Back to Journals » Neuropsychiatric Disease and Treatment » Volume 16
Risk Factors and a Nomogram for Predicting Intracranial Hemorrhage in Stroke Patients Undergoing Thrombolysis
Authors Zhou Z, Yin X, Niu Q, Liang S ![]() , Mu C, Zhang Y
, Mu C, Zhang Y ![]()
Received 20 February 2020
Accepted for publication 20 April 2020
Published 11 May 2020 Volume 2020:16 Pages 1189—1197
DOI https://doi.org/10.2147/NDT.S250648
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yu-Ping Ning
Zheren Zhou,1,* Xiaoyan Yin,2,3,* Qiuwen Niu,2 Simin Liang,2,4 Chunying Mu,2 Yurong Zhang2
1University Hospital, Xi’an Jiaotong University, Xi’an, Shaanxi, People’s Republic of China; 2Department of Neurology, The First Affiliated Hospital of Xi’an Jiaotong University, Xi’an, Shaanxi, People’s Republic of China; 3Department of Neurology, Wuqi People’s Hospital, Yan’an, Shaanxi, People’s Republic of China; 4Department of Neurology, The First Affiliated Hospital of Xi’an Medical College, Xi’an, Shaanxi, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yurong Zhang Email [email protected]
Purpose: Identifying stroke patients at risk of postthrombolysis intracranial hemorrhage (ICH) in the clinical setting is essential. We aimed to develop and evaluate a nomogram for predicting the probability of ICH in acute ischemic stroke patients undergoing thrombolysis.
Patients and Methods: A retrospective observational study was conducted using data from 345 patients at a single center. The patients were randomly dichotomized into training (2/3; n=233) and validation (1/3; n=112) sets. A prediction model was developed by using a multivariable logistic regression analysis.
Results: The nomogram comprised three variables: the presence of atrial fibrillation (odds ratio [OR]: 4.92, 95% confidence interval [CI]: 2.09– 11.57), the National Institutes of Health Stroke Scale (NIHSS) score (OR: 1.11, 95% CI: 1.04– 1.18) and the glucose level on admission (OR: 1.27, 95% CI: 1.08– 1.50). The areas under the receiver operating characteristic curve of the nomogram for the training and validation sets were 0.828 (0.753– 0.903) and 0.801 (0.690– 0.911), respectively. The Hosmer–Lemeshow test revealed good calibration in both the training and validation sets (P = 0.509 and P = 0.342, respectively). The calibration plot also demonstrated good agreement. A decision curve analysis demonstrated that the nomogram was clinically useful.
Conclusion: We developed an easy-to-use nomogram model to predict ICH, and the nomogram may provide risk assessments for subsequent treatment in stroke patients undergoing thrombolysis.
Keywords: stroke, intracranial hemorrhage, thrombolysis, nomogram, prognosis
Introduction
Stroke is the second leading cause of death and a major cause of disability worldwide.1 Intravenous recombinant tissue plasminogen activator (r-tPA) treatment is an effective therapy for acute ischemic stroke.2 However, intracerebral hemorrhage (ICH), especially symptomatic ICH (sICH), is the main complication of thrombolytic therapy and may increase the risk of poor and fatal outcomes.3 The ICH occurrence rate after thrombolysis varies by ethnicity; it has been reported to be 2.12-fold higher in Asian than in non-Asian populations.4,5
The accurate identification of stroke patients at increased risk of future postthrombolysis ICH in the clinical setting is essential. Several prognostic scores have been applied to identify stroke patients with a high risk of postthrombolysis ICH.5–10 However, most of these scores for individualized outcome predictions are limited by the dichotomization/categorization of continuous variables such as age and the National Institutes of Health Stroke Scale (NIHSS) score; dichotomization does not make use of within-category information and leads to the loss of information.5,8-10 Furthermore, the predictive value of these scores varies among different studies.6,7,11
A nomogram is a graphical tool for determining the probability of a clinical event in an individual patient based on a statistical predictive model. Nomograms using continuous variables are better visual tools for predicting clinical outcomes than the afore mentioned scores. Meanwhile, they are more accurate than the conventional method using odds ratios (ORs).12 To the best of our knowledge, there have been only 2 scholarly works carried out on prognostic nomograms for ICH events in stroke patients undergoing thrombolysis.13,14 The STARTING-SICH nomogram was designed to predict ICH after intravenous thrombolysis for stroke in Italy,13 and another nomogram model was developed in Asia.14 Considering the external validation and ethnic differences, a scoring system specific to China is needed.
In this study, we aimed to develop a nomogram based on the integration of parameters to predict the probability of postthrombolysis ICH in Chinese acute ischemic stroke patients.
Patients and Methods
Study Population and Design
A retrospective cohort study was conducted at the stroke center of the First Affiliated Hospital of Xi’an Jiaotong University between April 2014 and July 2019. Inclusion criteria in the study were as follows: 1) age ≥18 years; 2) diagnosis of acute ischemic stroke confirmed by cranial computed tomography (CT) or magnetic resonance imaging (MRI) within 24 hours after admission; 3) onset-to-treatment time for thrombolysis <4.5 hours; and 4) written informed consent obtained from the patient or their legal representative. In agreement with the current guidelines, the exclusion criteria were as follows: 1) systolic BP >185 mmHg; 2) diastolic BP>110 mmHg; 3) blood glucose <50 or >400 mg/dL; 4) prestroke oral anticoagulants with an international normalized ratio (INR) >1.7; and 5) direct oral anticoagulants. In addition, patients treated with endovascular procedures after intravenous thrombolysis and those without complete data on all the variables included in the nomogram were excluded from the analysis.
Among 411 patients undergoing intravenous r-tPA treatment, we excluded 13 patients who had missing data at admission (3.2%) and 53 patients who underwent intra-arterial thrombolysis or intravenous r-tPA treatment combined with mechanical thrombectomy (12.9%). After these exclusions, 345 patients were included in the final analysis in the present study. Patient data were extracted from their medical charts. The study was conducted in accordance with the Declaration of Helsinki and was approved by the ethics committee for medical research at the First Affiliated Hospital of Xi’an Jiaotong University. Due to the retrospective nature of the study, the requirement of written informed consent was waived by the review board. Confidential patient information was deleted from the entire data set prior to analysis.
Baseline Data Collection
At the time of admission, detailed lists of demographic, clinical and laboratory information were obtained for each patient. The data collected included age, sex, obesity (body mass index ≥ 30 kg/m2), current smoking status, glucose level on admission, triglyceride (TG) level, low-density lipoprotein cholesterol (LDL-C) level, platelet (PLT) count, antiplatelet therapy before enrollment, systolic and diastolic blood pressures (BPs), NIHSS score on admission, symptom onset to treatment (ONT), histories of hypertension, diabetes mellitus and atrial fibrillation, etc.
Thrombolysis Method
All patients were treated with r-tPA within 4.5 hours of stroke onset. Intravenous r-tPA (alteplase, 0.9 mg/kg, 90 mg maximum) was used, with 10% of the total dose as a bolus, followed by a 60-minute infusion of the remaining dose.
Ascertainment of Intracranial Hemorrhage
On admission, all patients underwent a CT scan within the first 4.5 hours of stroke onset. The scan was repeated 24 hours after intravenous r-tPA administration, and another CT scan was performed immediately in cases of rapid neurological deterioration to evaluate the presence of ICH. Symptomatic ICH was defined as any type of ICH on any posttreatment imaging after the initiation of thrombolysis and an increase in the NIHSS score by 4 points from baseline or death; asymptomatic ICH was defined as any type of ICH on any posttreatment imaging after the initiation of thrombolysis but not accompanied by neurological deterioration (European Cooperative Acute Stroke Study II [ECASS II]).15
Statistical Analysis
A descriptive analysis was conducted, with continuous variables described as medians with interquartile ranges (IQRs) or as means with standard deviations (SDs) if the variables had a normal distribution. Categorical variables are presented as numbers with percentages.
To generate the nomogram for the training set, a multivariable logistic regression analysis was performed to predict the probability of ICH using a forward stepwise method that included all variables with a probability (P) value <0.20 in the univariable analysis. Variables with P values that were less than 0.05 in the multivariable logistic regression were entered into the prediction model. Finally, we calculated regression coefficients and ORs with two-sided 95% confidence intervals (CIs) for each of the variables included in the model.
For nomogram construction and validation, we randomly assigned 67% (233) of the patients to the training set and 33% (112) to the validation set using the Statistical Product and Service Solutions (SPSS) software described below. The predictive accuracy of the nomogram model was assessed by calculating the area under the receiver operating characteristic curve (AUC-ROC). Calibration of the nomogram model, defined as concordance between the predicted and observed probabilities, was established using the Hosmer–Lemeshow goodness-of-fit test (P > 0.05) and a calibration plot. The clinical value of the predictive model was tested using a decision curve analysis (DCA).
The statistical analysis was performed using SPSS version 22.0 (SPSSInc., Chicago, IL, USA), Stata version 13.0 (Stata Corporation, College Station, TX,USA), and the statistical software package R, version 3.5.3 (https://cran.r-project.org/). DeLong’s test was used to compare the AUC-ROC of each of the models, which were analyzed using MedCalc Version 18.2.1. Two-tailed significance values were applied, and statistical significance was defined as P < 0.05.
Results
Baseline Patient Characteristics
From 2004 to 2019, there were 411 patients treated with intravenous thrombolysis in our center. After the removal of patients who met the exclusion criteria (n=66, 16.1%), 345 remaining patients were eligible for analysis (Figure 1).
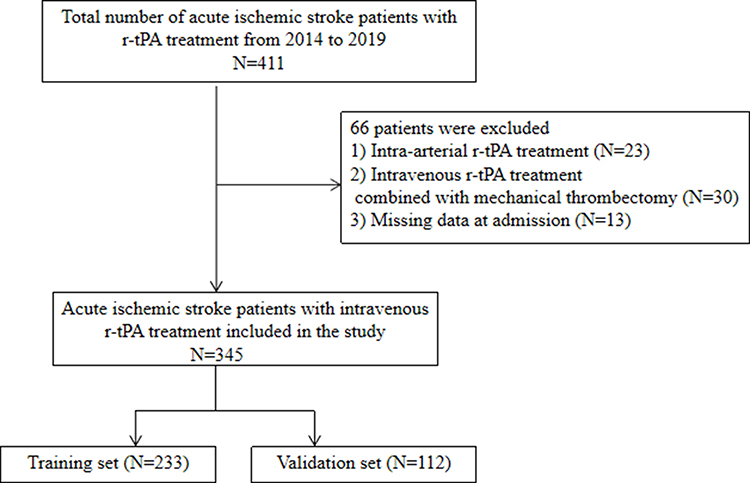 |
Figure 1 Flow diagram of the selection of eligible patients. |
The randomization process resulted in 233 and 112 patients with acute stroke undergoing thrombolysis being enrolled in the training and validation sets, respectively. The baseline characteristics of patients with and without ICH in the training and validation sets are shown in Table 1. The median age of the total group was 65 years (range, 27–93 years), and 67.2% of the patients were male. Of the 345 patients, 50 (14.5%) developed ICH. The proportion of ICH was 14.2% in the training set and 15.2% in the validation set. The ICH group was older and had higher baseline PLT and glucose levels, a greater baseline NIHSS score, and a higher frequency of atrial fibrillation and diabetes mellitus (Table 1).
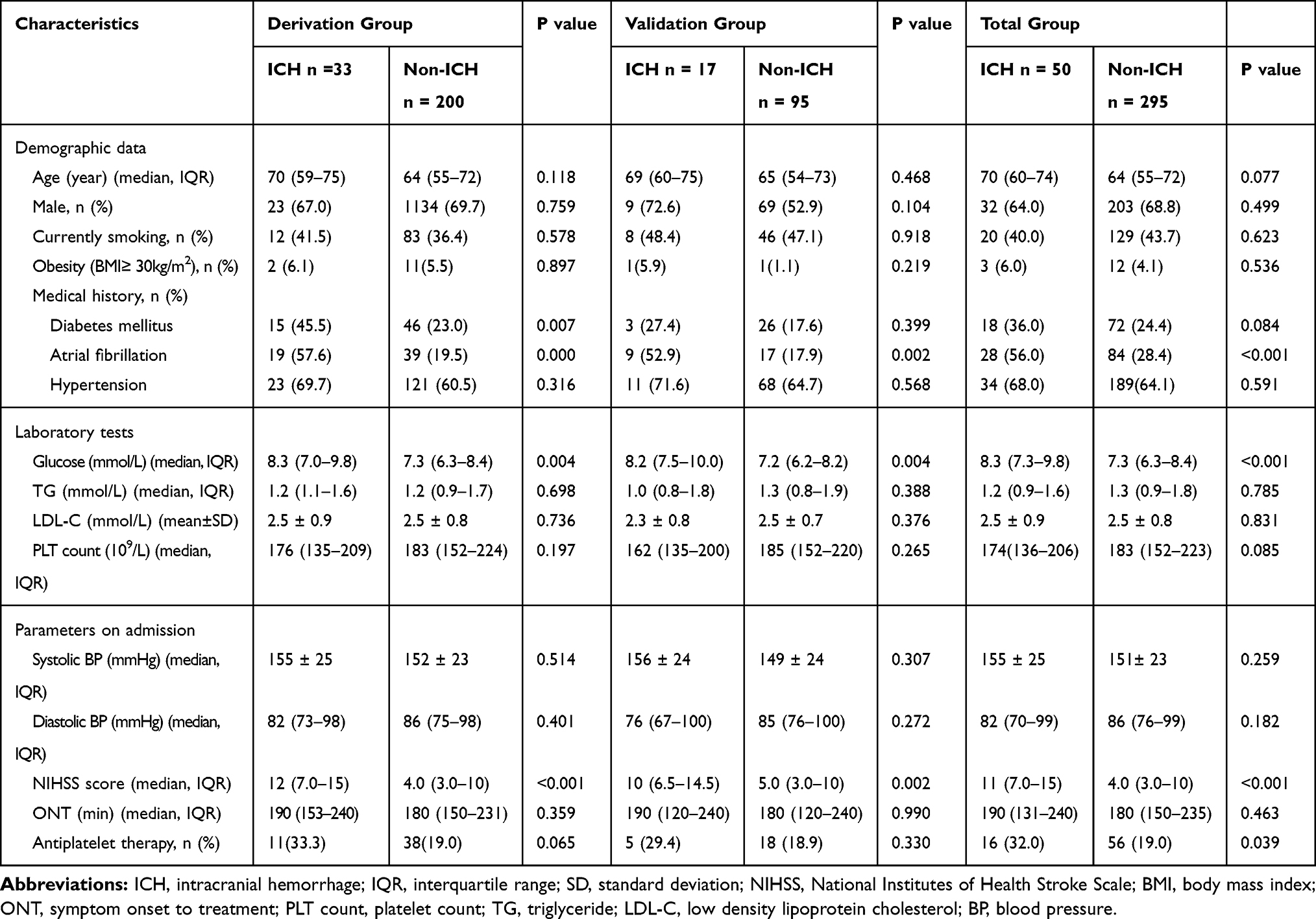 |
Table 1 Comparison of Baseline Characteristics Between ICH and Non-ICH Groups in the Training and Validation Groups |
Predictive Nomogram Development
The logistic regression results are shown in Table 2. The following three variables were entered into the predictive model based on the results of the stepwise regression: the presence of atrial fibrillation (OR:4.92, 95% CI: 2.09–11.57), NIHSS score (OR: 1.11, 95% CI: 1.04–1.18) and glucose level on admission (OR: 1.27, 95% CI: 1.08–1.50).
 |
Table 2 Associations of the Predictive Factors with Intracranial Hemorrhage |
The nomogram was developed by assigning a graphic initial score to each of the three independent prognostic factors, with a point range from 0 to 100. The scores for all variables were then summed to obtain the total score, and a vertical line was drawn from the total-points row to indicate the estimated probability of ICH being present (Figure 2). It was predicted that a higher total score in the nomogram was associated with a higher likelihood of ICH, while a lower total score was associated with a lower likelihood of ICH.
 |
Figure 2 Nomogram used for predicting postthrombolysis ICH after acute ischemic stroke in Chinese patients. The final score (ie, total points) is calculated as the sum of the individual score of each of the 3 variables included in the nomogram. Abbreviations: AF, atrial fibrillation; NIHSS, National Institutes of Health Stroke Scale; ICH, intracranial hemorrhage. |
Validation of the Nomogram
The AUC-ROC was used to validate the nomogram. The AUC-ROCs of the training set (Figure 3A) and the validation set (Figure 3B) were 0.828 (95% CI: 0.753–0.903) and 0.801 (95% CI: 0.690–0.911), respectively.
 |
Figure 3 ROC curve of the nomogram for predicting postthrombolysis ICH in stroke patients. (A) ROC curve in the training set; (B) ROC curve in the validation set. Abbreviations: AUC, area under the ROC curve; ROC, receiver operating characteristic; ICH, intracranial hemorrhage. |
The nomogram model was calibrated using the Hosmer–Lemeshow goodness-of-fit test and a calibration plot. The Hosmer–Lemeshow test revealed high concordance between the predicted and observed probabilities for both the training set (χ2 = 7.26, df = 8, P = 0.509) and the validation set (χ2 = 9.01, df = 8, P = 0.342). The calibration plot also showed good agreement between the predicted and observed outcomes for both the training set (Figure 4A) and the validation set (Figure 4B).
 |
Figure 4 Calibration curve of the nomogram for the training set (A) and the validation set (B). |
A DCA was applied to assess the clinical validity of the nomogram (Figure 5A and B). This corroborated the good clinical applicability of the nomogram in predicting ICH because the ranges of threshold probabilities were wide and practical for both the training and validation sets.
 |
Figure 5 Decision curve analysis for the training set (A) and the validation set (B). A horizontal line indicates that all samples are negative and not treated, with a net benefit of zero. An oblique line indicates that all samples are positive. The net benefit is a backslash with a negative slope. |
Discussion
We found that the presence of atrial fibrillation, the NIHSS score and the glucose level on admission were predictors for postthrombolysis ICH. We developed and validated a nomogram using these three independent variables to predict the probability of ICH for individual stroke patients undergoing thrombolysis.
The parameters constructed in our model are easily available in almost all medical centers and from all patients within a few minutes of their arrival to the emergency room. In addition, the nomogram does not require imaging, making it particularly suitable for nonneurologists. We also tested the nomogram in a validation set; its discriminative performance remained good, and there was good agreement between the predicted and observed probabilities of ICH. We also applied the latest analytical technique, a DCA, which has demonstrated benefits that have led to recommendations for its use. Therefore, the nomogram is both highly clinically applicable and easy to use.
Consistent with previous studies,16–22 the present study showed that atrial fibrillation, the NIHSS score and the glucose level on admission were independent predictors of postthrombolysis ICH. However, these risk factors, identified using the conventional method with ORs, accounted for only a proportion of the stroke patients who presented with ICH after intravenous thrombolysis, rather than determining a probabilistic estimate for clinicians. Therefore,an accurate and measurable prediction model for prognosis is pivotal for risk-optimized therapeutic strategies.
Six scoring systems have been produced to predict the risk of sICH after ischemic stroke thrombolysis in hyperacute settings.5,8-10,23,24 However, SEDAN and hemorrhage after thrombolysis (HAT) scores require training to read imaging for early infarct signs and hyperdense artery signs and therefore may be applicable only to specialists.25 Other scoring systems, including the Multicentre Stroke Survey (MSS) score,8 Safe Implementation of Thrombolysis in Stroke (SITS)-SICH score,9 Glucose Race Age Sex Pressure Stroke Severity (GRASPS) score5 and Stroke Prognostication using Age and NIHSS (SPAN-100) positive index,10 have no CT component in their scoring systems. However, for the individualized prediction of ICH, these scores are limited by the use of dichotomization/categorization of predictors because the process of categorizing discrete/continuous variables into 2 or more risk groups is often statistically inefficient and may decrease the predictive accuracy.26 Moreover, the disadvantage of dichotomization is that it does not make use of within-category information and leads to the loss of information. In addition, none of the previous scoring systems consider the influence of ethnicity except for the GRASPS, which is the only one that includes the Asian race as a variable in its calculation.5
Nomograms have emerged as a simpler and more advanced tool for prediction.They are a pictorial representation of a statistical predictive model that generates a numerical probability of a clinical event, so they are more accurate than the conventional method using ORs.12 Furthermore, unlike the above prognostic scores, the nomogram developed in this study assigns an accurate probability (from 10% to 80%) of ICH outcome. The nomogram can provide individualized and highly estimated ICH risk by combining three independent variables and assigning an appropriate weight to each variable based on its prognostic value, making it easy to use and able to facilitate management-related decision-making.
To the best of our knowledge, only two studies have been carried out on nomograms for the individualized prediction of the probability of postthrombolysis ICH in stroke patients.13,14 The STARTING-SICH nomogram uses 10 variables and was designed to predict sICH in stroke patients treated with intravenous thrombolysis in a large cohort study in Italy,13 but it has not been externally validated for Asian patients. Furthermore, the variables included in the nomogram are not easily obtainable upon patient admission, and data on ethnicity are lacking. However, race and ethnic differences can influence the outcome of thrombolysis in acute ischemic stroke patients.27 The other nomogram model, which includes 4 variables (age, atrial fibrillation, NIHSS score and glucose level on admission), was developed for Asian patients.14 However, the study did not include information about the total dose of r-tPA, and the percentage of ICH is reported to be higher (18.9%) in Asian populations at standard doses compared to the percentage of ICH in most Chinese studies.28
Our nomogram used only three prognostic factors, atrial fibrillation, NIHSS score and glucose level on admission, which are easily and readily obtainable during the patient’s admission to the hospital. The nomogram, with its noninvasive clinical characteristics, can provide an immediate and reliable estimation of ICH risk in acute ischemic stroke patients who require thrombolysis. This estimate can guide clinicians not only in counseling patients and/or families but also in the early identification of patients at high risk of ICH, in addition to supporting decisions regarding additional treatments or centers.
We included both symptomatic and asymptomatic postthrombolysis ICH as the outcomes for the scoring systems, as in previous studies.8,14 Many reports have demonstrated that both symptomatic and asymptomatic ICH may worsen clinical outcomes8,29,30 and influence the timing of reintroducing antithrombotic treatment after r-tPA treatment. Furthermore, predicting a greater risk of ICH preceding intravenous thrombolysis may help clinical decision-making by slanting treatment toward mechanical thrombectomy only, without intravenous r-tPA.14
There are some limitations of this study. First, our data were retrospectively collected in a single center, which might have limited the statistical power of the results. Due to the retrospective nature, some data at admission were not obtained. Second, our model has not been validated in external cohorts. We need to assess the applicability of our new nomogram in future prospective studies and validate it in a multicenter study. Third, our nomogram was based on only three available predictors. Whether increasing the number of variables will improve the nomogram requires further study, but the complexity of the nomogram could increase accordingly and may diminish the clinical utility. However, despite these limitations, we successfully identified three prognostic factors for postthrombolysis ICH in Chinese stroke patients. More importantly, the nomogram is simple and easy to use in most emergency settings, including in resource-limited areas.
Conclusions
We developed and internally validated a novel nomogram to predict the risk of postthrombolysis ICH in Chinese stroke patients. The nomogram could be a rapid, clinically applicable risk scoring system to predict ICH after intravenous r-tPA treatment in stroke patients. Additionally, it is imperative to confirm these findings through prospective, multicenter studies.
Acknowledgments
This work was supported by the clinical research of the First Affiliated Hospital of Xi’an Jiaotong University (XJTU1AF-CRF-2018-024) and the Key Science and Technology Program of Shaanxi Province, China (2018SF-089). The abstract of this paper was presented at the International Stroke Conference (ISC) 2020 as a poster presentation with interim findings.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Benjamin EJ, Muntner P, Alonso A, et al. Heart disease and stroke statistics-2019 update: a report from the American Heart Association. Circulation. 2019;139(10):e56–e528.
2. Wardlaw JM, Murray V, Berge E, Del Zoppo GJ. Thrombolysis for acute ischaemic stroke. Cochrane Database Syst Rev. 2014;7:CD000213.
3. Strbian D, Sairanen T, Meretoja A, et al. Patient outcomes from symptomatic intracerebral hemorrhage after stroke thrombolysis. Neurology. 2011;77(4):341–348. doi:10.1212/WNL.0b013e3182267b8c
4. Chao AC, Hsu HY, Chung CP, et al. Outcomes of thrombolytic therapy for acute ischemic stroke in Chinese patients: the Taiwan Thrombolytic Therapy for Acute Ischemic Stroke (TTT-AIS) study. Stroke. 2010;41(5):885–890. doi:10.1161/STROKEAHA.109.575605
5. Menon BK, Saver JL, Prabhakaran S, et al. Risk score for intracranial hemorrhage in patients with acute ischemic stroke treated with intravenous tissue-type plasminogen activator. Stroke. 2012;43(9):2293–2299. doi:10.1161/STROKEAHA.112.660415
6. Li M, Wang-Qin RQ, Wang YL, et al. Symptomatic intracerebral hemorrhage after intravenous thrombolysis in Chinese patients: comparison of prediction models. J Stroke Cerebrovasc Dis. 2015;24(6):1235–1243. doi:10.1016/j.jstrokecerebrovasdis.2015.01.026
7. Strbian D, Michel P, Seiffge DJ, et al. Symptomatic intracranial hemorrhage after stroke thrombolysis: comparison of prediction scores. Stroke. 2014;45(3):752–758. doi:10.1161/STROKEAHA.113.003806
8. Cucchiara B, Tanne D, Levine SR, Demchuk AM, Kasner S. A risk score to predict intracranial hemorrhage after recombinant tissue plasminogen activator for acute ischemic stroke. J Stroke Cerebrovasc Dis. 2008;17(6):331–333. doi:10.1016/j.jstrokecerebrovasdis.2008.03.012
9. Mazya M, Egido JA, Ford GA, et al. Predicting the risk of symptomatic intracerebral hemorrhage in ischemic stroke treated with intravenous alteplase: safe Implementation of Treatments in Stroke (SITS) symptomatic intracerebral hemorrhage risk score. Stroke. 2012;43(6):1524–1531. doi:10.1161/STROKEAHA.111.644815
10. Saposnik G, Guzik AK, Reeves M, Ovbiagele B, Johnston SC. Stroke prognostication using age and NIH stroke scale: SPAN-100. Neurology. 2013;80(1):21–28. doi:10.1212/WNL.0b013e31827b1ace
11. Van Hooff RJ, Nieboer K, De Smedt A, et al. Validation assessment of risk tools to predict outcome after thrombolytic therapy for acute ischemic stroke. Clin Neurol Neurosurg. 2014;125:189–193.
12. Balachandran VP, Gonen M, Smith JJ, DeMatteo RP. Nomograms in oncology: more than meets the eye. Lancet Oncol. 2015;16(4):e173–180. doi:10.1016/S1470-2045(14)71116-7
13. Cappellari M, Turcato G, Forlivesi S, et al. STARTING-SICH nomogram to predict symptomatic intracerebral hemorrhage after intravenous thrombolysis for stroke. Stroke. 2018;49(2):397–404. doi:10.1161/STROKEAHA.117.018427
14. Yeo LLL, Chien SC, Lin JR, et al. Derivation and validation of a scoring system for intravenous tissue plasminogen activator use in asian patients. J Stroke Cerebrovasc Dis. 2017;26(8):1695–1703. doi:10.1016/j.jstrokecerebrovasdis.2017.03.033
15. Hacke W, Kaste M, Bluhmki E, et al. Thrombolysis with alteplase 3 to 4.5 hours after acute ischemic stroke. N Engl J Med. 2008;359(13):1317–1329. doi:10.1056/NEJMoa0804656
16. Saposnik G, Gladstone D, Raptis R, et al. Atrial fibrillation in ischemic stroke: predicting response to thrombolysis and clinical outcomes. Stroke. 2013;44(1):99–104. doi:10.1161/STROKEAHA.112.676551
17. Yue R, Li D, Yu J, et al. Atrial fibrillation is associated with poor outcomes in thrombolyzed patients with acute ischemic stroke: a systematic review and meta-analysis. Medicine. 2016;95(10):e3054. doi:10.1097/MD.0000000000003054
18. Hong CT, Chiu WT, Chi NF, et al. Low-density lipoprotein level on admission is not associated with postintravenous thrombolysis intracranial hemorrhage in patients with acute ischemic stroke. J Investig Med. 2019;67(3):659–662. doi:10.1136/jim-2018-000827
19. Tanaka K, Matsumoto S, Furuta K, et al. Differences between predictive factors for early neurological deterioration due to hemorrhagic and ischemic insults following intravenous recombinant tissue plasminogen activator. J Thromb Thrombolysis. 2019.
20. Xu X, Li C, Wan T, et al. Risk factors for hemorrhagic transformation after intravenous thrombolysis in acute cerebral infarction: a retrospective single-center study. World Neurosurg. 2017;101:155–160. doi:10.1016/j.wneu.2017.01.091
21. Xu X, Wang D, Wang F, Norton C, Liu X, Selim M. The risk of hemorrhagic transformation after thrombolysis for acute ischemic stroke in chinese versus north americans: a comparative study. J Stroke Cerebrovasc Dis. 2018;27(9):2381–2387. doi:10.1016/j.jstrokecerebrovasdis.2018.04.027
22. Guo Y, Yang Y, Zhou M, He L. Risk factors of haemorrhagic transformation for acute ischaemic stroke in Chinese patients receiving intravenous recombinant tissue plasminogen activator: a systematic review and meta-analysis. Stroke Vasc Neurol. 2018;3(4):203–208. doi:10.1136/svn-2018-000141
23. Lou M, Safdar A, Mehdiratta M, et al. The HAT score: a simple grading scale for predicting hemorrhage after thrombolysis. Neurology. 2008;71(18):1417–1423. doi:10.1212/01.wnl.0000330297.58334.dd
24. Strbian D, Engelter S, Michel P, et al. Symptomatic intracranial hemorrhage after stroke thrombolysis: the SEDAN score. Ann Neurol. 2012;71(5):634–641. doi:10.1002/ana.23546
25. Lokeskrawee T, Muengtaweepongsa S, Patumanond J, et al. Prediction of symptomatic intracranial hemorrhage after intravenous thrombolysis in acute ischemic stroke: the symptomatic intracranial hemorrhage score. J Stroke Cerebrovasc Dis. 2017;26(11):2622–2629. doi:10.1016/j.jstrokecerebrovasdis.2017.06.030
26. Alvarez-Sabin J, Maisterra O, Santamarina E, Kase CS. Factors influencing haemorrhagic transformation in ischaemic stroke. Lancet Neurol. 2013;12(7):689–705. doi:10.1016/S1474-4422(13)70055-3
27. Mishra NK, Mandava P, Chen C, et al. Influence of racial differences on outcomes after thrombolytic therapy in acute ischemic stroke. Int J Stroke. 2014;9(5):613–617. doi:10.1111/ijs.12162
28. Chao AC, Liu CK, Chen CH, et al. Different doses of recombinant tissue-type plasminogen activator for acute stroke in Chinese patients. Stroke. 2014;45(8):2359–2365. doi:10.1161/STROKEAHA.114.005245
29. Lei C, Wu B, Liu M, Chen Y. Asymptomatic hemorrhagic transformation after acute ischemic stroke: is it clinically innocuous? J Stroke Cerebrovasc Dis. 2014;23(10):2767–2772. doi:10.1016/j.jstrokecerebrovasdis.2014.06.024
30. Kimura K, Iguchi Y, Shibazaki K, Aoki J, Terasawa Y. Hemorrhagic transformation of ischemic brain tissue after t-PA thrombolysis as detected by MRI may be asymptomatic, but impair neurological recovery. J Neurol Sci. 2008;272(1–2):136–142. doi:10.1016/j.jns.2008.05.012
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.