from a prospective cohort study. Am J Perinatol. 2017;34(11):1152–1159. doi:10.1055/s-0037-1604413
12. Torous VF, Roberts DJ. Placentas from women of advanced maternal age. Arch Pathol Lab Med. 2019.
13. Räisänen S, Georgiadis L, Harju M, Keski-Nisula L, Heinonen S. Risk factors and adverse pregnancy outcomes among births affected by velamentous umbilical cord insertion: a retrospective population-based register study. Eur J Obstet Gynecol Reprod Biol. 2012;165(2):231–234. doi:10.1016/j.ejogrb.2012.08.021
14. Li X-Y, Yu Y, Wu -Q-Q. Risk factors and perinatal outcomes of velamentous umbilical cord insertion. Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2015;37(3):355–357. doi:10.3881/j.issn.1000-503X.2015.03.022
15. Gutvirtz G, Baumfeld Y, Shoham I, Sheiner E. Risk factors, complications and outcomes of pregnancies with velamentous cord insertion. Harefuah. 2016;155(2):94–7, 132.
16. Jain A, Jain R, Baweja S. Variable placental attachment of umbilical cords and its effects on placental outcomes. Indian J Clin Anat Physiol. 2017;4(3):324–328.
17. Yampolsky M, Salafia CM, Shlakhter O, Haas D, Eucker B, Thorp J. Modeling the variability of shapes of a human placenta. Placenta. 2008;29(9):790–797. doi:10.1016/j.placenta.2008.06.005
18. Lydon-Rochelle M, Holt VL, Easterling TR, Martin DP. First-birth cesarean and placental abruption or previa at second birth(1). Obstet Gynecol. 2001;97(5 Pt 1):765–769. doi:10.1097/00006250-200105000-00023
19. Serfaty D., Yaneva H. The endometrium and the IUD. Femal Contracept. 1988;1(11):325–335.
20. Ozgur K, Bulut H, Berkkanoglu M, Basegmez FO, Coetzee K. six-months recovery needed after dilation and curettage (D & C) for reproductive outcomes in frozen embryo transfer. J Obstet Gynaecol. 2018;38:1150–1157. doi:10.1080/01443615.2018.1460335
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.