Back to Journals » International Journal of Women's Health » Volume 17
Risk Factors for Histologic Chorioamnionitis Among Women with Prenatal Fever During Preterm Delivery: A Retrospective Cohort Study
Authors Lin N, Shi Y, Xia Y, Yang Y, Hua R
Received 24 May 2025
Accepted for publication 14 October 2025
Published 23 October 2025 Volume 2025:17 Pages 3777—3788
DOI https://doi.org/10.2147/IJWH.S542606
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Nan Lin,1,2,* Yiru Shi,1,2,* Yuanqing Xia,1,2 Yunfan Yang,1,2 Renyi Hua1,2
1Department of Obstetrics, the International Peace Maternity and Child Health Hospital, School of Medicine, Shanghai Jiao Tong University, Shanghai, 200030, People’s Republic of China; 2Shanghai Key Laboratory of Embryo Original Diseases, Shanghai, 200030, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Renyi Hua, Email [email protected]
Background and Objective: Histologic chorioamnionitis (HCA) complicates preterm birth and adversely affects neonatal and maternal outcomes; however, early recognition remains challenging. Here, we aimed to identify risk factors for HCA and assess its impact on pregnancy outcomes in preterm deliveries with prenatal fever.
Design: Retrospective cohort analysis.
Setting: Tertiary obstetrics and Gynecology Hospital in Shanghai, China.
Participants: A total of 220 women who delivered preterm (gestational age < 37 weeks) with prenatal fever between January 2018 and December 2020 were ultimately included in the study. This included an HCA group (101 cases) and control group (119 cases).
Main Outcome Measures: HCA diagnosis by placental pathology; neonatal outcomes.
Results: The incidence of congenital infection (27.66 vs 15.38%, P=0.029) and neonatal sepsis (8.89 vs 0.90%, P=0.017) was significantly greater in the HCA group than in the control group. Fever interval and PROM between 24 to 48 h (aOR=3.603, 95% CI 1.027~12.644) and > 48 h (aOR=6.201, 95% CI 1.729~22.238) were associated with HCA. A maternal WBC count ≥ 11× 109/L demonstrated a sensitivity of 80%, a specificity of 46%, a positive predictive value of 56.3%, and a negative predictive value of 73.3% for HCA prediction. A maternal white blood cell count ≥ 11× 109/L demonstrated optimal discriminatory power for HCA (AUC=0.667, 95% CI 0.569~0.738).
Conclusion: HCA significantly increases the risks of neonatal sepsis and congenital infection in preterm infants. A prolonged PPROM-fever interval (> 24 h) and a maternal WBC ≥ 11× 109/L are key predictive factors for the need for active obstetric intervention. This study provides evidence-based cutoff values for clinical decision-making in preterm pregnancies with fever, potentially improving maternal and neonatal outcomes through timely intervention.
Plain Language Summary: 1.The study identified clinically relevant risk factors, including the novel finding of an optimal WBC cutoff value (11× 109/L) for predicting histological chorioamnionitis, which could assist obstetricians in early clinical decision-making.The study performed multiple logistic regression analysis to control for potential confounders, providing robust evidence for the association between various maternal factors and histological chorioamnionitis.The single-center design limits the generalizability of our findings, as practices and patient populations may vary across different institutions and regions.The observational retrospective design prevents establishment of causal relationships and may introduce unmeasured confounding factors despite our statistical adjustments.
Keywords: histologic chorioamnionitis, prenatal fever, preterm birth, preterm premature rupture of membranes
Introduction
Chorioamnionitis (CAM) is a common complication of pregnancy that affects more than 25% of preterm pregnancies and it can lead to various adverse neonatal and maternal outcomes.1–3 It is an acute inflammatory process of the intrauterine environment caused by pathogenic microorganisms that have invaded the chorion, placenta, and umbilical cord. This can lead to preterm delivery, premature rupture of membranes (PROM), fetal distress, stillbirth, neonatal sepsis, and postpartum infection, thus posing a threat to the health of both the mother and the infant.4–6 CAM can also place a great economic burden on individuals as well as the possibility of deteriorating neonatal outcomes in pregnant women with fever complicated with histologic chorioamnionitis (HCA).5,7,8
Chorioamnionitis (CAM) remains a significant obstetric complication, with a systematic review showing an overall incidence of 3.9% (95% CI 1.8–6.8%), dramatically increasing to 25–40% in preterm births.9,10 Based on different diagnostic criteria, CAM is classified into clinical chorioamnionitis (CCA) and HCA. The diagnosis of CCA is based on a maternal temperature ≥38°C accompanied by either fetal tachycardia, purulent vaginal discharge, or maternal leukocytosis. In contrast, HCA is based on a pathological examination of the placenta after delivery.11 However, the diagnosis of CCA does not necessarily lead to HCA, as HCA can often be clinically silent.12,13
HCA significantly affects perinatal outcomes and is strongly associated with preterm birth, which is the main cause of morbidity and mortality in neonates.4,12,14 Preterm neonates exposed to intrauterine infection face substantially increased risks of perinatal hypoxia, cerebral palsy, bronchopulmonary dysplasia, pneumonia, early-onset sepsis, and death.7,8,15 Early identification and timely intervention for HCA in preterm birth could improve neonatal outcomes. However, the contradiction of expectant treatment due to the immature fetus and the timing to terminate pregnancy remains unsolved when maternal fever occurs. The precise clinical predictors of HCA in preterm birth are still lacking. Here, we hypothesize that specific clinical and laboratory parameters, particularly the timing, duration, and magnitude of maternal fever combined with inflammatory biomarkers, can predict HCA in preterm births and guide clinical decision-making. Therefore, this retrospective study compared maternal-neonatal outcomes between preterm births with and without HCA and analyzed comprehensive clinical and laboratory characteristics. We aimed to provide clinical evidence for the diagnosis and the timing of intervention for HCA and to improve the associated maternal and neonatal prognosis.
Materials and Methods
Study Design
This retrospective study was conducted at the Department of Obstetrics and Gynecology of International Peace Maternal and Child Health Hospital between January 2018 and December 2020. This study was approved by the Ethics Review Board of the International Peace Maternity and Child Health Hospital Affiliated to the Shanghai JiaoTong University School of Medicine.
A total of 220 women were eligible for the study. On the basis of previous studies showing an HCA prevalence of 25–40% in preterm births,9,10 with an expected effect size of 0.3, α=0.05, and power=80%, a minimum sample size of 176 was needed. Our final sample of 220 participants provided adequate power for the analysis. The eligibility criteria included a singleton preterm live birth (28–36+6 weeks) with a body temperature ≥ 37.5 °C measured twice 30 minutes apart and available histopathological results of the placenta following delivery. Prenatal fever was defined as a body temperature ≥37.5°C measured twice 30 minutes apart during the antepartum period, occurring within 48 hours before delivery. This study included both spontaneous preterm births and medically indicated preterm deliveries due to maternal or fetal complications. Blood tests were performed immediately after the body temperature reached ≥ 37.5 °C.
The exclusion criteria were multiple pregnancies, stillbirths and missing pathological data. All the data were collected from the electronic medical records. On the basis of the pathological examination results of the placenta, the datasets were divided into an HCA group (101 cases) and a control group (119 cases). Study enrollment is illustrated in Figure 1.
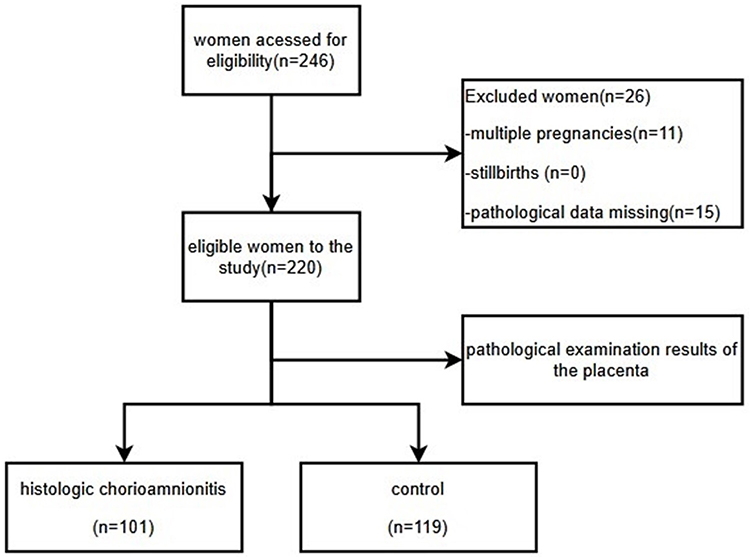 |
Figure 1 Flow chart of showing the pattern of recruitment. |
Patients were monitored for 34 weeks after conception, at which time labor was induced. Prophylactic antibiotics such as cephradine and penicillin were administered. Magnesium sulfate was administered intravenously for fetal neuroprotection and to inhibit uterine contraction. Steroids were given in 4 intramuscular doses of 6 mg for fetal lung maturation. Maternal and fetal status was closely monitored for the development of CCA, labor, or fetal compromise. Delivery was induced in the case of clinical CCA, active labor, fetal compromise or when the gestational age reached 34 weeks.
Methods and Data Collection
Baseline Characteristics
The baseline characteristics included maternal age, preconception body mass index (BMI), gravidity, parity, fertilization method (spontaneous or assisted) and pregnancy complications.
Obstetric Outcomes
CCA was diagnosed when there was a maternal fever ≥38 °C combined with one or more of the following symptoms: fetal tachycardia (≥160 bpm), maternal leukocytosis and purulent vaginal discharge.
The placenta was fixed in 10% neutral buffered formalin immediately after delivery. A minimum of two tissue samples were obtained from the placenta and routinely dehydrated, paraffin embedded, sliced and stained with hematoxylin-eosin by a single pathologist in the placental pathology department. The diagnostic criteria of HCA involved 5 visible neutrophils either confined to the layer of chorionic fibrous tissue or infiltrating in any of the structures of the placenta (fetal membranes, the placental disc, and the umbilical cord).16
Neonatal Outcomes
Neonatal outcomes included birth weight, 1-min Apgar score, neonatal intensive care unit (NICU) admission, asphyxia, hypoglycemia, respiratory distress syndrome, jaundice, deformities and fetal growth restriction. All neonates were weighed immediately after birth using a calibrated electronic scale and their 1-min Apgar scores were recorded. The association between HCA and neonatal outcomes was analyzed by multiple logistic regression. We also analyzed the impact of maternal antibiotic use on neonatal outcomes by multiple logistic regression.
Statistical Analysis
The data were analyzed by SPSS 24.0 statistical software and R3.5.1 statistical software with the Optimal Cutpoints software package. The Kolmogorov–Smirnov test was used to evaluate the normality of continuous variables. The continuous variables with normal distribution were compared using the t-test, whereas the variables with non-normal distribution were expressed as medians (quartiles), and the Mann‒Whitney U-test was used for comparison. Categorical variables were expressed as cases (%), and the chi-square test and Fisher’s exact test were used for comparison. Associated predictors were placed into a binary logistic regression model for identification of the independent relationships and to compute odds ratios (ORs), which are reported with 95% confidence intervals (CIs). Logistic regression modeling yielded adjusted odds ratios of the variables possibly linked to severe neonatal outcomes while controlling for prospective confounders. All statistically significant differences were defined as those for which the two-tailed P value was <0.05.
Results
The basic characteristics of the subjects in this study are given in Table 1, and they were not significantly different between the two groups. No significant difference was detected for the two groups when the mode of delivery and gestational age were compared.
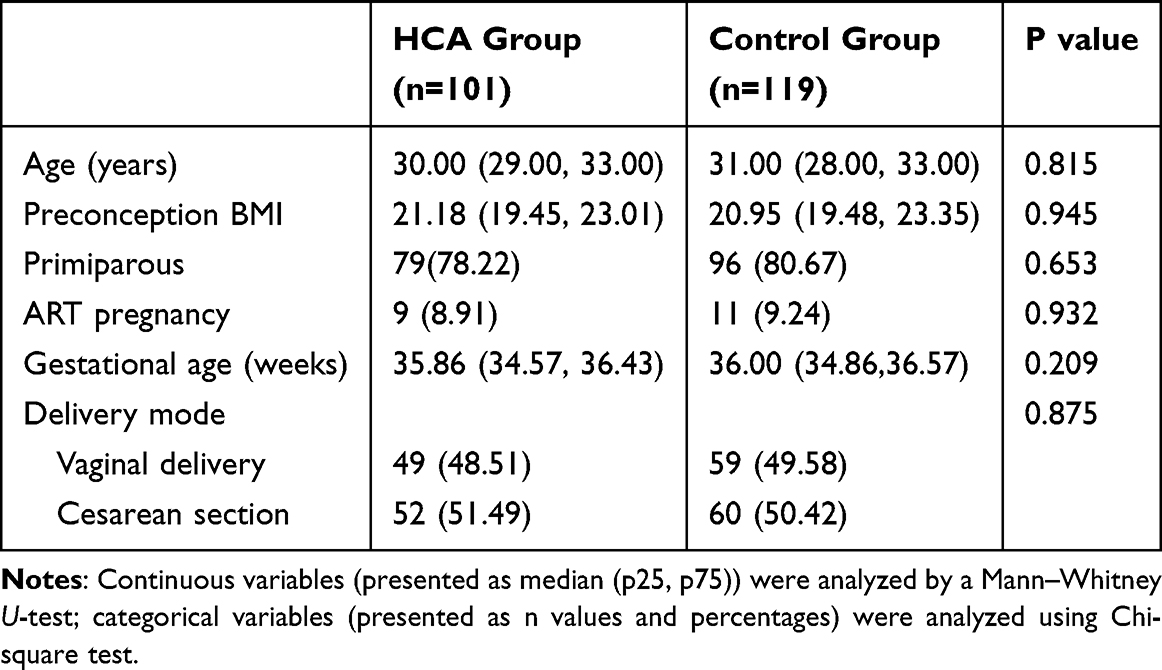 |
Table 1 Comparison of the Basic Characteristics of Pregnant Women Between the HCA and Control Groups |
Comparison of Obstetric and Neonatal Outcomes Between the Two Groups
The incidence of preterm premature rupture of membranes (PPROM) in the HCA group was significantly greater than that in the control group (75.25 vs 61.34%, P=0.028). However, the number of gestational weeks at which PPROM occurred differed between the two groups (median 35.45 vs 36.20 weeks, P=0.004). There was a significant difference in the interval between fever and PPROM between the two groups (P<0.05). In the HCA group, 45 (59.21%), 11 (14.47%) and 20 (26.32%) patients had intervals between fever and PPROM for t ≤ 24 h, 24 h < t ≤ 48 h and > 48 h, respectively. However, in the control group, the corresponding numbers of cases were 63 (86.30%), 5 (6.85%) and 5 (6.85%), respectively. The incidence of pregnancy-induced hypertension in the HCA group was lower than that in the control group (2.97 vs 11.76%, P<0.05). The prevalence of Ureaplasma urealyticum in the vaginal secretions of pregnant women in the HCA group was significantly greater than that in the control group (28.57% vs 16.07%, P<0.05) (Table 2).
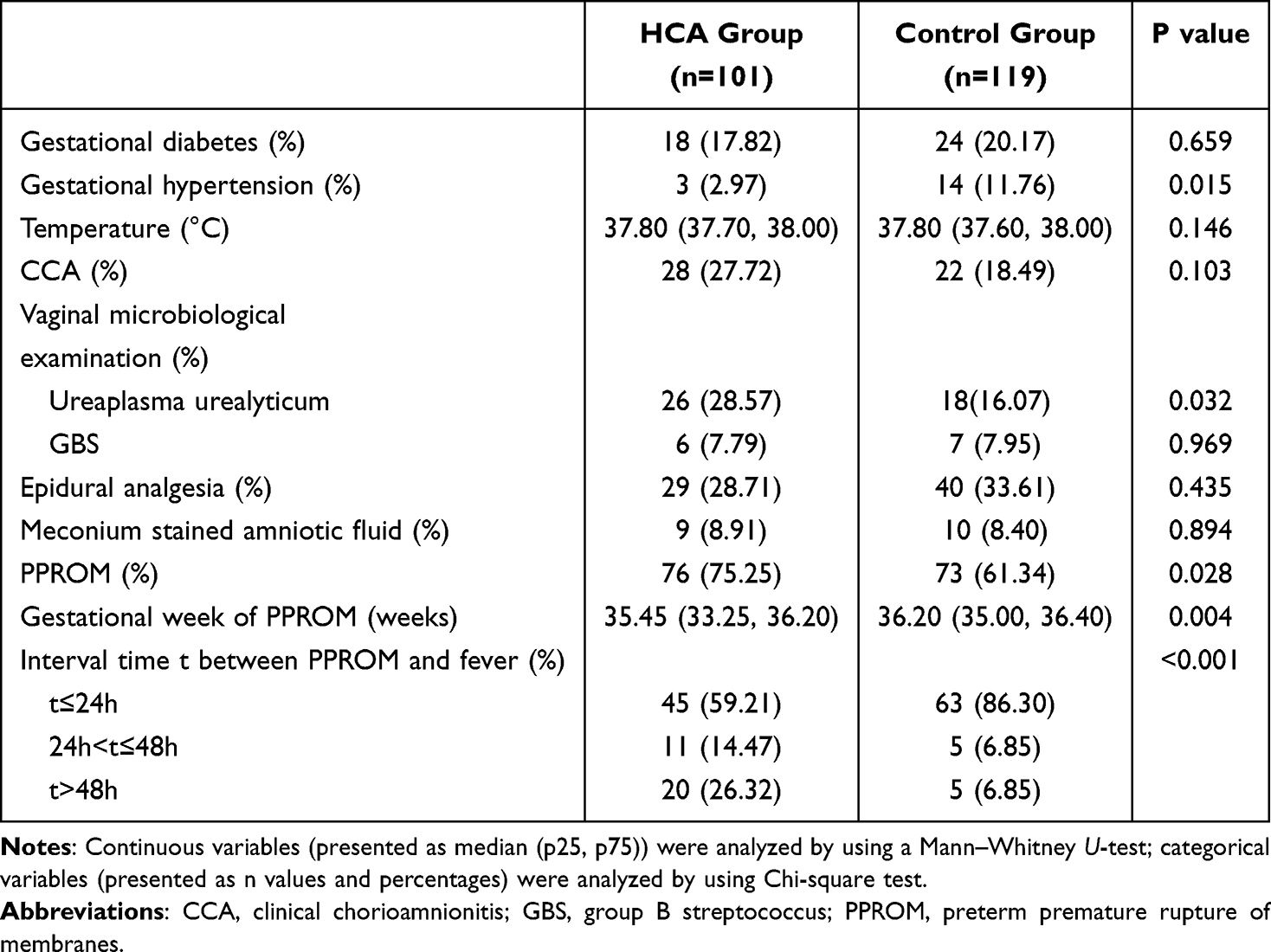 |
Table 2 Comparison of the Clinical Characteristics of Pregnant Women Between the HCA and Control Groups |
There was no significant difference between the two groups in terms of the incidence of gestational diabetes, fever temperature, clinical diagnosis of CCA, epidural analgesia, amniotic fluid pollution or the positive rate of Group B Streptococcus (GBS) in vaginal secretions (Table 2).
Birth weight and the 1-min APGAR did not significantly differ between the two groups. The incidence of congenital infection (27.66% vs 15.38%, P=0.029) and neonatal sepsis (8.89% vs 0.90%, P=0.017) in the HCA group was significantly greater than that in the control group (Table 3).
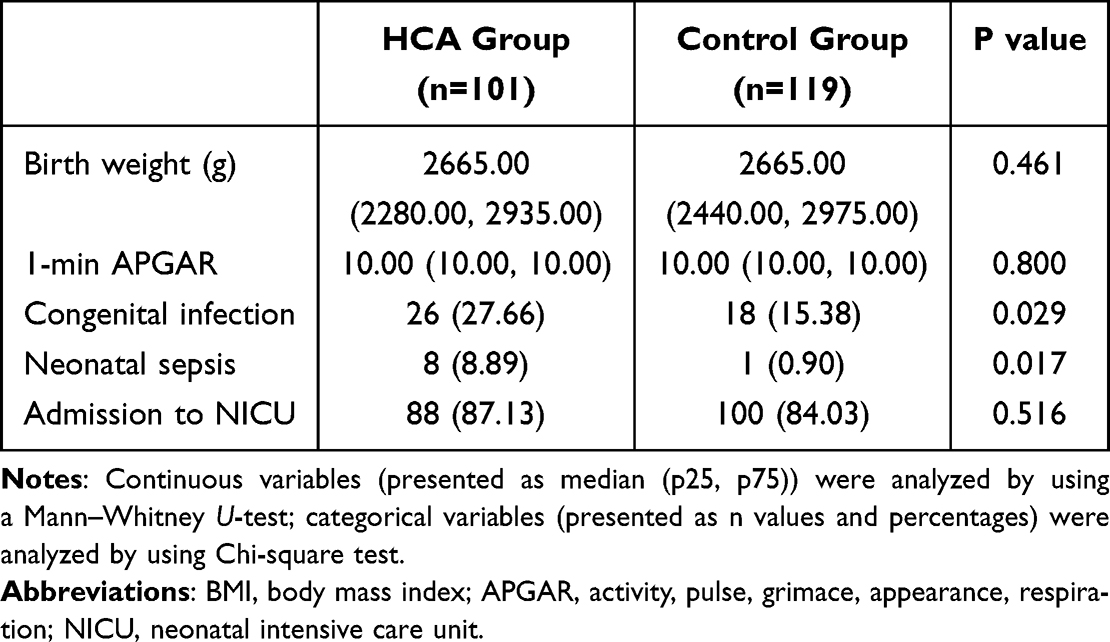 |
Table 3 Comparison of the Neonatal Outcomes Between the HCA and Control Groups |
Comparison of Maternal and Neonatal Blood Test results Between the Two Groups
Marked differences in the maternal WBC, neutrophil ratio and C-reactive protein (CRP) level were detected between the two groups (p < 0.05), whereas the neonatal WBC and neutrophil counts did not significantly differ. Neonatal CRP levels were significantly greater in the HCA group than in the control group (3.00 [0.00, 5.00] vs 4.00 [1.00, 6.50], P=0.002; Table 4).
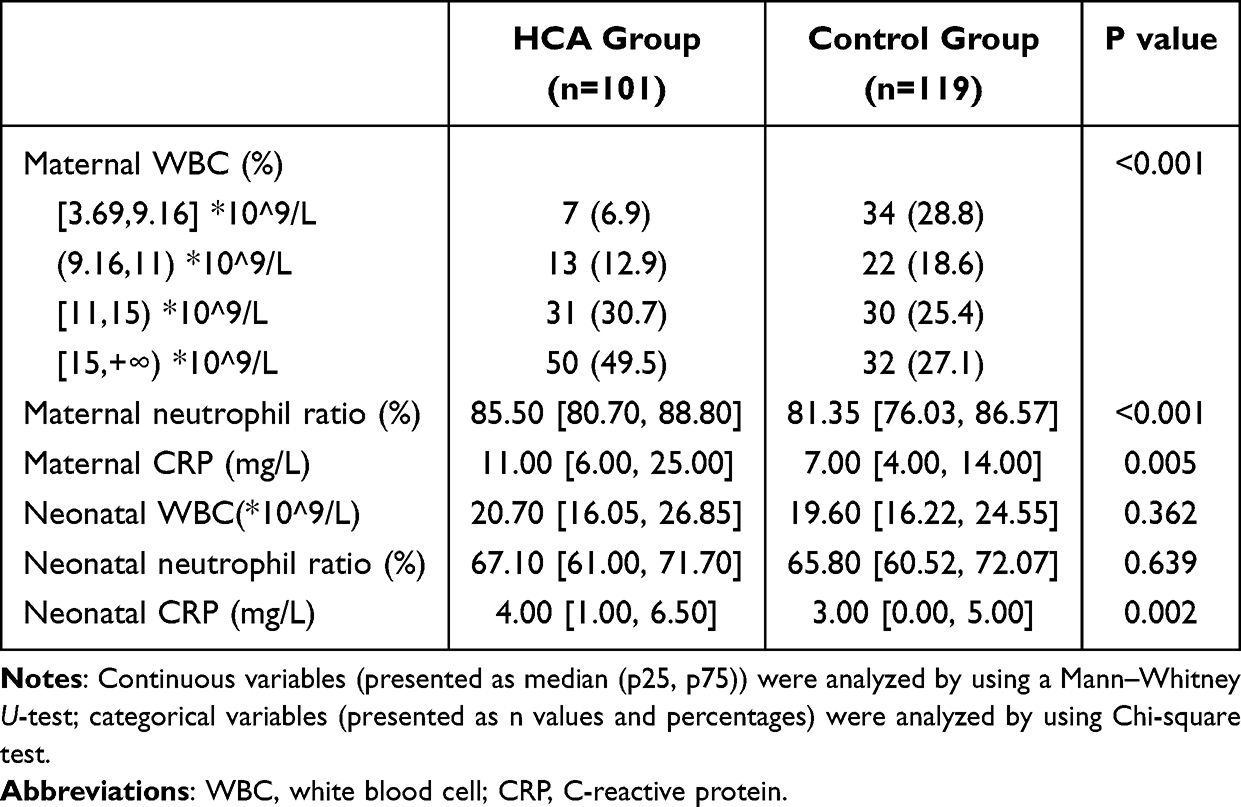 |
Table 4 Comparison of Characteristic of Maternal and Neonatal Blood Test results Between HCA Group and Control Group |
A receiver operating characteristic (ROC) curve was constructed to determine the ability of maternal WBC count to predict CAM. The WBC cutoff of 11×109/L had a sensitivity of 80%, a specificity of 46%, a positive predictive value of 56.3%, and a negative predictive value of 73.3%. The WBC cutoff value that best predicted CAM was 11*10^9/L (AUC = 0.667 (95% CI 0.569~0.738); sensitivity = 0.80; specificity = 0.46; Figure 2).
 |
Figure 2 ROC curve representing prediction of HCA by maternal WBC count. AUC: area under the curve is given with 95% confidence intervals. |
We also performed a correlation analysis of CRP levels in both maternal and neonatal blood. Since both CPRs had a non-normal distribution, Spearman correlation test was used, and the correlation coefficient was 0.183 (p = 0.010). A p-value less than 0.05 indicated that there was a significant monotonic relationship between maternal and neonatal CRP levels. A correlation coefficient >0 indicated that there was a positive correlation between maternal and neonatal CRP levels.
Multiple Logistic Regression Analysis of HCA Cases
The results of the independent tests for HCA pregnancies with PPROM, the gestational age at which PPROM occurred and the interval between PPROM and fever are shown in Table 5 (p < 0.05). Factors that showed significant differences when analyzed by univariate analysis were combined into a single logistic regression model to assess their independent effects on HCA (Table 5). We included these factors in the multiple logistic regression model, which controlled for potential confounders such as age, height, pre–pregnancy weight, gravidity, parity, gestational hypertension and gestational diabetes. Compared with pregnant women without PPROM, the risk of HCA among pregnant women whose interval between fever and PPROM was 24 h < t ≤ 48 h and > 48 h increased by 2.603 times (OR=3.603, 95% CI 1.027~12.644) and 5.201 times (aOR=6.201, 95% CI 1.729~22.238), respectively (Figure 3). Additionally, when the WBC count reached 11*10^9/L, the risk of HCA increased by 2.905 times (aOR=3.905, 95% CI 1.384~11.019), and the risk of CRP increased by 1.292 times (aOR=2.292, 95% CI 1.218~4.314) when it was over 10 (Figure 3).
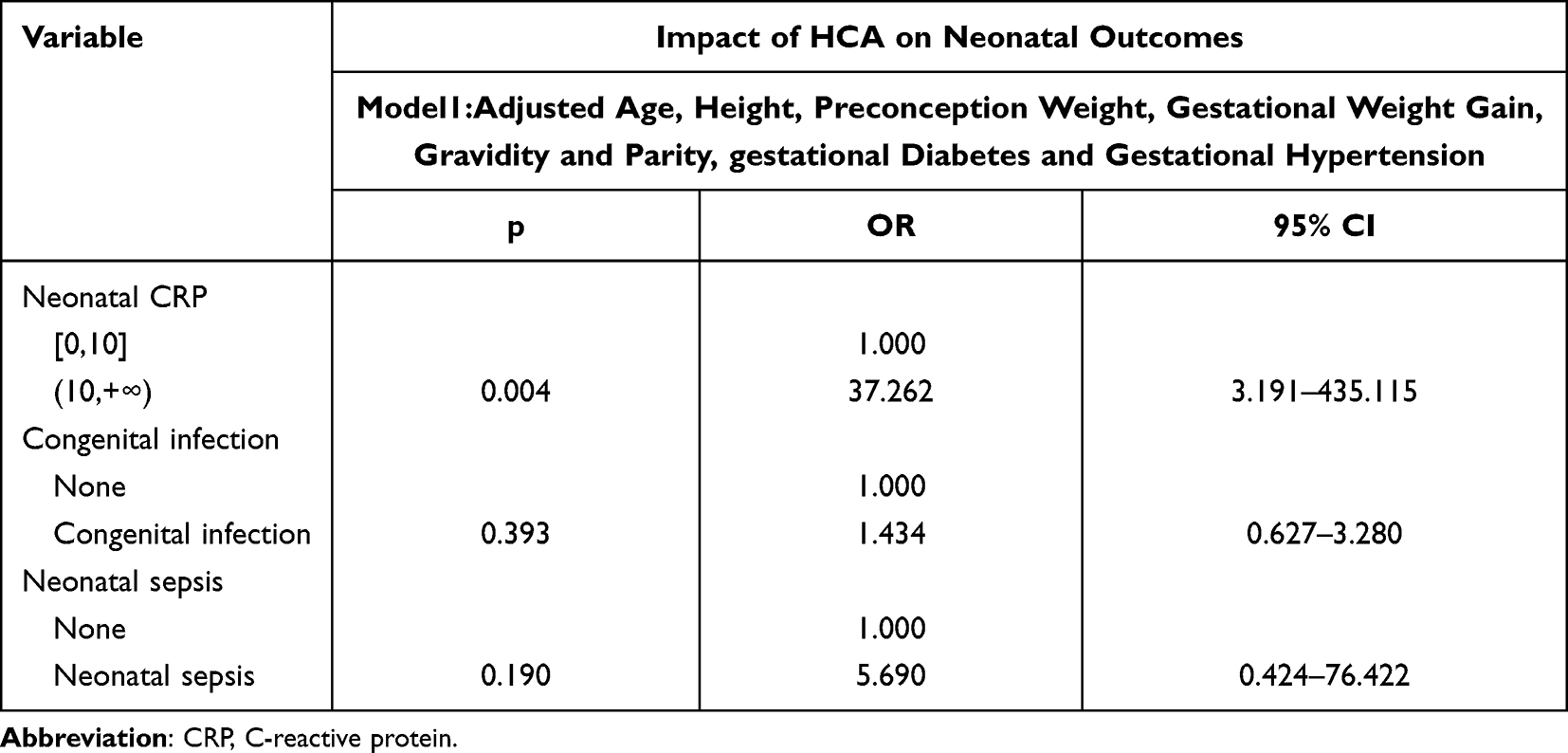 |
Table 5 The Association of HCA with Neonatal Outcomes When Analyzed by Multiple Regression Analysis |
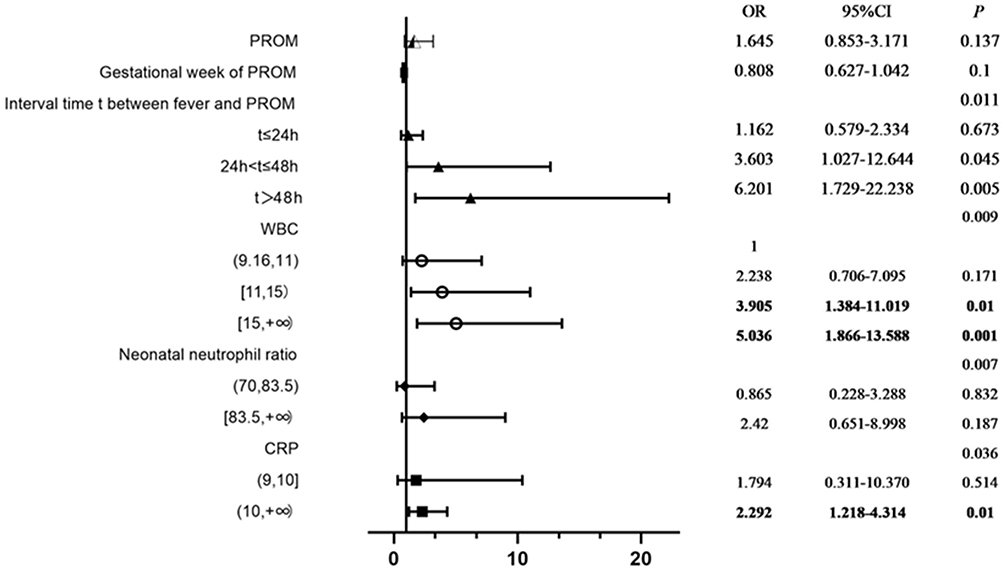 |
Figure 3 Forest plot of multiple logistic regression analysis of HCA with odds ratios and 95% confidence intervals. Abbreviations: HCA, histologic chorioamnionitis; PROM, premature rupture of membranes; WBC, white blood cell; CRP, C-reactive protein. Notes: Bold text indicates statistically significant associations (p<0.05). Error bars represent 95% confidence intervals. |
According to multiple regression models, HCA remained a significant risk factor for increased neonatal CRP levels (aOR: 37.262; 95% CI: 3.191~435.115; Table 5), whereas maternal administration of antibiotics for CAM provided little protection against congenital infection and neonatal sepsis according to the multivariate logistic regression model (aOR: 1.800; 95% CI: 1.258~2.575; aOR: 11.984; 95% CI: 2.353~61.026; Table 6).
 |
Table 6 The Association of Antibiotics with Neonatal Outcomes When Analyzed by Multiple Regression Analysis |
Discussion
Principal Findings
In our study of preterm births with confirmed HCA, we found that congenital infection, neonatal sepsis, PPROM, vaginal bacterial colonization, maternal leukocytosis and high levels of CRP were associated with HCA. Our results also indicated that the interval between PPROM and fever plays an important role in HCA.
Results
In regard to women diagnosed with prenatal fever, it is always difficult and controversial for obstetricians to decide the timing of induction, especially when the gestational age is less than 34 weeks. Our study aimed to determine the optimal timing so that we could maximize benefits and minimize complications for mothers and neonates. Previous studies have shown that PPROM is significantly associated with the incidence of HCA and is considered a clinical predictor.17–19 In our study, multiple logistic regression revealed a predominance of HCA-associated lesions in the interval between PPROM and fever >24 h and a WBC >11*10^9/L and a CRP >10. Other clinical parameters, such as age, parity, BMI and body temperature, did not significantly differ. It is well known that histological examination is always the gold standard for HCA diagnosis. With the prolongation of PPROM, especially in those with a duration of more than 24 h, the probability of early-onset sepsis can increase by 2–10 times.20 Although maternal fever is an important clinical sign, it is not a reliable marker for predicting intrauterine infection. In our study, the combination of the interval time between PPROM and fever, WBC and CRP could be used to predict the possibility of preterm HCA, so that obstetricians could implement timely interventions and minimize adverse complications for both the mother and the baby. The association between gestational hypertension and HCA disappeared after we controlled for potential confounding factors through multivariate logistic regression analysis. These findings suggested that the association with HCA was most likely mediated by an increased risk of other complications of pregnancy.
A meta-analysis of 107 studies revealed that when infection/inflammation was the trigger of preterm birth, neonates were more susceptible to developing neonatal sepsis.21 In this study, preterm neonates from pregnancies with HCA had a higher risk of congenital infections and neonatal sepsis, which were strongly associated with increased neonatal CRP levels. These interesting findings are consistent with those of a retrospective study conducted in Dublin in 2020.22
Once a diagnosis of CCA has been established, delivery should be considered, regardless of the gestational age. Vaginal delivery is considered a safer option and cesarean section should be performed under strict obstetric indications. Previous studies have shown that compared with women without CCA, women with CCA were more likely to have a cesarean delivery, which might be due to decreasing contractility after the onset of fever leading to either abnormal labor progression or prolonged labor.23–25 Consistent with the findings of Xie et al 26, we found that the incidence of cesarean section did not significantly differ between the two groups. However, women who underwent cesarean section were more likely to have adverse maternal outcomes, including admission to the intensive care unit (ICU), wound infection and blood transfusion.1 Thus, cesarean section should be considered under proper obstetric indications to avoid unnecessary adverse outcomes.
In our study, maternal WBC and CRP could be used as potential predictive markers for HCA in pregnant women with fever. Cho et al established a predictive equation for HCA derived from the combination of the CRP level, lymphocyte count and delta neutrophil index, which is also a non-invasive method to detect HCA in pregnant women with PPROM.26 Other studies have used invasive methods based on amniocentesis, which might result in complications.27,28 Kurakazu et al used a combination of maternal WBC and CRP levels and amniotic fluid biomarkers to improve the accuracy of predicting HCA.29 Roberts et al30 demonstrated that CAM can occur without demonstrable intra-amniotic infection. CAM can still be neglected even if amniocentesis is performed, therefore it is not ideal for predicting HCA. Predictive markers should be as accurate and non-invasive as possible to make clinical management and treatment plans easier.
UU is a common inhabitant in the vaginas of pregnant women with almost 70% of women harboring these organisms.31 However, studies have shown that UU recovered from the vagina and amniotic fluid is not associated with preterm birth, although its presence in the chorioamnion is strongly associated with HCA.31,32 Owing to its ability to vertically transmit and adhere to epithelial cells, the possibility of colonization in the respiratory tract increases as the duration of ruptured amniotic membranes is prolonged.33 However, whether medication therapy for UU can reduce the incidence of preterm birth and HCA remains controversial.34–36 One study indicated that solithromycin may be effective in treating UU-associated preterm delivery and for asymptomatic women with a high risk of preterm birth.34 Further prospective studies need to focus on the effectiveness of antibiotics on reducing HCA to determine the best management for UU infection.
Clinical and Research Implications
In this study population, compared with women without PPROM, women with PPROM were at an increased risk of HCA, highlighting the critical importance of vigilant monitoring of body temperature, blood test parameters, and amniotic fluid characteristics in this high-risk group. Here, we demonstrate that maternal WBC and CRP levels serve as valuable predictive biomarkers for HCA in pregnant women with fever, particularly when complicated by UU infection.
These findings have several important clinical implications for routine obstetric practice. First, our findings support the implementation of a standardized risk assessment protocol that incorporates WBC and CRP measurements for all pregnant women who present with PPROM and/or fever. This could enable early identification of women requiring intensive monitoring and prompt intervention. In addition, the predictive value of combined WBC and CRP levels, especially in UU-positive patients, suggests the need to develop evidence-based clinical algorithms that guide antibiotic prophylaxis timing and delivery planning. Clinicians should consider lower thresholds for intervention when the levels of both biomarkers are elevated. Additionally, given the time-sensitive nature of HCA management, implementing rapid point-of-care testing for inflammatory markers in labor and delivery units could facilitate real-time clinical decision-making and potentially improve maternal–neonatal outcomes. Future efforts for health care givers should focus on identifying women at the greatest risk of HCA in the early stage of pregnancy.
Strengths and Limitations
This study has several strengths. First, the data were derived from a tertiary hospital where all the placental pathology of the neonates was available. From a clinical perspective, this study was able to identify several risk factors, including the duration of PPROM, for obstetricians to identify preterm birth complicated with HCA at an early stage to improve both maternal and neonatal outcomes. We also found a cutoff value for WBCs that indicated HCA for the first time.
The limitations of our study included the single-center site and only women with fever were included. Further prospective studies with larger samples are needed to elucidate the predictive factors of HCA in asymptomatic pregnant women and to provide stronger evidence for eventual improvement.
Conclusions
In this retrospective study of singleton pregnancies, the duration of preterm premature rupture should be closely monitored. For pregnant women with PPROM comorbidity with fever whose rupture duration exceeded 24 h or whose maternal WBC count reached 11*10^9/L, obstetric interventions should be actively carried out to avoid adverse outcomes. It is envisaged that the identification of pregnant women at risk of infection-associated preterm birth would greatly improve both maternal and neonatal outcomes.
Abbreviations
ACOG, American College of Obstetricians and Gynecologists; BMI, body mass index; CAM, chorioamnionitis; CCA, clinical chorioamnionitis; CI, confidence intervals; CRP, C-reactive protein; GBS, group B streptococcus; HCA, histologic chorioamnionitis; ICU, intensive care unit; OR, odds ratios; PROM, premature rupture of membranes; PPROM, preterm premature rupture of membranes; ROC, Receiver operating characteristic; NICU, neonatal intensive care unit; UU: Ureaplasma urealyticum.
Data Sharing Statement
Data is provided within the main text and the supplementary information.
Ethics Approval and Consent for Publication
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Review Board of the International Peace Maternity and Child Health Hospital Affiliated to the Shanghai Jiao Tong University School of Medicine (GKLW 2019-19). All participants provided written informed consent before enrollment.
Acknowledgments
Nan Lin and Yiru Shi are co-first authors for this study. We thank all the staff who helped with the recording of this data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the National Key Research and Development Program of China (2018YFC1004600).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Perry AK, Rossi RM, DeFranco EA. Severe adverse maternal outcomes associated with chorioamnionitis. Am J Obstet Gynecol MFM. 2019;1(3):100027. doi:10.1016/j.ajogmf.2019.06.006
2. Carter SWD, Neubronner S, Su LL, et al. Chorioamnionitis: an update on diagnostic evaluation. Biomedicines. 2023;11(11):2922. doi:10.3390/biomedicines11112922
3. American College of Obstetricians and Gynecologists. Prelabor rupture of membranes: ACOG practice bulletin, number 217. Obstet Gynecol. 2020;135(3):e80–e97.
4. Han X, Du H, Cao Y, et al. Association of histological and clinical chorioamnionitis with perinatal and neonatal outcome. J Matern Fetal Neonatal Med. 2021;34(5):794–802. doi:10.1080/14767058.2019.1618824
5. Jain VG, Willis KA, Jobe A, Ambalavanan N. Chorioamnionitis and neonatal outcomes. Pediatr Res. 2022;91(2):289–296. doi:10.1038/s41390-021-01633-0
6. Gupta JK, Alfirevic A. Systematic review of preterm birth multi-omic biomarker studies. Expert Rev Mol Med. 2022;24:1–24. doi:10.1017/erm.2022.13
7. Villamor-Martinez E, Álvarez-Fuente M, Ghazi AMT, et al. Association of chorioamnionitis with bronchopulmonary dysplasia among preterm infants: a systematic review, meta-analysis, and metaregression. JAMA Network Open. 2019;2(11):e1914611. doi:10.1001/jamanetworkopen.2019.14611
8. Bierstone D, Wagenaar N, Gano DL, et al. Association of histologic chorioamnionitis with perinatal brain injury and early childhood neurodevelopmental outcomes among preterm neonates. JAMA Pediatr. 2018;172(6):534–541. doi:10.1001/jamapediatrics.2018.0102
9. Woodd SL, Montoya A, Barreix M, et al. Incidence of maternal peripartum infection: a systematic review and meta-analysis. PLoS Med. 2019;16(12):e1002984. doi:10.1371/journal.pmed.1002984
10. Liu PC, Hung YL, Shen CM, Chen PC, Hsieh WS. Histological chorioamnionitis and its impact on respiratory outcome in very-low-birth-weight preterm neonates. Pediatr Neonatol. 2021;62(3):258–264. doi:10.1016/j.pedneo.2020.11.009
11. Committee Opinion No. 712: intrapartum management of intraamniotic infection. Obstet Gynecol. 2017;130(2):e95–e101. doi:10.1097/AOG.0000000000002236
12. Matulova J, Kacerovsky M, Hornychova H, et al. Acute histological chorioamnionitis and birth weight in pregnancies with preterm prelabor rupture of membranes: a retrospective cohort study. Front Pharmacol. 2022;13:861785. doi:10.3389/fphar.2022.861785
13. Budal EB, Bentsen MHL, Kessler J, et al. Histologic chorioamnionitis in extremely preterm births, microbiological findings and infant outcome. J Matern Fetal Neonatal Med. 2023;36(1):2196599. doi:10.1080/14767058.2023.2196599
14. D’Antonio F, Eltaweel N, Prasad S, et al. Cervical cerclage for prevention of preterm birth and adverse perinatal outcome in twin pregnancies with short cervical length or cervical dilatation: a systematic review and meta-analysis. PLoS Med. 2023;20(8):e1004266. doi:10.1371/journal.pmed.1004266
15. Bethou A, Bhat BV. Neonatal Sepsis-Newer Insights. Indian J Pediatr. 2022;89(3):267–273. doi:10.1007/s12098-021-03852-z
16. Matsuguma C, Takahashi K, Okada S, et al. Clinical utility of gastric fluid cytokine levels in preterm infants for predicting histological chorioamnionitis. Cytokine. 2024;180:156642. doi:10.1016/j.cyto.2024.156642
17. Popowski T, Goffinet F, Maillard F, Schmitz T, Leroy S, Kayem G. Maternal markers for detecting early-onset neonatal infection and chorioamnionitis in cases of premature rupture of membranes at or after 34 weeks of gestation: a two-center prospective study. BMC Pregnancy Childbirth. 2011;11(1):26. doi:10.1186/1471-2393-11-26
18. Torricelli M, Voltolini C, Conti N, et al. Histologic chorioamnionitis at term: implications for the progress of labor and neonatal wellbeing. J Matern Fetal Neonatal Med. 2013;26(2):188–192. doi:10.3109/14767058.2012.722724
19. Lee KN, Cho I, Im EM, Oh E, Park KH. Plasma IGFBP-1, Fas, kallistatin, and P-selectin as predictive biomarkers of histologic chorioamnionitis and associated intra-amniotic infection in women with preterm labor. Am J Reprod Immunol. 2023;89(1):e13645. doi:10.1111/aji.13645
20. MS E. Postnatal Bacterial Infections. Martin RJ, Walsh MC, editor. Philadelphia: Mosby Elsevier; 2006:791–804.
21. Villamor-Martinez E, Lubach GA, Rahim OM, et al. Association of histological and clinical chorioamnionitis with neonatal sepsis among preterm neonates: a systematic review, meta-analysis, and meta-regression. Front Immunol. 2020;11:972. doi:10.3389/fimmu.2020.00972
22. Ryan E, Eves D, Menon PJ, et al. Histological chorioamnionitis is predicted by early infant C-reactive protein in preterm neonates and correlates with neonatal outcomes. Acta Paediatr. 2020;109(4):720–727. doi:10.1111/apa.15038
23. Conde-Agudelo A, Romero R, Jung EJ, Garcia Sánchez ÁJ. Management of clinical chorioamnionitis: an evidence-based approach. Am J Obstet Gynecol. 2020;223(6):848–869. doi:10.1016/j.ajog.2020.09.044
24. Zackler A, Flood P, Dajao R, Maramara L, Goetzl L. Suspected chorioamnionitis and myometrial contractility: mechanisms for increased risk of cesarean delivery and postpartum hemorrhage. Reprod Sci. 2019;26(2):178–183. doi:10.1177/1933719118778819
25. Bommarito KM, Gross GA, Willers DM, Fraser VJ, Olsen MA. The effect of clinical chorioamnionitis on cesarean delivery in the United States. Health Serv Res. 2016;51(5):1879–1895. doi:10.1111/1475-6773.12447
26. Cho HY, Jung I, Kwon JY, Kim SJ, Park YW, Kim YH. The delta neutrophil index as a predictive marker of histological chorioamnionitis in patients with preterm premature rupture of membranes: a retrospective study. PLoS One. 2017;12(3):e0173382. doi:10.1371/journal.pone.0173382
27. Ronzoni S, Cobo T, D’Souza R, et al. Individualized treatment of preterm premature rupture of membranes to prolong the latency period, reduce the rate of preterm birth, and improve neonatal outcomes. Am J Obstet Gynecol. 2022;227(2):296.e1–e18. doi:10.1016/j.ajog.2022.02.037
28. Park JW, Park KH, Jung EY. Clinical significance of histologic chorioamnionitis with a negative amniotic fluid culture in patients with preterm labor and premature membrane rupture. PLoS One. 2017;12(3):e0173312. doi:10.1371/journal.pone.0173312
29. Kurakazu M, Yotsumoto F, Arima H, et al. The combination of maternal blood and amniotic fluid biomarkers improves the predictive accuracy of histologic chorioamnionitis. Placenta. 2019;80:4–7. doi:10.1016/j.placenta.2019.03.007
30. Roberts DJ, Celi AC, Riley LE, et al. Acute histologic chorioamnionitis at term: nearly always noninfectious. PLoS One. 2012;7(3):e31819. doi:10.1371/journal.pone.0031819
31. Eschenbach DA. Ureaplasma urealyticum and premature birth. Clin Infect Dis. 1993;17(Suppl 1):S100–6.
32. Sweeney EL, Kallapur SG, Gisslen T, et al. Placental infection with ureaplasma species is associated with histologic chorioamnionitis and adverse outcomes in moderately preterm and late-preterm neonates. J Infect Dis. 2016;213(8):1340–1347.
33. Sprong KE, Mabenge M, Wright CA, Govender S. Ureaplasma species and preterm birth: current perspectives. Crit Rev Microbiol. 2020;46(2):169–181.
34. Bookstaver PB; as part of the Southeastern Research Group Endeavor (SERGE‐45) research network, Nguyen J, Madonia V, Bland CM, et al. A review of antibiotic safety in pregnancy-2025 update. Pharmacotherapy. 2025;45(4):227–237.
35. Berg TG, Philpot KL, Welsh MS, Sanger WG, Smith CV. Ureaplasma/mycoplasma-infected amniotic fluid: pregnancy outcome in treated and nontreated patients. J Perinatol. 1999;19(4):275–277. doi:10.1038/sj.jp.7200185
36. Gomez R, Romero R, Nien JK, et al. Antibiotic administration to patients with preterm premature rupture of membranes does not eradicate intra-amniotic infection. J Matern Fetal Neonatal Med. 2007;20(2):167–173. doi:10.1080/14767050601135485
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.