Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 20
Risk Factors for Acute Exacerbation in Patients with COPD Group E in Ningbo: Risk Analysis of Irregular Review, Cardiovascular Complications, and Lung Function Decline
Authors Qian Y, Sun C, Zhang L, Cai C ![]() , Sun M, Zhang J, Huang J, Ma H, Tan L, Zhao Y, Wang S, Lv D
, Sun M, Zhang J, Huang J, Ma H, Tan L, Zhao Y, Wang S, Lv D ![]()
Received 15 January 2025
Accepted for publication 22 July 2025
Published 8 August 2025 Volume 2025:20 Pages 2787—2799
DOI https://doi.org/10.2147/COPD.S510906
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Richard Russell
Yang Qian,1 Chao Sun,1 Liang Zhang,2 Chenting Cai,1 Mengqing Sun,1 Jiaqian Zhang,1 Jian Huang,3 Hongying Ma,1 Lin Tan,1 Yun Zhao,1 Shanshan Wang,1 Dan Lv1
1The First Affiliated Hospital of Ningbo University, Ningbo, 315010, People’s Republic of China; 2Ningbo Municipal Center for Disease Control and Prevention, Ningbo, 315000, People’s Republic of China; 3School of Big Data and Software Engineering, Zhejiang Wanli University, Ningbo, 315100, People’s Republic of China
Correspondence: Dan Lv, The First Affiliated Hospital of Ningbo University, 59 Liuting Street, Ningbo City, Zhejiang Province, People’s Republic of China, Email [email protected]
Objective: To understand the high-risk factors for disease progression in patients in the chronic obstructive pulmonary disease (COPD) group E in Ningbo, and to explore the impact of and treatment on the prognosis of these patients.
Methods: We retrospectively analyzed the clinical data of 101 COPD patients in terms of general demographics, physical baseline data, lung function, disease treatment, and prognosis and used crosstab analysis and logistic regression analysis to understand the characteristics of the population of patients at high risk of acute exacerbation of COPD (AECOPD) and the associated risk factors.
Results: Univariate analysis demonstrated that frequent acute exacerbation (AE) in the COPD group E population was significantly associated with more severe airflow limitation, a lower FEF75%, higher mMRC scores, and irregular disease management (P< 0.05). Comorbid cardiovascular disease increased AE risk 4.138-fold (P< 0.05). Multivariate analysis confirmed that irregular disease review, cardiovascular comorbidity, and mMRC grades 3– 4 were risk factors (P< 0.05). Regular review reduced AE risk, while cardiovascular disease and mMRC grades 3– 4 increased the risk 8.802-fold and 12.327-fold, respectively.
Conclusion: The severity of airflow restriction, instantaneous flow during forced exhalation of 75% of the lung capacity, cardiovascular disease complexity, higher mMRC scores, and irregular participation in intervention treatment were associated with disease deterioration in patients at high risk of AECOPD. Regular participation in standardized intervention management and treatment is a protective factor against worsening events in high-risk patients with AECOPD. These results may reduce medical resource utilization and AE frequency while improving quality of life, thereby informing evidence-based COPD management strategies and optimizing chronic disease care and resource allocation.
Keywords: COPD, intervention management, risk factors, regular review, acute exacerbation, high risk
Introduction
Chronic Obstructive Pulmonary Disease (COPD) is a respiratory disease characterized by chronic respiratory symptoms such as chronic cough and sputum, chest tightness, and shortness of breath. It is a prevalent global disease with significant morbidity, disability, and mortality rates, profoundly impacting the health and quality of life of affected individuals.1,2 Acute exacerbation of chronic obstructive pulmonary disease (AECOPD) is a critical event characterized by the worsening of respiratory symptoms. This exacerbation is triggered by factors such as microbial infections, airborne particulate pollutants, comorbidities (such as the cardiovascular system, respiratory system, or endocrine metabolism), negative psychological factors, and deficiency disease, which then require adjustments in medication management.3 Acute exacerbation (AE) is a significant point in the progression and treatment of COPD, serving as a critical event in the mortality of COPD patients and resulting in substantial health and economic implications for society and families.1,4 Patients in COPD group E are generally considered to be at a higher risk of developing AECOPD if they have experienced two or more AE events or at least one hospitalization for AE in the previous year.5 A higher frequency of AE, more severe disease symptoms (including typical respiratory symptoms such as cough, sputum production, chest constriction, and dyspnea), and a worse prognosis are observed in these patients.6–9 Therefore, the prompt identification of high-risk groups for AE and the application of efficient and standardized intervention and treatment techniques are critical for improving patient outcomes and reducing the need for medical resources.
Effective management of stable COPD involves addressing current symptoms and future risks to reduce the likelihood of AE, slow disease progression, and improve patient survival rates. During AE episodes, the focus shifts to minimizing negative impacts and preventing recurrence. Consistent with this, standardized management throughout COPD is crucial for successful prevention and rehabilitation.10 The complex and varied nature of AECOPD suggests that a multitude of factors can influence the likelihood and severity of exacerbations.11–14 Consequently, investigating the primary determinants of AECOPD, particularly the relationship between comprehensive disease management and the onset and progression of exacerbations in group E, is highly important for preventing AE. Despite the inclusion of intervention management for AECOPD in many diagnosis and treatment guidelines, there is still room for improvement in understanding the specific correlation between the two. This study aimed to investigate the biological, environmental, psycho-behavioral, socioeconomic, and healthcare-related risk factors for AE development in group E COPD patients in Ningbo, China. The clinical significance of modifiable risk factors in subsequent disease management was also examined, including behaviors such as smoking, vaccination status, adherence to medication regimens, management of comorbidities, and compliance with regular follow-up appointments. These findings may facilitate early identification of high-risk COPD patients and inform the development of effective intervention strategies.
Materials and Methods
Research Subjects
Patients in group E (high-risk AECOPD patients), who sought care at the outpatient department and ward of the Department of Respiratory and Critical Care Medicine at the Affiliated Hospital of Ningbo University School of Medicine between January 1, 2020, and December 31, 2021. Participants were rigorously screened according to predefined inclusion criteria and applicable exclusion criteria obtained through medical record review. Using the electronic medical record system (HIS) and health platform at the Affiliated Hospital of Ningbo University School of Medicine, potential subjects were identified for this study. The final cohort of 101 subjects was established after excluding individuals who either became lost to follow-up, declined to participate, or provided incomplete treatment histories or behavioral data, as determined through telephone interviews and outpatient follow-up evaluations. All subjects underwent comprehensive diagnostic evaluations and pulmonary function testing upon enrollment.
The inclusion criteria for this study are as follows: a) 40 ≤ age ≤ 80; b) The patients who fulfilled the diagnostic criteria outlined in the Guidelines for the Diagnosis and Treatment of COPD and global initiative for COPD (GOLD) established by the COPD Group of the Respiratory Society of the Chinese Medical Association. Specifically, following the exclusion of other diagnoses, patients with a pulmonary function test showing a post-inhalation bronchodilator FEV1 < 70% and clinical symptoms including a chronic cough, sputum, dyspnea, and/or a history of exposure to disease-related risk factors are definitively diagnosed with COPD; and c) COPD E group, AE-related hospitalizations, or at least two AE events in a year. Criteria for exclusion (satisfy any one of them): Individuals who have undergone anticancer therapy, have active pulmonary tuberculosis (TB) or pulmonary fibrosis, are deceased, are pregnant, have mixed cognitive and communicative abnormalities, are experiencing severe organ failure, or have been lost to follow-up.
Subjects were selected based on the number of AE times and hospitalizations in the preceding year. The patients were then categorized into two groups: the infrequent AE group (<2 times/year) and the frequent AE group (≥2 times/year or at least 1 hospitalization).
Clinical Data Collection
The electronic medical record system of the affiliated hospital of Ningbo University Medical School, health browser, telephone follow-up, and outpatient services were utilized to gather pertinent clinical data. Baseline demographic, physical, life-work behavior, and medical condition information were collected. Physical examination data were measured and entered into the system by healthcare professionals following standard procedures. The remaining clinical data were obtained by the collectors from the HIS and the health platform, and the missing parts were added through outpatient or telephone follow-up. Subjects’ baseline demographic, life-work behavior, and medical condition information were verified twice during outpatient or telephone follow-ups. Clinical data were collected from patients with stable COPD, with strict adherence to privacy protection protocols and ethical standards throughout the study.
Observation Indicators and Definitions
Educational Level
According to subjects’ educational status, including primary and below, junior high school, high school and technical secondary school, college or above.
Residential Area
Subjects were classified by usual place of residence (countryside/urban).
Smoking Behavior
Following WHO’s 1997 standardized smoking survey methodology, smokers are defined as those with ≥6 months of continuous smoking. Current smokers were actively smoking within 30 days pre-data collection, while quitters had ceased by that time. Smoking intensity was measured in pack-years: (daily cigarettes/20) × smoking years.15
Biomass
Biomass exposure refers to smoke from burning biofuels (wood, animal manure, crops). Participants were classified by exposure status (yes/no).16
Occupational Dust
Occupational dust exposure refers to prolonged workplace exposure to production-related dust. Subjects were categorized based on exposure history (yes/no).
Influenza Vaccination
Subjects were stratified by annual influenza vaccination adherence over the preceding 3 years (yes/no).
Live Alone
Subjects living without cohabitants for ≥1 year were classified as living alone (yes/no).
COPD/Lung Function Awareness
COPD and lung function awareness reflect subjects’ understanding of these concepts, categorized as yes or no.
Modified Medical Research Council (mMRC)
mMRC scores ranges from grade 0 (dyspnea only during strenuous exercise) to grade 4 (severe dyspnea preventing basic activities or leaving home, with intermediate grades reflecting progressively worse symptoms: grade 1 indicates dyspnea when walking fast or climbing slight inclines; grade 2 describes walking slower than peers or needing to rest on level ground; and grade 3 requires stopping after walking 100m or a few minutes on level ground. We defined grades 0–2 as low-grade and grades 3–4 as high-grade.
Body Mass Index (BMI)
It was categorized into four groups: underweight (BMI <18.5), normal weight (18.5–23.9), overweight (24.0–27.9), and obese (≥28.0).
Respiratory Symptoms
The primary clinical manifestations of COPD were categorized as cough, sputum, dyspnea, and chest tightness.
Regular Review
It was defined as regular tertiary hospital visits for comprehensive care, including symptom assessment, pulmonary evaluation (physical examination/imaging/lung function), medication guidance, and efficacy assessment. Participants were stratified by adherence: yes (≥4 annual visits) or no (<4).
Regular Medication
Subjects were categorized by medication adherence into yes (demonstrating correct inhalation technique with high adherence for ≥6 months) and no (failing to meet either the inhalation technique or adherence duration criteria).
COPD Grading
It was categorized into four groups: GOLD 1 (FEV1 ≥80%), GOLD 2 (50–79%), GOLD 3 (30–49%), and GOLD 4 (FEV1 <30%).
Lung Function
Forced expiratory volume in one second (FEV1), peak expiratory flow (PEF), maximum mid-expiratory flow (MMEF), forced expiratory flow, forced expiratory flow 25% (FEF25%), forced expiratory flow 50% (FEF50%), forced expiratory flow 75% (FEF75%).
Comorbidity
The comorbidities assessed included cardiovascular, digestive (excluding hepatobiliary), respiratory, musculoskeletal, genitourinary, hepatobiliary, and endocrine diseases.
Ethical Issues
This research, which was approved by the Ethics Committee of Ningbo University Medical College Hospital (KY20201123), is part of the application research of “Internet + Medical Treatment” for Urban and Rural COPD Precision Treatment and Whole Course Management. This study complies with the Declaration of Helsinki. Given that the study is retrospective, the Ethics Committee Review Board of the First Affiliated Hospital of Ningbo University determined that it was not necessary to obtain informed consent for participation. Researchers only used the data for research purposes and would strictly keep the personal information and privacy confidential.
Statistical Methods
Statistical analysis of the experimental data was carried out with SPSS 27.0 statistical software and the R programming language. The measurement data are presented  , and group comparisons were made using the independent sample t-test; the counting data are presented as rates, and the independence test was performed using the cross-contingency test. The quantitative influence link between the factors and the target was investigated using logistic regression analysis. The difference was statistically significant when P<α, with a significance level of α =0.05. The data have been well tested and none of them can reject the assumption of normality and are normally distributed.
, and group comparisons were made using the independent sample t-test; the counting data are presented as rates, and the independence test was performed using the cross-contingency test. The quantitative influence link between the factors and the target was investigated using logistic regression analysis. The difference was statistically significant when P<α, with a significance level of α =0.05. The data have been well tested and none of them can reject the assumption of normality and are normally distributed.
Results
Analysis of Influencing Factors Related to Disease Progression in the COPD Group E Population
Comparison of Differences in Baseline Characteristics Between the Two Groups
This study included 101 individuals, with 37 patients in the infrequent-AE group and 64 in the frequent-AE group. Table 1 shows the baseline characteristics of the individuals.
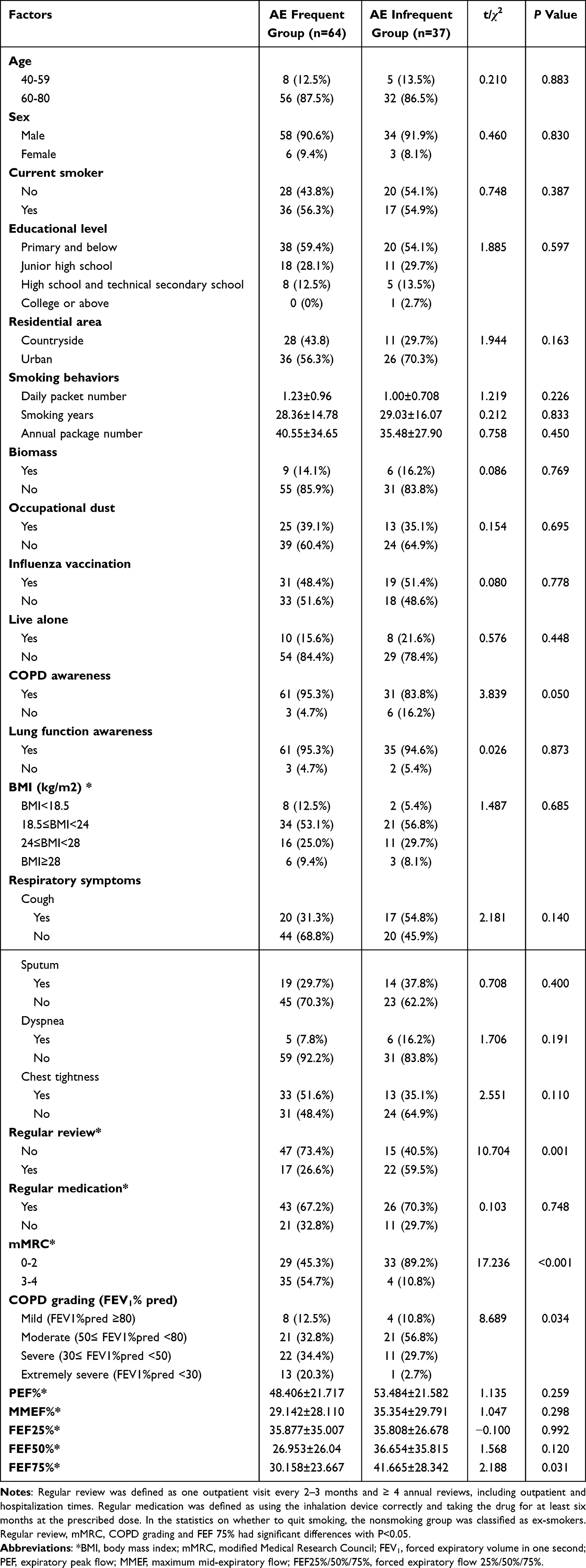 |
Table 1 Analysis of Factors Influencing the Occurrence of AE in a Population of Patients in Group E |
Statistical analysis revealed that the mMRC score, regular review, FEF 75%, and airflow limitation severity were significantly associated with the risk of disease exacerbation in patients in the COPD group E (P < 0.05). The findings indicated that the AE-frequent COPD group E had worse FEF75% levels, more participants with mMRC scores in the high grades, more severe airflow limitation, and a higher percentage of subjects who did not participate in regular review than did the AE-infrequent group. This study revealed no statistically significant differences between the two groups of subjects in terms of age, sex, tobacco smoking status, education status, living alone, biomass exposure, occupational dust exposure, influenza vaccination, medication regularity, respiratory clinical symptoms, etc. (P > 0.05). Patients in the frequent AE group smoked more average daily cigarettes, more total smokers, and a higher percentage of subjects reported chest tightness symptoms.
The influence of regular review against the mMRC score on disease exacerbation in group E patients was then explored further, and the probability of AE occurrence was plotted on the basis of the mMRC score under various regular review grading settings. This demonstrated that regular review decreased the incidence of AE events in the group E sample across all mMRC score levels. The risk of AECOPD increased dramatically when the mMRC score increased from 1 to 3 but only slightly as the mMRC score increased from 0 to 1 (Figure 1).
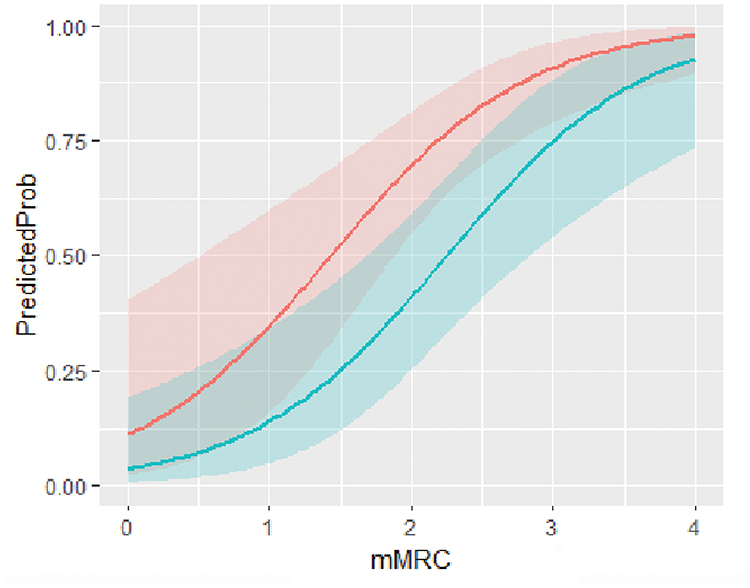 |
Figure 1 Probability of AECOPD corresponding to each grade of regular review and mMRC (The graph’s curves show how frequently the participants’ follow-up care was provided; a value of 1 denotes regular review, while a value of 0 denotes irregular review). |
Univariate Study of the Relationship Between Illness Progression and Systemic Comorbidities
To clarify the impact of various systemic comorbidities on the progression of AE in people at high risk, as well as the relationships among them, we included comorbidities from seven different systems: cardiovascular, digestive (except for liver and gallbladder diseases), respiratory, osteoarthritic, urinary, hepatobiliary, and endocrine system diseases. Univariate logistical regression analysis revealed that cardiovascular diseases may increase the probability of disease progression in group E individuals (P < 0.05). The study findings demonstrated that individuals at risk for AE who had cardiovascular disease had a 4.138-fold greater risk of experiencing disease exacerbation than those who did not (Table 2). More than half of the participants had atherosclerosis (54.5%) and hypertension (55.4%), the two most common disorders in the cardiovascular system category in our studies. However, no significant correlation was observed between the risk of disease exacerbation and other systemic comorbidities.
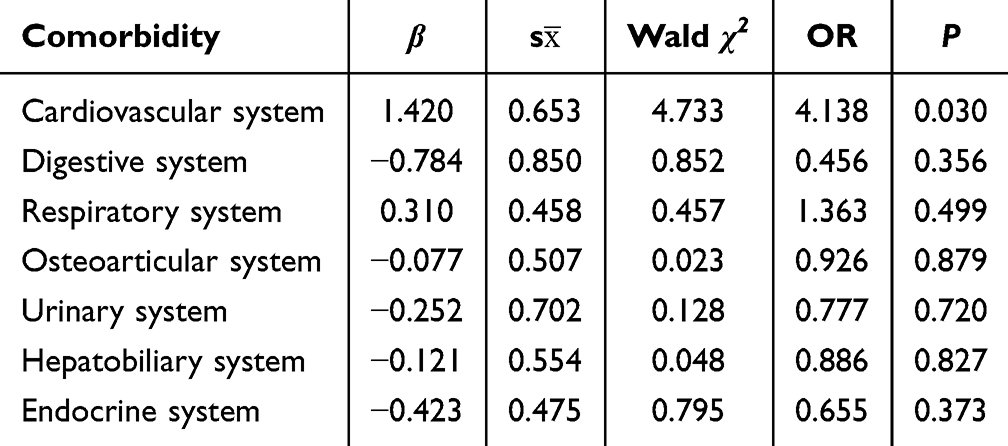 |
Table 2 Univariate Logistic Regression Analysis of Comorbidities Between the Two Groups |
Multivariate Logistic Regression Analysis
The degree of risk was further clarified by incorporating statistically significant variables into the multivariate logistic regression analysis model following the previous examination of the pertinent elements that may affect the group E subjects. Five variables in total were included in this multivariate logistic regression analysis (Table 3).
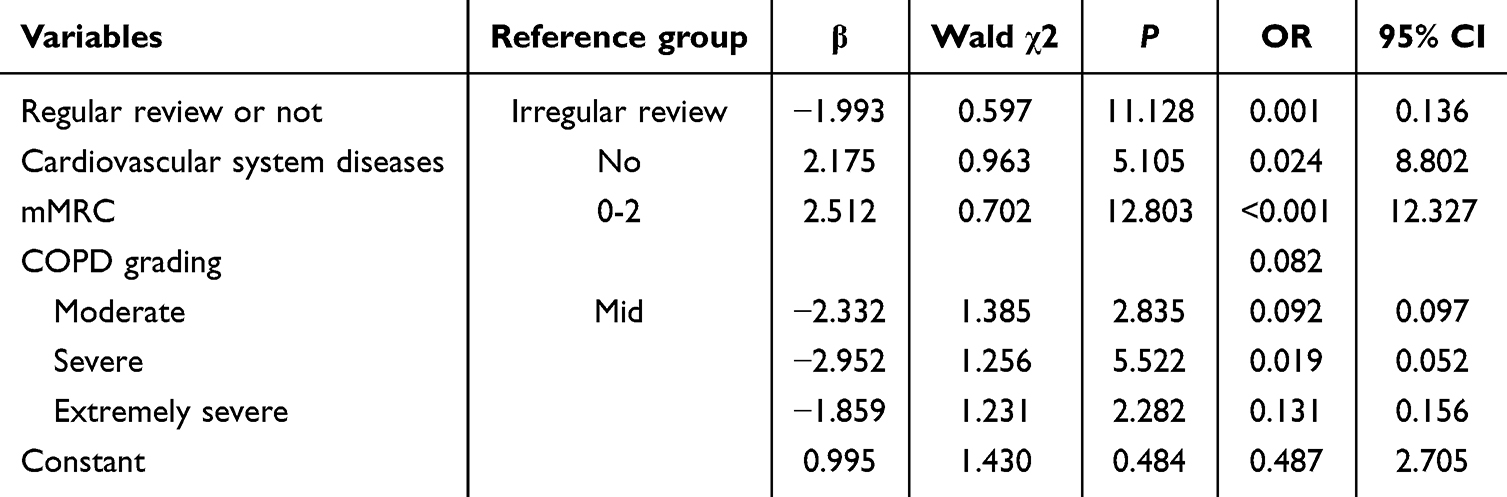 |
Table 3 Multivariate Logistic Regression Analysis of AECOPD in the High-Risk Population |
Multivariate logistic regression analysis revealed that cardiovascular disease, mMRC, and regular review may be risk factors for disease deterioration in group E subjects, and this relationship was statistically significant (P < 0.05). The odds ratio (OR) for patients with combined cardiovascular disease was 8.802 (95% CI: 1.334--58.072), indicating that individuals with more combined cardiovascular illness had an 8.802-fold greater risk of COPD exacerbation than those with less combined cardiovascular disease. The group E subjects with irregular reviews had a greater risk of illness deterioration (OR 0.136, 95% CI: 1.981--14.048). In addition, individuals with high mMRC scores (grades 3--4) were 12.327 times more likely to experience deterioration in their disease than those with relatively low mMRC scores (grades 0--2). Patients with mild airflow restriction had an OR of 8.799, but the difference was not statistically significant (P > 0.05).
Discussion
AE is the center of attention for the COPD process and is essential to the progression of the illness. A comprehensive analysis of the variables influencing the incidence of AE events in individuals at high risk of AE revealed that AE is not only a transient worsening of respiratory symptoms or airflow restriction but also the outcome of several multisystemic factors that are crucial in determining how the COPD disease process progresses. These factors include patient demographics, clinical background, social and environmental factors, and disease-modifying treatment approaches.2,3 AECOPD and various contributing factors must be recognized, the qualitative and quantitative relationships between them and AECOPD must be clarified, and comprehensive interventions to lower the risk of acute exacerbation must be implemented to better manage those at high risk of AE. To improve the prognosis of these patients, investigating the relationships between clinical traits, treatment features, and other influencing factors and disease exacerbation in group E subjects is beneficial clinically. To complement the existing experimental findings of the relevant topics and the content of the literature, we analyzed the clinical case data and disease examination data of 101 patients at high risk of AE from the Affiliated Hospital of Ningbo University Medical College. The final results of this study indicate that in the Ningbo-based AECOPD patient population, the occurrence of AE events may be influenced by multiple factors, including the severity of airflow limitation, FEF75%, cardiovascular comorbidities, mMRC scores, and adherence to regular review.
We investigated the connection between a few lung function markers and the development of COPD in the present study. The results revealed that FEF 75% and airflow limitation severity in COPD patients were associated with worse performance outcomes in the group E population, which has more frequent disease exacerbations. These findings are consistent with findings in previous studies and may suggest that a greater degree of airflow limitation and worse mid- and late expiratory flow rates are linked to the occurrence of disease progression in individuals at high risk of AE.17,18 The inflammatory response of the airways and the increase in small airway resistance can cause further decreases in lung ventilation function, the retention of carbon dioxide in the lungs, and worsening of patients’ conditions. Emphysema, sputum, and fibrous tissue production can also lead to pulmonary obstructive ventilation dysfunction, which causes persistent airflow limitation, affects metabolism and gas exchange, and results in disease deterioration in patients with COPD.19
Small airway dysfunction typically manifests early in the course of COPD, and there is a strong association between the severity of the condition and its progression.20–24 The literature indicates that assessments of small airway obstruction can serve as early predictors for future COPD and that pathologic changes such as reduced alveolar elastic rebound and increased small airway resistance can cause obstructive ventilation dysfunction in the lungs. Patients with small airway dysfunction are more likely to experience airflow restriction and declining lung function as their disease progresses.17,25,26 Although they have not received much attention, FEF25-75% and MMEF are frequently assessed in pulmonary function tests. These measurements probably represent minor airway branching, tube size, and airway cartilage.21 Clinical examinations are frequently used to quantify anomalies and severity using the percentage of anomalies measured against the expected values for these measures. In the current investigation, the FEF 75% level was lower in the group of participants with a high frequency of AE than in those with infrequent AE, even if we did not detect a significant correlation between MMEF and FEF 25–50% and the risk of AE. These data may suggest that in populations at high risk of adverse events, decreases in indicators of small airway function may be associated with an increased risk of adverse events. In addition, several studies have indicated that patients at high risk for AE with higher GOLD grades are also at increased risk for disease progression, with those with GOLD grades 3 and 4 being significantly more likely to be at high risk than those in the infrequent-AE group. The degree of airway compromise increases as the GOLD grade increases, with GOLD grade 1 having the least amount of airway compromise and GOLD grade 4 having the greatest amount.27 To further elucidate small airway function, we may add additional airway function scoring indices or combine them with imaging in subsequent experiments. This is because existing evidence suggests that predicting small airway function on the basis of only changes in various spirometric indices may lead to false positives or false negatives on the basis of age, height, sex, and interracial differences.21,28
These findings are similar to the results of previous studies on the risk of exacerbation of combined cardiovascular disease in the generalized COPD population.29–32 We also discovered in the comorbidity study that the risk of disease progression was 4.138 times greater in group E patients with cardiovascular disease, and that it was more pronounced in group E patients with comorbid cardiovascular disease. There was no significant correlation when the impact of other systemic diseases on the probability of disease advancement was examined in those who were at high risk of AE disease development (P > 0.05). In addition, cardiovascular system disease was found to be significantly correlated with patient’s risk of disease progression in a multifactorial regression analysis model. Compared with those without cardiovascular system disease, group E patients with cardiovascular comorbidities had an 8.802-fold greater risk of disease progression. In previous studies of a similar nature, those with AECOPD had a fourfold greater risk of cardiovascular events.33 By inducing vascular smooth muscle proliferation, pulmonary hypertension can increase the pulmonary artery diameter. Prolonged pulmonary hypertension can also result in a condition known as right heart overload and a reduction in the right heart’s ability to compensate. There is a subsequent increase in the risk of disease development when the ratio of pulmonary artery diameter to aortic diameter is greater than 1.34–36 Furthermore, extant research has established a correlation between coronary artery disease and the risk of disease progression. Specifically, patients with AECOPD who have severe airflow limitation and reduced lung function are at increased risk of developing coronary artery disease, potentially as a result of lung inflation, pulmonary hypertension, and the systemic inflammatory response.33,37–39 There was also a positive link between the length of hospital stay and the rate of ICU admission in COPD patients with concomitant coronary artery disease.40 Individual sex differences in AECOPD patients’ combined rates of coronary artery disease and the ensuing clinical consequences are noteworthy.40,41
Additionally, we discovered that in both groups with the two groups of patients with the two groups of patients with different frequencies of AE, the mMRC score and the presence or absence of regular reviews had an impact on disease exacerbation. The group E subjects with more frequent AE events had a higher proportion of mMRC scores with high grades. This finding shows that patients at higher risk who have more frequent exacerbations may also have more severe dyspnea symptoms and a higher degree of disease risk. An increase in the mMRC score suggests that patients at high risk of adverse events may have a worse clinical outcome since the mMRC score might, to some extent, reflect the patient’s activity tolerance, quality of life, and illness prognosis. The mMRC grade was strongly correlated with the risk of disease deterioration in according to the multivariate regression model. Specifically, group E subjects with mMRC grades 3--4 had a 12.327-fold greater risk of disease deterioration than did group E subjects with MMRC grades 0--2. Our research demonstrated that in group E subjects, following a regular review regimen throughout treatment significantly improved COPD disease control and prevented acute exacerbation. The occurrence of disease deterioration in individuals with a high risk of adverse events was then found to be negatively correlated with regular review, as demonstrated by multifactorial logistic regression analysis. Furthermore, after a thorough examination of the correlation between mMRC scores and adverse events, regular review was effective in reducing the risk of disease progression. However, differences exist across the range of mMRC scores. In contrast to the other ranges, the correlation between acute exacerbation and routine review was stronger when the mMRC score was grade 2. Therefore, timely intervention and management should be implemented for group E populations with elevated mMRC scores to minimize the risk of disease deterioration in clinical practice.
Consequently, it is anticipated that regular review, a crucial component of managing COPD, will increase the benefits for COPD patients during long-term management therapy. Many studies on COPD have shown that treating patients with interventions throughout both stable and acute exacerbation phases improves the prognosis of the disease.42–44 Regular review of the adverse events of group E individuals during disease control can help clinical medical staff monitor and manage the prognosis and development of the disease in group E individuals. This allows for timely adjustments to the patient’s treatment plans and enhances their capacity for self-management. The death and disability rates of COPD patients will increase in the future due to the high number of patients with this disease, as well as the persistence of numerous risk factors and the aging of the global population. For the group E patients, prompt diagnosis and treatment, as well as comprehensive intervention and management measures, are crucial. Long-term standardized management and intervention for COPD patients may also help improve the prognosis and quality of life of patients while lessening the negative effects of AE during disease.
Comparative analysis of the between-group differences between the frequent and infrequent deterioration groups revealed no significant relationships between the occurrence of disease deterioration in individuals at high risk of AE and baseline characteristics, including age, sex, education, place of residence, history of exposure to biofuel fumes, history of occupational exposure to dust, influenza vaccination, living alone, current smoking cessation, knowledge of COPD, knowledge of lung function, and BMI. Nonetheless, additional research conducted in different parts of the world has revealed some correlations between the aforementioned characteristics and AE.45–48 Research has demonstrated that for every ten years in which a patient’s age increases, the probability of an AE increases by 20%.49 In addition to age, the literature highlights the possibility that a BMI of less than 20 kg/m2 can act as a stand-alone risk factor for death from respiratory diseases; patients at high nutritional risk may experience abnormalities in their ability to swallow and breathe, which are strongly positively correlated with both the risk of adverse events and the risk of death.50–54 Higher education was associated with a lower risk of developing COPD, based on a 2018 large-scale epidemiological study conducted in China.2 A separate prospective study of 2499 participants found that COPD patients with elementary school education or less had a mortality risk over 4 times higher than those with university education or above, according to Cox regression analysis.51 Additionally, the 2024 GOLD report highlighted that COPD prevalence is higher in low and middle-income countries, identifying education level as one of the socioeconomic assessment indicators.10 These findings may reflect the association between educational attainment and progression of chronic lung disease.
The frequency and rate of AECOPD are significantly influenced by exposure to tobacco smoking.46,47 In recent years, there has been increasing emphasis on the threat that biomass smoke poses to the COPD community, particularly among female patients. Both types of smoke cause injury in the same way, eroding the mechanical barrier of the lungs, which increases the production of mucus in the sputum and fosters an environment that is more conducive to the survival of bacteria. This may exacerbate lung function decline, alter the host’s inflammatory response to microbes, and increase the risk of readmission and mortality in COPD patients.55–57 In light of these findings, more qualified participants (particularly females) might be added to later studies to better represent the target demographic in the data profile. By expanding the eligible sample size in the following experiments, in conjunction with other research in the literature, we can carry out more investigations into the distribution and baseline features of the group E subjects.
The findings of this study may offer some clinical support for screening, hierarchical diagnosis, and treatment of COPD by urban and rural general practitioners in Ningbo. They may also help to advance the “Internet-Medical Management Information System for accurate treatment and full management of COPD in urban and rural areas”. This study, however, still has certain shortcomings.
First, the sample data used in this retrospective research were preexisting and could have been influenced by several biases or confounding variables. These findings may have limited generalizability to all high-risk populations due to potential selection bias. The study cohort may overrepresent easily accessible individuals while underrepresenting harder-to-reach groups. Meanwhile, the results likely reflect characteristics of psychologically resilient and health-conscious high-risk patients, as some AECOPD patients declined participation due to privacy concerns, whereas others voluntarily consented to follow-up. Additionally, COPD progression involves multifactorial determinants - including individual, environmental, and socioeconomic factors - not all of which could be accounted for in this study, potentially influencing the outcomes. Second, it is not possible to establish causal links between variables using retrospective studies; they can only offer correlations between variable indicators. Finally, given the limitations of the sample size and representativeness, the findings of this study may not be fully applicable to all circumstances. However, future research may increase the sample size and enhance the sample selection process to increase the study’s external validity.
Conclusion
In high-risk AECOPD patients, AE is influenced by multiple factors, including airflow limitation, FEF75%, cardiovascular comorbidities, mMRC scores, and regular clinical review. Specifically, severe airflow obstruction, worse FEF75%, presence of cardiovascular comorbidities, higher mMRC scores, and irregular clinical review are all significantly associated with increased AE frequency. Promoting a healthy lifestyle, which includes maintaining a balanced diet, ensuring adequate sleep, and engaging in moderate exercise, along with urging smoking cessation and encouraging patients to exercise according to their fitness level, will mitigate the impact of cardiovascular disease. Meanwhile, we need to strengthen precise management and provide professional guidance for patients with higher mMRC scores. We should also encourage and supervise these patients to undergo regular assessment, take the initiative to understand their condition, and accept standardized interventions and management, thereby improving the disease prognosis.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Ningbo Science and Technology Bureau (No. 202003N4023), the Key Research and Development Plan of Ningbo City (No. 2023Z179), the Zhejiang Provincial Natural Science Foundation of China (No. LTGY24H010002) and the Zhejiang Public Welfare Fund (No. LGF21C010001).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Christenson SA, Smith BM, Bafadhel M, Putcha N. Chronic obstructive pulmonary disease. Lancet. 2022;399(10342):2227–2242. doi:10.1016/S0140-6736(22)00470-6
2. Wang C, Xu J, Yang L, et al. Prevalence and risk factors of chronic obstructive pulmonary disease in China (the China Pulmonary Health [CPH] study): a national cross-sectional study. Lancet. 2018;391(10131):1706–1717. doi:10.1016/S0140-6736(18)30841-9
3. Qian Y, Cai C, Sun M, Lv D, Zhao Y. Analyses of factors associated with acute exacerbations of chronic obstructive pulmonary disease: a review. Int J Chron Obstruct Pulmon Dis. 2023;18:2707–2723. doi:10.2147/COPD.S433183
4. Ko FW, Chan KP, Hui DS, et al. Acute exacerbation of COPD. Respirology. 2016;21(7):1152–1165. doi:10.1111/resp.12780
5. G.S. Committee, global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease (2024 report), 2024. Availabe from: https://goldcopd.org/.
6. Cardoso J, Coelho R, Rocha C, Coelho C, Semedo L, Bugalho Almeida A. Prediction of severe exacerbations and mortality in COPD: the role of exacerbation history and inspiratory capacity/total lung capacity ratio. Int J Chron Obstruct Pulmon Dis. 2018;13:1105–1113. doi:10.2147/COPD.S155848
7. Margüello MS, Garrastazu R, Ruiz-Nuñez M, et al. Independent effect of prior exacerbation frequency and disease severity on the risk of future exacerbations of COPD: a retrospective cohort study. NPJ Prim Care Respir Med. 2016;26:16046. doi:10.1038/npjpcrm.2016.46
8. Dixit D, Bridgeman MB, Andrews LB, et al. Acute exacerbations of chronic obstructive pulmonary disease: diagnosis, management, and prevention in critically ill patients. Pharmacotherapy. 2015;35(6):631–648. doi:10.1002/phar.1599
9. Suissa S, Dell’Aniello S, Ernst P. Long-term natural history of chronic obstructive pulmonary disease: severe exacerbations and mortality. Thorax. 2012;67(11):957–963. doi:10.1136/thoraxjnl-2011-201518
10. Wedzicha JAE-C-C, Miravitlles M, Hurst JR, et al. Management of COPD exacerbations: a European Respiratory Society/American Thoracic Society guideline. Eur Respir J. 2017;49(3):1600791. doi:10.1183/13993003.00791-2016
11. Muneeb Hassan M, Ameeq M, Jamal F, Tahir MH, Mendy JT. Prevalence of covid-19 among patients with chronic obstructive pulmonary disease and tuberculosis. Ann Med. 2023;55(1):285–291. doi:10.1080/07853890.2022.2160491
12. Hassan MM, Sikandar SM, Jamal F, Ameeq M, Kargbo A. The complex relationship between chronic obstructive pulmonary disease with cardiovascular disease and their interactions with COVID-19 vaccination: a retrospective study. Immun Inflamm Dis. 2024;12(11):e70068. doi:10.1002/iid3.70068
13. Hassan MM, Sikandar SM, Jamal F, Ameeq M, Kargbo A. Chronic obstructive pulmonary disease patients with community-acquired pneumonia on inhaled corticosteroid therapy: a comprehensive analysis of risk factors, disease burden, and prevention strategies. Health Sci Rep. 2025;8(1):e70395. doi:10.1002/hsr2.70395
14. Hassan MM, Tahir MH, Ameeq M, Jamal F, Mendy JT, Chesneau C. Risk factors identification of COVID-19 patients with chronic obstructive pulmonary disease: a retrospective study in Punjab-Pakistan. Immun Inflamm Dis. 2023;11(8):e981. doi:10.1002/iid3.981
15. Available from: https://www.who.int/.
16. Ortiz-Quintero B, Martínez-Espinosa I, Pérez-Padilla R. Mechanisms of lung damage and development of COPD due to household biomass-smoke exposure: inflammation, oxidative stress, MicroRNAs, and gene polymorphisms. Cells. 2022;12(1):67. doi:10.3390/cells12010067
17. Anzueto A, Miravitlles M. Pathophysiology of dyspnea in COPD. Postgrad Med. 2017;129(3):366–374. doi:10.1080/00325481.2017.1301190
18. Yamaya M, Usami O, Nakayama S, et al. Airflow limitation and severe emphysema are risks for exacerbation of chronic obstructive pulmonary disease in Japanese subjects: a retrospective single-center study. Int J Chron Obstruct Pulmon Dis. 2020;15:857–868. doi:10.2147/COPD.S238457
19. Zhenying C, Cheng TW, Pin NT. Frequent hospital readmissions duo to acute exacerbation of COPD and their associated factors. Chin J Clin Healthcare. 2005;2005:1.
20. Postma DS, Brightling C, Baldi S, et al. Exploring the relevance and extent of small airways dysfunction in asthma (ATLANTIS): baseline data from a prospective cohort study. Lancet Respir Med. 2019;7(5):402–416. doi:10.1016/S2213-2600(19)30049-9
21. Almeshari MA, Alobaidi NY, Sapey E, Stockley RA, Stockley JA. Small airways dysfunction: the importance of utilising Z-scores to define MMEF abnormalities in clinical practice. Heliyon. 2023;9(10):e20744. doi:10.1016/j.heliyon.2023.e20744
22. Kwon DS, Choi YJ, Kim TH, et al. FEF(25-75%) values in patients with normal lung function can predict the development of chronic obstructive pulmonary disease. Int J Chron Obstruct Pulmon Dis. 2020;15:2913–2921. doi:10.2147/COPD.S261732
23. Stockley JA, Ismail AM, Hughes SM, Edgar R, Stockley RA, Sapey E. Maximal mid-expiratory flow detects early lung disease in α 1 -antitrypsin deficiency. Eur Respir J. 2017;49(3):1602055. doi:10.1183/13993003.02055-2016
24. Alobaidi NY, Almeshari M, Stockley J, Stockley RA, Sapey E. Small airway function measured using forced expiratory flow between 25% and 75% of vital capacity and its relationship to airflow limitation in symptomatic ever-smokers: a cross-sectional study. BMJ Open Respir Res. 2022;9(1):e001385.
25. Quanjer PH, Weiner DJ, Pretto JJ, Brazzale DJ, Boros PW. Measurement of FEF25-75% and FEF75% does not contribute to clinical decision making. Eur Respir J. 2014;43(4):1051–1058. doi:10.1183/09031936.00128113
26. Knox-Brown B, Potts J, Santofimio VQ, et al. Isolated small airways obstruction predicts future chronic airflow obstruction: a multinational longitudinal study. BMJ Open Respir Res. 2023;10(1):1.
27. Lu L, Peng J, Wu F, et al. Clinical characteristics of airway impairment assessed by impulse oscillometry in patients with chronic obstructive pulmonary disease: findings from the ECOPD study in China. BMC Pulm Med. 2023;23(1):52. doi:10.1186/s12890-023-02311-z
28. Quanjer PH, Cooper B, Ruppel GL, et al. Defining airflow obstruction. Eur Respir J. 2015;45(2):561–562. doi:10.1183/09031936.00126014
29. Sievi NA, Senn O, Brack T, et al. Impact of comorbidities on physical activity in COPD. Respirology. 2015;20(3):413–418. doi:10.1111/resp.12456
30. Tsiligianni IG, Kosmas E, Van der Molen T, Tzanakis N. Managing comorbidity in COPD: a difficult task. Curr Drug Targets. 2013;14(2):158–176. doi:10.2174/1389450111314020004
31. de Miguel-Díez J, Carrasco-Garrido P, Rejas-Gutierrez J, et al. The influence of heart disease on characteristics, quality of life, use of health resources, and costs of COPD in primary care settings. BMC Cardiovasc Disord. 2010;10:8. doi:10.1186/1471-2261-10-8
32. Rogliani P, Calzetta L, Matera MG, et al. Inhaled therapies and cardiovascular risk in patients with chronic obstructive pulmonary disease. Expert Opin Pharmacother. 2019;20(6):737–750. doi:10.1080/14656566.2019.1570133
33. Donaldson GC, Hurst JR, Smith CJ, Hubbard RB, Wedzicha JA. Increased risk of myocardial infarction and stroke following exacerbation of COPD. Chest. 2010;137(5):1091–1097. doi:10.1378/chest.09-2029
34. Cuttica MJ, Bhatt SP, Rosenberg SR, et al. Pulmonary artery to aorta ratio is associated with cardiac structure and functional changes in mild-to-moderate COPD. Int J Chron Obstruct Pulmon Dis. 2017;12:1439–1446. doi:10.2147/COPD.S131413
35. Wells JM, Morrison JB, Bhatt SP, Nath H, Dransfield MT. Pulmonary artery enlargement is associated with cardiac injury during severe exacerbations of COPD. Chest. 2016;149(5):1197–1204. doi:10.1378/chest.15-1504
36. Wells JM, Washko GR, Han MK, et al. Pulmonary arterial enlargement and acute exacerbations of COPD. N Engl J Med. 2012;367(10):913–921. doi:10.1056/NEJMoa1203830
37. Rabe KF, Hurst JR, Suissa S. Cardiovascular disease and COPD: dangerous liaisons? Eur Respir Rev. 2018;27(149):180057. doi:10.1183/16000617.0057-2018
38. Zhang J, Yi Q, Zhou C, et al. A simple clinical risk score (ABCDMP) for predicting mortality in patients with AECOPD and cardiovascular diseases. Respir Res. 2024;25(1):89. doi:10.1186/s12931-024-02704-6
39. Leong P, Bardin PG. The untreated treatable trait: cardiovascular disease in COPD exacerbations. Respirology. 2021;26(5):413–415. doi:10.1111/resp.14036
40. Cui Y, Zhan Z, Ma Y, et al. Clinical and economic burden of comorbid coronary artery disease in patients with acute exacerbation of chronic obstructive pulmonary disease: sex differences in a nationwide cohort study. Respir Res. 2022;23(1):28. doi:10.1186/s12931-022-01945-7
41. Almagro P, López García F, Cabrera FJ, et al. Comorbidity and gender-related differences in patients hospitalized for COPD. ECCO study Respir Med. 2010;104(2):253–259. doi:10.1016/j.rmed.2009.09.019
42. Perera B, Barton C, Osadnik C. General practice care following acute exacerbations of COPD: a survey of Australian general practitioners. PLoS One. 2023;18(4):e0284731. doi:10.1371/journal.pone.0284731
43. Tandan M, Dunlea S, Cullen W, Bury G. Teamwork and its impact on chronic disease clinical outcomes in primary care: a systematic review and meta-analysis. Public Health. 2024;229:88–115. doi:10.1016/j.puhe.2024.01.019
44. Perera B, Barton C, Osadnik C. General practice management of COPD patients following acute exacerbations: a qualitative study. Br J Gen Pract. 2023;73(728):e186–e195. doi:10.3399/BJGP.2022.0342
45. Li X, Wu Z, Xue M, Du W. Smoking status affects clinical characteristics and disease course of acute exacerbation of chronic obstructive pulmonary disease: a prospectively observational study. Chron Respir Dis. 2020;17:1479973120916184. doi:10.1177/1479973120916184
46. Montserrat-Capdevila J, Godoy P, Marsal JR, Barbe F, Galvan L. Risk factors for exacerbation in chronic obstructive pulmonary disease: a prospective study. Int J Tuberc Lung Dis. 2016;20(3):389–395. doi:10.5588/ijtld.15.0441
47. Eisner M. The impact of SHS exposure on health status and exacerbations among patients with COPD. Int J Chronic Obstr. 2009;169. doi:10.2147/COPD.S4681
48. Saad AB, Adhieb A, Migaou A, et al. Effect of intensity of smoking intoxication on severity parameters of acute exacerbations of chronic obstructive pulmonary disease treated in a hospital milieu. Pan Afr Med J. 2021;38:91. doi:10.11604/pamj.2021.38.91.21512
49. Jarad N. Chronic obstructive pulmonary disease (COPD) and old age? Chron Respir Dis. 2011;8(2):143–151. doi:10.1177/1479972311407218
50. Keogh E, Mark Williams E. Managing malnutrition in COPD: a review. Respir Med. 2021;176:106248. doi:10.1016/j.rmed.2020.106248
51. Martinez CH, Diaz AA, Meldrum CA, et al. Handgrip strength in chronic obstructive pulmonary disease. Associations with acute exacerbations and body composition. Ann Am Thorac Soc. 2017;14(11):1638–1645.
52. Marco E, Sánchez-Rodríguez D, Dávalos-Yerovi VN, et al. Malnutrition according to ESPEN consensus predicts hospitalizations and long-term mortality in rehabilitation patients with stable chronic obstructive pulmonary disease. Clin Nutr. 2019;38(5):2180–2186. doi:10.1016/j.clnu.2018.09.014
53. Beek LT, van der Vaart H, Wempe JB, et al. Coexistence of malnutrition, frailty, physical frailty and disability in patients with COPD starting a pulmonary rehabilitation program. Clin Nutr. 2020;39(8):2557–2563. doi:10.1016/j.clnu.2019.11.016
54. Cvejic L, Bardin PG. Swallow and aspiration in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2018;198(9):1122–1129. doi:10.1164/rccm.201804-0704PP
55. Bauer CMT, Morissette MC, Stampfli MR. The influence of cigarette smoking on viral infections: translating bench science to impact COPD pathogenesis and acute exacerbations of COPD clinically. Chest. 2013;143(1):196–206. doi:10.1378/chest.12-0930
56. Mehta H, Nazzal K, Sadikot RT. Cigarette smoking and innate immunity. Inflammation Res. 2008;57(11):497–503. doi:10.1007/s00011-008-8078-6
57. Johnston S, Molyneaux P, Singanayagam A, Beasley, Joshi, Mallia P. Lung microbiology and exacerbations in COPD. Int J Chronic Obstr. 2012;555. doi:10.2147/COPD.S28286
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.