Back to Journals » Journal of Asthma and Allergy » Volume 15
Risk Factors for Immediate-Type Local Anesthetic Hypersensitivity Reactions in Pediatric Patients: A Retrospective Case-Control Study
Authors Suleyman A ![]() , Tamay Z, Guler N
, Tamay Z, Guler N
Received 18 December 2021
Accepted for publication 30 March 2022
Published 8 April 2022 Volume 2022:15 Pages 453—460
DOI https://doi.org/10.2147/JAA.S349637
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Luis Garcia-Marcos
Ayse Suleyman, Zeynep Tamay, Nermin Guler
Istanbul University, Istanbul Faculty of Medicine, Department of Pediatrics, Division of Pediatric Allergy and Immunology, Istanbul, Turkey
Correspondence: Ayse Suleyman, Istanbul University, Istanbul Faculty of Medicine, Department of Pediatrics, Division of Pediatric Allergy and Immunology, Capa, Istanbul, Turkey, Tel +90 535 4160702, Email [email protected]
Background: Local anesthetics (LA) are relatively safe and rarely cause immediate hypersensitivity reactions. The data on immediate LA hypersensitivity and its risk factors in children are limited.
Aim: To evaluate risk factors of immediate LA hypersensitivity.
Methods: The retrospective case-controlled study included 17 patients with confirmed immediate LA hypersensitivity. For each patient, three age- and gender-matched control subjects were included in the study. LA hypersensitivity was excluded by skin tests and subcutaneous drug provocation tests in all control subjects.
Results: The most common allergic assessment in the patient/control group was for lidocaine (n=5; 29.4%, vs n=23; 45.1%). Suspected LA hypersensitivity reactions were found to be associated with cutaneous manifestations in 14 (82.4%) patients and in 7 (13.7%) of the controls. A history of exposure to local anesthetics twice or more was present in 11 (64.7%) patients vs 6 (11.8%) controls. In conditional regression analysis, repeated LA exposure (≥ 2) and cutaneous findings were determined as significant risk factors (Odds Ratio [OR]:5.7; 95% Confidence Interval [CI]:1.2– 27.1; P=0.029 and (OR:17.3; 95% CI:3.6– 82.5; P< 0.001, respectively).
Conclusion: Cutaneous manifestations and a history of LA exposure twice or more were predictive factors for LA allergy confirmed by skin test in children.
Keywords: local anesthetic, immediate reactions, hypersensitivity, predictive factors, skin test, subcutaneous provocation test, children
Introduction
Local anesthetics (LA) are commonly used in outpatients to prevent and relieve pain in dental and minor surgical procedures and are even used topically in children prior to painful procedures such as intramuscular injections or catheterization.1–4 LA are divided into amide or ester groups according to their chemical structures.5–7 In broad patient series and pharmacological vigilance studies, immunoglobulin (Ig)E-mediated reactions to LA, particularly to those of amide class, have been reported to be rare.8–18
Immediate symptoms after the use of LA may be associated with anxiety, presyncope/syncope, toxicity from intravascular administration or overdose, reactions to co-administered substances such as epinephrine and methylparaben, and allergies to latex, chlorhexidine, or other drugs.9,14,18 Immediate LA-hypersensitivity reactions (HR), though rare, have also been reported as a cause of anaphylaxis.16,19–22 Moreover, patients necessitating evaluation for anaphylaxis-like symptoms after the use of LA are disproportionately common.18
Detailed history and physical examination are the first steps in the evaluation of drug allergy. In most cases, patient history is taken months or years after the occurrence of the reaction and the findings usually disappear during the examination. Therefore, patient history and examination are not sufficient for the diagnosis of drug allergy23,24 Although patient history is inadequate in diagnosing drug allergy, it is crucial to differentiate between non-allergic and possible allergic reactions, classify immunologically, and determine subsequent investigations. Skin tests (STs) performed for LA are the most widely preferred tools in the first stage of allergic assessment.24,25 However, subcutaneous drug provocation tests (DPTs) provide more precise results in patients without contraindications to confirm or exclude the diagnosis.24 These tests should be performed with solutions that do not contain vasoconstrictors since these substances may cause false tests results.23–25
Some risk factors for LA-HR, such as multiple drug allergies and mastocytosis, have been studied in adults.27,28 IgE-mediated LA allergy is highly rare in children and pediatric studies are few in the current literature.17,29 To our knowledge, there is not enough data evaluating risk factors for immediate LA-HR allergy in children. Furthermore, it is not always possible to apply adult data to pediatric patients. We investigated risk factors to predict LA hypersensitivity using a case-controlled study design.
Materials and Methods
Setting
Istanbul Faculty of Medicine is located in a socioeconomically and ethnically diverse area of Istanbul. The Division of Pediatric Allergy and Immunology in our University Hospital serves as the tertiary referral center in Istanbul. As a routine practice, children requiring allergic evaluation are admitted to our unit after undergoing a preliminary assessment in general pediatric outpatient clinic.
Patients and Controls
The retrospective and case-controlled study included 17 patients admitted to Istanbul University Faculty of Medicine, Pediatric Allergy Unit, and were confirmed to have immediate local anesthetic hypersensitivity by allergic evaluation between May 2010 and May 2020. A total of 51 controls, involving three age- and gender-matched children for each patient, who were selected among subjects who had been admitted at the closest date were included in the study. Controls were selected from children who applied to our pediatric allergy outpatient clinic with a history of suspected reaction to a local anesthetic and were found to be tolerant after allergic evaluation (skin and provocation tests). Immediate LA hypersensitivity was defined as the presence of clinically compatible findings and positive responses in STs and/or DPTs. LA hypersensitivity was excluded in patients who were found negative for both tests (STs and/or DPTs).
The Ethics Committee of Istanbul University, Istanbul Faculty of Medicine approved the study protocol (No: 2020/1559). Written informed consents were taken from parents and/or patients before allergic workups. The study was carried out in accordance with the Helsinki Declaration.
Data Collection
Demographic and clinical data were obtained using the European Network for Drug Allergy (ENDA) questionnaire.26 A detailed history including the culprit drug, and data on the spectrum and timing of the symptoms was obtained from each participant. In addition, the presence of previous drug reactions, family history of drug allergy, and concomitant chronic or atopic diseases were investigated. All data were obtained from medical records. Only children with complete and accurate clinical records were included in the study. Participants whose allergic evaluation for LA-HR could not be completed due to uncontrolled asthma, severe skin reaction, and parents’ refusal were excluded from the study.
Diagnostic Evaluation
Allergic assessments were performed within a minimum period of four weeks after suspected reactions. Prior to the tests, drugs that could affect the results were discontinued as recommended.23,-26 The patients were initially given a skin prick test (SPT) with LA; if negative, an intradermal test (IDT) was performed. If both tests were negative, DPT was applied.2 Patients with confirmed LA hypersensitivity subsequently underwent an allergic assessment with a safe alternative LA. Preservative and adrenaline-free vials were used for STs (prick and intradermal) and subcutaneous provocation test.2,7
Local Anesthetic Skin Tests
Skin tests were performed with a local anesthetic suspected to be responsible for the clinical reactions described. The drugs were used in the tests as follows: lidocaine 2%, 20 mg/mL; mepivacaine 3%, 30 mg/mL; prilocaine 2%, 20 mg/mL; articaine 2%, 20mg/mL. SPT was considered positive when the diameter of the wheal with surrounding erythema was at least 3 mm or larger than the negative control after 20 minutes.2,7,23 In the case of a negative SPT, IDTs were performed on the volar forearm (0.02 mL). After 20 minutes, IDT was evaluated and considered positive if the mean diameter of the bleb with surrounding erythema increased by ≥3 mm. IDTs were initiated at a concentration of 1:1000 mg/mL and reached 1:10 mg/mL in gradual increments. Histamine (10 mg/mL) was used as the positive control and 0.9%NaCl was used as the negative control.2,7
Subcutaneous Provocation Tests
Subcutaneous provocation tests were performed on patients who had a negative STs result for LA. Provocation tests were performed with the drugs used in SPTs at full concentration. DPT was administered as a single dose on the same day in two (0.1 mL and 1 mL) or three steps (0.01 mL, 0.1 mL, and 1 mL), at 30-minute intervals on the volar forearm. Due to ethical concerns, it was not applied to patients with positive STs. Patients were observed for at least two hours after the last injection.
Evaluation of Non-Local Anesthetic Drug Allergy
In the allergic evaluation of non-LA drug allergy, ENDA guidelines were strictly followed.24–26
Statistical Analysis
Statistical analyses were conducted using SPSS 23.0 software (Armonk, NY: IBM Corp.). Normal distribution of continuous variables was assessed using the skewness-kurtosis and the Kolmogorov–Smirnov test or Shapiro–Wilks test. Continuous variables with nonnormal distribution were expressed as median and interquartile range (IQR). Pearson’s Chi-Square test or Fisher’s exact test was used to compare categorical data. Initially, univariate regression analysis was used to describe the association of clinical risk factors and confirmed LA hypersensitivity. Subsequently, parameters that were found significant in univariate analysis were evaluated by conditional multivariate regression analysis. Results were presented as Odds Ratio (OR) with 95% Confidence Interval (CI), and a P value of <0.05 was considered significant.
Results
Median age was 8 (Interquartile range [IQR]: 6–11) years in patients and 9 (IQR: 6–12) years in controls. Eight of the patients and 24 of the controls were female. Median time between index reaction and allergic evaluation was 7 (IQR: 4–10) months in patients and 8 (IQR: 6.5–13) months in controls (P=0.232).
Lidocaine was the most common suspected agent in the patient group (n=5; 28.9%) and controls (n=23; 45.1%). Reactions with more than one local anesthetic were reported in 23.5% (n=4) of the patients and in 2% (n=1) of the controls.
In the patient group, 2 (11.8%) of the patients were diagnosed as having anaphylaxis (articaine in one and lidocaine in the other), 1 (5.9%) patient reported itching of the throat without shortness of breath, and the remaining 14 (82.4%) patients reported urticaria or urticaria-angioedema. In the control group, 7 (13.5%) subjects had urticaria-angioedema and the remaining 44 (86.5%) subjects had systemic or local findings that were not fully compatible with allergy.
Local anesthetic (LA) hypersensitivity was confirmed by SPT in 1 (5.9%) patient (accompanied by urticaria) and by IDT at a concentration of 1:100 in 9 (52.9%) and by 1:10 in 7 (41.2%) patients (Figure 1). Detailed characteristics of the patients are shown in the Supplementary Table. In the control subjects, LA-HR was excluded by STs and subcutaneous DPTs. During SPTs, bradycardia and pallor, which were accepted as clinical signs of a vasovagal reaction, were detected in 2 (3.9%) controls. No reaction was observed in the DPTs of both subjects. Moreover, the tryptase levels were within normal limits. Confirmation rates of non-LA drug allergy was 11.8% (non-steroidal anti-inflammatory drugs [NSAID]-paracetamol, n=2) in the patient group and 9.8% (β-lactam, n=3; NSAID, n=2) in controls.
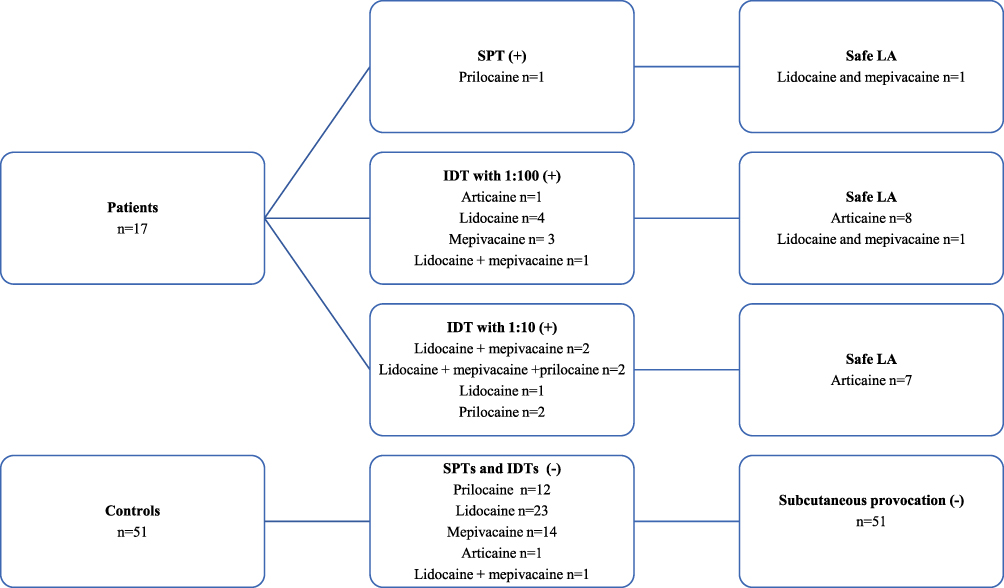 |
Figure 1 Results of allergic evaluation of the children (patients and controls) with suspected reactions to local anesthetics. Safe LA was determined by skin and drug provocation tests. Mepivacaine and lidocaine were determined as safe local anesthetics in the patient whose skin test was positive with articaine. Abbreviations: IDT: intradermal test, LA: local anesthetic; SPTs: skin prick tests, |
Comparison of the patients and controls showed the following risk factors: reactions to more than one local anesthetic (OR: 15.4; 95% CI:1.6–149.6; P=0.019), history of previous exposure to LA twice or more (OR:13.7; 95% CI: 3.7–50.9; P<0.001), and presence of cutaneous manifestations (OR:29.3; 95% CI: 6.7–128.9; P<0.001) (Table 1). There was no difference between the patients and controls in terms of the rates of subjects who underwent LA allergy assessment within the first year after suspected LA reaction, the prevalence of personal atopic and chronic diseases, confirmed non-LA drug allergy, and presence of a family history of drug allergy. Table 1 presents clinical characteristics of patients and controls.
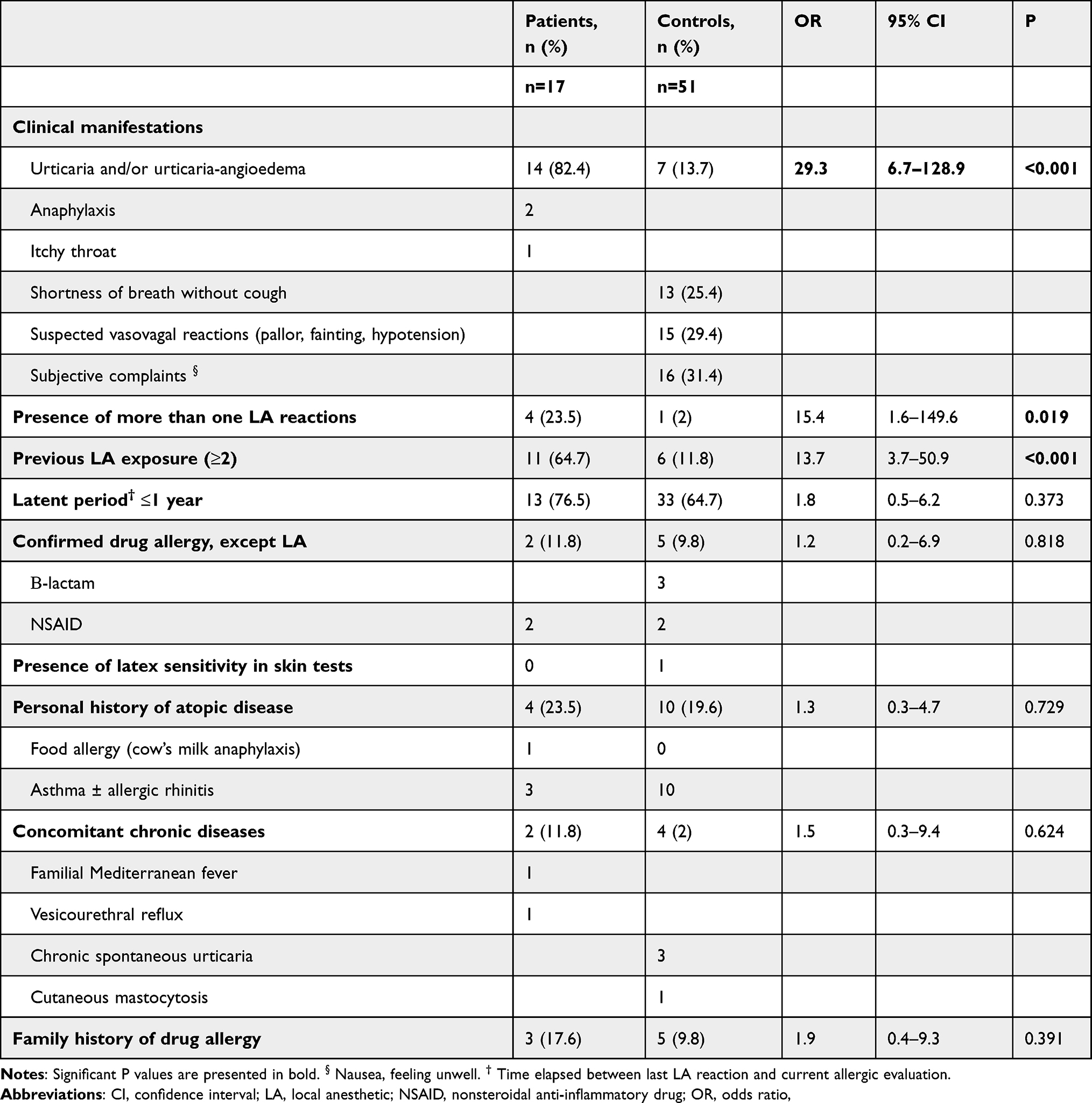 |
Table 1 Comparison of Clinical Characteristic of the Patients and Matched Controls |
Parameters that were included in the conditional multivariate analysis (presence of cutaneous manifestations, presence of more than one local anesthetic reaction, and previous exposure to LA twice or more) are listed in Table 2. The analysis indicated that the variables that were significant in predicting an LA-HR included a history of LA-HR with cutaneous manifestations (OR:17.3; 95% CI: 3.6–82.5; P<0.001) and presence of exposure to LA twice or more (OR: 5.7; 95% CI:1.2–27.7; P=0.029).
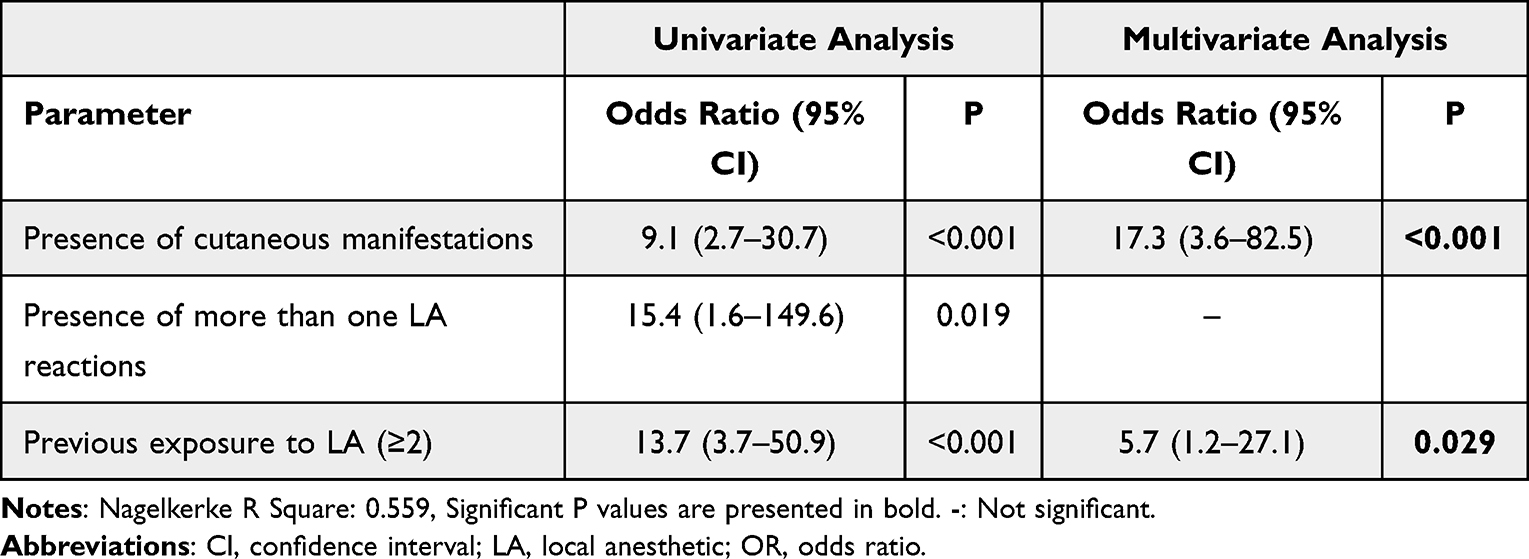 |
Table 2 Risk Factors for Local Anesthetic Hypersensitivity |
Discussion
This case-control study compared the clinical findings of 17 patients with confirmed LA hypersensitivity and 51 age- and gender-matched controls. A history of reactions accompanied by skin findings and prior exposure to LA twice or more were identified as independent risk factors for LA-HR.
Immediate LA allergy was shown to be remarkably rare in two recently published large series. Of these, a recent Danish study on perioperative allergies evaluated 162 patients who underwent subcutaneous DPTs and reported that none of theicases of immediate allergy to LA were confirmed over the ten-year period.14 The other study evaluated 402 patients among whom most of the patients had a reaction within 30 minutes of LA injection during outpatient treatment (dental or surgical procedures) at a German allergy clinic over a 20-year period and reported that only two patients had a confirmed LA allergy.18 In a pediatric study conducted in Turkey, however, LA allergy was confirmed in only 1 out of 73 patients.17
Although there are a large number of patients with suspected LA-HR, only a small percentage of them are confirmed, which can be explained in several ways. The first possibility is that a hypersensitivity reaction that results from a non-LA factor such as non-LA drugs or additives, foods, latex, and disinfectants might be incorrectly diagnosed as LA-HR. Studies evaluating LA allergy have reported that non-LA causes account for 1.7–32% of all causes, depending on the process requiring LA administration.9,14,18 In our study, there was no significant difference between the patients and controls with regard to confirmed drug allergy to NSAID or β-lactams. Another explanation is that non-allergic side effects may mimic clinical features of LA-HR. These effects may develop due to the LA itself or due to the adrenaline contained in the solution. Adrenaline-related effects also cause symptoms such as anxiety or fear of the dentist.18 These symptoms can easily be misdiagnosed as anaphylaxis by inexperienced clinicians.
Urticaria-angioedema is the most common skin manifestation of immediate drug allergy. Immediate LA-HRs have been reported to be more common in adult patients than in children.18 Our results showed that an immediate-type reaction with skin manifestations is a predictive factor of ST positivity in LA-HR. We also identified two or more LA exposures as independent risk factors for confirmed LA-HR. We attributed this situation to the fact that repeated LA exposures may have caused IgE-mediated sensitization.
It is well known that patient history is unreliable in the diagnosis of drug allergies. Therefore, as with other drug allergies, an allergic evaluation is necessary to confirm or often rule out LA allergy. STs and DPTs are widely used in clinical practice for the diagnosis of LA allergy, whereas specific IgE assessments and basophil activation testing are not common.7,18
Literature recommends that STs should be performed without preservatives and with solutions that do not contain vasoconstrictors such as adrenaline. However, positive results have been reported even with solutions containing adrenaline.9 In adult patients, the IDT performed at a concentration of 1:10 has been reported to have a sensitivity of 100% and a specificity of 94.5%. For this reason, in the case of positive IDT at a concentration of 1:10, it is recommended to repeat the test at a concentration of 1:100 and provoke the negative ones. We considered that some of the positive results obtained at the titer of 1:10 in patients who were found negative at 1:100 titer, might be false-positive. In our clinical practice, we accepted that IDT-positive patients had LA allergies and considered that it would not be ethical to perform DPT in these patients. Therefore, we could not distinguish true LA allergy from irritation or LA sensitivity in our IDT-positive patients at a concentration of 1:10. In our study, we had a higher diagnosis confirmation rate than those reported in the literature, which could be explained by the probability of false positivity by irritation. Considering that irritation of the skin is much more probable in children, this result is not surprising. A second explanation could be that patients with high allergy risk are referred to us since our institution is a tertiary referral center.
Subcutaneous DPT is the gold standard for the diagnosis of LA allergy in patients without contraindications. However, the general problem with DPTs is that the number of steps (one to six) and initial concentrations are considerably different. It has been reported that in selected patients with a history of reaction to LA and negative STs (prick and IDT) results, an alternative LA could safely be identified using a short protocol or only a single-dose subcutaneous provocation.1,2
Local anesthetics (LA) are low-molecular-weight substances (<300 Daltons) and have no commercial antigenic determinants.7 Ester LA are converted in plasma by pseudocholinesterase to the para-aminobenzoic acid metabolite, which is considered to be responsible for allergy via haptenization. Some amide solutions may contain a preservative, methylparaben, and their structure is similar to that of para-aminobenzoic acid.30 Parabens are often associated with late reactions (contact dermatitis). In some case reports, amide and ester have been shown to be a cause of immediate reactions in patients with LA sensitivity.5,7,30 In another case report, a case of delayed reaction with lidocaine, mepivacaine, and bupivacaine was shown in amide LA, where the common antigenic epitope may be meta-xylene.31 In our study, we detected allergic reactions to more than one LA and articaine tolerance in four patients, which implies that meta-xylene as an antigenic epitope may play a role in immediate reactions in addition to delayed reactions.
The most important limitation of our study was that it was conducted in a single tertiary center. Therefore, it may not be representative of the general population. In addition, the evaluations of LA-HR were made retrospectively depending on the clinical needs of the patients, not on the purpose of the study. DPT was not performed for ethical reasons in patients with a positive skin test; therefore, true LA allergy and irritation could not be distinguished.
In conclusion, the present study demonstrated that hypersensitivity reactions with cutaneous findings following LA administration and recurrent LA exposures are predictors of ST positivity in LA allergy. Diagnosis of LA allergy based on ST positivity may cause overestimation of confirmed LA allergy in children due to the possibility of irritation.
Author Contribitions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest.
References
1. Peroni D, Pasini M, Iurato C, Cappelli S, Giuca G, Giuca MR. Allergic manifestations to local anaesthetic agents for dental anaesthesia in children: a review and proposal of a new algorithm. Eur J Paediatr Dent. 2019;20(1):48–52. doi:10.23804/ejpd.2019.20.01.10
2. Bhole MV, Manson AL, Seneviratne SL, Misbah SA. IgE-mediated allergy to local anaesthetics: separating fact from perception: a UK perspective [published correction appears in Br J Anaesth. 2012;109(4):669]. Br J Anaesth. 2012;108(6):903–911. doi:10.1093/bja/aes162
3. Sridharan K, Sivaramakrishnan G. Pharmacological interventions for reducing pain related to immunization or intramuscular injection in children: a mixed treatment comparison network meta-analysis of randomized controlled clinical trials. J Child Health Care. 2018;22(3):393–405. doi:10.1177/1367493518760735
4. Gupta NK, Upadhyay A, Dwivedi AK, Agarwal A, Jaiswal V, Singh A. Randomized controlled trial of topical EMLA and vapocoolant spray for reducing pain during wDPT vaccination. World J Pediatr. 2017;13(3):236–241. doi:10.1007/s12519-017-0004-y
5. Ramsey A, Brodine AH. Allergy topics for dental practitioners. Gen Dent. 2019;67(4):38–45.
6. Lirk P, Hollmann MW, Strichartz G. The science of local anesthesia: basic research, clinical application, and future directions. Anesth Analg. 2018;126(4):1381–1392. doi:10.1213/ANE.0000000000002665
7. Malinovsky JM, Chiriac AM, Tacquard C, Mertes PM, Demoly P. Allergy to local anesthetics: reality or myth? Presse Med. 2016;45(9):753–757. doi:10.1016/j.lpm.2016.05.011
8. Koca Kalkan I, Koycu Buhari G, Ates H, et al. Identification of risk factors and cross-reactivity of local anesthetics hypersensitivity: analysis of 14-Years’ experience. J Asthma Allergy. 2021;14:47–58. doi:10.2147/JAA.S292442
9. Harboe T, Guttormsen AB, Aarebrot S, Dybendal T, Irgens A, Florvaag E. Suspected allergy to local anaesthetics: follow-up in 135 cases. Acta Anaesthesiol Scand. 2010;54(5):536–542. doi:10.1111/j.1399-6576.2009.02193.x
10. Venemalm L, Degerbeck F, Smith W. IgE-mediated reaction to mepivacaine. J Allergy Clin Immunol. 2008;121(4):1058–1159. doi:10.1016/j.jaci.2007.12.1154
11. Fuzier R, Lapeyre-Mestre M, Samii K, Montastruc JL. French association of regional pharmacovigilance centres. Adverse drug reactions to local anaesthetics: a review of the French pharmacovigilance database. Drug Saf. 2009;32(4):345–356. doi:10.2165/00002018-200932040-00008
12. Fuzier R, Lapeyre-Mestre M, Mertes PM, et al. Immediate- and delayed-type allergic reactions to amide local anesthetics: clinical features and skin testing. Pharmacoepidemiol Drug Saf. 2009;18(7):595–601. doi:10.1002/pds.1758
13. Kvisselgaard AD, Mosbech HF, Fransson S, Garvey LH. Risk of immediate-type allergy to local anesthetics is overestimated-results from 5 years of provocation testing in a Danish allergy clinic. J Allergy Clin Immunol Pract. 2018;6(4):1217. doi:10.1016/j.jaip.2017.08.010
14. Kvisselgaard AD, Krøigaard M, Mosbech HF, Garvey LH. No cases of perioperative allergy to local anaesthetics in the Danish anaesthesia allergy centre. Acta Anaesthesiol Scand. 2017;61(2):149. doi:10.1111/aas.12833
15. Broyles AD, Banerji A, Barmettler S, et al. Practical Guidance for the Evaluation and Management of Drug Hypersensitivity: Specific Drugs [published correction appears in J Allergy Clin Immunol Pract. 2021 Jan;9(1):603] [published correction appears in J Allergy Clin Immunol Pract. 2021 Jan;9(1):605]. J Allergy Clin Immunol Pract. 2020;8(9S):S16-S116. doi:10.1016/j.jaip.2020.08.06.
16. Domínguez-Ortega J, Phillips-Angles E, González-Muñoz M, et al. Allergy to several local anesthetics from the amide group. J Allergy Clin Immunol Pract. 2016;4(4):771. doi:10.1016/j.jaip.2016.02.009
17. Selmanoglu A, Güvenir H, Celik IK, et al. Immediate local anesthetic reactions and diagnostic test results in pediatric patients. Allergol Immunopathol. 2021;49(3):108–114. doi:10.15586/aei.v49i3.87
18. Trautmann A, Goebeler M, Stoevesandt J. Twenty years’ experience with anaphylaxis-like reactions to local anesthetics: genuine allergy is rare. J Allergy Clin Immunol Pract. 2018;6(6):2051–8.e1. doi:10.1016/j.jaip.2018.04.005
19. Wieshuber C, Stoevesandt J, Trautmann A. The needle in the haystack: allergic anaphylaxis caused by the local anesthetic articaine. Eur Ann Allergy Clin Immunol. 2014;46(1):38.
20. Al-Dosary K, Al-Qahtani A, Alangari A. Anaphylaxis to lidocaine with tolerance to articaine in a 12-year-old girl. Saudi Pharm J. 2014;22(3):280–282. doi:10.1016/j.jsps.2013.10.001
21. Caron AB. Allergy to multiple local anesthetics. Allergy Asthma Proc. 2007;28(5):600–601. doi:10.2500/aap2007.28.3035
22. Carrión Sari SK, Lezaun A, Colas Sanz C. Anaphylaxis due to perioperative intravenous lidocaine. J Investig Allergol Clin Immunol. 2021;31(2):164–165. doi:10.18176/jiaci.0626
23. Demoly P, Adkinson NF, Brockow K, Castells M, Chiriac AM, Greenberger PA. International consensus on drug allergy. Allergy. 2014;69(4):420–437. doi:10.1111/all.12350
24. Gomes ER, Brockow K, Kuyucu S, et al. Drug hypersensitivity in children: report from the pediatric task force of the EAACI Drug allergy interest group. Allergy. 2016;71(2):149–161. doi:10.1111/all.12774
25. Brockow K, Garvey LH, Aberer W, et al. Skin test concentrations for systemically administered drugs – an ENDA/EAACI Drug allergy interest group position paper. Allergy. 2013;68(6):702. doi:10.1111/all.12142
26. Brockow K, Ardern-Jones MR, Mockenhaupt M, et al. EAACI position paper on how to classify cutaneous manifestations of drug hypersensitivity. Allergy. 2019;74(1):14–27. doi:10.1111/all.13562
27. Yilmaz I, Özdemir SK, Aydin Ö, Çelik GE. Local anesthetics allergy: who should be tested? Eur Ann Allergy Clin Immunol. 2018;50(2):66–71. doi:10.23822/EurAnnACI.1764-1489.38
28. Bonadonna P, Olivieri E, Zanotti R, et al. Is the local anaesthetics a risk factor of anaphylaxis in mastocytosis patients? J Allergy Clin Immunol. 2020;145(2):AB238. doi:10.1016/j.jaci.2019.12.130
29. Duyuler Ayçin G. Local anesthetics allergies in children. Iran J Pediatr. 2020;30(1):e98213.
30. Macy E, Schatz M, Zeiger RS. Immediate hypersensitivity to methylparaben causing false-positive results of local anesthetic skin testing or provocative dose testing. Perm J. 2002;6(4):17–21.
31. Ing Lorenzini K, Gay-Crosier Chabry F, Piguet C, Desmeules J. Meta-xylene: identification of a new antigenic entity in hypersensitivity reactions to local anesthetics. J Allergy Clin Immunol Pract. 2016;4(1):162. doi:10.1016/j.jaip.2015.08.005
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.