Back to Journals » Infection and Drug Resistance » Volume 15
Risk Factors for Multidrug-Resistant Organisms Infection in Diabetic Foot Ulcer
Authors Liu X ![]() , Ren Q, Zhai Y, Kong Y, Chen D, Chang B
, Ren Q, Zhai Y, Kong Y, Chen D, Chang B
Received 20 January 2022
Accepted for publication 28 March 2022
Published 7 April 2022 Volume 2022:15 Pages 1627—1635
DOI https://doi.org/10.2147/IDR.S359157
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Xinbang Liu,1,2,* Qiuyue Ren,3,* Yangkui Zhai,1,2,* Yihan Kong,1,2 Dong Chen,4 Bai Chang1,2
1NHC Key Laboratory of Hormones and Development, Chu Hsien-I Memorial Hospital and Tianjin Institute of Endocrinology, Tianjin Medical University, Tianjin, 300134, People’s Republic of China; 2Tianjin Key Laboratory of Metabolic Diseases, Tianjin Medical University, Tianjin, 300134, People’s Republic of China; 3Department of Nephropathy, Wang Jing Hospital of China Academy of Chinese Medical Sciences, Beijing, 100102, People’s Republic of China; 4Graduate School, Tianjin University of Traditional Chinese Medicine, Tianjin, 301617, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Bai Chang, Email [email protected]
Objective: The aim of this study is to analyze the microbiological characteristics of diabetic foot ulcer (DFU) and drug resistance of multidrug-resistant organisms (MDROs) and to reveal the potential risk factors for MDROs. This provides a basis for early empiric antibiotic treatment.
Methods: This study included 348 patients with diabetic foot ulcer in Chu Hsien-I Memorial Hospital & Metabolic Disease Hospital of Tianjin Medical University between May 2020 and November 2021. A total of 475 strains of bacteria were cultured, among which 240 strains were multidrug-resistant bacteria, accounting for 51%. Binary logistic regression was used to analyze risk factors. First, univariate analysis was used to calculate the p value of variables, and then multivariate analysis was conducted for variables with p < 0.1 to analyze independent risk factors. Risk factors with p < 0.05 in multivariable analysis were considered as independent risk factors. The strength of the association was represented by odds ratio and 95% confidence interval.
Results: Univariable logistic regression analysis demonstrated that previous hospitalization, previous antibiotic therapy, ulcer size > 4cm2, surgical therapy, D-dimer, and CRP were associated with MDRO infection in patients with DFU. Multivariate logistic regression analysis demonstrated that previous hospitalization (OR = 1.91; 95% CI = 1.11– 3.28; p = 0.02), ulcer size > 4cm2 (OR = 1.68; 95% CI = 1.03– 2.76; p = 0.04), surgical therapy (OR = 2.14; 95% CI = 1.03– 4.47; p = 0.04), and CRP (OR = 1.01; 95% CI = 1.00– 1.01; p = 0.03) were independent risk factors for MDROs infection in diabetic foot patients. Drug resistance analysis may indicate that the proportion and drug resistance rate of Acinetobacter baumannii in Tianjin, China, have changed.
Conclusion: Previous hospitalization, ulcer size > 4cm2, surgical therapy and CRP were independent risk factors for MDROs infection in diabetic foot patients. Identifying these risk factors can help us identify the high-risk patients of diabetic foot with MDRO infection early. More attention to high-risk patients and more aggressive isolation precautions may reduce the incidence of MDRO infection in diabetic foot patients.
Keywords: diabetic foot ulcer, multidrug-resistant organisms, infection, risk factors, logistic regression analysis
Introduction
Diabetic foot ulcer (DFU) is one of the most serious complications of diabetes.1 Epidemiological investigation found that the global prevalence of DFU is 6.3%,2 and what is more troublesome is that DFU also has a high recurrence rate.3 Cohort studies have shown that DFU have a high mortality rate in both developed and developing countries, with a 5-year mortality rate of up to 42%.4–7 With high morbidity and mortality, DFU has been the main cause of nontraumatic lower-limb amputations.8,9 We have developed a model for predicting the risk of early DFU, which may potentially guide early intervention.10 Hyperglycemia impair immune cells activity in eliminating pathogens,11,12 while severe infection can cause stress hyperglycemia.13 The interaction of the two ways has resulted in a rapid development of diabetic foot infection (DFI) and sometimes a necrotizing abscess can be developed in just 6 days.14 Early empiric antibiotic treatment is necessary due to the long culture time of microorganisms and the lack of basic microbiology laboratories. But Multidrug-resistant organisms (MDROs) infection is easy to make antibiotic treatment failure, increasing the difficulty of diabetic foot treatment.
In recent years, MDRO infection in patients with DFU has received a lot of attention. Although there is insufficient evidence that MDRO delay wound healing,15 some studies have shown that MDRO significantly increase the rate of recurrence and amputation in patients with DFU.16,17 There are significant differences in the prevalence of MDROs in different regions,18–21 and there are few reports on the prevalence of MDROs in DFU in North China. The aim of this study is to analyze the microbiological characteristics of DFU and drug resistance of MDROs, and to reveal the potential risk factors for MDROs. This provides a basis for early empiric antibiotic treatment.
Patients and Methods
This study included 348 patients with diabetic foot ulcer in Chu Hsien-I Memorial Hospital & Metabolic Disease Hospital of Tianjin Medical University between May 2020 and November 2021. A total of 475 strains of bacteria were cultured, among which 240 strains were multidrug-resistant bacteria, accounting for 51%.
All patients were graded according to the University of Texas Wound Classification System after admission and grade 0 patients were excluded. Identify diabetic foot ulcer infection according to IWGDF/IDSA recommendations.22,23 Previous hospitalization was defined as hospital admissions for diabetic foot within 12 months. Previous antibiotic therapy was defined as the use of antibiotics within 30 days. Osteomyelitis was determined by X-ray and sterile forceps exploration. Ischemia was defined by an ankle brachial index <0.9, lower extremities CT angiography was performed when necessary. Peripheral neuropathy was defined as the absence of perception of the Semmes–Weinstein monofilament 5.07/10 g at 2 of 10 standardized plantar sites on either foot or vibration sense <5/8 grade of a 128-Hz tuning fork, neuroelectrophysiological examination was performed when necessary. Diabetic kidney disease (DKD) was determined by glomerular filtration rate (GFR) below 60 mL/min/1.73m2 or urinary albumin/creatinine ratio (ACR) above 30 mg/g for more than three months. Diabetic retinopathy (DR) was determined by dilated fundus examination that reveals microaneurysms or more serious lesions. Surgical therapy includes both minor and major amputations. Systolic blood pressure (SBP) and diastolic blood pressure (DBP) were measured with a standard ambulatory blood pressure monitor, and the mean value of 24-hour ambulatory blood pressure was obtained. All the laboratory results, including HbA1c, blood lipid and C-reactive protein (CRP), were taken from the first inspection after admission.
On admission, the skin around the wound was cleaned with povidone iodine solution. After careful irrigation of the wound with normal saline, remove necrotic tissue as needed. Irrigate the wound again, press a sterile cotton swab firmly into the wound and rotate to collect deep secretions. After 30 minutes, the swabs were transported to the microbiology laboratory in a sterile container. The specimens were inoculated and cultured, and the strains were identified by VIETK mass spectrometry (bioMérieux, Marcy l’Etoile, France), and drug sensitivity test was conducted by VITEK 2-Compact system (bioMérieux, Marcy l’Etoile, France). Sensitivity tests were performed using the disc diffusion method to determine sensitivity, according to the guidelines of Clinical and Laboratory Standards Institute (CLSI). MDROs were defined according to an international expert proposal set by the European Centre for Disease Prevention and Control (ECDC) and the Centers for Disease Control and Prevention (CDC).24 The ECDC criteria define MDRO as acquired non-susceptibility to at least one agent in three or more antimicrobial categories.
Treatment
After admission, all the patients were given insulin therapy, and insulin dose is adjusted according to blood glucose levels throughout the day. Empiric antibiotic treatment depended on DFI duration, previous antibiotic treatment and severity of infection. Antibiotics sensitive to gram-positive bacteria were mainly used for mild and moderate DFI patients with short DFI duration and no recent antibiotic treatment. Broad-spectrum antibiotic was mainly used for severe DFI patients. Therapy was adjusted according to the antibiotic susceptibility results and the clinical response. Infected wound care is once a day. Patients with deep abscess were treated with timely debridement and drainage with sterile gauze, and enclosed negative pressure drainage was used when necessary. The surgical treatment was adopted for the patients whose condition worsened with conservative treatment.
The patients received tertiary care at Chu Hsien-I Memorial Hospital & Metabolic Disease Hospital of Tianjin Medical University. Tianjin is located in the north temperate zone in the middle latitude east coast of Eurasia continent, a warm temperate zone semi-humid monsoon climate. Tianjin straddles the Haihe River, which is the largest river in North China.
Statistical Analysis
According to normality, quantitative variables were expressed as mean ± standard deviation and quartile, respectively, and Mann–Whitney U-test was used. Qualitative variables were expressed as percentages and Pearson’s chi-squared test was used. Binary logistic regression was used to analyze risk factors. First, univariate analysis was used to calculate the p value of variables, and then multivariate analysis was conducted for variables with p < 0.1 to analysis independent risk factors. Risk factors with p < 0.05 in multivariable analysis were considered as independent risk factors. The strength of the association was represented by odds ratio (OR) and 95% confidence interval (CI). All statistical analyses were performed using SPSS 25.0 software. p<0.05 was considered significant (Table 1).
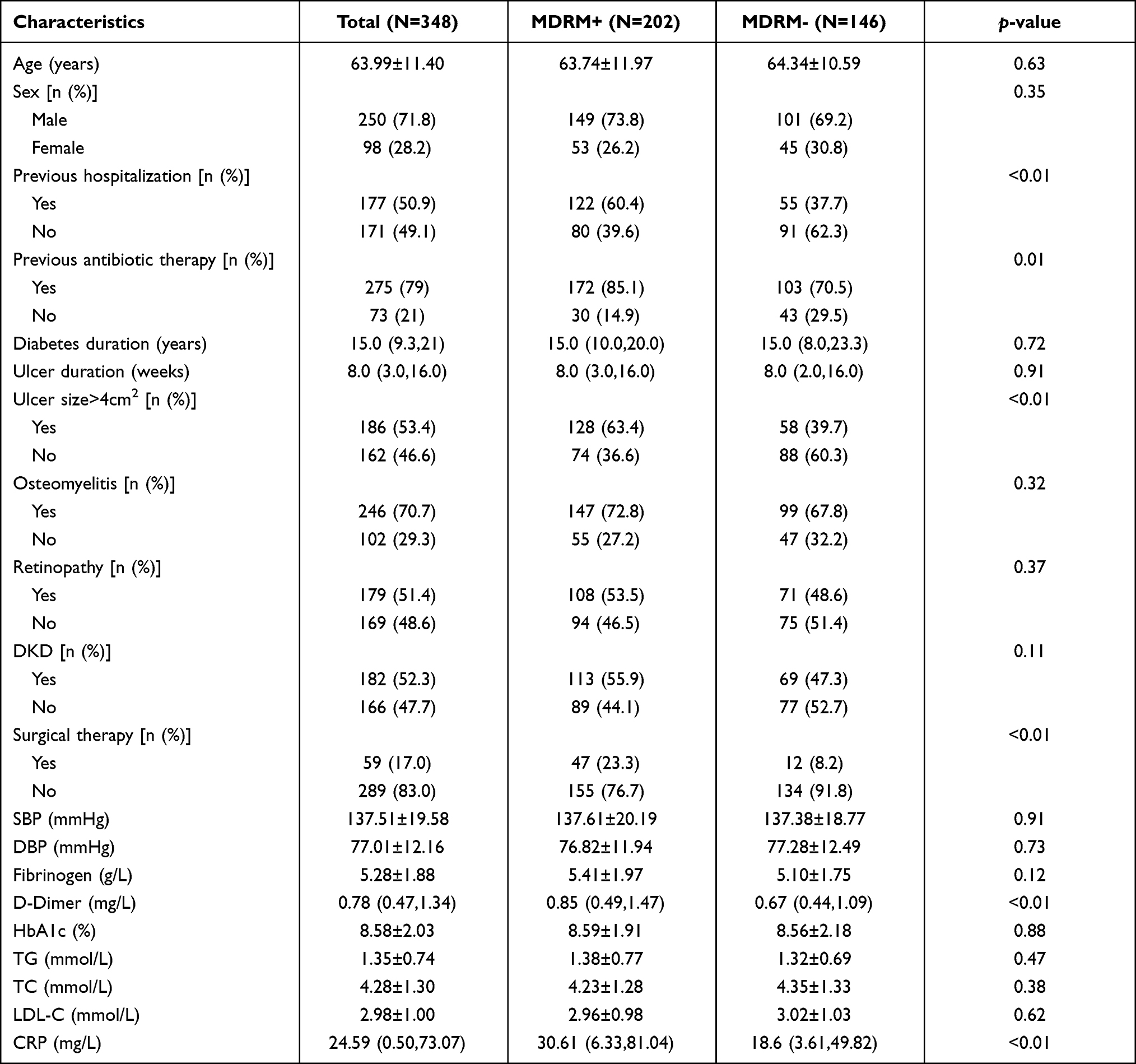 |
Table 1 Baseline Data of Patients with Diabetic Foot Ulcer |
Results
There was no statistical difference in Age, Sex, Diabetes duration, Ulcer duration, Osteomyelitis, Retinopathy, DKD, SBP, DBP, Fibrinogen, HbA1c, TG, TC and LDL-C of baseline data between the two groups. Logistic regression analysis demonstrated that Previous hospitalization (OR = 2.52; 95% CI = 1.63–3.91; p<0.01), previous antibiotic therapy (OR = 2.39; 95% CI = 1.41–4.05; p<0.01), ulcer size>4cm2 (OR = 2.62; 95% CI = 1.69–4.07; p<0.01), Surgical therapy (OR = 3.39; 95% CI = 1.72–6.65; p<0.01), D-Dimer (OR = 1.20; 95% CI = 1.01–1.42; p = 0.04), CRP (OR = 1.01; 95% CI = 1.00–1.01; p<0.01) were associated with MDRO infection in patients with DFU. Four independent risk factors were found after adjusting for potential confounders, were Previous hospitalization (OR = 1.91; 95% CI = 1.11–3.28; p = 0.02), ulcer size >4cm2 (OR = 1.68; 95% CI = 1.03–2.76; p = 0.04), Surgical therapy (OR = 2.14; 95% CI = 1.03–4.47; p = 0.04), CRP (OR = 1.01; 95% CI = 1.00–1.01; p = 0.03) (Table 2).
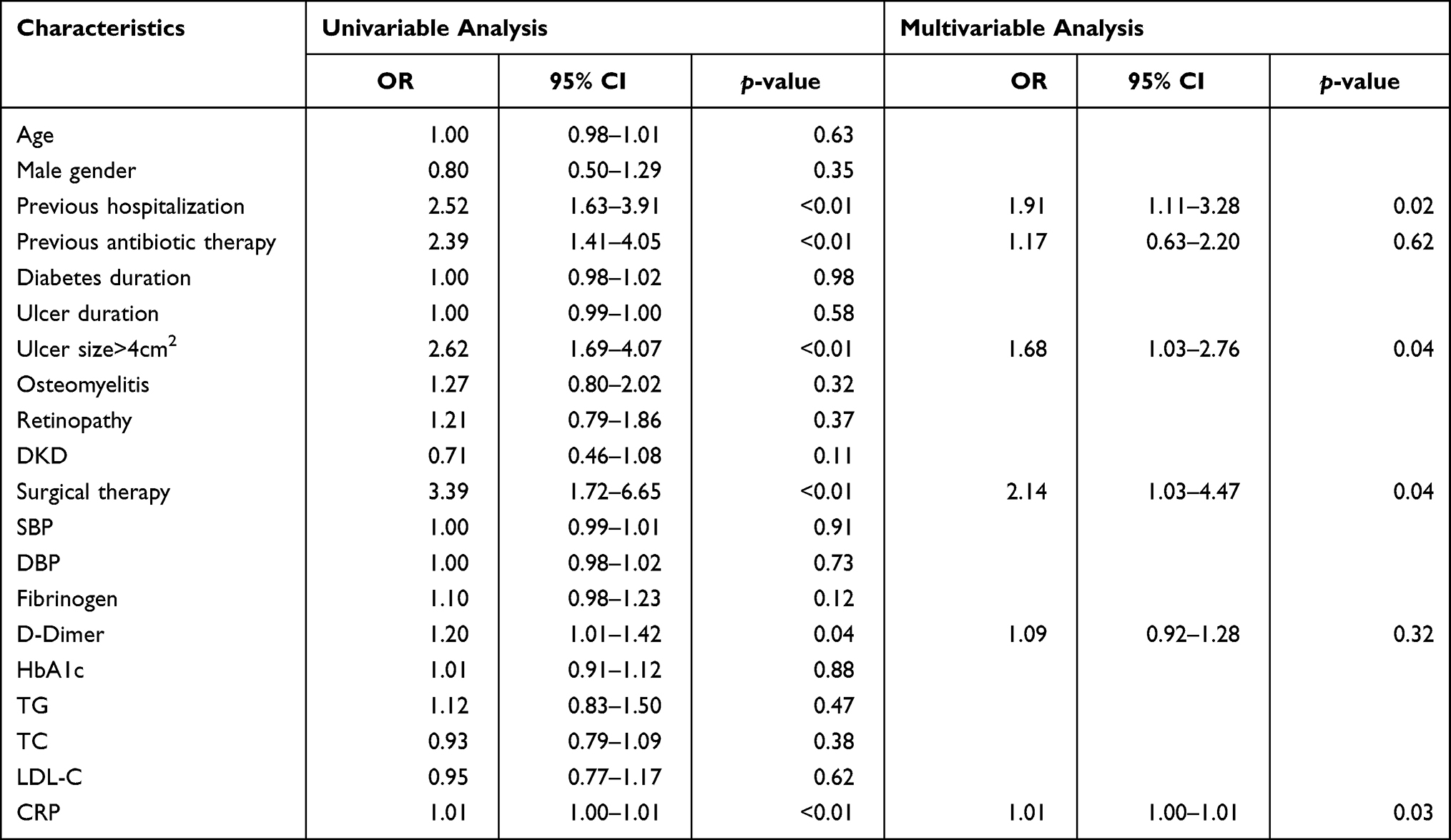 |
Table 2 Logistic Regression Analysis of MDRO Infection in DFU Patients |
A total of 475 strains of bacteria were cultured, including 240 strains of MDRO, accounting for 51%. Among them, there were 50 strains of Staphylococcus aureus with MDRO rate of 42%, 49 strains of Pseudomonas aeruginosa with MDRO rate of 24%, 47 strains of Acinetobacter baumannii with MDRO rate of 70%, 47 strains of Klebsiella pneumoniae with MDRO rate of 24%, 44 strains of Streptococcus spp. with MDRO rate of 45%, and 23 strains of Staphylococcus epidermidis with MDRO rate of 91% (Table 3).
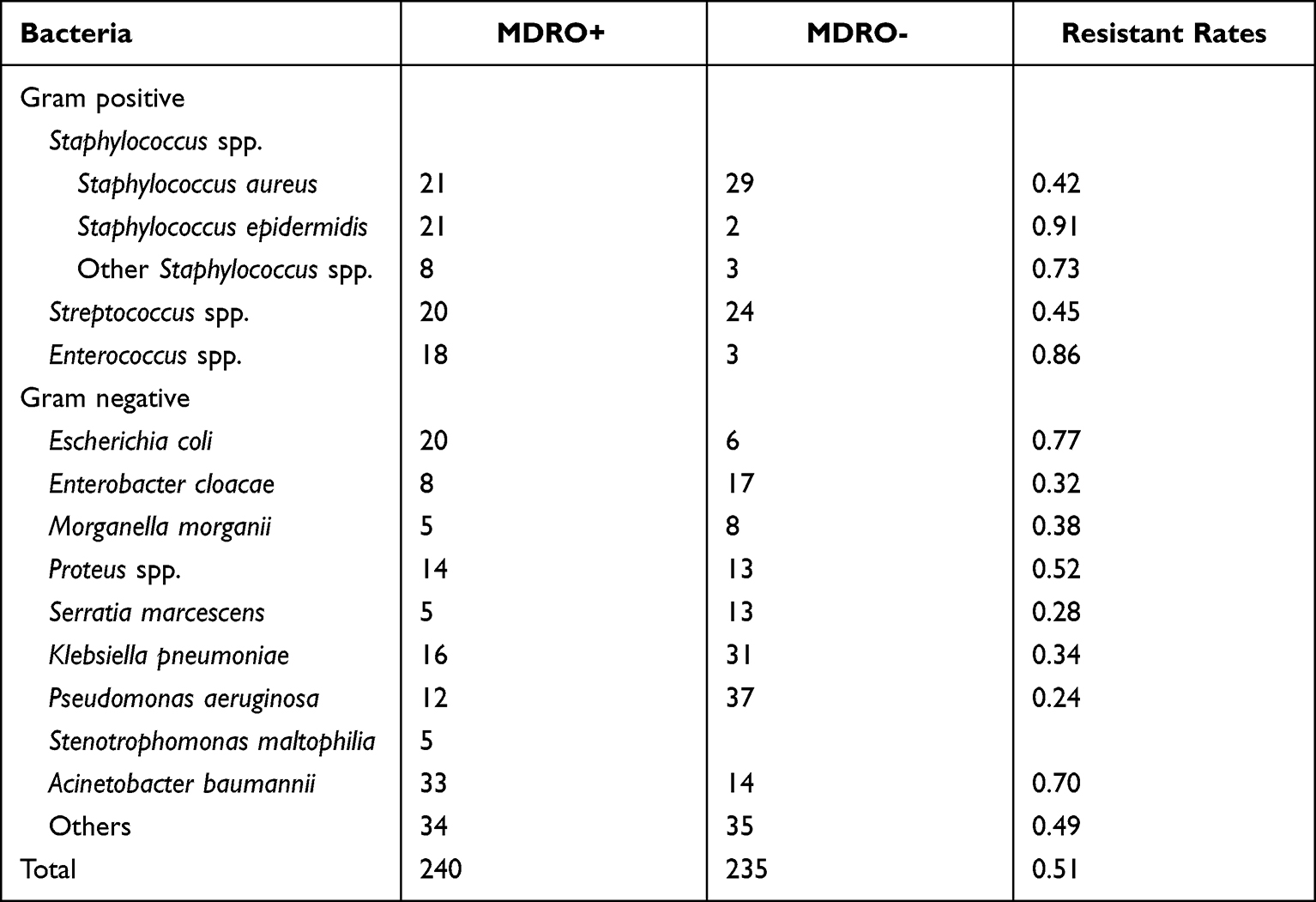 |
Table 3 Bacterial Distribution and Drug Resistance Rate |
In the analysis of multidrug-resistant bacteria, we found that 71.4% of Staphylococcus aureus were sensitive to oxacillin or cefoxitin. All Staphylococcus aureus were resistant to penicillin, but sensitive to vancomycin and quinupristin/dalfopristin. Most Staphylococcus epidermidis defined as multi-resistant because of combined fluoroquinolones or tetracycline resistance in addition to erythromycin and clindamycin resistance. Pseudomonas aeruginosa kept high resistance to several antibiotics, but higher sensitivity to aminoglycoside antibiotics. Acinetobacter baumannii was resistant to most antibiotics, only sulfamethoxazole and polymyxin had higher sensitivity. Escherichia coli had higher drug resistance rates to fluoroquinolones, tetracycline and first and second-generation cephalosporins, and higher sensitivity to ceftazidime, cefepime, penicillins + β-lactamase inhibitors and carbapenems (Table 4).
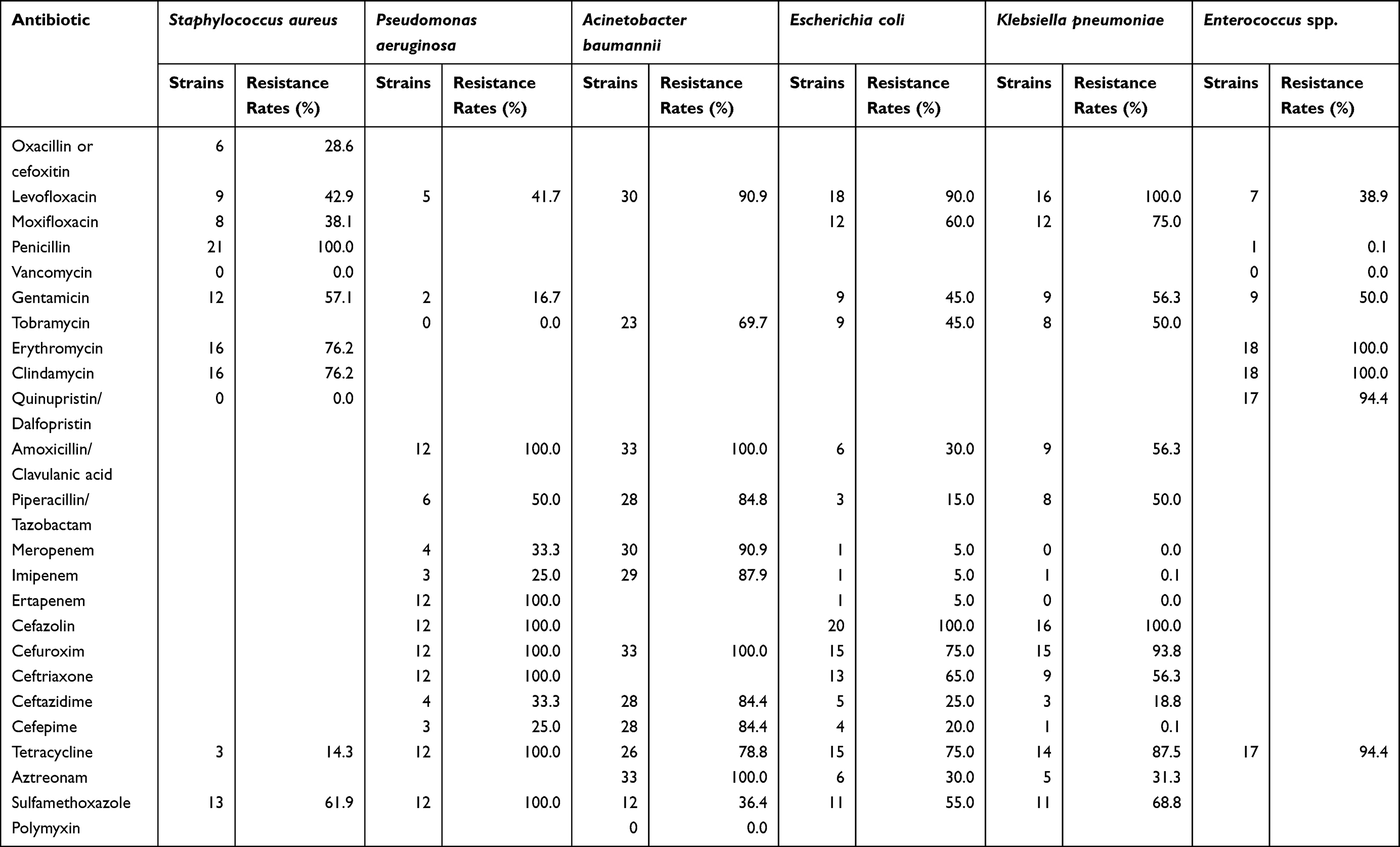 |
Table 4 Resistance Rate of Common MDRO to Commonly Used Antibiotics |
Discussion
The top MDRO in this study were Acinetobacter baumannii, Staphylococcus aureus, Staphylococcus epidermidis, Streptococcus spp. and Escherichia coli, while the top MDRO in a study of our hospital in 2012 were Staphylococcus aureus, Enterobacter spp, Pseudomonas aeruginosa and Staphylococcus epidermidis.25 This indicated that the detection rate of multidrug-resistant Acinetobacter baumannii in our hospital increased significantly. Since all bacteria were collected on admission, hospital acquired infection was almost impossible due to this hospitalization. The increase of Acinetobacter baumannii may indicate that the proportion and drug resistance rate of Acinetobacter baumannii in Tianjin, China, have changed.
Early empiric antibiotic treatment is necessary for patients at high risk of MDRO infection. Early detection of suspected Pseudomonas aeruginosa infection (green staining of toes clearance or wound dressing), early empiric use of tobramycin, ceftazidime, cefepime, imipenem, rather than ertapenem, amoxicillin/clavulanic acid, ceftriaxone, is recommended when secretion culture is not returned. Early detection of suspected Staphylococcus aureus infection (local suppurative infection, cellulitis), early empiric use of levofloxacin, quinupristin/dalfopristin, rather than penicillin, erythromycin, clindamycin, is recommended when secretion culture is not returned. Tobramycin, piperacillin/tazobactam, imipenem, ceftazidime and cefepime can be used to treat other suspected gram-negative bacterial infections, and antibiotics can be adjusted after the results of secretion culture and antibiotic treatment.
This study identified previous hospitalization as an independent risk factor for MDRO infection. Hospital-acquired infection is one of the most common causes of MDRO infection, which leads to a high mortality.26,27 The occurrence of hospital acquired infection is mainly due to the poor environment of the ward and the inadequate implementation of isolation measures for patients infected with MDRO. In order to avoid MDRO infection caused by hospitalization, we should strictly observe and implement the isolation measures for patients with MDRO infection, and discharge patients in stable condition as soon as possible and follow-up in the clinic to reduce the length of stay and the risk of hospital acquired infection.
Ulcer size >4cm2 is also an independent risk factor for MDRO infection. The decreased immune function of diabetic patients provides conditions for the propagation of opportunistic pathogen, and larger ulcer area means more exposure to pathogen. Studies have shown that ulcer size is important for the prognosis of diabetic foot.28,29 This suggests that more attention should be paid to patients with larger ulcers.
Surgical therapy is an independent risk factor for MDRO infection. Surgical therapy can result in changes in the biomechanics of the foot, and the ways in which surgical therapy increase the risk of multidrug-resistant infections remain to be explored. Some studies have shown that diabetic foot patients have a higher mortality rate after amputation.30–32 Amputation should be the last option, which can be devastating for patients with DFU. Timely vascular reconstruction and standardized debridement can effectively prevent amputation.
C-reactive protein is a marker for infection and inflammation, and its levels increase during bacterial infection.33 Our study showed that CRP is an independent risk factor for MDRO infection. The higher the CRP level, the greater the risk of MDRO infection. C-reactive protein is also an independent and strong predictor of cardiovascular diseases.34
This study has some limitations. Specimens were obtained using cotton swabs instead of tissue and bone, but none of the specimens was obtained as superficial swabs. Some studies have shown there is a high concordance rate between swab and deep tissue cultures.35,36 More than 95% of patients were diagnosed with different degrees of diabetic peripheral vascular disease and peripheral neuropathy, so these two factors were not included in the study. Despite the above limitations, our study found certain risk factors for DFUs infected with MDROs.
In conclusion, previous hospitalization, ulcer size >4cm2, surgical therapy and CRP were independent risk factors for MDROs infection in diabetic foot patients. Identifying these risk factors can help us identify the high-risk patients of diabetic foot with MDRO infection early. More attention to high-risk patients and more aggressive isolation precautions may reduce the incidence of MDRO infection in diabetic foot patients.
Ethics Statement
This study was approved by the Institutional Review Board of Tianjin Medical University Chu Hsien-I Memorial Hospital. This study is a retrospective non-interventional study, which does not interfere with routine diagnosis and treatment, does not affect any medical rights of patients, and does not increase the risk of patients. Consent was waived because most of the patients could not be found and the research project did not involve personal privacy or commercial interests.
In order to fully protect personal privacy, the names of the included patients were coded, and the medical records were stored in the special computer of the Department of Diabetic Foot, Chu Hsien-I Memorial Hospital of Tianjin Medical University, for researchers’ access only.
We declare that this study is in accordance with the Helsinki Declaration and the information of all patients included in the study was confidential.
Author Contributions
These authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the National Natural Science Foundation of China (81973614).
Disclosure
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Zha ML, Cai JY, Chen HL. A bibliometric analysis of global research production pertaining to diabetic foot ulcers in the past ten years. J Foot Ankle Surg. 2019;58(2):253–259. doi:10.1053/j.jfas.2018.08.052
2. Zhang P, Lu J, Jing Y, Tang S, Zhu D, Bi Y. Global epidemiology of diabetic foot ulceration: a systematic review and meta-analysis (dagger). Ann Med. 2017;49(2):106–116. doi:10.1080/07853890.2016.1231932
3. Fu XL, Ding H, Miao WW, Mao CX, Zhan MQ, Chen HL. Global recurrence rates in diabetic foot ulcers: a systematic review and meta-analysis. Diabetes Metab Res Rev. 2019;35(6):e3160. doi:10.1002/dmrr.3160
4. Walsh JW, Hoffstad OJ, Sullivan MO, Margolis DJ. Association of diabetic foot ulcer and death in a population-based cohort from the United Kingdom. Diabet Med. 2016;33(11):1493–1498. doi:10.1111/dme.13054
5. Al-Rubeaan K, Almashouq MK, Youssef AM, et al. All-cause mortality among diabetic foot patients and related risk factors in Saudi Arabia. PLoS One. 2017;12(11):e0188097. doi:10.1371/journal.pone.0188097
6. Rastogi A, Goyal G, Kesavan R, et al. Long term outcomes after incident diabetic foot ulcer: multicenter large cohort prospective study (EDI-FOCUS investigators) epidemiology of diabetic foot complications study: epidemiology of diabetic foot complications study. Diabetes Res Clin Pract. 2020;162:108113. doi:10.1016/j.diabres.2020.108113
7. Gazzaruso C, Gallotti P, Pujia A, Montalcini T, Giustina A, Coppola A. Predictors of healing, ulcer recurrence and persistence, amputation and mortality in type 2 diabetic patients with diabetic foot: a 10-year retrospective cohort study. Endocrine. 2021;71(1):59–68. doi:10.1007/s12020-020-02431-0
8. Moulik PK, Mtonga R, Gill GV. Amputation and mortality in new-onset diabetic foot ulcers stratified by etiology. Diabetes Care. 2003;26(2):491–494. doi:10.2337/diacare.26.2.491
9. Singh N, Armstrong DG, Lipsky BA. Preventing foot ulcers in patients with diabetes. JAMA. 2005;293(2):217–228. doi:10.1001/jama.293.2.217
10. Chen D, Wang M, Shang X, et al. Development and validation of an incidence risk prediction model for early foot ulcer in diabetes based on a high evidence systematic review and meta-analysis. Diabetes Res Clin Pract. 2021;180:109040. doi:10.1016/j.diabres.2021.109040
11. Berbudi A, Rahmadika N, Tjahjadi AI, Ruslami R. Type 2 diabetes and its impact on the immune system. Curr Diabetes Rev. 2020;16(5):442–449. doi:10.2174/1573399815666191024085838
12. Rastogi A, Mukhopadhyay S, Sahoo JP, et al. Intensive glycemic control for diabetic foot ulcer healing: a multicentric, randomized, parallel arm, single-blind, controlled study protocol (INGLOBE study). Int J Low Extrem Wounds;2020. 1534734620952245. doi:10.1177/1534734620952245
13. Marik PE, Bellomo R. Stress hyperglycemia: an essential survival response! Crit Care. 2013;17(2):305. doi:10.1186/cc12514
14. Tobalem M, Uckay I. Images in clinical medicine. Evolution of a diabetic foot infection. N Engl J Med. 2013;369(23):2252. doi:10.1056/NEJMicm1211053
15. Matta-Gutiérrez G, García-Morales E, García-álvarez Y, Álvaro-afonso FJ, Molines-Barroso RJ, Lázaro-Martínez JL. The influence of multidrug-resistant bacteria on clinical outcomes of diabetic foot ulcers: a systematic review. J Clin Med. 2021;10(9):1948. doi:10.3390/jcm10091948
16. Henig O, Pogue JM, Martin E, et al. The impact of multidrug-resistant organisms on outcomes in patients with diabetic foot infections. Open Forum Infect Dis. 2020;7(5):ofaa161. doi:10.1093/ofid/ofaa161
17. Saltoglu N, Surme S, Ezirmik E, et al. The effects of antimicrobial resistance and the compatibility of initial antibiotic treatment on clinical outcomes in patients with diabetic foot infection. Int J Low Extrem Wounds. 2021;15347346211004141. doi:10.1177/15347346211004141
18. Sannathimmappa MB, Nambiar V, Aravindakshan R, et al. Diabetic foot infections: profile and antibiotic susceptibility patterns of bacterial isolates in a tertiary care hospital of Oman. J Educ Health Promot. 2021;10:254. doi:10.4103/jehp.jehp_1552_20
19. Mashaly M, Kheir MAE, Ibrahim M, Khafagy W. Aerobic bacteria isolated from diabetic foot ulcers of Egyptian patients: types, antibiotic susceptibility pattern and risk factors associated with multidrug-resistant organisms. Germs. 2021;11(4):570–582. doi:10.18683/germs.2021.1292
20. Yan X, Song JF, Zhang L, Li X. Analysis of risk factors for multidrug-resistant organisms in diabetic foot infection. BMC Endocr Disord. 2022;22(1):46. doi:10.1186/s12902-022-00957-0
21. Rastogi A, Sukumar S, Hajela A, et al. The microbiology of diabetic foot infections in patients recently treated with antibiotic therapy: a prospective study from India. J Diabetes Complications. 2017;31(2):407–412. doi:10.1016/j.jdiacomp.2016.11.001
22. Monteiro-Soares M, Russell D, Boyko EJ, et al. Guidelines on the classification of diabetic foot ulcers (IWGDF 2019). Diabetes Metab Res Rev. 2020;36(Suppl 1):e3273.
23. Lipsky BA, Berendt AR, Cornia PB, et al. 2012 infectious diseases society of America clinical practice guideline for the diagnosis and treatment of diabetic foot infections. Clin Infect Dis. 2012;54(12):e132–173. doi:10.1093/cid/cis346
24. Magiorakos AP, Srinivasan A, Carey RB, et al. Multidrug-resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clin Microbiol Infect. 2012;18(3):268–281. doi:10.1111/j.1469-0691.2011.03570.x
25. Ji X, Jin P, Chu Y, Feng S, Wang P. Clinical characteristics and risk factors of diabetic foot ulcer with multidrug-resistant organism infection. Int J Low Extrem Wounds. 2014;13(1):64–71. doi:10.1177/1534734614521236
26. Neubeiser A, Bonsignore M, Tafelski S, et al. Mortality attributable to hospital acquired infections with multidrug-resistant bacteria in a large group of German hospitals. J Infect Public Health. 2020;13(2):204–210. doi:10.1016/j.jiph.2019.07.025
27. Barrasa-Villar JI, Aibar-Remón C, Prieto-Andrés P, Mareca-Doñate R, Moliner-Lahoz J. Impact on morbidity, mortality, and length of stay of hospital-acquired infections by resistant microorganisms. Clin Infect Dis. 2017;65(4):644–652. doi:10.1093/cid/cix411
28. Zimny S, Schatz H, Pfohl M. The effects of ulcer size on the wound radius reductions and healing times in neuropathic diabetic foot ulcers. Exp Clin Endocrinol Diabetes. 2004;112(4):191–194. doi:10.1055/s-2004-817932
29. Oyibo SO, Jude EB, Tarawneh I, et al. The effects of ulcer size and site, patient’s age, sex and type and duration of diabetes on the outcome of diabetic foot ulcers. Diabet Med. 2001;18(2):133–138. doi:10.1046/j.1464-5491.2001.00422.x
30. Thorud JC, Plemmons B, Buckley CJ, Shibuya N, Jupiter DC. Mortality after nontraumatic major amputation among patients with diabetes and peripheral vascular disease: a systematic review. J Foot Ankle Surg. 2016;55(3):591–599. doi:10.1053/j.jfas.2016.01.012
31. Cascini S, Agabiti N, Davoli M, et al. Survival and factors predicting mortality after major and minor lower-extremity amputations among patients with diabetes: a population-based study using health information systems. BMJ Open Diabetes Res Care. 2020;8(1):e001355. doi:10.1136/bmjdrc-2020-001355
32. Hoffstad O, Mitra N, Walsh J, Margolis DJ. Diabetes, lower-extremity amputation, and death. Diabetes Care. 2015;38(10):1852–1857. doi:10.2337/dc15-0536
33. Sproston NR, Ashworth JJ. Role of C-reactive protein at sites of inflammation and infection. Front Immunol. 2018;9:754. doi:10.3389/fimmu.2018.00754
34. Avan A, Tavakoly Sany SB, Ghayour-Mobarhan M, Rahimi HR, Tajfard M, Ferns G. Serum C-reactive protein in the prediction of cardiovascular diseases: overview of the latest clinical studies and public health practice. J Cell Physiol. 2018;233(11):8508–8525. doi:10.1002/jcp.26791
35. Huang Y, Cao Y, Zou M, et al. A comparison of tissue versus swab culturing of infected diabetic foot wounds. Int J Endocrinol. 2016;2016:8198714. doi:10.1155/2016/8198714
36. Andrianaki AM, Koutserimpas C, Kafetzakis A, et al. Diabetic foot infection and osteomyelitis. Are deep-tissue cultures necessary? Germs. 2020;10(4):346–355. doi:10.18683/germs.2020.1227
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.