")
Back to Journals » Vascular Health and Risk Management » Volume 18
Risk Assessment of Death of Tumor-Related PTE by CAR Combined with DD Detection
Authors Li X, Zheng J, Lu Y, Pan X
Received 7 March 2022
Accepted for publication 1 June 2022
Published 22 June 2022 Volume 2022:18 Pages 445—451
DOI https://doi.org/10.2147/VHRM.S365323
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Takashi Kajiya
Xinran Li,* Jiamin Zheng,* Ye Lu, Xiangtao Pan
Department of Hematology and Oncology, Suzhou Medical College of Soochow University, Taicang Hospital Affiliated of Soochow University, Taicang City, Jiangsu Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xiangtao Pan, Department of Hematology and Oncology, Suzhou Medical College of Soochow University, Taicang Hospital Affiliated of Soochow University, Taicang City, Jiangsu Province, 215400, People’s Republic of China, Tel +86 18915768003, Email [email protected]
Objective: To investigate the risk of death in patients with tumor-related PTE (pulmonary thromboembolism) detected by CAR (C-reactive protein/albumin ratio) combined with DD (D-dimer).
Methods: The peripheral hematology and coagulation-related indexes of 109 patients with tumor-related PTE diagnosed by PTCA were retrospectively analyzed, and the differences in relationship indexes between tumor-related PTE patients with good prognosis and poor prognosis were compared and analyzed. The receiver operating characteristic curve (ROC) was used to analyze the risk of death in patients with tumor-related PTE by CAR and DD.
Results: ① The values of CAR and DD in the poor prognosis group were 3.90 ± 2.69 and 21.25 ± 21.20, respectively, which were significantly higher than those in the good prognosis group (1.66 ± 1.77, 9.53 ± 3.57) (P all < 0.01). ② WBC, NE and SII in tumor-related PTE patients with poor prognosis were significantly higher than those in patients with good prognosis, while Hb in patients with poor prognosis was significantly lower than that in patients with good prognosis. ③ There was a significant positive correlation between CAR and DD (P=0.018). ④ The values of CAR and DD in the death group were 4.07 ± 2.42 and 19.65 ± 20.48, respectively, which were significantly higher than those in the survival group (1.94 ± 2.12, 11.52 ± 15.84) (P all< 0.05). ⑤ The results of logistic regression analysis showed that both CAR (P=0.000) and DD (P=0.031) were independent prognostic factors in patients with tumor-related PTE. ⑥ CAR combined with DD had high sensitivity (77.8%) and specificity (83.5%), and the Youden index was 0.613. ⑦ The area under the receiver operating characteristic curve of CAR combined with DD was the largest (up to 0.806).
Conclusion: CAR and DD were highly expressed in patients with poor prognosis of tumor-related PTE. CAR combined with DD detection is helpful to improve the correct assessment of the risk of death in patients with tumor-related PTE.
Keywords: pulmonary thromboembolism, neutrophil/lymphocyte, C-reactive protein, albumin, C-reactive protein/albumin ratio, plasma D-dimer, risk assessment of death
Corrigendum for this paper has been published
Introduction
Pulmonary embolism is a group of diseases or clinical syndromes caused by various emboli blocking the pulmonary artery or its branches, including pulmonary thromboembolism (PTE), fat embolism syndrome, amniotic fluid embolism, air embolism and so on. PTE is the most common type of pulmonary embolism, which is caused by thrombus from the venous system or right heart to block the pulmonary artery or its branches, with pulmonary circulatory and respiratory dysfunction as the main clinical and pathophysiological features. The thrombus that causes PTE mainly comes from deep venous thrombosis (DVT). DVT and PTE are essentially the manifestations of a disease process in different parts and stages, both of which are called venous thromboembolism (VTE), and PTE is the most dangerous type of VTE.1 In the general population, the first incidence of DVT or PTE is estimated at 17 per 100,000 people per year. Cancer increases this risk by more than four times, chemotherapy by 6.5 times, and it is estimated that one in every 200 cancer patients gets sick each year. The incidence of VTE varied greatly in clinical trials and case series involving cancer patients, but generally confirmed an increased risk in this population.2 Cancer and its treatment are recognized risk factors for VTE. There is evidence that the absolute risk of VTE in cancer patients depends on the type of tumor, the stage or degree of cancer, and the treatment of antineoplastic drugs. The most common types of cancer in patients with thrombosis are breast cancer, colorectal cancer and lung cancer, reflecting the prevalence of these malignant tumors in the general population. If the potential prevalence rate is taken into account, pancreatic, ovarian and brain cancer are most closely related to thrombotic complications.3 Exploring and summarizing the suspicious risk factors is helpful to determine the existence or non-existence of tumor-related PTE.1
Recently, studies have shown that the C-reactive protein(CRP)/albumin ratio (CAR) is of great significance in judging the prognosis of malignant tumors.4–7 The CAR is a new marker, which is calculated by the ratio of these acute phase reactants.8 However, there are few reports on the prognosis of thrombotic diseases with CAR and plasma D-dimer (DD).9 Therefore, this study retrospectively analyzed the characteristics of peripheral hematology and blood coagulation indexes in 109 patients with tumor-related PTE, so as to explore the clinical value of CAR combined with DD in predicting the prognosis and risk assessment of death in patients with tumor-related PTE.
Materials and Methods
Materials
From January 1, 2015, to December 31, 2019, 270,983 patients were discharged from the hospital, including 433 patients with PTE diagnosed by CTPA, etc., and 109 patients with tumor-related PTE with complete data and clear prognosis records. There were 63 males and 46 females, aged 28–91 years, with an average age of 69 years. Amniotic fluid embolism, fat embolism, and other cases of non-venous thromboembolism were excluded. The medical record number, name, gender, age, inpatient department, primary disease, inducing factors, location, preventive measures, relevant inspection results, treatment methods and prognosis of all cases were collected.
This research was conducted in accordance with the Declaration of Helsinki. This study was approved by the Ethics Committee of Taicang Hospital Affiliated to Soochow University, and informed consent was signed with relevant personnel. We confirm that the data were anonymous or confidential.
Research Methods
According to the data of VTE cases hospitalized from January 1, 2015, to December 31, 2019, provided by the VTE network of our hospital, all relevant medical records were reviewed by the hospital’s medical record center, referring to ultrasound or CTPA, DD, C-reactive protein (CRP), prothrombin time (PT), thrombin time (TT), antithrombin III (AT-III, AT for short), fibrinogen (FB), international standardized ratio (INR), as well as hemoglobin (Hb), white blood cells (WBC), neutrophils (NE), lymphocytes (LY), monocytes (MO), and platelets (PLT) count and other test data results.
Grouping Methods
According to the prognosis of the patients, the patients were divided into good prognosis group (including cure and improvement, a total of 78 cases, accounting for 71.56%) and poor prognosis group (including 18 cases deteriorated to death and 13 cases were not cured, a total of 31 cases, accounting for 28.44%). The death group (18 deaths, accounting for 16.51%) and the survival group (all surviving cases except death, 91 cases, accounting for 83.49%). To make a comparative analysis.
Statistical Analysis
SPSS 23.0 software was used for statistical analysis. The measurement data between the two groups was compared by t-test and u-test, and the count data was compared by Pearson correlation analysis. Binary logistic regression was used to analyze whether and to what extent the elevation of CAR and DD in tumor-related PTE patients resulted in death. The diagnostic value of CAR and DD for the risk of death in patients with tumor-related PTE was analyzed by receiver operating characteristic curve (ROC), with P<0.05 being considered statistically significant.
Results
The Test results of CAR and Other Indicators in the Two Groups with Good Prognosis and Poor Prognosis
From Table 1, it can be seen that the specific hematological indexes, inflammatory indexes and coagulation indexes of 109 cases of tumor-related PTE patients with good prognosis group and poor group were compared and analyzed. The WBC, NE, neutrophil/lymphocyte (neutrophil to lymphocyte ratio, NLR), systemic immune inflammatory index (SII), DD, CRP and CAR values in the group were significantly lower than those in the poor prognosis group. Other indicators including LY, MO, lymphocyte/monocyte ratio (LMR), PLT and platelet/lymphocyte ratio (PLR) were not statistically significant.
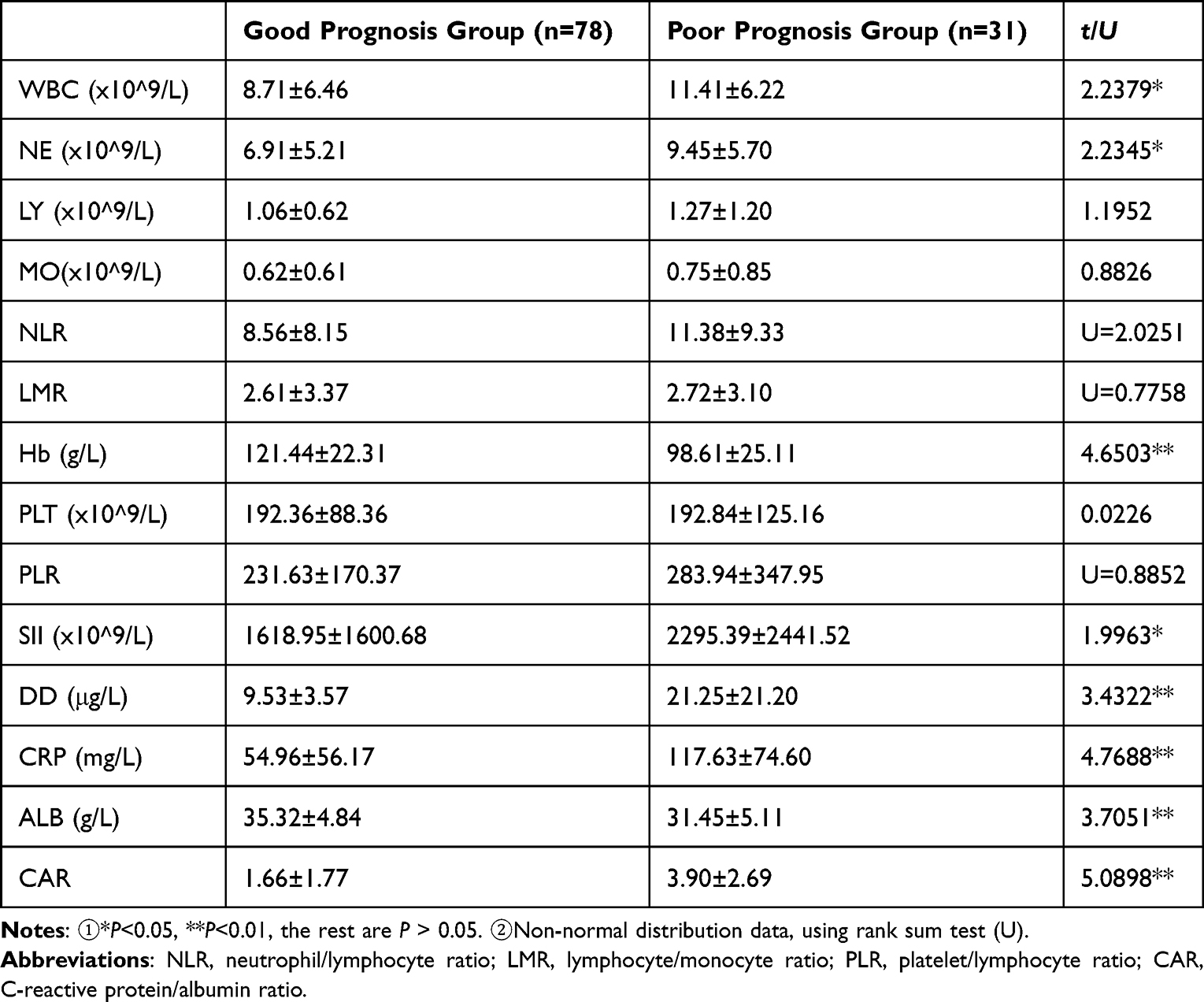 |
Table 1 Comparison of CAR and Other Indicators Between the Two Groups with Good Prognosis and Poor Prognosis in Tumor-Related PTE Patients |
Results of Correlation Analysis
Considering that there is statistical significance between WBC, NE, NLR, SII, DD, CRP and CRP/ALB values between the two groups of tumor-related PTE patients with good and poor prognosis, while CRP and albumin (ALB) constitute a new index (CRP/ALB, CAR), the correlation between CAR and DD, NLR, gender and age is analyzed. The specific results are shown in Table 2.
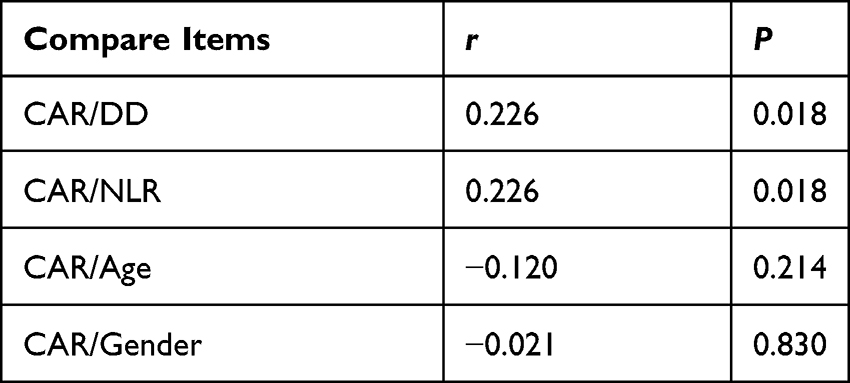 |
Table 2 Results of Correlation Analysis |
It can be seen from Table 3 that there is a significant correlation between CAR and DD and NLR (P all <0.05), and r=0.226 (r<0.3) indicates that the degree of correlation is weak. The correlation coefficient between CAR and age and gender was not statistically significant (P all >0.05).
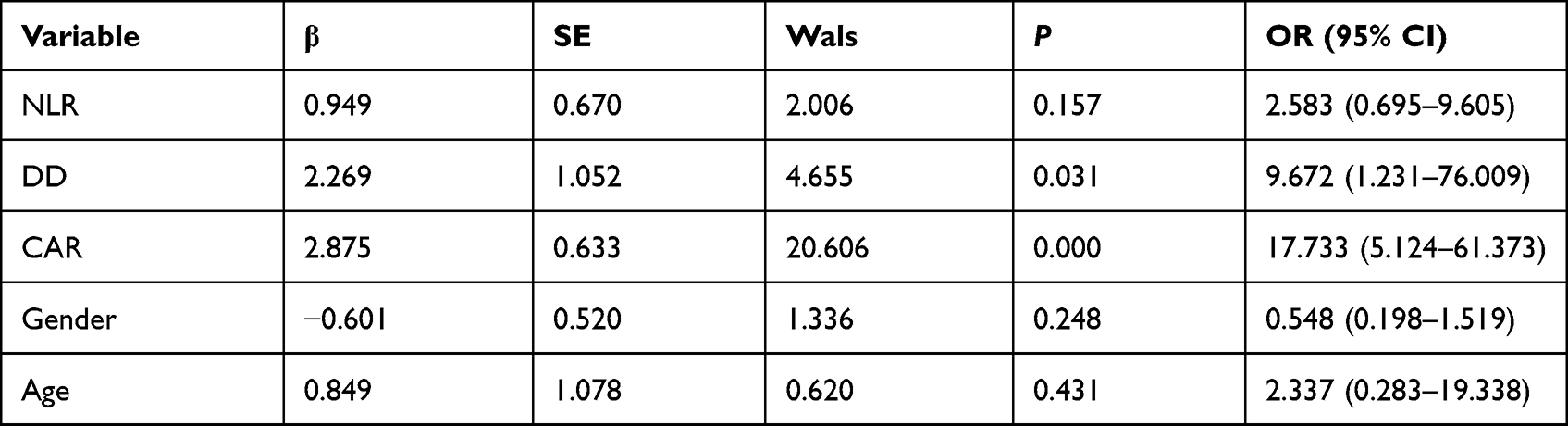 |
Table 3 Results of Logistic Regression Analysis |
Detection of CAR, DD and NLR in Survival Group and Death Group of Patients with Tumor-Related PTE
The detection results of various indexes in survival group and death group of 109 patients with tumor-related PTE are shown in Table 4.
 |
Table 4 Results of NLR, DD and CAR in Two Groups of Patients |
Logisitc Analysis of CAR, DD and Other Indicators in 109 Patients with Tumor-Related PTE
Taking CAR, DD, NLR, age and gender as covariates, and taking the death of tumor-related PTE patients as the dependent variable. The specific results are shown in Table 3.
Table 3 shows that CAR (P=0.000) and DD (P=0.031) are independent prognostic factors in patients with tumor-related PTE.
Combination or Separate Detection of CAR and DD for Risk Assessment of Death in Patients with Tumor-Related PTE
The receiver operating curve (ROC) was used to analyze and calculate the AUV. The specific results are shown in Table 5 and Figure 1.
 |
Table 5 Assessment of the Risk of Death in PTE Patients by Detecting DD and CAR Alone and in Combination |
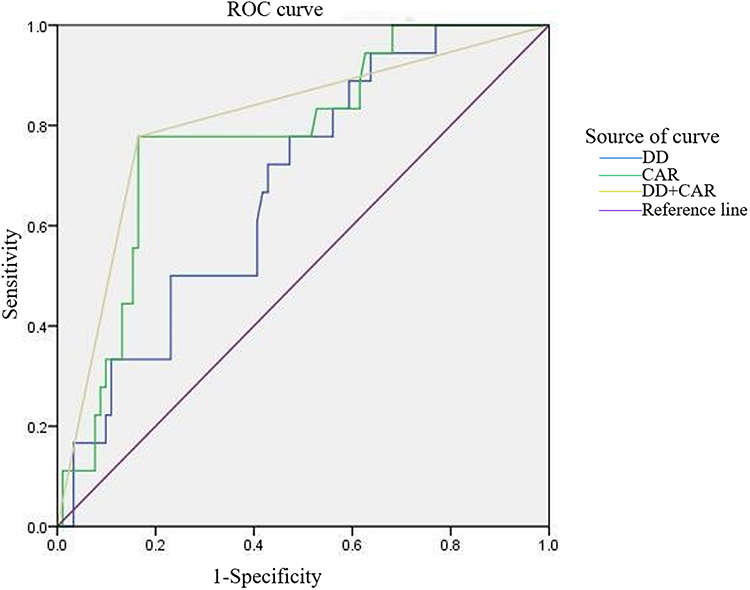 |
Figure 1 Risk assessment of death in patients with tumor-related PTE by single and combined detection of CAR and DD. |
As can be seen from Table 5, DD alone had the highest sensitivity (94.4%) but lower specificity (36.3%) in assessing the risk of death in patients. CAR combined with DD assessment had high specificity (83.5%), while having high sensitivity (77.8%). The area under the receiver operating characteristic curve of CAR combined with DD was the largest (up to 0.806).
Discussion
VTE is a common complication in patients with malignant diseases. Since Armand Trousseau first reported this observation in 1865, epidemiological and scientific data have supported a strong biological link between cancer and thrombosis. Recognizing that VTE in cancer patients has a different natural history from that in non-cancer patients, more studies have focused on the prevention and treatment of VTE in cancer patients.3 In spite of the advances in medical therapies, acute PTE is still a major cause of morbidity and mortality worldwide.10 The mortality rate of untreated PTE is 30%, and the short-term mortality rate with treatment can be reduced to 2% to 8%.11 Because there are many complications in tumor patients, there are many factors affecting the prognosis. Accurate and rapid diagnosis of PTE is essential to avoid significant morbidity and mortality in high-risk groups such as cancer patients.12,13
This study found that CAR, DD and CRP in patients with poor prognosis of tumor-related PTE were significantly higher than those in patients with good prognosis (NLR had no statistical significance because of its abnormal distribution, but it was also meaningful to change to rank sum test), suggesting that inflammatory reaction did exist in patients with tumor-related PTE. Previous studies have shown that changes in Hb are not the cause of PTE.14 Although the NLR of the group with good prognosis was significantly lower than that of the group with poor prognosis, and there was a positive correlation between NLR and CAR. However, further analysis showed that there was no statistical significance in NLR between the death group and the survival group, and logistic regression analysis showed that NLR, age and gender were not independent prognostic factors in patients with tumor-related PTE. Therefore, we do not combine NLR with CAR and DD for further study.
Many studies have shown the correlation between DD and tumor-related PTE. Qdaisat et al reviewed the records of patients who visited a large general cancer center during the study because they suspected PTE to determine whether cancer patients with normal DD levels could develop PTE. One thousand one hundred and fifty-six patients had PTE, of which only 35 (3.0%) had normal DD levels. There were 26 cases of acute PTE and 9 cases of subacute or chronic PTE. There were only 926 patients with normal DD and 4% (35 cases) of patients with normal DD developed PTE. After the activation of coagulation cascade, thrombus and DD were formed at the same time.15 This makes DD, the main biomarker of blood clot, an effective biomarker for the exclusion of VTE because of its high sensitivity.16 Cui et al determined the independent risk factors of PTE by stepwise logistic regression analysis. The results showed that high DD, chemotherapy, DVT, III–IV stage and adenocarcinoma were independent risk factors for PTE (P<0.05).1 The ROC curve results of this study showed that DD alone had the highest sensitivity (94.4%) in assessing the risk of death in patients, but the specificity was low (36.3%), and the Youden index was also low (0.307), so new indicators or integrated indicators need to be found. Combined detection to improve the diagnostic specificity of tumor-related PTE.
The level of Hb in the poor prognosis group of tumor-related PTE patients is lower than that in the good prognosis group, which is consistent with the results of our previous studies.17 Inflammation can lead to the high expression of hepcidin, which can lead to the inability of the body to use iron and lead to anemia.9 The values of WBC, NE and SII in the good prognosis group were significantly lower than those in the poor prognosis group, suggesting that the inflammatory response and immune function were abnormal in tumor-related PTE patients. This may explain why the NLR and CAR in the good prognosis group of tumor-related PTE patients were significantly lower than those in the poor prognosis group, which is consistent with the results reported in the literature.9,18–20
DD has the highest sensitivity (94.4%), but poor specificity (only 36.3%). The Youden index is only 0.307, indicating that it cannot correctly assess the risk of death in tumor-related PTE patients. The specificity of CAR was significantly higher than that of DD (83.5%), and the sensitivity was 77.8%. The Youden index is also up to 0.613, suggesting that it is of significance to evaluate the risk of death in patients with tumor-related PTE. After combining CAR and DD, although the sensitivity, specificity and Youden index were not significantly improved compared with CAR alone, the AUC increased to 0.806. It shows that CAR alone is helpful to evaluate the death risk of tumor-related PTE patients, and CAR combined with DD can further improve the value of evaluating the death risk of tumor-related PTE patients.
This study is a retrospective analysis, which is a single-center study, and does not fully include PTE underlying diseases and primary diseases as the research scope. The results may have limitations and biases. Therefore, we will combine multi-center expansion of the number of cases, unified diagnostic criteria and Parameter indicators, strict patient inclusion and exclusion criteria, and further research to clarify the significance of CAR combined with DD in tumor-related PTE death risk assessment.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Cui YQ, Tan XM, Liu B, et al. Analysis on risk factors of lung cancer complicated with pulmonary embolism. Clin Respir J. 2021;15(1):65–73. doi:10.1111/crj.13270
2. Nishioka J, Goodin S. Low-molecular-weight heparin in cancer-associated thrombosis: treatment, secondary prevention, and survival. J Oncol Pharm Pract. 2007;13(2):85–97. doi:10.1177/1078155207079169
3. Lee AY. Epidemiology and management of venous thromboembolism in patients with cancer. Thromb Res. 2003;110(4):167–172. doi:10.1016/S0049-3848(03)00347-5
4. Joffe L, Dwyer S, Glade Bender JL, et al. Nutritional status and clinical outcomes in pediatric patients with solid tumors: a systematic review of the literature. Semin Oncol. 2019;46(1):48–56. doi:10.1053/j.seminoncol.2018.11.005
5. Bairey O, Shacham-Abulafia A, Shpilberg O, et al. Serum albumin level at diagnosis of diffuse large B-cell lymphoma: an important simple prognostic factor. Hematol Oncol. 2016;34(4):184–192. doi:10.1002/hon.2233
6. Kinoshita A, Onoda H, Imai N, et al. The C-reactive protein/albumin ratio, a novel inflammation-based prognostic score, predicts outcomes in patients with hepatocellular carcinoma. Ann Surg Oncol. 2015;22(3):803–810. doi:10.1245/s10434-014-4048-0
7. Zhou T, Zhan J, Hong S, et al. Ratio of C-reactive protein/albumin is an inflammatory prognostic score for predicting overall survival of patients with small-cell lung cancer. Sci Rep. 2015;5:10481. doi:10.1038/srep10481
8. Efe SC, Ozdemir Candan O, Gundogan C, et al. Value of C-reactive protein/albumin ratio for predicting ischemia in myocardial perfusion scintigraphy. Mol Imaging Radionucl Ther. 2020;29(3):112–117. doi:10.4274/mirt.galenos.2020.88261
9. Shan T, Li X, Yan M, et al. Evaluation of prognosis and risk of death by neutrophil/lymphocyte ratio, C-reactive protein/albumin ratio and plasma D-dimer in patients with pulmonary thromboembolism. Int J Gen Med. 2021;14:9219–9225. doi:10.2147/IJGM.S343039
10. Oz A, Cinar T, Hayiroglu MI, et al. The predictive value of plasma osmolality for in-hospital mortality in patients with acute pulmonary embolism. Clin Respir J. 2019;13(3):174–183. doi:10.1111/crj.13001
11. Goldhaber SZ, Visani L, De Rosa M. Acute pulmonary embolism: clinical outcomes in the International Cooperative Pulmonary Embolism Registry (ICOPER). Lancet. 1999;353(9162):1386–1389. doi:10.1016/S0140-6736(98)07534-5
12. Khorana AA, Francis CW, Culakova E, et al. Thromboembolism is a leading cause of death in cancer patients receiving outpatient chemotherapy. J Thromb Haemost. 2007;5(3):632–634. doi:10.1111/j.1538-7836.2007.02374.x
13. Khorana AA, Francis CW, Culakova E, et al. Frequency, risk factors, and trends for venous thromboembolism among hospitalized cancer patients. Cancer. 2007;110(10):2339–2346. doi:10.1002/cncr.23062
14. Wu YY, Tan Y, Yan M, et al. Analysis of CRP, antithrombin, fibrinogen, and hematological changes in 433 patients with PTE. Int J Gen Med. 2021;14:7181–7185. doi:10.2147/IJGM.S333747
15. Adam SS, Key NS, Greenberg CS. D-dimer antigen: current concepts and future prospects. Blood. 2009;113(13):2878–2887. doi:10.1182/blood-2008-06-165845
16. Qdaisat A, Wu CC, Yeung SJ. Normal D-dimer levels in cancer patients with radiologic evidence of pulmonary embolism. J Thromb Thrombolysis. 2019;48(1):174–179. doi:10.1007/s11239-019-01863-4
17. Cheng Z, Yan M, Lu Y, et al. Expression of serum BMP6 and hepcidin in cancer-related anemia. Hematology. 2020;25(1):134–138. doi:10.1080/16078454.2020.1738098
18. Wiwanitkit V. Neutrophil to lymphocyte ratio in allergic rhinitis. Eur Arch Otorhinolaryngol. 2016;273(10):3443. doi:10.1007/s00405-015-3886-0
19. Lee H, Um SJ, Kim YS, et al. Association of the neutrophil-to-lymphocyte ratio with lung function and exacerbations in patients with chronic obstructive pulmonary disease. PLoS One. 2016;11(6):e0156511. doi:10.1371/journal.pone.0156511
20. Kolber W, Kusnierz-Cabala B, Maraj M, et al. Neutrophil to lymphocyte ratio at the early phase of acute pancreatitis correlates with serum urokinase-type plasminogen activator receptor and interleukin 6 and predicts organ failure. Folia Med Cracov. 2018;58(4):57–74.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.