Back to Journals » Patient Preference and Adherence » Volume 19
Medication Adherence to Semaglutide Once-Weekly Injection Among Type-2 Diabetes Patients in Tabuk, Saudi Arabia – A Cross-Sectional Study
Authors Amirthalingam P ![]() , Alatawi OS, Hamdan AME
, Alatawi OS, Hamdan AME ![]() , Aljabri A
, Aljabri A ![]() , Alqifari S
, Alqifari S ![]() , Alshareef H
, Alshareef H ![]() , Hakami FAM, Albalawi NS, A Albrahimi HM, Mubark Alanazi SM, Alatawi AM, Albalwi AAS, Ali MAS
, Hakami FAM, Albalawi NS, A Albrahimi HM, Mubark Alanazi SM, Alatawi AM, Albalwi AAS, Ali MAS ![]()
Received 27 May 2025
Accepted for publication 2 August 2025
Published 20 August 2025 Volume 2025:19 Pages 2535—2551
DOI https://doi.org/10.2147/PPA.S534534
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Palanisamy Amirthalingam,1 Olayan Salamah Alatawi,2 Ahmed Mohsen Elsaid Hamdan,1 Ahmed Aljabri,3 Saleh Alqifari,1 Hanan Alshareef,1 Faris Ahmed M Hakami,2 Nader Salem Albalawi,2 Hazem Moufeed A Albrahimi,4 Sultan Mohammed Mubark Alanazi,4 Ahmed Mutair Alatawi,4 Abdullah Abdalziz S Albalwi,4 Mostafa A Sayed Ali1
1Department of Pharmacy Practice, Faculty of Pharmacy, University of Tabuk, Tabuk, Saudi Arabia; 2King Salman Armed Forces Hospital, Northwestern Region, Tabuk, Saudi Arabia; 3Department of Pharmacy Practice, Faculty of Pharmacy, King Abdulaziz University, Jeddah, Saudi Arabia; 4Faculty of Pharmacy, University of Tabuk, Tabuk, Saudi Arabia
Correspondence: Palanisamy Amirthalingam, Department of Pharmacy Practice, Faculty of Pharmacy, University of Tabuk, P.O. Box 741, Tabuk, 71491, Saudi Arabia, Email [email protected]
Background: Semaglutide, a once-weekly injection (SOWI), is a glucagon-like peptide-1 receptor agonist for managing type-2 diabetes (T2D). However, it has a high discontinuation rate among users in the first year after treatment initiation. This study investigated the medication adherence level among T2D patients managed with SOWI.
Methods: This cross-sectional study was conducted among T2D patients aged 18 years or above who visited the outpatient pharmacy to refill their prescriptions for SOWI. The patients responded to their sociodemographic characteristics and the Adherence to Refills and Medications Scale (ARMS). The patient’s electronic health record obtained details of the proportion of days covered (PDC), glycosylated hemoglobin (HbA1C), and body mass index (BMI). The association of medication adherence and sociodemographic characteristics, as well as the clinical outcomes between patients with different levels of adherence, were analyzed.
Results: A total of 434 patients were included in this study. According to the ARMS score, only 32.48% (141) of the patients adhered to SOWI. Sociodemographic characteristics had lower odds association for medication non-adherence. However, non-adherent patients had a significant association with BMI (overweight and obese) and HbA1C (> 7). The adherence level of PDC for SOWI was significantly associated with the ARMS medication adherence level. The mean HbA1C and BMI between adherents and non-adherents were statistically significant (p< 0.001). The patients who adhered to both ARMS and PDC (n = 126) experienced a significant decline in mean BMI (p < 0.001) and HbA1C (p < 0.001) compared to patients who adhered to PDC but not ARMS and those who did not adhere to either ARMS or PDC.
Conclusion: Medication adherence to the SOWI is subjective to T2D patients and not influenced by sociodemographic characteristics. T2D patients need more motivation to refill and administer the SOWI according to the schedule since medication adherence directly impacts HbA1C and BMI.
Keywords: adherence to refills and medications scale, body mass index, glycosylated hemoglobin, medication adherence, proportion to days covered, semaglutide, type-2 diabetes
Introduction
Type 2 diabetes (T2D) is a chronic disorder characterized primarily by hyperglycemia due to insulin resistance.1 The prevalence of T2D was 10.5% in 2019 and is expected to increase to 11.3% and 12.2% in 2030 and 2040, respectively.2 It requires optimal glycemic control; if not controlled, it can result in several microvascular and macrovascular complications, along with increased healthcare costs and a poor quality of life.3,4 Glycemic control is influenced by various patient characteristics, particularly medication adherence (MA).5,6 MA is defined as the “active, voluntary, and collaborative involvement of the patient in a mutually acceptable course of behavior to produce a therapeutic result”.7 A lack of MA is already linked to suboptimal glycemic control, as previous researchers have established.8,9 Once-weekly dosing of Glucagon-like peptide-1 receptor agonists (GLP-1 RAs) was found to have better MA among T2D patients.10,11 MA with GLP-1 RAs was closely positively correlated with the clinical outcomes of T2D.12 In contrast, another study found that only half of the patients were adherent to the GLP-1 RAs, and one in five patients discontinued treatment within the first 12 months.13
Semaglutide once-weekly injection (SOWI) was approved by the Food and Drug Administration (FDA) in 201711 and established for its superior MA compared to other GLP-1 receptor agonists (GLP-1 RAs).10,14 The reduction in HbA1c and body weight was greater among users of SOWI compared to those using daily GLP-1 RAs. These would protect the patients from micro- and macrovascular complications of T2D.10 The real-world adherence and persistence data also favor SOWI over other GLP-1 RAs, and the patients were highly satisfied.15–17 There is no gold standard method for accurately measuring a patient’s medication adherence (MA), as each method has numerous disadvantages.18 Numerous researchers have measured the medication MA of GLP-1 receptor agonists (GLP-1 RAs) using the proportion of days covered (PDC) for refilling medications.10–14 Generally, the PDC is calculated by the denominator, the number of days between the first prescription fill date and a defined end date. At the same time, the numerator is the number of days covered by the prescription fills during the denominator period.19 The PDC indirectly observes MA, which has several disadvantages, including the lack of a standardized method to calculate the PDC in more complex medication-related issues, such as medication pre-supply, early refills, and changes within the same pharmacological class.20 Complex medication‐related issues regarding SOWI have risen to the patient’s preference for SOWI over other GLP-1 RAs since its approval for weight loss in June 2021, followed by a shortage.21,22
Such supply and refilling issues can be assessed using a self-reported questionnaire; the Adherence to Refills and Medications Scale (ARMS) consists of 12 items divided into two domains: refilling prescriptions and medication adherence, and performs well across various literacy levels. Self-reported questionnaires are widely used, and researchers need speed, efficiency, and cost-effective methods. A validated self-reported questionnaire must be used to assess MA and can test its efficacy by comparing it with clinical outcomes. The ARMS is widely used and is free of charge to assess MA. The ARMS has already been validated in the Arabic language among patients with chronic conditions, including diabetes and hypertension, and can be administered free of any cost.23–25
The ARMS is distinguished from other self-reported MA questionnaires since it focuses on the refilling behavior of patients. Hence the dual approaches of ARMS and PDC could highlight their association and additional benefits in assessing medication adherence in T2D patients administering SOWI. This study primarily aimed to assess the MA of SOWI among T2D patients using the ARMS. The secondary objectives were to assess the influence of patient demographics in MA and the impact of MA on clinical outcomes of T2D. Following this, the association between ARMS response and PDC for SOWI on clinical outcomes was evaluated.
Methods
Study Design and Site
A cross-sectional survey was conducted at the Governmental Hospital in Tabuk, Saudi Arabia, between 1st January and 31st December 2024. The study site was a multi-specialty tertiary care hospital equipped with adequate facilities for managing Type 2 diabetes (T2D) in its medical, pharmacy, and laboratory departments, as well as qualified healthcare professionals. The study conductance and manuscript were drafted according to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cross-sectional studies (Supplementary file 1).26
Ethical Approval and Informed Consent from the Patients
The study was approved by the Research Ethics Committee of the King Salman Armed Forces Hospital (protocol code KSAFH-REC-2023-541; approved on 31 December 2023). Informed consent was obtained from all study participants prior to their enrollment in the study.
Sample Size Calculation
The sample size calculation was done using the following method:27
Sample size (n) = (Z1-α/2)2 (p) (q)/d2
n = sample size.
Z1-α/2 = Critical value and a standard corresponding confidence interval (CI).
(a 95% CI or 5% level of significance (type-I error), it is 1.96).
d = Margin of error or precision considered 5% (0.05)
P = prevalence or based on previous research; q = 1-p.
According to recent statistics, the prevalence of T2D in Saudi Arabia was 28% (0.28).28
Sample size (n) = (1.96)2 (0.28) (0.72)/(0.05)2
n = 0.7744/0.0025 = 309.78 ≈ 310
The expected participant refusal rate is 30% = 310/100*30 = 93
Total sample size = 310 + 93 = 403 T2D patients
Patients’ Recruitment
The patients were initially screened for inclusion and exclusion criteria. The study included all patients with T2D aged 18 years or above who visited the outpatient pharmacy to refill their prescriptions for SOWI. T2D patients with non-metabolic comorbidities (eg, cancer, autoimmune disease) were excluded. Patients who were prescribed SOWI for under six months were excluded from the study. The study was explained to the patients in detail, and their consent was requested to participate. Patients were included in the survey after they consented to participate. In addition, the reasons for refusal were recorded for those who were unwilling to participate in the study.
Data Collection
Instrument
The ARMS was adopted for the SOWI, and the patients were informed that they would respond. The questionnaire has two parts: 1. Patient demographics, and 2. ARMS. Patient demographics include age, gender, marital status, level of education, employment status, monthly income in Saudi Arabian Riyals (SAR), duration of T2D, and any metabolic comorbidities. The ARMS is a 4-point Likert scale with 12 items. The responses were recorded as “none”, “some”, “most”, or “all” of the time, which were given values from 1 to 4. A total ARMS score of less than 16 is considered adherence, and 16 or more is considered non-adherence.23,24 It has two subscales: 1. To assess the patient’s ability to administer the medication according to the prescribed schedule (Items 1, 2, 5, 6, 7, 8, 9, and 10), and 2. To assess the patient’s ability to refill the medications (3, 4, 11, and 12).23 Both the validated English and Arabic versions of the instrument were adopted, which minimizes potential recall and social desirability biases. The Arabic version of the ARMS was adopted for patients who could speak and understand Arabic, and the English version was used for those who could not.23,24
Clinical Outcomes and Medications
The studied clinical outcomes included body mass index (BMI), glycosylated hemoglobin (HbA1C), number of medications, details of medications, and SOWI dose obtained from the patient’s electronic health records in the hospital. The BMI is categorized as underweight (15–19.9), normal weight (20–24.9), overweight (25–29.9), and obese (more than 30).29 Glycemic control was assessed using HbA1c levels: values <7% were considered within target, 7–9% were considered above target, and >9% indicated uncontrolled T2D.30 A patient who was taking five or more medications, including SOWI, is considered polypharmacy.31
PDC Calculation
The PDC calculation is illustrated as follows.
Example
PDC = (Number of days covered by the pharmacy-supplied SOWI ÷ Number of days an SOWI is required during the period of interest) x 100
PDC = 28 (days)/30 (days) x 100 = 93.33%
PDC of SOWI ≥ 80% considered adherence, and < 80% was nonadherence.19
Statistical Methods
The distribution of patient characteristics among the adherents and non-adherent patients was assessed using chi-square statistics. Simple logistic regression was used to assess the association between patient characteristics using an unadjusted odds ratio. Multinomial logistic regression analysis was used to assess the effects of confounding variables (patient characteristics) on medication adherence. The mean±SD (standard deviation) of the clinical outcome variables (BMI and HbA1C) and PDC of SOWI were compared between adherent and non-adherent patients using a Mann–Whitney U-test. One-way Analysis of Variance (ANOVA) was used to compare the mean±SD between different patient groups (ie, Adherence according to both ARMS and PDC, adherence to PDC and non-adherence to ARMS, non-adherence according to both ARMS and PDC, adherence to ARMS and non-adherence to PDC). Normality and homogeneity of variance were not tested. Tukey’s post-hoc analysis was conducted to assess the inter-group variability. Differences were considered statistically significant with p < 0.05 at a 95% confidence interval, was considered statistically significant. Statistical Package for Social Sciences version 25.0 was used in statistical analysis.
Results
Patient Recruitment
Figure 1 represents the patient recruitment process. A total of eleven hundred and forty-five T2D patients were screened initially, followed by 676 eligible to participate in the study. SOWI treatment of less than six months (n=274) was a primary reason for exclusion, followed by diagnosis with other comorbidities (n=195). Two hundred forty-two patients were refused participation in the study. One hundred and twenty-six patients were not interested in participating, followed by 77 who had no time, and 39 did not disclose the reason for refusal. Finally, 434 patients were recruited for this cross-sectional survey.
 |
Figure 1 Schematic diagram of the study participants’ recruitment. |
Prevalence of Medication Adherence Among T2D Patients Prescribed with SOWI
Among the 434 patients, 141 (32.48%) who scored an ARMS score of less than 16 were considered adherents to the medications, while 293 (67.51%) were nonadherent, as they scored an ARMS score of 16 or higher (Table 1).
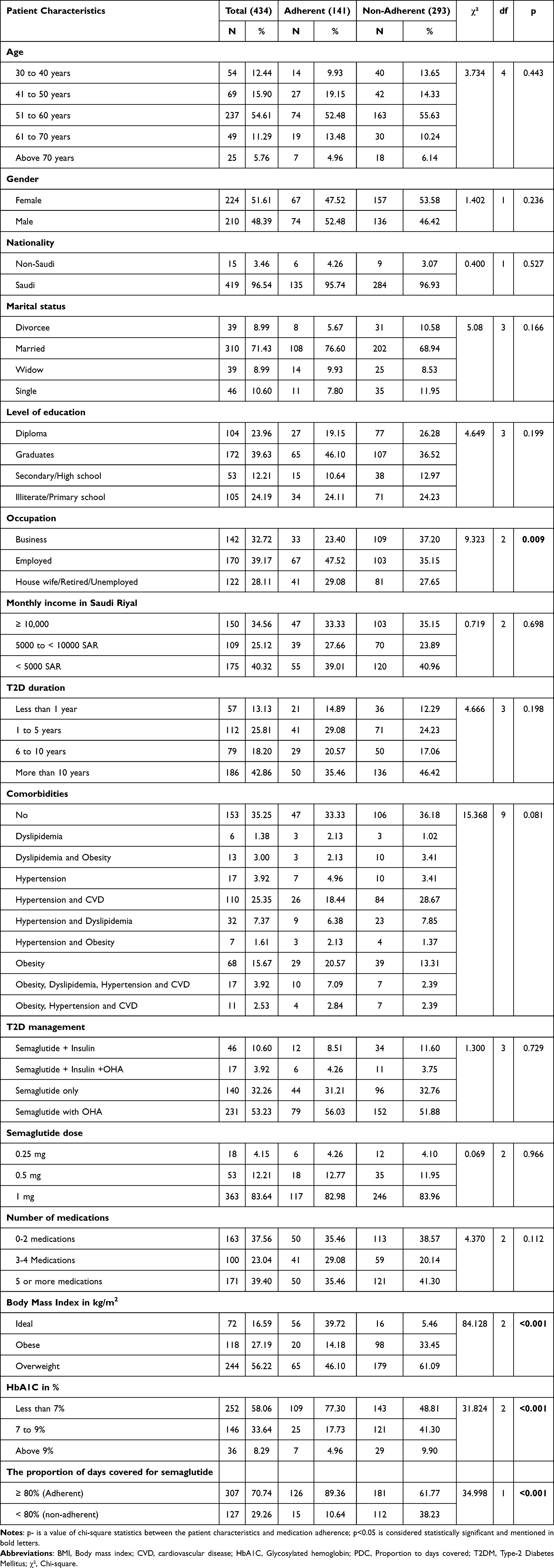 |
Table 1 Distribution of Sociodemographic and Clinical Characteristics Between Adherents and Non-Adherents |
Association of Characteristics Between Adherents and Non-Adherents
The distribution of patient characteristics between adherent and non-adherent patients is illustrated in Table 1. Most of the patients (54.61%) were between 51 and 60 years old; however, they were distributed almost equally among adherents (52.48%) and non-adherents (55.63%). However, this difference was not statistically significant. 51.61% were female, most were married (71.43%), and Saudi (96.54%). There was no statistically significant difference in the distribution of gender, marital status, and nationality between adherents and non-adherents. Most adherents (46.10%) and non-adherents (36.52%) had graduated with no significant statistical difference. Graduation (39.63%) and diploma-level education (23.96%) were the predominant qualifications of patients in this study. Most adherents (46.10%) and non-adherents (36.52%) had graduated, with no statistically significant difference. Predominant adherents were employed (47.52%), and 35.15% of non-adherents were doing business. This association showed a statistically significant difference between the two groups (p = 0.016). Most patients earned less than 5000 Saudi Riyals per month (40.32%) and have a duration of T2D of more than ten years (42.86%). These characteristics were not statistically different between the adherent and nonadherent groups. Many patients had no metabolic comorbidities (35.25%), followed by hypertension with cardiovascular disease (25.35%) and obesity (15.67%); however, the distribution of comorbidities between adherent and non-adherent patients was not significantly different. The number of medications, management of T2D, and SOWI dose were not statistically different between adherents and non-adherent patients. Patients with overweight were significantly more likely to be non-adherents (61.09%) than adherents (46.10%), and this difference was statistically significant (p = 0.005). The HbA1c level was on target (<7%) in adherents (77.30%) compared to non-adherents (48.81%), with statistically significant differences (p < 0.001). According to the PDC score (≥80%), adherence was predominant (89.36%), and only 61.77% were non-adherents, with statistical significance (p < 0.001).
Logistic regression analysis was employed to investigate the relationship between the patient characteristics and medication adherence (Table 2). Age, gender, marital status, education, occupation, monthly income, duration of T2D, management of T2D, SOWI dose, and number of medications showed no significant association with medication adherence before and after adjusting for confounding variables. The patients who were employed had a higher odds association with medication adherence after adjusting for confounding variables (OR=9.976; p=0.025).
- Non-adherent patients were significantly associated with obesity and overweight before (Overweight: OR=0.103; p=0.000; Obese: OR=0.058; p=0.000) and after (Overweight: OR=0.012; p=0.000; Obese: OR=0.000; p=0.000) adjusting for confounding variables.
- Also, non-adherent patients most likely to have HbA1C 7 to 9 and more than 9 before (HbA1C 7 to 9: OR=0.271; p=0.000; HbA1C more than 9: OR=0.316; p=0.008) and after (HbA1C 7 to 9: OR=0.134; p=0.000; HbA1C more than 9: OR=0.168; p=0.008) adjusting for confounding variables.
- The adherence to PDC for SOWI was predominantly associated with adherence to the ARMS score before (unadjusted odds ratio, 11.614; p = 0.000) and after adjusting for confounding patient characteristics (adjusted odds ratio, 21.310; p = 0.000).
 |
Table 2 Regression Analysis of Characteristics Between Adherents and Non-Adherents According to the ARMS Score |
Patient Responses to ARMS
The mean difference was statistically significant (p<0.001) between adherents and non-adherents regardless of items in ARMS according to the Mann–Whitney U-test (Table 3). Items 3, 4, 11, and 12 are related to refilling medications. The lowest mean ± SD value of item 11 reflects the poor influence of the cost of medication among both adherents (1.057 ± 0.23) and non-adherents (1.27 ± 0.54). Meanwhile, the higher mean difference between adherent and non-adherent patients in item 3 (−0.796), item 4 (−0.686), and item 12 (−0.795) contributed significantly to non-adherence. The remaining items in ARMS (1, 2, 5, 6, 7, 8, 9, and 10) concern the patient’s ability to administer the medication according to the prescribed schedule. In this regard, the major cause of poor adherence since higher mean difference noticed on non-adherents from adherents was due to: 1. They miss taking their medicine when they feel better (item 6; mean difference: −0.767), 2. Change the dose of their medicines to suit their needs (item 9; mean difference: −0.646), 3. Forget to take their medicine when they are supposed to take it more than once a day (item 10; mean difference: −0.584), 4. They decide not to take their medicine (item 2; mean difference: −0.548), and 5. They skip a dose of their medicine before going to the doctor (item 5; mean difference: −0.543). The following items has least influence for non-adherence since the mean difference between adherents and non-adherents was low among the items 1 (How often do you forget to take your medicine?; mean difference: −0.302), 7 (How often do you miss taking your medicine when you feel sick?; mean difference: −0.299), and 8 (How often do you miss taking your medicine when you are careless?; mean difference: −0.202).
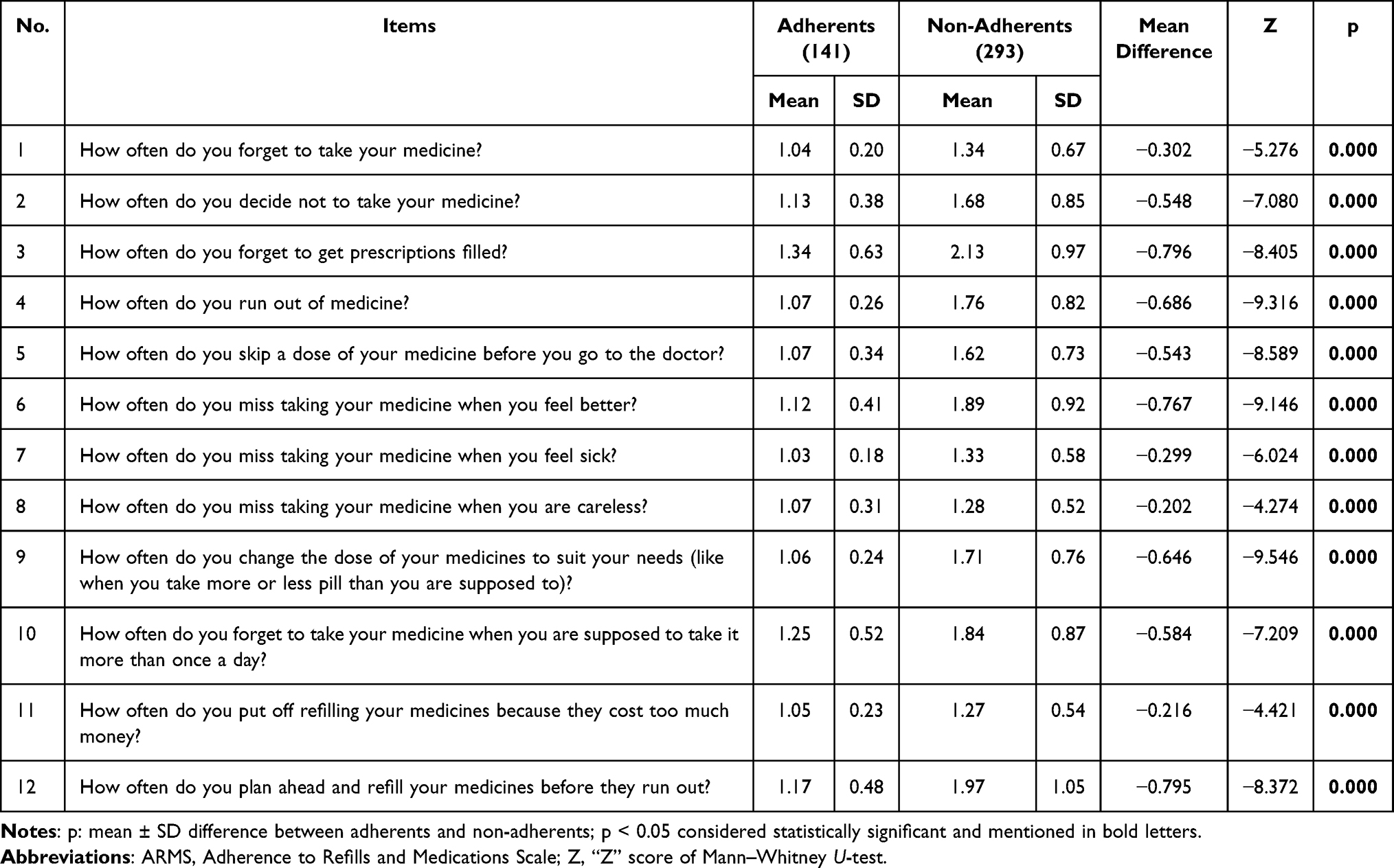 |
Table 3 Responses of Adherents and Non-Adherents to ARMS |
Differences in Medication Adherence Score and Clinical Outcomes
The differences between medication adherence and clinical outcomes using the Mann–Whitney U-test have been revealed in Table 4. The mean (SD) BMI of adherents was significantly lower than the non-adherents according to the ARMS score (p<0.001) and PDC score (p<0.043). Meanwhile, according to the ARMS score, the mean HbA1C level is significantly lower in adherents (p<0.001) but not in PDC (p=0.357). The mean (SD) PDC score between the adherents and non-adherents according to the ARMS was statistically significant (p<0.001); in vice-versa, the mean (SD) ARMS score between the adherents and non-adherents according to the PDC for SOWI was also statistically significant (p<0.001).
 |
Table 4 Differences in HbA1C and BMI, ARMS, and PDC Scores Between the Adherents and Non-Adherents |
In Table 5, the patients were divided into four groups: 1. Adherence according to both ARMS and PDC (126), adherence to PDC and non-adherence to ARMS (181), non-adherence according to both ARMS and PDC (112), and Adherence to ARMS and Non-adherence to PDC (15). The means (SD) of HbA1C and BMI between the groups mentioned above were statistically significant (p<0.001). Further, a post-hoc analysis was performed to understand the inter-group differences in the mean (SD) of HbA1C and BMI (Table 6). Adherence, according to both the ARMS and PDC groups of patients, has a significantly lower HbA1C and BMI than the groups’ adherence to PDC and non-adherence to ARMS (p=0.000), and non-adherence according to both ARMS and PDC (p=0.027). Notably, there was no significant difference between adherence to ARMS and non-adherence to the PDC group of patients in HbA1C (p=0.834) and BMI (p=0.999). The patient group with adherence to ARMS and non-adherence to PDC had significantly lower HbA1C (p=0.005) and BMI (0.012) than the group with adherence to PDC and non-adherence to ARMS. Meanwhile, the patient group with adherence to ARMS and non-adherence to PDC had significantly lesser BMI (p=0.018) than those with non-adherence according to the ARMS and PDC group. However, these groups have significant differences in HbA1C (p=0.136).
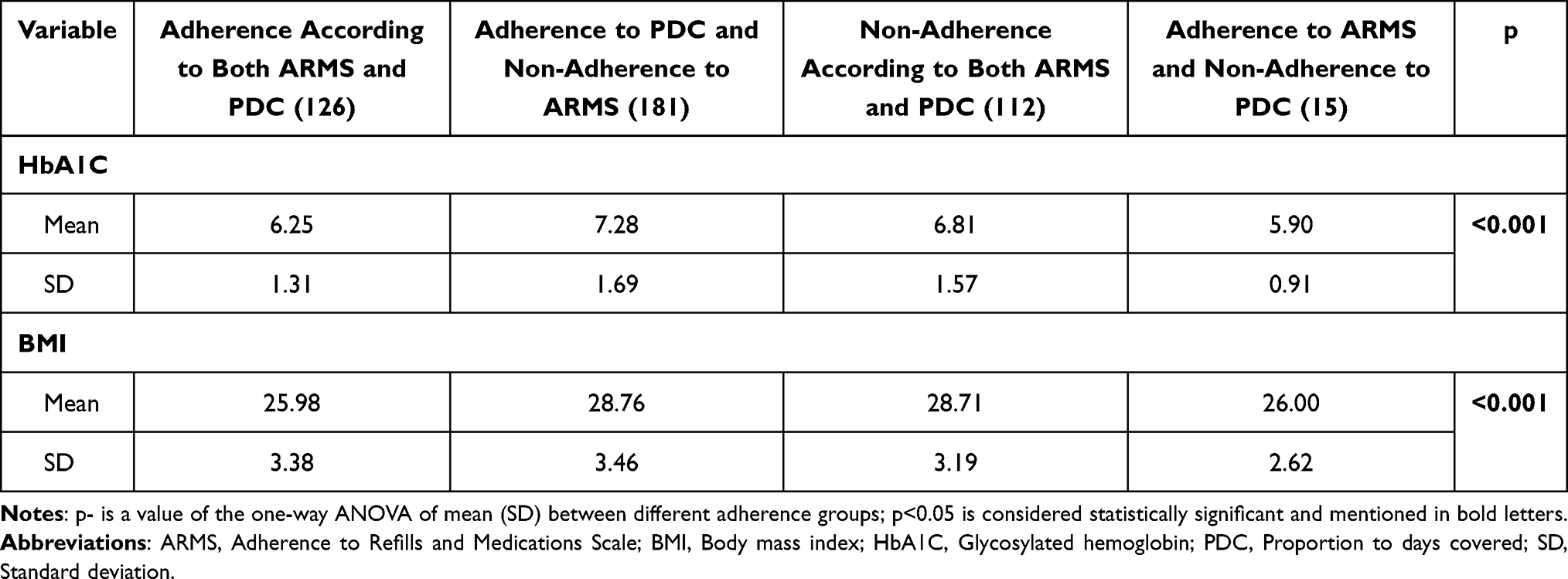 |
Table 5 Comparison of Clinical Outcome Variables Between Patients’ Adherence with ARMS and PDC Score |
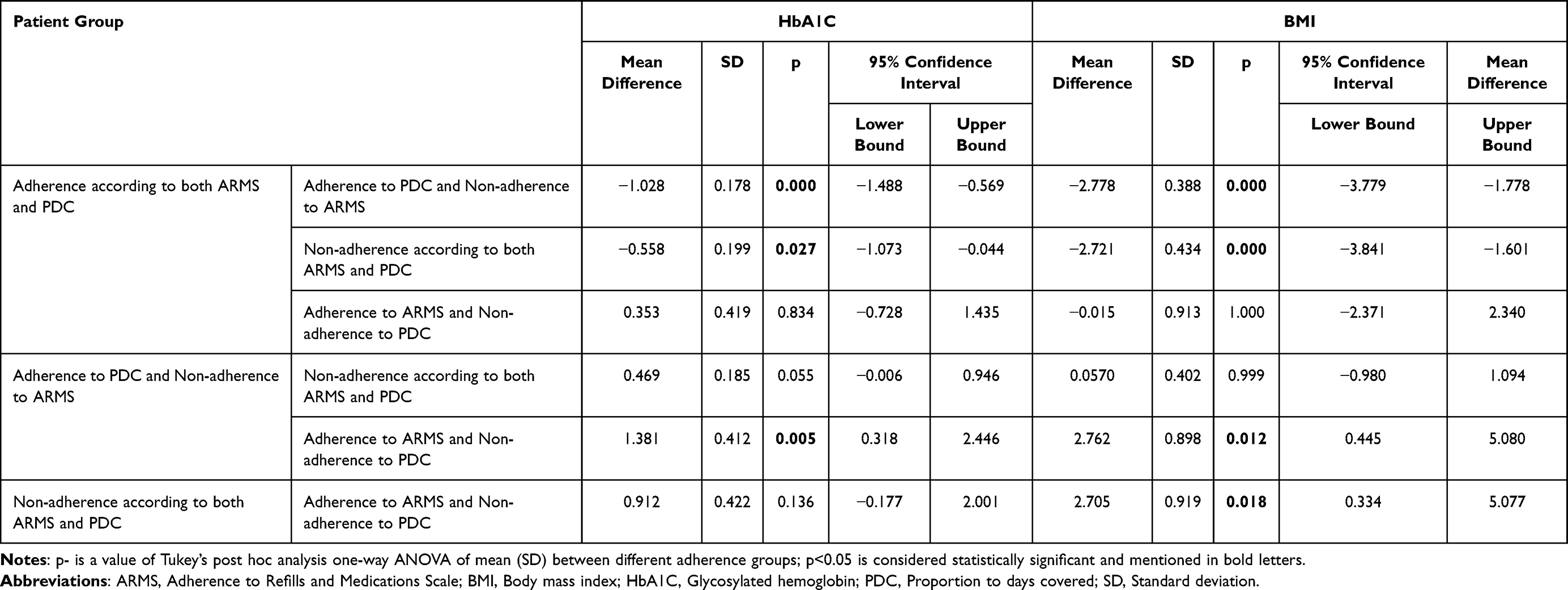 |
Table 6 Tukey’s Posthoc Analysis on the Comparison of Clinical Outcome Variables Between Patients’ Adherence with ARMS and PDC Score |
Discussion
This is the first cross-sectional study to assess medication adherence using ARMS among patients with T2D who were administered SOWI. Although previous studies have already documented good medication adherence to once-weekly SOWI, this study showed medication non-adherence (ARMS score ≥16) in 67.51% (n=293) of T2D patients.10,16,17 This higher non-adherence rate could be due to the adverse effects and patients’ perceived inconvenience with injectables.32–34
This study includes patients who had more than six months of SOWI treatment since absolute discontinuation of SOWI was at least 6 months, as reported by the recent nationwide registry study in Denmark and another researcher from the United States addressed that only 50% of patients are consistent with SOWI in their first year of treatment due to adverse drug reactions.13,34 Previous studies have highlighted that SOWI has higher patient satisfaction and improved clinical benefits compared to other GLP-1 RAs.16,17,35 Also, a recent study has suggested that adherence to SOWI could improve glycemic control.32 Hence, this study highlights that SOWI benefits T2D patients who adhere to treatment more than non-adherents in terms of clinical outcomes, including BMI and HbA1C.
This study is consistent with a recently published Danish cohort study regarding the SOWI, which is predominantly used among females at a median age of 50 with T2D and metabolic comorbidities.34 We did not find the patients between the age groups of 18–29 years in the study site during the study period. The patient’s sociodemographic and clinical characteristics (that includes age, gender, nationality, marital status, level of education, occupation, monthly income, T2D duration, metabolic comorbidities, T2D management, SOWI dose, and number of medications) in this study were not associated with medication adherence, either before or after adjusting for confounding variables using logistic regression analysis. According to the previous studies, regardless of age, gender, comorbidities, semaglutide dose, and co-prescribed medications for T2D, SOWI substantially decreased body weight and HbA1C, which was verified in the present study, particularly for those who adhered. As reported in previous studies,35 SOWI in T2D management remains complex in clinical practice and varies according to the individual patient. Meanwhile, the present study found no significant association between medication adherence and the patient’s treated SOWI monotherapy or SOWI administered in combination with other medications.32
Monthly income was not associated with medication adherence (Table 2), as medications were provided free of charge at the study site, which is under the governance of the Ministry of Defense, Saudi Arabia. Additionally, among all the items in ARMS, the very low mean difference between adherents and non-adherents regarding item 11 (How often do you put off refilling your medicines because they cost too much money?) suggests that the cost has minimal influence on medication adherence (Table 3). SOWI was reported to be cost-effective for the healthcare system, particularly in managing T2D with existing metabolic comorbidities.36 Other items related to refill in the ARMS (3, 4, and 12) had a higher mean difference between adherents and non-adherents, ascertaining that the refilling of SOWI potentially influences patient medication adherence. The present study did not investigate the barriers to SOWI refilling, and future studies are warranted to investigate and rule out them for enhancing the adherence followed by better clinical outcomes.13,21,22,34
Eight items (1, 2, 5, 6, 7, 8, 9, and 10) in ARMS were relevant to the patient’s ability to administer the medication according to the prescribed schedule. The higher mean difference was noticed among the items that include 1. They miss taking their medicine when they feel better (item 6), 2. Change the dose of their medicines to suit their needs (item 9), 3. Forget to take their medicine when they are supposed to take it more than once a day (item 10), 4. They decide not to take their medicine (item 2), and 5. They skip a dose of their medicine before going to the doctor (item 5). This study contradicts earlier literature, despite previous studies reporting that patients were more satisfied with SOWI regarding its use.16,17,36,37 Therefore, ARMS can help practitioners assess what causes non-adherence to SOWI among T2D patients. Also, many studies in the future still need to highlight the barriers involved in medication adherence to SOWI, which help the practitioners rule out them and achieve the desired clinical outcomes.
According to ARMS and PDC scores (p=0.043), adherents have a significantly lower mean (SD) body mass index than non-adherents (Table 4). Moreover, according to ARMS, adherents have lower HbA1c Levels (p < 0.001) than non-adherents, whereas there was no significant difference between them according to the PDC score. Meanwhile, patients who adhered to both ARMS and PDC experienced a significant decline in BMI and HbA1C compared to those who adhered to PDC but not ARMS, as well as those who adhered to neither ARMS nor PDC. In this regard, according to the ARMS and PDC scores, the adherence level clearly demonstrates the impact on clinical outcomes and is consistent with previous findings (Table 5).10,13,17,35,37 Therefore, the combined monitoring with ARMS and PDC in T2D patients initiated with the SOWI could help enhance their clinical outcomes.
The adherence level of patients in this study, as measured by ARMS and PDC, was inconsistent, with ARMS detecting 67.05% (291) of non-adherence, whereas PDC detected only 29.2% (127) of non-adherence. In this regard, the threshold level of PDC ≥80% for adherence remains questionable, as only 18% of studies in a scoping review and 1% of studies in another systematic review recommended this threshold to improve health outcomes.20,38 The PDC calculation could be more appropriate with the prescribed daily dose, which is difficult to calculate with a once-weekly SOWI.39 Hence, the pitfalls in implementing the PDC method for SOWI must be ruled out in future studies to assess adherence accurately.
Strengths and Limitations
The study assessed medication adherence among the T2D patients who were prescribed SOWI using ARMS for the first time. The patient’s responses are explored under two domains of the ARMS. Patient adherence was evaluated in a real-world setting based on a combination of self-report and prescription refill data, which is likely more reflective of the medication adherence patterns encountered by clinicians when treating patients in clinical practice. The patients were grouped into four according to their adherence to ARMS and PDC. This study highlights monitoring medication adherence and its impact on clinical outcomes by combining the ARMS and PDC. To improve the integrity of the findings, the authors of this study had face-to-face meetings with the patients for data collection. The ARMS was already validated in both English and Arabic, and it helps minimize the bias among the diverse, multilingual population in this study. However, the study has several limitations: 1. The single-center study findings cannot be generalized; 2. The power analysis has not been performed in the sample size calculation to detect differences between subgroups. 3. The patients were prescribed drugs other than SOWI, which might have influenced their response, even though they were informed of the responses for only SOWI; 4. Baseline BMI and HbA1C were unknown, which limits our ability to attribute changes solely to adherence.
Conclusion
This study found that sociodemographic characteristics were not significant predictors of adherence. SOWI can be effective in improving glycemic control and BMI among adherent patients. The ARMS could help healthcare practitioners measure adherence to SOWI and be more accurate when combined with the PDC method. This should be adopted routinely in each clinical visit of the patient until the dosage optimization of SOWI. Those who are not adhering need to be investigated further to address the barrier to non-adherence and need to be counseled accordingly. In this regard, future studies need to explore the barriers to non-adherence in two domains of ARMS: the patient’s refilling ability and the patient’s ability to administer the medication according to the prescribed schedule.
Data Sharing Statement
The datasets used and analyzed during the current study are available from the corresponding author upon reasonable request.
Ethical Approval and Patient Consent
The Research Ethics Committee of the King Salman Armed Forces Hospital approved the study (KSAFH-REC-2023-541), which complies with the Declaration of Helsinki. Written consent was obtained from all participants before enrolment.
Acknowledgments
The authors thank the hospital administrators and the participants for conducting this study.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. American Diabetes Association Professional Practice Committee. 2. classification and diagnosis of diabetes: standards of medical care in diabetes-2022. Diabetes Care. 2022;45(Suppl 1):S17–S38. doi:10.2337/dc22-S002
2. Magliano DJ, Boyko EJ, committee IDFDAtes. IDF diabetes atlas. IDF diabetes atlas Vol. 2021. Brussels: International Diabetes Federation © International Diabetes Federation (2021).
3. Mansour A, Mousa M, Abdelmannan D, Tay G, Hassoun A, Alsafar H. Microvascular and macrovascular complications of type 2 diabetes mellitus: exome wide association analyses. Front Endocrinol. 2023;14:1143067. doi:10.3389/fendo.2023.1143067
4. Shahtaheri RS, Bayazidi Y, Davari M, et al. Long-term cost-effectiveness of quality of diabetes care; experiences from private and public diabetes centers in Iran. Health Econ Rev. 2022;12(1):44. doi:10.1186/s13561-022-00377-9
5. Dinavari MF, Sanaie S, Rasouli K, Faramarzi E, Molani-Gol R. Glycemic control and associated factors among type 2 diabetes mellitus patients: a cross-sectional study of Azar cohort population. BMC Endocr Disord. 2023;23(1):273. doi:10.1186/s12902-023-01515-y
6. Sendekie AK, Netere AK, Kasahun AE, Belachew EA. Medication adherence and its impact on glycemic control in type 2 diabetes mellitus patients with comorbidity: a multicenter cross-sectional study in Northwest Ethiopia. PLoS One. 2022;17(9):e0274971. doi:10.1371/journal.pone.0274971
7. Delamater AM. Improving patient adherence. Clin Diabetes. 2006;24(2):71–77. doi:10.2337/diaclin.24.2.71
8. Jarab S, Al-Qerem A, Hamam WA, et al. Glycemic control and its associated factors among diabetic heart failure outpatients at two major hospitals in Jordan. PLoS One. 2023;18(10):e0285142. doi:10.1371/journal.pone.0285142
9. Yahaya JJ, Doya IF, Morgan ED, Ngaiza AI, Bintabara D. Poor glycemic control and associated factors among patients with type 2 diabetes mellitus: a cross-sectional study. Sci Rep. 2023;13(1):9673. doi:10.1038/s41598-023-36675-3
10. Kassem S, Khalaila B, Stein N, Saliba W, Zaina A. Efficacy, adherence and persistence of various glucagon-like peptide-1 agonists: nationwide real-life data. Diabetes Obes Metab. 2024;26(10):4646–4652. doi:10.1111/dom.15828
11. Weeda ER, Muraoka AK, Brock MD, Cannon JM. Medication adherence to injectable glucagon-like peptide-1 (GLP-1) receptor agonists dosed once weekly vs once daily in patients with type 2 diabetes: a meta-analysis. Int J Clin Pract. 2021;75(9):e14060. doi:10.1111/ijcp.14060
12. Svensson AM, Toll A, Lebrec J, Miftaraj M, Franzén S, Eliasson B. Treatment persistence in patients with type 2 diabetes treated with glucagon-like peptide-1 receptor agonists in clinical practice in Sweden. Diabetes Obes Metab. 2021;23(3):720–729. doi:10.1111/dom.14276
13. Lassen MCH, Johansen ND, Modin D, et al. Adherence to glucagon-like peptide-1 receptor agonist treatment in type 2 diabetes mellitus: a nationwide registry study. Diabetes Obes Metab. 2024;26(11):5239–5250. doi:10.1111/dom.15872
14. Chen W, Cai P, Zou W, Fu Z. Psychiatric adverse events associated with GLP-1 receptor agonists: a real-world pharmacovigilance study based on the FDA adverse event reporting system database. Front Endocrinol. 2024;15:1330936. doi:10.3389/fendo.2024.1330936
15. Uzoigwe C, Liang Y, Whitmire S, Paprocki Y. Semaglutide once-weekly persistence and adherence versus other GLP-1 RAs in patients with type 2 diabetes in a US real-world setting. Diabetes Ther. 2021;12(5):1475–1489. doi:10.1007/s13300-021-01053-7
16. Baba Y, Watanabe S, Hayashi S, et al. Semaglutide improves treatment satisfaction and eating behaviour in Japanese patients with type 2 diabetes mellitus. Diabetes Obes Metab. 2024;26(10):4787–4790. doi:10.1111/dom.15823
17. Al Hayek AA, Al Dawish MA. Evaluation of patient-reported satisfaction and clinical efficacy of once-weekly semaglutide in patients with type 2 diabetes: an ambispective study. Adv Ther. 2022;39(4):1582–1595. doi:10.1007/s12325-022-02053-0
18. Lam WY, Fresco P. Medication adherence measures: an overview. Biomed Res Int. 2015;2015:1–12. doi:10.1155/2015/217047
19. Prieto‐Merino D, Mulick A, Armstrong C, et al. Estimating proportion of days covered (PDC) using real‐world online medicine suppliers’ datasets. J Pharm Policy Pract. 2021;14(1):113. doi:10.1186/s40545-021-00385-w
20. Dalli LL, Kilkenny MF, Arnet I, et al. Towards better reporting of the proportion of days covered method in cardiovascular medication adherence: a scoping review and new tool TEN-SPIDERS. Br J Clin Pharmacol. 2022;88(10):4427–4442. doi:10.1111/bcp.15391
21. Blum D. The Wegovy shortage continues, leaving patients on the weight loss drug in limbo. New York Times. 2023. Available from: https://www.nytimes.com/2023/10/05/well/live/wegovy-shortageozempic-fda.html.
22. Baig K, Dusetzina SB, Kim DD, Leech AA. Medicare Part D coverage of antiobesity medications—challenges and uncertainty ahead. N Engl J Med. 2023;388(11):961–963. doi:10.1056/NEJMp2300516
23. Kripalani S, Risser J, Gatti ME, Jacobson TA. Development and evaluation of the adherence to refills and medications scale (ARMS) among low-literacy patients with chronic disease. Value Health. 2009;12(1):118–123. doi:10.1111/j.1524-4733.2008.00400.x
24. Stirratt MJ, Dunbar-Jacob J, Crane HM, et al. Self-report measures of medication adherence behavior: recommendations on optimal use. Transl Behav Med. 2015;5(4):470–482. doi:10.1007/s13142-015-0315-2
25. Alammari G, Alhazzani H, AlRajhi N, et al. Validation of an Arabic version of the adherence to refills and medications scale (ARMS). Healthcare. 2021;9(11):1430. doi:10.3390/healthcare9111430
26. Cuschieri S. The STROBE guidelines. Saudi J Anaesth. 2019;13(Suppl 1):S31–S34. PMID: 30930717; PMCID: PMC6398292. doi:10.4103/sja.SJA_543_18
27. Pourhoseingholi MA, Vahedi M, Rahimzadeh M. Sample size calculation in medical studies. Gastroenterol Hepatol Bed Bench. 2013;6(1):14–17.
28. Alwadeai KS, Alhammad SA. Prevalence of type 2 diabetes mellitus and related factors among the general adult population in Saudi Arabia between 2016-2022: a systematic review and meta-analysis of the cross-sectional studies. Medicine. 2023;102(24):e34021. doi:10.1097/MD.0000000000034021
29. World Health Organization. Physical status: the use and interpretation of anthropometry: report of a world health organization (WHO) expert committee. Geneva, Switzerland: World Health Organization; 1995.
30. American Diabetes Association. 6. glycemic targets: standards of medical care in diabetes-2021. Diabetes Care. 2021;44(Suppl 1):S73–S84. doi:10.2337/dc21-S006
31. Masnoon N, Shakib S, Kalisch-Ellett L, Caughey GE. What is polypharmacy? A systematic review of definitions. BMC Geriatr. 2017;17(1):230. doi:10.1186/s12877-017-0621-2
32. Giorgino F, Penfornis A, Pechtner V, et al. Adherence to antihyperglycemic medications and glucagon-like peptide 1-receptor agonists in type 2 diabetes: clinical consequences and strategies for improvement. Patient Prefer Adherence. 2018;12:707–719. doi:10.2147/PPA.S151736
33. Swift C, Frazer M, Sargent A, et al. Real-world treatment patterns among us patients with type 2 diabetes mellitus initiating treatment with once weekly semaglutide for diabetes. Clin Ther. 2025;47(4):277–283. doi:10.1016/j.clinthera.2024.12.014
34. Ladebo L, Ernst MT, Mailhac A, Dirksen C, Bojsen-Møller KN, Pottegård A. Real-world use of semaglutide for weight management: patient characteristics and dose titration-a Danish cohort study. Diabetes Care. 2024;47(10):1834–1837. doi:10.2337/dc24-1082
35. Alsheikh A, Alshehri A, Alzahrani S, et al. Evaluating the clinical effectiveness and safety of semaglutide in individuals with uncontrolled type 2 diabetes. real-world evidence from Saudi Arabia: the observational, multicenter, 15-month EVOLUTION study. Diabetes Ther. 2024;15(2):473–485. doi:10.1007/s13300-023-01516-z
36. Rennert-May E, Manns B, Clement F, et al. Cost-effectiveness of semaglutide in patients with obesity and cardiovascular disease. Can J Cardiol. 2025;41(1):128–136. doi:10.1016/j.cjca.2024.09.025
37. Sørensen MS, Pottegård A, Andersen NE, Thomsen RW, Lundby C. Survey among adult users of semaglutide for weight loss in Denmark: user characteristics, treatment expectations and experienced effects. Diabetes Obes Metab. 2025;27(4):2214–2222. doi:10.1111/dom.16222
38. Baumgartner PC, Haynes RB, Hersberger KE, Arnet I. A systematic review of medication adherence thresholds dependent of clinical outcomes. Front Pharmacol. 2018;9:1290. doi:10.3389/fphar.2018.01290
39. Ung D, Dalli LL, Lopez D, et al. Assuming one dose per day yields a similar estimate of medication adherence in patients with stroke: an exploratory analysis using linked registry data. Br J Clin Pharmacol. 2021;87(3):1089–1097. doi:10.1111/bcp.14468
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Medication Adherence to Semaglutide versus Empagliflozin in Adults with Type 2 Diabetes: A Retrospective Observational Study in Saudi Arabia
Ali MAS, Amirthalingam P, Alshareef H, Alqifari SF, Elsaid Hamdan AM, Alatawi O, Hakami FAM, Albalawi NS, Aljabri A
Patient Preference and Adherence 2025, 19:4179-4190
Published Date: 19 December 2025
Risk Factors for Hypoglycemia in Type 2 Diabetes Mellitus Patients Using Once-Weekly Semaglutide: A Matched Case-Control Study
Amirthalingam P, Alarawi FA, Jassas Alagwar LM, Alatawi MS, Saeed Alfahmi Alzahrani MS, A Albalwi AO, Alrashidi A, Elsaid Hamdan AM, Fahad Alqifari S, Alshareef H, Aljabri A, Sirag N, Pakkir Mohamed SH, Ali MAS
Therapeutics and Clinical Risk Management 2026, 22:610579
Published Date: 4 June 2026