Back to Archived Journals » Open Access Journal of Sports Medicine » Volume 13
Rib Fractures in Professional Baseball Pitchers: Mechanics, Epidemiology, and Management
Authors Schowalter S, Le B ![]() , Creps J
, Creps J ![]() , McInnis KC
, McInnis KC
Received 8 June 2022
Accepted for publication 14 September 2022
Published 10 October 2022 Volume 2022:13 Pages 89—105
DOI https://doi.org/10.2147/OAJSM.S288882
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Andreas Imhoff
Sean Schowalter,1 Bryan Le,1 James Creps,2 Kelly C McInnis1,3
1Department of Physical Medicine and Rehabilitation, Harvard Medical School, Spaulding Rehabilitation Hospital, Charlestown, MA, USA; 2Sports Medicine Service, Boston Red Sox, Boston, MA, USA; 3Division of Sports Medicine, Massachusetts General Hospital, Boston, MA, USA
Correspondence: Sean Schowalter, Department of Physical Medicine and Rehabilitation, Harvard Medical School, Spaulding Rehabilitation Hospital, 300 1st Avenue, Charlestown, MA, 02129, USA, Tel +1 617 952 5000, Email [email protected]
Abstract: Pitching is a complex kinetic chain activity requiring the transfer of energy from the lower body, through the core and trunk, and finally through the arm to generate explosive acceleration of the baseball. As a result, large forces are generated in the trunk musculature and rib attachments from the late cocking phase of pitching through deceleration. The repetitive cumulative load and high pitch velocities put professional pitchers at risk of rib stress fracture. Given the potential for a prolonged recovery course and high rate of recurrence, early recognition of rib bone stress injury is critical to optimize care. Identifying torso strength imbalances, suboptimal pitching biomechanics (such as late or inadequate pelvic rotation), as well as metabolic deficiencies that may adversely affect bone health are essential to expedite safe return to play and prevent future injury. In this review, we discuss risk factors, mechanism of injury, typical clinical presentation, diagnostic imaging findings, and propose treatment and prevention strategies for rib stress fractures in overhand pitchers.
Keywords: ribs, stress fracture, stress injury, pitchers, trunk anatomy, biomechanics
Introduction
Bone stress injury (BSI), including stress fracture, is common in sports medicine with reports of incidence between 1.4% and 4.4% of athletes.1,2 They most commonly occur in the weight-bearing bones of the lower extremity. Upper extremity bone stress injuries are less common, but have been reported in many different athletes, including rowers, weightlifters, gymnasts, swimmers, golfers, and pitchers.3–6 Bone stress injuries in throwing athletes generally occur around the shoulder girdle and trunk, and have been reported in the clavicle, ribcage (primarily 1st rib), humerus, olecranon, and ulna.5 Case reports of rib stress injuries in pitchers indicate that the first rib may be the most common site in the ribcage, with injuries at the lower ribs less commonly reported.7–9
Unlike bone stress injuries of the lower extremity, which are often related to repetitive impact from running and jumping, stress fractures in the ribs are thought to be due to repetitive trunk muscle contraction leading to tensile, angular, and torsional stresses on the bone. Over time, these forces can result in cumulative microstructural damage that results in a stress injury at the muscle-bone insertion. Clinically, this pathophysiology coincides with an insidious presentation, with slow progression over time. Athletes generally describe the pain as vague discomfort in the shoulder and upper thorax that may only occur during a brief phase of pitching, making localization difficult. Given the obscure presentation and greater incidence of other shoulder/truncal injuries in pitchers such as rotator cuff pathology, labral tears, shoulder impingement, and intercostal muscle strains, these injuries are often misdiagnosed in the early stages. In the authors’ experience treating major league baseball players however, rib stress fractures are likely underrecognized due to the difficulty of diagnosis and may be more common than currently reported in the literature.
Compared to intercostal and abdominal oblique muscle strains, major league baseball pitchers who sustain rib stress fractures have a prolonged recovery, generally requiring 8–10 weeks before returning to play, versus an average of 5 weeks for muscle strains.7,10 Given the prolonged healing time and high risk of recurrence, it is important to consider the diagnosis of rib stress injury in order to accurately diagnose these athletes as early as possible, determine prognosis, and optimize treatment.
In this review, the authors aim to discuss the mechanisms of rib bone stress injuries, associated risk factors and clinical evaluation, and propose best practice treatment and prevention strategies for rib stress fractures in pitchers.
Trunk Anatomy and Pitching Mechanics
The thorax contains two sets of 12 ribs.11 Ribs 1–7, also known as the “true ribs”, attach directly with the manubrium or sternum via the costal cartilage. Ribs 8–10, or the “false ribs”, connect indirectly to the sternum through a cartilaginous connection to the superior rib. Finally, the floating ribs (ribs 11–12), do not have any anterior connection to the sternum.
The ribs have additionally been classified as “typical” and “atypical”.12 The typical ribs, ribs 3–10, all have two articular facets posteriorly, an inferior facet which articulates with its corresponding vertebra, and a superior articular facet which attaches to the vertebra above (ie, rib 3 articulates with the vertebral body of vertebrae 2 and 3). In addition, typical ribs contain a tubercle which articulates with the transverse process of the analogous vertebra. Finally, each typical rib contains a notch on the underside, named the costal groove, which carries the intercostal nerve, artery and vein. Atypical ribs include ribs 1–2, and 11–12. Ribs 1, 11, and 12 only have one facet posteriorly, where they articulate with their corresponding vertebra. In addition, ribs 11–12 are missing tubercles and do not articulate with a vertebral transverse process. Rib 2 is atypical because of its large tubercle that serves as an origin for the serratus anterior. Lastly, it is important to note that the first rib is thinner than the other ribs, with grooves for the subclavian artery and vein, where the rib thins even more.8 The scalene tubercle is located between these grooves and serves as the attachment for the anterior scalene muscle.
Attaching to the ribcage are several important muscles for pitching mechanics. These include the scalenes, intercostals, serratus anterior, pectoralis major and minor, latissimus dorsi, rectus abdominis, and abdominal oblique muscles. The origin, insertion, and action of each of these muscles can be seen in (Table 1). We will focus our discussion on the relationship of the trunk musculature to pitching mechanics in the throwing athlete.
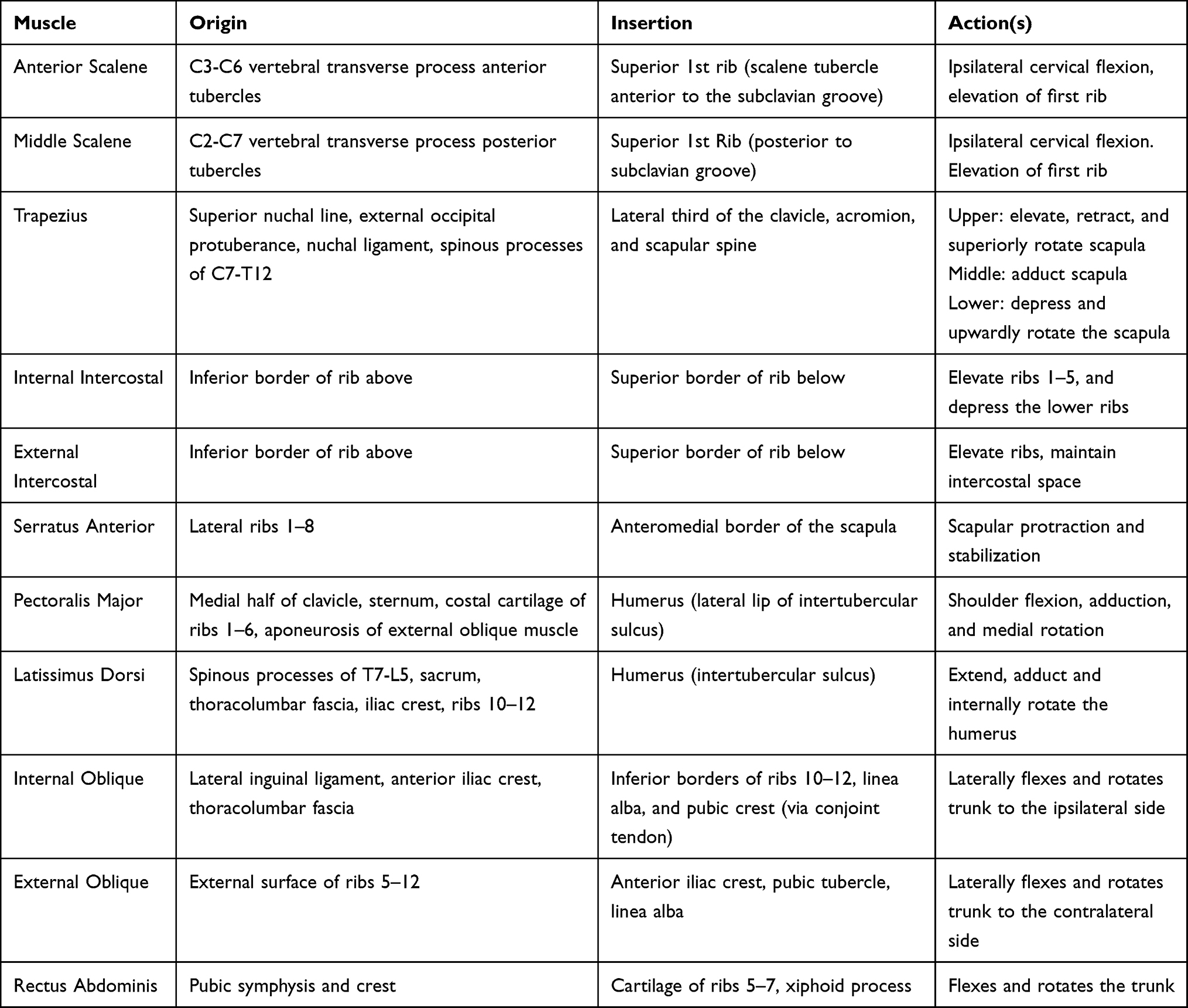 |
Table 1 Truncal Muscles Involved in Pitching |
The pitching motion is a complex sequence of movements which generate energy in the lower extremity and efficiently transfers this energy through the core and trunk resulting in explosive motion of the upper extremity.13 The 6 phases of pitching include the windup, stride, late cocking, acceleration, deceleration, and follow-through (Table 2).14 The trunk muscles begin to activate in the stride phase, starting from maximal lead leg height to initial contact of the lead foot on the pitching mound. This phase has been hypothesized to generate approximately 60% of resultant pitch velocity.15 During this time, the knee and hip of the lag (stance) leg extend, allowing transfer of energy into pelvic rotation, while the abdominal obliques eccentrically contract to prevent excess lumbar hyperextension. A short stride length during this phase may result in increased abdominal muscle load secondary to increased demands on the oblique musculature to accelerate the trunk.14
 |
Table 2 Phases of Pitching and Corresponding Active Truncal Muscles |
The late cocking phase is defined as the time between lead foot contact and the point of maximal rotation of the throwing shoulder. The trunk begins to rotate through a co-contraction of the lead side internal oblique and stance side external oblique. At the same time, the shoulder is moving into abduction and external rotation, requiring a retracted and upwardly rotated scapula to maintain the subacromial space and reduce the risk of impingement. This is accomplished through actions of the serratus anterior and trapezius muscle.16 Subsequently, in the acceleration phase, the trunk reaches maximal rotation speed corresponding with peak activation of the abdominal obliques.17 The rectus abdominis also concentrically contracts at this time to create lumbopelvic flexion and provide additional acceleration.13 As the trunk accelerates forward, activation of the anterior and middle scalene muscles is required to stabilize the head and prevent extension of the neck.18 Meanwhile, the serratus continues to exhibit high levels of activity in order to maintain scapular protraction until ball release, as the humerus undergoes explosive internal rotation and adduction through actions of the pectoralis major and latissimus dorsi.19,20 Finally, in the deceleration and follow-through phases, the shoulder girdle muscles along with the trapezius, serratus, and rhomboids produce high forces as they stabilize the scapula and eccentrically decelerate the arm.21
Mechanism of Injury
The repetitive bending and torsional forces placed on the ribs from the muscular contractions described in the previous section can lead to microstructural damage of the bone.22 Histopathologic studies have demonstrated that trunk overuse leads to skeletal remodeling, beginning with osteoclastic resorption of cortical bone.23 This phase continues for two to three weeks, after which refilling of the resorption cavities by osteoblasts occurs. Replacement, however, is a slow process, which may take months to complete. If microstructural damage occurs at a rate faster than repair can take place, a bone stress injury and potential fracture results.5 Over a season, major league pitchers average 2800 and 1200 in-game pitches for starters and relievers, respectively. When including warm-up pitches, spring training, and off-season training, this number is easily doubled. The increased volume of pitches likely puts starting pitchers at greater risk for rib stress fracture compared to relieving pitchers, although formal epidemiological studies have not yet been performed. Further research is also needed to determine whether sidearm versus overhead throwing, and pitch type (curveball, fast ball, changeup, etc.) place a pitcher at increased risk of stress fracture.
Stress injuries of the first rib have been the most commonly reported rib stress injury in pitchers.5,8,9,24 In a study of 24 first rib stress fractures in overhead throwing athletes, three types of rib fractures were discovered.24 The majority of the fractures (75%) occurred at the attachment of the middle scalene muscle (intrascalene type), while 12.5% were located at the subclavian artery groove (groove type) and 12.5% occurred posteriorly near the costovertebral articulation (posterior type), suggesting differing mechanisms of injury. Of note, 20% of these injuries occurred on the side of the nonthrowing arm. Further investigation is needed to understand the mechanism of injury of the nondominant arm.
Indwelling, fine-wire EMG analysis performed during pitching demonstrates activity of the serratus anterior during late cocking, reaching maximal activity during acceleration, and continued activity through the follow-through phase.20 During these phases, the serratus acts as a scapular stabilizer, resulting in a downward force at its point of origin on the first rib. In contrast, the anterior and middle scalene muscles originate from the cervical transverse processes and insert onto the superior aspect of the first rib. In addition to their function in neck flexion and rotation, they also elevate and, in effect, counteract depression of the first rib. It is hypothesized that these repeated opposing forces from the serratus anterior and scalene muscles result in the majority of first rib stress fractures (groove and intrascalene types).25 Additionally, the first rib is vulnerable at the subclavian artery groove, where the bone is thinnest and, therefore, mechanically weakest.8 Posterior type first rib fractures are hypothesized to have a different mechanism of injury, where inferior and posterior translation of the clavicle during arm abduction and external rotation (such as during the late cocking phase of pitching), can lead to a posterior force on the first rib.26 Further biomechanical research is needed to better define this mechanism.
Though lower rib BSIs are common in rowers (ribs 4–8 accounting for around 80%), stress injuries of ribs 2–12 are rarely reported in pitchers, but may be largely underrecognized.4,7,27–29 Case reports describe injuries at ribs 7–9, as well as the floating ribs (ribs 11–12).28,29 Bone stress injuries occurring between ribs 7–9 have been attributed to the opposing anterior/caudad rotational force of the external oblique muscles and posterior/cephalad force of the serratus anterior.28,30 Supporting this hypothesis, cadaveric studies of the serratus anterior demonstrate maximal tensile load at the posterolateral rib, consistent with the location of most stress fractures.30 Pain during the late cocking and early acceleration phases, where the serratus is most active, further supports this theory.28
Rib fractures of the floating ribs have been described at their distal, non-articulating ends. Anatomically, the external oblique muscle arises from the external and inferior surfaces of the lower eight ribs where it interdigitates with the latissimus dorsi and serratus posterior inferior on ribs 9–12.31 The traction forces from these opposing muscles is hypothesized to be the mechanism of these distal floating rib fractures.29
Risk Factors
Currently, there is no literature investigating risk factors for rib bone stress injury, however we can extrapolate risk factors based on the more commonly affected areas that have been studied. Nonmodifiable risk factors include family history, prior history of bone stress injury, and Caucasian ethnicity.32–36 Although no studies have been performed on specific genes involved in stress fracture, a family history increases the risk of athletes sustaining stress fracture, suggesting a genetic component.36 In a prospective study investigating sex-specific risk factors for tibial stress fractures, prior fracture reflected the strongest predictor of stress fractures regardless of sex.32
Modifiable risk factors can be broken down into biomechanical (such as overhead vs sidearm throwers, and pitch count), and biochemical risk factors. Overhead pitching mechanics may increase risk of rib bone stress injury over side arm throwers.37 When reviewing literature for pitching injuries more broadly, starting pitchers have a higher incidence of shoulder injuries when compared to relief pitchers.38 Additionally, starting pitchers typically throw four different types of pitches compared to relief pitchers who have one or two. The variety and volume of pitches expected from a starting pitcher may factor into an increased risk of bone stress injury. Studies in rowers have also shown that the incidence of rib stress fracture is higher in sweepers (rowers with one oar) compared to scullers (two-oared rowers).39 This may imply that one-sided activity, such as pitching, or muscle imbalances associated with one-sided activity, may predispose athletes to sustain fractures. Deficits in the kinetic chain (upper, lower extremity and core) can play a role as well, as improper transfer of energy in one phase of pitching can cause compensatory changes that increase strain to other tissues.14,40 External factors include a low aerobic fitness level prior to training, tobacco use, and a high intensity of physical training.41 In studies of rowers, higher level of performance has been shown to correlate with higher levels of rib bone stress injury.27 This may also be the case with elite level pitchers, but epidemiologic studies do not yet exist.
Biochemical risk factors for rib bone stress injury include vitamin D and vitamin C deficiencies, iron deficiency, and low estrogen levels. Serum 25 (OH) vitamin D concentrations below 30ng/mL have been specifically associated with stress injuries. Although calcium supplementation has been shown to improve bone mineral density, there is no strong evidence to suggest a correlation between calcium deficiency and stress fractures. Potassium and vitamin C intake from fruits and vegetables has also been implicated in improving bone mineral status in adolescents, independent of calcium.42 Many of these biochemical risk factors may be part of the clinical entity termed relative energy deficiency in sport (RED-S), which refers to impaired physiological function that includes metabolic rate, bone health, immunity, protein synthesis, and cardiovascular health due to energy imbalance, with deficiency of caloric intake relative to output through exercise.43 RED-S has been shown to be an independent factor of poor bone health due to decreased IgF-1 and bone formation marker levels, which can increase the risk of developing bone stress injury.44 While more common in females, men can also present with this syndrome and should be considered when evaluating for any bone stress injury.
Clinical Presentation
Although some athletes may describe a clear onset, such as a popping sensation while pitching, the majority of pitchers who present with rib stress injury describe an insidious onset of discomfort on their dominant throwing side, without obvious insult.9,24 This discomfort may be described as a nonspecific ache at the base of the neck, shoulder, posterior arm, upper thoracic, or interscapular regions, making localization difficult.29 A large proportion of these athletes will describe provocation of pain while pitching (resulting in decreased pitch control and velocity), or swinging a bat.8,24,28 Notably, the pain while pitching often occurs during the late cocking and early acceleration phases, coinciding with the time of peak serratus anterior activity.20 Worsening pain with inspiration is also a common complaint.9,24,28 Interestingly, a history of change in pitching mechanics, training intensity or volume is often absent.9,28
Given the vague history, these injuries are difficult to diagnose, and a differential diagnosis should include other truncal pathologies such as intercostal or abdominal muscle strain, serratus anterior muscle strain, myofascial pain, costochondritis, Tietze syndrome, slipping rib syndrome, costovertebral joint dysfunction, intercostal neuralgia, thoracic spine dysfunction (discogenic or radicular pain), and shingles.11
Physical Examination
The athlete should be examined with the torso exposed. Most often there is no visible abnormality; however, swelling and/or rib deformity can rarely be seen at the site of stress fracture.28 Structural abnormalities that can lead to abnormal pitching mechanics should be assessed including muscle hypertrophy vs atrophy, thoracolumbar scoliosis and kyphosis, scapular malignment, and scapulothoracic abnormal motion.45 Evaluation of the athlete performing a pitch (live or video footage) can be helpful as well, with attention to improper mechanics, such as late pelvic rotation or early trunk rotation, which can cause less efficient transfer of energy and compensatory changes that increase trunk muscle strain and rib bone stress.40
Most patients with rib bone stress injuries have tenderness, which can be pinpoint over the area of fracture or more diffuse in nature.8,28 In pitchers, special attention should be given to the first rib, as it may be affected more frequently than the remaining ribs.5,8,9,24 The first rib can be palpated in the supraclavicular fossa, lateral and posterior to the sternocleidomastoid, where the middle scalene attaches to the first rib and the majority of first rib stress fractures occur.24 Palpation should be directed inferiorly given the course of the first thoracic rib behind the clavicle (Figure 1A). The posterior first rib can be palpated by moving laterally from the C7 spinous process and pressing deep to the trapezius muscle (Figure 1B). In contrast to first rib stress fractures, stress injuries of ribs 6–10 generally occur posterolaterally, while stress fractures of the floating ribs (11–12) typically occur anteriorly at their distal tip due to mechanisms described earlier.7,28,29 Tenderness at these specific locations should increase suspicion for stress fracture and the need for diagnostic imaging.
 |
Figure 1 Palpating the First Rib. Palpation of the first rib anteriorly (A), and posteriorly (B). To palpate the first rib anteriorly, press inferiorly into the clavicular fossa, lateral and inferior to the sternocleidomastoid muscle. To palpate the posterior first rib press lateral to the C7 spinous process, deep to the trapezius muscle. |
Most athletes with bone stress injuries of the ribs will have full active and passive range of motion in the shoulders and cervical spine, but those with first rib fractures may have pain with certain shoulder movements, especially abduction greater than 90 degrees.9,18,46,47 Thoracic spine rotation and lateral flexion may also provoke pain in rib fractures, whereas pain with forward flexion is more suggestive of discogenic back pain.
Activation of musculature that attaches to the injured rib may cause pain as well, for example activation of serratus anterior with scapular protraction in injuries to ribs 1–8 (Table 1). More specifically, placing the cervical or thoracic spine in the theorized position of injury, and then proceeding with specific resistive testing of the associated musculature, is often the most effective method of eliciting the athlete’s pain. For example, if a right-handed pitcher complains of pain in the right first rib during the late cocking phase of the pitching, have them sit on the table and position their cervical spine in left lateral flexion and rotation, while the thoracic spine is placed in right rotation and extension to match positioning of the spine during this phase. Resisted neck flexion (testing the anterior scalenes) and resisted posterior translation of the humerus with the shoulder flexed to 90 degrees (testing the serratus anterior) in this position, maximizes force on the first rib and is more likely to generate pain and aid in diagnosis than isolated muscle testing alone. Pain with deep inspiration is also a common finding.9,24,28
A full neurovascular exam of the bilateral upper extremities including strength and sensation testing should also be performed, as vague exertional upper extremity pain may be due to peripheral nerve entrapment or vascular etiologies such as peripheral vascular disease, deep vein thrombosis or thoracic outlet syndrome.45 Strength and sensory exams, as well as tests for shoulder impingement, biceps pathology, and labral injuries, should all be normal.8,28
Diagnostic Imaging
Radiographs
Imaging often begins with a PA (posteroanterior) chest and oblique rib radiographs.47,48 However, given the difficulty localizing pain in rib stress injuries, shoulder and cervical spine radiographs are often obtained at initial workup. Funakoshi et al demonstrated that 46% of the first rib is visible on a shoulder x-ray, whereas 97% is visible on cervical spine x-rays. Therefore, the authors recommend cervical spine and chest x-rays as initial screening for suspected first rib stress fracture.24
The earliest sign of a stress fracture on conventional radiographs is the “gray cortex” sign; focal “graying” or lucency of the cortical bone.49 As the injury progresses, the area of stress reaction will coalesce into a lucent intracortical fracture line or even a displaced fracture.50 Faint linear foci of sclerosis may also be visualized, representing microcallus formation.50 Given the subtlety of these findings, early radiographs are commonly negative until several weeks after injury when periosteal reaction and callus formation occur, which can be seen as a hazy opacity around the area of bony injury (Figure 2A and B).51,52
 |
Figure 2 Radiographs/MRI of a Rib Stress Fracture. AP chest radiograph (A) zoomed in to visualize pathology (B) obtained weeks after chest pain began in a left-hand dominant pitcher. The red arrowhead demarcates callous formation at the right 8th rib. On coronal (C) and sagittal MRI (D) the nondisplaced fracture is visualized (blue arrowhead), with moderate osseous edema and callus formation at the fracture site. |
Extrapolating from lower extremity stress fracture literature, x-ray has a sensitivity of roughly 28% at initial presentation, increasing to 54–80% at follow-up (2–6 weeks later).53,54 Radiographic changes such as focal sclerosis and periosteal bone formation occurred, on average, 25 days after the onset of symptoms.54 Reviews of traumatic rib fractures also demonstrate poor sensitivity, with chest x-rays missing over 50% of fractures.55,56 Therefore, initial negative x-rays, and even negative follow-up x-rays do not rule out a rib bone stress injury. If suspicion remains high for rib fracture, advanced imaging is indicated.
Ultrasound
Sonographic findings may include fluid collection adjacent to the rib, with increased vascularity, as well as periosteal elevation, subperiosteal hematoma, and increased posterior shadowing. Color Doppler ultrasound is also potentially beneficial in detecting increased vascularity around the fracture callus formation, reflecting a healing fracture.57 Studies evaluating ability of therapeutic ultrasound to diagnose tibial stress fractures have shown variable results, with sensitivity ranging from 81.8% to 86% and specificity ranging from 66.6% to 77.27%, as compared to MRI and bone scintigraphy.58,59
Therapeutic ultrasound (TUS) involves applying a frequency of up to 3 MHz to the site of a suspected fracture. The patient reports on the level of pain perceived at each intensity, and the result is compared with the unaffected side. The positive predictive value ranged from 41% to 99% and negative predictive value ranged from 13.4% to 51%.60
Ultrasound has advantages due to its ease of access without exposure to radiation, however it is not as sensitive as MRI for assessing stress fracture, and the diagnostic quality of ultrasound is user dependent. Anatomically, the first rib is also difficult to visualize. Additionally, retroscapular ribs and the infraclavicular portion of the first rib are difficult to access via sonography.61
CT Scan
There are limitations to consider when assessing ribs via chest computerized tomography (CT). A standard CT technique is oblique to the anatomic long and the short axes of the rib, which makes interpretation of fractures difficult. However, the use of angulated thin-section helical CT offers the possibility of obtaining true axial slices of any selected rib, allowing for a view analogous to those obtained for long tubular bones.62 Stress fracture findings include an intramedullary area of bone sclerosis or osteolysis.
In lower limb stress fractures, the level of sensitivity was 32% and specificity was found to be 98%.63 However, Gaeta et al found that CT can be superior to MRI (51% vs 41%) when analyzing cortical abnormalities such as osteopenia, resorption cavity, and striation, which may be early lesions preceding a stress fracture. In the United States, the annual effective dose from background radiation is on average 3 mSv/y; ranging from 1 to 10 mSv.64 The radiation from a typical chest CT is 7 mSv, although a thin-sliced, focused study over the area of suspected pathology can limit radiation exposure.65 Given the radiation exposure and decreased sensitivity, CT remains inferior to MRI and bone scintigraphy for the detection of stress fractures.63
Magnetic Resonance Imaging (MRI)
MRI of the chest wall (CW) can detect bone edema and lower grade injuries without cortical fracture.66 The ideal sequence includes short tau inversion recovery (STIR) or fat-suppressed T2-weighted images. A T1 weighted image depicts anatomy but does not detect edema as effectively.
Typical MRI features include rib periosteal or adjacent soft tissue edema and band-like bone marrow edema (Figure 2C and D). MRI is also able to rule out other sources of bone or soft tissue pain. The best field of view for the first rib, specifically, would be in the axial and sagittal plane. Coronal views are also useful for comparing to the contralateral side, improving visualization of subtle changes. A small field of view in the area of suspected injury can provide a more targeted evaluation, however there are no studies comparing different fields of view for rib injuries. Though 1.5 Tesla (T) MRI has been shown to be comparable to 3T MRI in the assessment of BSI in the foot, the authors recommend 3T MRI CW specifically for rib BSI.67 Anecdotally, this approach provides the highest quality visualization of the ribcage, especially of subtle bone marrow edema.
There are accepted MRI classification systems (ie, Fredericson and Arendt) that can identify the severity of injury and help guide expectations for return to play.68,69 However, it is difficult to extrapolate these leg-based systems to the ribcage as the mechanics and load patterns vary significantly. In the authors’ experience, rib stress injuries with cortical disruption and fracture lines extending across one or both cortices portend a less favorable prognosis and longer recovery. Contrast studies are sometimes used to differentiate stress fracture from pathological fracture, however contrast studies are not necessary in the great majority of rib BSI in sport.70,71
Zero Echo Time (ZTE) MRI has been studied in its clinical relevance in assessing osseous features. A study of ZTE MRI in the shoulder found that the majority of ZTE images provided superior visualization of osseous features when compared with CT.72 In the setting of bone stress injury, MRI remains superior to CT, therefore more MRI studies of ZTE are required to assess its clinical superiority over other imaging modalities.
Comparing MRI with bone scintigraphy in lower extremity stress fractures, the sensitivity of MR imaging was 100% and the specificity was 86%.73 Fredericson et al performed radiographs, scintigraphy (technetium bone scan) and MRI scans in runners with symptomatic leg pain and revealed that the exact anatomical region of the lesion could be defined more precisely by MRI than by scintigraphy.68 Given the high sensitivity and specificity, MRI is considered the gold standard imaging modality in the indentification of bone stress injuries.
Bone Scan
Historically, technetium bone scanning was an imaging modality of choice in the diagnosis of bone stress injuries due to its high sensitivity, with ability to detect stress fractures as early as 7 hours after injury.74 In addition, the high sensitivity meant that lack of uptake on bone scan beyond 3 days likely excluded a fracture.74 Radiopharmaceutical uptake at any area of active bone turnover, however, can also lead to many false positives.75 These asymptomatic areas likely represent normal remodeling of bone due to stress. In addition, bone scans expose patients to radiation of approximately 4.2 mSv.76 This can be compared to 7 mSv for a standard-dose chest CT examination, and an average annual effective dose from background radiation of 3 mSv per year.64,77 Given the risk of false positives and radiation exposure, MRI has usurped bone scan as the preferred method of diagnosis.
Treatment
Similar to other bone stress injuries, treatment of rib bone stress injury begins with a period of relative rest followed by a gradual return to sport.11 Athletes should be restricted from motions that can increase load on the injured rib such as throwing, batting, and weightlifting. Patients with pain provoked by deep breathing should also restrict activities that lead to increased ventilatory demands, such as cycling, as the muscles of inspiration can place additional strain on the ribs.
If pain control with relative rest is not adequate, additional pain control can be achieved with ice, acetaminophen and nonsteroidal anti-inflammatory drugs (NSAIDs). Supportive taping of the ribs can also be used to decrease pain by reducing excursion of the ribs during inspiration and upper extremity movements.78,79 Similarly, rib belts can be an easy and effective tool in transitioning the athlete to higher levels of activity early in the recovery process. Supportive devices should be discontinued as soon as the athlete is asymptomatic to ensure restoration of normal trunk mobility and strength can be achieved during the rehab process. Some physicians prefer to avoid NSAIDs given animal studies which showed impaired fracture healing, however these animal studies involved high doses of NSAIDs for prolonged periods of time.80,81 Retrospective and prospective studies in humans, however, have shown that short courses of NSAIDs are not detrimental to fracture healing, and thus a short course of NSAIDs, as needed, up to 14 days is likely safe after fracture.80,82,83 It should also be noted that pain is a good gauge of when an athlete can increase their physical activity. Therefore, care should be taken to avoid masking pain, which could lead to an overly rapid return to sporting activities and prolonged disability.
As soon as pain free deep breathing is achieved, generally 2 days to a week after initiating rest, a staged rehabilitation program can expedite return to play compared to prolonged rest.78 Training generally begins with nonimpact aerobic exercise such as stationary biking without use of a grip, aquatic therapy, arm and leg cycling, and zero-gravity running to maintain cardiovascular endurance.39,84 Once low-impact activities can be performed for prolonged periods without pain, higher impact activities such as running and jumping can be incorporated.85 At this point, athletes can also begin specific exercises aimed at preventing future injuries. It is important to remember that the trunk musculature works both concentrically and eccentrically during the process of overhead throwing, and that inadequate control of deceleration can be an underlying component of the athlete’s injury. Consequently, eccentric muscle conditioning is an important component in promoting trunk stability and reinforcing neuromuscular control, throughout the throwing motion. Athletes with groove type fractures of the first rib should undergo stretching of the scalene muscles to decrease strain on the first rib, while those with lower rib stress fractures should undergo core strengthening and stretching of the thoracic musculature, such as the serratus anterior and latissimus dorsi, in an attempt to balance opposing forces on the lower ribs.26,28 In addition, strengthening of specific muscles, such as the serratus anterior has been suggested in the literature.86,87 This seems counterintuitive, given several of these fractures are partially attributed to forces generated by the serratus anterior.88 Although there are no trials comparing specific strengthening of the serratus anterior versus a generic rehabilitation program, it could be that strengthening of the muscle balances opposing forces, and therefore neutralizes load on the affected rib.
After a couple of weeks, a slow return to sport-specific exercise can be initiated, including fielding drills, batting, and a throwing program. Pitching mechanics should be evaluated at this time to fix any deficiencies, such as decreased hip internal rotation (IR) during the wind-up phase or a lack of hip IR in the landing leg during follow through. Similarly, a lack of hip external rotation in the driving leg can impact the timing of appropriate pelvic rotation. Late pelvic rotation during the stride phase can lead to compensatory truncal muscle use and rib strain.40 In addition, assessment of the range of motion of the thoracic spine is also important, given the high rotational demands placed on the body during the late cocking and follow-through phases of the pitching motion. Specifically, the combined motions of ipsilateral rotation and side bend, referred to as rotexion in the manual therapy literature, should be evaluated in thoracic extension to ensure that adequate thoracic mobility exists as the athlete transitions from the stride to late cocking phases of the throwing motion. Similarly, ipsilateral side bend with contralateral rotation, referred to as latexion in the manual therapy literature, should be assessed in thoracic flexion to ensure that adequate thoracic mobility is present in follow-through. Limitations in these movements can be present from either soft-tissue or articular dysfunctions, so it is important to complete passive intervertebral motion and rib mobility testing, in addition to the combined motion testing described above, to determine the underlying etiology of the restriction when one is found. In the presence of normal passive vertebral and rib mobility testing, restrictions in scapular and trunk muscle flexibility should be assessed.
After 4–6 weeks of a gradual return to a throwing program, most bone stress injuries will heal uneventfully. Radiographs can be useful at this time and will show bone healing with callus formation.8 Asymptomatic patients with evidence of bone healing on radiography can return to competition at this time. First rib and complete fractures are at greater risk for nonunion, however, and may require a longer period of restricted activity (up to 6–12 months) for healing.18,89 In a retrospective cohort of 23 throwing athletes (primarily baseball players) with first rib stress fractures, 7 (29%) developed nonunion of the first rib at 7.5 months.24 Fortunately, documented cases of nonunion in the literature have been able to return to their previous levels of competition.18
Physicians should also be mindful of other complications of rib fractures, including pneumothorax, thoracic outlet syndrome, brachial plexus palsy, and Horner’s syndrome.8,90 Shortness of breath, decreased breath sounds, and asymmetric lung sounds should prompt radiographs to look for a pneumothorax.9 Nonunion or excessive callus formation can lead to thoracic outlet syndrome, and thus any patient with clinical signs of claudication, pallor, swelling or weakness in the arm should be worked up further with imaging of the brachial plexus and subclavian artery/vein.91,92 The proximity of the first rib to the carotid artery and sympathetic chain also places patients with first rib fractures at risk of carotid injury manifesting as Horner’s syndrome (classically described as ptosis, miosis, and anhidrosis), which would require additional workup to evaluate the integrity of the carotid artery.93,94 When thoracic outlet syndrome, brachial plexus injury or other injury to surrounding structures is diagnosed, referral to surgery for resection of callus and a portion of the first rib is indicated.90
Lastly, there has been recent interest in the use of ultrasonic (low-intensity ultrasound and extracorporeal shockwave therapies), orthobiologic injections, as well as bone stimulator units to expedite bone healing.95 Evidence supporting these modalities is currently lacking, although there may be some data supporting bone stimulator therapy for higher grade or recalcitrant stress fractures.96–98 Additionally, teriparatide has shown promise in improving fracture healing and bone strength in animal studies, and human studies are ongoing.99,100
Prevention
Since prior stress fractures are the strongest predictor of future stress injury, considerable treatment emphasis should be placed on preventing recurrent stress fracture.32 As above, athletes should work with a pitching coach to correct any improper throwing techniques. Thorough biomechanical evaluation of the spine, shoulders and hips, with early recognition and treatment of joint restrictions can be key to reducing compensatory trunk muscle activation that may predispose athletes to rib injuries.14,40 In addition to assessment of hip and thoracic range of motion as mentioned in the treatment section, pitchers frequently demonstrate segmental motion limitations in the cervical and shoulder regions. Glenohumeral internal rotation deficit (GIRD), described as increased shoulder external rotation and decreased internal rotation of the dominant throwing arm, is commonly discussed in the literature, and may be due to osseous adaptation to pitching with glenohumeral retroversion, or selective stretching of the anterior capsule and tightening of the posterior capsule.101 Although adaptive GIRD may show protective effects at the shoulder, studies of kinematics on pitchers with GIRD showed significantly decreased trunk rotation, shoulder adduction, and increased shoulder rotation during pitching compared to a control group without GIRD. This suggests inefficient transfer of energy from the trunk to the upper extremity, and the possibility of increased load/injury to surrounding tissues.102,103 To address the deficits in internal shoulder rotation, stretches such as the cross-body stretch, sleeper stretch, and corner pectoralis stretch have been demonstrated to be effective.104 Studies also show an association between restricted neck flexion/rotation and pitching injuries.105 Although the pathophysiology is unclear, it is hypothesized that limited cervical range of motion can interfere with the ability to maintain head stability while the trunk rapidly flexes, twists and side bends during pitching. This could contribute to increased stress on the scalene muscles as they work to maintain head stability, with consequent increased stress to the first rib, although this is speculative at this point.
Furthermore, the muscles which attach to the ribs (Table 1) should also be assessed for weakness, strength imbalances, or tightness that could lead to unequal tensile, or torsional forces on the ribs. Specifically, imbalances in pull from the serratus anterior and scalene muscles are thought to contribute to first rib fractures, while imbalances in the external obliques, latissimus dorsi, and serratus anterior may contribute to lower rib fractures. If weakness or tightness is detected, strengthening and stretching are important to balance opposing muscular forces and neutralize the forces on the rib.
It is also important to remember that the deceleration phase of pitching can contribute to injury given the extreme velocities obtained with pitching. During the deceleration phase, eccentric muscle contractions are required to stabilize and slow rotation of the trunk and throwing arm which can generate high forces on the muscle, and in turn, their bony/tendinous origins. Thus, eccentric muscle conditioning is important for inducing adaptive changes in muscle that can improve trunk stability and reduce injury in the deceleration phases of pitching.106 Commonly recommended eccentric abdominal exercises include diagonal abdominal chops, cable rotations, and eccentric trunk rotation/extension (Figure 3A–H). Furthermore, care should be taken to avoid overtraining. Athletes should also be taught to monitor for early signs of pain, as early recognition and adequate rest may prevent progression to stress fracture.91
 |
Figure 3 Eccentric Abdominal Exercises. Three eccentric abdominal exercises consisting of a half-kneeling diagonal chop (A and B), a standing cable rotation (C, D and E), and eccentric trunk rotation with extension utilizing a glute ham bench (F, G and H). For the half-kneeling diagonal chop, the athlete starts in position (A) and controls the movement of his upper extremities against the resistance band until reaching position (B) meanwhile keeping the trunk still. Standing cable rotations are performed starting in position (C) with the arm close to the body. The athlete then extends his elbow while maintaining rotation of his trunk (D), followed by controlled rotation to the opposite side (E). Lastly, eccentric trunk rotation with extension is performed starting in position (F) on a glute ham bench. The athlete then side bends his body into position (G) followed by rotation and extension into position (H). |
A metabolic workup, especially measurement of 25-hydroxy vitamin D level, is often helpful given the association between low vitamin D levels and stress fracture.107,108 If vitamin D deficiency is discovered, supplementation has been shown to decrease the risk of stress fracture.109,110 Supplementation with calcium, on the other hand, has less evidence, but may also be beneficial in preventing the risk of stress fracture.109,111 This is supported by studies linking low bone mineral density (BMD) and stress fracture, as well as the association of increased calcium intake and higher BMD.111–113 Finally, in females, low ferritin and iron levels have been found to correlate with a higher risk of stress fractures, however this association has not yet been demonstrated in males.114,115
In cases of repeat stress fracture, bone density scans can be helpful in ruling out low or excessively high BMDs, which may benefit from an endocrinology referral and further evaluation of the hormones involved in bone homeostasis.108 Despite the association of low BMD and stress fracture, prophylactic treatment with bisphosphonates has not been shown to be effective in reducing stress fracture in military recruits.116 Additionally, animal studies have shown impaired healing of stress fracture with the use of bisphosphonates.117,118
Finally, athletes should be examined for relative energy deficiency in sport using tools such as the RED-S clinical assessment tool, which assesses several risk factors for stress fracture such as low body mass index (BMI), caloric intake, low BMD, and amenorrhea. An assessment of 323 college female athletes using this tool to stratify athletes into low, moderate, or high risk of stress fracture, found that moderate-risk athletes were 2.6 times more likely to develop bone stress injuries, and high-risk athletes were 3.8 times more likely.119 In a study of male college athletes using a modified risk calculator, each 1 point increase in the cumulative risk score was associated with a 37% increased risk of a bone stress injury.120 Therefore, these risk assessment models exemplify the importance of nutrition optimization, adequate energy availability, and appropriate BMI to maintain appropriate bone health. Consultation with the team sports dietician is recommended to ensure adequate caloric intake and individualize nutrient requirements both during recovery and for secondary prevention.
Conclusion
Although studies have not defined the incidence of rib stress fractures in pitchers, the repetitive forces though the core and trunk required to generate arm acceleration in professional pitching appears to put these elite athletes at risk of bone stress injury. Typically, pitchers present with poorly localized, insidious onset of pain on the dominant throwing side, worse with the late cocking and early acceleration phases of pitching. They often describe vague pain at the base of the neck, scapula, shoulder, or chest wall without a well-defined area of tenderness. As a result, these injuries are often underrecognized and misdiagnosed in the early stages, which puts the athlete at risk of injury progression and prolonged recovery. We recommend a heightened index of suspicion of rib bone stress injury in pitchers and considering advanced imaging with MRI Chest Wall (3T) early.
Once diagnosed, assessment of modifiable biomechanical and metabolic risk factors is essential for guiding management, as well as secondary prevention. We specifically recommend a rehabilitation program focused on improving pitching mechanics, targeting deficits in the kinetic chain (such as decreased hip/pelvic/truncal mobility, as well as core weakness), and imbalances in opposing trunk musculature (ie, first rib: scalene vs serratus anterior, and middle ribs: serratus anterior vs external oblique). Bone health and metabolic profile should be investigated with consideration for DEXA scan, vitamin D and ferritin levels, especially in cases of recurrent injury. With increased awareness, early diagnosis and appropriate management, we can optimize care in elite pitchers and expedite safe return to play.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Monteleone GP. Stress fractures in the athlete. Orthop Clin North Am. 1995;26(3):423–432. doi:10.2165/00007256-199214050-00005
2. Iwamoto J, Takeda T. Stress fractures in athletes: review of 196 cases. J Orthop Sci. 2003;8(3):273–278. doi:10.1007/s10776-002-0632-5
3. Lee AD. Golf-related stress fractures: a structured review of the literature. J Can Chiropr Assoc. 2009;53(4):290–299.
4. Harris R, Trease L, Wilkie K, Drew M. Rib stress injuries in the 2012–2016 (Rio) Olympiad: a cohort study of 151 Australian rowing team athletes for 88 773 athlete days. Br J Sports Med. 2020;54(16):991–996. doi:10.1136/bjsports-2019-101584
5. Sinha AK, Kaeding CC, Wadley GM. Upper extremity stress fractures in athletes: clinical features of 44 cases. Clin J Sport Med. 1999;9(4):199–202. doi:10.1097/00042752-199910000-00003
6. Heincelman C, Brown S, England E, Mehta K, Wissman RD. Stress injury of the rib in a swimmer. Skeletal Radiol. 2014;43(9):1297–1299. doi:10.1007/s00256-014-1863-0
7. Gerrie BJ, Harris JD, Lintner DM, et al. Lower thoracic rib stress fractures in baseball pitchers. Physician Sportsmed. 2016;44(1):93–96.
8. Coris EE, Higgins HW. First rib stress fractures in throwing athletes. Am J Sports Med. 2005;33(9):1400–1404. doi:10.1177/0363546505275349
9. Chimenti PC, Elfar JC, Giordano BD. Dominant-sided first-rib stress fracture in a Collegiate baseball pitcher. JBJS Case Connect. 2013;3(4):e108. doi:10.2106/jbjs.cc.m.00019
10. Conte SA, Thompson MM, Marks MA, Dines JS. Abdominal muscle strains in professional baseball: 1991–2010. Am J Sports Med. 2012;40(3):650–656. doi:10.1177/0363546511433030
11. Gundersen A, Borgstrom H, McInnis KC. Trunk injuries in athletes. Curr Sports Med Rep. 2021;20(3):150–156. doi:10.1249/JSR.0000000000000819
12. Graeber GM, Nazim M. The anatomy of the ribs and the sternum and their relationship to chest wall structure and function. Thorac Surg Clin. 2007;17(4):473–489. doi:10.1016/j.thorsurg.2006.12.010
13. Seroyer ST, Nho SJ, Bach BR, Bush-Joseph CA, Nicholson GP, Romeo AA. The kinetic chain in overhand pitching: its potential role for performance enhancement and injury prevention. Sports Health. 2010;2(2):135–146. doi:10.1177/1941738110362656
14. Calabrese GJ. Pitching mechanics, revisited. Int J Sports Phys Ther. 2013;8(5):652–660.
15. McNally MP, Borstad JD, Oñate JA, Chaudhari AMW. Stride leg ground reaction forces predict throwing velocity in adult recreational baseball pitchers. J Strength Cond Res. 2015;29(10):2708–2715. doi:10.1519/JSC.0000000000000937
16. Moynes DR, Perry J, Antonelli DJ, Jobe FW. Electromyography and motion analysis of the upper extremity in sports. Phys Ther. 1986;66(12):1905–1911. doi:10.1093/ptj/66.12.1905
17. Pappas AM, Zawacki RM, Sullivan TJ. Biomechanics of baseball pitching: a preliminary report. Am J Sports Med. 1985;13(4):216–222. doi:10.1177/036354658501300402
18. Edwards TB, Murphy C. Nonunion of a dominant side first rib stress fracture in a baseball pitcher. Orthopedics. 2001;24(6):599–600. doi:10.3928/0147-7447-20010601-20
19. Gowan ID, Jobe FW, Tibone JE, Perry J, Moynes DR. A comparative electromyographic analysis of the shoulder during pitching: professional versus amateur pitchers. Am J Sports Med. 1987;15(6):586–590. doi:10.1177/036354658701500611
20. Jobe FW, Moynes DR, Tibone JE, An PJ. EMG analysis of the shoulder in pitching: a second report. Am J Sports Med. 1984;12(3):218–220. doi:10.1177/036354658401200310
21. DiGiovine NM, Jobe FW, Pink M, Perry J. An electromyographic analysis of the upper extremity in pitching. J Shoulder Elb Surg. 1992;1(1):15–25. doi:10.1016/S1058-2746(09)80011-6
22. Schaffler MB, Radin EL, Burr DB. Mechanical and morphological effects of strain rate on fatigue of compact bone. Bone. 1989;10(3):207–214. doi:10.1016/8756-3282(89)90055-0
23. Sweet DE, Allman RM. RPC of the month from the AFIP. Radiology. 1971;99(3):687–693. doi:10.1148/99.3.687
24. Funakoshi T, Furushima K, Kusano H, et al. First-Rib stress fracture in overhead throwing athletes. J Bone Jt Surg Am. 2019;101(10):896–903. doi:10.2106/JBJS.18.01375
25. Mintz AC, Albano A, Reisdorff EJ, Choe KA, Lillegard W. Stress fracture of the first rib from serratus anterior tension: an unusual mechanism of injury. Ann Emerg Med. 1990;19(4):411–414. doi:10.1016/S0196-0644(05)82349-2
26. Kawashima K, Terabayashi N, Asano H, Akiyama H. Classification of stress fractures of the first rib in adolescent athletes. J Pediatr Orthop Part B. 2020;29(4):409–411. doi:10.1097/BPB.0000000000000720
27. McDonnell LK, Hume PA, Nolte V. Rib stress fractures among rowers: definition, epidemiology, mechanisms, risk factors and effectiveness of injury prevention strategies. Sport Med. 2011;41(11):883–901. doi:10.2165/11593170-000000000-00000
28. Noonan TJ, Sakryd G, Espinoza LM, Packer D. Posterior rib stress fracture in professional baseball pitchers. Am J Sports Med. 2007;35(4):654–658. doi:10.1177/0363546506296834
29. Tullos HS, Erwin WD, Woods GW, Wukasch DC, Cooley DA, King JW. Unusual lesions of the pitching arm. Clin Orthop Relat Res. 1972;88:169–182. doi:10.1097/00003086-197210000-00029
30. Satou S, Konisi N. The mechanism of fatigue fracture of the ribs. J Japanese Orthop Assoc. 1991;3:1–5.
31. Jeno SH, Varacallo M. Anatomy, Back, Latissimus Dorsi. Statpearls; 2019.
32. Tenforde AS, Sayres LC, McCurdy ML, Sainani KL, Fredericson M. Identifying sex-specific risk factors for stress fractures in adolescent runners. Med Sci Sports Exerc. 2013;45(10):1843–1851. doi:10.1249/MSS.0B013E3182963D75
33. Bulathsinhala L, Hughes JM, McKinnon CJ, et al. Risk of stress fracture varies by Race/Ethnic origin in a cohort study of 1.3 million US army soldiers. J Bone Miner Res. 2017;32(7):1546–1553. doi:10.1002/JBMR.3131
34. Bennell KL, Malcolm SA, Thomas SA, et al. Risk factors for stress fractures in track and field athletes. A twelve-month prospective study. Am J Sports Med. 1996;24(6):810–818. doi:10.1177/036354659602400617
35. Mattila VM, Niva M, Kiuru M, Pihlajamäki H. Risk factors for bone stress injuries: a follow-up study of 102,515 person-years. Med Sci Sports Exerc. 2007;39(7):1061–1066. doi:10.1249/01.MSS.0B013E318053721D
36. Loud KJ, Micheli LJ, Bristol S, Austin SB, Gordon CM. Family history predicts stress fracture in active female adolescents. Pediatrics. 2007;120(2):e364–e372. doi:10.1542/PEDS.2006-2145
37. Escamilla RF, Slowik JS, Diffendaffer AZ, Fleisig GS. Differences among overhand, 3-quarter, and sidearm pitching biomechanics in professional baseball players. J Appl Biomech. 2018;34(5):377–385. doi:10.1123/jab.2017-0211
38. Bullock GS, Thigpen CA, Collins GS, et al. Starting pitchers demonstrate a greater hazard of arm injury compared to relief pitchers. J Athl Train. 2021;57(1):65–71. doi:10.4085/1062-6050-0262.21
39. Karlson KA. Rib stress fractures in elite rowers. A case series and proposed mechanism. Am J Sports Med. 1998;26(4):516–519. doi:10.1177/03635465980260040701
40. Lin YC, Chou PPH, Lin HT, Su FC, Shih CL, Lu CC. A new method for evaluating pelvic and trunk rotational pitching mechanics: from qualitative to quantitative approaches. Int J Environ Res Public Health. 2021. doi:10.3390/ijerph18030905
41. Jones BH, Thacker SB, Gilchrist J, Kimsey CD, Sosin DM. Prevention of lower extremity stress fractures in athletes and soldiers: a systematic review. Epidemiol Rev. 2002;24(2):228–247. doi:10.1093/epirev/mxf011
42. Prynne CJ, Mishra GD, O’Connell MA, et al. Fruit and vegetable intakes and bone mineral status: a cross-sectional study in 5 age and sex cohorts. Am J Clin Nutr. 2006;83(6):1420–1428. doi:10.1093/AJCN/83.6.1420
43. Mountjoy M, Sundgot-Borgen J, Burke L, et al. The IOC consensus statement: beyond the female athlete triad—Relative Energy Deficiency in Sport (RED-S). Br J Sports Med. 2014;48(7):491–497. doi:10.1136/BJSPORTS-2014-093502
44. Lambrinoudaki I, Papadimitriou D. Pathophysiology of bone loss in the female athlete. Ann N Y Acad Sci. 2010;1205(1):45–50. doi:10.1111/J.1749-6632.2010.05681.X
45. Miller TL, Harris JD, Kaeding CC. Stress fractures of the ribs and upper extremities: causation, evaluation, and management. Sport Med. 2013;43(8):665–674. doi:10.1007/s40279-013-0048-7
46. Powell FI. Fracture of the first rib: its occurrence and clinical diagnosis. Br Med J. 1950;1(4648):264–282. doi:10.1136/bmj.1.4648.282
47. Sakellaridis T, Stamatelopoulos A, Andrianopoulos E, Kormas P. Isolated first rib fracture in athletes. Br J Sports Med. 2004;38(3):e5–e5. doi:10.1136/bjsm.2003.009225
48. Turk F, Kurt AB, Saglam S. Evaluation by ultrasound of traumatic rib fractures missed by radiography. Emerg Radiol. 2010;17(6):473–477. doi:10.1007/s10140-010-0892-9
49. Mulligan ME. The “gray cortex”: an early sign of stress fracture. Skeletal Radiol. 1995;24(3). doi:10.1007/BF00228923
50. Anderson MW. Imaging of upper extremity stress fractures in the athlete. Clin Sports Med. 2006;25(3):489–504. doi:10.1016/j.csm.2006.02.006
51. Lampton LM. Conn’s current therapy 2021. In: Conn’s Current Therapy 2021; 2021.
52. Jones GL. Upper extremity stress fractures. Clin Sports Med. 2006;25(1):159–74, xi. doi:10.1016/j.csm.2005.08.008
53. Greaney RB, Gerber FH, Laughlin RL, et al. Distribution and natural history of stress fractures in U.S. marine recruits. Radiology. 1983;146(2):339–346. doi:10.1148/radiology.146.2.6217486
54. Prather JL, Nusynowitz ML, Snowdy HA, Hughes AD, McCartney WH, Bagg RJ. Scintigraphic findings in stress fractures. J Bone Jt Surg. 1977;59(7):869–874. doi:10.2106/00004623-197759070-00006
55. Livingston DH, Shogan B, John P, Lavery RF. CT diagnosis of rib fractures and the prediction of acute respiratory failure. J Trauma. 2008;64(4):905–911. doi:10.1097/TA.0b013e3181668ad7
56. Luceri RE, Glass NE, Bailey JA, et al. First rib fracture: a harbinger of severe trauma? Am J Surg. 2018;216(4):740–744. doi:10.1016/j.amjsurg.2018.07.034
57. Caruso G, Lagalla R, Derchi L, et al. Monitoring of fracture calluses with color Doppler sonography. J Clin Ultrasound. 2000;28(1):20–27. doi:10.1002/(SICI)1097-0096(200001)28:1<20::AID-JCU3>3.0.CO;2-W
58. Papalada A, Malliaropoulos N, Tsitas K, et al. Ultrasound as a primary evaluation tool of bone stress injuries in elite track and field athletes. Am J Sports Med. 2012;40(4):915–919. doi:10.1177/0363546512437334
59. Rao A, Pimpalwar Y, Sahdev R, Sinha S, Yadu N. Diagnostic ultrasound: an effective tool for early detection of stress fractures of Tibia. J Arch Mil Med. 2017;5:2. doi:10.5812/JAMM.57343
60. Boam WD, Miser WF, Yuill SC, Delaplain CB, Gayle EL, MacDonald DC. Comparison of ultrasound examination with bone scintiscan in the diagnosis of stress fractures. J Am Board Fam Pract. 1996;9(6):414–417. doi:10.3122/JABFM.9.6.414
61. Griffith JF, Rainer TH, Ching ASC, Law KL, Cocks RA, Metreweli C. Sonography compared with radiography in revealing acute rib fracture. Am J Roentgenol. 1999;173(6):1603–1609. doi:10.2214/ajr.173.6.10584808
62. De Maeseneer M, De Mey J, Lenchik L, Everaert H, Osteaux M. Helical CT of rib lesions: a pattern-based approach. Am J Roentgenol. 2004;182(1):173–179. doi:10.2214/ajr.182.1.1820173
63. Groves AM, Cheow HK, Balan KK, Housden BA, Bearcroft PWP, Dixon AK. 16-Detector multislice CT in the detection of stress fractures: a comparison with skeletal scintigraphy. Clin Radiol. 2005;60(10):1100–1105. doi:10.1016/J.CRAD.2005.05.014
64. NCRP. Ionizing Radiation Exposure of the Population of the United States. National Council on Radiation Protection and Measurements; Vol. 29. 2009.
65. McCollough CH, Bushberg JT, Fletcher JG, Eckel LJ. Answers to common questions about the use and safety of CT scans. Mayo Clin Proc. 2015;90(10):1380–1392. doi:10.1016/j.mayocp.2015.07.011
66. Choi S; Surgery JY-J of C. Stress fracture of the first rib; 2009. Available from: koreascience.or.kr.
67. Sormaala MJ, Ruohola JP, Mattila VM, Koskinen SK, Pihlajamäki HK. Comparison of 1.5T and 3T MRI scanners in evaluation of acute bone stress in the foot. BMC Musculoskelet Disord. 2011;12(1):128. doi:10.1186/1471-2474-12-128
68. Fredericson M, Bergman AG, Hoffman KL, Dillingham MS. Tibial stress reaction in runners: correlation of clinical symptoms and scintigraphy with a new magnetic resonance imaging grading system. Am J Sports Med. 1995;23(4):472–481. doi:10.1177/036354659502300418
69. Arendt EA, Griffiths HJ. The use of MR imaging in the assessment and clinical management of stress reactions of bone in high-performance athletes. Clin Sports Med. 1997;16(2):291–306. doi:10.1016/S0278-5919(05)70023-5
70. Datir AP, Saini A, Connell D, Saifuddin A. Stress-related bone injuries with emphasis on MRI. Clin Radiol. 2007;62(9):828–836. doi:10.1016/j.crad.2007.02.018
71. Schmid MR, Hodler J, Vienne P, Binkert CA, Zanetti M. Bone marrow abnormalities of foot and ankle: STIR versus T1-weighted contrast-enhanced fat-suppressed spin-echo MR imaging. Radiology. 2002;224(2):463–469. doi:10.1148/radiol.2242011252
72. Breighner RE, Endo Y, Konin GP, Gulotta LV, Koff MF, Potter HG. Zero echo time imaging of the shoulder: enhanced osseous detail by using MR imaging. Radiology. 2018;286(3):960–966. doi:10.1148/radiol.2017170906
73. Kiuru MJ, Pihlajamaki HK, Hietanen HJ, Ahovuo JA. MR imaging, bone scintigraphy, and radiography in bone stress injuries of the pelvis and the lower extremity. Acta Radiol. 2002;43(2):207–212. doi:10.1080/028418502127347790
74. Rosenthall L, Hill RO, Chuang S. Observation on the use of 99Tc(m) phosphate imaging in peripheral bone trauma. Radiology. 1976;119(3):637–641. doi:10.1148/119.3.637
75. Matheson GO, Clement DB, McKenzie DC, Taunton JE, Lloyd-Smith DR, Macintyre JG. Scintigraphic uptake of 99mTc at non-painful sites in athletes with stress fractures: the concept of bone strain. Sport Med. 1987. doi:10.2165/00007256-198704010-00007
76. Dinh T, McWhorter N. Triple Phase Bone Scan. StatPearls; 2018.
77. Larke FJ, Kruger RL, Cagnon CH, et al. Estimated radiation dose associated with low-dose chest CT of average-size participants in the national lung screening trial. Am J Roentgenol. 2011;197(5):1165–1169. doi:10.2214/AJR.11.6533
78. Wajswelner H. Management of rowers with rib stress fractures. Aust J Physiother. 1996;42(2):157–161. doi:10.1016/S0004-9514(14)60448-7
79. Hickey GJ, Fricker PA, McDonald WA. Injuries to elite rowers over a 10-yr period. Med Sci Sports Exerc. 1997;29(12):1567–1572. doi:10.1097/00005768-199712000-00004
80. Geusens P, Emans PJ, de Jong JJA, van den Bergh J. Van Den Bergh J. NSAIDs and fracture healing. Curr Opin Rheumatol. 2013;25(4):524–531. doi:10.1097/BOR.0b013e32836200b8
81. Goodman SB, Ma T, Mitsunaga L, Miyanishi K, Genovese MC, Smith RL. Temporal effects of a COX-2-selective NSAID on bone ingrowth. J Biomed Mater Res. 2005. doi:10.1002/jbm.a.30231
82. Marquez-Lara A, Hutchinson ID, Nuñez F, Smith TL, Miller AN. Nonsteroidal anti-inflammatory drugs and bone-healing: a systematic review of research quality. JBJS Rev. 2016;4(3). doi:10.2106/JBJS.RVW.O.00055
83. Wheatley BM, Nappo KE, Christensen DL, Holman AM, Brooks DI, Potter BK. Effect of NSAIDs on bone healing rates: a meta-analysis. J Am Acad Orthop Surg. 2019;27(7):e330–e336. doi:10.5435/JAAOS-D-17-00727
84. May T, Marappa-Ganeshan R. Stress Fractures. StatPearls [Internet]; 2021. Available from: https://www.ncbi.nlm.nih.gov/books/NBK554538/.
85. Boden BP, Osbahr DC, Jimenez C. Low-risk stress fractures. Am J Sports Med. 2001;29(1):100–111. doi:10.1177/03635465010290010201
86. Galilee-Belfer A, Guskiewicz KM. Stress fracture of the eighth rib in a female collegiate rower: a case report. J Athl Train. 2000;35(4):445–449.
87. Lord MJ, Ha KI, Song KS. Stress fractures of the ribs in golfers. Am J Sports Med. 1996;24(1):118–122. doi:10.1177/036354659602400121
88. Warden SJ, Gutschlag FR, Wajswelner H, Crossley KM. Aetiology of rib stress fractures in rowers. Sport Med. 2002;32(13):819–836. doi:10.2165/00007256-200232130-00002
89. Gurtler R, Pavlov H, Torg JS. Stress fracture of the ipsilateral first rib in a pitcher. Am J Sports Med. 1985;13(4):277–279. doi:10.1177/036354658501300412
90. Ochi M, Sasashige Y, Murakami T, Ikuta Y. Brachial plexus palsy secondary to stress fracture of the first rib: case report. J Trauma. 1994;36(1):128–130. doi:10.1097/00005373-199401000-00024
91. Karlson KA. Thoracic region pain in athletes. Curr Sports Med Rep. 2004;3(1):53–57. doi:10.1249/00149619-200402000-00010
92. Brooke BS, Freischlag JA. Contemporary management of thoracic outlet syndrome. Curr Opin Cardiol. 2010;25(6):535–540. doi:10.1097/HCO.0b013e32833f028e
93. Lin YC, Chuang MT, Hsu CH, Tailor ARA, Lee JS. First rib fracture resulting in Horner’s syndrome. J Emerg Med. 2015;49(6):868–870. doi:10.1016/j.jemermed.2015.07.031
94. Ofri A, Malka V, Lodh S. Horner’s syndrome in traumatic first rib fracture without carotid injury; review of anatomy and pathophysiology. Trauma Case Rep. 2017;8:1–4. doi:10.1016/j.tcr.2017.01.007
95. Patel DS, Roth M, Kapil N. Stress fractures: diagnosis, treatment, and prevention. Am Fam Physician. 2011;83(1):39–46.
96. Griffin XL, Parsons N, Costa ML, Metcalfe D. Ultrasound and shockwave therapy for acute fractures in adults. Cochrane Database Syst Rev. 2014. doi:10.1002/14651858.CD008579.pub3
97. Beck BR, Matheson GO, Bergman G, et al. Do capacitively coupled electric fields accelerate tibial stress fracture healing?: a randomized controlled trial. Am J Sports Med. 2008;36(3):545–553. doi:10.1177/0363546507310076
98. Mollon B, Da Silva V, Busse JW, Einhorn TA, Bhandari M. Electrical stimulation for long-bone fracture-healing: a meta-analysis of randomized controlled trials. J Bone Jt Surg. 2008;90(11):2322–2330. doi:10.2106/JBJS.H.00111
99. Babu S, Sandiford NA, Vrahas M. Use of Teriparatide to improve fracture healing: what is the evidence? World J Orthop. 2015;6(6):457. doi:10.5312/wjo.v6.i6.457
100. Carswell AT, Eastman KG, Casey A, et al. Teriparatide and stress fracture healing in young adults (RETURN – research on efficacy of teriparatide use in the return of recruits to Normal duty): study protocol for a randomised controlled trial. Trials. 2021;22(1). doi:10.1186/s13063-021-05556-3
101. Crockett HC, Gross LB, Wilk KE, et al. Osseous adaptation and range of motion at the glenohumeral joint in professional baseball pitchers. Am J Sports Med. 2002;30(1):20–26. doi:10.1177/03635465020300011701
102. Noonan TJ, Thigpen CA, Bailey LB, et al. Humeral torsion as a risk factor for shoulder and elbow injury in professional baseball pitchers. Am J Sports Med. 2016;44(9):2214–2219. doi:10.1177/0363546516648438
103. Lin HT, Lin YC, Chou YL, Wu HC, Wang RT, Chou PPH. Effect of glenohumeral internal rotation deficit on shoulder in baseball pitchers during fastball pitching. Int J Environ Res Public Health. 2020;17(21):8211. doi:10.3390/ijerph17218211
104. Sciascia A, Cromwell R. Kinetic chain rehabilitation: a theoretical framework. Rehabil Res Pract. 2012. doi:10.1155/2012/853037
105. Devaney LL, Denegar CR, Thigpen CA, Lepley AS, Edgar C, DiStefano LJ. Preseason neck mobility is associated with throwing-related shoulder and elbow injuries, pain, and disability in college baseball pitchers. Orthop J Sport Med. 2020;8(5):232596712092055. doi:10.1177/2325967120920556
106. Proske U, Morgan DL. Muscle damage from eccentric exercise: mechanism, mechanical signs, adaptation and clinical applications. J Physiol. 2001;537(2):333–345. doi:10.1111/j.1469-7793.2001.00333.x
107. Ruohola JP, Laaksi I, Ylikomi T, et al. Association between serum 25(OH)D concentrations and bone stress fractures in Finnish young men. J Bone Miner Res. 2006;21(9):1483–1488. doi:10.1359/jbmr.060607
108. Li X, Heffernan MJ, Mortimer ES. Upper extremity stress fractures and spondylolysis in an adolescent baseball pitcher with an associated endocrine abnormality: a case report. J Pediatr Orthop. 2010;30(4):339–343. doi:10.1097/BPO.0b013e3181dac0c1
109. Lappe JM, Cullen D, Haynatzki G, Recker R, Ahlf R, Thompson K. Calcium and vitamin d supplementation decreases incidence of stress fractures in female navy recruits. J Bone Miner Res. 2008;23(5):741–749. doi:10.1359/JBMR.080102
110. Williams K, Askew C, Mazoue C, Guy J, Torres-McGehee TM, Jackson III JB. Vitamin D3 supplementation and stress fractures in high-risk collegiate athletes – a pilot study. Orthop Res Rev. 2020;12:9–17. doi:10.2147/orr.s233387
111. Myburgh KH, Hutchins J, Fataar AB, Hough SF, Noakes TD. Low bone density is an etiologic factor for stress fractures in athletes. Ann Intern Med. 1990;113(10):754–759. doi:10.7326/0003-4819-113-10-754
112. Lauder TD, Dixit S, Pezzin LE, Williams MV, Campbell CS, Davis GD. The relation between stress fractures and bone mineral density: evidence from active-duty army women. Arch Phys Med Rehabil. 2000;81(1):73–79. doi:10.1053/apmr.2000.0810073
113. Nieves JW, Melsop K, Curtis M, et al. Nutritional factors that influence change in bone density and stress fracture risk among young female cross-country runners. PM R. 2010;2(8):740–750. doi:10.1016/j.pmrj.2010.04.020
114. Abbott A, Wang C, Stamm M, Mulcahey M. Part II: risk factors for stress fractures in female military recruits. Mil Med. 2022. doi:10.1093/milmed/usac033
115. Moran DS, Heled Y, Arbel Y, et al. Dietary intake and stress fractures among elite male combat recruits. J Int Soc Sports Nutr. 2012;9(1). doi:10.1186/1550-2783-9-6
116. Milgrom C, Finestone A, Novack V, et al. The effect of prophylactic treatment with risedronate on stress fracture incidence among infantry recruits. Bone. 2004;35(2):418–424. doi:10.1016/j.bone.2004.04.016
117. Sloan AV, Martin JR, Li S, Li J. Parathyroid hormone and bisphosphonate have opposite effects on stress fracture repair. Bone. 2010;47(2):235–240. doi:10.1016/j.bone.2010.05.015
118. Kidd LJ, Cowling NR, Wu ACK, Kelly WL, Forwood MR. Bisphosphonate treatment delays stress fracture remodeling in the rat ulna. J Orthop Res. 2011;29(12):1827–1833. doi:10.1002/jor.21464
119. Tenforde AS, Carlson JL, Chang A, et al. Association of the female athlete triad risk assessment stratification to the development of bone stress injuries in collegiate athletes. Am J Sports Med. 2017;45(2):302–310. doi:10.1177/0363546516676262
120. Kraus E, Tenforde AS, Nattiv A, et al. Bone stress injuries in male distance runners: higher modified female athlete triad cumulative risk assessment scores predict increased rates of injury. Br J Sports Med. 2019;53(4):237–242. doi:10.1136/bjsports-2018-099861
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.