")
Back to Journals » Risk Management and Healthcare Policy » Volume 16
Risk Characteristics of Catastrophic Health Expenditure in Multidimensional Borderline Poor Households in China
Received 18 July 2022
Accepted for publication 16 November 2022
Published 5 January 2023 Volume 2023:16 Pages 15—29
DOI https://doi.org/10.2147/RMHP.S382812
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Xiaocang Xu,1 Xiuquan Huang2
1School of Economics and Management, Huzhou University, Huzhou, 313000, People’s Republic of China; 2Faculty of Humanities and Social Sciences, Macao Polytechnic University, Macao, 999078, People’s Republic of China
Correspondence: Xiuquan Huang, Email [email protected]
Background: Ending poverty and realizing common prosperity are the essential requirements for the localization of Marxism in China. The ongoing COVID-19 pandemic in the post-poverty era further aggravates the risk of catastrophic health expenditure for borderline poor households and increases the uncertainty of returning to poverty due to illness, potentially undermining decades of hard-won efforts to eradicate poverty in China.
Methods: Based on the latest data released by China Health and Retirement Longitudinal Survey (CHARLS) database, this paper uses the Logit model to empirically explore the risk characteristics of catastrophic health expenditure of multidimensional borderline poor households based on identifying multidimensional borderline poor households.
Results: The results show that factors such as family income level, child support, and medical insurance have different impacts on catastrophic health expenditure, and the risk of catastrophic health expenditure of multidimensional borderline poor households is much higher than that of non- multidimensional borderline poor households, and there is a certain difference between urban and rural areas.
Discussion: The government should strengthen and improve the social security system and health service system, such as medical insurance, and more resources should be allocated to multidimensional borderline poor households, especially in rural areas.
Keywords: common prosperity, multidimensional borderline poor households, catastrophic health expenditure, urban-rural differences, insurance system
Introduction
Future healthy well-being should “achieve universal health protection, including financial risk protection; Quality basic health services for everyone; Access to safe, effective, quality and affordable essential medicines and vaccines for everyone. (United Nations 2030 Agenda for Sustainable Development, Seventieth Session of the General Assembly, 2015)”. China has achieved universal coverage of basic medical insurance and basic public health services,1 but family economic difficulties caused by high out-of- pocket medical expenditures are still an important problem faced by China and even developing countries.2–5 Out-of-pocket medical expenditure refers to the doctor’s consultation fee, drug fee, medical treatment fee and hospital bill that a person needs to pay for medical care).6 China has set a target of reducing the proportion of out-of-pocket medical expenditures to around 25% by 2030 (Outline of healthy China 2030, State Council of China, 2016). Figure 1 shows the annual average and rate of change in the proportion of out-of-pocket medical expenditures by individuals since 1978. China reformed its health system from government-run to market-based, resulting in a dramatic increase in out-of-pocket health spending by patients (which at one point soared to nearly 60%) after 1978. Then the government alleviated this situation through a series of measures such as the new rural cooperative medical plan and the basic medical insurance plan for urban residents after 2000. The proportion of personal out-of-pocket medical expenses decreased year by year after reaching the peak in 2000, but the downward trend slowed down and stabilized after 2015.
 |
Figure 1 Proportion of individual out-of-pocket medical expenditure in total health expenditure. Note: Compiled from the data of China Statistical Yearbook in 2020. |
The high level of individual out-of-pocket medical expenditure indicates the irrationality of current health system financing. The outbreak and continuation of the COVID-19 pandemic has also prompted governments around the world to pay close attention to resilient health systems, balancing healthcare costs and avoiding personal healthcare financial risks while ensuring quality health services.7,8 Individual medical financial risk can be quantified by catastrophic health expenditure,9 which refers to the reduction of other consumption expenditures in life to a certain threshold due to the payment of medical expenses in a certain period of time.10 It also reflects individual health status to some extent.11,12 China has a high incidence of catastrophic health expenditure. The average incidence rate of catastrophic health expenditure from 2018 to 2020 is about 25.5%, and the number of people facing catastrophic health expenditure nationwide is as high as 360 million.13 This poses a severe realistic challenge to avoid a large-scale return to poverty due to disease in China, which has just lifted itself out of poverty in 2020.
The research on catastrophic health expenditure by global scholars is relatively sufficient, mainly focusing on the following four aspects. First, the influencing factors of catastrophic health expenditure and the characteristics of vulnerable populations. For example, Lian L et al14 used social stratification and social risk theory to find that factors affecting catastrophic health expenditure include medical security, family income, population, and health status Lu X et al15 used binomial Logistic regression model to find that family economic conditions, access to information, and social support system have a significant impact on poor families’ catastrophic health expenditure. Xu et al16 made a regression analysis of household survey data in 59 countries and concluded that it was disastrous for poor families, female-headed families, families with elderly members, rural families, families with large populations, families with chronic diseases and families without insurance. The second is the regional calculation of the incidence of catastrophic health expenditure. For example, Wang Y et al17 estimated that the incidence of catastrophic health expenditure in rural poor households was 28.20%, the average intensity was 7.6%, and the rate of poverty caused by disease was 32.40% in 2018 in China. Yan et al18 found that there was a significant difference in the incidence of catastrophic household health expenditures before and after the new medical reform in Rural Shaanxi Province. The third is the impact of basic medical insurance on catastrophic health expenditure. For example, Ding J et al19 obtained by using Logit model that different medical insurance has significant differences in reducing the incidence of catastrophic health expenditures for the elderly. Ekman20 found that instead of providing financial protection against catastrophic payment risk, medical insurance increased such risk in Zambia in 1998. Fourth, country differences in the level of catastrophic health expenditure. For example, research by Rasanathan and Evans21 shows that the vast majority of people [87%) who suffered large out-of-pocket medical expenses in 2015 lived in middle-income countries. Pal22 found that the economic and social status of Indian families was an important determinant of the incidence of catastrophic health expenditures, and education reduced the possibility of catastrophic health expenditures. Van Minh et al23 used data from a nationally representative household survey in Vietnam and found that catastrophic expenditures and poverty problems were more common in households with a large number of elderly people and rural households. Proano Falconi and Bernabe24 using data from 30,966 families in the 2016 Peruvian National Household Survey, found that many Peruvian families are forced to pay for their health care through out-of-pocket expenses and this seriously affects their standard of living.
The correlation between health and poverty has always been the focus of researchers around the world. Shahrawat and Rao25 and Van Minh23 confirmed that high out-of-pocket medical expenditure would lead to catastrophic health expenditure and poverty. In addition, diseases caused by poor health and poverty are a vicious circle of two-way causality.15,26 Factors influencing catastrophic health expenditures include household per capita income, chronic disease, disability, and head of household education,17,19,27 which can also be regarded as factors affecting poverty. Other scholars have applied Amartya Sen’s feasible capacity framework to determine the family development capacity that influences catastrophic health expenditure.15 In general, when analyzing the factors affecting individual health, factors of socioeconomic status such as income, education and occupation and individual characteristics are the focus of scholars’ research, while few scholars have studied the impact of multidimensional borderline poverty on health.5
China’s policies and regulations related to poverty have always included multidimensional ideas. For example, “Two no worries, three guarantees” policy and the targeted poverty alleviation policy show that China no longer uses absolute income as the sole criterion to measure poverty. The concept of multidimensional poverty was proposed by Amartya Sen based on the theory of “deprivation of feasible ability”, which refers to the lack of free choice rights caused by deprivation of multidimensional feasible ability. The poor are not only financially constrained, but also limited or deprived in feasible ability. For example, the ability to resist life risks, obtain opportunities and change life conditions is deprived, that is, there is poverty in multiple dimensions.28 Especially after 2020, China has entered the “post-poverty alleviation era”, and it is a basic trend to adopt multidimensional poverty or multidimensional borderline poor households to measure relative poverty in the process of common prosperity.29,30 Absolute poverty in China has been historically resolved,31 while relative poverty is universal and long-term.32 However, the distinction between relative poverty and multidimensional poverty is vague and different.33 Therefore, the concept of multidimensional border poverty seems to be more appropriate in order to reflect the multidimensional concept of poverty based on different people and perspectives in a specific background.
In summary, some scholars have studied the characteristics of catastrophic health expenditures and multidimensional poverty itself in detail, but most of the studies on catastrophic health expenditures in China focus on the single-dimensional poverty centered on the level of economic income. With the advent of the post-poverty era in China after 2020, the research on the concept of poverty has expanded from a single dimension to a multi-dimension, and the occurrence of catastrophic health expenditure will lead to the increase of the risk of returning to poverty due to illness. Therefore, it is necessary to explore the risk characteristics of catastrophic health expenditures among borderline poor households in China in order to provide suggestions for future policies.
Theoretical Hypothesis and Research Design
Core Concept Definition
Catastrophic Health Expenditure
It refers to the medical expenditure that exceeds a certain level of the patient’s income, that is, when the medical expenditure generated for some reason exceeds a certain critical value of the family’s ability to pay, it is considered to have produced catastrophic medical expenditure. According to the research of WHO, this critical value is selected as 40%.9 Since then, scholars have mainly carried out research based on this critical value.
Multidimensional Borderline Poor Households
Multidimensional borderline poor households is mainly measured by the A-F method, and the “double boundary” method is generally used, that is, single dimension poverty identification and multidimensional borderline poor households identification. Firstly, set the multidimensional borderline poor households dimension, index j and corresponding weight qj(0 < qj < 1) in time t. Then, the value of individual i on index j is identified  , which is unit poverty identification. Finally, multiplied and summed with the weight qj and
, which is unit poverty identification. Finally, multiplied and summed with the weight qj and  get
get  , where
, where  reflects the extent of deprivation of individual i. If
reflects the extent of deprivation of individual i. If  exceeds a certain critical value, the individual is said to be in multidimensional borderline poor households. If
exceeds a certain critical value, the individual is said to be in multidimensional borderline poor households. If  does not exceed the critical value, it is called non-multidimensional borderline poor households.
does not exceed the critical value, it is called non-multidimensional borderline poor households.
Research Hypothesis
In this paper, a binary Logit model (Formula 1) is used to explore the factors influencing catastrophic health expenditure.

where, Y is a dichotomous variable, that is, whether catastrophic health expenditure occur; Xi is the specific influencing factor; β0 and βi are regression coefficients. εi is the random perturbation term.
Based on this, this paper proposes the following hypotheses on the basis of other scholars’ research:
Hypothesis 1: The income level, whether children provide financial support to the elderly, and whether have Medical insurance or Endowment insurance significantly affect the level of catastrophic health expenditure. Hypothesis 2: Multidimensional borderline poor households face a significantly higher risk of catastrophic health expenditures than non-multidimensional borderline poor households. Hypothesis 3: The risk of catastrophic health expenditures is significantly higher for multidimensional boundaries poor households in rural areas than in urban areas.
Variable Declaration
Dependent Variable
The dependent variable selected in this study is whether a family has a catastrophic health expenditure. Catastrophic health expenditure(CHE) refers to the medical expenditure that exceeds a certain level of the patient’s income, that is, when the medical expenditure generated for some reason exceeds a certain critical value of the family’s ability to pay, it is considered to have produced catastrophic health expenditure. WHO9 defines that out-of-pocket medical expense accounts for 40% of household consumption and more could be regarded as CHE. As mentioned above, a catastrophic health expenditure occurs when the out-of-pocket medical expenditure accounts for 40% or more of its affordability, and the value is 1. Otherwise 0 is a dichotomous variable. The specific calculation is shown in Formula 2 and 3:


where, OOPEi refers to the out-of-pocket medical expenses of individual i; ctpi refers to the affordability of individual i. It is the difference between the total consumption expenditure of individual i and the expenditure on food purchase, as well as the non-food expenditure of individual i. If the above formula is true, catastrophic health expenditure are considered.
Independent Variables
The core independent variable is weighted average level of deprivation (WALD) of the household. In this paper, WALD was measured by referring to relevant indexes of calculating the Multidimensional Poverty Index (MPI, Human Development Report 2010) (as shown in Table 1) and other studies.34 The formula for calculating the Multidimensional Poverty Index (MPI) was first proposed in the Human Development Report 2010 (see Formula 4–6).
 |
Table 1 Dimension, Index, Deprivation Critical Value and Weight Setting of Multidimensional Poor Index |



where, H is the ratio of poverty population, which refers to the proportion of poverty population in multidimensional borders. q is the number of poverty-stricken people in multidimensional boundary; n is the total population; A is poverty intensity, which reflects the ratio of the average deprivation number of poor people to the number of weighted component indicators. c is the weighted average amount of deprivation; d is the number of indicators adopted and it is 8 in this study.
However, the MPI represents the proportion of people trapped in multidimensional borderline poor households, while the individual sample is directly matched by the weighted average number of family deprivation. This study refers to the studies of other scholars.35,36 The weighted average level of deprivation (WALD) was measured by seven indicators from four dimensions of economy, health, life and education level, with equal weight for each dimension. Multidimensional borderline poor households is identified only when it exceeds the critical value K. Since the change of critical value and weight does not affect MPI, the critical value K =0.3 is taken this time.
- Economic level. The commonly used dimension is income level, but asset poverty can measure structural poverty and random poverty, which cannot be measured by income poverty, and is the third-generation poverty measurement method.37 The index selected in this study is current assets, namely the sum of cash and deposits, and the income poverty line with current assets below 25% is considered as asset poverty.38 Since the statistical year of data used in this research is 2018, and the poverty standard in 2018 is 2995 yuan, the current assets less than 748.75 yuan are considered as asset poverty, and the value is 1. Otherwise 0.
- Health level. The respondents’ self-rated health responses were selected, and those who chose “bad” or “very bad” were identified as healthy and poor, with a value of 1. Select “Fine”, “good”, and “fair” and assign a value of 0.
- Living level. Four basic living indicators are selected: cooking fuel, running water facilities, bathing facilities, lighting facilities. For each of these metrics, if the answer is none, the value is assigned to 1; Otherwise 0.
- Education level. If the interviewee does not receive compulsory education, he/she is considered as educational poverty and is assigned a value of 1. Otherwise 0.
The weighted average level of deprivation (WALD) was calculated as shown in Formula 7:

where, cj refers to the weighted average number of individual i deprived; j represents a specific indicator, and qi represents the corresponding weight of the indicator. The four dimensions, corresponding indicators, deprivation critical value and weight allocation are shown in Table 1.
Control Variables
Referring to the research results of other scholars, variables selected in this study include: annual family income level, age, gender, marital status, urban and rural areas, whether children provide economic support, whether they have medical insurance and whether they have endowment insurance. Except age as a continuous variable, the other variables are dichotomous.
Data Source
All the data in this study are from the micro data of the 2018 National Baseline Survey of China Health and Retirement Longitudinal Survey (CHARLS). Due to the lag in the data release of domestic large micro databases, CHARLS released its latest data in September 2020, namely the data of 2018. CHARLS was presided over by the national development research institute of Peking University, Beijing university of Chinese Academy of Social Sciences research center row long-term tracking projects, the project is mainly to provide research data, the basis of an aging population survey for China to 45 years old and above 17,000 people in 10,000 elderly people in families, covering 150 units at the county level, 450 village-level units with detailed socio-economic data and high quality physical and mental health status data. The baseline survey was conducted in 2011 and samples have been followed every two to three years since.
In this paper, 3903 valid samples were obtained by eliminating some of the data samples under 45 years old, missing values and extreme outliers in the latest 2018 data sample. First, we use the logit model discussed the different effects of different factors such as WALD on catastrophic health expenditures(CHE). And then, Further discussed are the factors affecting CHE in different populations (Non-multidimensional borderline poor households group vs multidimensional borderline poor households group) and Rural-urban comparison.
Results
Statistical Description of Samples
There is difference between the multidimensional boundary poor and non-multidimensional boundary poor in the sample. Among them, the monthly per capita consumption expenditure of the multidimensional borderline poor households is about 1586 yuan, lower than that of the non-multidimensional borderline poor households 2318 yuan. However, the average monthly medical expenditure of the multidimensional borderline poor households was 1015 yuan, almost double the 527 yuan of the non-multidimensional borderline poor households. There is also a significant difference in the percentage of medical expenditure in per capita consumption between the two groups. The percentage of poor people in multi-dimensional border areas is as high as 64%, while the percentage of poor people in non-dimensional border areas is only 22.7%.
The above sample description indicates that the multidimensional boundary poor do face higher health care costs. Poor people in multidimensional border areas not only have poor economic conditions, but also spend most of their consumption on medical expenses. This is mainly reflected in the higher frequency of the multidimensional borderline poor households going to the outpatient clinic to buy medicine and hospitalization: their frequency of visiting the outpatient clinic in the past month is 0.472; The frequency of hospitalizations in the past year was 1.743. The data above show that poor people in multidimensional borders have worse health outcomes, resulting in higher out-of-pocket health expenditures and higher risk of catastrophic health expenditures. The mean annual income is between the poor and the middle, and the standard deviation of income is 1.121. The income level fluctuates greatly in the sample population.
Specific variables and detailed statistical description of samples are shown in Table 2.
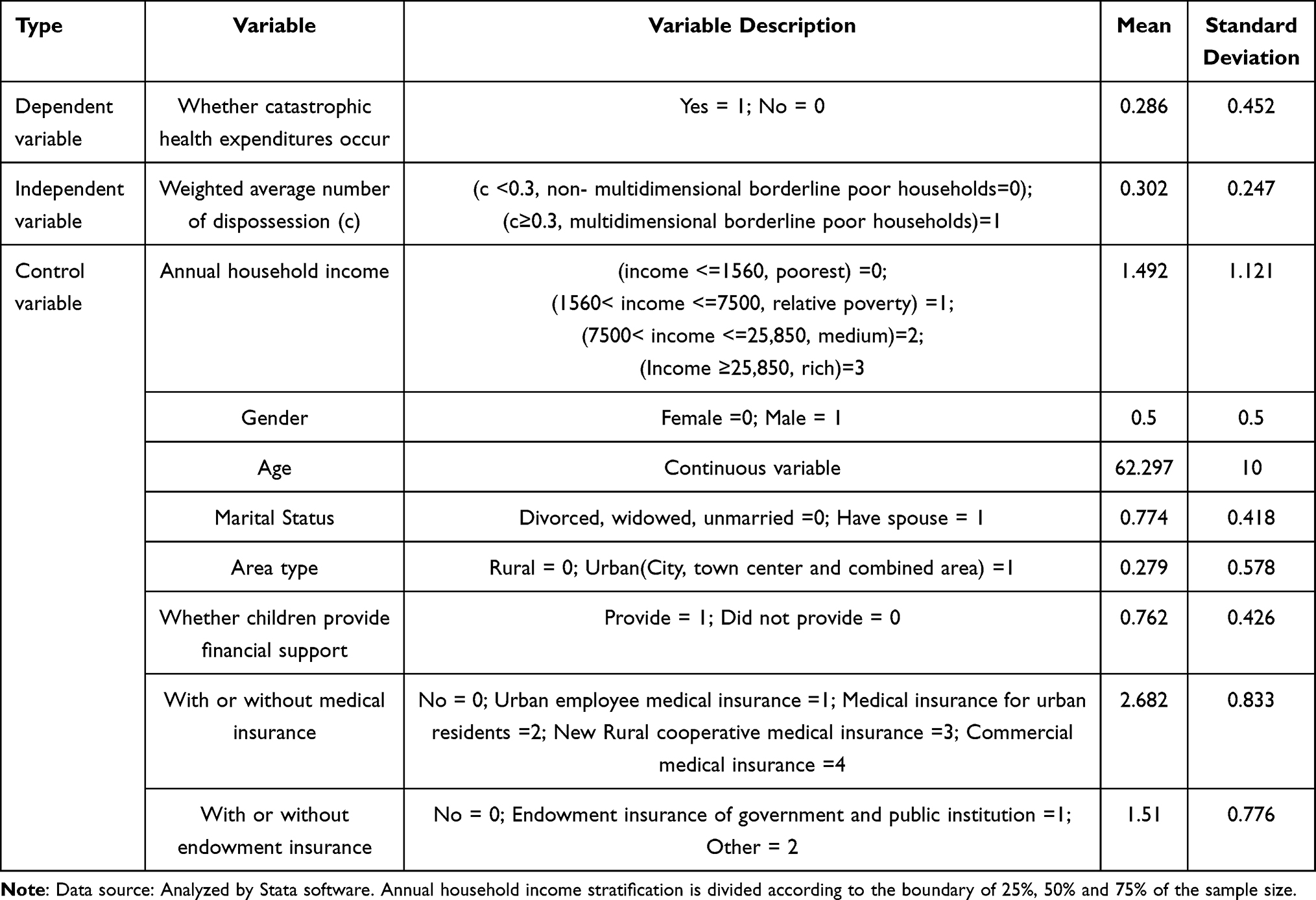 |
Table 2 Variable introduction and Descriptive Statistics(N=3903) |
Factors Influencing Catastrophic Health Expenditures
Table 3 shows the different effects of different factors on catastrophic health expenditures.
 |
Table 3 Regression Results of Factors Influencing Catastrophic Health Expenditure |
Income Level
There was no significant difference in the level of catastrophic health expenditure between the Relative poverty group and the Poorest group. Medium and Rich group were less likely to incur catastrophic health expenditure, and their risk was only 0.77 times higher than that of the poorest households (OR=0.77) and 0.53 times higher (OR=0.528).
Economic Support of Children
To some extent, the financial support provided by children adds a life and medical security to the middle-aged and elderly. Providing financial support significantly increased the risk of catastrophic health expenditure for middle-aged and older adults by 30% compared with no financial support from children (OR=1.3).
Insurance
Some medical insurance passed the significance test, but the endowment insurance did not. Medical insurance did not significantly reduce the incidence of catastrophic health expenditure compared with those without Medical insurance. The population with urban employees’ medical insurance and urban residents’ medical insurance is 1.7 times more likely to have catastrophic health expenditure than the population without medical insurance, which passes the significance test at the confidence level of P<0.1. While the new rural cooperative medical insurance and commercial medical insurance have no significant impact on the level of catastrophic health expenditure, but the risk is slightly higher than that of the population without medical insurance. In addition, compared with the group without Endowment insurance, 85.3% of the group with urban and rural residents’ Endowment insurance, new rural Endowment insurance and urban residents’ Endowment insurance were in the group without insurance (OR=0.853). However, Endowment insurance has no significant effect on the occurrence of catastrophic health expenditure.
Differences Among Poor Groups
Multidimensional borderline poor households groups have a significant impact on the occurrence of catastrophic health expenditure (P <0.01), and their risk of facing catastrophic health expenditure is twice that of non-multidimensional borderline poor households groups (OR=2.092).
Urban-Rural Differences
The risk of catastrophic health expenditure varies between urban and rural areas. Compared with rural areas, the risk probability in urban areas was only 82.7% (OR=0.827). However, in this regression test, there are only differences between urban and rural areas, and there is no significant difference.
Differences in Age, Gender and Marital Status
For older adults over 45 years of age, the risk of catastrophic health expenditure increased by 1.5% for each additional year (OR=1.015); In addition, men were less likely than women to face the risk of catastrophic health expenditure, only 79% of the time (P <0.01); Marital status also passed the significance test of the model, with catastrophic health expenditure 1.26 times higher in households with a spouse than in those with a single spouse (OR=1.258).
Heterogeneity Test: Households Group Comparison
As shown in Table 4, there are significant differences in the influencing factors of catastrophic health expenditure between the multidimensional borderline poor households and the non-multidimensional borderline poor households, so the differences between the two groups are further analyzed.
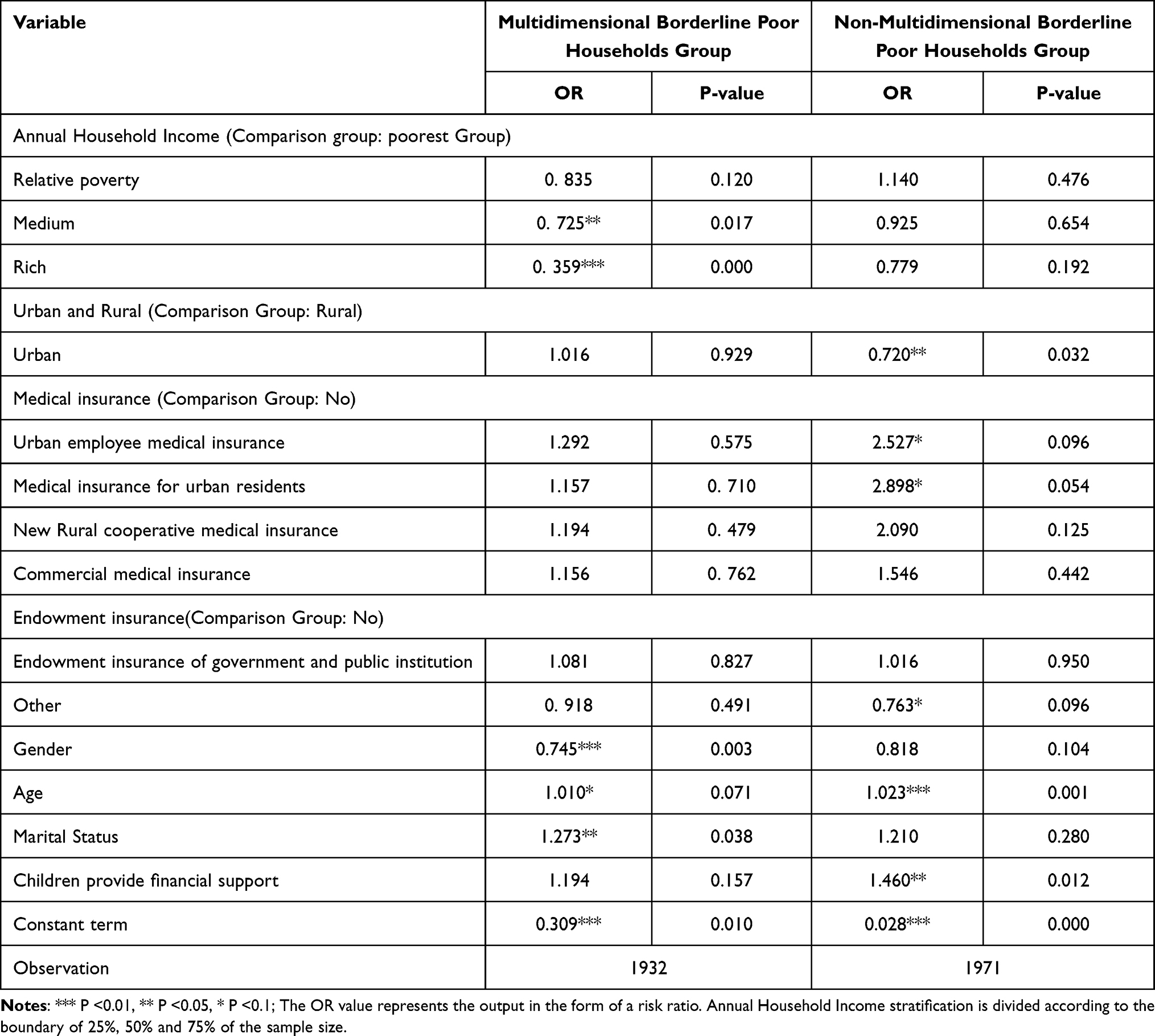 |
Table 4 Regression Results of Factors Affecting Catastrophic Health Expenditure of Different Populations |
Income Level
The regression results showed that the higher the income, the lower the risk of catastrophic health expenditure, regardless of the multidimensional borderline poor households group, but this difference was more obvious in the multidimensional borderline poor households group. The income level of the multidimensional borderline poor households group passed the significance test, which was consistent with the conclusion in Table 3, but the difference continued to expand. The risk of catastrophic health expenditure was only 72.5% (OR=0.725) and 35.9% (OR=0.359) in the middle and wealthy groups compared with the poorest group. However, for the non-multidimensional boundary poor group, income level did not significantly affect the level of catastrophic health expenditure.
Economic Support of Children
The impact of financial support from children on catastrophic health expenditure did not differ significantly between the two groups, making both expenditures more risky. The risk of catastrophic health expenditure increased 19.4% (OR=1.194) and 46% (OR=1.460) in the multidimensional and non-multidimensional boundary poor groups, respectively, compared with no financial support from their children.
Insurance
Table 4 shows that different types of medical insurance increase the risk of catastrophic health expenditure to different degrees, but the degree is different, which is consistent with the conclusion in Table 3. Especially in the non-multidimensional borderline poor households group, the medical insurance of urban workers and urban residents passed the test at the significance level of P <0.1, and the risk of catastrophic health expenditure with these two kinds of insurance was 2.527 times (OR=2.527) and 2.898 times (OR=2.898), respectively, than that of the group without medical insurance.
Urban-Rural Differences
The rural-urban sub-regression results of the multidimensional borderline poor households group showed that the risk of catastrophic health expenditure was about 1.6% higher in urban areas than in rural areas (OR=1.016). The difference between urban and rural areas in the non-multidimensional borderline poor households group was consistent with the regression conclusion in Table 3. The risk of catastrophic health expenditure for urban people in the non-multidimensional borderline poor households group was only 72% of that for rural people (P <0.05).
Differences in Age, Gender and Marital Status
The multidimensional and non-multidimensional borderline poor households groups showed the same overall characteristics, that is, female individuals and individuals with spouses face lower levels of catastrophic health expenditures. For the multidimensional borderline poor households group that passed the level of significance test, the risk of catastrophic health expenditure for males was only 74.5% of that for females (OR=0.745). The risk level of individuals with a spouse was 1.273 times higher than that of individuals without a spouse (OR=1.273).
Heterogeneity Test: Rural-Urban Comparison
In the previous two regressions, rural areas were generally more prone to catastrophic health expenditure than urban areas, which was consistent with previous studies.17,39 However, the regression analysis of the factors affecting catastrophic health expenditure of different groups shows that poor families in multi-dimensional boundary areas in urban areas are at greater risk of catastrophic health expenditure. Therefore, a sub-regression analysis was conducted on the urban and rural areas of multidimensional borderline poor households to further understand the difference in the risk of catastrophic health expenditure faced by multidimensional borderline poor households in urban and rural areas (Table 5).
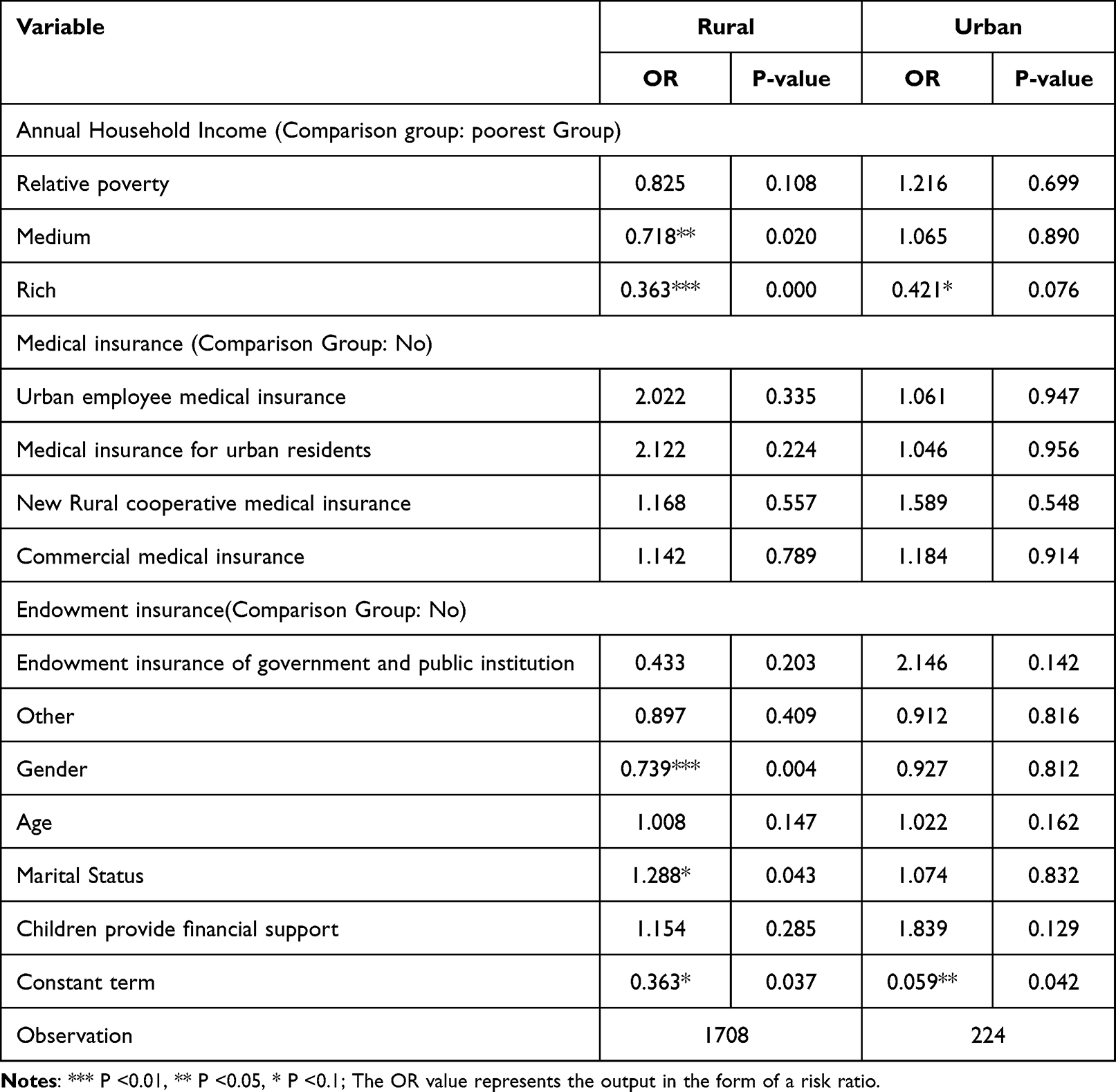 |
Table 5 Sub-Regional Regression Results of Factors Influencing Catastrophic Health Expenditures of Multidimensional Poor Households |
Income Level
The impact of income level of Multidimensional borderline poor households on catastrophic health expenditure varies between urban and rural areas. Especially in rural areas, the impact of income level shows great differences. With the increase of income level, the risk of catastrophic health expenditure for poor families in multi-dimensional boundary areas increases first and then decreases. In rural areas, the risk decreased with the increase of income level. The Medium group and the Rich group passed the test at the significance level of P <0.05 and P <0.01, and their risk of facing catastrophic health expenditure was only 71.8% (0.718) and 36.3% of that in the Poorest group.
Economic Support of Children
Financial support from children increases the risk of catastrophic health expenditures in both urban and rural areas. The level of catastrophic health expenditure was 1.839 times (OR=1.839) and 1.154 times (OR=1.154) in rural and urban areas, respectively, compared with the lack of financial support from children. But it does not pass the significance test.
Insurance
Neither type of Medical insurance mitigates the risk of catastrophic health expenditures for the multidimensional poor, but rather increases it. However, the performance of Endowment insurance is different. Taking the multidimensional borderline poor households group in rural areas as an example, compared with the group without Endowment insurance, the risk of catastrophic health expenditure in the group with government, public institution OR employee Endowment insurance was only 43.3% (OR=0.433). The risk of catastrophic health expenditure was only 89.7 (OR=0.897) in the group with urban residents’ insurance, new rural cooperative medical insurance and endowment insurance for urban and rural residents.
Differences in Gender and Marital Status
In urban areas, individual differences among middle-aged and elderly people in multidimensional borderline poor households do not significantly affect the level of catastrophic health expenditures. However, in rural areas, gender and marital status were still important factors influencing the level of catastrophic health expenditure in the multidimensional border poverty group: males were 73.9% more likely to face catastrophic health expenditure than females (P <0.01); The risk of individuals with spouse was 1.288 times higher than that of individuals without spouse (P <0.1).
Summary of Regression Results: Responses to Research Hypothesis
Part of Hypothesis 1 is true. In three regressions, the income level of the multidimensional borderline poor households group significantly affected the level of catastrophic health expenditures. The lower the income level, the higher the probability of catastrophic medical expenditure risk, showing an obvious “love poverty” effect. Only in the overall sample and in the non-multidimensional borderline poor did financial support from children significantly affect the level of catastrophic health expenditures. The results show that the financial support provided by children, namely supporting support, has a positive impact on the middle-aged and elderly, which increases the medical expenditure and increases the risk of catastrophic medical expenditure. However, in the three regressions of Medical insurance and Endowment insurance, most of the results did not pass the significance test, and partial insurance increased the risk of catastrophic health expenditure. Therefore, only the income level hypothesis in hypothesis 1 is valid.
(2) Hypothesis 2 is valid. In the first regression analysis, the level of catastrophic health expenditure in the multidimensional boundary poor group was significantly higher than that in the non-multidimensional boundary poor group, proving that poor families with multidimensional deprivation did indeed face a higher risk of catastrophic health expenditure. In the second regression analysis of the two groups, income differences and individual differences were important factors influencing catastrophic health expenditures in the multidimensional borderline poor households group.
(3) Hypothesis 3 is not valid, but the urban-rural difference exists objectively. In the first regression, the risk of catastrophic health expenditures in rural areas was higher than in urban areas, but the regression was not significant. In the second regression, only non-multidimensional boundary poor families showed significant urban-rural differences, and the urban-rural differences of multidimensional boundary poor groups were not significant, and even the catastrophic health expenditure level was higher in urban areas. In the third sub-regional regression of the multidimensional borderline poor households group, there are obvious differences between urban and rural areas in the multidimensional borderline poor households group.
Discussion and Policy Implications
Discussion
Multidimensional Borderline Poor Households are More Vulnerable to Catastrophic Health Expenditure Risks
In the empirical regression results, it can be seen that the multidimensional boundary poor are twice as likely to face catastrophic health expenditure as the non-multidimensional boundary poor. On the one hand, the disease treatment of multidimensional borderline poor households is more dependent on income, and the security mode is relatively simple. Therefore, the income level is a relatively important factor influencing the risk of catastrophic health expenditure, which is consistent with the research conclusions of other scholars.17 Although the contribution rate of income dimension to multidimensional border poverty is very low, the increase of income level will significantly reduce the risk of catastrophic health expenditure for multidimensional borderline poor households. In addition, for the multi-dimensional border poor in rural areas, their own conditions such as gender and marital status still have an impact on catastrophic health expenditures. After its feasible ability is limited, it is difficult to make a big change in its current living conditions without the help of external forces because it is faced with poverty in various dimensions. Moreover, it gets worse with age. On the other hand, income, gender and marital status had no significant impact on catastrophic health expenditures for the non-multidimensional borderline poor households. Therefore, the factors affecting catastrophic health expenditure of different populations are different, and objective differences should be taken into account when making policies.
The Risk of Catastrophic Health Care Expenditure for Multidimensional Borderline Poor Households Varies Significantly Between Urban and Rural Areas
In the sub-regression analysis of urban and rural differences, multiple factors in rural households significantly increase the level of catastrophic health expenditure, while only the income level passes significance. Compared to the multidimensional borderline poor households in rural areas, the risk of catastrophic health expenditures was only 82.7% in urban areas. In addition to the differences in income, living standards and other objective differences, rural areas also have a traditional ideological understanding of diseases, often “minor diseases are no need to treat, big diseases are no ability to treat”. The medical expenditure caused by chronic diseases is relatively average in each period of a certain period, while sudden serious diseases will greatly increase the medical expenditure of poor people in multidimensional border areas in a short term, and it is more likely to produce catastrophic health expenditure. Wang and Zhang17 and Liu and Zhang40 all confirmed that poor rural households face a higher risk of catastrophic health expenditure. Therefore, the analysis of catastrophic health expenditure in rural areas is still the focus of academic research in the future.
The Insurance System Has an Obvious Protective Effect on Non-Multidimensional Boundary Poor Households
In the regression results, only part of the medical insurance and endowment insurance of the non-multidimensional borderline poor households n passed the significance test, indicating that the coverage of the insurance system is for the population with certain foundation in all aspects. There is disagreement about the impact of Medical insurance on catastrophic health expenditure, and most studies agree with this study. Wang and Xu27 concluded that although complete coverage of basic medical insurance has realized in China, but still unable to effectively resist the rural households catastrophic health expenditure risk occurs when a serious illness due to the existence of moral hazard. Wang and Zhang17 found that the per capita guarantee level of residents’ medical insurance has no significant impact on the catastrophic health expenditure of poor families. But some scholars disagree. Ding and You19 argue that the different medical insurance to reduce the incidence of catastrophic health expenditure and the intensity of obvious differences, such as city as compared to the city in risks and new farming can effectively reduce the incidence of catastrophic health expenditure and the occurring intensity. Endowment insurance mainly alleviates the burden of out-of-pocket expenditures through income effect.41 Our study supports this idea.
Policy Implications
This paper empirically analyzes the impact of multidimensional border poverty on the risk of catastrophic health expenditure and draws the following enlightenment. Firstly, the allocation of health system resources should be tilted towards the multidimensional borderline poor households. Compared with non-multidimensional borderline poor households, multidimensional borderline poor households have worse economic conditions, and it is difficult to improve their current living conditions due to their limited “feasible ability”. Out-of-pocket medical expenditures of the multidimensional borderline poor households account for 64% of their consumption expenditure, and the risk of catastrophic health expenditure is twice that of the non-multidimensional borderline poor households. People living in multidimensional border poverty are more likely to suffer catastrophic health expenditure, especially without financial support from their children. The reason may be that their feasible ability is limited, and they need to be more careful in budgeting or do not choose medical treatment if it is not necessary. However, their poorer quality of life leads to more severe chronic diseases as people age, leading to catastrophic health expenditure. Therefore, there is a need to provide more welfare subsidies for out-of-pocket medical expenditures of the multidimensional borderline poor households.
Secondly, the government should strengthen the insurance system for the multidimensional borderline poor households and further expand the coverage of endowment insurance. In this study, neither medical insurance nor endowment insurance passed the significance test, and only had a certain protective effect on non-multidimensional borderline poor households. It shows that insurance does not play a significant role in curbing the occurrence of catastrophic health expenditure, and some scholars even concluded that basic medical insurance may increase the probability of catastrophic health expenditure and serious disease medical expenditures.27 This clearly defeats the purpose of the insurance system. For example, the new rural cooperative medical insurance for rural groups requires participants to pay their own medical expenses in advance before reimbursing them later. Without the participation of their children, many middle-aged and elderly people do not know how to reimburse their bills, which is more likely to cause catastrophic health expenditure. In the aspect of financing, endowment insurance for employing unit workers, the company bears more premiums. For most workers, they need to pay the premium in full. On the one hand, poor people in multi-dimensional border areas may not have enough ability to pay due to their economic conditions. On the other hand, they may not have the awareness of this aspect and cannot be covered by the Endowment insurance system when they need medical treatment.
Data Sharing Statement
Please refer to: http://charls.pku.edu.cn/index.html. More data that if the reader has a personal request, we will provide it to him.
Ethics Approval and Consent to Participate
The data of this study came from China Health and Retirement Longitudinal Survey (CHARLS), which Peking University sponsored. It was ethical reviewed by Biomedical Ethics Committee, Peking University, Ethics Review and Approval No. IRB00001052-11015. We also obtain the confirmation of the need for ethical applications was waived by Peking University and CHARLS Research Group, since CHARLS is an open and accessible (publicly-available) database, and the authors only used the data for academic research.
Acknowledgment
Thanks to The National School of Development and The Chinese Center for Social Science Surveys at Peking University for providing CHARLS data. We also thank Miss Haoran Yang of Chongqing Technology and Business University for her help in the initial data collation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This paper is a phased achievement of The National Social Science Fund of China: Research on the blocking mechanism of the Borderline poor families returning to poverty due to illness, No: 20BJY057.
Disclosure
The authors declare that they have no competing interests.
References
1. Xu X, Wang Q, Li C. The Impact of Dependency Burden on Urban Household Health Expenditure and Its Regional Heterogeneity in China: based on Quantile Regression Method. Front Public Health. 2022;10(10):876088. doi:10.3389/fpubh.2022.876088
2. Jakovljevic M, Sugahara T, Timofeyev Y, Rancic N. Predictors of (in)efficiencies of Healthcare Expenditure Among the Leading Asian Economies - Comparison of OECD and Non-OECD Nations. Risk Manag Healthc Policy. 2020;13:2261–2280. doi:10.2147/RMHP.S266386
3. Jakovljevic M, Lamnisos D, Westerman R, et al. Future health spending forecast in leading emerging BRICS markets in 2030: health policy implications. Health Res Policy Sys. 2022;20(1):23. doi:10.1186/s12961-022-00822-5
4. Li Y, Wu Q, Xu L, et al. Factors affecting catastrophic health expenditure and impoverishment from medical expenses in China: policy implications of universal health insurance. Bull World Health Organ. 2012;90(9):664–671. doi:10.2471/BLT.12.102178
5. Mohanty SK, Agrawal NK, Mahapatra B, et al. Multidimensional poverty and catastrophic health spending in the mountainous regions of Myanmar, Nepal and India. Int J Equity Health. 2017;16(1):21. doi:10.1186/s12939-016-0514-6
6. Xu X, Yang H, Theoretical Model LC. Actual Characteristics of Air Pollution Affecting Health Cost: a Review. Int J Environ Res Public Health. 2022;19:3532. doi:10.3390/ijerph19063532
7. Jakovljevic M, Arsenijevic J, Pavlova M, Verhaeghe N, Laaser U, Groot W. Within the triangle of healthcare legacies: comparing the performance of South-Eastern European health systems. J Med Econ. 2017;20(5):483–492. doi:10.1080/13696998.2016.1277228
8. Jakovljevic M. Therapeutic innovations: the future of health economics and outcomes research – increasing role of the Asia-Pacific. J Med Econ. 2021;24. doi:10.1080/13696998.2021.2014164
9. World Health Organization. The World Health Report 2000. Health systems: improving performance. Geneva: World Health Organization;2000.
10. Chu F. Research on catastrophic medical expenditurecatastrophic health expenditure. China Med Insurance. 2016;3:24–26+30.
11. Lei T, Zhang H. Multi-dimensional poverty measurement and structural decomposition in Rural China: an empirical study based on CFPS 2018. Social Security Res. 2021;14:1–8.
12. Zhu M, Yu X, Wang M, et al. on the relationship between family catastrophic health expenditure and critical illness insurance compensation in China. Eco Res J. 2017;52(09):133–149.
13. Yuan Q, Wu Y, Li F, et al. Economic status and catastrophic health expenditures in China in the last decade of health reform: a systematic review and meta-analysis. BMC Health Serv Res. 2021;21(1):600. doi:10.1186/s12913-021-06408-1
14. Lian L, Mao Z. A study on catastrophic health expenditure of poor urban families in China. Northwest Population. 2008;5:79–82+87.
15. Lu X, Ci Q. The influence factors of catastrophic health expenditure and medical assistance policy choice of poor families: based on Amartya Sen’s feasible capability perspective. Guangxi Soc Sci. 2017;8:152–157.
16. Xu K, Evans DB, Kawabata K, et al. Household catastrophic health expenditure: a multi-country analysis. Lancet. 2003;362(9378):111–117. doi:10.1016/S0140-6736(03)13861-5
17. Wang Y, Zhang C. Risk and influencing factors of catastrophic health expenditure in poor rural households: based on 2018 CHARLS data. China Health Policy Res. 2021;14(01):44–49.
18. Yan JE, Nina H, Liao SM, et al. Changes and influencing factors of catastrophic health expenditure of rural households before and after the new Medical reform: based on a sample survey in Meixian County, Shaanxi Province. China Health Policy Res. 2013;6(02):30–33.
19. Ding J, You L. The impact of basic medical insurance on catastrophic health expenditure of the elderly. Insurance Res. 2019;12:98–107.
20. Ekman B. Catastrophic health payments and health insurance: some counterintuitive evidence from one low-income country. Health Policy (New York). 2007;83(2–3):304–313. doi:10.1016/j.healthpol.2007.02.004
21. Rasanathan K, Evans TG. Primary health care, the Declaration of Astana and COVID-19. World Health Org. 2020;98(11):801–808. doi:10.2471/BLT.20.252932
22. Pal R. Measuring incidence of catastrophic out-of-pocket health expenditure: with application to India. Int J Health Care Finance Econ. 2012;12(1):63–85. doi:10.1007/s10754-012-9103-4
23. Van Minh H, Kim Phuong NT, Saksena P, et al. Financial burden of household out-of pocket health expenditure in Viet Nam: findings from the National Living Standard Survey 2002–2010. Soc Sci Med. 2013;96:258–263. doi:10.1016/j.socscimed.2012.11.028
24. Proaño Falconi D, Bernabé E. Determinants of catastrophic healthcare expenditure in Peru. Int J Health Economics Manag. 2018;18(4):425–436. doi:10.1007/s10754-018-9245-0
25. Shahrawat R, Rao KD. Insured yet vulnerable: out-of-pocket payments and India’s poor. Health Policy Plan. 2012;27(3):213–221. doi:10.1093/heapol/czr029
26. Xie Y, Yang J. The effect of medical insurance coverage on the reduction of poverty due to illness. J Beijing Normal Univ. 2018;4:141–156.
27. Wang Y, Xu D. Can basic medical insurance reduce residents’ catastrophic health expenditure? Empirical analysis based on CHARLS data. Financial Theory Practice. 2019;2:87–94.
28. Sen A. Commodities and Capabilities. Amsterdam: North-Holland; 1985.
29. Lin K, Shen Q. Relative Standard of Absolute Poverty, Multi-dimensional poverty and Policy practice of large aid System Construction. Soc Dev Studies. 2020;7(03):48–60.
30. Zhu X, Duan C. Study on poverty of Migrant Workers from the perspective of “survival. Dev Risk Population Res. 2016;40(03):30–44.
31. Chen Z, Huang Y. Research on relative poverty governance and countermeasures in China. Contemporary Eco Sci. 2021;43(05):1–19.
32. Chen Z, Shen Y, Zhou Y. Absolute and Relative Changes of Rural Poverty in China-Also on the Setting of relative poverty Line. Manage World. 2013;1:67–75+77+76+187–188.
33. Cao Y, Ye Y. Research status and Frontier analysis of multidimensional relative poverty in. China Statistics Decision. 2021;37(16):33–37.
34. Alkire S, Apablaza M, Chakravarty S, et al. Measuring chronic multidimensional poverty. J Policy Modeling. 2017;39(6):983–1006. doi:10.1016/j.jpolmod.2017.05.020
35. Huang X, Feng C, Qin J, Wang X, Zhang T. Measuring China’s agricultural green total factor productivity and its drivers during 1998–2019. Sci Total Environ. 2022;829:54477. doi:10.1016/j.scitotenv.2022.154477
36. Li B, Zhang Q, Zhou Q, et al. A comparative analysis of income poverty and multidimensional poverty in China. J Quantitative Tech Eco. 2018;35(8):39–55.
37. Carter MR, Barrett CB. The economics of poverty traps and persistent poverty: an asset-based approach. J Dev Studies. 2006;42(2):178–199. doi:10.1080/00220380500405261
38. Bian S, Feng M, Sun Y. The analysis of household asset poverty in Rural China. China Population Sci. 2018;4:54–67+127.
39. Xu W, Chu F. Study on the level and Influencing factors of catastrophic health expenditure-Based on CHARLS Data. Social Security Res. 2018;5:64–72.
40. Liu S, Zhang Q. Measurement and influencing factors of catastrophic health expenditure of middle-aged and elderly families: an empirical study based on CHARLS Data. Population Southern China. 2020;35(02):67–80.
41. Ma C, Li Z, Sun Z, et al. The effect of pension on relieving medical burden of Rural Residents--Why income subsidy is better than medical insurance subsidy. China Industrial Eco. 2021;4:43–61.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.