")
Back to Journals » Clinical Interventions in Aging » Volume 16
Risk Factors for Hospital Readmission and Death After Discharge of Older Adults from Acute Geriatric Units: Taking the Rank of Admission into Account
Authors Visade F , Babykina G, Puisieux F, Bloch F , Charpentier A, Delecluse C, Loggia G , Lescure P, Attier-Żmudka J, Gaxatte C, Deschasse G, Beuscart JB
Received 1 July 2021
Accepted for publication 15 September 2021
Published 29 October 2021 Volume 2021:16 Pages 1931—1941
DOI https://doi.org/10.2147/CIA.S327486
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Nandu Goswami
Fabien Visade,1,2 Genia Babykina,1 François Puisieux,3 Frédéric Bloch,4,5 Anne Charpentier,3 Céline Delecluse,2 Gilles Loggia,6,7 Pascale Lescure,7 Jadwiga Attier-Żmudka,8,9 Cédric Gaxatte,3 Guillaume Deschasse,1,4 Jean-Baptiste Beuscart1,3
1University Lille, CHU Lille, ULR 2694 - METRICS: Évaluation des technologies de santé et des pratiques médicales, Lille, F-59000, France; 2Geriatrics Department, Lille Catholic Hospitals, Lille, F-59000, France; 3Department of Geriatrics, CHU Lille, Lille, F-59000, France; 4Department of Geriatrics, CHU Amiens-Picardie, Amiens, F-80054, France; 5Laboratory of Functional Neurosciences EA 4559, University of Picardie – Jules-Verne, Amiens, France; 6UNICAEN, INSERM, COMETE, Normandie Univ, Caen, France; 7Department of Geriatrics, Normandie Univ, UNICAEN, CHU de Caen Normandie, Caen, France; 8Geriatric Department, General Hospital of Saint-Quentin, Saint-Quentin, France; 9CHIMERE EA 7516 Head and Neck Research Group, Jules Verne University, Amiens, France
Correspondence: Fabien Visade
University Lille, CHU Lille, ULR 2694 - METRICS: Évaluation des technologies de santé et des pratiques médicales, Lille, F-59000, France
Tel +33-320-626-969
Fax +33-320-626-881
Email [email protected]
Objective: To analyze the impact of the number of hospital readmissions on the risks of further hospital readmission and death after adjustment for a range of risk factors.
Methods: We performed a multicentre prospective study of the DAMAGE cohort in the Hauts-de-France region of France. Patients aged 75 and over hospitalized initially in an acute geriatric unit (AGU) were included and followed up for 12 months. The risk of hospital readmission was analyzed using a Cox model, and its extension for recurrent events and the risk of death were analyzed using a Cox model for time-dependent variables.
Results: A total of 3081 patients were included (mean (SD) age: 86.4 (5.5)). In the multivariate analysis, the relative risk (95% confidence interval [CI]) of hospital readmission rose progressively to 2.66 (1.44; 5.14), and the risk of death rose to 2.01 (1.23; 3.32) after five hospital admissions, relative to a patient with no hospital readmissions. The number of hospital readmissions during the follow-up period was the primary risk factor and the best predictor of the risk of hospital readmission and the risk of death.
Conclusion: Hospital readmission is the primary risk factor for further hospital readmissions and for death in older subjects discharged from an AGU.
Keywords: hospital readmission, death, older patients, acute geriatric unit, risk factors, recurrent events
Plain Language Summary
Recurrent hospital admission is a major problem among older people. Each hospital readmission increases the risks of further hospital readmissions and death. However, the importance of the number of hospital readmissions (relative to other known risk factors) has not previously been determined.
Our findings show that the number of hospital readmissions during the follow-up period of 12 months is the main risk factor for further hospital readmission and for death in older patients discharged from an acute geriatric medicine unit. A simultaneous analysis of the risks of hospital readmission and death enables us to identify the factors more associated with organic phenomena (such as the presence of a cancer) or more associated with life decisions and circumstances (such as living in a retirement home).
The many risk factors associated with hospital readmission and death are key issues, and a number of interventions have been developed with a view to reducing the occurrence of these events. Our results show that studies of hospital readmission should consider the number of consecutive admissions (ie the rank) for each patient because it is the main risk factor.
Introduction
In older patients, hospital readmissions increase morbidity, mortality, the loss of functional independence, and healthcare costs.1–4 Although many researchers have focused on the readmission of older people to hospital, the studies were limited to the analysis of the first hospital readmission during a set period (ranging from 30 days to 24 months after the index discharge).5–9 The effect of each new hospital readmission on the risk of further hospital readmissions has barely been studied. Moreover, research on hospital readmissions has not analyzed deaths, whereas certain characteristics (such as polypharmacy, comorbidities and malnutrition) have been linked to hospital readmission in some studies8,10 and to death in others.7,11
In fact, it is possible to analyze death and multiple hospital readmissions during follow-up by using appropriate statistical models.12 Models for recurrent event analysis are developed in the framework of counting process theory and are used to analyse the impact of previous hospital stays on the risk of hospital readmission and death. We have used this type of model to show that each hospital readmission during the follow-up period is a major risk factor for further hospital readmission and death in older patients.13 However, the number of adjustment variables was limited, and the model suggested that the study population was heterogeneous. It therefore remained to be determined whether hospital readmission per se is a major risk factor for further hospital readmissions or whether it is an indirect marker of other risk factors. If hospital readmission per se is a major risk factor for further hospital readmissions, then hospital readmission should promote specific interventions (eg communication) that could reduce the risk of further hospital readmissions.14,15
The most fragile older patients are managed in acute geriatric units (AGUs). In France, all AGUs are labelled and have similar equipment, medical staffs, and quality of care. The incidence of hospital readmission and/or death after hospitalization in an AGU is high16 The French DAMAGE (Patient Outcomes After Hospitalization in Acute Geriatric Unit) multicentre study involved a standardized evaluation of many known risk factors for death and hospital readmission after discharge from an AGU and followed the patients up for 12 months.
The primary objective of the present analysis of the DAMAGE cohort was to determine the impact of the number of consecutive readmission (ie the rank) on the risks of future hospital readmissions and death after discharge from an AGU. The analyses were adjusted for the many known risk factors for hospital readmission and death.
Methods
Study Design
The DAMAGE study is a multicentre, prospective cohort study of patients aged 75 or over hospitalized in an AGU in the Hauts-de-France and Normandie regions of France (NCT02949635). The six recruiting centres are Lille University Hospital (Lille, France; 2 AGUs), Saint Philibert Hospital (Lille, France; 1 AGU), Amiens-Picardie University Hospital (Amiens, France; 1 AGU), Caen University Hospital (Caen, France; 1 AGU), and Saint Quentin General Hospital (Saint Quentin, France; 1 AGU). Patients discharged from the AGU to a non-acute facility (the patient’s home, a residential home, or a rehabilitation unit) were followed up for one year. The inclusion period ran from September 14th, 2016, to January 29th, 2018. The last 12-month follow-up visit was performed on January 29th, 2019.
Ethical Approval
The DAMAGE study was performed in compliance with the terms of the Declaration of Helsinki and was approved by the local independent ethics committee (CPP Nord-Ouest IV, Lille, France) on February 13th, 2015, with an amendment approved on January 21st, 2016 (reference: IDRCB 2014 A01670 47, CNIL. bxA15352514).
The patients and their primary family caregivers or legal representatives were given detailed verbal and written information about the study, in order to ensure that the patients fully understood the potential risks and benefits of participation. In accordance with the French legislation on observational, non-interventional studies of routine clinical care, written consent was not required. The patients were informed that they could refuse to participate in the study and that refusal would not have any impact on their treatment in the AGU. If the patient was unable to refuse to participate in the DAMAGE study (notably because of severe neurocognitive disorders), the next of kin or legal representative could refuse participation. All participants were free to withdraw from the study at any time. This withdrawal had no impact on the care received.
Inclusion and Exclusion Criteria
All patients aged 75 and over, with health insurance coverage and hospitalized in an AGU were eligible for inclusion in the study. Patients hospitalized in the AGU for less than 48 hours were not included because this short duration prevented the completion of a comprehensive geriatric assessment. Patients admitted for immediate palliative care were not considered for inclusion in the study because of the high risk of death. Lastly, patients who refused to participate to the study (as notified by the patient or his/her primary family caregiver or legal representative) were not included. However, cognitive impairment was not an exclusion criterion per se.
Patients who died in the AGU were excluded because one of the study’s objectives concerned the assessment of the death rate after discharge. Patients transferred to another acute care ward (a surgical ward or a non-geriatric ward) without returning to the AGU were also excluded. Patients transferred to palliative care units or having received palliative care during the stay in the AGU were also excluded because of the above-mentioned high risk of death.
Collection of Data During the Stay in the AGU
Data were collected at various time points during the stay in the initial AGU, using a case report form. The social, medical and geriatric variables recorded within 72 hours of admission, during hospitalization, and upon discharge are listed in Supplement 1.
- The social and medical variables recorded on admission included the age, sex, type of home environment (own home or residential home), number of previous hospital stays, the Charlson Comorbidity Index (CCI),17 and presence of cancer. The geriatric variables recorded on admission included the number of medications usually taken, dependency before hospitalization (the Katz Index of independence in activities of daily living (Katz ADL)),18 malnutrition (weight loss and body mass index), cognitive disorders, history of depression, swallowing disorders, and walking ability. Standard laboratory variables were also recorded.
- During the hospital stay, a daily evaluation of clinical status enabled us to classify the patient into one of five predefined states: late discharge, a medical obstacle to discharge (other than infection), treatment of a community-acquired infection, treatment of a hospital-acquired infection, and palliative care. These clinical states were mutually exclusive (ie only one state per day and per patient) and were determined by the patient’s attending physician.
- On the day of discharge, geriatric variables were also recorded: the patient’s bodyweight, the bodyweight difference between admission and discharge, the Katz ADL on discharge, the difference in Katz ADL between admission and discharge, and the discharge destination (the patient’s own home, a residential home, or a rehabilitation unit). The collected data were audited.
Follow-Up
The exact date of hospital readmission and the exact date of death were collected at 3 and 12 months after the index discharge from the AGU; this was done by phoning the patient (if alive), his/her next of kin or caregiver or the referent healthcare professional in a community setting (eg the general practitioner). Mortality was also evaluated by consulting freely available national mortality data.
Statistical Analysis
Categorical variables were expressed as the frequency (percentage). Continuous variables were expressed as the mean ± standard deviation (SD) if normally distributed or as the median [interquartile range (IQR)]. Normal data distributions were checked graphically and by applying the Shapiro–Wilk test. The median time intervals between consecutive hospital stays were calculated according to the hospital stay’s rank and were then represented graphically on boxplots.
The impact of clinical and laboratory variables on the outcomes (time to death, and time to a hospital admission) was assessed in a bivariate analysis (Supplement 2) and a multivariate analysis, using as semi-parametric Cox regression model and its extension to recurrent events. Number of patients will be refered to as the sample size (N = 3081).
The impact of consecutive hospitalizations on hospital readmission was assessed as a time-dependent variable. Hospital readmission counts were entered as categorical variables. The frailty model12 was used to account for multiple events (hospital readmissions). The frailty model enabled us to take account of interindividual variability in the risk of hospital readmission potentially not explained by the observed variables.
Likewise, the risk of death was estimated with a semi-parametric Cox model for time-dependent variables.19
The log-linearity hypothesis in the Cox proportional risks model was checked against the Martingale residuals.20 If the log-linearity hypothesis was not met for a given variable, it was dichotomized as a categorical variable. The dichotomization threshold was defined with a graphical assessment of the Martingale residuals and a chi-squared test (for death) and on the basis of an expert medical consensus.
An automatic stepwise procedure based on the Akaike information criterion21 was applied to both models.
To avoid case loss in the univariate and multivariate analyses, missing data for candidate predictors (missing data rate: from 0% to 8.6%, depending on the variable) were imputed by multiple imputation with a regression-switching approach (chained equations, m=5 imputations).22 The imputation procedure was performed with the missing-at-random assumption plus the predictive mean-matching method for continuous variables and logistic regression (binary, ordinal, or multinomial) models for categorical variables. Rubin’s rules were used to combine the estimates derived from multiple imputed data sets.23 Lastly, the relative importance of the predictors of hospital readmission and death was assessed with Wald’s test.24
In all analyses, we considered a maximum of five hospital stays per patient because the proportion of patients with more than five hospital stays was low (1%, data not shown); hence, reliable estimation of the study endpoint would not have been possible beyond this point.
All the analyses were performed with R software (version 3.4.3),25 using the survival package for the survival analyses and the mice package for the multiple imputation of the missing data.
Results
The Study Population
Of the 3509 patients hospitalized in the AGU, 202 died there, 97 were transferred to another non-geriatric medical or surgical acute unit (without returning to the AGU), and 98 were lost to follow-up after palliative care and/or were transferred to a palliative care unit. Overall, 3112 patients met all the inclusion criteria and none of the exclusion criteria. 31 patients presented errors in the hospitalization date during the follow-up period. Our analyses therefore covered a total of 3081 patients.
The study population’s general characteristics are summarized in Table 1. The population was very old (mean (SD) age: 86.4 (5.5)), with female predominance (66%), a high proportion of polypharmacy (mean number of drugs taken at home: 7.9 (3.6)). The prevalence of cognitive disorders was high (54.4%).
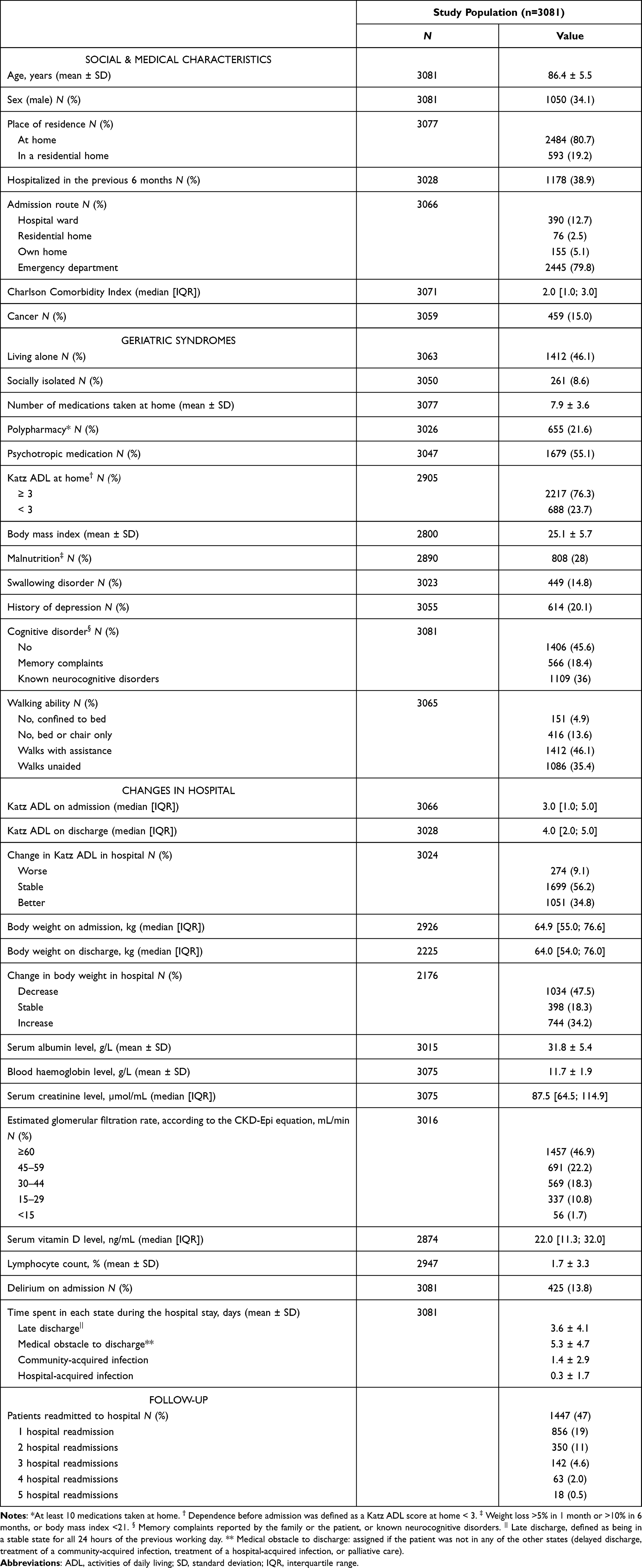 |
Table 1 The Characteristics of the Study Population |
Follow-Up and Events
A total of 1531 (49.7%) patients were readmitted to hospital at least once during the follow-up period, and 608 (19.7%) patients were readmitted to hospital twice or more. The median [IQR] time interval between two consecutive hospitalizations decreased as the rank of hospitalization increased (Figure 1); it decreased from 88 [45, 179] days between the initial hospitalization and the first hospital readmission to 31 [26, 47] days between the fourth and fifth hospital readmissions. During the follow-up, 1014 (32.9%) patients died, including 427 (13.9%) who had not been readmitted to hospital and 587 (19.1%) readmitted to hospital at least once.
 |
Figure 1 Median time interval between two consecutive hospitalizations. Median time intervals between consecutive hospital readmissions. The rank of the hospital stay corresponds to the ordered number of the readmission (1: time between the start date of the index hospitalization and the start date of the first hospital readmission, 2: the time between the start date of the first hospital readmission and the start date of the second hospital readmission, etc.). |
Importance of Consecutive Hospitalizations on the Risks of Hospital Readmission and Death
The results of the bivariate analysis are summarized in Supplement 2 and those of the multivariate analysis are summarized in Table 2. Consecutive hospital readmissions significantly increased both the risk of further hospital readmission and the risk of death. Indeed, the relative risk (RR) (95% CI) for hospital readmission rose from 1.31 (1.08, 1.60) after one hospital admission to 2.66 (1.44, 5.14) after five hospital admission (relative to a patient not readmitted to hospital). The risk (95% CI) of death (hazard ratio) also increased with the number of consecutive hospitalizations, it rose from 1.61 (1.48, 1.76) after one hospital readmissions to 2.01 (1.23, 3.32) after five hospital readmissions (relative to a patient not readmitted to hospital). The number of hospital readmissions during the follow-up period was the variable that best predicted the risks of further hospital readmission and death (Figure 2).
 |
Table 2 Multivariate Analyses of the Risk of Hospital Readmission (Using a Frailty Model) and the Risk of Death (Using a Time-Dependent Cox Regression Model) in the Study Population (N=3081 Patients) |
 |
Figure 2 Importance of the variables of the model in the prediction of the risks of hospital readmission and death. Wald’s test was performed. Each variable in the model was tested against the empty model, in order to determine which best predicted the risks of hospital readmission and death. The variable “Number of previous hospitalizations” was the most predictive for the two outcomes, as shown below. The proportion of the overall chi-square for each variable was calculated as a proportion of the sum of chi-squared statistics, obtained from Wald tests for each variable separately. |
Importance of Other Factors with Regard to the Risks of Hospital Readmission and Death
Some characteristics were significantly associated with both hospital readmission and death. Thus, cancer and each extra day in hospital due to a medical obstacle were significantly associated with greater risks of hospital readmission and death. In contrast, female sex was significantly associated with lower risks. Lastly, living in a retirement home was associated with a lower risk (95% CI) for hospital readmission (relative risk (RR) = 0.81 (0.68, 0.92)) but a greater risk (95% CI]) for death (hazard ratio (HR) = 1.20 (1.08, 1.34), relative to people living at home.
Some characteristics were associated only with the risk of hospital readmission: weight gain during the hospital stay (RR (95% CI) = 1.17 (1.02, 1.33)) and polypharmacy (1.24 (1.11, 1.36)). In contrast, older age and some geriatric syndromes were associated only with the risk of death: malnutrition (HR (95% CI) = 1.13 (1.04, 1.26)), confinement to bed (1.24 (1.01, 1.53)) and limited independence one month before hospitalization (1.05 (1.02, 10.8)).
Discussion
Our study confirmed the importance of taking account of consecutive hospitalizations when analyzing the risks of further hospital readmissions and death in older people. Hospital readmission is a major event that accelerates and increases the likelihood of further new hospital readmission and of death. Consequently, the statistical analysis of hospital readmission should not be considered without considering death, and vice versa.26
We analyzed the risks of hospital readmission and death after adjusting for many variables known to be associated with one or both of these outcomes.1,3,4,6–11 We have previously reported that the risks of hospital readmission and death were strongly influenced by the hospital readmission process.13 However, this analysis was limited by the number of available adjustment variables (ie age, sex, and the CCI). Our present results confirmed the importance of the rank and time to hospital readmission on the change in the risks of hospital readmission and death. Our results showed that the hospital readmission rank was the primary risk factor for hospital readmission and death in older patients discharged alive from an AGU. The risk of hospital readmission increased slowly until the second hospital readmission and then rose sharply until five hospital readmissions. The risk of death increased more slowly with the number of hospital readmissions, from the first readmission onwards. Consecutive hospitalizations, therefore, capture risk in addition to the other proxy, in connection with a possible inter-individual variability, present in older people.
The bothrisks of hospital readmission and death enabled us to highlight the influence of other characteristics related to these two outcomes. Some corresponded to “organic” patient characteristics, such as the presence of cancer27 or a medical obstacle to discharge from the AGU.2 These characteristics probably reflect the severity of the patient’s illness. Other characteristics appeared to correspond to “decisional” processes. For example, living in a retirement home increased the risk of death but decreased the risk of being readmitted to hospital. This suggests that a consensual ethical decision (involving the patient and/or his/her family) had been taken in favour of care (and perhaps palliative care) in the retirement home rather than in hospital. More surprisingly, a few characteristics were related only to hospital readmission or only to death. Some of these increased the risk of hospital readmission without increasing the risk of death; they included some known risk factors documented in the literature (such as polypharmacy8) and factors more specifically linked to clinical practice in the AGU (such as weight loss during the hospital stay). The latter variable certainly testified to the presence of medical signs of an unstable clinical state (such as volume expansion or decompensated oedema). In contrast, some factors were associated with a greater risk of death but not a greater risk of hospital readmission. This was true for known risk factors frequently observed among older patients in the AGU, such as loss of independence,28 malnutrition,7 and walking difficulties.29
All these results showed that a specific methodological framework should be applied to the analysis of the risks of hospital readmission and death. The analysis of the risk of hospital readmission just a few days30 or at 30 days1,2,5 after an index discharge does not appear to be appropriate because it fails to fully take account of the patient’s consecutive hospitalizations. The use of statistical models designed for studying recurrent events is therefore more appropriate when a patient has been admitted to hospital several times.13 Hospital readmissions should thus be analyzed precisely because they reflect a frequent clinical picture among older adults. Most of the studies of patient pathways in this population have focused on the occurrence of events like hospital readmission or death. Our results show that these patient pathways should take account of all the patient’s hospital admissions and should use appropriate analytical methods, such as those applied here. Lastly, the conjoint analysis of the risks of hospital readmission and death is recommended because death is a competing risk that prevents hospital readmission. Some specific statistical models have recently been developed for this purpose31 but have not yet been applied to large cohorts like DAMAGE.
The present study had a number of strengths. Firstly, we used high-quality data from a multicentre cohort of AGU patients AGU (N = 3081), with a low proportion of missing data (often below 5%). Secondly, this was (to the best of our knowledge) the first multicentre study of older patients discharged from an AGU to have included with standardized geriatric evaluation. Thirdly, we had few exclusion criteria. Lastly, we used specific statistical models to study of recurrent events with time-dependent covariables.
However, our study also had some limitations. Firstly, the older patients in our cohort were discharged from an AGU and were often very old, with multiple comorbidities. Our results cannot therefore, be extrapolated to the population of older adults as a whole. Secondly, we considered that the duration of each hospital readmission was negligible relative to the risk of subsequent hospital readmission. This might have been be an overly simple assumption because the length of stay has been linked to the risk of readmission.2 However, we included the length of the index hospital stay in the model and divided it into time with a medical obstacle to discharge and late discharge. Thirdly, we were unable to account for all comorbidities in detail or for all acute or new diagnosis at the time of the index hospitalization. Such a level of detail might have allowed us to identify pathological situations at higher risk of death or hospital readmission. However, we used a comorbidity score that has been validated in geriatrics17,32 and that can be used in routine practice. Furthermore, there is no validated classification or scoring method for acute pathologies in geriatrics. We therefore proposed a simple 5-stage classification (delayed discharge, medical obstacle to discharge, community-acquired infection, hospital-acquired infection, palliative care) that was associated with hospital readmission and death. Such a classification would deserve to be tested and validated in other studies. Lastly, the presence of potentially inappropriate medications or potential medication omissions on admission to the hospital were recently associated with HR and death33 but were not collected in our cohort. Polypharmacy has been strongly associated with PIMs and PPOs but polypharmacy was significantly associated with hospital readmission only in our study.
Conclusions
Hospital readmission is the primary risk factor for further hospital readmission and for death in older adults discharged from an AGU. Taken as a whole, our present results suggest that studies of hospital readmission or death among older patients should include (i) all hospital readmissions, (ii) a sufficiently long follow-up period, and (iii) a simultaneous analyses of the two outcomes.
Abbreviations
ADL, activities of daily living; AGU, acute geriatric unit; CI, confidence interval; HR, hazard ratio; RR, relative risk; SD, standard deviation.
Acknowledgments
We thank all the physicians who helped to recruit patients in the centres (Lille University Hospital, Saint Philibert Hospital, Amiens-Picardie University Hospital, Caen University Hospital, and Saint Quentin General Hospital.
We thank David Fraser PhD (Biotech Communication SARL, Ploudalmézeau, France) for copy-editing assistance.
Funding
The DAMAGE cohort study is funded by the French government’s inter-regional hospital-based clinical research programme (reference: PHRC I 13-097).
Disclosure
Professor Jean-Baptiste Beuscart reports grants from French government’s inter-regional hospital-based clinical research programme, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Lanièce I, Couturier P, Dramé M, et al. Incidence and main factors associated with early unplanned hospital readmission among French medical inpatients aged 75 and over admitted through emergency units. Age Ageing. 2008;37(4):416–422. doi:10.1093/ageing/afn093
2. Garcia-Perez L, Linertova R, Lorenzo-Riera A, Vazquez-Diaz JR, Duque-Gonzalez B, Sarria-Santamera A. Risk factors for hospital readmissions in elderly patients: a systematic review. QJM. 2011;104(8):639–651. doi:10.1093/qjmed/hcr070
3. Sharma Y, Miller M, Kaambwa B, et al. Malnutrition and its association with readmission and death within 7 days and 8–180 days postdischarge in older patients: a prospective observational study. BMJ Open. 2017;7(11):e018443.
4. Lau D, Padwal RS, Majumdar SR, et al. Patient-Reported Discharge Readiness and 30-Day Risk of Readmission or Death: a Prospective Cohort Study. Am J Med. 2016;129(1):89–95. doi:10.1016/j.amjmed.2015.08.018
5. Gauthier J, Kisterman JP, Chapalain F, Texier A, Manckoundia P. Réhospitalisation précoce des personnes âgées d’au moins 75 ans admises dans un service de médecine polyvalente post-urgence: taux et facteurs prédictifs. Rev Médecine Interne. 2016;37(8):521–528.
6. Franchi C, Nobili A, Mari D, et al. Risk factors for hospital readmission of elderly patients. Eur J Intern Med. 2013;24(1):45–51. doi:10.1016/j.ejim.2012.10.005
7. Dramé M, Lang PO, Novella J-L, et al. Six-month outcome of elderly people hospitalized via the emergency department: the SAFES cohort. Rev DÉpidémiologie Santé Publique. 2012;60(3):189–196.
8. Sganga F, Landi F, Volpato S, et al. Predictors of rehospitalization among older adults: results of the CRIME Study: predictors of rehospitalization. Geriatr Gerontol Int. 2016. doi:10.1111/ggi.12938
9. Crane SJ, Tung EE, Hanson GJ, Cha S, Chaudhry R, Takahashi PY. Use of an electronic administrative database to identify older community dwelling adults at high-risk for hospitalization or emergency department visits: the elders risk assessment index. BMC Health Serv Res. 2010;10:338. doi:10.1186/1472-6963-10-338
10. Rosted E, Schultz M, Sanders S. Frailty and polypharmacy in elderly patients are associated with a high readmission risk. Dan Med J. 2016;63(9):548.
11. Masnoon N, Kalisch Ellett L, Shakib S, Caughey GE. Predictors of Mortality in the Older Population: the Role of Polypharmacy and Other Medication and Chronic Disease-Related Factors. Drugs Aging. 2020;37(10):767. doi:10.1007/s40266-020-00794-7
12. Wei LJ, Lin DY, Weissfeld L. Regression Analysis of Multivariate Incomplete Failure Time Data by Modeling Marginal Distributions. J Am Stat Assoc. 1989;84(408):1065–1073. doi:10.1080/01621459.1989.10478873
13. Visade F, Babykina G, Lamer A, et al. Importance of previous hospital stays on the risk of hospital re-admission in older adults: a real-life analysis of the PAERPA study population. Age Ageing. 2021;50(1):141–146. doi:10.1093/ageing/afaa139
14. Becker C, Zumbrunn S, Beck K, et al. Interventions to Improve Communication at Hospital Discharge and Rates of Readmission: a Systematic Review and Meta-analysis. JAMA Netw Open. 2021;4(8):e2119346. doi:10.1001/jamanetworkopen.2021.19346
15. Berntsen GKR, Dalbakk M, Hurley JS, et al. Person-centred, integrated and pro-active care for multi-morbid elderly with advanced care needs: a propensity score-matched controlled trial. BMC Health Serv Res. 2019;19(1):682. doi:10.1186/s12913-019-4397-2
16. Campbell SE, Seymour DG, Primrose WR; ACMEPLUS Project. A systematic literature review of factors affecting outcome in older medical patients admitted to hospital. Age Ageing. 2004;33(2):110–115. doi:10.1093/ageing/afh036
17. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
18. Katz S, Downs TD, Cash HR, Grotz RC. Progress in Development of the Index of ADL. Gerontologist. 1970;10(1Part 1):20–30. doi:10.1093/geront/10.1_Part_1.20
19. Zhang Z, Reinikainen J, Adeleke KA, Pieterse ME, Groothuis-Oudshoorn CGM. Time-varying covariates and coefficients in Cox regression models. Ann Transl Med. 2018;6(7):121. doi:10.21037/atm.2018.02.12
20. Therneau TM, Grambsch PM, Fleming TR. Martingale-based residuals for survival models. Biometrika. 1990;77(1):147–160. doi:10.1093/biomet/77.1.147
21. Wood AM, White IR, Royston P. How should variable selection be performed with multiply imputed data? Stat Med. 2008;27(17):3227–3246. doi:10.1002/sim.3177
22. Rubin DB. Multiple Imputation for Nonresponse in Surveys. Hoboken NJ. Wiley-Interscience; 2004. 287. Wiley classics library.
23. Buuren S, Groothuis-Oudshoorn K. mice: multivariate Imputation by Chained Equations in R. J Stat Softw. 2011;45(3). doi:10.18637/jss.v045.i03
24. Heller G. A measure of explained risk in the proportional hazards model. Biostat Oxf Engl. 2012;13(2):315–325.
25. R Core Team. R: a language and environment for statistical computing. Vienna, Austria: r Foundation for Statistical Computing; 2013. Available from: http://www.R-project.org/.
26. Putter H, Fiocco M, Geskus RB. Tutorial in biostatistics: competing risks and multi-state models. Stat Med. 2007;26(11):2389–2430. doi:10.1002/sim.2712
27. Heijnsdijk EAM, Csanádi M, Gini A, et al. All-cause mortality versus cancer-specific mortality as outcome in cancer screening trials: a review and modeling study. Cancer Med. 2019;8(13):6127–6138. doi:10.1002/cam4.2476
28. Seguchi M, Sakakura K, Tsukui T, et al. Determinants of In-Hospital Death Among the Very Elderly with Acute Myocardial Infarction. Int Heart J. 2020;61(5):879–887. doi:10.1536/ihj.20-165
29. Lum HD, Studenski SA, Degenholtz HB, Hardy SE. Early Hospital Readmission is a Predictor of One-Year Mortality in Community-Dwelling Older Medicare Beneficiaries. J Gen Intern Med. 2012;27(11):1467–1474. doi:10.1007/s11606-012-2116-3
30. Cunha Ferré MF, Gallo Acosta CM, Dawidowski AR, Senillosa MB, Scozzafava SM, Saimovici JM. 72-hour hospital readmission of older people after hospital discharge with home care services. Home Health Care Serv Q. 2019;38(3):153–161. doi:10.1080/01621424.2019.1616024
31. Choi Y-H, Jacqmin-Gadda H, Król A, Parfrey P, Briollais L, Rondeau V. Joint nested frailty models for clustered recurrent and terminal events: an application to colonoscopy screening visits and colorectal cancer risks in Lynch Syndrome families. Stat Methods Med Res. 2020;29(5):1466–1479. doi:10.1177/0962280219863076
32. Novella A, Elli C, Tettamanti M, et al. Comparison between drug therapy-based comorbidity indices and the Charlson Comorbidity Index for the detection of severe multimorbidity in older subjects. Aging Clin Exp Res. 2021;33(7):1929–1935. doi:10.1007/s40520-020-01706-w
33. Thomas RE, Nguyen LT, Jackson D, Naugler C. Potentially Inappropriate Prescribing and Potential Prescribing Omissions in 82,935 Older Hospitalised Adults: association with Hospital Readmission and Mortality within Six Months. Geriatrics. 2020;5(2):37. doi:10.3390/geriatrics5020037
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.