Back to Journals » Clinical Ophthalmology » Volume 17
Risk Factors for Descemet Membrane Endothelial Keratoplasty Rejection: Current Perspectives- Systematic Review
Authors Gurnani B ![]() , Kaur K, Lalgudi VG
, Kaur K, Lalgudi VG ![]() , Tripathy K
, Tripathy K ![]()
Received 30 November 2022
Accepted for publication 27 January 2023
Published 1 February 2023 Volume 2023:17 Pages 421—440
DOI https://doi.org/10.2147/OPTH.S398418
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Bharat Gurnani,1 Kirandeep Kaur,2 Vaitheeswaran Ganesan Lalgudi,3 Koushik Tripathy4
1Department of Cornea and Refractive Surgery, Sadguru Netra Chikitsalaya, Shri Sadguru Seva Sangh Trust, Janaki-kund, Madhya Pradesh, India; 2Department of Pediatric Ophthalmology, Sadguru Netra Chikitsalaya, Shri Sadguru Seva Sangh Trust, Janaki-kund, Madhya Pradesh, India; 3Department of Cornea, The Ottawa Hospital, University of Ottawa Eye Institute, Ontario, Canada; 4Department of Vitreoretinal and Cataract, ASG Eye Hospital, Kolkata, West Bengal, India
Correspondence: Bharat Gurnani, Consultant, Cataract, Cornea, External Diseases, Trauma, Ocular Surface, Uvea and Refractive Surgery, Sadguru Netra Chikitsalaya, Shri Sadguru Seva Sangh Trust, Janaki-kund, Madhya Pradesh, 485334, India, Tel +919080523059, Email [email protected]
Abstract: Descemet membrane endothelial keratoplasty (DMEK) is a corneal endothelial transplantation procedure with selective removal of a patient’s defective Descemet membrane and endothelium. It is replaced with a healthy donor Descemet membrane and endothelium without a stromal component. Corneal graft rejection can be at the level of epithelium, stroma as well endothelium. DMEK graft rejection is relatively less common than rejection with DSAEK or penetrating keratoplasty, and a good outcome may be achieved with prompt management. The clinical picture of DMEK rejection is usually similar to endothelial rejection in Descemet Stripping Endothelial Keratoplasty (DSEK/DSAEK), which generally manifests as pain, redness, reduction in visual acuity, stromal edema, endothelial rejection line, keratic precipitates at the back of the cornea and corneal neovascularization. However, more subtle forms of rejection or immune reactions are more common in DMEK compared to DSAEK eyes. Early clinical diagnosis, prompt intervention, and meticulous management safeguard visual acuity and graft survival in these cases. Intensive topical steroids form the mainstay in the management of DMEK rejection. Sometimes, oral or intravenous steroids or other systemic immunomodulators may be required. DMEK graft failure can be primary or secondary, and failure usually requires a second procedure in the form of repeat DMEK or DSEK or penetrating keratoplasty (PKP). A detailed literature search was performed using search engines such as Google Scholar, PubMed, and Google books, and a comprehensive review on DMEK rejection was found to be lacking. This review is a comprehensive update on the risk factors, pathophysiology, primary and secondary graft failure, recent advances in diagnosis, prevention of rejection, and updates in the management of DMEK rejection. The review also discusses the differential diagnosis of DMEK failure and rejection, prognosis, and future perspectives considering DMEK failure and rejection.
Keywords: descemet membrane endothelial keratoplasty, DMEK rejection, primary graft failure, secondary graft failure, rebubbling
Introduction
Corneal blindness is one of the leading cause of avoidable blindness worldwide.1 Corneal blindness can result from multiple pathologies such as corneal ulceration, corneal opacities, trauma, keratoconus, pseudophakic bullous keratopathy, aphakic bullous keratopathy, chemical injury, and graft failure.2 The problem statement is very high, as approximately 13 million people suffer from corneal blindness globally. Corneal transplantation is the gold standard for managing this blindness.3 The transplantation technique has evolved from full-thickness therapeutic and optical penetrating keratoplasty (TPK, OPK) to lamellar corneal transplantation such as Deep Anterior Lamellar Keratoplasty (DALK), Descemet Stripping Endothelial Keratoplasty (DSEK), and DMEK.4 The corneal endothelial transplant has become the gold standard for managing corneal endothelial failure and has gradually overtaken penetrating keratoplasty. DMEK became increasingly popular in the last few years due to decreased risk of immunological rejection, excellent visual outcome, and faster recovery.5 DMEK has undergone various modifications to achieve a safe and perfect outcome over the years. A corneal transplant may not always be successful and can result in graft rejection.6 Graft rejection can be at the level of the epithelium, stroma, or endothelium. The incidence of endothelial graft rejection is comparatively less than that of stromal or epithelial rejection.7 As per previous reports, the DMEK rejection rate varies from 0% to 2.4%, and a mean rate of 1% has been reported over two years.8 The significant risk factors for DMEK rejection are robust immune system, young age, previous penetrating keratoplasty, corneal vascularization, previous glaucoma surgery, sudden discontinuation of topical steroids, systemic comorbidities, peripheral anterior synechiae, African American ancestry, and immunosuppression.9 Recently, active COVID-19 infection and COVID-19 vaccination have also been reported as risk factors for DMEK rejection. Intraoperative graft handling is the key in DMEK to achieve perfect graft adherence, longevity, and success rate. This, in turn, reduces the endothelial cell loss, rebubbling rate, and the number of patient visits to the operating room.6 As per the detailed literature review, a comprehensive review article on risk factors for DMEK rejection is lacking. There is also a lack of consensus in the definition for DMEK rejection, primary and secondary failure as well. This current perspective focusses on DMEK rejection, DMEK primary and secondary graft failure, and recent advances in diagnosis and management of DMEK rejection. This article also provides additional literature on close differentials of DMEK failure, rejection, prognosis, and future perspective of DMEK.
Method of Search
We performed a detailed systematic literature search using search engines such as PubMed, Cochrane Library database, Google Scholar, Google books, and ePub publications. The search was performed using keywords and boolean operators such as descemet membrane endothelial keratoplasty (DMEK), (AND) risk factors, (OR) DMEK immune reaction, (OR) outcomes of DMEK, (OR) DMEK rejection, (OR) Endothelial keratoplasty, (OR) indications of Endothelial keratoplasty, (OR) (rejection treatment). The search was done for all recent case reports, case series, review articles, original articles, clinical trials, and editorials. We reviewed all the articles in English, and articles in languages other than English were also checked for their abstracts and relevant literature. Tables 1 and 2 and CONSORT flow diagram (Figure 1) discuss all the articles from 2017 to 2022 (last 5 years).
 |
Table 1 Review of Literature of DMEK Graft Rejection (Larger Case Series) of the Past 5 Years |
 |
Table 2 Review of Literature of DMEK Graft Rejection (Case Reports) of the Past 5 Years |
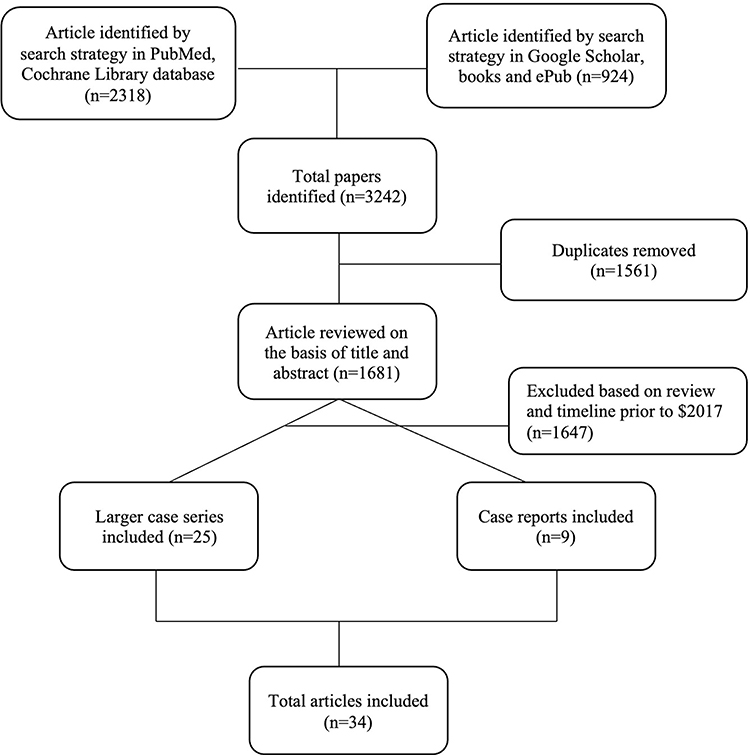 |
Figure 1 Depicting the CONSORT flowchart of the systematic review. |
Pathophysiology of Graft Rejection
The corneal avascularity, absence of lymphatics, and immune privilege are responsible for a high success rate of corneal transplantation. The avascularity prevents the inflammatory cell load and also prevents the infiltration of immune-responsive cells. When there is the absence of lymphatics, the foreign antigen load is also limited.10 Of all the corneal transplants, the endothelial rejection rate is the least. Khodadoust and Silverstein showed that corneal epithelium, stroma, and endothelial layer are independently prone to endothelial rejection. Graft eccentricity, graft size, stromal vascularization, and suture placement are the factors responsible for initiating graft rejection. The endothelial rejection is governed by cellular infiltration from the anterior chamber as well as from stromal vessels. Another report demonstrated that immune privilege resides in the anterior chamber and endothelium and that epithelium and stroma are more prone to immune reactions. They also showed that endothelium is less antigenic than stroma and epithelium. In DMEK, there is the absence of sutures, and there is no stromal tissue transplanted either. Hence, there is a reduction in antigenic load, and there is a reduced risk of rejection.10,11
Differential Diagnosis of Graft Failure
While PGF presents as persistent edema not clearing since the surgery with or without rebubbling interventions, SGF presents as new onset edema.12 It is imperative to wait for 2–3 months, according to the literature, to diagnose PGF. In our experience, sometimes DMEK corneas have cleared even after three months for unknown reasons and continued to do well after that. One significant differential or confounder that must be ruled out is ocular hypertension-related epithelial edema. IOP spikes at any stage could present with isolated epithelial microcystic edema, which could be falsely labelled as PGF or SGF. Graft failure demonstrates corneal stromal edema with or without Descemet folds and not as isolated epithelial edema, reversible with IOP control. Frank or subclinical graft rejection or hypertensive uveitis also pose a challenge.13 Typically, graft failure does not show any evidence of AC inflammation or keratic precipitates on endothelium and is a normotensive process. Viral endotheliitis is another important differential diagnosis of DMEK graft rejection.
Descemet Membrane Endothelial Keratoplasty Graft Failure
It is essential to differentiate failure from rejection and understand each process in relation to the other. Many of the risk factors for these two entities overlap, and clinicians tend to misdiagnose one condition with the other. While rejection can sometimes be one of the reasons for failure, there are many different reasons for DMEK failure. Graft failure is typically classified as “Primary (PGF)” and ‘Secondary (SGF).12 After the surgery, if the cornea fails to clear at all, it is considered PGF. The duration considered post-DMEK before diagnosing PGF varies between 2 and 3 months. If the cornea fails or becomes oedematous after remaining clear in the first 2–3 months, it is considered SGF.12 PGF is one of the most common causes of transplant failure post-DMEK compared to PKP, DALK, and DSAEK, where rejection and ocular surface issues dominate.14
The percentage of graft failure reported in DMEK varies depending on the centre’s experience, the indication for DMEK, and whether they include or exclude the cases in their learning curve, apart from other reasons. A meta-analysis comparing DMEK and DSAEK found an overall failure rate of 2.14% (6 out of 280 eyes) for DMEK.15 A report from the American Academy of Ophthalmology (AAO) based on over 47 studies reported a PGF of 0–12.5% and SGF of 0–6.3%.16 A large retrospective study by Birbal et al of a 5-year follow-up of 500 eyes post-DMEK reported a 0.2% PGF and 2.8% SGF.17 They did not specifically compare outcomes when performed for different indications. A study by Vasiliauskaite et al of 10-year outcomes of DMEK reported no PGF and 6% SGF over the ten years. They excluded the first 25 cases of DMEK owing to learning curve-related complications and reported the outcomes of only the subsequent 100 cases.18 Besek et al reported outcomes in 150 eyes post-DMEK with a follow-up duration of 7 years. Out of 150 eyes studied, 11.3% of eyes had PGF, and 9.3% had SGF.12 A total of 59.3% of their cohort had been operated on for bullous keratopathy, and they also did not exclude their initial cases from analysis. The above are probable reasons for a higher rate of graft failure.
Risk Factors for Descemet Membrane Endothelial Keratoplasty Graft Failure
Multiple distinct and overlapping factors lead to primary versus secondary graft failure. Poor quality of graft (Endothelial cell density (ECD) <2300 cells/mm2), inverse positioning, persistent detachment, and excessive manipulation during graft preparation or surgery commonly lead to PGF.19 SGF typically occurs as a slow process due to endothelial cell loss (ECL) over time for several reasons. One of the reasons for ECL could be related to a subclinical or frank immune reaction. But, there are other more common and essential reasons or risk factors for ECL loss, such as age, iatrogenic trauma, graft diameter, rebubbling, culture medium, type of gas tamponade, donor source, donor age, and type of surgery (DMEK alone or triple DMEK).20 When ECD goes below a variable threshold, the cornea begins to decompensate and show evidence of SGF.
A prospective observational study by Cakmak et al reported that preoperative low anterior chamber depth (ACD) and central corneal thickness (CCT) were associated with DMEK failure.21 While CCT >770 microns increased the risk of repeat keratoplasty by 8.75 times, ACD<2.5mm did so by 2.92-fold.21
Rebubbling post-DMEK within the first couple of months has a controversial role in the etiopathogenesis of graft failure. Rebubbling has been shown clearly to have a role in increased ECD loss.22 While one rebubbling could lead to around 157 cells/mm2 loss, ECD loss, when more than one rebubbling is done, could go up to 504 cells/mm.23 Despite the above, by controlling the other surgical and patient factors, rebubbling has not been shown to increase the graft failure rate by Gundlach et al23 While more extensive studies with more extended periods of follow-up are needed to prove or disprove the causative role of rebubbling in graft failure, it is at least transparent that rebubbling causes ECD loss,22,23 and all situations that predispose to rebubbling indirectly lead to the same.
Combined DMEK with cataract extraction (DMEK triple) has been shown to increase early detachment and rebubbling rates leading to higher ECL compared to DMEK alone by Leon et al24 Shahnazaryan et al also found higher ECL with DMEK triple but did not find an increase in the rebubbling rate.25 Leon et al also noted in their study that an anterior chamber (AC) air fill <75% in the first 2–3 hours postoperatively poses an independent risk (Odds ratio 2.66) for graft detachment.24
Eyes with previous trabeculectomy or glaucoma drainage devices tend to lose AC air much quicker than normal eyes, thereby increasing the risk of graft detachment and ECL loss. In addition, tubes in AC could also rub against the endothelium in the normal state or during eye rubbing leading to greater ECL.26 Success with rebubbling is also lower in these eyes as obtaining a good air fill is often difficult. Different study groups have shown a significantly higher rate of rebubbling and risk of DMEK graft failure in eyes with previous GDD or trabeculectomy, with GDD posing a higher risk of failure than trabeculectomy.26–29
Complex anterior segment situations such as Aniridia or Aphakia have been shown to have a higher rate of complications than hyphema, in addition to the risk of large graft detachments and very poor graft survival (44% at one year and 17% at two years).30
Descemet Membrane Endothelial Keratoplasty Graft Rejection
DMEK is generally known to have a low incidence of rejection among corneal transplants.14,31 Reasons for the low rejection rate have not been well established yet. ACAID (Anterior chamber-associated immune deviation) is a concept that has been built primarily based on animal studies. ACAID is an immunological tolerance process hypothesized to work through the splenic axis, which provides immune tolerance to foreign antigens in immune-privileged sites such as the eye’s anterior chamber.32 While it was shown that splenectomised rodents rejected corneal grafts more than others, it has not been proven in humans.33 A recent report from 2019, which showed the successful survival of DMEK graft for over four years in a splenectomised patient, has raised questions about this theory in humans.34 Another theory that the host cells replace the donor cells in the posterior lamellar transplant, thereby serving minimal alloantigen load, has also been proven wrong by a recent FISH (Fluorescence in situ hybridization) based study.34 In 6 post-mortem eyes that had received sex-mismatched DMEK tissues over 4.5 years before death, FISH consistently showed the presence of donor endothelial cells signalling the opposite sex chromosomes within the region of the transplant.35 While there may be other unknown factors altering the immune response in DMEK, it is crucial to understand the epidemiology and known risk factors for rejection (Figure 2).
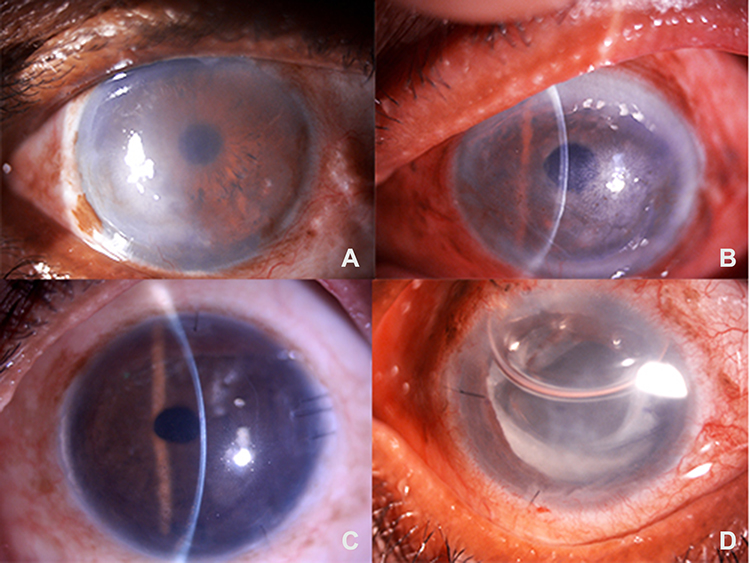 |
Figure 2 (A) Digital slit lamp image depicting a patient with pseudophakic bullous keratopathy planned for DMEK (B) Digital slit lamp image of a patient with Fuch’ Endothelial Corneal Dystrophy planned for DMEK (C) and (D) Digital slit lamp images of patients post-DMEK depicting a well opposed lenticule with relatively clear cornea. |
While allograft rejection is the most common cause of transplant failure in PKP, PGF leads as the cause of DMEK transplant failure.2 These depend on the experience of the centres reporting the data. In well-experienced centres, the incidence of PGF has become significantly low, and rejection and SGF are taking over as more common causes of transplant failure.17,18
Price et al have reported a rate of <1% for DMEK in their experience compared to around 7.9% for DSEK.36 A meta-analysis comparing DMEK and DSAEK based on 11 studies reported no rejection episodes in 158 DMEK eyes compared to 4 out of 196 DSAEK eyes.15 Another meta-analysis comparing DMEK and DSAEK in Fuchs dystrophy eyes reports a 60% less chance of rejection with DMEK than with DSAEK.37 Birbal et al report allograft rejection in 2.8% of eyes in their cohort of 500 DMEK eyes over five years.17 Among 78 eyes followed up post DMEK for two years, Basak et al reported 2.6% graft rejection.38 In a group of 150 DMEK eyes with a predominant underlying indication of bullous keratopathy over Fuchs dystrophy, Besek et al documented a 4.7% rejection rate over seven years of follow-up.12 A report from the American Academy of Ophthalmology reviewing 47 studies with a follow-up up to 68 months post-DMEK reports a range of 0–5.9% rejection rate.16 The DMEK study with the most extended follow-up of 10 years by Vasiliauskaite et al reported up to a 4% rejection rate.6 Studies reporting outcomes of DMEK performed for failed PKP report between 4% and 21% rejection rates, and vascularisation in the host cornea increases the risk.39 Eyes undergoing DMEK in the presence of a previous glaucoma surgery have been shown to have rejection rates between 7.7% and 20.8%, with higher rates for those with a glaucoma drainage device in comparison to trabeculectomy.26–29 Overall, we can see from the above that the rates of rejection with DMEK can range from 0 to 21% depending on several factors, which include duration of follow-up, indication for surgery, and presence or absence of associated glaucoma surgery (Figure 3).
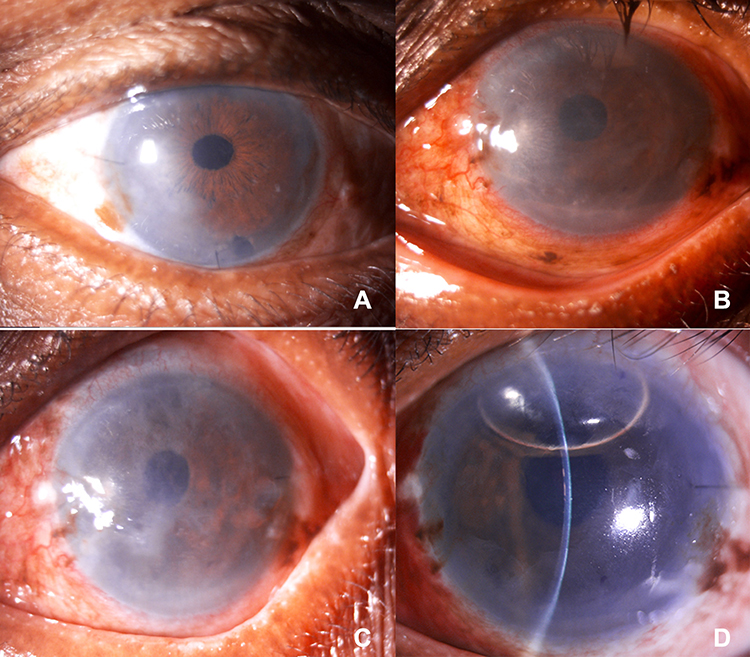 |
Figure 3 (A) Digital slit lamp image of a patient post DMEK, depicting stromal edema in the inferior one-third of cornea suggestive of early graft rejection.(B) Digital slit lamp image of a patient on a postoperative day 1, post-DMEK, depicting corneal haze with stromal edema suggestive of primary graft failure. (C) Digital slit lamp image of a patient on postoperative one month, post DMEK, depicting conjunctival congestion, corneal haze with stromal edema suggestive of primary graft failure. (D) Digital slit lamp image of a patient post DMEK following rebubbling, depicting clear cornea, well opposed lenticule with an air bubble occupying 1/3rd anterior chamber. |
Risk Factors for Descemet Membrane Endothelial Keratoplasty Rejection
It is essential to understand the risk factors to plan targeted preventive strategies. As discussed above, some of the high-risk factors for rejection are previous penetrating keratoplasty, corneal vascularisation, and previous glaucoma surgery. African Americans have been shown to have a higher risk of DMEK and DSEK rejection.40,41 Presence of pre-existing glaucoma and steroid responders also fall into the high-risk group for rejection.42 Proteomic analysis of aqueous from eyes with glaucoma shunt device show significantly higher levels of proteins involved in apoptotic, inflammatory, and oxidative pathways suggestive of breach of blood-aqueous barrier or chronic trauma.42 This could explain the poor endothelial cell survival and higher rejection rates in these eyes.
The presence of peripheral anterior synechiae has been reported in a few cases as a sign associated with DMEK graft rejection.38,43 Study of eyes with anterior synechiae in murine models showed that the synechiae could induce cytotoxic T cells activity, probably explaining the increased risk of rejection.39 Discontinuation of steroid use one year after surgery has been prospectively studied, and discontinuation leads to around 6% incidence of immune reaction.44 Hence, patients who are not on topical steroids may be considered at a higher risk of rejection.
From the beginning of the COVID-19 pandemic in early 2020, numerous reports on ocular manifestations and the possible role of transmission through the ocular surface have surfaced.45 Interestingly, COVID-19 infection and vaccination against COVID-19 are associated with DMEK graft rejection.9,46–48 Though it is difficult to prove the exact pathogenesis pathway of rejection following infection or vaccination, a strong biological plausibility is present. A few cases of DMEK rejection have been reported, including bilateral rejections in a few situations 2–3 weeks after vaccination with the BNT162b2 mRNA COVID-19 vaccine.9,46 Cases of DMEK graft rejection have also been reported in those with recent COVID-19 systemic infection. They were diagnosed only after recovery, as ophthalmic care was impossible during the acute phase.47,48 Hence, it is difficult to figure out whether the rejection occurred during or after the phase of active infection.
Clinical Presentation of Descemet Membrane Endothelial Keratoplasty Rejection
The clinical presentation of immune reaction or rejection in DMEK could vary a lot, ranging from a frank Khodadoust line49 with corneal edema, keratic precipitates (KPs), and anterior chamber (AC) inflammation to just subtle subclinical AC inflammation and KPs.32 KPs are usually granulomatous and could either be restricted to the DMEK grafts or go beyond the graft to involve areas of host cornea denuded of Descemet. It is essential to differentiate these from the melanin deposits, which could sometimes be found in the periphery of the graft. Most patients (over 60–70%) with immune reactions have been reported to be asymptomatic.50,51 Hos et al have studied the course of eyes following the adequately treated immune reaction.51 Except for a drop in the ECDs compared to before the rejection episode, they had no changes in vision or CCT. ECD further continued to remain stable without worsening over a period of up to 3 years. 3 out of 17 eyes that had an episode of rejection required regraft.52 Jordan et al studied 598 eyes, among which immunological graft rejection occurred in 54 eyes of 48 patients. The common signs of immunological rejection included keratic precipitates in 69%, corneal edema in 11%, and both in 20%. Khadadoust line was not noted in any of the patients and 35% were asymptomatic.53 Similarly, Fu and Hollick analyzed 10-year outcome of DSEK including risk factors for graft failure. The mean percentage endothelial cell loss was 46.6% ± 17.3% at year 1, 54.9% ± 18.7% at year 3, 59.6% ± 17.4% at year 5, and 73.1% ± 9.7% at year 10 years. Preoperative glaucoma and previous glaucoma surgery were labelled as the major risk factors for graft failure.54
Looking at the subtle asymptomatic nature of the presentation of the majority of the rejection episodes, it is possible that rejection is often underdiagnosed, and the percentage of graft rejection reported could be falsely lower. On the other hand, in a few situations, such as herpetic or CMV-related keratouveitis, they are falsely diagnosed as rejection.38,55 It is vital to have a high index of suspicion for infective processes when there is hypertensive uveitis in the presence of discoidal (HSV) or coin-shaped KPs (CMV) or when the corneal edema and AC inflammation do not respond adequately to topical steroids.38 AC tap with PCR for HSV, CMV, and VZV may be required at times.
Diagnosis of Descemet Membrane Endothelial Keratoplasty Rejection
While the diagnosis of DMEK rejection is clinically based on the description above, various investigative modalities help establish the diagnosis and predict the occurrence of rejection. AC tap PCR for ruling out viral aetiologies is especially useful, as indicated above, in situations where there is an inadequate or absence of response to topical steroids.
A 360-degree Scheimpflug imaging helps in picking up the inflammatory retro corneal deposits.39 This helps in 2 ways. Firstly, sometimes when a graft rejection presents with moderate to severe edema obscuring the view of the posterior cornea, this imaging helps establish the diagnosis and differentiate it from a graft failure. But, a fascinating utility of this tool has been shown by Baydoun et al50 This imaging modality could show subtle retro corneal deposits in 53% (9 out of 17) of eyes around eight months before the development of frank rejection. This imaging could play a significant role in predicting rejection episodes as ophthalmologists could not recognize these deposits during those visits using slit lamp examination.50
Specular microscopy is another invaluable tool with great utility in this field. Monnereau et al56 studied pre-rejection endothelial cell morphology and density in 7 eyes that developed rejection and compared them to control eyes. They found that these eyes displayed specific changes in cell morphology with disorganization of size, shape, and distribution along with prominent cell nuclei several months before the presentation of the clinical rejection episode. Zygoura et al termed this nuclear activation in these cells as ‘dark spots’ in specular imaging. When these were found along with a reduction in ECD, they could be a heralding sign of graft rejection.57 Baydoun et al studied the combined ability of specular microscopy with Scheimpflug imaging and reported that up to 90% of graft rejections could be predicted several months before the onset of rejection.58 Our understanding of the above two imaging modalities also opens up a possibility that DMEK rejection may be a slow chronic process rather than an acute pathological one.
Laser flare photometry is a device to quantify aqueous flare. Baydoun et al studied aqueous flare in postoperative DMEK eyes and found that the flare decreased quickly within one month from the surgery. Eyes with a persistent flare over ten ph/ms are at a higher risk of developing immunological rejection.59 In Vivo Confocal microscopy (IVCM) can recognize the inflammatory cells in the endothelium and posterior stroma during or before rejection. They are less commonly available, are challenging to use, and the findings are not very specific to rejection.60 Their utility comes up when suspecting viral etiologies in these eyes. They can pick up certain particular features like owl’s-eye endothelial cells, which are suggestive of CMV endotheliitis.55
Muijzer et al from Dutch Cornea Transplant Registry used artificial intelligence-based machine learning approach to predict graft detachment post posterior lamellar keratoplasty. They used a 91 factors coded questionnaire to understand the centre-specific practice patterns. Out of 3647 transplants, the graft detachment rate was 9.9%. The risk factors were DMEK procedure, previous graft failure and use of SF6 gas. Reduced risk was seen with combined procedures, use of pre-cut tissues and preoperative laser iridotomy.61
Management of Graft Rejection and Failure
The management of endothelial rejection is based on prompt recognition and aggressive corticosteroid therapy. Post-DMEK patients should be counselled well for the symptoms of graft rejection, such as pain, redness, photophobia, and reduced visual acuity. The patient should report immediately to the surgeon if any of these symptoms are encountered.62
Corticosteroids
Corticosteroids are the mainstay and gold standard in managing DMEK rejection due to their many beneficial properties.62 The steroid regimen varies from centre to centre. Once graft rejection is detected, an hourly or two hourly topical steroid regimen (1% prednisolone or 0.1% dexamethasone) should be followed till the signs of reversal are seen, or graft rejection is halted. These have good anterior chamber penetration compared to surface-acting steroids such as 0.1% fluorometholone or 0.5% loteprednol and have effective immunosuppressive properties. Topical steroids should be supplemented with oral and intravenous steroids such as prednisolone.63 It has been seen that after the first days of intravenous steroids, oral prednisolone plays a crucial role in reversing or arresting graft rejection. The oral steroids are started daily at 1mg/kg body weight. The initial dose is around 60–80 mg daily and tapered over 2–3 weeks based on the response.64 Intravenous methylprednisolone (IVMP) plays a vital role in reversing and arresting graft rejection from the day of presentation. IVMP is given as a pulse therapy of 500 mg in 150 mL saline twice daily for three days under close systemic monitoring.65
Adjuvant Therapy
Apart from corticosteroids, adjuvant therapy in the form of cycloplegics, such as 1% atropine or 2.5% homatropine, antiglaucoma drugs like 0.5% timolol, and oral anti-inflammatory drugs, such as diclofenac are required. Cycloplegic help relieves ciliary spasm and pain and prevents the formation of synechiae. Antiglaucoma drugs help in controlling IOP due to steroid response, and anti-inflammatory drugs take care of the pain component.66
Strategies to prevent rejection and failure primarily come from our knowledge of the discussed risk factors. Understanding the role played by each or combination of the risk factors along with a well-devised plan helps in customizing the preventive care in these eyes. Topical steroids are the mainstay in preventing graft rejection. While the standard is to maintain patients on potent steroids like prednisolone in the first month after the surgery, switching to Loteprednol 0.5% in tapering doses between 1 month to 1 year has been shown as effective as prednisolone in a similar regime.67 This could be of significant help to steroid responders. While Loteprednol, after one month of DMEK, has been shown to be as effective as prednisolone in preventing rejection, fluorometholone 0.1% has been reported to be inferior.68 Studies by Price et al have also shown the importance of continuing any topical steroid beyond one year in preventing rejection, as those who discontinued had a 6% rejection rate.44 However, there is no evidence at this point to prove the utility of steroids beyond two years.
Eyes at higher risk of rejection based on the analysis of risk factors may need to be maintained at a higher baseline dose of steroids and closely monitored. Those eyes with a herpetic or CMV-related keratouveitis affecting the course of DMEK will also benefit from oral antiviral medications.69–71 Some centres have also started routinely performing PCR for these viruses from intra-operative AC tap of all patients undergoing DMEK/DSEK. It is essential to routinely perform imaging modalities such as Scheimpflug or specular imaging as available in high-volume DMEK centres to predict rejection and accordingly manage steroid taper. To manage steroid-induced glaucoma, procedures like SLT (Selective laser trabeculoplasty) have also been safe and effective in post-DMEK eyes.72 Sex matching of donor-recipient or HLA matching is only indicated for high-risk penetrating keratoplasty, and they have not been recommended currently in preventing DMEK rejections.40,73
Prognosis After Descemet Membrane Endothelial Keratoplasty Rejection
Price et al showed that the rejection rate at five years was lower in DMEK (2.6%) compared to DSEK (7.9%) though topical steroids were tapered early in 25% of the DMEK cases.40 In this study, 44 of 705 DMEK cases failed or needed regraft due to multiple causes, including inadequate attachment of the graft, failure of clearing of the cornea, late decompensation of the endothelium, rejection, and unsatisfactory vision.1 Only 1 of these 44 cases was due to graft rejection.40 Anshu and co-workers42 noted that the risk of rejection episodes with DMEK was 15 and 20 times lesser than with DSEK and penetrating keratoplasty, respectively. The cumulative probability of rejection episodes in the 1st and 2nd years was 1% and 1%, respectively.2 The single patient with DMEK rejection in this series responded well to intensive topical steroid therapy achieving a best-corrected visual acuity (BCVA) 20/50 and endothelial cell count of 1789/mm2.42
Repeat Endothelial Keratoplasty or Penetrating Keratoplasty After Descemet Membrane Endothelial Keratoplasty Failure or Rejection
Repeat DMEK for failed primary DMEK has higher rates of failure73 and takes the patient one step closer to a penetrating keratoplasty with its known risks. Hence, it is essential to understand strategies to prevent and predict DMEK rejection. Repeat DMEK for failed DMEK has been shown to have a higher failure rate of >20% at one year and up to 30% in 6 months by different groups.73,74 Eyes undergoing repeat DMEK in the presence of a complex anterior segment as aniridia, aphakia, or ACIOL or iris fixated IOL have been shown to have up to 50% risk of re-DMEK failure.74 When DMEK is performed for failed Penetrating keratoplasty (PKP), there is variable documentation of graft failure between 14% and 53%.20,75 Over 50% of these failures are PGF due to persistent detachment. The risk of failure also increases when the failed PKP eyes have stromal vascularization.76 Moura-Coelho et al reported the results of 14 cases that needed repeat DMEK for failed primary DMEK.73 Mean best-corrected visual acuity improved after re-DMEK. Graft failure was noted in 3 eyes that also achieved at least 20/40 after tertiary keratoplasty.73 The rebubbling rate was around 30% and endothelial cell loss at one year was approximately 15%. Various postoperative complications were noted in about 43% of eyes undergoing DMEK, including high intraocular pressure, macular edema, opacification of the intraocular lens, and immune rejection.30 Graft failure was noted in 3 re-DMEK eyes due to immune rejection (2 eyes) and exhaustion of endothelial cells (1 eye).73 Baydoun et al77 evaluated the results of re-DMEK in 17 eyes, including three eyes with endothelial graft failure. After two years, 86% of patients achieved a BCVA of at least 20/40. Agha et al78 showed that BCVA was similar in eyes undergoing re-DMEK or primary DMEK, and BCVA improved after surgery in both groups.
Future Perspectives
Endothelial keratoplasty, including DMEK, have multiple limitations. The limitations include availability, preservation, and preparation of graft. Cultivated human corneal endothelial cells (CEC) are promising in this aspect. Such cells can be delivered to the posterior cornea using magnetic attraction,79 prone positions, or both via an intracameral injection.80 These cells may be delivered via multiple methods, including sphere colonies,79 ultrathin sheets, and cell-seeded scaffolds made of paramagnetic microspheres, chitosan, porcine Descemet’s membrane, and hydrogel lens.80 Stem cells [including induced pluripotent stem cells (iPSC) and mesenchymal stem cells (MSC)] offer another promising therapy for the replacement of damaged corneal endothelial cells. The sources of MSC include adipose tissue,81 bone marrow, umbilical cord, skeletal muscle, and umbilical cord blood.
A detailed literature review of DMEK Graft Rejection over the past 5 years is listed in Table 1 (Larger case series) and 2 (Case reports).9,12,17,18,28–30,37,38,43,46–48,74,76,82–98
Conclusion
Among all the corneal graft rejection subtypes, DMEK rejection accounts for the least proportion of cases. For any clinician, a thorough knowledge of the spectrum of clinical presentation of DMEK graft rejection, the risk factors and differential diagnosis is imperative for prompt diagnosis and management of these cases. The targeted treatment strategies govern the long-term visual outcome and prognosis after graft rejection and failure. Prolonged use of steroids such as prednisolone or dexamethasone for at least 1 year in steroid non-responders in the correct tapering regimen is essential to maintain graft survival. It is also imperative to differentiate immunological rejection from infectious etiology, as the management strategy will differ. We believe this article will provide a detailed understanding of DMEK rejection and its risk factor and will serve as a benchmark for the clinician while managing DMEK rejection.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gupta N, Tandon R, Gupta SK, Sreenivas V, Vashist P. Burden of corneal blindness in India. Indian J Community Med. 2013;38(4):198–206. doi:10.4103/0970-0218.120153
2. Jamali H, Gholampour AR. Indications and surgical techniques for corneal transplantation at a tertiary referral center. J Ophthalmic Vis Res. 2019;14(2):125–130. doi:10.4103/jovr.jovr_92_18
3. Wong KH, Kam KW, Chen LJ, Young AL. Corneal blindness and current major treatment concern-graft scarcity. Int J Ophthalmol. 2017;10(7):1154–1162. doi:10.18240/ijo.2017.07.21
4. Singh R, Gupta N, Vanathi M, Tandon R. Corneal transplantation in the modern era. Indian J Med Res. 2019;150(1):7–22. doi:10.4103/ijmr.IJMR_141_19
5. Fernandez MM, Afshari NA. Endothelial Keratoplasty: from DLEK to DMEK. Middle East Afr J Ophthalmol. 2010;17(1):5–8. doi:10.4103/0974-9233.61210
6. Trindade BLC, Eliazar GC. Descemet membrane endothelial keratoplasty (DMEK): an update on safety, efficacy and patient selection. Clin Ophthalmol. 2019;13:1549–1557. doi:10.2147/OPTH.S178473
7. Sugar J, Montoya M, Dontchev M, et al. Donor risk factors for graft failure in the cornea donor study. Cornea. 2009;28(9):981–985. doi:10.1097/ICO.0b013e3181a0a3e6
8. Gibbons A, Leung EH, Yoo SH. Cost-effectiveness analysis of descemet’s membrane endothelial keratoplasty versus descemet’s stripping endothelial keratoplasty in the United States. Ophthalmology. 2019;126(2):207–213. doi:10.1016/j.ophtha.2018.09.033
9. Phylactou M, Li JO, Larkin DFP. Characteristics of endothelial corneal transplant rejection following immunisation with SARS-CoV-2 messenger RNA vaccine. Br J Ophthalmol. 2021;105(7):893–896. doi:10.1136/bjophthalmol-2021-319338
10. Gurnani B, Czyz CN, Mahabadi N, Havens SJ. Corneal graft rejection. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2022.
11. Qazi Y, Hamrah P. Corneal allograft rejection: immunopathogenesis to therapeutics. J Clin Cell Immunol. 2013;2013(Suppl 9):006. doi:10.4172/2155-9899.S9-006
12. Beşek NK, Yalçınkaya G, Kırgız A, et al. Graft survival and clinical outcomes of Descemet membrane endothelial keratoplasty: long-term results. Int Ophthalmol. 2022;42(1):269–279. doi:10.1007/s10792-021-02078-4
13. Miyoshi Y, Ono T, Seki S, et al. Corneal graft rejection after descemet’s membrane endothelial keratoplasty with peripheral anterior synechiae. Case Rep Ophthalmol. 2022;13(1):17–22. doi:10.1159/000520877
14. Gómez-Benlloch A, Montesel A, Pareja-Aricò L, et al. Causes of corneal transplant failure: a multicentric study. Acta Ophthalmol. 2021;99(6):e922–e928. doi:10.1111/aos.14708
15. Pavlovic I, Shajari M, Herrmann E, Schmack I, Lencova A, Kohnen T. Meta-analysis of postoperative outcome parameters comparing descemet membrane endothelial keratoplasty versus descemet stripping automated endothelial keratoplasty. Cornea. 2017;36(12):1445–1451. doi:10.1097/ICO.0000000000001384
16. Deng SX, Lee WB, Hammersmith KM, et al. Descemet membrane endothelial keratoplasty: safety and outcomes: a report by the American Academy of Ophthalmology. Ophthalmology. 2018;125(2):295–310. doi:10.1016/j.ophtha.2017.08.015
17. Birbal RS, Ni Dhubhghaill S, Bourgonje VJA, et al. Five-year graft survival and clinical outcomes of 500 consecutive cases after descemet membrane endothelial keratoplasty. Cornea. 2020;39(3):290–297. doi:10.1097/ICO.0000000000002120
18. Vasiliauskaitė I, Oellerich S, Ham L, et al. Descemet membrane endothelial keratoplasty: ten-year graft survival and clinical outcomes. Am J Ophthalmol. 2020;217:114–120. doi:10.1016/j.ajo.2020.04.005
19. Droutsas K, Alexopoulos P, Giachos I, Giallouros E, Sekundo W, Lazaridis A. Secondary DMEK following failed primary DMEK. Int Ophthalmol. 2021;41(10):3287–3293. doi:10.1007/s10792-021-01890-2
20. Cohen E, Mimouni M, Sorkin N, et al. Risk factors for repeat descemet membrane endothelial keratoplasty graft failure. Am J Ophthalmol. 2021;226:165–171. doi:10.1016/j.ajo.2021.01.004
21. Çakmak S, Kirgiz A, Yildirim Y, Taşkoparan S, Genç S, Ağca A. The effect of anterior segment parameters on surgical success of Descemet membrane endothelial keratoplasty: a prospective study. Int Ophthalmol. 2022. doi:10.1007/s10792-022-02416-0
22. Gundlach E, Pilger D, Dietrich-Ntoukas T, Joussen AM, Torun N, Maier AB. Impact of re-bubbling after descemet membrane endothelial keratoplasty on long-term results. Curr Eye Res. 2021;46(6):784–788. doi:10.1080/02713683.2020.1842459
23. Hayashi T, Schrittenlocher S, Siebelmann S, et al. Risk factors for endothelial cell loss after descemet membrane endothelial keratoplasty (DMEK). Sci Rep. 2020;10(1):11086. doi:10.1038/s41598-020-68023-0
24. Leon P, Parekh M, Nahum Y, et al. Factors associated with early graft detachment in primary descemet membrane endothelial keratoplasty. Am J Ophthalmol. 2018;187:117–124. doi:10.1016/j.ajo.2017.12.014
25. Shahnazaryan D, Hajjar Sese A, Hollick EJ. Endothelial cell loss after descemet’s membrane endothelial keratoplasty for fuchs’ endothelial dystrophy: DMEK compared to triple DMEK. Am J Ophthalmol. 2020;218:1–6. doi:10.1016/j.ajo.2020.05.003
26. Schrittenlocher S, Grass C, Dietlein T, et al. Graft survival of Descemet membrane endothelial keratoplasty (DMEK) in corneal endothelial decompensation after glaucoma surgery. Graefes Arch Clin Exp Ophthalmol. 2022;260(5):1573–1582. doi:10.1007/s00417-021-05506-4
27. Alshaker S, Mimouni M, Batawi H, et al. Four-year survival comparison of endothelial keratoplasty techniques in patients with previous glaucoma surgery. Cornea. 2021;40(10):1282–1289. doi:10.1097/ICO.0000000000002585
28. Sorkin N, Mimouni M, Kisilevsky E, et al. Four-year survival of descemet membrane endothelial keratoplasty in patients with previous glaucoma surgery. Am J Ophthalmol. 2020;218:7–16. doi:10.1016/j.ajo.2020.05.020
29. Boutin T, Sorkin N, Einan-Lifshitz A, et al. Descemet membrane endothelial keratoplasty in patients with prior glaucoma surgery. Eur J Ophthalmol. 2021;31(4):2121–2126. doi:10.1177/1120672120936178
30. Santaella G, Sorkin N, Mimouni M, et al. Outcomes of descemet membrane endothelial keratoplasty in aphakic and aniridic patients. Cornea. 2020;39(11):1389–1393. doi:10.1097/ICO.0000000000002387
31. Hos D, Schlereth S, Schrittenlocher S, et al. “Descemet membrane endothelial keratoplasty” (DMEK) bei Transplantatversagen nach perforierender Keratoplastik und in vaskularisierten Hochrisikoaugen [Descemet membrane endothelial keratoplasty (DMEK) for graft failure after penetrating keratoplasty and in vascularized high-risk eyes]. Ophthalmologe. 2021;118(6):536–543. doi:10.1007/s00347-021-01384-7
32. Stein-Streilein J, Streilein JW. Anterior chamber associated immune deviation (ACAID): regulation, biological relevance, and implications for therapy. Int Rev Immunol. 2002;21(2–3):123–152. doi:10.1080/08830180212066
33. Hos D, Matthaei M, Bock F, et al. Immune reactions after modern lamellar (DALK, DSAEK, DMEK) versus conventional penetrating corneal transplantation. Prog Retin Eye Res. 2019;73:100768. doi:10.1016/j.preteyeres.2019.07.001
34. Hos D, Schaub F, Cursiefen C. Does anterior chamber-associated immune deviation (ACAID) play a role in posterior lamellar keratoplasty? Case report of a splenectomized patient. BMC Ophthalmol. 2019;19(1):100. doi:10.1186/s12886-019-1114-1
35. Lavy I, Verdijk RM, Bruinsma M, et al. Sex chromosome analysis of postmortem corneal endothelium after sex-mismatch descemet membrane endothelial keratoplasty. Cornea. 2017;36(1):11–16. doi:10.1097/ICO.0000000000001019
36. Price MO, Price FW
37. Marques RE, Guerra PS, Sousa DC, Gonçalves AI, Quintas AM, Rodrigues W. DMEK versus DSAEK for Fuchs’ endothelial dystrophy: a meta-analysis. Eur J Ophthalmol. 2019;29(1):15–22. doi:10.1177/1120672118757431
38. Basak SK, Basak S, Gajendragadkar N. Outcomes of descemet membrane endothelial keratoplasty using cornea from elderly donors aged 80 years and older: in the aftermath of current donor shortage. Cornea. 2021;41:1437–1443. doi:10.1097/ICO.0000000000002902
39. Price MO, Jordan CS, Moore G, Price FW
40. Price DA, Kelley M, Price FW Jr, Price MO. Five-year graft survival of descemet membrane Endothelial Keratoplasty (EK) versus descemet stripping EK and the effect of donor sex matching. Ophthalmology. 2018;125(10):1508–1514. doi:10.1016/j.ophtha.2018.03.050
41. Moshirfar M, Thomson AC, Ronquillo Y. Corneal endothelial transplantation. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2022.
42. Anshu A, Price MO, Richardson MR, et al. Alterations in the aqueous humor proteome in patients with a glaucoma shunt device. Mol Vis. 2011;17:1891–1900.
43. Carreras-Castañer X, Batlle-Ferrando S, Marin-Martinez S, Miguel L, Feu-Basilio S, Peraza-Nieves JE. Anterior synechiae related to an incipient Descemet’s membrane endothelial keratoplasty (DMEK) allograft rejection. J Fr Ophtalmol. 2020;43(10):e389–e391. doi:10.1016/j.jfo.2020.01.033
44. Price MO, Scanameo A, Feng MT, Price FW
45. Shetty R, D’Souza S, Lalgudi VG. What ophthalmologists should know about conjunctivitis in the COVID-19 pandemic? Indian J Ophthalmol. 2020;68(5):683–687. doi:10.4103/ijo.IJO_869_20
46. Forshaw TRJ, Jørgensen C, Kyhn MC, Cabrerizo J. Acute bilateral descemet membrane endothelial keratoplasty graft rejection after the BNT162b2 mRNA COVID-19 vaccine. Int Med Case Rep J. 2022;15:201–204. doi:10.2147/IMCRJ.S362698
47. Bitton K, Dubois M, Courtin R, Panthier C, Gatinel D. Descemet’s membrane endothelial keratoplasty (DMEK) rejection following COVID-19 infection: a case report. Am J Ophthalmol Case Rep. 2021;23:101138. doi:10.1016/j.ajoc.2021.101138
48. Moriyama AS, Campos MSQ. Presumed DMEK graft rejection associated with COVID-19 infection. Cornea. 2022;41(2):e1. doi:10.1097/ICO.0000000000002882
49. Dapena I, Ham L, Netuková M, van der Wees J, Melles GR. Incidence of early allograft rejection after Descemet membrane endothelial keratoplasty. Cornea. 2011;30(12):1341–1345. doi:10.1097/ICO.0b013e31820d8540
50. Baydoun L, Livny E, Ham L, Bruinsma M, Melles GR. 360-degree scheimpflug imaging to predict allograft rejection after descemet membrane endothelial keratoplasty. Cornea. 2016;35(11):1385–1390. doi:10.1097/ICO.0000000000001007
51. Hos D, Tuac O, Schaub F, et al. Incidence and clinical course of immune reactions after descemet membrane endothelial keratoplasty: retrospective analysis of 1000 consecutive eyes. Ophthalmology. 2017;124(4):512–518. doi:10.1016/j.ophtha.2016.12.017
52. Schaub F, Bachmann BO, Cursiefen C, Hos D. Midterm follow-up of immune reactions after Descemet membrane endothelial keratoplasty (DMEK). Graefes Arch Clin Exp Ophthalmol. 2019;257(8):1811–1812. doi:10.1007/s00417-019-04357-4
53. Jordan CS, Price MO, Trespalacios R, Price FW
54. Fu L, Hollick EJ. Long-term outcomes of descemet stripping endothelial keratoplasty: ten-year graft survival and endothelial cell loss. Am J Ophthalmol. 2022;234:215–222. doi:10.1016/j.ajo.2021.08.005
55. Moshirfar M. Recurrent endothelial rejection after DSAEK and DMEK causing corneal perforation in a patient with history of Fuchs endothelial dystrophy: October consultation #1. J Cataract Refract Surg. 2017;43(10):1358–1359. doi:10.1016/j.jcrs.2017.10.004
56. Monnereau C, Bruinsma M, Ham L, Baydoun L, Oellerich S, Melles GR. Endothelial cell changes as an indicator for upcoming allograft rejection following descemet membrane endothelial keratoplasty. Am J Ophthalmol. 2014;158(3):485–495. doi:10.1016/j.ajo.2014.05.030
57. Zygoura V, Baydoun L, Monnereau C, Satué M, Oellerich S, Melles GRJ. Dark endothelial spots after descemet membrane endothelial keratoplasty may appear as recurrent fuchs dystrophy or herald graft failure or rejection. Cornea. 2017;36(12):1480–1485. doi:10.1097/ICO.0000000000001375
58. Baydoun L, Bruinsma M, Santander-García D, Ham L, Oellerich S, Melles GRJ. Combined specular microscopy and Scheimpflug imaging to improve detection of an upcoming allograft rejection after DMEK. Acta Ophthalmol. 2020;98(3):261–266. doi:10.1111/aos.14234
59. Baydoun L, Chang Lam F, Schaal S, et al. Quantitative assessment of aqueous flare after descemet membrane endothelial keratoplasty for fuchs endothelial dystrophy. Cornea. 2018;37(7):848–853. doi:10.1097/ICO.0000000000001576
60. Okumura N, Velumani T, Hadiya F, et al. Analysis of immune cells on donor corneal endothelium after corneal transplantation using the HRT-Rostock cornea module. Cornea. 2021;40(11):1445–1452. doi:10.1097/ICO.0000000000002706
61. Muijzer MB, Hoven CMW, Frank LE, Vink G, Wisse RPL; Netherlands Corneal Transplant Network (NCTN). A machine learning approach to explore predictors of graft detachment following posterior lamellar keratoplasty: a nationwide registry study. Sci Rep. 2022;12(1):17705. doi:10.1038/s41598-022-22223-y
62. Hill JC, Maske R, Watson PG. The use of a single pulse of intravenous methylprednisolone in the treatment of corneal graft rejection. A preliminary report. Eye. 1991;5(Pt 4)):420–424. doi:10.1038/eye.1991.67
63. Nguyen NX, Seitz B, Martus P, Langenbucher A, Cursiefen C. Long-term topical steroid treatment improves graft survival following normal-risk penetrating keratoplasty. Am J Ophthalmol. 2007;144(2):318–319. doi:10.1016/j.ajo.2007.03.028
64. Hill JC, Maske R, Watson P. Corticosteroids in corneal graft rejection. Oral versus single pulse therapy. Ophthalmology. 1991;98(3):329–333. doi:10.1016/S0161-6420(91)32291-7
65. Young AL, Rao SK, Cheng LL, Wong AK, Leung AT, Lam DS. Combined intravenous pulse methylprednisolone and oral cyclosporine A in the treatment of corneal graft rejection: 5-year experience. Eye. 2002;16(3):304–308. doi:10.1038/sj.eye.6700144
66. Azevedo Magalhaes O, Shalaby Bardan A, Zarei-Ghanavati M, Liu C. Literature review and suggested protocol for prevention and treatment of corneal graft rejection. Eye. 2020;34(3):442–450. doi:10.1038/s41433-019-0517-9
67. Price MO, Feng MT, Scanameo A, Price FW
68. Price MO, Price FW Jr, Kruse FE, Bachmann BO, Tourtas T. Randomized comparison of topical prednisolone acetate 1% versus fluorometholone 0.1% in the first year after descemet membrane endothelial keratoplasty. Cornea. 2014;33(9):880–886. doi:10.1097/ICO.0000000000000206
69. Friehmann A, Myerscough J, Giannaccare G, Mazzoni M, Bovone C, Busin M. Successful descemet membrane endothelial keratoplasty in proven herpetic endothelial decompensation requires intensive antiviral therapy. Cornea. 2020;39(2):196–199. doi:10.1097/ICO.0000000000002215
70. Basak SK, Basak S. Descemet membrane endothelial keratoplasty in irreversible corneal edema due to herpes simplex virus endotheliitis. Cornea. 2020;39(1):8–12. doi:10.1097/ICO.0000000000002135
71. Tan TE, Tan DTH. Cytomegalovirus corneal endotheliitis after descemet membrane endothelial keratoplasty. Cornea. 2019;38(4):413–418. doi:10.1097/ICO.0000000000001847
72. Davidson M, Berkowitz E, Roberts H, Wanas A, Myerscough J. Selective laser trabeculoplasty for steroid-induced ocular hypertension following endothelial keratoplasty. Curr Eye Res. 2022;47(10):1362–1365. doi:10.1080/02713683.2022.2088800
73. Böhringer D, Schwartzkopff J, Maier PC, Reinhard T. Immunologie der keratoplastik: macht HLA-matching bei lamellären verfahren sinn? [HLA matching in keratoplasty: lessons learned from lamellar techniques]. Klin Monbl Augenheilkd. 2013;230(5):490–493. doi:10.1055/s-0032-1328256
74. Moura-Coelho N, Manero F, Elies D, et al. Repeat descemet membrane endothelial keratoplasty for failed primary descemet membrane endothelial keratoplasty at a referral center for keratoplasty in Spain: DIMOEK study. Am J Ophthalmol. 2020;215:49–55. doi:10.1016/j.ajo.2020.03.015
75. Wu J, Wu T, Li J, Wang L, Huang Y. DSAEK or DMEK for failed penetrating keratoplasty: a systematic review and single-arm meta-analysis. Int Ophthalmol. 2021;41(7):2315–2328. doi:10.1007/s10792-021-01778-1
76. Einan-Lifshitz A, Mednick Z, Belkin A, et al. Comparison of descemet stripping automated endothelial keratoplasty and descemet membrane endothelial keratoplasty in the treatment of failed penetrating keratoplasty. Cornea. 2019;38(9):1077–1082. doi:10.1097/ICO.0000000000001993
77. Baydoun L, van Dijk K, Dapena I, et al. Repeat Descemet membrane endothelial keratoplasty after complicated primary Descemet membrane endothelial keratoplasty. Ophthalmology. 2015;122(1):8–16. doi:10.1016/j.ophtha.2014.07.024
78. Agha B, Shajari M, Slavik-Lencova A, Kohnen T, Schmack I. Functional outcome of repeat Descemet membrane endothelial keratoplasty (DMEK) for corneal decompensation following graft failure after primary DMEK. Clin Ophthalmol. 2019;13:477–482. doi:10.2147/OPTH.S192424
79. Mimura T, Shimomura N, Usui T, et al. Magnetic attraction of iron-endocytosed corneal endothelial cells to Descemet’s membrane. Exp Eye Res. 2003;76(6):745–751. doi:10.1016/S0014-4835(03)00057-5
80. Nuzzi R, Marolo P, Tridico F. From DMEK to corneal endothelial cell therapy: technical and biological aspects. J Ophthalmol. 2018;2018:6482095. doi:10.1155/2018/6482095
81. Zuk PA, Zhu M, Ashjian P, et al. Human adipose tissue is a source of multipotent stem cells. Mol Biol Cell. 2002;13(12):4279–4295. doi:10.1091/mbc.e02-02-0105
82. Shah AP, Dzhaber D, Kenyon KR, Riaz KM, Ouano DP, Koo EH. Acute Corneal Transplant Rejection After COVID-19 Vaccination. Cornea. 2022;41(1):121–124. doi:10.1097/ICO.0000000000002878
83. Basak SK, Basak S, Gajendragadkar N, Ghatak M. Overall clinical outcomes of Descemet membrane endothelial keratoplasty in 600 consecutive eyes: a large retrospective case series. Indian J Ophthalmol. 2020;68(6):1044–1053. doi:10.4103/ijo.IJO_1563_19
84. Crnej A, Khoueir Z, Cherfan G, Saad A. Acute corneal endothelial graft rejection following COVID-19 vaccination. J Fr Ophtalmol. 2021;44(8):e445–e447. doi:10.1016/j.jfo.2021.06.001
85. Balidis M, Mikropoulos D, Gatzioufas Z, de Politis PB, Sidiropoulos G, Vassiliadis V. Acute corneal graft rejection after anti-severe acute respiratory syndrome-coronavirus-2 vaccination: a report of four cases. Eur J Ophthalmol. 2021;2021:11206721211064033.
86. Fu L, Hollick EJ. Rebubbling and graft detachment in Descemet membrane endothelial keratoplasty using a standardised protocol. Eye. 2022. doi:10.1038/s41433-022-02362-2
87. Maier AB, Pilger D, Gundlach E, Winterhalter S, Torun N, Dietrich-Ntoukas T. Graft failure rate and complications after Descemet membrane endothelial keratoplasty in eyes with pre-existing glaucoma. Graefes Arch Clin Exp Ophthalmol. 2022;30:1.
88. Jung YH, Yoon CH, Kim MK. Clinical outcome of Descemet membrane endothelial keratoplasty (DMEK) with imported donor corneas in eyes of Asian patients; endothelium-in versus endothelium-out method. PLoS One. 2022;17(6):e0270037. doi:10.1371/journal.pone.0270037
89. Sorkin N, Gouvea L, Din N, et al. Five-year safety and efficacy of femtosecond laser-assisted descemet membrane endothelial keratoplasty. Cornea. 2022. doi:10.1097/ICO.0000000000003019
90. Mittal V, Sehdev N, Mittal R. Descemet membrane endothelial keratoplasty in congenital hereditary endothelial dystrophy: initial experiences. Cornea. 2021;40(8):972–976. doi:10.1097/ICO.0000000000002701
91. Hayashi T, Zhang W, Hos D, et al. Descemet membrane endothelial keratoplasty in vascularized eyes: outcome and effect on corneal neovascularization. Cornea. 2021;40(6):685–689. doi:10.1097/ICO.0000000000002502
92. Mednick Z, Sorkin N, Einan-Lifshitz A, et al. Long-term outcomes of descemet membrane endothelial keratoplasty in post vitrectomized eyes with the use of pars plana infusion. Cornea. 2020;39(4):457–460. doi:10.1097/ICO.0000000000002228
93. Sorkin N, Mimouni M, Santaella G, et al. Comparison of manual and femtosecond laser-assisted descemet membrane endothelial keratoplasty for failed penetrating keratoplasty. Am J Ophthalmol. 2020;214:1–8. doi:10.1016/j.ajo.2019.11.015
94. Woo JH, Ang M, Htoon HM, Tan D. Descemet membrane endothelial keratoplasty versus descemet stripping automated endothelial keratoplasty and penetrating keratoplasty. Am J Ophthalmol. 2019;207:288–303. doi:10.1016/j.ajo.2019.06.012
95. Birbal RS, Tong CM, Dapena I, et al. Clinical outcomes of descemet membrane endothelial keratoplasty in eyes with a glaucoma drainage device. Am J Ophthalmol. 2019;199:150–158. doi:10.1016/j.ajo.2018.11.014
96. Showail M, Obthani MA, Sorkin N, et al. Outcomes of the first 250 eyes of Descemet membrane endothelial keratoplasty: Canadian centre experience. Can J Ophthalmol. 2018;53(5):510–517. doi:10.1016/j.jcjo.2017.11.017
97. Pasari A, Price MO, Feng MT, Price FW
98. Fajgenbaum MAP, Kopsachilis N, Hollick EJ. Descemet’s membrane endothelial keratoplasty: surgical outcomes and endothelial cell count modelling from a UK centre. Eye. 2018;32(10):1629–1635. doi:10.1038/s41433-018-0152-x
99. Weller JM, Kruse FE, Tourtas T. Descemet membrane endothelial keratoplasty: analysis of clinical outcomes of patients with 8–10 years follow-up. Int Ophthalmol. 2022;42(6):1789–1798. doi:10.1007/s10792-021-02176-3
100. Schrittenlocher S, Schaub F, Hos D, Siebelmann S, Cursiefen C, Bachmann B. Evolution of consecutive descemet membrane endothelial keratoplasty outcomes throughout a 5-year period performed by two experienced surgeons. Am J Ophthalmol. 2018;190:171–178. doi:10.1016/j.ajo.2018.03.036
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.