Back to Journals » Therapeutics and Clinical Risk Management » Volume 22
Risk Factors for Hypoglycemia in Type 2 Diabetes Mellitus Patients Using Once-Weekly Semaglutide: A Matched Case-Control Study
Authors Amirthalingam P ![]() , Alarawi FA, Jassas Alagwar LM
, Alarawi FA, Jassas Alagwar LM ![]() , Alatawi MS, Saeed Alfahmi Alzahrani MS
, Alatawi MS, Saeed Alfahmi Alzahrani MS ![]() , A Albalwi AO, Alrashidi A, Elsaid Hamdan AM
, A Albalwi AO, Alrashidi A, Elsaid Hamdan AM ![]() , Fahad Alqifari S
, Fahad Alqifari S ![]() , Alshareef H
, Alshareef H ![]() , Aljabri A
, Aljabri A ![]() , Sirag N
, Sirag N ![]() , Pakkir Mohamed SH
, Pakkir Mohamed SH ![]() , Ali MAS
, Ali MAS ![]()
Received 19 March 2026
Accepted for publication 24 May 2026
Published 4 June 2026 Volume 2026:22 610579
DOI https://doi.org/10.2147/TCRM.S610579
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Garry Walsh
Palanisamy Amirthalingam,1 Fawaz Ahmed Alarawi,2 Loay Mohammed Jassas Alagwar,2 Mohammed Sulaiman Alatawi,2 Mohanad Saleh Saeed Alfahmi Alzahrani,2 Ali Oudah A Albalwi,3 Ahmed Alrashidi,3 Ahmed Mohsen Elsaid Hamdan,4 Saleh Fahad Alqifari,1 Hanan Alshareef,1 Ahmed Aljabri,5 Nizar Sirag,6 Shahul Hameed Pakkir Mohamed,7,8 Mostafa A Sayed Ali1
1Department of Pharmacy Practice, Faculty of Pharmacy, University of Tabuk, Tabuk, Saudi Arabia; 2Pharm D Program, Faculty of Pharmacy, University of Tabuk, Tabuk, Saudi Arabia; 3Pharmaceutical Care Department, King Fahad Specialist Hospital, Tabuk, Saudi Arabia; 4Department of Pharmacology and Toxicology, Faculty of Pharmacy, University of Tabuk, Tabuk, Saudi Arabia; 5Department of Pharmacy Practice, Faculty of Pharmacy, King Abdulaziz University, Jeddah, Saudi Arabia; 6Department of Natural Products and Alternative Medicine, Faculty of Pharmacy, University of Tabuk, Tabuk, Saudi Arabia; 7Department of Health Rehabilitation Sciences, Faculty of Applied Medical Sciences, University of Tabuk, Tabuk, Saudi Arabia; 8Saveetha College of Physiotherapy, Saveetha Institute of Medical and Technical Sciences (Deemed to be a University), Chennai, Tamil Nadu, India
Correspondence: Palanisamy Amirthalingam, Department of Pharmacy Practice, Faculty of Pharmacy, University of Tabuk, Tabuk, 71491, Saudi Arabia, Email [email protected]
Background: The semaglutide once-weekly injection (Sema-OWI) is widely accepted for managing type-2 diabetes mellitus (T2DM) patients, particularly those seeking weight loss. However, hypoglycemia is continually challenging healthcare practitioners, and the underlying factors have yet to be conclusively reported. The study aimed to investigate the underlying characteristics of T2DM patients undergoing sema-OWI treatment.
Methods: A matched case-control study design was employed with a 1:4 (case:control) ratio. Univariable conditional logistic regression was used for the preliminary analysis of the association between patient characteristics and the occurrence of hypoglycemia using a matched odds ratio (mOR). Then, multivariable conditional logistic regression was performed using the predictors, with adjusted mOR (mORadj), including body mass index (BMI) and glycosylated hemoglobin (HbA1C), adjusted for the significant confounders identified in the univariable conditional logistic regression.
Results: Forty-five cases diagnosed with the hypoglycemic event and 180 controls were recruited according to a 1:4 (case:control) ratio. According to univariable conditional logistic regression, Patients treated with sema-OWI for 4– 6 months (mOR = 0.052; p< 0.001) and more than 6 months (mOR = 0.045; p = 0.001) were least likely to experience hypoglycemia. Obese patients (mOR = 0.110; p = 0.041) and those with an HbA1C level > 9 (mOR = 0.254; p < 0.001) were also least likely to experience hypoglycemia. According to multivariable conditional logistic regression analysis, the model was adjusted for the number of T2DM medications and Sema-OWI duration, confirming that obesity and higher HbA1C levels (> 9) were associated with a lower likelihood of hypoglycemia. On the other hand, the above results establish that the normal body mass index and lower HbA1C levels (< 7) were associated with a higher likelihood of hypoglycemia.
Conclusion: Patients with T2DM treated with sema-OWI require careful monitoring, particularly during the first 3 months. Normal BMI and HbA1C levels < 7 are considered risk factors for hypoglycemia.
Keywords: body mass index, HbA1C, hypoglycemia, semaglutide once-weekly injection, type-2 diabetes mellitus
Introduction
Glucagon-like peptide-1 (GLP-1) is one of the incretin hormones released from the gut, augmenting insulin secretion. Consequently, it inhibits glucagon secretion, leading to improved glycemic control. It also limits weight gain by inhibiting gastric emptying and food intake and increasing nutrient absorption.1 GLP-1 receptor agonists (RAs) have been a milestone in managing type-2 diabetes mellitus (T2DM) since 2005, as exenatide was the first drug introduced in this class, followed by liraglutide, lixisenatide, dulaglutide, semaglutide, and tirzepatide in the respective years 2010, 2013, 2014, 2017, and 2022.2
However, it has been associated with adverse effects, as 14,512 adverse events have been reported in the FDA Adverse Event Reporting System (FAERS) database as of 2023. Adverse effects related to the gastrointestinal tract were predominant (10,214), followed by metabolic and nutrition-related effects (1981), nervous system effects (568), endocrine system effects (458), and hepatobiliary system effects (424). Also, 14.68% were hospitalized due to the severe outcomes of semaglutide.3 Hypoglycemia (0.5%), which requires hospitalization, was reported commonly after gastrointestinal adverse effects in a retrospective observational study.4
Semaglutide, the first GLP-1RAs available in both oral and subcutaneous formulations, has already been widely accepted by physicians for managing patients with T2DM and cardiovascular and renal complications. These patients may already be more vulnerable to hypoglycemia, and this underscores the need to understand its safety profile, including its hypoglycemia risk, across diverse patient populations.5 Though Semaglutide is associated with a lower risk of hypoglycemia as it stimulates insulin secretion in a glucose-dependent manner, meaning it primarily acts when blood glucose levels are elevated and does not cause excessive insulin release during normal or low glucose levels. However, its rapid action lowers the blood sugar level, increasing the risk of hypoglycemia. It rapidly reduces glycosylated hemoglobin (HbA1C) and exerts potent effects on appetite suppression, delayed gastric emptying, and enhanced satiety, contributing to more effective weight loss than other GLP-1 receptor agonists. Therefore, HbA1C and BMI are considered potential key factors in understanding hypoglycemic risk.6–9
The Semaglutide Unabated Sustainability in Treatment of Type 2 Diabetes (SUSTAIN 6) trial reported 23.1% and 21.7% severe or confirmed severe hypoglycemic symptomatic episodes with sema-OWI 0.5 mg and 1 mg, respectively.6 Moreover, real-world data reported that the median onset of hypoglycemia for sema-OWI was two days, and sema-OWI 0.25 mg would typically be initiated for the first four weeks.7 All SUSTAIN trials reported no hypoglycemic events related to the sema-OWI 0.25 mg.8 The global real-world Semaglutide Real-world Evidence (SURE) program reported that 1.3% of hypoglycemic events and 0.1% were severe, particularly in patients with microvascular complications.9 Meanwhile, 42.86% of patients with hypoglycemic events were hospitalized with no fatality report, according to the FAERS database until 2020.7
An observational cohort study from Canada reported no change in patients’ self-reported hypoglycemic events between baseline (4.3%) and follow-up (4.7%). Additionally, hypoglycemic events among T2DM patients were not associated with the co-prescription of sulfonylurea and insulin.10 However, a recent multicenter observational 15-month follow-up study reported that there was a decline in the mean (standard deviation) of hypoglycemic event frequency from the baseline [4.60 (1.10)], followed by 3 months [2.30 (0.80)], 6- and 12-month follow-up [0.80 (0.50)].11 The varying hypoglycemic rates of Sema-OWI between trials and real-world data were influenced by various factors, including combination with other antidiabetic therapies, patient characteristics, dosage, and real-world factors.7–11
As mentioned above, numerous uncertainties remain regarding the causal relationship between sema-OWI and hypoglycemia, with various underlying factors, such as the onset of the event, dose, and follow-up.7 In this context, the present study aimed to investigate the clinical characteristics of hospitalized T2DM patients who experienced hypoglycemic events, after matching them with T2DM patients who had no incidence of hypoglycemia. Additionally, the influence of sociodemographic characteristics on this aspect was also investigated.
Methods
Study Design and Site
A matched case-control study was conducted from November 2024 to April 2025 in a Government Hospital in Tabuk, Saudi Arabia. The hospital has adequate facilities and healthcare practitioners who can manage diabetes and its complications at no cost, regardless of nationality. Furthermore, all medications are dispensed according to the prescription at no additional charge. The study adhered to Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.12 The STROBE checklist is provided as Supplementary Material.
Sample Size
The sample size estimation was performed as follows.13 According to SUSTAIN 6, the probability of hypoglycemia (p1) with semaglutide was 44.8%, and the probability of the hypoglycemia control group (p0=1-p1) was 55.2%.6 The study employed a matched case–control design with a 1:4 ratio (case: control) to relate the potential exposures of the hypoglycemic event with a matched odds ratio (mOR) of 3 or higher using conditional logistic regression at a 5% significance level (α) with a statistical power (1-β) of 80%.14 Hence, the sample sizes for cases, controls, and the total sample were determined to be 46, 184, and 230, respectively https://riskcalc.org/samplesize/].13
Drug Selection and Dosing Escalation of Sema-OWI at the Study Site
Sema-OWI was prescribed at the study site to the T2DM patients with one of the following conditions, including overweight, obesity, cardiovascular disease, and chronic kidney disease, and aiming to minimize the risk of hypoglycemia. Sema-OWI dose escalation from 0.25 mg to 0.5 mg or from 0.5 mg to 1mg was taking place at 4-week intervals, provided no serious adverse effects were reported by patients at the study site.9 A dose-reduction strategy for concomitant antidiabetic medications, particularly insulin and sulfonylureas, was routinely implemented at the study site during the initiation and titration of Sema-OWI, in accordance with established guidelines.15
Criteria for Case Inclusion
Hospitalized patients of T2DM aged ≥18 years with the chief complaint of hypoglycemia who had already undergone the treatment of semaglutide during the study period. According to the Saudi Diabetes Clinical Practice Guidelines (SDCPG), Patients presenting with clinically significant hypoglycemia—defined as hypoglycemia associated with severe cognitive impairment requiring external assistance for recovery, regardless of measured glucose level were considered for hospital admission, while less severe cases were managed in the outpatient setting.16 CGM is strongly recommended in the SDCPG to monitor hypoglycemia in patients with clinically significant hypoglycemia, which was implemented at the study site. The patient classified level 1, level 2, or level 3/severe hypoglycemia has been included in the case group.17
Criteria for Control Inclusion
Controls were selected from the outpatient population and matched to cases based on predefined criteria, including age (±5 years), sex, nationality, and semaglutide (sema-OWI) dose. This matching approach was intended to minimize confounding by key demographic and treatment-related variables.18
Exclusion Criteria for Case and Control Groups
The following were exclusion criteria of the study: 1. The patients with a history of comorbidities other than metabolic (obesity, hypertension, dyslipidemia, and cardiovascular disease), 2. The patients were already reported to have hypoglycemia before the exposure to sema-OWI.
Data Collection
The data collection was divided into two parts: (1) Sociodemographic characteristics (age, gender, marital status, education, occupation, and smoking status) were directly obtained from the patient; and (2) Clinical characteristics (Diagnosis, comorbidities, T2DM duration, and details of medications) and laboratory data (BMI, and HbA1C) were obtained from the hospital database’s electronic health records. A face-to-face interview was conducted with a case or control to obtain the sociodemographic characteristics. For cases, all clinical characteristics and laboratory data were obtained on the day of admission. Random blood glucose and HbA1C levels were measured and reported when patients complained of hypoglycemia. The clinical characteristics and laboratory data of the controls were obtained during the outpatient pharmacy visit. Fasting blood glucose level and HbA1C were documented upon their visit to the study site.
Data Interpretation of Clinical Outcome and Predictor Variables
Hypoglycemia has been classified according to the American Diabetes Association (ADA) guidelines into 1. Level 1 hypoglycemia (blood glucose ≤70 mg/dL [3.9 mmol/L]), which requires treatment with fast-acting carbohydrates and adjustment of glucose-lowering therapy; 2. Level 2 hypoglycemia (blood glucose <54 mg/dL (3.0 mmol/L), and 3. Level 3 or severe hypoglycemia with the presence of severe cognitive impairment, which needs external assistance for recovery regardless of the glucose level.17 The BMI is categorized as underweight (<18.5kg/m2), normal weight (18.5–24.9kg/m2), overweight (25–29.9kg/m2), and obese (≥30kg/m2).19 Hemoglobin A1C less than 7% was considered target glycemic control, 7–9% was considered above target, and more than 9% was uncontrolled T2DM.20
Statistical Analysis
Descriptive statistics were performed to analyze the distribution of sociodemographic characteristics between cases and controls using Pearson’s chi-square test. Univariable conditional logistic regression was initially performed, and a p-value of less than 0.05 was used to determine which variables to include in the multivariable conditional logistic regression model. In multivariable conditional logistic regression, we assumed that BMI and HbA1C were predictors of hypoglycemia, adjusted for other significant confounding demographic variables identified in univariable conditional logistic regression. Adjusted matched odds ratios (mOR) and their 95% confidence intervals (CI) were calculated from the parameter estimates of the final model.17 A p-value of less than 0.05 was considered statistically significant, indicating an association between patient characteristics and hypoglycemic events. The Statistical Package for the Social Sciences (version 25.0) was used for statistical analysis.
Results
Eight hundred and twenty-six T2DM patients had been prescribed sema-OWI during the study period at the study site. Forty-five patients (5.44%) with blood glucose levels below 3.9 mmol/L and/or severe cognitive impairment were admitted to the hospital. Level 1 hypoglycemia (26; 57.78%) was the most predominant, followed by level 2 hypoglycemia (13; 28.89%) and level 3 hypoglycemia (6; 13.33%), as illustrated in Figure 1.
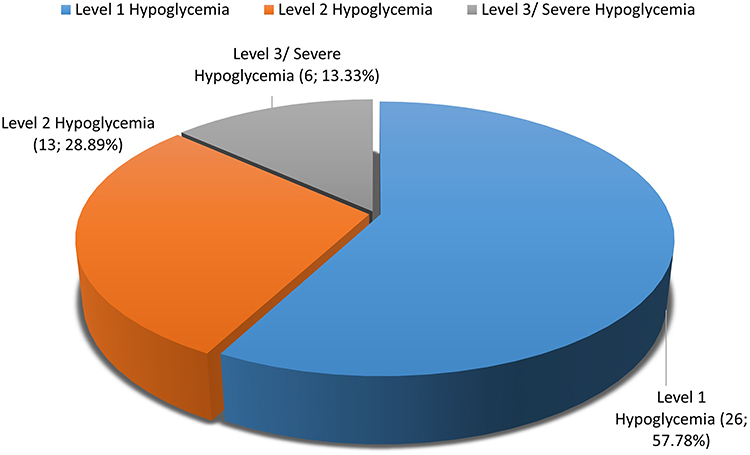 |
Figure 1 Distribution of types of hypoglycemic events in the case group. |
Matching Cases with Controls
All 45 cases were matched (1:4) with patients who did not develop hypoglycemia, using criteria including age, gender, nationality, and duration of sema-OWI treatment. Hence, 180 matched control subjects were recruited for the study. All cases involved individuals of Saudi nationality.
Demographics of the Study Population
Table 1 illustrates the demographics of the cases and controls. Many cases identified during this study were between 41 and 50 years old (15; 33%), males (25; 55.56%), married (26; 57.78%), diploma holders or graduates (25; 55.56%), and those engaged in business or employment (40; 88.89%). These associations were not statistically significant. About 73% of the control group were non-smokers, and only 57.78% of the cases were non-smokers, which was a statistically significant association (p=0.022). The distribution of metabolic comorbidities showed no significant variation between the case and control groups. However, cases were predominantly treated with two other medications for managing T2DM (19; 42.22%), whereas 49.44% of the controls did not receive any other medications, and this distribution was statistically significant (p<0.001). There was a statistically significant difference in the sema-OWI duration of treatment (p<0.001), as 22.22% (10) of the cases treated received the drug for 1–3 months, whereas only 1.11% (2) of the controls received the same treatment duration. Predominant cases (32; 71.11%) and controls (118; 65.56%) were overweight, followed by those with a normal BMI (cases: 12; 26.67% and controls: 36; 20%). Many cases had an HbA1c level of less than 7 (26; 57%). Meanwhile, controls predominantly belonged to the 7 to 9 age group (102; 56.67%).
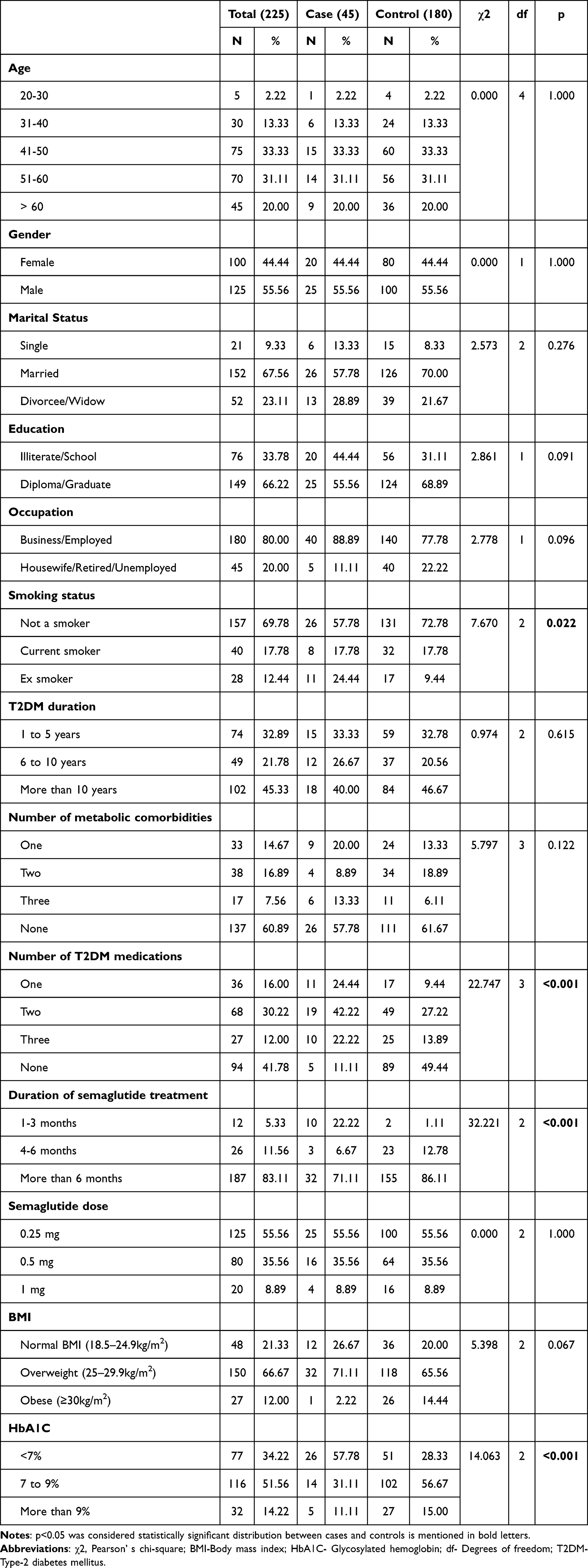 |
Table 1 Distribution of Characteristics Between the Matched Case-Control Group |
Univariable Conditional Logistic Regression
Table 2 shows that patients treated with sema-OWI for 4–6 months (mOR = 0.052; p<0.001) and those treated for more than 6 months (mOR = 0.045; p = 0.001) were least likely to be associated with hypoglycemia. It also indicated that those with sema-OWI for 1–3 months were most likely to be associated with hypoglycemia. Obese patients (mOR = 0.110; p = 0.041) and those with an HbA1C level greater than 9 (mOR = 0.254; p < 0.001) were also least likely to experience hypoglycemia (Table 2). Meanwhile, patients who received one T2DM medication other than semaglutide (mOR 0.060; p<0.001) were least likely to be associated with hypoglycemia (Table 2). Hence, these characteristics were considered in a multivariable conditional logistic regression analysis. Marital status, occupation, duration of type 2 diabetes mellitus (T2DM), and the number of metabolic comorbidities were not associated with hypoglycemia.
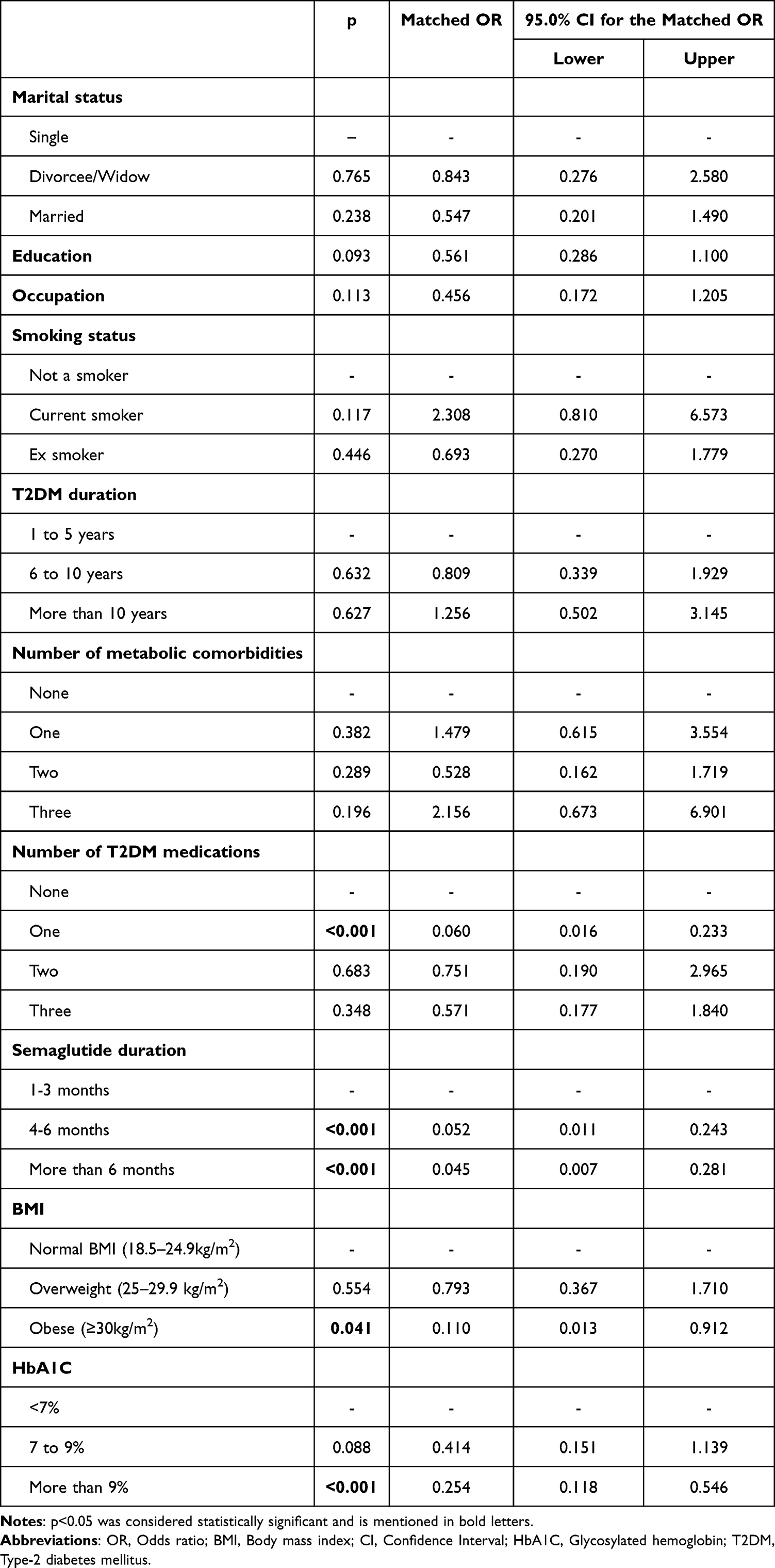 |
Table 2 Analysis of Risk Factors Associated with Hypoglycemia Using Univariable Conditional Logistic Regression |
Multivariable Conditional Logistic Regression
The multivariable conditional logistic regression model, which included variables such as BMI and HbA1C, was adjusted for the number of T2DM medications and sema-OWI treatment duration (Tables 3 and 4). It confirmed the results of univariable conditional logistic regression. Obesity remained least likely to be associated with hypoglycemia even after adjusting for the number of T2DM medications (mORadj = 0.065; p = 0.023) and duration of sema-OWI treatment (mORadj = 0.116; p = 0.049). Also, higher HbA1C levels (>9) were associated with a lower likelihood of hypoglycemia even after adjusting for the number of T2DM medications (mORadj = 0.288; p = 0.005) and duration of sema-OWI treatment (mORadj = 0.194; p<0.001). On the other hand, these results indicate that HbA1C <7 and a normal BMI were the most significant risk factors for hypoglycemia among T2DM patients treated with sema-OWI (Tables 3 and 4).
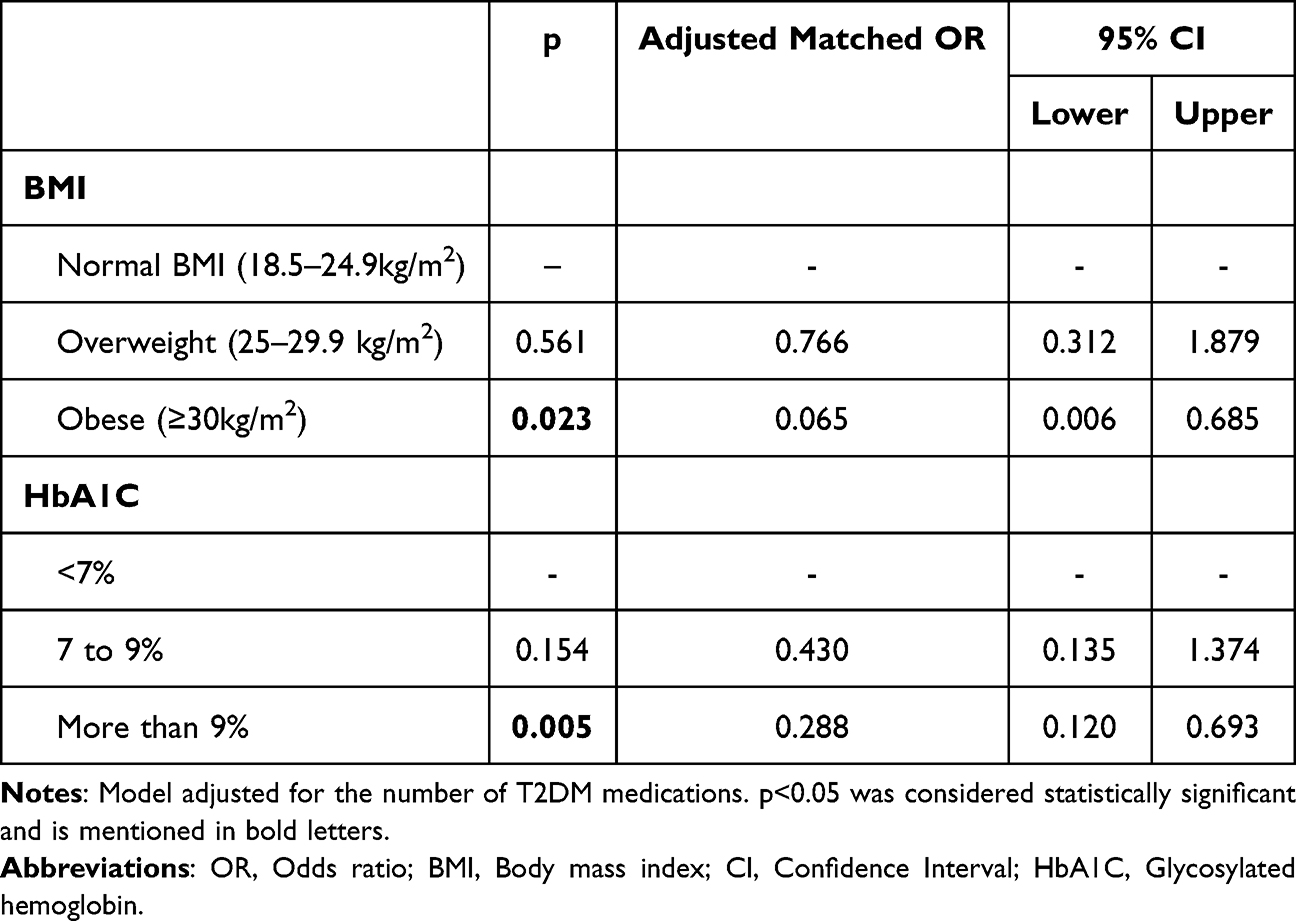 |
Table 3 Analysis of Risk Factors Associated with Hypoglycemia Using Multivariable Conditional Logistic Regression After Adjusting with the Number of T2DM Medications |
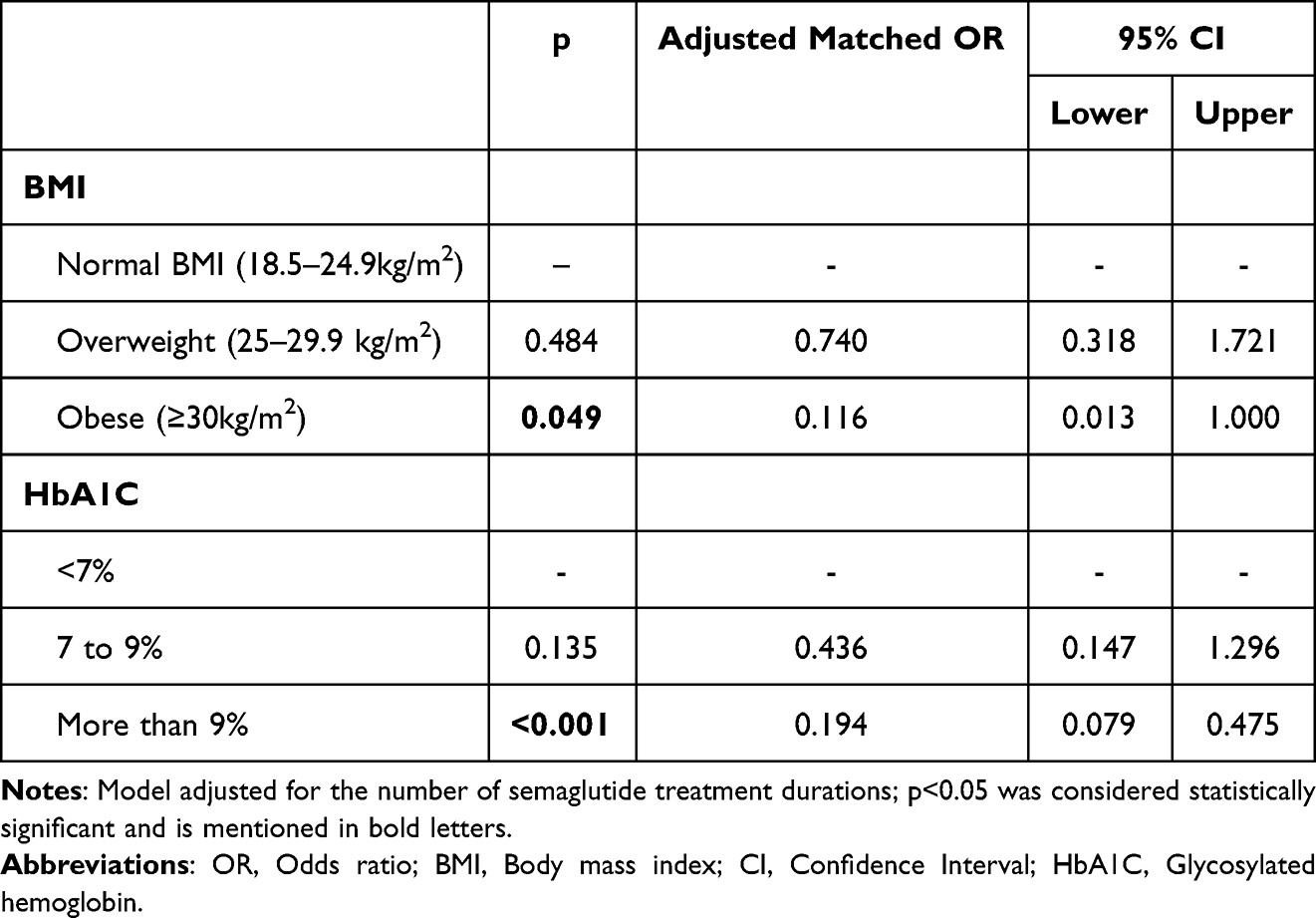 |
Table 4 Analysis of Risk Factors Associated with Hypoglycemia Using Multivariable Conditional Logistic Regression After Adjusting for Semaglutide Treatment Duration |
Discussion
This study observed 5.44% hypoglycemic events with sema-OWI, which were comparatively higher than recent real-world evidence from Canada [baseline (4.3%) and follow-up (4.7%)] and the SURE program (1.3%) as global evidence.9,10 This disparity warranted institution-based vigilance for hypoglycemia, particularly during sema-OWI dose titration. This matched case-control study investigated the association between T2DM patient characteristics and hypoglycemia under sema-OWI treatment. Multivariable conditional logistic regression analysis revealed that the patient’s normal body mass index and HbA1c level of less than 7 were associated with an increased likelihood of hypoglycemic event after adjusting for confounders, including the number of co-administered T2DM medications and the duration of sema-OWI treatment. This result substantiates the previous finding of a significant reduction in HbA1C (less than 7%) in the first three months among up to 81% of T2DM patients treated with sema-OWI, which is considered a significant risk factor for hypoglycemia.5,21,22
Sema-OWI usually begins with 0.25 mg in the first four weeks, then is titrated up to 0.5 mg in the next four weeks, followed by 1 mg. The dose titration was conducted to achieve glycemic goals.23 Doses of 0.5 mg and 1 mg were associated with a significant decline in BMI and HbA1c compared to other agents used to manage T2DM.24 These results support earlier findings that sema-OWI has a shorter median onset of hypoglycemia, and the risk is reduced after two months of treatment. In the first four weeks, there was a decline in mean fasting blood sugar from 0.5 to 2.6 mmol/L, corresponding to a dose of 0.1 to 1.6 mg of sema-OWI, which was reported in a Phase 2 randomized 12-week trial.21 Therefore, the first few months are crucial, as the doses are optimized for individual patients, and careful monitoring of symptoms of hypoglycemia, including tremors, palpitations, sweating, headaches, blurred vision, dizziness, and nausea, is necessary.7,25
According to this study’s findings, obese patients with a sema-OWI treatment were the least likely to have hypoglycemia since they successfully achieved glycemic control in T2DM patients.26 These findings support previous reports that increased BMI independently reduces the risk of hypoglycemia.27 Hence, careful monitoring of blood sugar, HbA1C, and BMI is needed to prognosticate the risk of hypoglycemia among T2DM patients managed with sema-OWI, particularly in the first three months. This study found that patients who received one T2DM medication other than sema-OWI were least likely to have hypoglycemia risk, and no association with two or three co-prescribed T2DM drugs. The association between BMI and HbA1C with hypoglycemic risk remains significant after adjusting for the number of T2DM medications using a multivariable conditional logistic regression model. Hence, in the present study, several medications did not affect the associations of BMI and HbA1c with hypoglycemic event among T2DM patients treated with sema-OWI, substantiating the previous findings from SUSTAIN 2–4 and 10.28
Glycemic control of sema-OWI was observed in a previous study, regardless of the co-administered T2DM medications. Hypoglycemia of sema-OWI has already been associated with co-administered sulfonylurea rather than metformin. Additionally, mean dose adjustment in units was necessary for insulin therapy, as sema-OWI dose titration was initiated.28,29 In this context, a recent descriptive analysis found that patient-related adverse events were predominantly due to incorrect and extra doses administered, which might be the underlying factors for hypoglycemia that need to be investigated in the future.30 Medication adherence and dietary patterns, which were not assessed in this study, may influence glycemic outcomes, including HbA1c and hypoglycemia risk.31 While semaglutide is associated with a lower risk of severe hypoglycemia compared with other glucose-lowering agents, appropriate dietary management and careful monitoring remain essential, particularly in patients receiving combination therapy (notably insulin and sulfonylureas) or those with pre-existing risk factors for hypoglycemia.8 There is no evidence that dietary changes associated with Sema-OWI increased hypoglycemic risk, and a conclusive report is still needed.
This study did not conduct a subgroup analysis to assess the impact of co-administered medications and a sensitivity analysis to assess unmeasured confounding or hidden bias (if any) on the risk of hypoglycemia. Future longitudinal assessments should address this association with a larger sample size, particularly in T2DM patients treated with sema-T2DM in the first 3 months.
This case-control study matched cases with controls in a 1:4 ratio according to variables influencing glycemic control, including age, gender, nationality, and sema-OWI dose.7,21,24,26,32,33 The distribution of variables between cases and controls, including marital status, education, occupation, duration of type 2 diabetes mellitus (T2DM), and the number of comorbidities, does not significantly impact hypoglycemic risk, as determined by chi-square analysis. The univariable conditional logistic regression also reveals similar results in these variables. These results authenticate the previous findings.11,30
While HbA1c and BMI for cases were measured at the time of hospital admission for hypoglycemia, these values for controls were obtained during outpatient visits. This discrepancy may not accurately reflect the true baseline status at the initiation of semaglutide treatment and may have influenced the observed differences in HbA1c and BMI between groups. Accordingly, these findings should be interpreted with caution.
Continuous variables are often preferred in multivariable logistic regression when the goal is to maximize information, statistical power, and flexibility in modeling risk. While the present study primarily used categorized versions of BMI and HbA1c to enhance clinical interpretability, future studies may benefit from modeling these predictors as continuous variables to generate more precise and clinically informative risk estimates.
Given the growing use of once-weekly semaglutide and the evolving understanding of hypoglycemia risk among individuals with type 2 diabetes, integrating CGM-derived dynamic markers with machine learning may help identify early metabolic shifts associated with semaglutide response. Such approaches could improve real-time monitoring, personalize dose titration, and reduce the risk of hypoglycemia, particularly during the critical first months of therapy.34,35
Strengths and Limitations of the Study
The study has several strengths: First, the study design employed a matched case-control approach with a 1:4 ratio of age, gender, nationality, and sema-OWI dose to control for and remove the influence of these risk factors on hypoglycemia. Second, the confounding factors in univariable conditional logistic regression include sema-OWI 1–3 months and one co-administered T2DM medication among the study groups, compared with the predictors of hypoglycemia (BMI and HbA1C).
The study also had some limitations, including 1. Blood sugar level was not included as an outcome variable because the control group was measured using fasting blood sugar, whereas the case group was measured at hospital admission, including not only fasting but also postprandial and random blood sugar levels. 2. The incidence of hypoglycemic events may not be accurate, as the cases were self-reported and followed by hospital admission, and there was a possibility of missing cases among those who did not volunteer to report. 3. The results cannot be generalized, as the study was conducted at a single institution among T2DM patients of similar nationalities. 4. The study design does not account for regression to the mean, which may have contributed to the observed associations between lower HbA1c/BMI and hypoglycemia, particularly during the early treatment period. 5. A key limitation of this study is the mismatch in baseline timing between cases and controls. While HbA1c and BMI for cases were measured at the time of hospital admission for hypoglycemia, these values for controls were obtained during outpatient visits, which may not accurately reflect their baseline status at the start of sema-OWI treatment. This discrepancy could have influenced the observed differences in HbA1c and BMI between the groups.
Conclusion
T2DM patients treated with sema-OWI need careful monitoring, particularly in the first 3 months, normal BMI and HbA1C <7 were associated with an increased risk of hypoglycemia. Although the study identified significant associations, these findings should be interpreted cautiously due to the baseline timing mismatch between cases and controls, which may affect the validity of comparisons. Future studies should ensure consistent timing of baseline measurements to better clarify these relationships. Also, these findings need to be substantiated by future research through longitudinal assessment, accounting for additional potential confounders, including metabolic comorbidities, medication adherence, and dietary changes related to hypoglycemic risk. Meanwhile, we recommend that healthcare practitioners pay careful attention, and patients must be adequately educated about the symptoms and reporting of hypoglycemia.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Ethical Approval and Patient Consent
The study was conducted in accordance with the guidelines of the Declaration of Helsinki. The Institutional Review Board of the Ministry of Health, Tabuk, Saudi Arabia, approved the study protocol (TU-07110231196; Date: October 31, 2024). Informed consent was obtained from all participants regarding their rights during the interview, and the right to withdraw at any stage was clearly provided.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
No funding received.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Drucker DJ. Mechanisms of action and therapeutic application of glucagon-like peptide-1. Cell Metab. 2018;27(4):740–13. doi:10.1016/j.cmet.2018.03.001
2. Gong B, Yao Z, Zhou C, Wang W, Sun L, Han J. Glucagon-like peptide-1 analogs: miracle drugs are blooming? Eur J Med Chem. 2024;269:116342. doi:10.1016/j.ejmech.2024.116342
3. Du Y, Zhang M, Wang Z, et al. A real-world disproportionality analysis of semaglutide: post-marketing pharmacovigilance data. J Diabetes Investig. 2024;15(10):1422–1433. doi:10.1111/jdi.14229
4. Butt MI, Alkhalifah KM, Riazuddin M, et al. Efficacy and safety of semaglutide: real-world tertiary care experience from Saudi Arabia. Ann Saudi Med. 2024;44(6):361–368. doi:10.5144/0256-4947.2024.361
5. Røder ME. Clinical potential of treatment with semaglutide in type 2 diabetes patients. Drugs Context. 2019;8:212585. doi:10.7573/dic.212585
6. Marso SP, Bain SC, Consoli A, et al. Semaglutide and cardiovascular outcomes in patients with type 2 diabetes. N Engl J Med. 2016;375(19):1834–1844. doi:10.1056/NEJMoa1607141
7. Zhao Z, Tang Y, Hu Y, Zhu H, Chen X, Zhao B. Hypoglycemia following the use of glucagon-like peptide-1 receptor agonists: a real-world analysis of post-marketing surveillance data. Ann Transl Med. 2021;9(18):1482. doi:10.21037/atm-21-4162
8. Smits MM, Van Raalte DH. Safety of Semaglutide. Front Endocrinol. 2021;12:645563. doi:10.3389/fendo.2021.645563
9. Yale JF, Major-Pedersen A, Catarig AM, Jain R, Menzen M, Holmes P. Real-world safety profile of once-weekly semaglutide in people with type 2 diabetes: analysis of pooled data from the SemaglUtide Real-world Evidence (SURE) programme. Diabetes Obes Metab. 2024;26(10):4429–4440. doi:10.1111/dom.15794
10. Brown RE, Bech PG, Aronson R. Semaglutide once weekly in people with type 2 diabetes: real-world analysis of the Canadian LMC diabetes registry (SPARE study). Diabetes Obes Metab. 2020;22(11):2013–2020. doi:10.1111/dom.14117
11. Alsheikh A, Alshehri A, Alzahrani S, et al. Evaluating the clinical effectiveness and safety of semaglutide in individuals with uncontrolled type 2 diabetes. Real-world evidence from Saudi Arabia: the observational, multicenter, 15-Month EVOLUTION Study. Diabetes Ther. 2024;15(2):473–485. doi:10.1007/s13300-023-01516-z
12. von Elm E, Altman DG, Egger M, et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Ann Intern Med. 2007;147(8):573–577. doi:10.7326/0003-4819-147-8-200710160-00010
13. Wang X, Ji X. Sample size estimation in clinical research: from randomized controlled trials to observational studies. Chest. 2020;158(1S):S12–S20. doi:10.1016/j.chest.2020.03.010
14. Iwagami M, Shinozaki T. Introduction to matching in case-control and cohort studies. Ann Clin Epidemiol. 2022;4(2):33–40. doi:10.37737/ace.22005
15. American Diabetes Association Professional Practice Committee for Diabetes*. 9. Pharmacologic approaches to glycemic treatment: standards of care in diabetes-2026. Diabetes Care. 2026;49(Supplement_1):S183–S215. doi:10.2337/dc26-S009
16. Saudi Diabetes Clinical Practice Guidelines (SDCPG), Saudi National Diabetes Center (SNDC), Saudi Health Council; 2021.
17. Bajaj M, McCoy RG, Balapattabi K; American Diabetes Association Professional Practice Committee for Diabetes*. 6. Glycemic goals, hypoglycemia, and hyperglycemic crises: standards of care in diabetes-2026. Diabetes Care. 2026;49(Supplement_1):S132–S149. doi:10.2337/dc26-S006
18. El-Muzaini H, Akhtar S, Alroughani R. A matched case-control study of risk factors associated with multiple sclerosis in Kuwait. BMC Neurol. 2020;20(1):64. doi:10.1186/s12883-020-01635-1
19. Dwyer JT, Melanson KJ, Sriprachy-anunt U, et al. Dietary Treatment of Obesity. [Updated February 28, 2015]. In: Feingold KR, Adler RA, Ahmed SF, et al, editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000. Table 4, Classification of Weight Status by Body Mass Index (BMI). Available from: https://www.ncbi.nlm.nih.gov/books/NBK278991/table/diet-treatment-obes.table4clas/.
20. American Diabetes Association. 6. Glycemic targets: standards of medical care in diabetes-2021. Diabetes Care. 2021;44(Suppl 1):S73–S84. doi:10.2337/dc21-S006
21. Nauck MA, Petrie JR, Sesti G, et al. A phase 2, randomized, dose-finding study of the novel once-weekly human GLP-1 analog, semaglutide, compared with placebo and open-label liraglutide in patients with type 2 diabetes. Diabetes Care. 2016;39(2):231–241. doi:10.2337/dc15-0165
22. Yu S, Fu AZ, Engel SS, Shankar RR, Radican L. Association between hypoglycemia risk and hemoglobin A1C in patients with type 2 diabetes mellitus. Curr Med Res Opin. 2016;32(8):1409–1416. doi:10.1080/03007995.2016.1176017
23. Kommu S, Whitfield P. Semaglutide. [Updated February 11, 2024]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025. Available from: https://www.ncbi.nlm.nih.gov/books/NBK603723/.
24. Andreadis P, Karagiannis T, Malandris K, et al. Semaglutide for type 2 diabetes mellitus: a systematic review and meta-analysis. Diabetes Obes Metab. 2018;20(9):2255–2263. doi:10.1111/dom.13361
25. Iqbal A, Heller S. Managing hypoglycaemia. Best Pract Res Clin Endocrinol Metab. 2016;30(3):413–430. doi:10.1016/j.beem.2016.06.004
26. Boye KS, Lage MJ, Thieu V, Shinde S, Dhamija S, Bae JP. Obesity and glycemic control among people with type 2 diabetes in the United States: a retrospective cohort study using insurance claims data. J Diabetes Complications. 2021;35(9):107975. doi:10.1016/j.jdiacomp.2021.107975
27. Plečko D, Bennett N, Mårtensson J, Bellomo R. The obesity paradox and hypoglycemia in critically ill patients. Crit Care. 2021;25(1):378. doi:10.1186/s13054-021-03795-z
28. Capehorn M, Ghani Y, Hindsberger C, Johansen P, Jódar E. Once-weekly semaglutide reduces HbA1c and body weight in patients with type 2 diabetes regardless of background common OAD: a subgroup analysis from SUSTAIN 2-4 and 10. Diabetes Ther. 2020;11(5):1061–1075. doi:10.1007/s13300-020-00796-z
29. Wajid M, Sattar S, Khalid F, Masood MQ. Efficacy and tolerability of semaglutide in patients with type-2 diabetes mellitus: experience of a Tertiary Care Hospital, Pakistan. Clin Med Insights Endocrinol Diabetes. 2023;16:11795514231213568. doi:10.1177/11795514231213568
30. Amirthalingam P. A descriptive analysis from VigiAccess on drug-related problems associated with the glucagon-like peptide-1 receptor agonists. Curr Drug Saf. 2025;20. doi:10.2174/0115748863367086250420011411
31. Amirthalingam P, Alatawi OS, Hamdan AME, et al. Medication adherence to semaglutide once-weekly injection among type-2 diabetes patients in Tabuk, Saudi Arabia–a cross-sectional study. Patient Prefer Adherence. 2025;19:2535–2551. doi:10.2147/PPA.S534534
32. DeSouza C, Cariou B, Garg S, Lausvig N, Navarria A, Fonseca V. Efficacy and safety of semaglutide for type 2 diabetes by race and ethnicity: a post hoc analysis of the SUSTAIN trials. J Clin Endocrinol Metab. 2020;105(2):dgz072. doi:10.1210/clinem/dgz072
33. Silbert R, Salcido-Montenegro A, Rodriguez-Gutierrez R, Katabi A, McCoy RG. Hypoglycemia among patients with type 2 diabetes: epidemiology, risk factors, and prevention strategies. Curr Diab Rep. 2018;18(8):53. doi:10.1007/s11892-018-1018-0
34. Montaser E, Farhy LS, Kovatchev BP. Novel detection and progression markers for diabetes based on continuous glucose monitoring data dynamics. J Clin Endocrinol Metab. 2024;110(1):254–262. doi:10.1210/clinem/dgae379
35. Montaser E, Farhy LS, Rich SS. Enhancing type 1 diabetes immunological risk prediction with continuous glucose monitoring and genetic profiling. Diabetes Technol Ther. 2025;27(4):292–300. doi:10.1089/dia.2024.0496
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Normoglycemia and Weight Reduction: Perspectives of People with Type 2 Diabetes in Australia
Newson RS, Barraclough H, Lapthorn J, Stewart M, Colman S, D’Emden M
Patient Preference and Adherence 2025, 19:897-905
Published Date: 4 April 2025
Medication Adherence to Semaglutide Once-Weekly Injection Among Type-2 Diabetes Patients in Tabuk, Saudi Arabia – A Cross-Sectional Study
Amirthalingam P, Alatawi OS, Hamdan AME, Aljabri A, Alqifari S, Alshareef H, Hakami FAM, Albalawi NS, A Albrahimi HM, Mubark Alanazi SM, Alatawi AM, Albalwi AAS, Ali MAS
Patient Preference and Adherence 2025, 19:2535-2551
Published Date: 20 August 2025