Back to Journals » Risk Management and Healthcare Policy » Volume 19
Risk Factors and Development of a Risk Prediction Model for PICC-Related Thrombosis in Radiotherapy Inpatients: A Single-Center Retrospective Cohort Study
Authors Lin QM, Guo QL, Lin ZB, Chen AY, Chen Z, Zhang QY, Chen LY, Lin BH
Received 17 March 2026
Accepted for publication 20 May 2026
Published 12 June 2026 Volume 2026:19 608590
DOI https://doi.org/10.2147/RMHP.S608590
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gulsum Kaya
Qin-Mei Lin,1,* Qin-Lin Guo,2,* Zhuang-Bin Lin,3 Ai-Ying Chen,2 Zhen Chen,4 Qiu-Yan Zhang,2 Li-Yuan Chen,4 Bi-Hua Lin2
1Department of Outpatient Nursing, Fujian Medical University Union Hospital, Fuzhou, Fujian, 350001, People’s Republic of China; 2Department of Radiation Oncology Nursing, Fujian Medical University Union Hospital, Fuzhou, Fujian, 350001, People’s Republic of China; 3Department of Radiation Oncology, Fujian Medical University Union Hospital, Fuzhou, Fujian, 350001, People’s Republic of China; 4Department of Vascular Access, Fujian Medical University Union Hospital, Fuzhou, Fujian, 350001, People’s Republic of China
*These authors contributed equally to this study
Correspondence: Bi-Hua Lin, Department of Radiation Oncology Nursing, Fujian Medical University Union Hospital, No. 29 of Xinquan Road, Gulou District, Fuzhou, Fujian, 350001, People’s Republic of China, Tel +86-13799325903, Email [email protected]
Objective: This study aimed to identify independent risk factors associated with peripherally inserted central catheter-related venous thrombosis (PICC-RVT) in patients undergoing radiotherapy and to develop a risk prediction model to support early identification and inform targeted preventive strategies.
Methods: A single-center retrospective cohort study was conducted involving 335 patients with malignant tumors who underwent PICC placement in the Department of Radiotherapy Oncology between August 2023 and September 2024. Participants were randomly assigned to a modeling group (n = 250) and a validation group (n = 85) in a 3:1 ratio. Univariate analyses were conducted to identify potential risk factors, followed by multivariate logistic regression to determine independent predictors. A risk prediction model was subsequently constructed, and its performance was assessed using receiver operating characteristic (ROC) curve analysis.
Results: Of the 335 patients who underwent ultrasound examination, 70 were found to have thrombosis, yielding a PICC-related thrombosis incidence of 20.89% (70/335). Of these, 5 cases (7.14%) were symptomatic and 65 (92.86%) were asymptomatic. Univariate analysis indicated significant associations between thrombosis and both disease diagnosis (p = 0.007) and total cumulative radiation dose (p = 0.049). Multivariate logistic regression identified total cumulative radiation dose (odds ratio = 1.020, 95% confidence interval: 0.962– 0.999) and a history of thrombosis (odds ratio = 6.838, 95% confidence interval: 1.084– 43.157) as independent risk factors. The area under the ROC curve was 0.589 in the modeling group and 0.591 in the validation group. Sensitivity values were 74.5% and 83.3%, respectively; however, specificity remained limited (43.9% in the modeling group and 39.4% in the validation group).
Conclusion: The predictive model identified total cumulative radiation dose and a prior history of thrombosis as independent risk factors for PICC-RVT in patients receiving radiotherapy. However, the model’s specificity was low, restricting its utility to preliminary screening. Future studies with larger sample sizes and multicenter validation are needed to optimize the model and improve its predictive performance.
Keywords: influencing factors, PICC-related thrombosis, prediction models, radiotherapy
Introduction
Peripherally inserted central catheters have become the preferred modality for intravenous access among patients undergoing chemoradiotherapy, particularly in the referenced institution, owing to their ease of insertion, favorable safety profile, extended dwell time, ease of maintenance, minimal discomfort, and low infection rates.1–3 Despite these advantages, numerous studies have reported that the overall incidence of peripherally inserted central catheter (PICC)-related complications remains high, ranging from 30% to 40%, with PICC-related venous thrombosis (PICC-RVT) representing one of the most frequent and severe complications. Reported incidence rates for PICC-RVT vary widely from 1.9% to 71.9%.4–8 This condition frequently necessitates unplanned catheter removal, potentially disrupting treatment regimens and contributing to increased healthcare costs.3,9,10
External Beam Radiation Therapy is widespread applied in the treatment of malignant tumors. Radiotherapy has been identified as a contributing factor to the increased risk of PICC-RVT in patients with malignancies.11 However, the inclusion of radiotherapy variables in existing risk prediction models remains controversial, with inconsistent conclusions across studies regarding its statistical significance. For example, in the PICC-RVT risk scoring model developed by Huguet et al12 for outpatients undergoing chemotherapy, radiotherapy was not retained as a significant predictor. In contrast, Liang et al13 reported that, among patients with nasopharyngeal carcinoma receiving radiotherapy, symptomatic PICC-RVT was significantly associated with poorer survival outcomes. These discrepancies suggest that the pro-thrombotic effects of radiotherapy may be context-dependent, influenced by treatment regimen, tumor type, and the extent of vascular exposure.
As a localized cancer treatment modality, radiotherapy is distinguished by its ability to preserve surrounding healthy tissue and maintain organ function, thereby enhancing patient quality of life when compared to other therapeutic approaches.14 The mechanism underlying the increased thrombotic risk may involve a synergistic interaction between radiotherapy-induced endothelial cell activation and endothelial damage associated with PICC placement, ultimately triggering local activation of the coagulation cascade.15 Although the longitudinal studies by Song et al16 and Hu et al17 advanced our understanding of the dynamic risk factors for thrombosis in cancer patients, their models did not specifically examine radiotherapy parameters or the temporal relationship between radiotherapy and PICC placement.
The development of PICC-RVT can disrupt therapeutic continuity, extend hospitalization, increase economic burden, and necessitate modifications of the therapeutic plan. Effective management of PICC-RVT necessitates early identification of patients at risk, followed by stratified and individualized preventive strategies. Although asymptomatic thrombosis may not immediately produce clinical symptoms, existing studies have shown that it is significantly associated with an increased risk of delayed pulmonary embolism, catheter dysfunction, and treatment interruption.18 However, early prediction tools specifically targeting asymptomatic thrombosis in patients undergoing radiotherapy are still lacking.
In recent years, an increasing number of researchers worldwide have developed risk prediction models specifically for PICC-RVT. Known risk factors include disease stage, treatment modalities, and laboratory parameters such as D-dimer and platelet count.1,19–27 Existing assessment tools, such as the Michigan Risk Score, can be applied to general patient populations; however, studies focusing on risk prediction models for PICC-RVT among hospitalized patients receiving radiotherapy remain scarce. This model is intended to provide an evidence-based foundation for PICC-RVT prevention in radiotherapy, support clinical decision-making, and facilitate early identification of patients at high-risk. Its application holds potential to enable timely intervention, reduce patient suffering, mitigate disease burden, and optimize healthcare resource allocation.
Participants and Methods
Research Participants
Patients admitted to the Department of Radiation Oncology at the study institution between August 2023 and September 2024 who underwent PICC placement were selected as research participants. PICC insertion was performed by personnel from the institution’s PICC Vascular Access Center. To minimize radiation-induced endothelial injury to the catheterized vessels, the upper limb contralateral to the radiotherapy field was selected for PICC placement, and all catheterizations conducted via the basilic vein of the upper limb. Maintenance procedures were implemented in accordance with the revised standards of the PICC Maintenance Operation Technique issued by the Nursing Department. Dressing changes were performed weekly, and maintenance procedures were carried out by nursing staff with a minimum of three years of experience in the radiotherapy department. All patients received radiotherapy according to a standardized fractionation protocol consisting of 2 Gy per fraction in a 5+2 schedule (five consecutive treatment sessions per week from Monday to Friday, followed by a 2-day weekend break), with all patients completing the full prescribed course of radiotherapy.
Ethical approval for this study was granted by the Ethics Committee of Fujian Medical University Union Hospital (ethics number: 2023KY147).
Inclusion criteria were as follows:
(1) Diagnosis of malignant tumor and receipt of radiotherapy at the study institution; (2) Age ≥ 18 years; (3) Placement of a non-pressure-resistant single-lumen PICC in the upper arm under B-ultrasound guidance (the upper limb contralateral to radiotherapy); (4) Completion of radiotherapy and PICC maintenance within the institution; (5) Provision of informed consent by participants and / or their families.
Exclusion criteria were as follows:
(1) Inability to complete continuous in-hospital PICC maintenance during the catheterization period; (2) Initiation of anticoagulant therapy following catheter placement; (3) Presence of severe systemic infection; (4) Coexisting severe medical conditions or an estimated life expectancy of less than one month.
Elimination criteria were defined as: (1) Death during treatment due to disease progression; (2) Failure to complete the radiotherapy regimen; (3) Incomplete or missing clinical or procedural data.
All patients included in the study had a PICC inserted within 24 hours prior to radiotherapy, and no new PICCs were placed once radiotherapy had commenced.
Investigation Methods
A retrospective survey design was employed in this study. An information questionnaire for PICC catheterization in hospitalized patients receiving radiotherapy was developed based on a review of relevant literature, as well as existing domestic and international guidelines, policies, and standards. The questionnaire was constructed using the Delphi expert consultation method. The final questionnaire comprised four sections.
Part 1 collected general demographic and clinical information. Part 2 focused on basic clinical and treatment-related factors, encompassing 15 items including tumor staging, radiotherapy parameters (radiotherapy modality and total cumulative radiation dose, defined as the overall radiation dose delivered across the entire treatment course), comorbidities, underlying medical history, and treatment characteristics. Part 3 included seven hematologic indicators, all were based on the most recent blood test report obtained within 7 days prior to the Doppler ultrasound examination, such as D-dimer levels, platelet count, white blood cell count, and coagulation parameters. Part 4 focused on PICC-related variables, comprising three items: catheter model, insertion length, and tip position.
To ensure data validity, all questionnaires were collected on-site and reviewed for completeness. Any case with missing data was directly excluded from the study. A total of 25 potential risk factors were included in the analysis. According to the requirements for statistical variable analysis—specifically, a minimum sample size of at least ten times the number of independent variables—a minimum of 250 cases was deemed necessary. Ultimately, 335 eligible participants were included and randomly assigned to a model development group and a validation group at a 3:1 ratio.
Only cases with complete data across all variables were included in the analysis. Missing data were handled using complete-case analysis.
Outcome Indicators
The primary outcome was the occurrence of PICC-RVT, as confirmed by color Doppler flow imaging. Thrombus formation was classified into the following categories:1
(1) Venous wall thrombosis; (2) Fibrous sheath thrombus adherent to the external surface of the catheter; (3) Mixed thrombosis, characterized by both venous wall thrombosis and a fibrous sheath thrombus attached to the catheter surface. Ultrasound examinations were performed using two approaches: ① Routine standardized screening: all enrolled patients underwent Doppler ultrasonography before PICC removal at the end of treatment to assess the presence of venous thrombosis. ② Symptom-triggered screening: if patients developed clinical signs suggestive of thrombosis at the catheter insertion site, such as redness, swelling, pain, or increased skin temperature, an urgent Doppler ultrasound examination was performed immediately to determine whether PICC-related venous thrombosis had occurred.
Quality Control
Data Collection
The questionnaire design, data collection procedures, and database construction were conducted under the guidance of a professional intravenous therapy nurse from the Department of Radiotherapy. All personnel involved in case screening, case review, and database development received standardized training.
Data Collation and Entry
Double data entry was performed using EpiData 3.1. Logical constraints and valid value ranges were predefined to enable the detection of interval and logical errors within the dataset, thereby enhancing the accuracy of data entry.
Privacy Protection
Strict confidentiality measures were implemented to safeguard participant information. These measures were intended to reduce psychological stress and promote cooperation among participants, contributing to the comprehensiveness and reliability of the collected data.
Quality Control of Ultrasound Diagnosis
All thrombosis assessments using color Doppler ultrasound were independently performed by two experienced radiologists, each with ≥5 years of experience in vascular ultrasound. In cases of disagreement, a third senior radiologist served as an arbitrator.
Statistical Methods
Data analysis was conducted using SPSS 26.0 and MedCalc software. Participants were assigned to either the model development group or the validation group in a 3:1 ratio based on the timing of catheterization. Variables potentially influencing the occurrence of PICC-RVT were treated as independent variables, while the presence of thrombosis served as the dependent variable. Univariate analyses were conducted to assess associations between each factor and the occurrence of PICC-RVT.
Multivariate logistic regression analysis was subsequently applied to variables demonstrating statistically significant associations in the univariate analysis to identify independent risk factors associated with PICC-RVT in patients receiving radiotherapy. Model performance was assessed in both the development and validation groups.
Results
Basic Information
A total of 367 cases who met the inclusion criteria were collected, of whom 32 (8.72%) were excluded due to missing variable data, leaving 335 cases for analysis. To ensure objectivity and minimize selection bias, participants were randomly assigned to the modeling group (n = 250) or the validation group (n = 85) using a digital random generator. Cases were ranked by their assigned random numbers, with the first 250 allocated to the modeling group and the remaining 85 to the validation group.
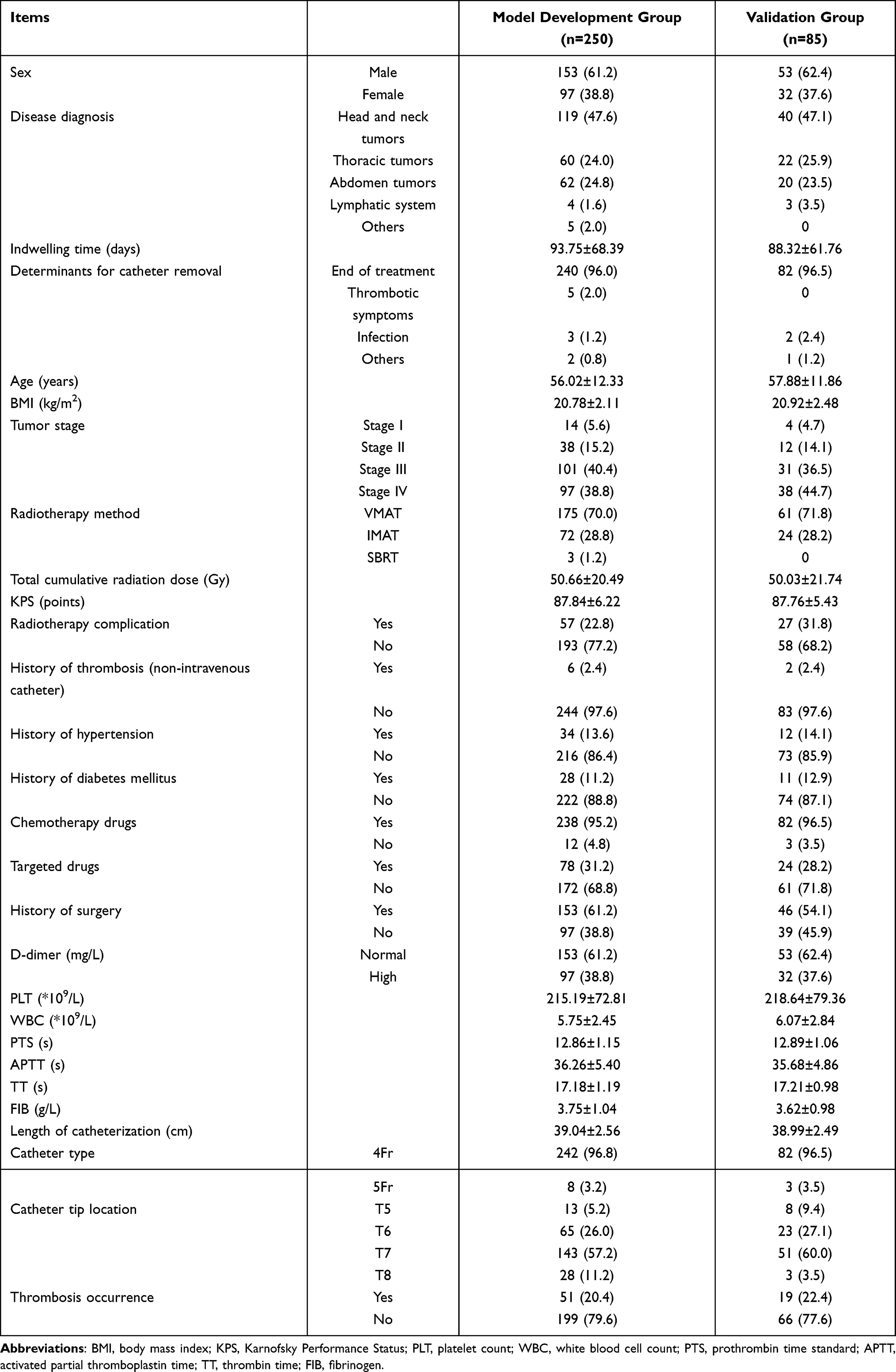
The presence of PICC-RVT was confirmed by color Doppler ultrasound in 70 participants—55 cases (78.57%) in the modeling group and 15 cases (21.43%) in the validation group—yielding an overall incidence rate of 20.89% among hospitalized individuals undergoing radiotherapy. Of these, 5 cases (7.14%) were classified as symptomatic thrombosis, while 65 cases (92.86%) were asymptomatic. The detailed general characteristics of the participants are presented in Table 1.
 |

Univariate Analysis of Risk Factors for PICC-Related Thrombosis
Univariate analysis was conducted on 25 variables potentially associated with the risk of PICC-RVT among the 250 participants in the model development group. The results indicated that disease diagnosis (p = 0.007) and total cumulative radiation dose (p = 0.049) were significantly associated with the occurrence of thrombosis. Detailed results are presented in Table 2.
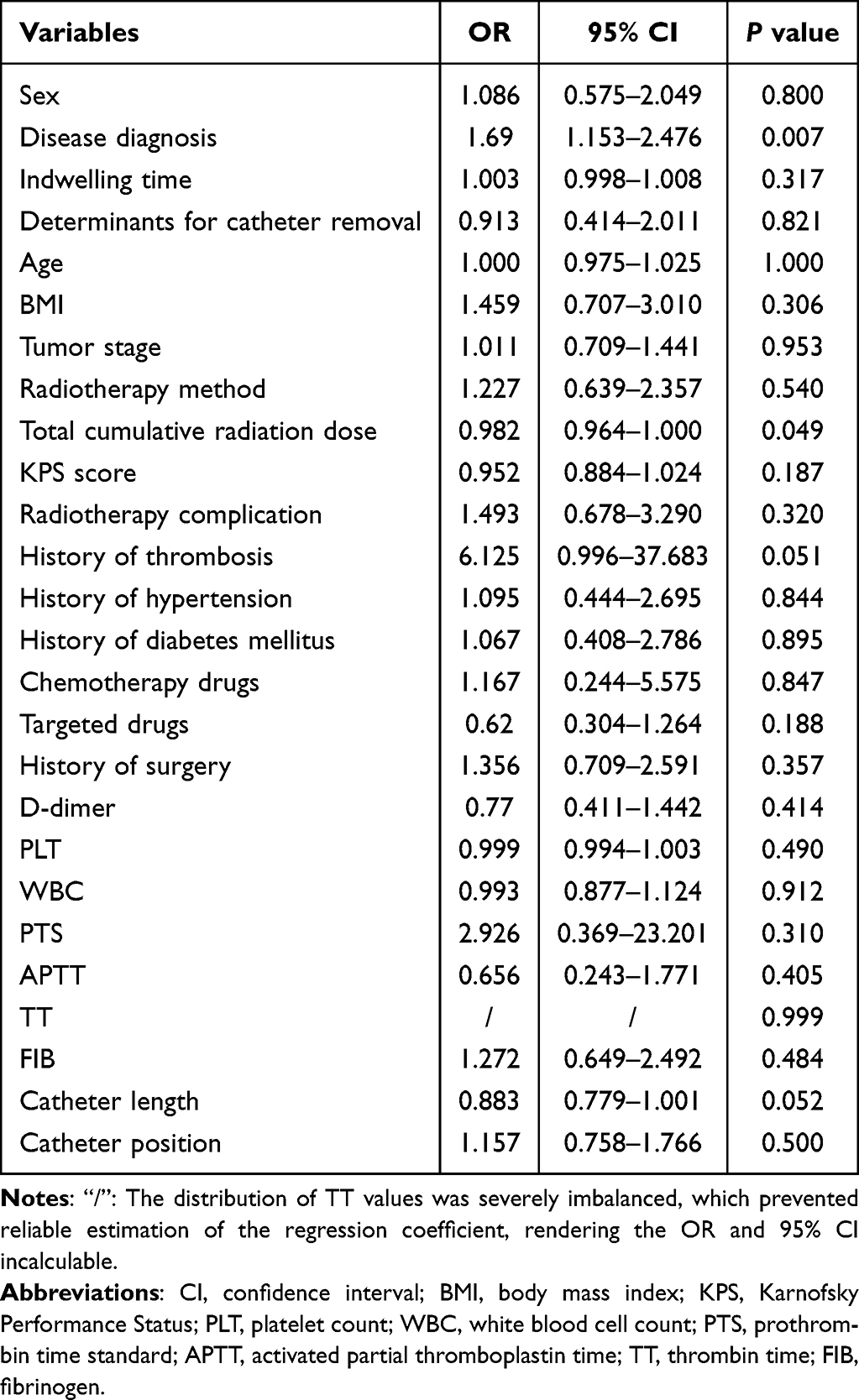 |
Table 2 Univariate Analysis of Risk Factors for PICC-RVT in the Model Development Group |
Logistic Regression Analysis of Risk Factors for PICC-Related Thrombosis
Logistic regression analysis was conducted using variables with a P-value less than 0.2 in the univariate analysis. These variables included catheter length, total cumulative radiation dose, Karnofsky Performance Status, history of thrombosis, targeted therapy, and disease diagnosis. Prior to inclusion, multicollinearity diagnostics were performed. All variables demonstrated a tolerance value ≥ 0.1 and a variance inflation factor ≤ 10, indicating the absence of significant collinearity; thus, all variables were retained for analysis. Detailed results are presented in Table 3.
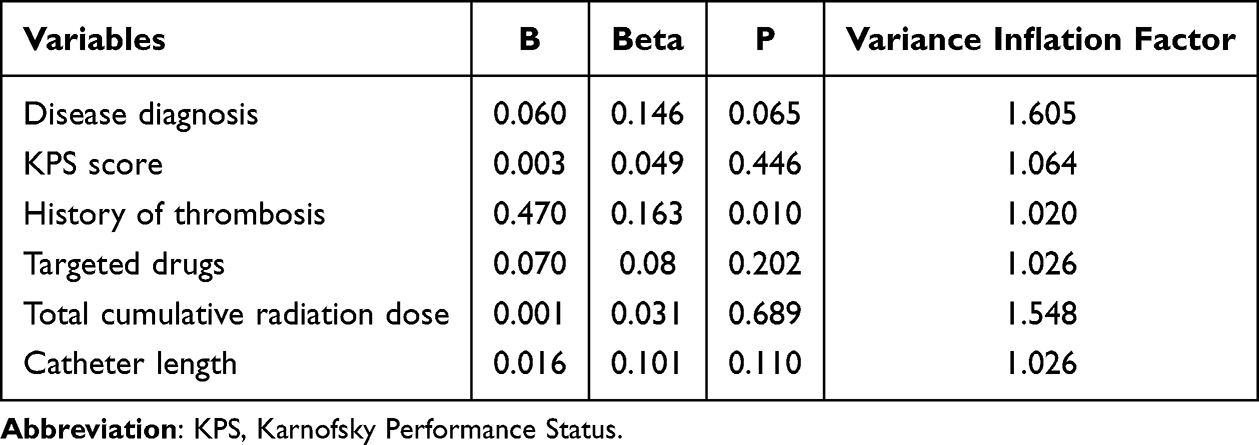 |
Table 3 Multicollinearity Analysis |
Subsequent multivariate logistic regression analysis indicated that total cumulative radiation dose was independently associated with an increased risk of PICC-related thrombosis (OR = 0.980, 95% CI: 0.962–0.999, p < 0.05), indicating that higher total cumulative radiation dose may elevate thrombosis risk following PICC placement. Additionally, a history of thrombosis emerged as a significant independent predictor, indicating the need for intensified surveillance in individuals with prior thrombotic events. Detailed results are provided in Table 4.
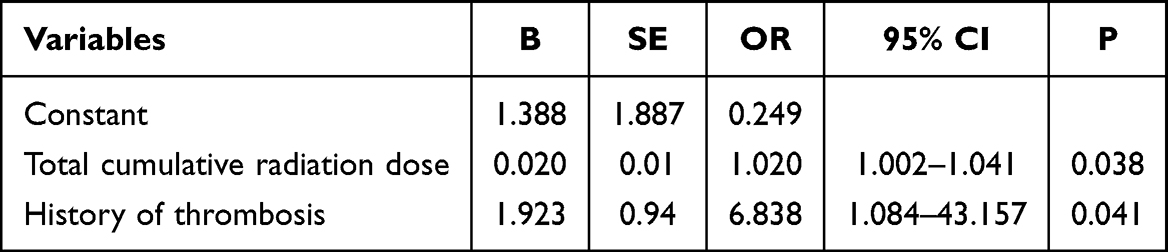 |
Table 4 Multivariate Logistic Regression Analysis of PICC-RVT Risk Factors |
Construction and Validation of PICC-Related Thrombosis Risk Prediction Model
The risk prediction model developed in this study incorporated two variables identified as independent predictors: total cumulative radiation dose and prior history of thrombosis. In the model development group, the area under the ROC curve (AUC) was 0.589, indicating poor overall discriminative ability and limited predictive performance. The model demonstrated a sensitivity of 0.745, correctly identifying approximately 74.5% of individuals who developed thrombosis. However, the specificity was 0.439, reflecting limited accuracy in identifying patients without thrombosis, with only 43.9% of non-thrombotic cases correctly classified (Figure 1).
 |
Figure 1 ROC Curve for Training Data. |
In the validation group, the model yielded as AUC of 0.591, which similarly falls below an acceptable threshold for clinical discrimination. Sensitivity improved to 0.833, allowing for correct identification of approximately 83.3% of patients with thrombosis. Conversely, specificity further declined to 0.394, with only 39.4% of non-thrombotic cases accurately identified (Figure 2).
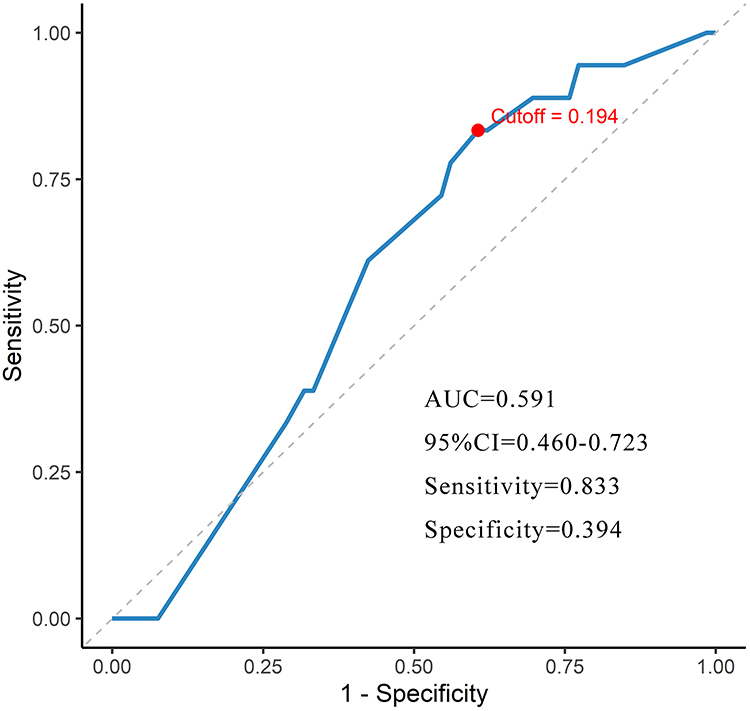 |
Figure 2 ROC Curve for Testing Data. |
The optimal cut-off values were determined by maximizing the Youden index. For the training set, the Youden index was 0.18, while for the testing set, it was 0.23, further confirming the model’s limited discriminative ability across both datasets.
Discussion
Currently, most studies on PICC-RVT have focused on populations with malignancies, critically ill individuals, and older adults. However, research specifically addressing the incidence and risk factors of PICC-RVT during radiotherapy remains limited. The investigation of associations between radiotherapy-related factors and PICC-RVT risk represents a novel contribution to the field of radiotherapy nursing, highlighting the need for increased attention to PICC safety management in this context.
In the present study, univariate and multivariate analyses were employed to examine factors associated with the development of PICC-RVT, and a corresponding risk prediction model was constructed. The findings identified disease diagnosis, total cumulative radiation dose, and a history of thrombosis as significant risk factors for PICC-RVT. The constructed model demonstrated an area under the curve (AUC) of 0.591, indicating limited but potentially useful predictive capability for early clinical risk identification. However, further refinement of the model is warranted to improve its predictive performance.
High-Dose Radiotherapy May Increase the Risk of PICC-RVT Formation
In the present study, a significant association was observed between total cumulative radiation dose and the risk of developing PICC-RVT (OR = 1.020, 95% CI: [1.002, 1.041], p = 0.038). Notably, this finding differs from the conclusions of a meta-analysis conducted by Ma et al, which reported no significant association between radiotherapy and the development of PICC-RVT in individuals with malignancies.28
From a pathophysiological standpoint, increasing total cumulative radiation dose may lead to progressive damage to vascular endothelial cells. Radiotherapy is known to induce inflammatory responses in these cells, thereby impairing their anticoagulant functions and promoting the release of procoagulant substances.29,30 This process can result in a hypercoagulable state, which, upon reaching a certain threshold of total radiation dose accumulation, may increase the risk of thrombosis.
The findings of this study hold potential clinical relevance. When planning radiotherapy regimens, especially those involving high-dose protocols, it may be prudent to evaluate thrombosis risk more carefully. In patients anticipated to receive high-dose radiotherapy, consideration should be given to prophylactic measures like anticoagulant therapy and routine vascular ultrasonography.
This study preliminarily analyzed the association between radiotherapy techniques (including VMAT, IMRT, and SBRT) and PICC-RVT; however, univariate analysis showed no statistically significant difference (p = 0.21). Possible explanations include: (1) Technique homogeneity: All patients received image-guided precision radiotherapy, resulting in minimal differences in target dose distribution between techniques. (2) Sample size limitation: SBRT cases accounted for only 12% of the cohort (40/335), limiting the statistical power of subgroup analyses. (3) Dose-dominant effect: Thrombosis risk appears to depend more on cumulative radiation dose (Gy) rather than the type of technique (eg, VMAT vs. IMRT). Consequently, the final predictive model retained cumulative dose rather than radiotherapy technique as a predictor. Future research should explore the impact of varying radiotherapy techniques and dose fractionation schemes on PICC-RVT risk. Although this study contributes to the understanding of PICC-RVT risk assessment during radiotherapy, additional investigations are necessary to further elucidate this complex relationship and to support the development of more precise prevention and treatment strategies in clinical practice.
Prior Thrombosis History as a Significant Risk Factor for PICC-RVT
Multivariate analysis in this study indicated that a prior history of thrombosis was associated with a nearly seven-fold increase in the risk of PICC-RVT (OR = 6.838, 95% CI: [1.084, 43.157]). This finding holds significant implications for clinical decision-making and preventive strategies. This finding aligns with the 2020 guidelines issued by the American Society of Hematology, which recognize a previous thrombotic event as an independent risk factor for catheter-related thrombosis.31
It has been demonstrated that endothelial cell activation induced by radiotherapy may act synergistically with PICC-related endothelial damage, resulting in localized activation of the coagulation cascade.14 Xie et al reported that concurrent chemoradiotherapy influences the development of PICC-RVT in individuals with malignant tumors, and that the duration of such therapy exerts varying effects on thrombosis formation.11
These findings offer practical guidance for clinical decision-making. In patients undergoing radiotherapy with a prior history of thrombosis, careful consideration should be given to both the indication for PICC placement and the management of catheter-related care. A thorough pre-catheterization assessment of thrombosis risk is essential. Where PICC insertion is deemed necessary, individualized catheter management plans should be implemented, including close post-insertion monitoring of coagulation parameters. In select high-risk individuals, prophylactic anticoagulation may be considered, balancing the benefits against potential bleeding risks. Additionally, health education should be reinforced to ensure awareness of thrombosis-related risks and facilitate early detection and timely intervention.
Clinical Value and Limitations of the Prediction Model
The risk prediction model developed in this study demonstrated an AUC of 0.591, indicating limited overall discriminative ability, with high sensitivity but limited specificity. This finding indicates that the model may be more appropriate as a preliminary screening tool rather than a definitive diagnostic method. Although the AUC was 0.589, its potential clinical relevance warrants contextual interpretation. PICC-RVT in the setting of radiotherapy often presents with subtle or nonspecific clinical manifestations, and its development may be influenced by treatment-specific factors not captured by conventional thrombosis risk assessment tools, such as the Caprini scale.
The sensitivity of 0.745 observed in this model may provide some reference value for the preliminary screening of high-risk populations; however, it does not confer a distinct clinical advantage and should be considered only as an auxiliary screening tool. The inclusion of radiotherapy-specific parameters—such as the anatomical relationship between the irradiation field and catheter trajectory, or biomarkers indicative of radiation-induced inflammation—may enhance the model’s predictive value and differentiate it from conventional assessment tools.
However, the AUC value of 0.589 reflects only marginal discriminative ability. This limitation may stem from both methodological and clinical factors. From a methodological perspective, the pathogenesis of thrombosis in radiotherapy settings involves complex radiobiological mechanisms, including vascular endothelial injury and hemorheological changes, and systemic hypercoagulability associated with malignancy. Current models may not fully account for these multifactorial processes. Previous research has demonstrated that the tumor-secreted chemokine CXCL13 can activate pulmonary mesenchymal macrophages, leading to the release of small extracellular vesicles containing integrin β2, which subsequently contribute to thrombus formation.32
At the clinical level, dynamic variations occurring over the course of radiotherapy—such as changes in cumulative fractionated dose or adjustments in concurrent chemotherapy regimens—may introduce risk fluctuations that exceed the predictive capacity of static models. Despite this, the relatively high sensitivity (0.745) retains clinical significance. For patients receiving radiotherapy to the head, neck, or thoracic regions, overlap between the PICC catheter tip and the radiation field may substantially increase thrombosis risk. The model provides only limited screening value and cannot directly guide clinical treatment decisions; it should be used solely as an auxiliary reference for clinical consideration: (1) modification of catheter pathway planning; (2) increased frequency of hemodynamic monitoring in high-risk patients; and (3) evaluation of the risk-benefit balance for early initiation of prophylactic anticoagulation. This approach may be particularly valuable in immunocompromised individuals, in whom invasive diagnostic procedures carry greater risk, and stratified risk management is essential.
Several limitations of the current model should be acknowledged. The model showed modest discriminative ability and limited clinical utility, with incremental value that remains to be established. In comparison with other predictive models, such as those developed by Chen et al33 which reported an AUC of 0.876 (95% CI: 0.818–0.925) with more balanced sensitivity and specificity, the present model demonstrated inferior performance. Additionally, previous studies have demonstrated the potential of machine learning algorithms to enhance predictive accuracy for PICC-RVT, suggesting a promising avenue for future model improvements.34,35
The relatively low AUC of our model may be attributable to several methodological and clinical factors that limited its discriminative ability: (1) Limited predictor variables: Our model included only two final predictors (radiotherapy dose and history of thrombosis), whereas high-performance models typically incorporate 5–8 variables. (2) Single-center design limitations: All patients were recruited from a single hospital, potentially restricting generalizability. Standardized PICC insertion and maintenance protocols may have reduced variability commonly observed in multicenter studies. Additionally, the sample size was relatively small (n = 335), whereas some machine learning studies often include >1000 cases. (3) Radiotherapy-specific challenges: Conventional predictors may not fully capture the complex radiobiological mechanisms underlying radiation-induced thrombosis. Interactions between radiation effects and catheter-related factors may require more sophisticated modeling approaches. (4) Data collection constraints: Most predictors were derived from static observational data and did not reflect the dynamic evolution of thrombosis risk during radiotherapy. High-performance models often utilize real-time imaging or continuous monitoring data, which were unavailable in our dataset.
Although the predictive performance of our model has certain limitations compared with some existing methods, it may provide directions for model improvement and lays a foundation for the development of more precise, radiotherapy-specific predictive tools. Modeling PICC-RVT risk in the context of radiotherapy presents unique challenges, particularly the dynamic biological effects of radiation and their interactions with catheter-related factors, which may require specialized modeling approaches beyond conventional thrombosis risk models.
Limitations
First, although a sufficient number of hospitalized patients undergoing radiotherapy were included in the study, the overall sample size remains relatively limited and may not sufficiently capture the full spectrum of potential contributing factors. A larger cohort may be more effective in detecting subtle associations and capturing complex relationships among risk factors for PICC-RVT. Second, the restriction of analysis to cases with complete data may have introduced selection bias. Cases with missing data may differ systematically from complete cases in key variables such as radiotherapy details, comorbidities, medical history, and treatment information, meaning that the analytical sample may not fully represent the target population and the generalizability of the findings may be limited. Future studies should consider more robust approaches to missing data, such as multiple imputation, to reduce the risk of bias and further validate the findings. Third, despite efforts to conduct a comprehensive analysis of influencing factors, certain key variables that could significantly impact the risk of PICC-RVT may have been omitted. Furthermore, complex interactions between various influencing factors may not have been fully investigated, potentially limiting the understanding of their combined effects on PICC-RVT risk. To address these limitations, future research should consider increasing sample size across multiple centers, incorporate more granular and dynamic clinical variables, and adopt advanced analytical methods capable of modeling complex variable interactions. Refinement of prediction models and validation across diverse clinical settings will be essential for improving their robustness, accuracy, and clinical utility.
Conclusion
This study analyzed the factors influencing PICC-RVT development and constructed a risk prediction model. The results indicated that disease diagnosis, cumulative radiotherapy dose, and a history of thrombosis are key risk factors for PICC-RVT. The predictive model achieved an AUC of 0.591, with limited discriminative ability characterized by high sensitivity but low specificity. Its clinical early-warning and practical utility are therefore also quite limited. Further optimization is needed to improve its applicability and overall performance. Potential improvements include incorporating radiotherapy-specific variables (eg, catheter–irradiation field overlap, dose fractionation) and conducting prospective multicenter validation to enhance model performance. Such efforts could improve the accuracy of PICC-RVT risk prediction and prevention in hospitalized patients receiving radiotherapy, ultimately providing better clinical care.
Abbreviations
PICC, Peripherally Inserted Central Catheter; PICC-RVT, Peripherally Inserted Central Catheter-Related Venous Thrombus; BMI, Body Mass Index; VMAT, Volumetric Modulated Arc Therapy; IMAT, Intensity-Modulated Arc Therapy; SBRT, Stereotactic Body Radiotherapy; PTS, Prothrombin time standard; APTT, Activated Partial Thromboplastin Time; TT, Thrombin Time; FIB, Fibrinogen.
Data Sharing Statement
All data generated or analysed during this study are included in this article. Further enquiries can be directed to the corresponding author.
Ethics Approval and Consent to Participate
This study was conducted with approval from the Ethics Committee of Fujian Medical University Union Hospital (ethics number: 2023KY147). This study was conducted in accordance with the declaration of Helsinki. All patients provided informed consent.
Acknowledgments
We would like to acknowledge the hard and dedicated work of all the staff that implemented the intervention and evaluation components of the study.
Funding
1. 2023 Special Nursing Research Project on Intravenous Therapy by the Chinese Journal of Nursing, No.: ZHHLZZS-202334; 2. Fujian Provincial Clinical Research Center for Radiation and Therapy of Digestive, Hematologic, and Breast Malignancies (2021Y007); 3. Fujian Provincial Key Clinical Specialty in Radiation Oncology; 4. Fujian Provincial Key Laboratory of Intelligent Imaging and Precision Radiotherapy for Oncology (2025YGPT005).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Song X, Lu H, Chen F, et al. A longitudinal observational retrospective study on risk factors and predictive model of PICC associated thrombosis in cancer patients. Sci Rep. 2020;10(1):10090. doi:10.1038/s41598-020-67038-x
2. Gorski LA, Hadaway L, Hagle ME, et al. Infusion therapy standards of practice, 8th edition. J Infus Nurs. 2021;44(1S Suppl 1):S1–13. doi:10.1097/NAN.0000000000000396
3. Chen Y, Chen H, Yang J, et al. Patterns and risk factors of peripherally inserted central venous catheter-related symptomatic thrombosis events in patients with malignant tumors receiving chemotherapy. J Vasc Surg Venous Lymphat Disord. 2020;8(6):919–929. doi:10.1016/j.jvsv.2020.01.010
4. Kang J, Chen W, Sun W, et al. Peripherally inserted central catheter-related complications in cancer patients: a prospective study of over 50,000 catheter days. J Vasc Access. 2017;18(2):153–157. doi:10.5301/jva.5000670
5. Al-Asadi O, Almusarhed M, Eldeeb H. Predictive risk factors of venous thromboembolism (VTE) associated with peripherally inserted central catheters (PICC) in ambulant solid cancer patients: retrospective single Centre cohort study. Thromb J. 2019;17(1):2. doi:10.1186/s12959-019-0191-y
6. Taxbro K, Hammarskjöld F, Thelin B, et al. Clinical impact of peripherally inserted central catheters vs implanted port catheters in patients with cancer: an open-label, randomised, two-centre trial. Br J Anaesth. 2019;122(6):734–741. doi:10.1016/j.bja.2019.01.038
7. Wang G, Li Y, Wu C, et al. The clinical features and related factors of PICC-related upper extremity asymptomatic venous thrombosis in cancer patients: a prospective study. Medicine. 2020;99(12):e19409. doi:10.1097/MD.0000000000019409
8. Itkin M, Mondshein JI, Stavropoulos SW, Shlansky-Goldberg RD, Soulen MC, Trerotola SO. Peripherally inserted central catheter thrombosis—reverse tapered versus nontapered catheters: a randomized controlled study. J Vasc Interv Radiol. 2014;25(1):85–91.e1. doi:10.1016/j.jvir.2013.10.009
9. Chopra V, Anand S, Krein SL, Chenoweth C, Saint S. Bloodstream infection, venous thrombosis, and peripherally inserted central catheters: reappraising the evidence. Am J Med. 2012;125(8):733–741. doi:10.1016/j.amjmed.2012.04.010
10. Marnejon T, Angelo D, Abu Abdou A, Gemmel D. Risk factors for upper extremity venous thrombosis associated with peripherally inserted central venous catheters. J Vasc Access. 2012;13(2):231–238. doi:10.5301/jva.5000039
11. Xie J, Xu L, Xu X, Huang Y. Complications of peripherally inserted central catheters in advanced cancer patients undergoing combined radiotherapy and chemotherapy. J Clin Nurs. 2017;26(23–24):4726–4733. doi:10.1111/jocn.13825
12. Huguet M, Morgades M, Fernández M, et al. A risk score for single-lumen peripherally inserted central catheter (PICC)-related venous thrombosis in cancer patients undergoing ambulatory chemotherapy. Blood. 2022;140(Suppl 1):8542–8543. doi:10.1182/blood-2022-165328
13. Liang YJ, Tang LQ, Sun XS, et al. Symptomatic venous thromboembolism associated with PICCs predicts worse survival in nasopharyngeal carcinoma. BMC Cancer. 2018;18(1):1297. doi:10.1186/s12885-018-5213-9
14. Chandra RA, Keane FK, Voncken FEM, Thomas CR. Contemporary radiotherapy: present and future. Lancet. 2021;398(10295):171–184. doi:10.1016/S0140-6736(21)00233-6
15. Verso M, Agnelli G, Kamphuisen PW, et al. Risk factors for upper limb deep vein thrombosis associated with the use of central vein catheter in cancer patients. Intern Emerg Med. 2008;3(2):117–122. PMID: 18317868. doi:10.1007/s11739-008-0125-3
16. Song X, Zhang Q, Wu D, et al. A longitudinal observational retrospective study on risk factors and predictive model of PICC-associated thrombosis in cancer patients. Sci Rep. 2020;10(1):10095. doi:10.1038/s41598-020-67068-5
17. Hu Z, Luo M, He R, et al. Development and validation of a risk prediction model for PICC-related venous thrombosis in patients with cancer: a prospective cohort study. Sci Rep. 2025;15(1):4654. doi:10.1038/s41598-025-89260-1
18. Wang TF, Kou R, Carrier M, Delluc A. Management of catheter-related upper extremity deep vein thrombosis in patients with cancer: a systematic review and meta-analysis. J Thromb Haemost. 2024;22(3):749–764. PMID: 38065528. doi:10.1016/j.jtha.2023.11.017
19. Gu S. Research on the risk prediction model of PICC associated thrombosis in cancer patients. Jiangsu university; 2019. Chinese. Available from: https://med.wanfangdata.com.cn/Paper/Detail?id=DegreePaper_D01871021&dbid=WF_XW.
20. Yang FY, Hua RY, Wu WY, et al. Establishment of risk predictive nomogram model of upper extremity venous thrombosis associated with peripherally venous inserted central catheter in cancer patients. Cancer Res Clin. 2020;32(7):456–461. doi:10.3760/cma.j.cn115355-20200221-00065
21. Tao L. Development of PICC related venous thrombosis risk assessment form for cancer patients. Hefei: Anhui Medical University; 2019. Chinese. Available from: https://med.wanfangdata.com.cn/Paper/Detail?id=DegreePaper_D01808247&dbid=WF_XW.
22. He YY. Construction of PICC related risk assessment model for upper limb venous thrombosis in patients with breast cancer undergoing chemotherapy. Bengbu: Bengbu Medical College; 2019. Chinese. Available from: https://med.wanfangdata.com.cn/Paper/Detail?id=DegreePaper_D01797615&dbid=WF_XW.
23. Chen JQ, Yan CS, Zhang J, Kang N, Hu F. Development and validation of a risk scoring model to predict peripherally inserted central catheter-related upper extremity venous thrombosis. J Nurs Sci. 2018;33(17):1–5. doi:10.3870/j.issn.1001-4152.2018.17.001
24. Tian X, Chen H, Song GM, Bian W, Liu XL, Chen WQ. Establishment of risk predictive model of venous thromboembolism associated with peripherally inserted central catheters among cancer patients based on meta-analysis. J Clin Patholog Res. 2017;37(4):772–778. doi:10.3978/j.issn.2095-6959.2017.04.021
25. Lin Y, Zeng Z, Lin R, Zheng J, Liu S, Gao X. The Caprini thrombosis risk model predicts the risk of peripherally inserted central catheter-related upper extremity venous thrombosis in patients with cancer. J Vasc Surg Venous Lymphat Disord. 2021;9(5):1151–1158. doi:10.1016/j.jvsv.2020.12.075
26. Ploton G, Brebion N, Guyomarch B, et al. Predictive factors of venous recanalization in upper-extremity vein thrombosis. PLoS One. 2021;16(5):e0251269. doi:10.1371/journal.pone.0251269
27. Herc E, Patel P, Washer LL, Conlon A, Flanders SA, Chopra V. A model to predict central-line-associated bloodstream infection among patients with peripherally inserted central catheters: the MPC score. Infect Control Hosp Epidemiol. 2017;38(10):1155–1166. doi:10.1017/ice.2017.167
28. Ma S, Shen C, Li Q, et al. Clinical factors of PICC-RVT in cancer patients: a meta-analysis. Support Care Cancer. 2023;31(7):393. doi:10.1007/s00520-023-07855-8
29. Chen F, Shen M, Zeng D, et al. Effect of radiation-induced endothelial cell injury on platelet regeneration by megakaryocytes. J Radiat Res. 2017;58(4):456–463. doi:10.1093/jrr/rrx015
30. Wijerathne H, Langston JC, Yang Q, et al. Mechanisms of radiation-induced endothelium damage: emerging models and technologies. Radiother Oncol. 2021;158:21–32. doi:10.1016/j.radonc.2021.02.007
31. Ortel TL, Neumann I, Ageno W, et al. American society of hematology 2020 guidelines for management of venous thromboembolism: treatment of deep vein thrombosis and pulmonary embolism. Blood Adv. 2020;4(19):4693–4738. doi:10.1182/bloodadvances.2020001830
32. Lucotti S, Ogitani Y, Kenific CM, et al. Extracellular vesicles from the lung pro-thrombotic niche drive cancer-associated thrombosis and metastasis via integrin beta 2. Cell. 2025;188(6):1642–1661.e24. doi:10.1016/j.cell.2025.01.025
33. Chen L, Lu Y, Wang L, Pan Y, Zhou X. Construction of a nomogram risk prediction model for PICC-related venous thrombosis and its application. Asian J Surg. 2024;47(1):107–111. doi:10.1016/j.asjsur.2023.05.043
34. Li Y, Nie S, Wang L, et al. Integrating deep learning in public health: a novel approach to PICC-RVT risk assessment. Front Public Health. 2025;12:1445425. doi:10.3389/fpubh.2024.1445425
35. Hu H, Wu Z, Zhao J. Peripherally inserted central-related upper extremity deep vein thrombosis and machine learning. Vascular. 2024;32(6):1346–1351. doi:10.1177/17085381241236543
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.