Back to Journals » Journal of Inflammation Research » Volume 18
Risk Factor Analysis for Recurrence of Subacute Necrotizing Lymphadenitis in Children
Authors Wu Y, Wen Y, Long Y, Chen Y, Ding Y
Received 13 March 2025
Accepted for publication 17 September 2025
Published 10 October 2025 Volume 2025:18 Pages 14161—14170
DOI https://doi.org/10.2147/JIR.S527982
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ning Quan
Yali Wu,1,* Yini Wen,1,* Yuan Long,2,* Yujun Chen,3 Yan Ding1
1Department of Rheumatology and Immunology, Wuhan Children’s Hospital (Wuhan Maternal and Child Healthcare Hospital), Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430016, People’s Republic of China; 2Department of Emergency, Wuhan Children’s Hospital (Wuhan Maternal and Child Healthcare Hospital), Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430016, People’s Republic of China; 3Department of Pharmacy, Wuhan Children’s Hospital (Wuhan Maternal and Child Healthcare Hospital), Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430016, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yan Ding, Department of Rheumatology and Immunology, Wuhan Children’s Hospital (Wuhan Maternal and Child Healthcare Hospital), Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430016, People’s Republic of China, Email [email protected] Yujun Chen, Department of Pharmacy, Wuhan Children’s Hospital (Wuhan Maternal and Child Healthcare Hospital), Tongji Medical College, Huazhong University of Science and Technology, Wuhan, 430016, People’s Republic of China, Email [email protected]
Objective: To analyze the clinical features of subacute necrotizing lymphadenitis (SNL) in children and to explore the risk factors for recurrence.
Methods: A retrospective case–control method was used to analyze 91 children with SNL admitted to Wuhan Children’s Hospital from June 2016 to December 2024. A total of 91 children diagnosed with SNL were included, including 8 cases with recurrence and 83 without recurrence. Sixty-seven of the 91 children with SNL included underwent lymph node pathology, and 24 did not undergo lymph node biopsy. The 91 clinically diagnosed SNL patients were divided into a recurrence group and a non-recurrence group. The 67 SNL cases that underwent lymph node pathological examination were also divided into recurrence and non-recurrence groups. Baseline information, clinical manifestations, and laboratory data were compared between the two groups, and univariate analysis was performed on the difference indicators. Binary logistic regression analysis was then used to explore the risk factors for recurrent SNL.
Results: Analyze of 91 SNL patients revealed significant differences in age at onset (p=0.032), fever duration (p=0.01), IL-4 (p=0.037), and complement C3 (p=0.01) levels between recurrent and non-recurrent groups. Multivariate analysis identified older age (OR=1.32, CI: 1.04– 1.69, p=0.025) and elevated complement C3 (OR=41.96, CI: 1.68– 1049.04, p=0.023) as independent recurrence risk factors. In a distinct cohort of 67 children with pathologically confirmed SNL, significant differences emerged between recurrent and non-recurrent cases for age (p=0.023), fever duration (p=0.027), IL-4 (p=0.012), complement C3 (p=0.023), and serum creatinine (p=0.043). Here, multivariate analysis demonstrated that elevated complement C3 (OR=45.23, CI: 1.46– 1402.72, p=0.030) at diagnosis was an independent risk factor for recurrence.
Conclusion: Older age of onset and elevated complement C3 may be risk factors for recurrence of SNL, with particular attention to elevated complement C3, and clinical follow-up is needed for this group of children.
Keywords: subacute necrotizing lymphadenitis, recurrence, risk factor
Introduction
Subacute necrotizing lymphadenitis (SNL), also known as Kikuchi-Fujimoto disease (KFD) or histiocytic necrotizing lymphadenitis (HNL), was initially described by Masahiro Kikuchi and Yoshihide Fujimoto in 1972.1,2 SNL is a benign self-limiting disease in which lymph nodes are the main lesions. Clinical manifestations lack specificity, mainly prolonged fever, enlarged lymph nodes, accompanied by leukopenia, hepatosplenomegaly, rash, etc.3 Definitive diagnosis relies on lymph node pathological examination. Histology revealed paracortical foci of coagulative necrosis (with karyorrhectic debris) surrounded by abundant CD68+/MPO⁺ histiocytes, CD68+/CD123⁺ plasmacytoid dendritic cells, and fewer variably sized CD8⁺ lymphocytes and immunoblasts.4 SNL typically occurs in individuals aged <40 years and shows higher prevalence in Asia,3 though cases exist worldwide across ethnicities.5 Pediatric SNL is infrequently reported, and relapse occurs in some children with undefined probability. Crucially, risk factors for pediatric SNL relapse are poorly characterized due to limited studies. We retrospectively analyzed 91 children with SNL treated at our center since 2016, described their clinical presentation, and explored recurrence risk factors to improve prognostic strategies.
Materials and Methods
Study Population
The Institutional Review Board of Wuhan Children’s Hospital, Tongji Medical College, Huazhong University of Science and Technology, gave its approval to this retrospective case–control study (NO.2025R016-E01). We included in the study children who were diagnosed with SNL at Wuhan Children’s Hospital between June 2016 and December 2024.
SNL Inclusion Criteria
①Children under 18 years of age with unexplained fever lasting more than two weeks; ②Superficial lymph node enlargement, with or without tenderness; ③Leukopenia; ④Ineffective response to antimicrobial therapy for more than one week; ⑤The pathological changes of lymph node biopsy are consistent with SNL: Histology revealed paracortical foci of coagulative necrosis (with karyorrhectic debris) surrounded by abundant CD68+/MPO⁺ histiocytes, CD68+/CD123⁺ plasmacytoid dendritic cells, and fewer variably sized CD8⁺ lymphocytes and immunoblasts.6 ⑥ Children whose guardians declined lymph node biopsy, a complete examination was required to exclude infectious diseases (eg, tuberculosis infection), and other rheumatological-immunological and haemato-oncological diseases were excluded, and those whose temperature could be controlled by glucocorticoid treatment and did not recur within 4 weeks of stopping hormone administration could be included.
SNL Exclusion Criteria
(1) Those with incomplete clinical data; (2) participants lost to follow-up. We identified 95 potential SNL cases. The final cohort comprised 91 children after excluding two cases lost to follow-up and two with incomplete data, of which 67 were diagnosed by lymph node pathology (Show in Figure 1).
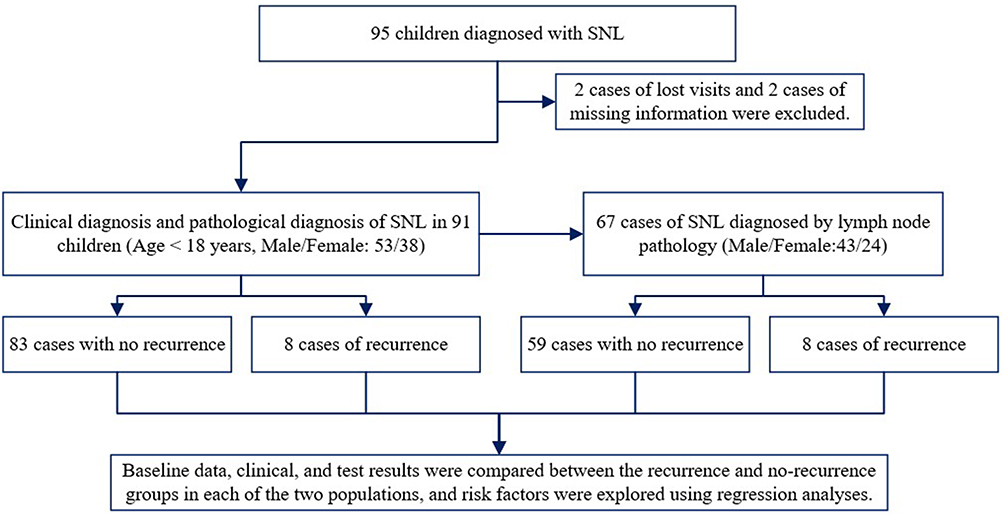 |
Figure 1 Flow chart of the patient selection process. Abbreviation: SNL, Subacute necrotizing lymphadenitis. |
Data Collection
Data on 91 children diagnosed with SNL were retrieved from the electronic medical record system and data platform of Wuhan Children’s Hospital: ①collected general demographic data: gender, age, body mass index (BMI) and hospitalization days. ②Clinical manifestations: fever, fever duration, fatigue, loss of appetite, rash, lymphadenopathy, lymph node tenderness, and maximum lymph node diameter. ③Laboratory results: white blood cells (WBC), hemoglobin (Hb), neutrophil (NEU), lymphocyte (LYM), platelets (PLT), eosinophil (EOS), C reactive protein (CRP), erythrocyte sedimentation rate (ESR), procalcitonin (PCT), serum ferritin (SF), serum Na, Potassium (K), alanine aminotransferase (ALT), aspartate aminotransferase (AST), serum globulin (GLB), serum albumin (ALB), serum creatinine (Scr), uric acid (UA), urea nitrogen (BUN), creatine kinase (CK), creatine kinase-MB (CK-MB), lactate dehydrogenase (LDH), triglycerides (TG), high-density lipoprotein Cholesterol (HDL), total cholesterol (TC), low-density lipoprotein cholesterol (LDL), activated partial thromboplastin time (APTT), thrombin time (TT), prothrombin time (PT), fibrinogen (FIB), international normalized ratio (INR), IL-2, IL-4, IL-6, IL-10, IFNγ, and TNFα, IgE, IgM, IgG, IgA, Complement C3, Complement C4, anti-streptolysin O(ASO), CD3+T, CD4+T, CD8+T, CD19+B, CD4+/CD8+T.
Statistical Analyze
Statistical analyses were performed using R version 4.4.1. The recurrence and non-recurrence groups were explicitly compared. Measurement data were assessed for normality; normally distributed continuous variables were expressed as mean ± standard deviation and compared using independent t-tests, between recurrence and non-recurrence groups. Non-normally distributed data were expressed as median (Q1, Q3) and analyzed with Mann–Whitney U-tests. Categorical data were reported as counts (%) and compared by chi-square tests. Univariate logistic regression (with recurrence status as the dependent variable) was first performed for variables showing significant intergroup differences (p<0.05). Multiple collinearity analysis was performed using Variance Inflation Factor (VIF). Variables with p<0.05 in univariate analysis were then entered into a multivariate logistic regression model to identify independent risk factors for recurrence group. Backward selection of control variables was used in regression analysis to validate the above results. Statistical significance was defined as p<0.05. Effect sizes are reported as odds ratios (OR) with 95% confidence intervals.
Results
General Demographic Data and Clinical Manifestations of SNL Non Recurrence Group and Recurrence Group
All SNL Children
The study cohort comprised 91 children with clinically and pathologically confirmed SNL, including 83 non-recurrent cases and 8 recurrent cases (recurrence rate: 8.8%; 53 males, 38 females). All patients presented with fever and lymphadenopathy. Constitutional symptoms included malaise (4.4%), anorexia (12.1%), skin rashes (20.9%), and lymph node tenderness (74.7%). Compared to the non-recurrent group (8.98±3.06), the recurrence group (11.54±4.42) showed significantly older age at onset (p =0.032) and prolonged fever duration (p = 0.01). No significant differences were observed in other baseline characteristics or clinical symptoms (Show in Table 1).
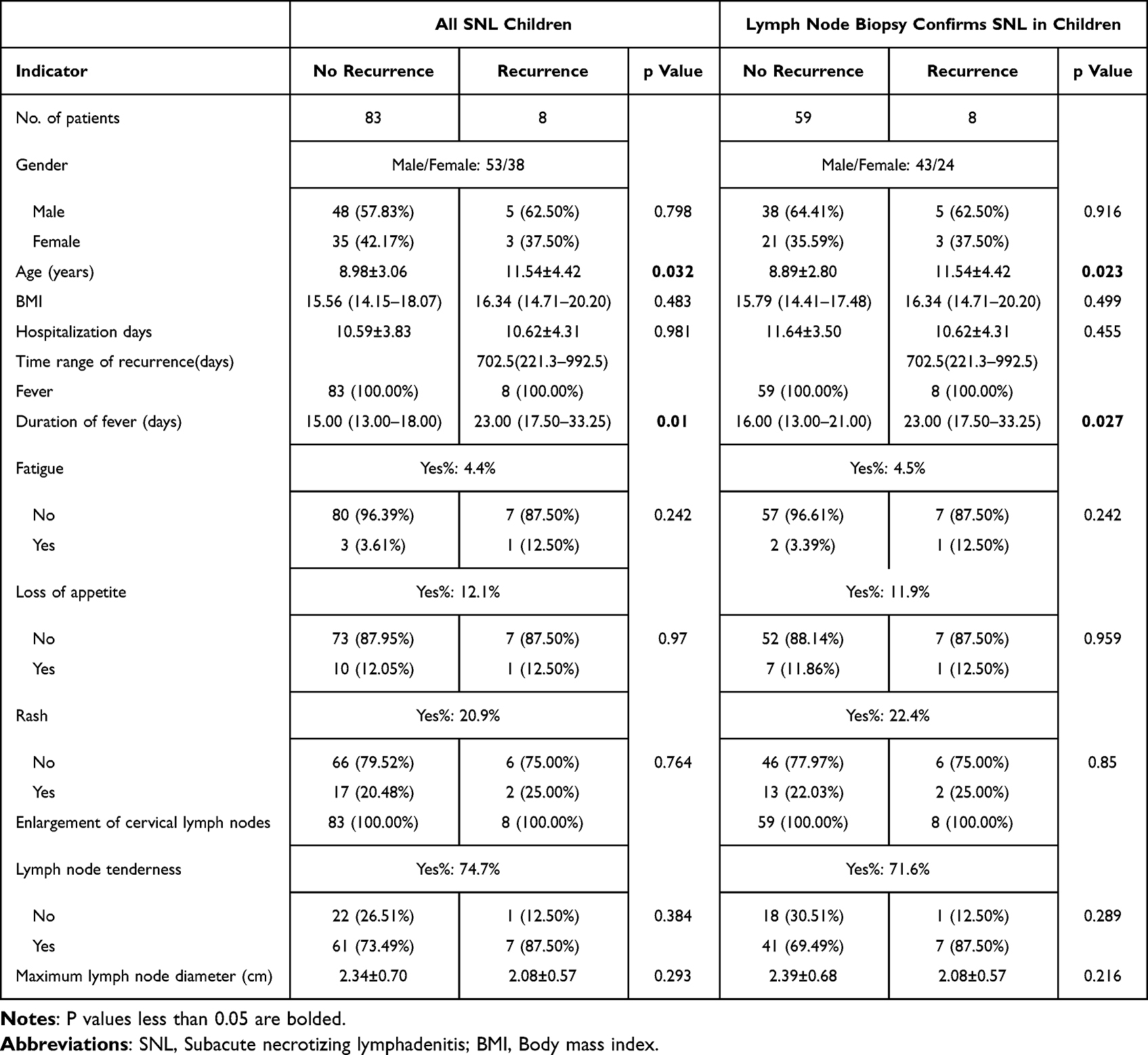 |
Table 1 General Demographic Data and Clinical Manifestations of SNL Non Recurrence Group and Recurrence Group |
Children with Lymph Node Biopsy-Confirmed SNL
The cohort comprised 67 children with pathologically confirmed SNL, including 59 non-recurrent cases and 8 recurrent cases (recurrence rate: 11.9%; 43 males, 24 females). All patients presented with fever and lymphadenopathy. Associated symptoms included malaise (4.5%), anorexia (11.9%), rash (22.4%), and lymph node tenderness (71.6%). Compared to the non-recurrent group (8.89±2.80), the recurrence group (11.54±4.42) exhibited significantly older age at onset (p =0.023) and longer fever duration (p = 0.027). No significant differences were observed in other baseline characteristics or clinical symptoms (Show in Table 1).
Routine Blood Counts, Inflammatory Markers, Biochemical and Coagulation Results of SNL Non Recurrence Group and Recurrence Group
All SNL Children
Laboratory parameters including complete blood counts, inflammatory markers, biochemical, and coagulation profiles showed no significant differences (p>0.05) between recurrent and non-recurrent SNL cases (Show in Table 2).
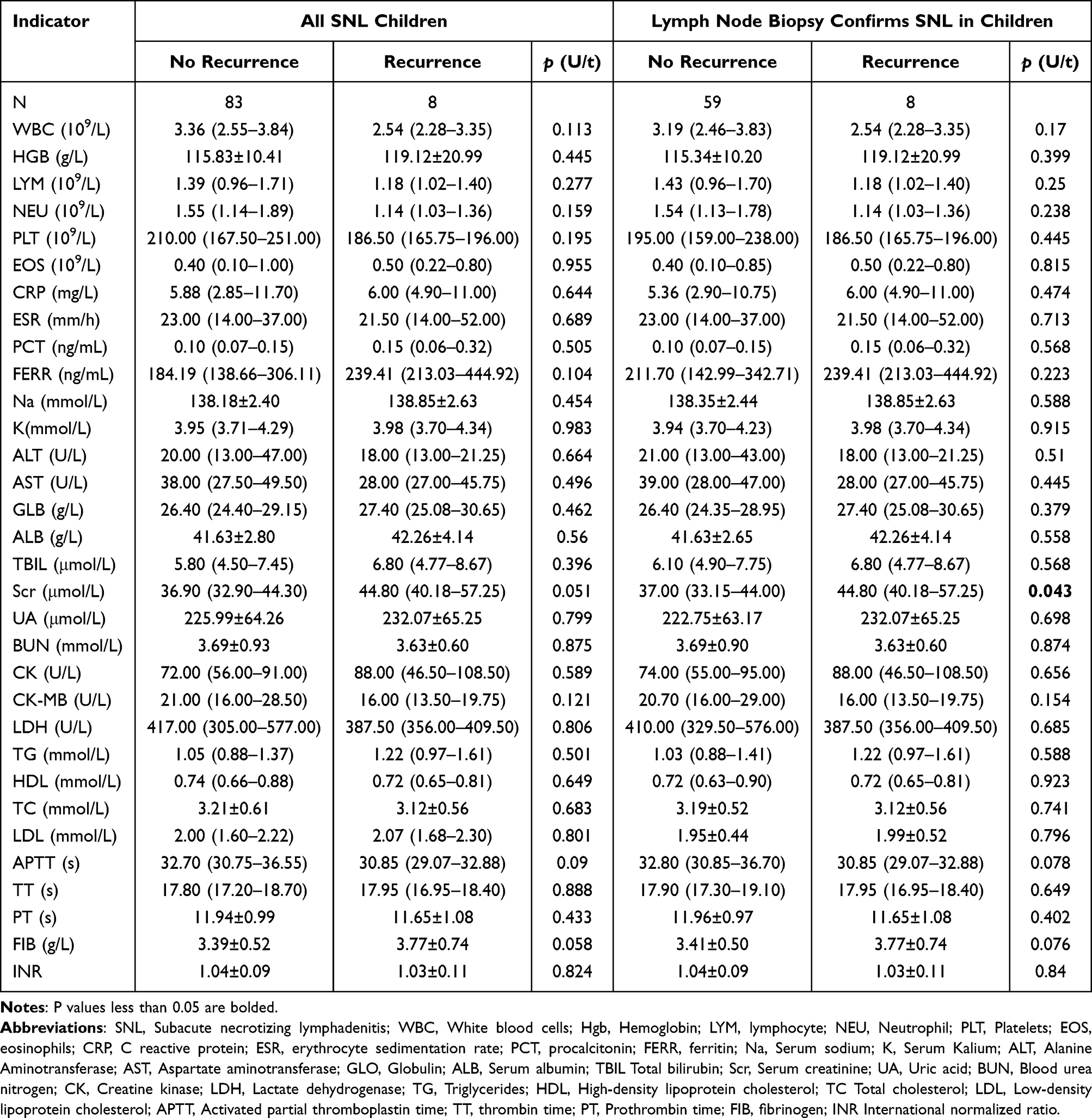 |
Table 2 Routine Blood Counts, Inflammatory Markers, Biochemical and Coagulation Results of SNL Non Recurrence Group and Recurrence Group |
Children with Lymph Node Biopsy-Confirmed SNL
Among the included children with pathological diagnosis of SNL, the difference in creatinine elevation in the recurrence group was statistically significant (p =0.043) when compared to the no recurrence group, and the remaining indicators were not statistically different between the two groups (Show in Table 2).
Humoral Immunity, Cellular Immunity, Cytokines and Other Immunological Indicators of SNL Non Recurrence Group and Recurrence Group
All SNL Children
Among all the children with SNL included, complement C3 (p =0.01) was higher, and IL-4 (p =0.037) was instead lower in the recurrence group, which was a statistically significant difference, and the remaining immune indices were not statistically different between the two groups (Show in Table 3).
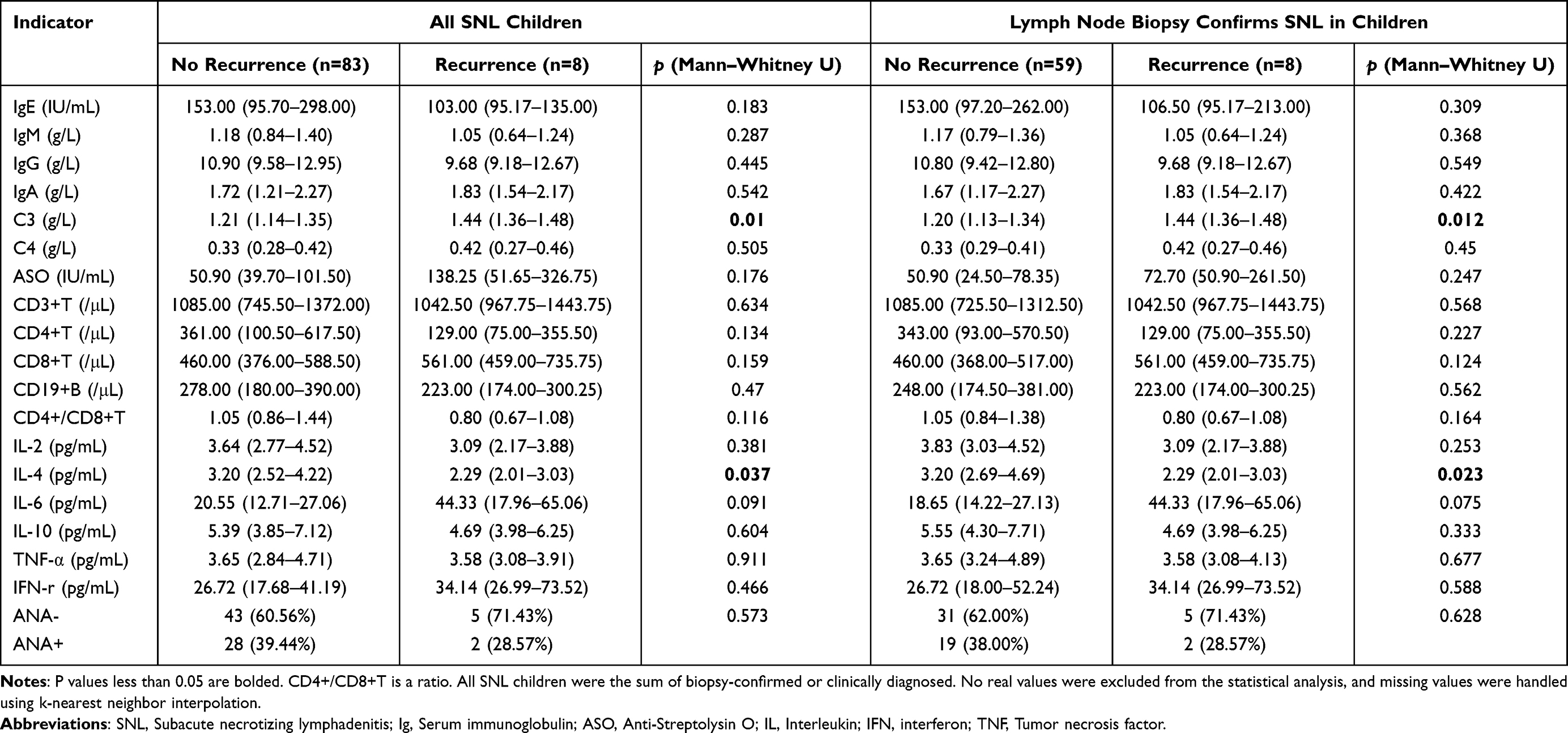 |
Table 3 Humoral Immunity, Cellular Immunity, Cytokines and Other Immunological Indicators of SNL Non Recurrence Group and Recurrence Group |
Children with Lymph Node Biopsy-Confirmed SNL
In children with pathologically diagnosed SNL, consistent with the results of all children with SNL, complement C3 (p =0.012) was higher and IL-4 (p =0.023) was lower in the recurrence group, which was significantly different from the no recurrence group, while other immune indices were not statistically significant between the two groups (Show in Table 3).
Risk Factors of SNL Non Recurrence Group and Recurrence Group
All SNL Children
Among 91 children with SNL, significant differences emerged between recurrent and non-recurrent groups for age of onset, fever duration, IL-4, and complement C3 levels (p < 0.05). Multicollinearity diagnostics revealed no concerning correlations among predictors (VIF: duration of fever=1.07, age=1.06, IL-4=1.10, C3=1.17; all < 2.0). Logistic regression univariate analysis identified older age (OR=1.32, CI: 1.04–1.69, p=0.025) and elevated complement C3 (OR=41.96, CI: 1.68–1049.04, p=0.023) as significant risk factors. Subsequent multivariate analysis confirmed both as independent risk factors for recurrence. (Show in Table 4). The goodness-of-fit test showed satisfactory fit (χ² = 6.64, df = 8, p = 0.576).
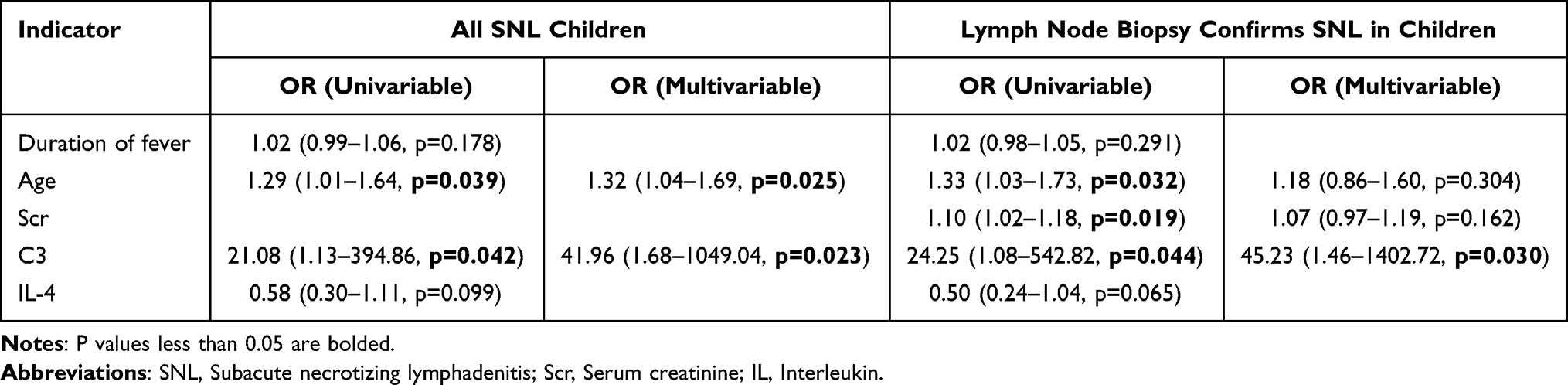 |
Table 4 Logistic Regression Distribution for Screening Risk Factors of SNL Non Recurrence Group and Recurrence Group |
In 91 pediatric patients with SNL, the backward selection method based on the AIC criterion validated the core findings of traditional regression analysis: age (OR=1.30, 95% CI: 1.03–1.74) and complement C3 (OR=92.4, 95% CI: 2.89–4570) remain independent risk factors for recurrence (both p < 0.05). IL-4 showed a protective trend in the multivariate interaction model (OR=0.50, 95% CI: 0.21–0.97, p=0.075), supporting its potential clinical value (Show in Table 5).
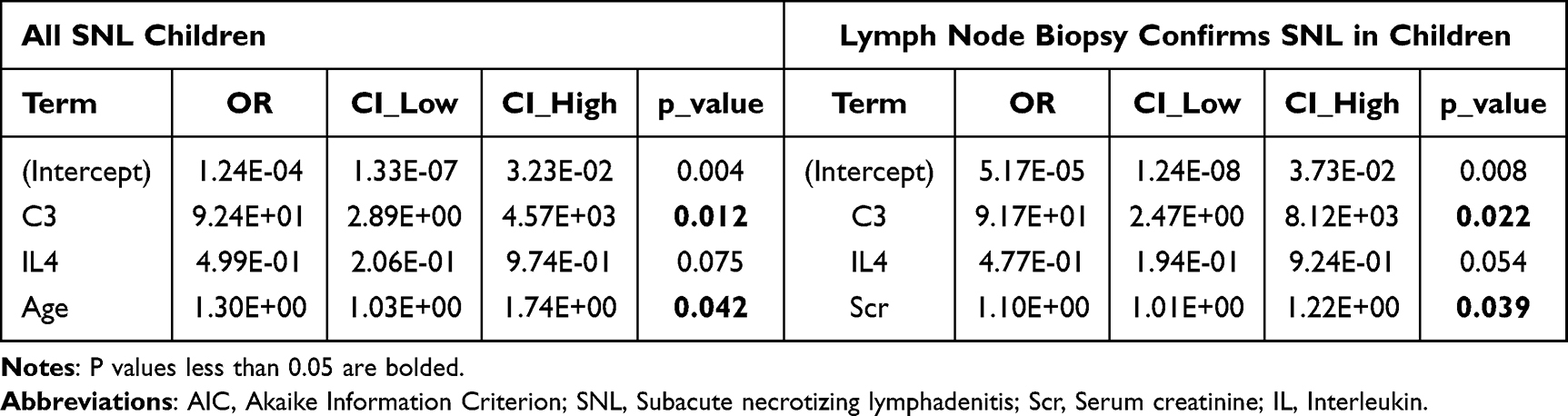 |
Table 5 Backward Selection Method Based on AIC Criteria for Screening Risk Factors |
Children with Lymph Node Biopsy-Confirmed SNL
Among the 67 children with pathological diagnosis of SNL included, the differences in age, duration of fever, IL-4, complement C3, and serum creatinine among the above indexes between the recurrence group and the non-recurrence group were statistically significant. Multicollinearity diagnostics revealed no concerning correlations among predictors (VIF: duration of fever=1.07, age=1.89, IL-4=1.14, C3=1.21, Scr=1.95; all < 2.0), and the one-way regression analyses were performed separately, and the P-values of older age, high complement C3, and elevated creatinine were <0.05, and the results of the multifactorial regression analyses showed that elevated complement C3 (OR=45.23, CI: 1.46–1402.72, p=0.030) was an independent Risk factor. (Show in Table 4). The goodness-of-fit test showed satisfactory fit (χ² = 11.23, df = 8, p = 0.188).
In 67 pediatric patients with SNL, the backward selection method based on the AIC criterion revealed that C3 (OR=91.7, CI: 2.47–8120, p=0.022) remained a significant risk factor with a larger effect size (OR increased from 45.23 to 91.7), further emphasizing the importance of C3. For newly emerging Scr, although it was not significant in the traditional multivariate model (p=0.162), it became significant in the backward selection method (OR=1.1, CI: 1.01–1.22, p=0.039) (Show in Table 5).
Discussion
SNL is a rare and complex disease of unknown etiology and pathogenesis,7 and its diagnosis usually relies on a combination of clinical features, laboratory tests, and histopathological examination. The probability of recurrence of the disease has been reported variably, with earlier reports ranging from 3% to 7%,8–10 and reports from Korea mentioning a prevalence of 20.6%,11 and some even as high as 38.1%,12 and our findings of SNL recurrence in children ranging from 8.8% to 11.9%. Given the rarity of the disease, there is limited available data on the recurrence pattern and associated risk factors of SNL in children. To address this gap, we analyzed the clinical features of 91 pediatric SNL cases, one of the largest cohorts to date and examined a wide range of laboratory indices to identify potential risk factors for recurrence.
We analyzed all children with a clinical diagnosis and a pathological diagnosis, as well as children with confirmed lymph node pathology, separately, which ensured data completeness. We included children with fever and enlarged lymph nodes, and the male-to-female ratio analyzed by both methods was 53:38 and 43:24, both with a high prevalence in male children. There was a significant difference in clinical symptoms between the recurrent and no recurrence groups in terms of older age and longer duration of fever in the recurrent group. The reason may be related to the relative maturity of the immune system of older children and the change of response pattern to certain pathogens,13 such as the relative insufficiency of regulatory T-cells (Treg),14 which may have a low level of response to some immune processes, and therefore the prolonged duration of fever, which has been confirmed in the previous report,11 and the susceptibility to cause a second immune response if re-exposed to the same type of antigenic stimulus. Older age was found to be an independent risk factor for recurrence in all children with SNL in multifactorial regression analyses (OR=1.32, 95% CI 1.06–1.64) and backward selection method (OR=1.3, 95% CI 1.03–1.74), which confirmed the reliability of the conclusions. However, it failed to enter the multifactorial model in the pathologically confirmed group, which may be related to the relatively restricted biopsy sample size.
In pediatric SNL patients with pathological confirmation, elevated serum creatinine distinguished recurrent cases (p<0.05) and persisted as an independent risk factor (backward selection p=0.039) in multivariate modeling, thus revealing its independent contribution when considering more variable combinations. Although none of the children met the criteria for acute kidney injury, our data suggest the potential for subclinical renal involvement in SNL, a finding not previously reported. The mechanisms may include the following causes: lymph node necrosis that may release procoagulant substances such as tissue factor may lead to renal capillary microthrombus;15 or tubular interstitial inflammation mediated by complement deposition that activates renal tubular epithelial cells and releases chemokines.16 We therefore recommend that children with SNL with elevated creatinine need regular monitoring of routine urine and urine protein/creatinine ratio.
In a study by In Yoo IH et al,12 low C3 expression levels were found in the recurrence group of SNL patients. However, data from Zhidan et al17 in China showed a slight increase in C3 values in the recurrence group. Although the differences between these two studies were not statistically significant. Our study found that in both the overall SNL cohort and the pathologically confirmed pediatric subgroup, complement C3 levels were significantly higher in the recurrent group compared to the non-recurrent group. Furthermore, using both statistical methods, elevated C3 levels were identified as an independent risk factor for SNL recurrence, strengthening the evidence for a robust association between high C3 and recurrence. However, the mechanism by which complement contributes to SNL remains unclear, we speculate that it may involve the following two aspects. First, C3 is the intersection of the complement classical/bypass pathway, and its elevation may reflect immune complex deposition,18 which can activate macrophages, release pro-inflammatory factors such as TNF-α and IL-1β, and exacerbate the necrosis of lymph node tissues.19 Second, complement activation products such as C5a can induce endothelial cells to express tissue factor and promote microthrombus,20 which may result in characteristic local necrotic changes. Therefore, we believe that complement C3 has a predictive value for SNL, and shorter follow-up intervals are recommended for children with elevated C3 levels at initial diagnosis (complement C3 > 1.48 g/L).
IL-4, a typical T helper 2 cell (Th2) cytokine,21 was significantly reduced in both all children with SNL and in the recurrence group of children with pathologically confirmed SNL, suggesting a suppressed Th2 immune response and thus a relative advantage for Th1 (eg, elevated interferon-γ (IFN-γ)) possibly prolonging the process of lymph node necrosis by activating cytotoxic T cells and macrophages.22 Meanwhile, it should be noted that decreased IL-4 was negatively correlated with elevated C3 (r=−0.37, p=0.02), suggesting that overactivation of the complement system may inhibit the process of Th2 differentiation. Previously, dendritic cells affected by C3a were found to inhibit IL-4 secretion in animal experiments,23 and whether this mechanism is present in SNL needs to be further verified.
Our study confirmed that older children and elevated complement C3 are independent risk factors for SNL recurrence, but the study has some limitations. Compared with previous studies,11,12 although our center included more cases of children with SNL, the sample size was still limited, with only 8 cases in the recurrence group, and the analysis was retrospective, which may have caused bias in the results; therefore, it is necessary to conduct a multicenter prospective large-sample cohort study at a later stage to establish a relatively robust recurrence risk scoring model.
Conclusion
This study establishes for the first time that elevated complement C3 is an independent risk factor for SNL recurrence in children. Clinically, children with elevated C3 at initial diagnosis warrant intensified follow-up. We further identified older age as a potential recurrence predictor and observed possible subclinical renal impairment. Collectively, these findings directly enable risk-stratified clinical management and targeted therapies while providing novel mechanistic insights into SNL pathogenesis.
Abbreviations
SNL, Subacute necrotizing lymphadenitis; BMI, Body mass index; WBC, White blood cells; Hgb, Hemoglobin; PYM, lymphocyte; NEU, Neutrophil; PLT, Platelets; EOS, eosinophils; CRP, C reactive protein; ESR, erythrocyte sedimentation rate; PCT, procalcitonin; FERR, ferritin; Na, Serum sodium; K, Serum Kalium; ALT, Alanine Aminotransferase; AST, Aspartate aminotransferase; GLO, Globulin; ALB, Serum albumin; TBIL Total bilirubin; Scr, Serum creatinine; UA, Uric acid; BUN, Blood urea nitrogen; CK, Creatine kinase; LDH, Lactate dehydrogenase; TG, Triglycerides; HDL, High-density lipoprotein cholesterol; TC Total cholesterol; LDL, Low-density lipoprotein cholesterol; APTT, Activated partial thromboplastin time; TT, thrombin time; PT, Prothrombin time; PT, fibrinogen; FIB, fibrinogen; INR International normalized ratio; Ig, Serum immunoglobulin; IL, Interleukin; IFN, interferon; TNF, Tumor necrosis factor.
Data Sharing Statement
The original contributions presented in the study are included in the article, further inquiries can be directed to the corresponding author.
Ethical Approval and Informed Consent
This research was reviewed and approved by the Ethics Committee of Wuhan Children’s Hospital, Tongji Medical College, Huazhong University of Science and Technology (NO.2025R016-E01). The research protocol complied with the Declaration of Helsinki in 1964 and its current amendments. This research was a retrospective analyze, and all the data were collected from previous clinical records. The Ethics Committee of Wuhan Children’s Hospital, Tongji Medical College, Huazhong University of Science and Technology approved the informed consent exemption due to anonymous patient records.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analyze and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
A portion of this work was funded by the Soaring Program of Youth Talent Development at Wuhan Children’s Hospital (grant number 2024TFJH02) and the Funding for Scientific Research Projects from Wuhan Municipal Health Commission (WX23Z66).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. KikuchiM I. Lymphadenitisshowingfocalreticulumcellhyperplasia with nucl ear debris and ph agocytosis. Nippon Ketsueki Gakki Zashi. 1972;35:379–380. (in Japanese).
2. Fujimoto Y. Cervical subacute necrotizing lymphadenitis. Naika. 1972;30:920–927.
3. Hutchinson CB, Wang E. Kikuchi-Fujimoto disease. Arch Pathol Lab Med. 2010;134:289–293. doi:10.5858/134.2.289
4. Pepe F, Disma S, Teodoro C, Pepe P, Magro G. Kikuchi-Fujimoto disease: a clinicopathologic update. Pathologica. 2016;108:120–129.
5. Perry AM, Choi SM. Kikuchi-Fujimoto Disease: a Review. Arch Pathol Lab Med. 2018;142(11):1341–1346. doi:10.5858/arpa.2018-0219-RA
6. Kim KH, Jung SH, Park C, Choi IJ. Subacute necrotizing lymphadenitis--a collective clinicopathological and immunohistochemical study. Yonsei Med J. 1992;33:32–40. doi:10.3349/ymj.1992.33.1.32
7. Mauleón C, Valdivielso-Ramos M, Cabeza R, Rivera T, García I. Kikuchi disease with skin lesions mimicking lupus erythematosus. J Dermatol Case Rep. 2012;286:82–85. doi:10.3315/jdcr.2012.1108
8. Choi JW, Lee JH, Lee JH, Chae YS, Kim I. The clinicopathologic analysis of Kikuchi’s lymphadenitis. J Pathol Transl Med. 2004;38:289–294.
9. Takano Y, Saegusa M, Okudaira M. Pathologic analyses of non-overt necrotizing type Kikuchi and Fujimoto’s disease. Acta Pathol Jpn. 1993;43:635–645. doi:10.1111/j.1440-1827.1993.tb02547.x
10. Tsang WY, Chan JK, Ng CS. Kikuchi’s lymphadenitis. A morphologic analysis of 75 cases with special reference to unusual features. Am J Surg Pathol. 1994;18:219–231. doi:10.1097/00000478-199403000-00001
11. Song JY, Lee J, Park DW, et al. Clinical outcome and predictive factors of recurrence among patients with Kikuchi’s disease. Int J Infect Dis. 2009;13:322–326. doi:10.1016/j.ijid.2008.06.022
12. Yoo IH, Na H, Bae EY, et al. Recurrent lymphadenopathy in children with Kikuchi-Fujimoto disease. Eur J Pediatr. 2014;173:1193–1199. doi:10.1007/s00431-014-2306-6
13. Leaver BA, Smith BJ, Irving L, Johnson DF, Tong SYC. Hospitalisation, morbidity and outcomes associated with respiratory syncytial virus compared with influenza in adults of all ages. Influenza Other Respir Viruses. 2022;16:474–480. doi:10.1111/irv.12909
14. Chuang CH, Yan DC, Chiu CH, et al. Clinical and laboratory manifestations of Kikuchi’s disease in children and differences between patients with and without prolonged fever. Pediatr Infect Dis J. 2005;24:551–554. doi:10.1097/01.inf.0000167246.24500.21
15. Levi M, van der Poll T. Coagulation and sepsis. Thromb Res. 2017;149:38–44. doi:10.1016/j.thromres.2016.11.007
16. Noris M, Remuzzi G. Glomerular diseases dependent on complement activation, including atypical hemolytic uremic syndrome, membranoproliferative glomerulonephritis, and C3 glomerulopathy: core curriculum 2015. Am J Kidney Dis. 2015;66:359–375. doi:10.1053/j.ajkd.2015.03.040
17. Zhidan HNYHZYF. Risk factor analysis for the prognosis of subacute necrotizing lymphadenitis in children. J Southeast University. 2016;35:189–192.
18. Ricklin D, Reis ES, Mastellos DC, Gros P, Lambris JD. Complement component C3 - The “Swiss Army Knife” of innate immunity and host defense. Immunol Rev. 2016;274:33–58. doi:10.1111/imr.12500
19. Mastellos DC, Ricklin D, Lambris JD. Clinical promise of next-generation complement therapeutics. Nat Rev Drug Discov. 2019;18:707–729. doi:10.1038/s41573-019-0031-6
20. Huber-Lang M, Sarma JV, Zetoune FS, et al. Generation of C5a in the absence of C3: a new complement activation pathway. Nat Med. 2006;12:682–687. doi:10.1038/nm1419
21. Paul WE. Interleukin-4: a prototypic immunoregulatory lymphokine. Blood. 1991;177:1859–1870. doi:10.1182/blood.V77.9.1859.1859
22. Spagnolo P, Tonelli R, Samarelli AV, et al. The role of immune response in the pathogenesis of idiopathic pulmonary fibrosis: far beyond the Th1/Th2 imbalance. Expert Opin Ther Targets. 2022;26:617–631. doi:10.1080/14728222.2022.2114897
23. Peng Q, Li K, Sacks SH, Zhou W. The role of anaphylatoxins C3a and C5a in regulating innate and adaptive immune responses. Inflamm Allergy Drug Targets. 2009;8:236–246. doi:10.2174/187152809788681038
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Long-Term Outcomes of Traditional Chinese Medicine in the Treatment of Granulomatous Lobular Mastitis: A Two-Year Follow-Up Study on Recurrence and New Occurrence Rates with Analysis of Risk Factors
Hua C, Li F, Shi Y, Xu Y, Zhu M, Wang Y, Zhou X, Liu S
Journal of Inflammation Research 2024, 17:7389-7399
Published Date: 16 October 2024