")
Back to Archived Journals » Core Evidence » Volume 15
Riociguat in the Treatment of Chronic Thromboembolic Pulmonary Hypertension: An Evidence-Based Review of Its Place in Therapy
Authors Donaldson S , Ogunti R, Kibreab A, Mehari A
Received 31 May 2020
Accepted for publication 8 August 2020
Published 25 August 2020 Volume 2020:15 Pages 31—40
DOI https://doi.org/10.2147/CE.S172791
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Sahai Donaldson,1,2 Richard Ogunti,1 Angesom Kibreab,1,3 Alem Mehari1,2
1Howard University College of Medicine, Washington, DC, USA; 2Division of Pulmonary and Critical Care, Washington, DC, USA; 3Division of Gastroenterology and Hepatology, Washington, DC, USA
Correspondence: Alem Mehari
Department of Medicine, Division of Pulmonary and Critical Care, Howard University College of Medicine, 2041 Georgia Ave, NW, Washington, DC 20060, USA
Tel +1 202-865-6280
Fax +1 202-865-4669
Email [email protected]
Abstract: Chronic thromboembolic pulmonary hypertension (CTEPH) is classified as group-4 pulmonary hypertension caused by organized thrombi in pulmonary arteries and vasculopathy in nonoccluded areas leading to right heart failure and death. In addition to chronic anticoagulation therapy, each patient with CTEPH should receive treatment assessment starting with evaluation for pulmonary endarterectomy (PEA), which is the guideline recommended treatment. There is increasing experience with balloon pulmonary angioplasty (BPA) for inoperable patients; this option, like PEA, is reserved for specialized centers with expertise in this treatment method. Inoperable patients are candidates for targeted drug therapy. Riociguat remains the only approved medical therapy for CTEPH patients deemed inoperable or with persistent pulmonary hypertension after PEA. The role of riociguat therapy preoperatively or in tandem with BPA is currently under investigation. The purpose of this review is to evaluate the safety and efficacy of riociguat in the treatment of CTEPH.
Keywords: riociguat, CTEPH, PEA, PH
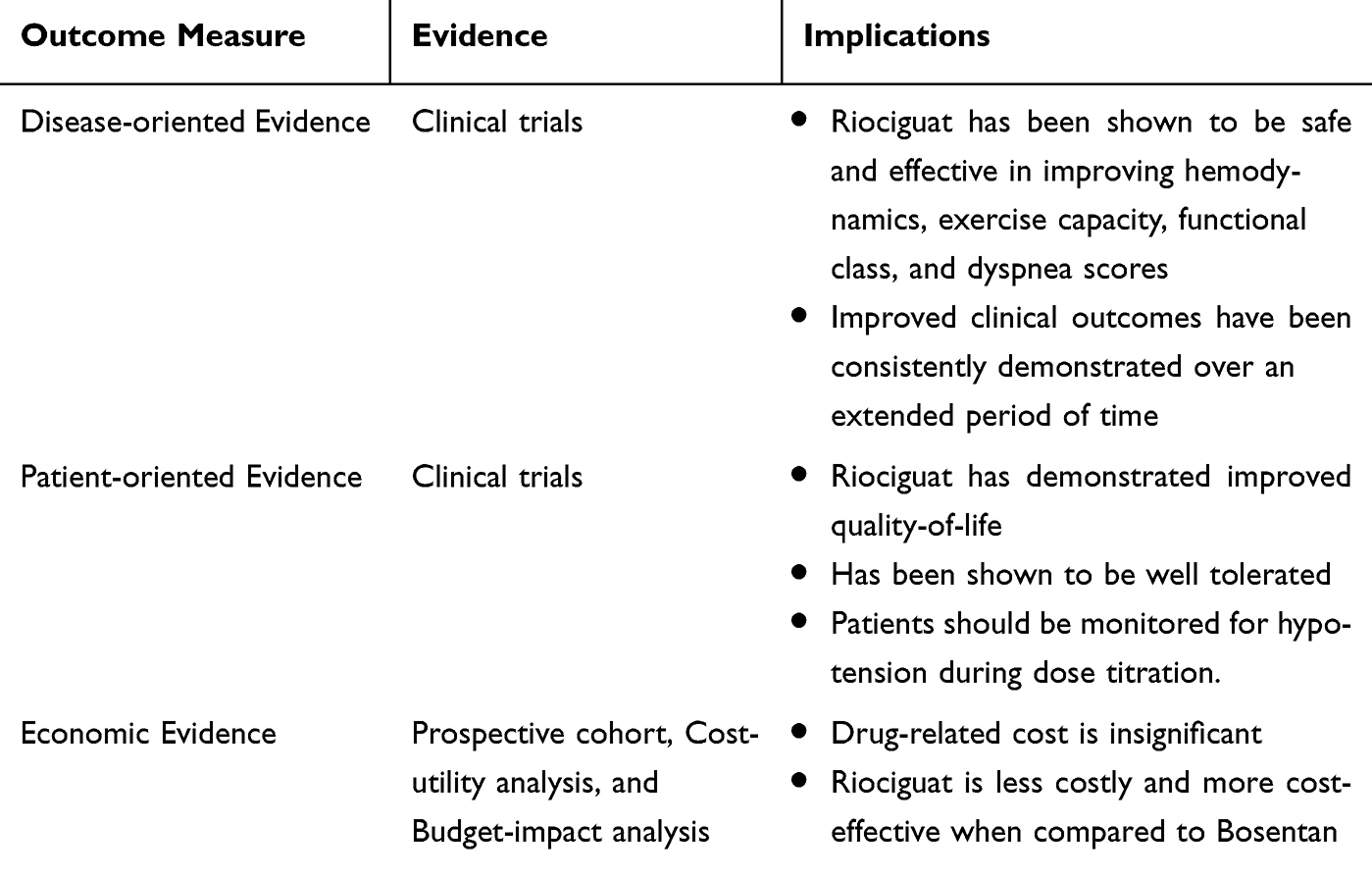
Core Evidence Clinical Impact Summary for Riociguat
 |
|
Introduction
Chronic thromboembolic pulmonary hypertension (CTEPH) is a rare, progressive pulmonary vascular disease that is usually a consequence of prior acute pulmonary embolism (PE). CTEPH is characterized by the nonresolution of organized thrombi in proximal or distal pulmonary arteries and micro vasculopathy in nonoccluded areas, leading to elevated pulmonary vascular resistance (PVR), progressive pulmonary hypertension (PH), and right heart failure, which can lead to death if left untreated.1,2
The pooled incidence of CTEPH following symptomatic acute PE was 3.4% (95% CI=2.1–4.4%).2,3 However, despite this association, 25% of CTEPH patients have no history of symptomatic PE.4,5 Several other thrombosis risk factors including circulating antiphospholipids, increased factor VIII, non-O blood groups, chronic inflammatory diseases, splenectomy, infections, and cancer are implicated.4,6,7
A diagnosis of CTEPH is based on the presence of precapillary PH measured by right heart catheterization, in combination with chronic flow-limiting thrombi within pulmonary arteries (with at least one segmental perfusion defect at scintigraphy and typical findings at conventional or computer tomography (CT) pulmonary angiography), after at least 3 months of effective anticoagulation.2,4 Pre-capillary PH is best defined by the concomitant presence of mPAP >20 mmHg, PAWP ≤15 mmHg, and PVR ≥3 WU by right heart catheterization at rest.8
CTEPH is classified as group 4 PH, the only subtype of PH that is potentially curable with pulmonary endarterectomy (PEA).9 The majority of operated on patients experience almost complete normalization of hemodynamics and improvements in symptoms. However, up to 40% of CTEPH patients are ineligible for PEA for various reasons, such as distal lesions, severe comorbidities, and surgeon expertise.2,9,10 Furthermore, 17–31% of operated on patients will develop persistent or recurrent PH.10
For such inoperable patients, refined balloon pulmonary angioplasty (BPA) is a new alternative option, and it may be another curative treatment in the future, particularly in combination with prior PEA.2 Recent studies have demonstrated that BPA can improve exercise capacity, heart function, and hemodynamics.11,12 Nevertheless, 23% of patients still suffer from persistent PH after BPA.13 Inoperable patients are candidates for targeted medical therapy. Riociguat is a Food and Drug Administration (FDA) approved medical therapy for patients with inoperable or persistent CTEPH despite surgery.14
Riociguat
Pulmonary vascular endothelial cells secrete nitric oxide (NO), an important vasoprotective factor, which diffuses into surrounding vascular smooth muscle cells (SMC). It then activates soluble guanylate cyclase (sGC) and thereby increases the intracellular concentration of cyclic guanosine monophosphate (cGMP). cGMP is an important intracellular second messenger, regulating vascular tone, proliferation, fibrosis and inflammation. cGMP leads to relaxation of vascular SMCs, thereby leading to vasodilation and increased blood flow.15 Furthermore, endothelial cell-derived NO inhibits vascular SMC proliferation and hypertrophy, and inhibits platelet aggregation and adhesion.16 A deficient NO-sGC-cGMP signaling seems to be involved in the development of PH and therefore strategies to increase NO in the pulmonary vasculature have been developed. Riociguat, a first-in-class stimulator of sGC, has a dual mode of action. Firstly, it sensitizes sGC to endogenous NO as well as it directly stimulates sGC independently of NO, this results in the activation of the enzyme converting guanosine triphosphate (GTP) to cGMP.17,18 cGMP then results in cellular influx of calcium by activation of the ligand-gated calcium channel, resulting in vasodilation and inhibition of smooth-muscle remodeling.17 Riociguat induces vasodilation and has antiproliferative, antifibrotic, and anti-inflammatory effects.19
Riociguat is available as an oral tablet, which may be safely stored at 77°F. There are five strengths: 0.5, 1, 1.5, 2, and 2.5 milligrams (mg), which allows for dosing flexibility.20 Dosing is individualized to avoid hypotension, with a usual starting dose of 1 mg orally three times daily (TID) for 2 weeks, with up titration by 0.5 mg every 2 weeks to a maximum dose of 2.5 mg TID if tolerated. It is 95% bound to plasma proteins, namely albumin and alpha-1-acidic glycoprotein.20
Riociguat’s bioavailability is approximately 94%, with peak plasma concentrations within 1.5 hours after oral intake. It’s half-life is approximately 12 hours.21 Pharmacokinetics is not affected by food intake, however antacids should not be taken within 1 hour after administration of riociguat.22 There is no evidence of time- or dose-dependent alterations of riociguat or its main active metabolite, M123 and it is eliminated via urine (40%) and feces (53%), mostly as metabolites. Smokers and patients taking bosentan showed higher clearance of riociguat necessitating dose adjustments.20,23 Riociguat was not studied in end-stage renal disease (ESRD) or severe hepatic impairment (Child Pugh C).20 There are no recommended dosing adjustments for creatinine clearance greater than 15 mL/min or Child-Pugh class A and B.
Riociguat can only be accessed via speciality pharmacies and females must comply with the Risk Evaluation and Mitigation Strategy (REMS) Program. It is known to be embryotoxic in rats and was also present in their lactation; as such it is currently not recommended while breastfeeding. It should not be used in pulmonary veno-occlusive disease (PVOD) or concomitantly with phosphodiesterase inhibitors due to cumulative hypotension. It is a strong CYP inhibitor, however no interaction was noted with warfarin or aspirin.20
Riociguat for the Treatment of CTEPH
CHEST-1 (The Chronic Thromboembolic Pulmonary Hypertension Soluble Guanylate Cyclase-Stimulator Trial-1) and PATENT-1 (The Pulmonary Arterial Hypertension sGC Stimulator Trial-1) were two randomized, double blind, multi-national, placebo-controlled Phase III studies, which lead to the approval of riociguat for the treatment of adult patients with WHO functional class II to III PAH, inoperable CTEPH and persistent/recurrent CTEPH after surgical treatment.14
The landmark CHEST-1 trial was a Phase 3 multicenter randomized control double-blinded trial that compared riociguat with placebo in 261 patients aged 18–80 years with inoperable or persistent/recurrent CTEPH post-PEA with WHO functional class I–IV.14 In the CHEST-1 study, riociguat significantly improved 6-minute walking distance (6MWD) (primary end-point) with a least-squares mean difference of +46 meters (95% CI=25–67 m; P<0.0001) compared with placebo at week 16. A number of secondary end-points were also significantly improved compared with placebo, including mean pulmonary vascular resistance (PVR) by −226 dyn/s/cm-5 (P<0.0001), a significant reduction of N-terminal prohormone of brain natriuretic peptide (NT-proBNP) levels (−291 ng/mL) (P<0.0001), and improvement in World Health Organization (WHO) functional class (FC) (P=0.003). There was a higher number of clinical worsening events in the placebo group vs the riociguat group (6% vs 2%, respectively), although this was not statistically significant. Riociguat showed a favorable benefit–risk profile, with the most frequently occurring serious adverse events (SAEs) in CHEST-1 being right ventricular failure (3% of patients in each group), syncope (2% in the riociguat group, and 3% in the placebo group) and hemoptysis (2% of the riociguat group).
The CHEST-2, open label extension study of CHEST-1, evaluated the long-term safety and tolerability of riociguat.10 This study included 155 riociguat-treated and 82 placebo-treated participants. All participants were 18–80 years with inoperable or persistent/recurrent CTEPH post-PEA with WHO functional class I–IV. Participants were enrolled for 2–232 weeks with median enrollment of 116 weeks. The median treatment duration was 75 weeks. At 1 year, 90% of participants were still receiving riociguat at 7.5 mg a day, supporting the long-term tolerability of riociguat. Only 3% of participants discontinued riociguat treatment due to adverse events (AEs). Serious AEs were reported in 5% of participants; among these AEs, the most common were syncope and hypotension (2% and 1%, respectively), both of which were properly handled in all cases. Hemoptysis or pulmonary hemorrhage was found in 3% of participants, and the authors advised clinicians to regularly evaluate the patient’s risk of pulmonary bleeding during riociguat therapy. No riociguat-related deaths were reported. Moreover, the former riociguat group showed better improvements in the 6MWD and WHO FC than the former placebo group, which supports the early administration of riociguat.
Based on the CHEST-1 and CHEST-2 studies, a post hoc analysis was done to assess the impact of riociguat on the REVEAL risk score (RRS) in CHEST-1 as well as the predictive value of change in RRS over time for long-term outcomes in CHEST-2. Riociguat use was associated with improvement in RRS (P<0.0001) and risk stratum (P<0.0001) at CHEST-1 week 16 compared with placebo from baseline. At baseline, mean±standard deviation (SD) RRS was 7.3±2.0 for the riociguat group and 7.1±1.9 for the placebo group. At CHEST-1 week 16, the mean±SD RRS changes from baseline in the riociguat group was −1.1±1.6 and −0.1±1.4 in the placebo group. A 1-point difference in RRS at baseline or CHEST-1 week 16 was associated with an approximate reduction of 30% in the relative risk of death in CHEST-2. In the first 12 weeks of CHEST-2, this improvement continued in patients who received riociguat in CHEST-1 and former placebo patients who started receiving riociguat in CHEST-2 also demonstrated improvement similar to riociguat patients in CHEST-1.24 The RRS as well as change in the RRS was shown to be a significant predictor of survival and clinical worsening-free survival over 2-years in CHEST-2.24
A Phase II long-term extension study sharing similar objectives with the CHEST-2 study included 41 inoperable CTEPH patients and 27 PAH patients.25 In contrast to 75 weeks in the CHEST-2 study,10 the median treatment duration was 77 months in this study. At the final data cutoff point, 56% of the CTEPH patients and 48% of the PAH patients remained on the treatment regimen. In 18 (44%) of CTEPH patients riociguat was discontinued because of adverse event in two (5%), death in six (15%), insufficient treatment response in one (2%), lost to follow-up in one (2%), noncompliance in one (2%), consent withdrawn in one (2%), and withdrawn by the investigator in six (15%) of the patients. In 14 (52%) of PAH patients riociguat was discontinued due to adverse event in four (15%), death in five (19%), consent withdrawn in three (11%), and withdrawn by the investigator in two (11%) patients. The safety profiles were similar to those in the CHEST studies.10,14 Improvements in the 6MWD and WHO FC observed in the initial stage of this study (3 months) were maintained for up to 48 months.
A phase IIIb CTEPH early access study also shared similar objectives with the CHEST-2 study which included 300 adults with CTEPH patients.26 Two hundred and sixteen were treatment-naive and 84 were switched from other PAH therapies, who were deemed technically inoperable or had persistent/recurrent PH after PEA. The primary outcome was safety and tolerability of riociguat. Exploratory efficacy endpoints such as WHO FC and 6MWD were assessed, however data collection for the latter was optional. The study reported that the safety, tolerability, and improvements in the 6MWD and WHO FC were comparable between switched and treatment-naïve patients. In 130 participants, 6MWD increased by 33±42 meters and in 264 participants WHO FC improved in 58 (22%), stabilized in 193 (73%), and worsened in 13 (5%) at week 12 in full analysis of both treatment-naive and switched subgroups.26 The safety profile was similar to that of the CHEST-1 and CHEST-2 studies.
In 2018, a prospective observational cohort study aimed to study the treatment of inoperable CTEPH with sequential treatment with riociguat and BPA.27 The primary outcomes were improvement in pulmonary hemodynamic parameters and WHO FC. A total of 123 participants were enrolled with inoperable CTEPH, and mean PAP of at least 25 mmHg with WHO FC ≥II that were considered BPA eligible. Only 69 participants completed 6 months follow-up post-BPA treatment. Of these, 36 patients were without targeted medication at the time of referral, which formed the study cohort and received targeted medical therapy, riociguat, before BPA. Of the 36 participants that took riociguat, when compared with baseline; the WHO FC improved by at least one class in 13 (36.1%) patients and remained unchanged in 23 (63.9%) patients (P=0.01) with increased 6MWD on an average of 20 meters (P=0.88) and hemodynamic improvements including, mPAP (49±12 mmHg vs 43±12 mmHg; P=0.003) and PVR (956±501 dyn·s·cm–4 vs 517 ± 279 dyn·s·cm–5; P=0.0001). NT-proBNP levels were significantly decreased compared to baseline (P=0.02). The median interval from commencing riociguat to first BPA was 5 months, with a median number of BPA sessions per patient of five. The median duration from first BPA to 6 month follow-up was 14 months. Combination therapy, riociguat and BPA, compared to riociguat alone after 3 months showed improvement in WHO FC in 34 (94.4%) participants. 6MWD improved on average 58 meters after combination therapy when compared to riociguat alone (after BPA=467±95 metersvs riociguat mean=409±102 meters, P=0.0001). Hemodynamic assessment showed significant improvement in mPAP (43±12 mmHg vs 34±14 mmHg; P=0.0001) and PVR (517±279 dyn·s·cm–5 vs 360±175 dyn·s·cm–5; P=0.0001). NT-proBNP was significantly decreased 6 months after BPA.
Riociguat use was assessed in a small retrospective case series of patients with sickle cell disease (SCD) related CTEPH.28 Following initiation of standard of care for SCD-PH: hydroxyurea or blood transfusion, supplemental oxygen to maintain oxygen saturation of 90% and diuretics, PH therapy with riociguat was commenced. Initial concerns about riociguat safety in view of a negative trial with sildenafil in Walk-PHaSST was discussed with participants. However, riociguat does not rely on NO only and was considered a suitable vasodilator. An average increase of 56.8 meters in 6MWD was reported. Two participants had an increase in 6MWD of 68 and 162 meters and three had increases of 7, 20, and 27 meters, with minimal increase attributed to preserved baseline in 6MWD. In two patients riociguat was discontinued due to side-effects, intractable headaches in one and pain crisis, nausea, vomiting in one with dose titration to 1.5 mg. Overall, five of six patients had improvements in right ventricular systolic pressure (RVSP), functional class, and NT-proBNP similar to CHEST-1. One participant had a lack of efficacy.
The impact of riociguat on hemodynamics, functional status from the above trials, and economic cost benefit analysis in CTEPH patients is further summarized in Table 1 for simplicity for readers.
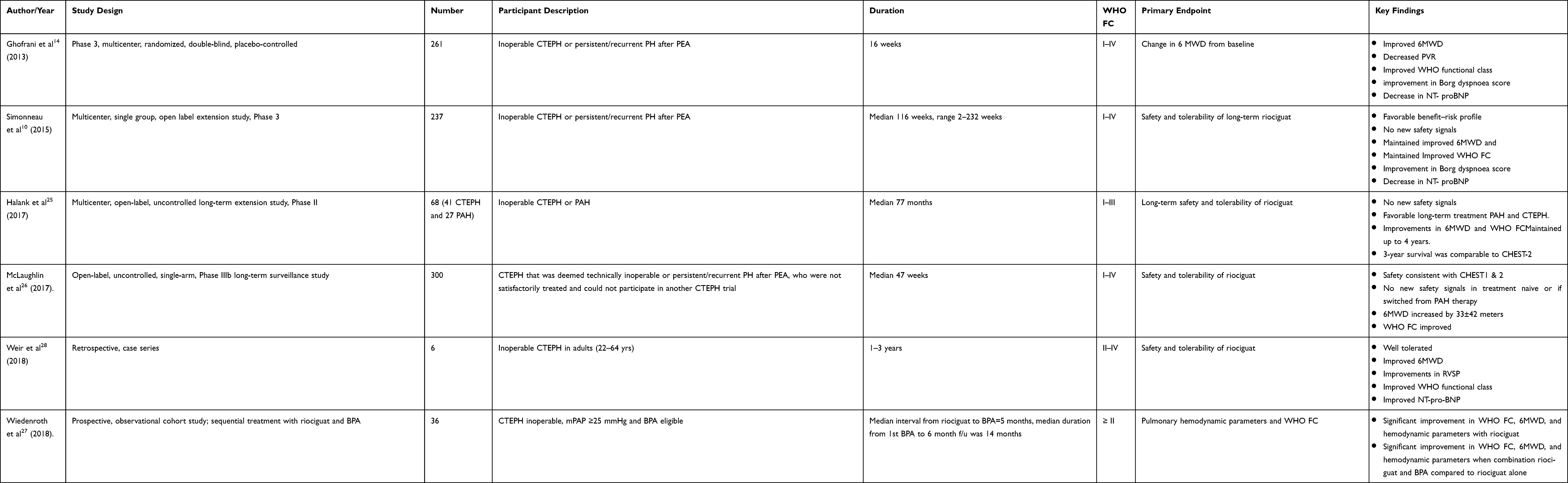 |
Table 1 Summary of Riociguat Impact on Hemodynamics, Functional Status, and Economic Cost in CTEPH Patients |
Riociguat’s role as a bridge to PEA is controversial, as concerns of delaying timely surgical referral for PEA which is the definitive therapy. However, its role as a bridge to PEA is to be assessed in a randomized, double-blind, placebo-controlled, multicenter, multinational, prospective study in patients with operable chronic thromboembolic pulmonary hypertension (CTEPH) prior to pulmonary endarterectomy (PEA) with high preoperative pulmonary vascular resistance (PVR). Patients will be randomized in a 1:1 ratio to receive riociguat or matching placebo for 3 months before undergoing PEA. The primary objective of this study is to assess the efficacy of riociguat on preoperative PVR compared to placebo in patients with operable CTEPH (ClinicalTrials.gov identifier NCT0327357).
Safety and Tolerability
Safety
Several studies have reported no new safety signals since riociguat’s FDA approval in 2013. Adverse events (AE) are reported in 93–96%. The most commonly reported AEs were nasopharyngitis (23–59%), peripheral edema (18–39%), dizziness (19–24%), diarrhea (14–17%) and cough (14–27%). The most commonly reported serious AEs (SAE) include syncope (2–17%), RV failure (3–15%), hypotension (9–24%), and hemoptysis/pulmonary hemorrhage (2–4%).10,25,26
Hemoptysis or pulmonary hemorrhage may be a sequelae of CTEPH, however it most commonly occurs in CTEPH patients on anticoagulation.
In the CHEST-1, hypotension occurred in 16 (9%) and syncope in four (2%) participants in the riociguat arm. SAE were reported in four (2%) participants, which included right heart decompensation, vaginal bleeding, overdose (attempted suicide), and worsening of general condition. None of which were thought to be related to the study. However, drug-related SAEs such as syncope (n=3), gastritis (n=1), acute renal failure (n=1), and hypotension (n=1) occurred. Hemoptysis or pulmonary hemorrhage was reported in 2% of the riociguat arm, with an exposure-adjusted rate of 5.9 cases per 100 patient-years.
In a phase II long-term extension (LTE) trial with both PAH and CTEPH patients (n=68) the long-term safety and tolerability of riociguat showed no new safety signals.25 Adverse events were reported by 93% of patients, with the most common being nasopharyngitis (57%) and peripheral edema (37%). SAEs were reported in 76% of all participants and the most common was RV failure, syncope, and worsening PH. Among CTEPH participants, RV failure, syncope, and worsening PH occurred in 15%, 17%, and 29% respectively. Hemoptysis was reported in the study but only among participants with PAH. A total of six (9%) participants discontinued riociguat due to AEs as the primary reason such as clinical worsening of PH (n=2), worsening PAH (n=1), pneumonia (n=1), hepatocellular carcinoma (n=1), and vascular event described as headache, flushing, and vertigo (n=1).
Following riociguat’s FDA approval in 2013, CHEST-2 followed 237 participants, of which 228 (96%) had an AE. However, serious adverse events occurred in only 100 (42%), and subsequent discontinuation in seven (3%). Special interest adverse events include hypotension, which occurred in 15 (6%) and syncope in 17 (7%) participants. Hemoptysis or pulmonary hemorrhage were reported as eight (3%) AEs and four (2%) SAEs, with an exposure-adjusted rate of 1.1 cases per 100 patient-years, notably less than in CHEST-1 initial reports of exposure-adjusted rate of 5.9 cases per 100 patient-years. Drug-related AEs were reported in 109 (46%) participants, of which the most common were dizziness (10%), dyspepsia (8%), and hypotension (5%). The most common AEs were nasopharyngitis (23%), dizziness (19%), peripheral edema (18%), diarrhea (14%), and cough (14%).10 Thirteen-people died during CHEST-2, however none were considered to be drug-related by investigators.
In a phase IIb open label, uncontrolled single arm long-term surveillance study that enrolled 300 CTEPH participants, of which 216 were treatment-naive and 84 were switched from other pulmonary arterial hypertension therapies,26 the safety profile was consistent with CHEST-1 and CHEST-2 trials and no new safety signals were seen. In clinical practice, participants that switched from other PAH therapies to riociguat with a treatment-free washout period (median=4 days, range=3–74 days) had no variation in safety when compared with treatment naive patients.26
Tolerability
Riociguat has been relatively well tolerated when dosing is commenced at 1 mg po TID, uptitrated in an 8-week period. Despite commonly reported side-effects, it is tolerated by 87–92%.10,14,26 In CHEST-1, 92% of participants completed the study in the riociguat arm, compared with 94% in the placebo arm. In the riociguat arm at week 16, 77% of participants were taking the maximal riociguat dose of 2.5 mg po TID. Of the 13 (8%) participants in the riociguat arm that did not complete treatment, four (2%) had AE, two (1%) died, two (1%) had lack of efficacy, two (1%) withdrew, and three (2%) did not adhere to treatment or violated protocol.14 In CHEST-2, 26 (11%) of 237 participants did not complete the study, seven (2.95%) participants withdrew due to AEs, three (1.3%) for lack of efficacy, four (1.7%) withdrew, and 13 (5.49%) died, although no deaths were thought to be drug-related.10 In the McLaughlin et al phase IIIb trial, 38 (13%) of 300 participants did not complete treatment, of which five (2%) died, 14 (5%) had an AE, two (1%) lack of efficacy, seven (2%) withdrew consent, two (1%) were lost to follow-up, and eight (<9%) were physician withdrawn or had protocol deviations or screening failures.26
In a select group of SCD-related CTEPH, riociguat was well tolerated in four of six participants.28 Increased VOC was reported in one participant with riociguat doses of 1.5 mg TID, however improved following down titration to 1 mg TID. Notably, it ultimately lacked efficacy in the aforementioned participant and was discontinued. Another participant experienced intractable headaches resulting in termination of riociguat. One patient died after 3 years on riociguat; however, this was not thought to be due to the drug. In total, four participants tolerated riociguat well. Otherwise there were mild GI side-effects reported. In a retrospective multicenter study with 125 participants with PAH and inoperable or recurrent/persistent CTEPH, the CAPTURE trial, most AEs were noted to occur during the 8-week dose-adjustment period of riociguat, with 77% of participants reaching a maximum dose during that time period.29
Pharmacoeconomics
Kirson et al30 assessed the direct cost of CTEPH and found that inpatient services accounted for 54% of the total direct healthcare costs per patient-month for privately insured patients in the US; compared to outpatient and other services (33%) and prescriptions (11%). A subsequent retrospective cohort study with 191 CTEPH patients matched with 955 controls to assess the economic burden of CTEPH found that pharmacy costs were 3-times higher in CTEPH patients vs controls.31 However, in a cost-utility analysis, riociguat cost less and was more effective in treating persons with inoperable CTEPH than bosentan.32
In 2015, the price of riociguat from the manufacturer was Canadian (CAD) $42.75 per tablet for all strengths, which was daily CAD$128.25 and annually CAD$46,811 per patient.33 However, a 30-day supply of riociguat 2.5 mg tablet three times a day may cost up to US $11,449.72 cash without insurance. In a budget impact analysis of adding riociguat to a hypothetical US health plan’s drug formulary with a model monthly wholesale cost of $7500 for a hypothetical population of 1 million, the economic impact on the health plan was minimal, with a per-member per-year cost of US$0.27.34 While CTEPH remains a relatively uncommon illness, the economic cost, both direct and indirect, may be reasonably averted with optimal outpatient care with a cost-effective drug, riociguat for persons with inoperable or persistent/recurrent CTEPH.
Conclusion
PEA remains the treatment of choice for patients with operable CTEPH. Patients with persistent/recurrent symptomatic PH following PEA should receive medical therapy and be considered for BPA. Riociguat is FDA approved medical therapy for patients with non-operable CTEPH and sustained CTEPH after pulmonary endarterectomy. Existing data have shown that riociguat was effective and well tolerated and has a favorable safety profile that was sustained over a long-term treatment period. Due to teratogenic effects, female patients can only receive riociguat through the Adempas Risk Evaluation and Mitigation Strategy (REMS) Program from a certified prescriber, certified pharmacy and must undergo baseline and monthly pregnancy testing during treatment, with defined contraception requirements. Hypotension seems to be the most bothersome adverse effect, therefore a stepwise dose titration is important, especially in old and fragile patients with chronic renal disease. Riociguat should be avoided in patients with a creatinine clearance < 30 mL/min and should not be used together with NO donors, due to a high risk of hypotension.
Disclosure
All authors report no conflicts of interest in this work.
References
1. Moser KM, Bloor CM. Pulmonary vascular lesions occurring in patients with chronic major vessel thromboembolic pulmonary hypertension. Chest. 1993;103(3):685–692. doi:10.1378/chest.103.3.685
2. Kim NH, Delcroix M, Jais X, et al. Chronic thromboembolic pulmonary hypertension. Eur Respir J. 2019;53(1):1801915. doi:10.1183/13993003.01915-2018
3. Simonneau G, Torbicki A, Dorfmüller P, Kim N. The pathophysiology of chronic thromboembolic pulmonary hypertension. Eur Respir J. 2017;26(143):143. doi:10.1183/16000617.0112-2016
4. Delcroix M, Kerr K, Fedullo P. Chronic thromboembolic pulmonary hypertension. epidemiology and risk factors. Ann Am Thorac Soc. 2016;13(Suppl 3):S201–S206. doi:10.1513/AnnalsATS.201509-621AS
5. Pepke-Zaba J, Delcroix M, Lang I, et al. Chronic thromboembolic pulmonary hypertension (CTEPH): results from an international prospective registry. Circulation. 2011;124(18):1973–1981. doi:10.1161/CIRCULATIONAHA.110.015008
6. Bonderman D, Wilkens H, Wakounig S, et al. Risk factors for chronic thromboembolic pulmonary hypertension. Eur Respir J. 2009;33(2):325–331. doi:10.1183/09031936.00087608
7. Matthews DT, Hemnes AR. Current concepts in the pathogenesis of chronic thromboembolic pulmonary hypertension. Pulm Circ. 2016;6(2):145–154. doi:10.1086/686011
8. Simonneau G, Montani D, Celermajer DS, et al. Haemodynamic definitions and updated clinical classification of pulmonary hypertension. Eur Respir J. 2019;53(1). doi:10.1183/13993003.01913-2018.
9. Galiè N, Humbert M, Vachiery JL, et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: the joint task force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS): endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur Heart J. 2016;37(1):67–119. doi:10.1093/eurheartj/ehv317
10. Simonneau G, D’Armini AM, Ghofrani HA, et al. Riociguat for the treatment of chronic thromboembolic pulmonary hypertension: a long-term extension study (CHEST-2). Eur Respir J. 2015;45(5):1293–1302. doi:10.1183/09031936.00087114
11. Pesavento R, Prandoni P. Prevention and treatment of the chronic thromboembolic pulmonary hypertension. Thromb Res. 2018;164:150–156. doi:10.1016/j.thromres.2018.02.149
12. Tanabe N, Kawakami T, Satoh T, et al. Balloon pulmonary angioplasty for chronic thromboembolic pulmonary hypertension: A systematic review. Respir Investig. 2018;56(4):332–341. doi:10.1016/j.resinv.2018.03.004
13. Tsuji A, Ogo T, Ueda J, et al. Predictors of residual pulmonary hypertension after balloon pulmonary angioplasty in patients with chronic thromboembolic pulmonary hypertension. Int J Cardiol. 2017;226:118–120. doi:10.1016/j.ijcard.2016.09.132
14. Ghofrani HA, D’Armini AM, Grimminger F, et al. Riociguat for the treatment of chronic thromboembolic pulmonary hypertension. N Engl J Med. 2013;369(4):319–329. doi:10.1056/NEJMoa1209657
15. Moraes DL, Colucci WS, Givertz MM. Secondary pulmonary hypertension in chronic heart failure: the role of the endothelium in pathophysiology and management. Circulation. 2000;102(14):1718–1723. doi:10.1161/01.CIR.102.14.1718
16. Moncada S, Radomski MW, Palmer RM. Endothelium-derived relaxing factor. Identification as nitric oxide and role in the control of vascular tone and platelet function. Biochem Pharmacol. 1988;37(13):2495–2501. doi:10.1016/0006-2952(88)90236-5
17. Stasch JP, Pacher P, Evgenov OV. Soluble guanylate cyclase as an emerging therapeutic target in cardiopulmonary disease. Circulation. 2011;123(20):2263–2273. doi:10.1161/CIRCULATIONAHA.110.981738
18. Sandner P, Becker-Pelster EM, Stasch JP. Discovery and development of sGC stimulators for the treatment of pulmonary hypertension and rare diseases. Nitric Oxide. 2018;77:88–95. doi:10.1016/j.niox.2018.05.001
19. Conole D, Scott LJ. Riociguat: first global approval. Drugs. 2013;73(17):1967–1975. doi:10.1007/s40265-013-0149-5
20. Khaybullina D, Patel A, Zerilli T. Riociguat (adempas): a novel agent for the treatment of pulmonary arterial hypertension and chronic thromboembolic pulmonary hypertension. P T. 2014;39(11):749–758.
21. Ghofrani HA, Humbert M, Langleben D, et al. Riociguat: mode of action and clinical development in pulmonary hypertension. Chest. 2017;151(2):468–480. doi:10.1016/j.chest.2016.05.024
22. Frey R, Becker C, Saleh S, Unger S, van der Mey D, Clinical Pharmacokinetic MW. Pharmacodynamic profile of Riociguat. Clin Pharmacokinet. 2018;57(6):647–661. doi:10.1007/s40262-017-0604-7
23. Saleh S, Becker C, Frey R, Mück W. Population pharmacokinetics and the pharmacokinetic/pharmacodynamic relationship of riociguat in patients with pulmonary arterial hypertension or chronic thromboembolic pulmonary hypertension. Pulm Circ. 2016;6(Suppl 1):S86–S96. doi:10.1086/685404
24. Benza RL, Farber HW, Frost A, et al. REVEAL risk score in patients with chronic thromboembolic pulmonary hypertension receiving riociguat. J Heart Lung Transplant. 2018;37(7):836–843. doi:10.1016/j.healun.2018.02.015
25. Halank M, Hoeper MM, Ghofrani HA, et al. Riociguat for pulmonary arterial hypertension and chronic thromboembolic pulmonary hypertension: results from a phase II long-term extension study. Respir Med. 2017;128:50–56. doi:10.1016/j.rmed.2017.05.008
26. McLaughlin VV, Jansa P, Nielsen-Kudsk JE, et al. Riociguat in patients with chronic thromboembolic pulmonary hypertension: results from an early access study. BMC Pulm Med. 2017;17(1):216. doi:10.1186/s12890-017-0563-7
27. Wiedenroth CB, Ghofrani HA, Adameit MSD, et al. Sequential treatment with riociguat and balloon pulmonary angioplasty for patients with inoperable chronic thromboembolic pulmonary hypertension. Pulm Circ. 2018;8(3):2045894018783996.
28. Weir NA, Conrey A, Lewis D, Mehari A. Riociguat use in sickle cell related chronic thromboembolic pulmonary hypertension: a case series. Pulm Circ. 2018;8(4):2045894018791802. doi:10.1177/2045894018791802
29. Gall H, Vachiéry JL, Tanabe N, et al. Real-world switching to Riociguat: management and practicalities in patients with PAH and CTEPH. Lung. 2018;196(3):305–312. doi:10.1007/s00408-018-0100-3
30. Kirson NY, Birnbaum HG, Ivanova JI, Waldman T, Joish V, Williamson T. Excess costs associated with patients with chronic thromboembolic pulmonary hypertension in a US privately insured population. Appl Health Econ Health Policy. 2011;9(6):377–387. doi:10.2165/11592440-000000000-00000
31. Said Q, Martin BC, Joish VN, Kreilick C, Mathai SC. The cost to managed care of managing pulmonary hypertension. J Med Econ. 2012;15(3):500–508. doi:10.3111/13696998.2012.665109
32. Chapman R, Quon P, Brand S, Sikirica M, Joish VN. Cost-effectiveness of riociguat for the treatment of Chronic Thromboembolic Pulmonary Hypertension (CTEPH) in the United States. In: A56. Pulmonary Embolism: Acute and Chronic; 2014:A1872.
33. CADTH Common Drug Reviews. Pharmacoeconomic Review Report: Riociguat (Adempas). Ottawa (ON): Canadian Agency for Drugs and Technologies in Health. Copyright © 2015 Canadian Agency for Drugs and Technologies in Health; 2015.
34. Burudpakdee C, Shah A, Joish VN, Divers C, Yaldo A. Budgetary impact of adding riociguat to a US health plan for the treatment of patients with pulmonary arterial hypertension or chronic thromboembolic pulmonary hypertension. Am Health Drug Benefits. 2014;7(9):479–487.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.