Back to Journals » International Journal of General Medicine » Volume 14
Risk Factors for Epilepsy: A National Cross-Sectional Study from National Health and Nutrition Examination Survey 2013 to 2018
Authors Yang L, Wang Y, Chen X, Zhang C, Chen J, Cheng H, Zhang L
Received 3 June 2021
Accepted for publication 29 July 2021
Published 11 August 2021 Volume 2021:14 Pages 4405—4411
DOI https://doi.org/10.2147/IJGM.S323209
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Lixiang Yang,1,* Yue Wang,2,* Xun Chen,3,* Can Zhang,4 Junhui Chen,2 Huilin Cheng,1 Lihua Zhang5
1Department of Neurosurgery, Zhongda Hospital, School of Medicine, Southeast University, Nanjing, 210009, People’s Republic of China; 2Department of Neurosurgery, 904th Hospital of Joint Logistic Support Force of PLA, Wuxi Clinical College of Anhui Medical University, Wuxi, People’s Republic of China; 3Department of cognitive neurolinguistics, School of Foregin Language, East China University of Science and Techonology, Shanghai, 200237, People’s Republic of China; 4Department of Neurosurgery, The Second People’s Hospital of HeFei, Hefei, People’s Republic of China; 5Department of Pathology, School of Medicine, Zhongda Hospital, Southeast University, Nanjing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Huilin Cheng
Department of Neurosurgery, Zhongda Hospital, School of Medicine, Southeast University, Nanjing, 210009, Jiangsu, People’s Republic of China
Email [email protected]
Lihua Zhang
Department of Pathology, School of Medicine, Zhongda Hospital, Southeast University, Nanjing, People’s Republic of China
Email [email protected]
Objective: The purpose of this study is to investigate the risk factors of epilepsy based on the National Health and Nutrition Examination Survey (NHANES).
Methods: The data in this study was obtained from the NHANES database between 2013 and 2018. It included 14,290 participants aged between 20 and 80. We defined people with epilepsy (PWE) when they self-reported took at least one treatment medication for seizures or epilepsy. Analysis of risk factors for epilepsy mainly includes Student’s t-test, chi-square test, univariate and multivariate logistic regression analysis.
Results: People aged 40– 59 shared 1.8 times the risk of epilepsy than those who aged 20– 39, P=0.034. People who never married had a 2.8-fold higher risk of epilepsy than those who married/living with partner, P< 0.001. The risk of epilepsy in subjects with very good/good general health was 0.4 times than that of subjects with fair/poor general health, P< 0.001. Moreover, subjects without sleep disorders had a 0.4-fold higher risk of epilepsy than those who had sleep disorders, P=0.042.
Conclusion: People who are older, unmarried, and have sleep disorders are at higher risk of epilepsy. In addition, good/good general health condition is associated with a lower risk of epilepsy.
Keywords: epilepsy, risk factors, epidemiology, NHANES database
Introduction
Epilepsy is a common neurological disease caused by a group of different causes. It can occur in patients of any age, region, and race.1 The main clinical manifestations are recurrent muscle twitches, short-term abnormalities in sensation, consciousness, and others. In severe cases, it may develop symptom of loss of consciousness, general tonic clonus etc. At present, many research reports show that the annual incidence rate of epilepsy is 20–70 per 100,000 people, and the point prevalence of active epilepsy was 6.38 per 1000 population (95% CI: 5.57–7.30).2 It has been estimated that at least 50 million people worldwide had been affected. It has become a common neurological disease second only to stroke. The World Health Organization has listed epilepsy as one of the main neuropsychiatric diseases that require prevention and treatment.3
Epilepsy can easily cause damage to the patient’s mental and physical health, adding a heavy burden to the family and society. Although most PWE can effectively control seizures after regular medical treatment, patients would still feel shame, impaired dignity, and often worry about the recurrence of epilepsy. According to different diagnostic criteria and scales, the incidence of anxiety and depression in PWE varies from 20% to 50%.4 More seriously, the total death rate due to suicide was 0.5% (95% CI: 0.002–0.016).5 Therefore, epilepsy is not only harmful to the health of patients, but can cause a series of social problems as well. Early recognition and prevention of epilepsy is of great importance.
However, there is currently a lack of cross-sectional studies on risk factors of epilepsy with a large enough sample size. To explore more risk factors of epilepsy besides stroke, traumatic brain injury, brain tumor and other universally accepted epileptic factors, the participants’ age, blood pressure, smoking history, sleep disorder, etc were selected as risk factors based on the NHANES database. Then, statistical analysis and testing of the above-mentioned related risk factors are carried out. This study will provide a reference for the prevention and treatment of epilepsy.
Methods
Data Source
This study conducted a retrospective cross-sectional analysis using data from NHANES 2013–2018. NHANES is a complex, multistage, large-scale civilian survey jointly conducted by the Centers for Disease Control and Prevention (CDC) and the National Center for Health Statistics. The survey content includes health status, population nutrition, lifestyle factors, physical examination, etc. Detailed descriptions of the NHANES protocol have been published elsewhere.6 In short, NHANES is a survey that uses a stratified, multistage probability sampling design to draw representative samples from American civilians to assess the nutritional status and physical conditions of American children and adults.
Definition of Diseases
In NHANES Questionnaire data, participants listed the names and main reasons for prescription medications they had taken in the past 30 days. After confirming that the prescription medication was a standard antiseizure medication, we defined the participants who answered at least one medication for “epilepsy and recurrent seizures” (G40) as PWE.7
Based on previous studies, we assessed some covariates in association analysis, including gender, age, race, marital status, hypertension, smoking status, diabetes, general health, depression, sleep duration, and sleep disorders. The race was classified as Mexican American, other Hispanic, non-Hispanic white, non-Hispanic black, and others. Marital status was classified as married/living with a partner, widow/divorced/separated, and never married. Hypertension was defined as the current use of antihypertensive medication, or self-reported history of hypertension, or uncontrolled blood pressure greater than 140/90mmHg at the time of physical examination. We classified smoking status as never smoking (less than 100 cigarettes in a lifetime) and current or ever smoking (more than 100 cigarettes in a lifetime) according to the National Center for Health Statistics definitions.8 General health condition was classified as excellent, very good/good, and fair/poor. The depression score was calculated according to the Patient Health Questionnaire (PHQ-9), which total score ranged from 0 to 27. The severity of depression was classified as “none or minimum” (0–4), “mild” (5–9), “moderate” (10–14), and “moderately severe or severe” (15–27).9 Sleep time was determined according to the participants’ answers to the question “ Number of hours usually sleep on weekdays or workdays?” and was classified as short sleep duration (<7 hours), optimal sleep duration (7 to 9 hours), and long sleep duration (>9 hours). Whether participants have sleep disorders was judged by their answers to the specific question “Ever told doctor had sleep disorders?”. In this study, a total of 29,400 subjects was extracted from the 2013–2018 NHANES database. After selecting subjects aged 20–80 and excluding all subjects with incomplete covariate data, we included a total of 14,290 subjects for analysis.
Ethics Statement
The National Center for Health Statistics Research Ethics Review Board approved the NHANES study and all those who participated in the survey signed an informed consent form. The NHANES database was open to the public and did not require any ethical or administrative permission. More details are available on the web (www.cdc.gov/nchs/nhanes/).
Statistical Analysis
We extracted 2013–2018 NHANES data with R studio (version 3.5.3), analyzed all data by SPSS software (version 19.0), and designed figures by GraphPad prism (version 7.0). The continuous variables in the basic characteristics were analyzed by Student’s t-test, while categorical variables were analyzed by Chi-square test or Fisher’s test and presented as frequency (%). Univariate and multivariate logistic regression analyses were used to analyze some possible risk factors for epilepsy. P<0.05 was considered statistically significant.
Results
Baseline Characteristics of the Study Population
The baseline characteristics of the participants were shown in Table 1. 14,290 cases with complete data were included in our study, including 6927 (48.5%) males and 7363 (51.5%) females. 120 PWE and 14,170 non-epilepsy controls were identified. Compared with controls, PWE were older (54.30 vs 49.66, P<0.01), and most of the subjects were aged 60 and 80 (42.5%; n=51), followed by 40–59 years old (37.5%; n=45). As shown in Figure 1, when the age groups were divided in more detail, the age of PWE was mainly between 41–65 years old. In addition, they rarely had been married or had partners (42.5% vs 60.0%, P<0.01), more people had hypertension (60.8% vs 41.9%, P<0.01), diabetes (24.2% vs 14.0%, P<0.01), smoking history (52.5% vs 42.9%, P<0.05), depression (10.8% vs 3.2%, P<0.01), less optimal sleep duration (53.3% vs 62.6%, P<0.05), poor general health (50.8% vs 24.1%, P<0.01), and sleep disorders (47.5% vs 27.4%, P<0.01). The different degree of general health condition of epilepsy and control subjects were shown in Figure 2. In terms of excellent, very good, and good general health, the ratio of PWE was lower than that of the control, while in the general health of fair and poor, the result was the opposite. Besides, Figure 3 also showed that sleep disorders were more common in PWE in different years compared with controls.
 |
Table 1 Basic Characteristics of the Included Study |
 |
Figure 1 Age distribution of subjects in the NHANES survey. The age of PWE was mainly between 41–65 years old. |
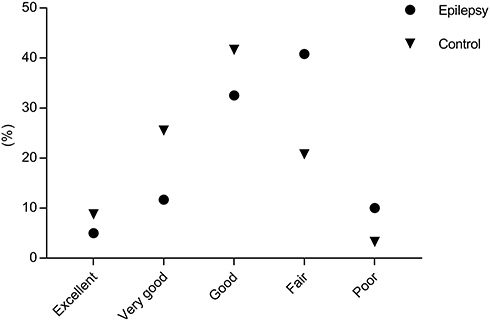 |
Figure 2 General health distribution of subjects in the NHANES survey. In terms of excellent, very good, and good general health, the ratio of PWE was lower than that of the control, while in the general health of fair and poor, the result was the opposite. |
 |
Figure 3 The sleep disorder of subjects in 2013–2014, 2015–2016, and 2017–2018. Sleep disorders were more common in PWE in different years compared with controls. |
Univariate and Multivariate Logistic Regression Analysis of Epilepsy Risk Factors
In univariate analyses, older age (40–59, OR=1.9, P=0.012; 60–80, OR=2.1, P=0.003), widow/divorced/separated (OR=2.0, P=0.002) and never married (OR=2.1, P=0.001), moderate (OR=2.6, P=0.002) and moderately severe or severe (OR=4.4, P<0.001) depression were risk factors for epilepsy. Subjects with excellent (OR=0.3, P=0.002) and very good/good (OR=0.3, P<0.001) general health, no hypertension (OR=0.5, P<0.001), no smoking (OR=0.7, P=0.036), no diabetes (OR=0.5, P=0.001), and no sleep disorders (OR=0.4, P<0.001) were protective factors for epilepsy. To further determine the risk factors of epilepsy, we conducted multivariate logistic regression analysis. As shown in Table 2, the risk of epilepsy in people aged 40–59 was 1.8 times higher than that in people aged 20–39, P=0.034. Never married subjects had a 2.8-fold higher risk of epilepsy than married/living with partner subjects, P<0.001. The risk of epilepsy was 0.4 times higher in subjects with very good/good general health than in subjects with fair/poor general health, P<0.001. Moreover, subjects without sleep disorders had a 0.4-fold higher risk of epilepsy than those with sleep disorders, P=0.042.
 |
Table 2 Logistic Regression Analysis of Epilepsy Risk Factors |
Discussion
Epilepsy has the characteristics of long duration, recurrent seizures, long-term medication, and severe cases that need surgical treatment, which will seriously damage the quality of life of patients. In this study, we conducted a large cross-sectional study to explore the risk factors of epilepsy using NHANES data. A total of 14,290 subjects aged 20–80 were enrolled in the analysis, including 120 PWE. Results showed that subjects who were older and never married had a higher risk of epilepsy, while individuals with very good/good general health and no sleep disorders had a lower risk of epilepsy.
As previously reported, the incidence and prevalence of epilepsy are generally age-related with a bimodal distribution, and the risk is highest in older age and infant groups.10 Our research also found that older people were at greater risk of epilepsy. However, the age of PWE in this study was all ≥ 20 years old, so it could not reflect the prevalence of infants and children. Besides, due to the limitations of the included cases and uneven age distribution, there may be bias in selection.
Although some studies focused on the mental health and marital status of PWE, there is still a lack of cross-sectional surveys with large samples. In this study, our results showed that never married was a high-risk factor for epilepsy, while having very good/good general health was a protective factor for epilepsy. According to previous research, never married was a high-risk factor for epilepsy and the possible reasons were as follows. For PWE, the embarrassment of epileptic seizures in public may lead to self-doubt, being denied by others, and questioning the meaning of one’s own survival.11 In a study investigating the impact of epilepsy on life, Baker stated that 36% of subjects sometimes kept their epilepsy as a secret from others due to fear of discrimination, while 47% of the subjects even thought that people should not know.12 Compared with the general population, these patients are less likely to get married and more likely to divorce.13 In addition, compared with the healthy control group, PWE received less emotional and instrumental support from the family, which would undoubtedly increase their risk of fair/poor general health.14 Therefore, although this is a cross-sectional study, it can only suggest risk factors for the disease, but cannot disentangle reverse causation. However, our results still suggested that more attention should be paid to the mental health and marital quality of PWE.
Sleep plays a vital role in human physical activity and consciousness, but sleep disorders have become a serious health problem in the world. There are many forms of sleep disorders in PWE, and the complex relationship between sleep disorders and epilepsy has been widely concerned. On the one hand, PWE have longer rapid eye movement (REM) sleep latency and less REM sleep, but more non-REM sleep, leading to disturbances in the sleep-wake cycle and lower sleep efficiency.15 On the other hand, sleep disorders can also affect seizures. For example, sleep deprivation may aggravate seizures, while difficulty in falling asleep and maintaining sleep, and obstructive sleep apnea syndrome can affect the control of epileptic seizures. Besides, some seizures mainly occur while sleeping.16 Ismayilova studied 212 PWE and showed that the sleep structure of the patients was disordered and the sleep quality was worse than that of the normal control group.17 De Weerd conducted a study on 486 patients with partial seizures and showed that the incidence of sleep disorders in PWE was twice as high as that of controls.18 Consistent with previous research, our research showed that no sleep disorder was a protective factor for epilepsy. This suggests that we should pay more attention to the sleep disorders of PWE, and if necessary, carry out drug or other interventions to improve the quality of sleep, thereby improving the outcome of epilepsy.
However, our study also has some limitations. First, the criteria for inclusion of epilepsy rely on self-reported medication history, lack of information on the methods of diagnosing epilepsy and the type of epilepsy, and no doctors or other health professionals to confirm. Second, it is the subjects or proxies who answered the questionnaire, and some people may conceal the history of epilepsy due to stigma. For some elderly people, they may receive less attention at normal times and may not go to the doctor in time when they have symptoms of epilepsy. Third, although the sample size of this study is large enough, the number of PWE is much smaller than that of the control group, which may affect the power of the analysis.
Conclusion
In summary, we conducted a nationwide, cross-sectional study using NHANES data to explore risk factors for epilepsy, and the results showed that older age and never married were high-risk factors for epilepsy, while very good/good general health and no sleep disorder were protective factors. We believe that these results have important public health significance and provide a basis for policymakers and doctors to formulate evidence-based medical interventions to improve the quality of life of PWE.
Abbreviations
NHANES, National Health and Nutrition Examination Survey; PWE, People with epilepsy; CDC, Centers for Disease Control and Prevention; PHQ-9, Patient Health Questionnaire; REM, Rapid eye movement.
Funding
This work was supported by grants from National Natural Science Foundation of China (No. 82071393).
Disclosure
The authors declare that they have no conflict of interest in connection with this work.
References
1. Bonansco C, Fuenzalida M. Plasticity of hippocampal excitatory-inhibitory balance: missing the synaptic control in the epileptic brain. Neural Plast. 2016;2016:8607038. doi:10.1155/2016/8607038
2. Fiest KM, Sauro KM, Wiebe S, et al. Prevalence and incidence of epilepsy: a systematic review and meta-analysis of international studies. Neurology. 2017;88(3):296–303. doi:10.1212/WNL.0000000000003509
3. Ibrahim A, Umar UI, Usman UM, Owolabi LF. Economic evaluation of childhood epilepsy in a resource-challenged setting: a preliminary survey. Epilepsy Behav. 2017;76:84–88. doi:10.1016/j.yebeh.2017.08.023
4. Kanner AM. Management of psychiatric and neurological comorbidities in epilepsy. Nat Rev Neurol. 2016;12(2):106–116. doi:10.1038/nrneurol.2015.243
5. Mesraoua B, Deleu D, Hassan AH, et al. Dramatic outcomes in epilepsy: depression, suicide, injuries, and mortality. Curr Med Res Opin. 2020;36(9):1473–1480. doi:10.1080/03007995.2020.1776234
6. Santos D, Dhamoon MS. Trends in antihypertensive medication use among individuals with a history of stroke and hypertension, 2005 to 2016. JAMA Neurol. 2020;77(11):1382. doi:10.1001/jamaneurol.2020.2499
7. Terman SW, Hill CE, Burke JF. Disability in people with epilepsy: a nationally representative Cross-Sectional Study. Epilepsy Behav. 2020;112:107429. doi:10.1016/j.yebeh.2020.107429
8. Semenov YR, Herbosa CM, Rogers AT, et al. Psoriasis and mortality in the US: data from the national health and nutrition examination survey. J Am Acad Dermatol. 2019;85(2):396–403. doi:10.1016/j.jaad.2019.08.011
9. Wang Y, Lopez JM, Bolge SC, Zhu VJ, Stang PE. Depression among people with type 2 diabetes mellitus, US National Health and Nutrition Examination Survey (NHANES), 2005–2012. BMC Psychiatry. 2016;16(1):88. doi:10.1186/s12888-016-0800-2
10. Thijs RD, Surges R, O’Brien TJ, Sander JW. Epilepsy in adults. Lancet. 2019;393(10172):689–701. doi:10.1016/S0140-6736(18)32596-0
11. Goodall J, Salem S, Walker RW, et al. Stigma and functional disability in relation to marriage and employment in young people with epilepsy in rural Tanzania. Seizure. 2018;54:27–32. doi:10.1016/j.seizure.2017.11.016
12. Baker GA, Hargis E, Hsih MM, et al. Perceived impact of epilepsy in teenagers and young adults: an international survey. Epilepsy Behav. 2008;12(3):395–401. doi:10.1016/j.yebeh.2007.11.001
13. Ak PD, Atakli D, Yuksel B, Guveli BT, Sari H. Stigmatization and social impacts of epilepsy in Turkey. Epilepsy Behav. 2015;50:50–54. doi:10.1016/j.yebeh.2015.05.014
14. Wang YH, Haslam M, Yu M, Ding J, Lu Q, Pan F. Family functioning, marital quality and social support in Chinese patients with epilepsy. Health Qual Life Outcomes. 2015;13(1):10. doi:10.1186/s12955-015-0208-6
15. Staniszewska A, Maka A, Religioni U, Olejniczak D. Sleep disturbances among patients with epilepsy. Neuropsychiatr Dis Treat. 2017;13:1797–1803. doi:10.2147/NDT.S136868
16. Ong LC, Yang WW, Wong SW, AlSiddiq F, Khu YS. Sleep habits and disturbances in Malaysian children with epilepsy. J Paediatr Child Health. 2010;46(3):80–84. doi:10.1111/j.1440-1754.2009.01642.x
17. Ismayilova V, Demir AU, Tezer FI. Subjective sleep disturbance in epilepsy patients at an outpatient clinic: a Questionnaire-Based Study on prevalence. Epilepsy Res. 2015;115:119–125. doi:10.1016/j.eplepsyres.2015.06.009
18. de Weerd A, de Haas S, Otte A, et al. Subjective sleep disturbance in patients with partial epilepsy: a Questionnaire-Based Study on prevalence and impact on quality of life. Epilepsia. 2004;45(11):1397–1404. doi:10.1111/j.0013-9580.2004.46703.x
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.