Back to Journals » Journal of Blood Medicine » Volume 17
Risk Factors for Post-Operative Blood Transfusion and Association with Outcomes in Hip Fracture Surgery
Authors Al-Husinat L, Haddad F, Al Sharie S ![]() , Araydah M, Al Hseinat L
, Araydah M, Al Hseinat L ![]() , Kharashgah M, Alsharei A, AL Modanat Z, Alisi MS
, Kharashgah M, Alsharei A, AL Modanat Z, Alisi MS ![]() , Al-Ajlouni J
, Al-Ajlouni J ![]() , Dawod MS
, Dawod MS ![]() , De Rosa S, Battaglini D
, De Rosa S, Battaglini D
Received 18 June 2025
Accepted for publication 8 January 2026
Published 13 January 2026 Volume 2026:17 547898
DOI https://doi.org/10.2147/JBM.S547898
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Chang Kim
Lou’i Al-Husinat,1 Fadi Haddad,2 Sarah Al Sharie,3 Mohammad Araydah,4 Laith Al Hseinat,5 Mohamad Kharashgah,1 Adel Alsharei,1 Zaid AL Modanat,1 Mohammed S Alisi,6 Jihad Al-Ajlouni,7 Mohd Said Dawod,8 Silvia De Rosa,9,10,* Denise Battaglini11,12,*
1Department of General Surgery and Anesthesia, Faculty of Medicine, Yarmouk University, Irbid, Jordan; 2Department of Internal Medicine, Trinity Health Oakland, Pontiac, MI, USA; 3Office of Scientific Affairs and Research, King Hussein Cancer Center, Amman, Jordan; 4Department of Internal Medicine, Istishari Hospital, Amman, Jordan; 5Department of Orthopaedics, Royal Medical Services, Amman, Jordan; 6Faculty of Medicine, Islamic University of Gaza, Gaza, Palestine; 7Department of Orthopedic Surgery, School of Medicine, University of Jordan, Amman, Jordan; 8Department of Special Surgery, College of Medicine, Mutah University, Al-Karak, Jordan; 9Centre for Medical Sciences - Cismed, University of Trento, Trento, Italy; 10Anesthesia and Intensive Care, Santa Chiara Regional Hospital, APSS, Trento, Italy; 11Department of Surgical Sciences and Integrated Diagnostics (DISC), University of Genova, Genova, Italy; 12Anesthesia and Intensive Care, IRCCS Ospedale Policlinico San Martino, Genova, Italy
*These authors contributed equally to this work
Correspondence: Lou’i Al-Husinat, Department of General Surgery and Anesthesia, Faculty of Medicine, Yarmouk University, Irbid, Jordan, Email [email protected]
Background: Blood transfusion during hip fracture surgery can significantly influence patient outcomes. This study aimed to identify risk factors for post-operative blood transfusions and their impact on clinical outcomes, including all-cause mortality.
Methods: A post-hoc analysis was conducted on data from a multicentric observational study in Jordan. Demographics, preoperative variables, intraoperative details, and postoperative outcomes were analyzed. Logistic regression identified risk factors for transfusions, and Cox proportional hazards models assessed associations with mortality.
Results: The study included 1040 patients who underwent hip fracture repair (35.87% received transfusion and 64.13% did not receive transfusion). Patients who received transfusion were older (median age 79 vs 77 years, p=0.0015), more frequently females (60.59%), and had lower preoperative hemoglobin levels (10.85± 1.75 vs 12.62± 1.61 g/dL, p< 0.001). Clopidogrel use (10.99% vs 6%, p=0.004), unstable intertrochanteric fractures (53.08% vs 42.13%, p=0.001), and ICU admissions (19.03% vs 6.45%; p< 0.001) were significantly more common in patients who received transfusion. Transfused patients experienced longer hospital stays (median 7 [IQR=5– 10] vs 6 [IQR=4– 8] days, p< 0.001), higher readmission rates (13.4% vs 8.85%; p=0.021), and increased all-cause mortality (18.23% vs 11.24%; p=0.002). However, this observed increase in mortality did not remain significant after multivariate adjustment. At multivariate analysis, blood transfusion was independently associated with ICU admission (OR=2.17, 95% CI=1.28– 3.66,p=0.004), and longer hospital stay (OR=1.05, 95% CI=1.02– 1.09, p=0.005), while no independent association between blood transfusion and all-cause mortality was found (HR=1.15, 95% CI=0.79– 1.66, p=0.465).
Conclusion: Blood transfusion in hip fracture surgery are linked to longer hospital stay and ICU admission, but not to increased all-cause mortality. Careful management of hemoglobin levels and transfusion practices is crucial.
Keywords: anemia, hip fractures/surgery, blood transfusion, postoperative outcomes, retrospective studies
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Ahmad has been published for this article.
Introduction
Anemia, characterized by a deficiency in hemoglobin concentration, is a prevalent illness in older persons, particularly in those having surgery for a hip fracture.1 According to the World Health Organization (WHO), anemia in adults is defined as a hemoglobin (Hb) level of less than 12 g/dL in women and less than 13 g/dL in men at sea level.2
Anemia can develop due to various underlying factors, including gastrointestinal bleeding and chronic medical conditions such as chronic kidney disease (CKD).3,4 The trauma of the hip fracture itself, along with blood loss during surgery and perioperative fluid shifts, can exacerbate pre-existing anemia or lead to new-onset anemia.3 Patients having surgery for an acute hip fracture frequently have anemia (39–69%).4 Globally, the annual number of hip fractures is projected to rise from approximately 1.6 million in 1990 to more than 4.5–6 million by 2050, reflecting population aging and increased fall risk. In the United States alone, estimates predict 500,000–1 million new cases annually by 2050, with costs exceeding $10 billion.5–7 Understanding the effects of anemia and the part blood transfusions play in the outcomes of hip fracture surgery becomes more crucial as the population ages and the prevalence of hip fractures is predicted to increase.
There has been extensive research on the link between anemia and mortality in surgical patients. An estimated 60% increase in the likelihood of postoperative 30-day death in noncardiac surgical patients was found in one study.8 The physiological effects of anemia, such as a decreased capacity for carrying oxygen, might limit the function of essential organs and compromise tissue perfusion, which can have a negative impact on postoperative results.
Allogenic blood transfusion (ABT) is frequently employed as a therapeutic intervention in hip fracture surgery to address anemia and its associated effects.9 However, despite its common use, there is ongoing debate regarding the benefits and risks of blood transfusion. One study found higher rates of death and more severe morbidity were seen in patients who underwent intraoperative infusion of 1 unit of packed red blood cells. Moreover, these rates increased significantly in a dose-dependent manner when more than one unit was transfused intraoperative.10 ABT has been linked to increased postoperative complications such as infection, postoperative delirium, systemic inflammation, and respiratory problems. In certain transfused patients, significant side effects such transfusion-related acute lung injury (TRALI) and transfusion-associated circulatory overload (TACO) have been reported.11–14
Furthermore, there is still disagreement over the ideal blood transfusion threshold. Over time, transfusion procedures have changed, with an increasing trend toward limiting transfusion strategies in particular surgical populations, such as patients with hip fractures. Restrictive transfusion strategies seek to reduce the number of transfusions and eliminate any dangers that might be involved with transfusion, particularly in patients who do not have obvious anemic symptoms or stable hemodynamics. Recent AABB (American Association of Blood Banks) guidelines, based on evidence from more than 45 randomized controlled trials involving over 20,000 adults, support the use of a restrictive transfusion strategy. For most hemodynamically stable adults, transfusion is recommended only when hemoglobin levels fall below 7 g/dL, as outcomes are comparable to more liberal thresholds. Slightly higher cutoffs, 7.5 g/dL for cardiac surgery and 8 g/dL for orthopedic or cardiovascular patients, may be used when clinically appropriate. These recommendations emphasize that restrictive thresholds are safe, reduce unnecessary transfusions, and do not compromise patient outcomes across a wide range of populations.15
The aim of this post-hoc analysis was to investigate the risk factors for receiving a post-operative blood transfusion and its impact on all-cause mortality in hip fracture surgery.
Methods
Study Design and Participant Selection
This study was a retrospective, multicenter analysis focusing on patients who underwent hip fracture repair surgeries between 2019 and 2021. Data were collected from three centers in Jordan. Yarmouk University Institutional Review Board in Irbid, Jordan, following Good Clinical Practice and the Declaration of Helsinki guidelines, approved this study (IRB Reference: IRB/2023/315). Patient data confidentiality was fully protected throughout the study. All collected data were de-identified prior to analysis, stored securely, and handled in compliance with institutional regulations and the Declaration of Helsinki.
Inclusion and Exclusion Criteria
Participants were selected based on the following criteria: age 65 years and older, diagnosis of femur or hip fractures resulting from a fall from standing height and having undergone hip fracture surgery at the specified institutions with informed consent. Exclusion criteria included non-surgical cases, surgeries performed at other institutions, or cases with missing medical records. To ensure a uniform study population, additional exclusion criteria were applied. Patients with open hip fractures, pathological fractures secondary to malignancy or metabolic bone disease, or polytrauma involving fractures at other anatomical sites were excluded. Furthermore, patients presenting with fractures older than two weeks from the time of injury were not included, as delayed presentations may influence perioperative management and outcomes. Only closed, acute hip fractures resulting from low-energy mechanisms (such as a fall from standing height) were analyzed. Moreover, for this post-hoc analysis, patients without documented preoperative hemoglobin levels, blood transfusion status, or essential postoperative outcome data were excluded. Decisions regarding perioperative blood transfusion followed institutional guidelines, where transfusion was indicated for symptomatic anemia (eg, hypotension, tachycardia, dyspnea, chest pain, or fatigue unresponsive to fluid resuscitation) or hemoglobin levels <8 g/dL, consistent with AABB recommendations. Figure 1 demonstrates a flowchart showing patient selection and inclusion in the study cohort.
 |
Figure 1 Flowchart showing patient selection and inclusion in the study cohort. |
Preoperative Procedures
Preoperative management included the administration of 1 liter of normal saline prior to spinal anesthesia and 500 mL before general anesthesia. Patients on anticoagulant therapy received subcutaneous calcium heparin 12 hours after admission. Oral anticoagulants were temporarily discontinued: low molecular weight heparin was stopped 24 hours before surgery, aspirin 7 days prior, and clopidogrel (Plavix) 14 days prior, as per standard protocols.
Only packed red blood cell transfusions were considered, plasma or platelet transfusions were not included. Preoperative hemoglobin levels were routinely measured within 24 hours prior to surgery. Transfusion decisions followed standardized institutional protocols applied across all participating centers. According to these guidelines, transfusion was indicated for symptomatic anemia (manifested by hypotension, tachycardia, dyspnea, chest pain, or signs of poor perfusion unresponsive to fluid therapy) or when hemoglobin levels fell below 8 g/dL. These criteria were consistent with the 2023 AABB international transfusion guidelines, ensuring a uniform approach to perioperative blood management.
Intraoperative Management
Standard intraoperative monitoring included electrocardiography (ECG), pulse oximetry, and non-invasive blood pressure measurements. Spinal anesthesia was administered in the lateral position using a 22/25-gauge Quincke spinal needle at the L3-L4 level, with a dose of 10 mg of bupivacaine combined with 25 µg of fentanyl. For patients receiving general anesthesia, intravenous administration of 100 mg of propofol and 100 µg of fentanyl was followed by tracheal intubation and muscle relaxation with rocuronium. Sevoflurane was used for maintenance of anesthesia, adjusted based on hemodynamic parameters.
The choice between spinal and general anesthesia was guided by institutional practice standards and patient clinical status. Spinal anesthesia was preferred for hemodynamically stable patients without contraindications to neuraxial blockade (eg, coagulopathy, infection at puncture site, or severe spinal deformity). General anesthesia was used when spinal anesthesia was contraindicated, failed, or when patient factors (such as severe anxiety, cognitive impairment, or inability to maintain the required position) precluded safe neuraxial administration. The final decision was made jointly by the anesthesiologist and attending orthopedic surgeon to optimize perioperative safety.
Postoperative Care
Postoperative pain management included 5 mg of morphine sulfate. For deep vein thrombosis (DVT) prophylaxis, 40 mg of apixaban was administered for 14 days, extended to 35 days for patients at high risk. Postoperative monitoring focused on identifying complications such as cardiovascular events, blood transfusion requirements, and mortality, with a particular emphasis on the first postoperative day.
Data Compilation and Definitions
Clinical data were extracted from electronic medical records and included information on demographics, preoperative characteristics, fracture type, intraoperative data, and postoperative outcomes such as ICU admissions, hemoglobin levels, blood transfusions, and mortality rates up to 12 months post-surgery. All-cause mortality was determined through review of electronic medical records, and when records were incomplete, telephone follow-up with patients or next of kin was conducted to confirm survival status up to 12 months post-surgery.
Statistical Analyses
Due to the retrospective design of the study, a formal sample size calculation was not performed; instead, all patients who underwent hip fracture repair during the study period were included in the analysis. The normality of continuous variables was assessed using histograms, quantile-quantile plots, and the Kolmogorov–Smirnov and Shapiro–Wilk tests. For normally distributed continuous variables, means and standard deviations (SD) were reported, while medians and interquartile ranges (IQR) were used for non-normally distributed continuous variables. Categorical variables were described using frequencies and percentages.
Comparisons between groups were performed using the Student’s t-test for normally distributed continuous variables and the Mann–Whitney U-test for non-normally distributed continuous variables. The chi-square test was used to compare categorical variables.
To identify risk factors associated with post-operative blood transfusion, logistic regression analysis was conducted. All potential risk factors were converted into dichotomous variables and entered into the univariate analysis. These factors composed age, gender, smoking status, comorbidities, preoperative hemoglobin levels, type of anesthesia, fracture stability, use of anticoagulants, preoperative and postoperative ICU admission, duration of hospital stay, need for readmission within one month, and mortality outcomes.
Variables that were statistically significant in the univariate analysis were further analyzed using multivariable logistic regression, adjusting for potential confounders. Variables with a p-value < 0.10 in univariate analyses and those considered clinically relevant (eg, age, sex, comorbidities, preoperative Hb, type of anesthesia) were included in the multivariable model. A forward stepwise logistic regression approach was used, with entry and removal criteria of p < 0.05 and p > 0.10, respectively. This procedure allowed for identification of independent predictors while minimizing collinearity and overfitting. Model calibration and discrimination were assessed using the Hosmer–Lemeshow test and c-statistics, respectively. Cox proportional hazards regression was used for time-to-event analysis of mortality.
All statistical analyses were conducted using Stata version 17 (Stata Corp, 2021). A two-sided p-value <0.05 was considered statistically significant.
Results
General Characteristics of the Study Sample
A total of 1040 patients were included in this post-hoc analysis, with 373 who received transfusion and 667 who did not receive transfusion. The general clinical and demographic features of patients receiving hip fracture repair are provided in Table 1.
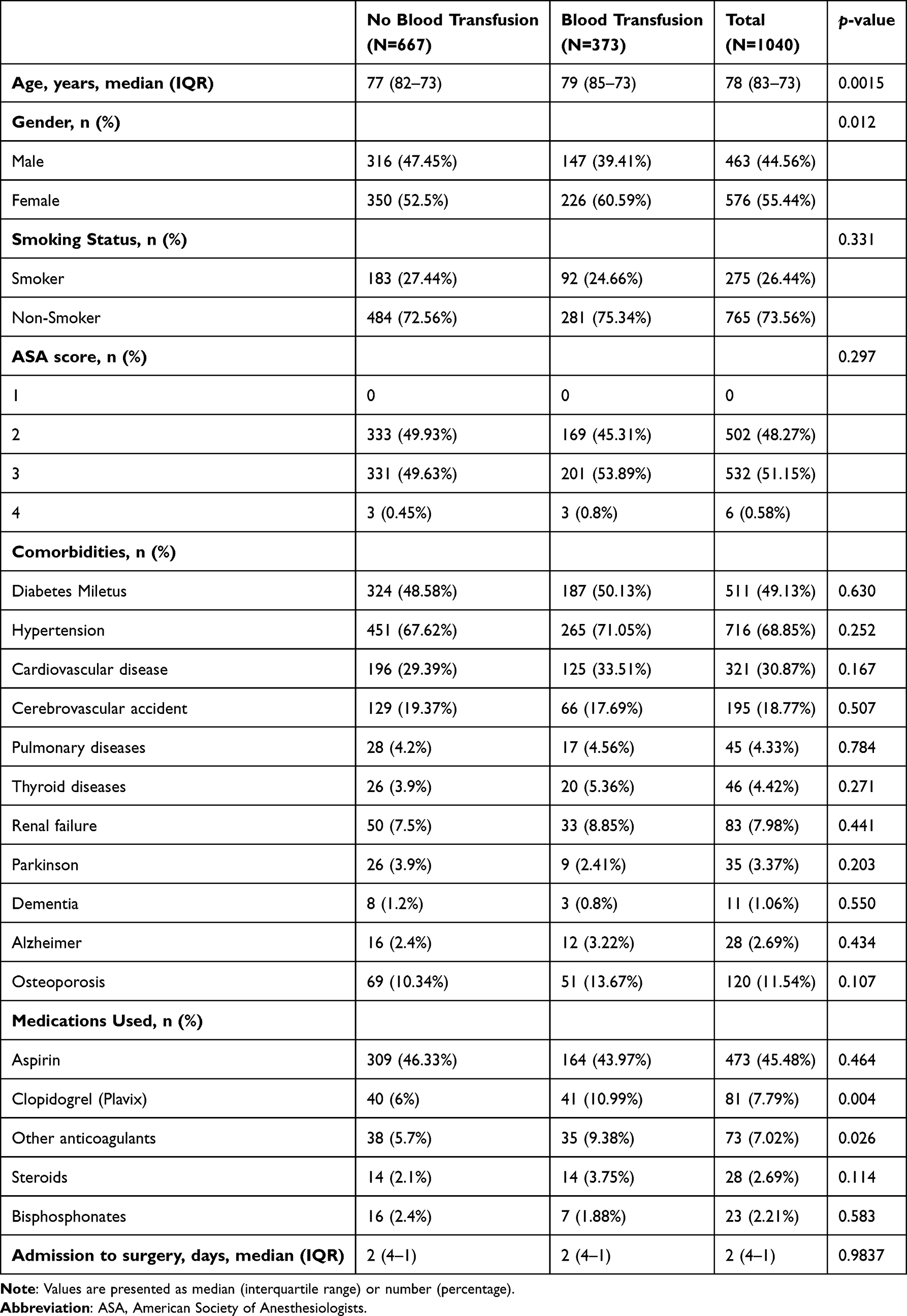 |
Table 1 Demographic and Clinical Characteristics of Patients Undergoing Hip Fracture Repair |
Patients in the transfusion group were older [median age: 79 (IQR=73–85) vs 77 (IQR=73–82) years, p=0.0015], and included a higher proportion of females (60.59% vs 52.5%, p=0.012) compared to patients who did not receive transfusion. The transfusion group had a higher prevalence of clopidogrel use (10.99% vs 6%, p=0.004), and other anticoagulants (9.38% vs 5.7%, p=0.026).
Preoperative Characteristics
Preoperative characteristics of patients are summarized in Table 2. Patients who received blood transfusion had significantly lower pre-operatively Hb levels (10.85 ± 1.75 vs 12.62 ± 1.61 g/dL, p<0.001), and were frequently treated with opioids (45.58% vs 37.78%, p=0.014). They also received antibiotics more frequently, including cephalosporins (p=0.025) or vancomycin in combination with cephalosporins (p=0.002).
 |
Table 2 Preoperative Variables of Patients Undergoing Hip Fracture Repair |
Intraoperative Characteristics
Intraoperative characteristics are detailed in Table 3. Patients receiving transfusion underwent more frequently spinal anesthesia (66.76% vs 58.77%, p = 0.011), had a higher prevalence of unstable intertrochanteric fractures (53.08% vs 42.13%, p = 0.001), and used less frequently cannulated screws (0% vs 1.05%, p = 0.047).
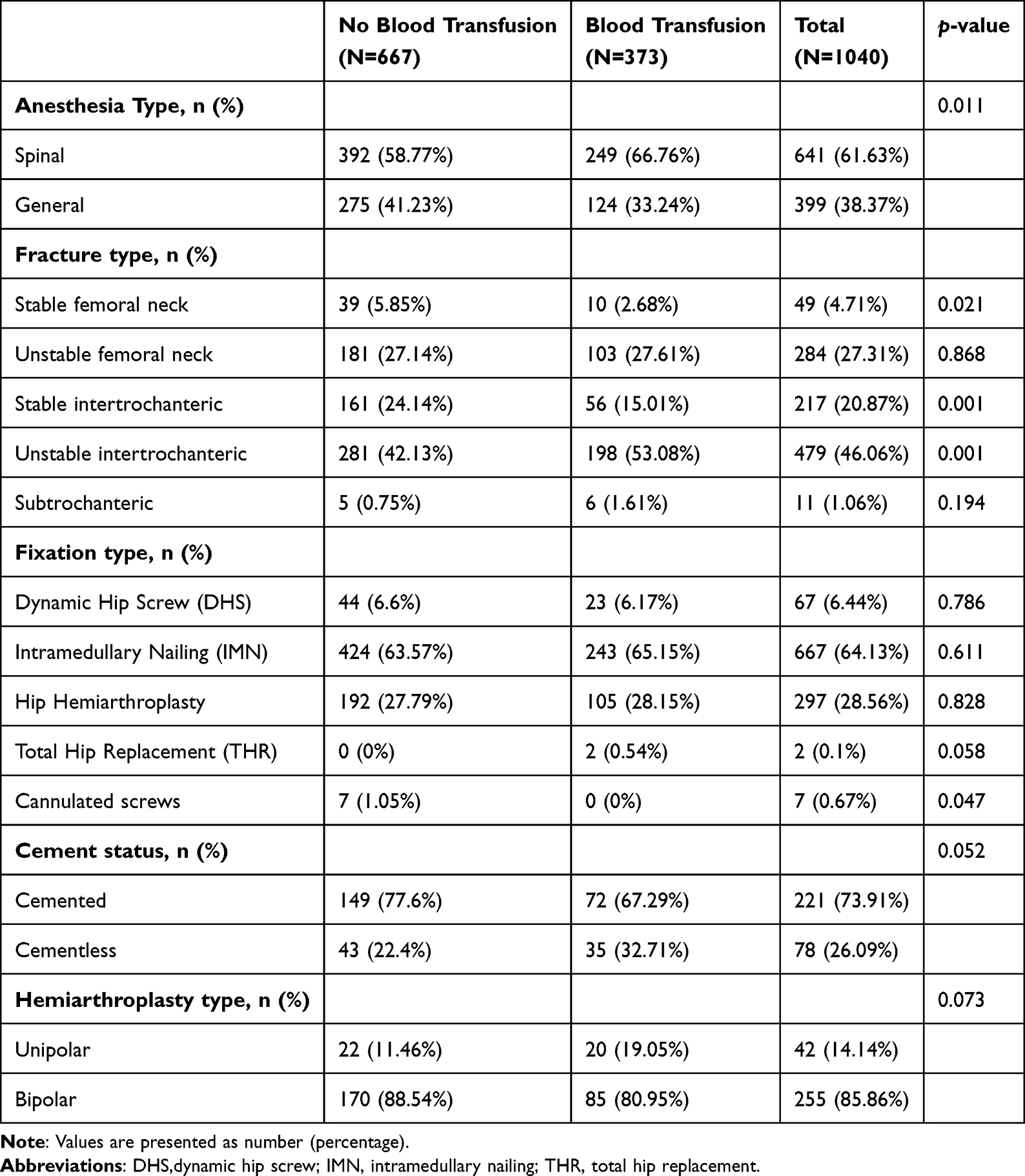 |
Table 3 Intraoperative Variables of Patients Undergoing Hip Fracture Repair |
Postoperative Outcomes
Postoperative outcomes are presented in Table 4. Patients who received transfusions were more likely to be admitted to the ICU (19.03% vs 6.45%, p < 0.001) and had a longer hospital stay [median: 7 (IQR = 5–10) vs 6 (IQR = 4–8) days, p < 0.001]. They also had higher readmission rates within one month (13.4% vs 8.85%, p = 0.021). Postoperative analgesic use (NSAIDs and opioids) was higher among transfused patients, who also had lower postoperative hemoglobin levels [median 9.3 (IQR=8.5; 10.5) vs 10.8 (IQR=9.8; 11.7) g/dL, p<0.001].
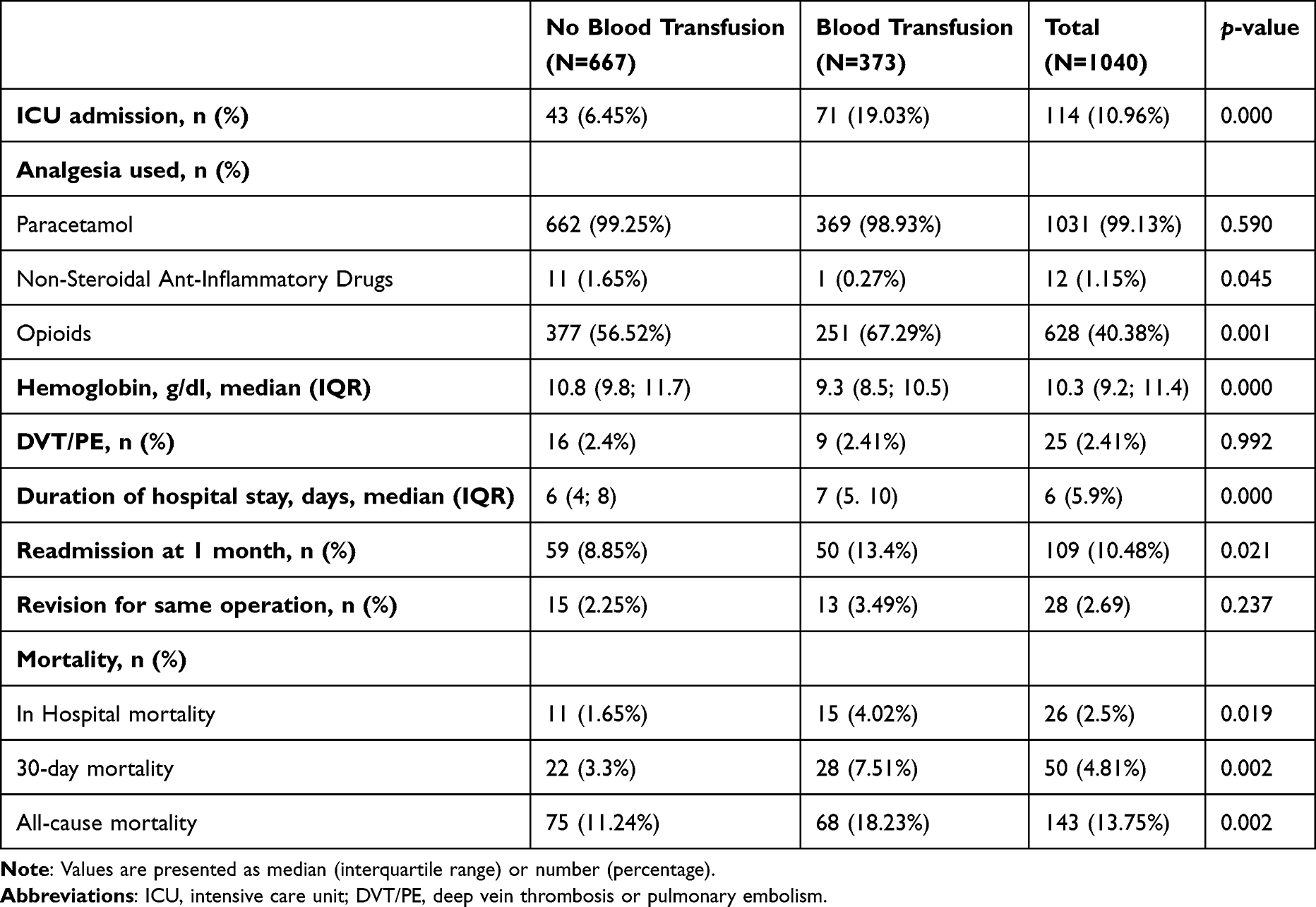 |
Table 4 Postoperative Variables of Patients Undergoing Hip Fracture Repair |
In-hospital, 30-day, and all-cause mortality rates were higher in the transfusion group than the non-transfusion group [4.02% vs 1.65% (p=0.019); 7.51% vs 3.3% (p=0.002); and 18.23% vs 11.24% (p=0.002), respectively].
Risk Factors for Post-Operative Blood Transfusion
Risk factors for receiving blood transfusion are shown in Electronic Supplementary Material [ESM], Table S1. Use of clopidogrel was with a higher likelihood blood transfusion (OR = 1.80, 95% CI = 1.02–3.18, p = 0.044). In contrast, higher pre-operative Hb levels were associated with a reduced likelihood of blood transfusions (OR = 0.52, 95% CI = 0.47–0.58, p = 0.000). Patients with stable femoral neck fractures had a lower risk of requiring transfusions compared to those with other fracture types (OR = 0.39, 95% CI = 0.16–0.95, p = 0.038).
Association Between Blood Transfusion and Clinical Outcomes
Blood transfusion was independently associated with higher odds of ICU admission (OR = 2.17, 95% CI = 1.28–3.66, p = 0.004), and longer hospital stay (OR = 1.05, 95% CI = 1.02–1.09, p = 0.005). Blood transfusion was not significantly associated with increased risk of DVT/PE, readmission to the hospital at one month, or the need for revision surgery (ESM Tables S2–S5). Cox proportional hazards regression indicated that ICU admission and prolonged hospital stay were independently associated with increased all-cause mortality (HR = 2.56, 95% CI = 1.67–3.92, p < 0.001; and HR = 1.06, 95% CI = 1.04–1.08, p < 0.001, respectively). Blood transfusion was not independently associated with increased all-cause mortality (HR = 1.15, 95% CI = 0.79–1.66, p = 0.465).
Discussion
Our research investigated the demographic, clinical, and procedural factors that impact patient outcomes following hip fracture repair. The key findings include:1 patients who received transfusions were more likely to be older, female, and have lower preoperative hemoglobin levels compared to those who did not receive transfusions;2 the use of clopidogrel, the presence of unstable intertrochanteric fractures, and ICU admissions were significantly more prevalent among transfused patients;3 transfused patients experienced longer hospital stay, higher readmission rates, and increased all-cause mortality; and4 while blood transfusion was independently associated with ICU admission and prolonged hospital stay, it did not correlate with all-cause mortality.
Risk Factors for Postoperative Blood Transfusion
Although older age,16–18 female sex,19,20 and opioid use21–24 were more common among transfused patients, they were not independently predictive after adjustment. Similarly, although a higher proportion of transfused patients received spinal anesthesia, this association did not retain statistical significance after multivariate adjustment. Prior research offers conflicting evidence on the impact of anesthesia type on transfusion risk, with some studies suggesting benefits of spinal over general anesthesia,25 while a meta-analysis report no significant differences in blood loss.26
In the multivariable logistic regression analysis, several other variables emerged as independent predictors of postoperative blood transfusion. Lower preoperative hemoglobin levels were strongly associated with an increased likelihood of transfusion. Our findings align with previous evidence that reported a stepwise increase in transfusion risk as hemoglobin levels declined.27 This reinforces the importance of preoperative anemia correction and patient blood management strategies.4,9
Moreover, while previous studies have yielded mixed results regarding clopidogrel’s effect on transfusion requirements, our findings highlight its significant clinical relevance in hip fracture surgery. The use of clopidogrel and the presence of unstable intertrochanteric fractures independently increased the likelihood of transfusion, likely reflecting greater surgical complexity and bleeding risk.25–28 These results emphasize the importance of preoperative hemoglobin optimization and meticulous perioperative planning, particularly for patients with unstable fractures or on antiplatelet therapy.28–31
The observed associations also highlight the need for broader patient blood management programs that incorporate individualized thresholds and non-transfusion strategies when feasible.4,9,32
Previous studies investigating the perioperative use of tranexamic acid (TXA) in pelvic and acetabular fracture surgery have demonstrated that TXA administration significantly reduces intraoperative blood loss, transfusion requirements, and operative duration, while also shortening hospitalization and lowering overall cost.33 Incorporating TXA into perioperative protocols represents an evidence-based strategy consistent with the risk-adapted blood management approach highlighted in our study.
In our cohort, fixation type was not significantly associated with transfusion need, except for cannulated screw fixation, which was used only in stable fractures and showed no transfusion cases (p = 0.047). This supports that fracture stability and surgical invasiveness, rather than implant design, primarily determine blood loss. Similarly, studies comparing PFNA (Proximal Femoral Nail Antirotation) and InterTAN nails reported no long-term differences in complications or functional outcomes, reinforcing that patient and fracture factors have a greater impact on perioperative results than the specific fixation system.34
Association Between Transfusion and Clinical Outcomes
Postoperative blood transfusion was independently associated with increased ICU admissions and prolonged hospital stay, even after adjusting for confounders. Similar findings have been reported in prior orthopedic and arthroplasty cohorts, linking transfusion to critical care utilization and extended hospitalization.35–37 Notably, ICU admission and extended hospitalization were also the strongest independent predictors of mortality in this cohort, suggesting that while transfusion may be a marker of severity, it is not a direct driver of poor long-term outcomes.
Although unadjusted analysis showed that the in-hospital, 30-day, and all-cause mortality rates were significantly higher patients who received transfusion than those who did not, these associations did not retain significance after multivariable adjustment. In our Cox proportional hazards regression, blood transfusion was not independently associated with increased all-cause mortality.
These findings suggest that transfusion may be a marker of higher clinical acuity or complexity, rather than a direct cause of increased mortality. This interpretation aligns with previous studies that found elevated mortality in transfused patients, although many of these studies did not fully adjust for confounding variables such as comorbidities or care intensity.38 Our results underscore the importance of careful risk adjustment when evaluating mortality outcomes associated with transfusion.
Our findings also have important implications for clinical practice. The identification of low preoperative hemoglobin, clopidogrel use, and unstable intertrochanteric fractures as predictors of postoperative transfusion supports the implementation of Patient Blood Management (PBM) strategies and structured preoperative optimization pathways. Early correction of anemia, careful coordination of antiplatelet therapy, and measures to minimize intraoperative blood loss should be integrated into standard care protocols. Moreover, the association between transfusion, ICU admission, and prolonged hospitalization highlights the importance of proactive ICU resource planning and close postoperative monitoring for high-risk patients. Incorporating these findings into multidisciplinary hip fracture pathways may enhance outcomes, reduce transfusion exposure, and improve resource utilization.Our study has several strengths. It is a large multicentric analysis involving 1,040 patients from multiple centers, enhancing the generalizability of the findings. The research comprehensively evaluates a range of preoperative, intraoperative, and postoperative variables related to postoperative blood transfusion, providing key insights into patient outcomes. Notably, the study highlights the clinical relevance of blood transfusion in relation to ICU admissions, prolonged hospital stay, and readmission rates, which can inform perioperative management strategies. Focusing on an elderly population, it underscores the need for optimized care for those vulnerable to hip fractures. The identification of modifiable risk factors, such as preoperative anemia and clopidogrel use, suggests opportunities for early interventions to reduce transfusion needs and improve outcomes. Additionally, this research is among the first in the Middle East to explore postoperative blood transfusion in hip fracture patients, filling a significant gap in regional data and potentially influencing transfusion protocols and evidence-based approaches.
Limitations
There are several limitations that must be addressed. First, although menopause, race, multiparity, socioeconomic level, addictions, and family history have all been commonly recognized risk factors for osteoporosis, these details have not been included in the records of patients and analyses. Moreover, there is a lack of information on the preoperative vitamin-D insufficiency or hormonal medication use that may have affected the frequency of fractures, which mostly occur in females. Second, neither the number of patients treated conservatively, nor the causes of surgical avoidance are known to us. Additionally, we lack information on the length of time between admission and surgery, the cause of the delay, the method of surgery, and postoperative complications for patients who ended up being taken into consideration for analysis because they were receiving surgical care. Further, there was no documentation in the medical record on the patients’ choices for the kind of anesthesia.
Moreover, the rationale behind the particular anesthetic technique selected was not disclosed. There may be concerns over the decision-making process due to this lack of information. Furthermore, no information concerning precise dosage, degree of neuraxial block, and premedication utilized are available. Moreover, there is a chance that the study’s findings were biased or ambiguous due to the absence of information on the patients’ prior coagulopathy. As such, care should be taken when interpreting the findings. Further studies that make use of comprehensive patient coagulopathy data could clarify the results. More extensive RCTs are required, and the clinical trial’s design should take these factors into account.
Conclusions
Our study highlights that patients who received blood transfusions after hip fracture surgery experienced higher rates of ICU admission, opioid use, and mortality; however, transfusion itself was not an independent predictor of mortality after adjustment. These findings emphasize the importance of a patient-specific approach guided by preoperative hemoglobin levels, comorbidities, and fracture characteristics. They also support the integration of patient blood management protocols and suggest that transfusion may reflect underlying clinical complexity rather than serve as an independent driver of adverse outcomes.
Data Sharing Statement
Data supporting the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
Yarmouk University Institutional Review Board in Irbid, Jordan, following Good Clinical Practice and the Declaration of Helsinki guidelines, approved this study (IRB Reference: IRB/2023/315). Patient data confidentiality was fully protected throughout the study. All collected data were de-identified prior to analysis, stored securely, and handled in compliance with institutional regulations and the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Consent for Publication
Due to the retrospective nature of this article, informed consent were waived by the IRB protocol.
Funding
No specific funding was received for this study.
Disclosure
The authors declare that they have no competing interests.
References
1. Newhall DA, Oliver R, Lugthart S. Anaemia: a disease or symptom. Neth J Med. 2020;78(3):104–13.
2. WHO. Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity. Vitamin and Mineral Nutrition Information System Geneva, World Health Organization. 2011.
3. Lewis JR, Hassan SK, Wenn RT, Moran CG. Mortality and serum urea and electrolytes on admission for Hip fracture patients. Injury. 2006;37(8):698–704. doi:10.1016/j.injury.2006.04.121
4. Spahn DR. Anemia and patient blood management in Hip and knee surgery: a systematic review of the literature. Anesthesiology. 2010;113(2):482–495. doi:10.1097/ALN.0b013e3181e08e97
5. Gupta NK, Chmait HR, Gill V, et al. Risk analysis index for estimation of 30-day postoperative mortality in hip fractures. JAMA Network Open. 2025;8(5):e2512689–e. doi:10.1001/jamanetworkopen.2025.12689
6. Dy CJ, McCollister KE, Lubarsky DA, Lane JM. An economic evaluation of a systems-based strategy to expedite surgical treatment of Hip fractures. J Bone Joint Surg Am Vol. 2011;93(14):1326–1334. doi:10.2106/JBJS.I.01132
7. Brown CA, Starr AZ, Nunley JA. Analysis of past secular trends of Hip fractures and predicted number in the future 2010-2050. J of Orthop Trauma. 2012;26(2):117–122. doi:10.1097/BOT.0b013e318219c61a
8. Saager L, Turan A, Reynolds LF, Dalton JE, Mascha EJ, Kurz A. The association between preoperative anemia and 30-day mortality and morbidity in noncardiac surgical patients. Anesth Analg. 2013;117(4):909–915. doi:10.1213/ANE.0b013e31828b347d
9. Duarte GC, Catanoce AP, Zabeu JL, et al. Association of preoperative anemia and increased risk of blood transfusion and length of hospital stay in adults undergoing Hip and knee arthroplasty: an observational study in a single tertiary center. Health Sci Rep. 2021;4(4):e448. doi:10.1002/hsr2.448
10. Ferraris VA, Davenport DL, Saha SP, Austin PC, Zwischenberger JB. Surgical outcomes and transfusion of minimal amounts of blood in the operating room. Arch Surg. 2012;147(1):49–55. doi:10.1001/archsurg.2011.790
11. Shander A, Lobel GP, Javidroozi M. Transfusion practices and infectious risks. Expert Rev Hematol. 2016;9(6):597–605. doi:10.1586/17474086.2016.1164593
12. Semple JW, Rebetz J, Kapur R. Transfusion-associated circulatory overload and transfusion-related acute lung injury. Blood. 2019;133(17):1840–1853. doi:10.1182/blood-2018-10-860809
13. Dunne JR, Malone DL, Tracy JK, Napolitano LM. Allogenic blood transfusion in the first 24 hours after trauma is associated with increased systemic inflammatory response syndrome (SIRS) and death. Surg Infect. 2004;5(4):395–404. doi:10.1089/sur.2004.5.395
14. Guo Y, Jia P, Zhang J, Wang X, Jiang H, Jiang W. Prevalence and risk factors of postoperative delirium in elderly Hip fracture patients. J Int Med Res. 2016;44(2):317–327. doi:10.1177/0300060515624936
15. Carson JL, Stanworth SJ, Guyatt G, et al. Red blood cell transfusion: 2023 AABB international guidelines. JAMA. 2023;330(19):1892–1902. doi:10.1001/jama.2023.12914
16. Alvarez-Payares JC, Rivera-Arismendy S, Ruiz-Bravo P, et al. Unexplained anemia in the elderly. Cureus. 2021;13(11):e19971. doi:10.7759/cureus.19971
17. Girelli D, Marchi G, Camaschella C. Anemia in the Elderly. HemaSphere. 2018;2(3):e40. doi:10.1097/HS9.0000000000000040
18. Romano AD, Paglia A, Bellanti F, et al. Molecular aspects and treatment of iron deficiency in the elderly. Int J Mol Sci. 2020;21(11):3821. doi:10.3390/ijms21113821
19. Pass B, Malek F, Rommelmann M, et al. The influence of malnutrition measured by hypalbuminemia and body mass index on the outcome of geriatric patients with a fracture of the proximal femur. Medicina. 2022;58(11):1610. doi:10.3390/medicina58111610
20. Yokoyama K, Ukai T, Watanabe M. Effect of nutritional status before femoral neck fracture surgery on postoperative outcomes: a retrospective study. BMC Musculoskelet. Disord. 2021;22(1):1027. doi:10.1186/s12891-021-04913-2
21. Pagan DN, Hernandez VH, Reddy GB, D’Apuzzo MR. Chronic opioid use independently increases complications and resource utilization after primary total joint arthroplasty. J Arthroplasty. 2023;38(6):1004–1009. doi:10.1016/j.arth.2022.12.021
22. Zvetkova E, Antonova N, Ivanov I, Savov Y, Gluhcheva Y. Platelet morphological, functional and rheological properties attributable to addictions. Clin Hemorheol Microcirc. 2010;45(2–4):245–251. doi:10.3233/CH-2010-1305
23. Quraishi R, Kathiresan P, Verma K, Rao R, Jain R. Effect of chronic opioid use on the hematological and inflammatory markers: a retrospective study from North India. Indian J Psychiatry. 2022;64(3):252–256. doi:10.4103/indianjpsychiatry.indianjpsychiatry_751_21
24. Holm M, Tornvall P, Henareh L, et al. The MOVEMENT Trial. J Am Heart Assoc. 2019;8(2):e010152. doi:10.1161/JAHA.118.010152
25. Morgan L, McKeever TM, Nightingale J, Deakin DE, Moppett IK. Spinal or general anaesthesia for surgical repair of Hip fracture and subsequent risk of mortality and morbidity: a database analysis using propensity score-matching. Anaesthesia. 2020;75(9):1173–1179. doi:10.1111/anae.15042
26. Pu X, Sun JM. General anesthesia vs spinal anesthesia for patients undergoing total-Hip arthroplasty: a meta-analysis. Medicine. 2019;98(16):e14925. doi:10.1097/MD.0000000000014925
27. Salido JA, Marín LA, Gómez LA, Zorrilla P, Martínez C. Preoperative hemoglobin levels and the need for transfusion after prosthetic Hip and knee surgery: analysis of predictive factors. J Bone Joint Surg Am. 2002;84(2):216–220. doi:10.2106/00004623-200202000-00008
28. Wu CT, Lien TH, Chen IL, Wang JW, Ko JY, Lee MS. The risk of bleeding and adverse events with clopidogrel in elective hip and knee arthroplasty patients. J Clin Med. 2022;11(7).
29. Lin PH, Chien JT, Hung JP, Hong CK, Tsai TY, Yang CC. Unstable intertrochanteric fractures are associated with a greater hemoglobin drop during the perioperative period: a retrospective case control study. BMC Musculoskelet. Disord. 2020;21(1):244. doi:10.1186/s12891-020-03208-2
30. Lou L, Xu L, Wang X, Xia C, Dai J, Hu L. Comprehensive assessment of risk factors and development of novel predictive tools for perioperative hidden blood loss in intertrochanteric femoral fractures: a multivariate retrospective analysis. Eur. J. Med. Res. 2024;29(1):626. doi:10.1186/s40001-024-02244-1
31. Usami T, Takada N, Kosuwon W, et al. A lateral fracture line affects femoral trochanteric fracture instability and swing motion of the intramedullary nail: a biomechanical study. JB & JS open access. 2024;9(1).
32. Kotzé A, Carter LA, Scally AJ. Effect of a patient blood management programme on preoperative anaemia, transfusion rate, and outcome after primary Hip or knee arthroplasty: a quality improvement cycle. Br J Anaesth. 2012;108(6):943–952. doi:10.1093/bja/aes135
33. Sönmez E, Gökmen MY, Pazarcı Ö. The effects of prophylactic administration of tranexamic acid on the operative time and the amount of blood transfused during open fixation of pelvis and acetabulum fractures. J Orthopaedic Surg Res. 2024;19(1):606. doi:10.1186/s13018-024-05100-4
34. Varmış HO, Gökmen MY, Tan İ. A retrospective comparative study of the clinical and radiological outcomes of intertrochanteric fractures treated with proximal femoral nail antirotation (PFN-A) and INTERTAN nail. PLoS One. 2025;20(1):e0316954. doi:10.1371/journal.pone.0316954
35. AbdelSalam H, Restrepo C, Tarity TD, Sangster W, Parvizi J. Predictors of intensive care unit admission after total joint arthroplasty. J Arthroplasty. 2012;27(5):720–725. doi:10.1016/j.arth.2011.09.027
36. Memtsoudis SG, Rosenberger P, Walz JM. Critical care issues in the patient after major joint replacement. J Intensive Care Med. 2007;22(2):92–104. doi:10.1177/0885066606297692
37. Courtney PM, Melnic CM, Gutsche J, Hume EL, Lee GC. Which patients need critical care intervention after total joint arthroplasty?: a prospective study of factors associated with the need for intensive care following surgery. Bone Joint J. 2015;97–b;(11):1512–8.
38. Smeets SJM, Verbruggen J, Poeze M. Effect of blood transfusion on survival after Hip fracture surgery. Eur J Orthop Surg Traumatol. 2018;28(7):1297–1303. doi:10.1007/s00590-018-2205-z
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Perioperative Blood Transfusion Strategies in Orthopaedic Surgery: A Comprehensive Review and Analysis
Yaregal Melesse D, Admass BA, Admassie BM
Open Access Surgery 2024, 17:55-62
Published Date: 11 March 2024