Back to Journals » Cancer Management and Research » Volume 11
rhTPO combined with chemotherapy and G-CSF for autologous peripheral blood stem cells in patients with refractory/relapsed non-Hodgkin’s lymphoma
Authors Zhu J, Hao SG, Hu J, Zhuang JL ![]() , Wang C, Bai HT
, Wang C, Bai HT
Received 12 June 2019
Accepted for publication 19 August 2019
Published 13 September 2019 Volume 2019:11 Pages 8371—8377
DOI https://doi.org/10.2147/CMAR.S219242
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ahmet Emre Eşkazan
Jun Zhu,1 Si-Guo Hao,2 Jiong Hu,3 Jing-Li Zhuang,4 Chun Wang,1 Hai-Tao Bai1
1Department of Haematology, Shanghai General Hospital, Shanghai 200080, People’s Republic of China; 2Department of Haematology, Shanghai Jiaotong University Affiliated Xinhua Hospital, Shanghai 200092, People’s Republic of China; 3Department of Haematology, Shanghai Jiaotong University Affiliated Ruijing Hospital, Shanghai 200020, People’s Republic of China; 4Department of Haematology, Fudan University Affiliated Zhongshan Hospital, Shanghai 200032, People’s Republic of China
Correspondence: Chun Wang; Hai-Tao Bai
Department of Haematology, Shanghai General Hospital, No. 100 Haining Road, Hongkou District, Shanghai 200080, People’s Republic of China
Tel +86 216 324 0090; +86 216 324 0090-3171
Fax +86 213 779 8078
Email [email protected]; [email protected]
Objective: The mobilization and collection of sufficient autologous peripheral blood stem cells (APBSCs) are important for the fast and sustained reconstruction of hematopoietic function after autologous transplantation. This study aims to evaluate the mobilization effect and safety of thrombopoietin (TPO) combined with chemotherapy + G-CSF for APBSCs in patients with refractory/relapsed non-Hodgkin’s lymphoma.
Methods: A total of 78 patients were included in the present study. After receiving mobilization chemotherapy, all patients were randomly divided into two groups: TPO group (n=40), patients were given subcutaneous injection of rhTPO + G-CSF, and control group (n=38), patients were given subcutaneous injection of G-CSF. The primary endpoint was the total number of obtained CD34+ cells. The secondary endpoints were the mononuclear cell count, the proportion of target and minimum mobilization, the engraftment time of neutrophils and platelets after APBSCT, the number of platelet and red blood cell infusions, the incidence of infectious fever and fever duration, and TPO-related side effects in patients.
Results: TPO participation significantly increased the total CD34+ cell count. A higher proportion of patients in the TPO group achieved the minimum and target CD34+ cells, when compared to the control group. TPO-related adverse events were not observed in either of these groups. In addition, there were no significant differences in engraftment time, the number of platelet and red blood cell transfusions, the incidence of infectious fever, and fever duration between these two groups.
Conclusion: TPO combined with chemotherapy + G-CSF can safely and effectively enhance the mobilization effect for APBSCs in patients with refractory/relapsed non-Hodgkin’s lymphoma.
Keywords: recombinant human thrombopoietin, mobilization, non-Hodgkin’s
Introduction
Autologous peripheral blood stem cell transplantation (APBSCT) has been widely used in the treatment of hematologic and solid tumours and autoimmune diseases, and has achieved significant efficacy, especially for non-Hodgkin’s lymphoma (NHL).1 The mobilization and collection of sufficient peripheral blood stem cells is a prerequisite to ensure the fast and sustained reconstruction of hematopoietic function after autologous transplantation in patients. In general, when the collected CD34+ cell count is greater than 5×106 cells/kg, the successful engraftment of neutrophils and platelets can be guaranteed in almost patients. In contrast, transplanted CD34+ cells of less than 1–2×106 cells/kg may cause delayed hematopoietic recovery or engraftment failure. Therefore, the collection of 2×106 CD34+ cells/kg is considered the minimal cell threshold for autologous stem cell transplantation.2 Mobilization efficacy is influenced by many factors, including the disease type, patient age, disease stage, previous chemotherapy and treatment course, previous history of radiotherapy, mobilization program, and determination of whether the tumour cells have invaded the bone marrow.3 In particular, the number and intensity of previous chemotherapy and radiotherapy have the greatest impact on the mobilization effect of autologous stem cells. For most patients with refractory/relapsed NHL, mobilization efficacy may be poor due to multiple previous cytotoxic therapies. As reported in literature, nearly 30% of patients lose their chance for autologous stem cell transplantation, because the number of mobilized stem cells could not reach the minimum threshold (2×106 cells/kg).4,5 Therefore, the optimization of the mobilization program to increase the number of collected hematopoietic stem cells has important clinical significance.
For lymphoma patients, the commonly used standard mobilization regimen is chemotherapy combined with cytokines. These chemotherapy regimens include high-dose cyclophosphamide (CTX) and high doses of etopside, ESHAP (a combination of etoposide, solu-medrone, high-dose Ara C, and cisplatin) and DHAP (a combination of dexamethasone, high-dose Ara C and cisplatin), with granulocyte colony stimulating factor (G-CSF) commonly used as the cytokine.6,7 Thrombopoietin (TPO) is one of the cytokinins, and is a plasma glycoprotein. TPO can affect the proliferation and maturation of megakaryocytes and release platelets in blood, which is the major physiological factor involved in the regulation of platelet levels in the circulatory system.8 It has been reported that recombinant human thrombopoietin (rhTPO) can enhance the mobilization of peripheral blood progenitor cells (PBPCs) in cancer patients.9 A recent cohort study also revealed that rhTPO augments the efficacy of intermediate-dose cyclophosphamide and G-SCF in the mobilization of peripheral blood stem cells in patients with multiple myeloma.10 Furthermore, a study has confirmed that the mobilization program of rhTPO combined with G-CSF and chemotherapy could improve the mobilization efficacy of peripheral blood stem cells in breast cancer patients.11
Therefore, it is speculated that rhTPO can effectively improve the mobilization efficacy of peripheral blood stem cells in refractory/relapsed lymphoma. The present prospective, multi-center and randomized controlled clinical study was conducted to evaluate the efficacy and safety of rhTPO in mobilizing peripheral blood stem cells in patients with relapsed/refractory lymphoma.
Materials and methods
Patients
The age of these 78 patients included in the present study ranged within 18–60 years old. These patients had refractory/recurring NHL, and experienced failure of first-line chemotherapy. The initial diagnosis was confirmed by pathological biopsy and immunohistochemical staining. The Eastern Cooperative Oncology Group (ECOG) performance status scale was 0 or 1, showing normal organ function. The exclusion criteria were as follows: liver dysfunction (alanine aminotransferase or bilirubin greater than two times the normal upper limit); renal dysfunction (creatinine or urea higher than 1.5 times the normal upper limit); cardiac dysfunction (cardiac insufficiency over level II); respiratory failure; history of venous thrombosis; ischemic heart disease; stroke; arrhythmias, uncontrolled hypertension, or diabetes; severe diabetic retinopathy; previous treatment with high-dose chemotherapy, followed by autologous stem cell transplantation; the administration of cytokines other than G-CSF within three weeks prior to mobilization; uncontrolled active infection; rhTPO allergies; pregnant or lactating women; severe acute or chronic mental illness. This study was conducted in accordance with the declaration of Helsinki and approved by the Institutional Review Board of Shanghai General Hospital, and is registered under the Chinese Clinical Trial Registry (Trial registry number: ChiCTR-IIR-17010787). All patients provided a signed informed consent.
Study design
The present study was a prospective, multi-center and randomized controlled study. A total of 78 cases of NHL were enrolled from Shanghai General Hospital, Fudan University Affiliated Zhongshan Hospital, Shanghai Jiaotong University Affiliated Ruijin Hospital, and Shanghai Jiaotong University Affiliated Xinhua Hospital from July 2010 to July 2015. All patients received CTX and etoposide chemotherapy, with a detailed regimen of intravenous CTX (2.0 g/m2) on day one and two, and VP16 (200 mg/m2) on day one. All patients were randomly divided into two groups: TPO group and control group. For patients in the control group, 7.5 μg/kg of G-CSF (Filgrastin, Kirin Do., Japan) was subcutaneously injected from day four to the end of the stem cell collection. For patients in the TPO group, 15,000 U of rhTPO (Shenyang Sunshine Pharmaceutical Co. Ltd., China) was subcutaneously injected daily from day four to the end of the stem cell collection in addition to G-CSF. When the peripheral blood white blood cell count was ≥10×109 cells/L, mononuclear cells (MNCs) were collected from the peripheral blood using a cell separator (COBESpectra, USA), and the total blood volume processed for each patient varied between 10 L and 15 L. Flow cytometry was used for CD34+ cell counting. The collection was stopped when the number of CD34+ cells reached 5×106 cells/kg. The collection was performed for no more than three times. The mobilization was considered a failure when the collected CD34+ cells in any of the three attempts did not reach 2×106 cells/kg.
The collected peripheral blood MNCs were placed in an immortalization solution containing 10% dimethyl sulfoxide (DMSO) and phenol for cryopreservation at −80 °C. According to CTC 3.0, the type, incidence, severity and duration of adverse events, as well as the correlation with TPO, were evaluated. The primary endpoint of the mobilization phase was the total CD34+ cell count. The secondary endpoints included the total mononuclear cell count, the number of days from mobilization to stem cell collection, the “optimal” rate (the proportion of patients with CD34+ cells >5×106 cells/kg) and “minimum” rate (the proportion of patients with CD34+ cells >2×106 cells/kg) of collection, and TPO-related side effects.
Patients with a collected cell number that reached the minimum cell number threshold (2×106 CD34+ cells/kg) for transplantation received the subsequent high-dose chemotherapy and autologous stem cell reinfusion. The BEAM regimen was used for conditioning (BCNC 300 mg/m2, d-6; etoposide 150 mg/m2, d-5-d-2; cytarabine 300 mg/m2, d-5-d-2; melphalan 140 mg/m2, d-1). At 48 hrs after the end of the pre-treatment, PBPC reinfusion was performed. In order to promote hematopoietic recovery, G-CSF (5 μg/kg/d) was subcutaneously injected when neutrophils were less than 0.5×109 cells/L, and until these were higher than 2×109 cells/L. No other cytokine types, including GM-CSF, IL-11, or TPO, were used. Patients with platelet counts <20×109 platelets/L or a tendency for bleeding were given platelet transfusions, while patients with hemoglobin (HB) of <80 g/L or severe symptoms of anemia were given red blood cell transfusions. All blood products were irradiated with 2.5 GY to inactivate the lymphocytes. The endpoints of the hematopoietic reconstitution phase were as follows: time of platelet engraftment (defined as platelet count >20×109 platelets/L for seven consecutive days without platelet transfusion), time of neutrophil engraftment (defined as the absolute value of neutrophils >0.5×109 cells/L for three consecutive days), the number of platelet and red blood cell transfusions, and the proportion of patients with infectious fever and fever duration.
Statistical analysis
Statistical analysis software SAS 9.13 was used for the computation. All statistical tests were performed using two-sided tests. Differences with P-values ≤0.05 were considered statistically significant. For the comparison of demographic and clinical data between groups, Fisher’s exact test was used for binary data or unordered multi-category data, two-sample rank sum test was used for ranked data or measurement data that are not normally distributed, and a Student's t-test was used for normally distributed data.
Results
Patient information
These 78 NHL patients were randomly divided into two groups: TPO group (n=40) and control group (n=38) (Table 1). The diagnoses of patients in the TPO group were as follows: diffuse large B-cell lymphoma (DLBCL, n=32), mantle cell lymphoma (MCL, n=4), follicular lymphoma (FL, n=2), and peripheral T-cell lymphoma (PTCL, n=2). The diagnoses of patients in the control group were as follows: DLBCL (n=33), MCL (n=3), FL (n=1), and Burkitt lymphoma (n=1). These two groups of patients had no significant differences in age, gender, clinical stage, disease status prior to mobilization, the determination of whether they received radiotherapy, bone marrow invasion, the number of courses of previous chemotherapy, and the number of different diagnoses. In the control group, five patients were considered to have failed stem cell mobilization, because the collected CD34+ cells did not meet the standard (<2×106 CD34+ cells/kg). Therefore, these patients did not receive the subsequent high-dose chemotherapy + autologous stem cell transplantation.
 |
Table 1 Patient characteristics |
Mobilization efficacy of TPO
TPO participation did not significantly increased the mononuclear cell count, when compared to controls (6.89 vs 6.35×108 cells/kg, P>0.05; Table 2). However, the total number of CD34+ cells in the TPO group was nearly twice of that in the control group (6.35 vs 3.3×106 cells/kg, P<0.01). Furthermore, there was no mobilization failure cases in the TPO group, because the CD34+ cells collected from all patients met the minimal threshold (>2×106 cells/kg), while five patients (14%) in the control group failed to meet this standard. The TPO group had a greater advantage in the optimarate (>5×106 CD34+ cells/kg) in the mobilization (72.9% vs 41.3%, P<0.05). The days from the beginning of mobilization to stem cell collection were not significantly different, with 11 days in both groups. The numbers of apheresis were also not significantly different between the two groups. The total number of patients in the TPO group who received 8–14 injections had a median value of 11. The cost of the TPO mobilization cycle ranged within 8,504–14,882 yuan, with a median value of 11,693 yuan (equivalent to 1,131–1,984 euros, with a median value of 1,558). Furthermore, TPO-related side effects were not observed during the mobilization.
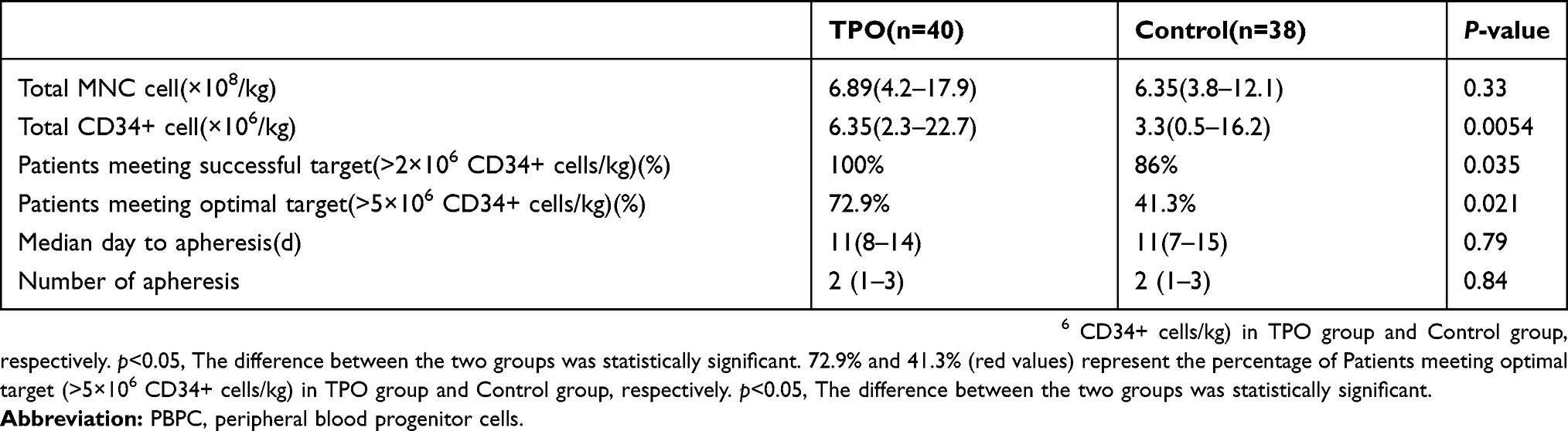 |
Table 2 Results of PBPC collection |
Impact of TPO on hematopoietic reconstitution after autologous transplantation
The addition of TPO in the mobilization program had no effect on neutrophil engraftment time, with a median of 12 days in both groups (Table 3). The platelet engraftment time was slightly shorter in the TPO group, when compared to the control group, but the difference was not statistically significant (12 vs 14, P>0.05). During the autologous transplantation phase, the TPO and control groups received a median of three and four times of platelet transfusions, respectively, and both groups received a median of four times of red blood cell transfusions. Furthermore, the proportion of patients with infectious fever was 42% and 48%, respectively, and the median day of fever was four days and three days, respectively, which was not significantly different.
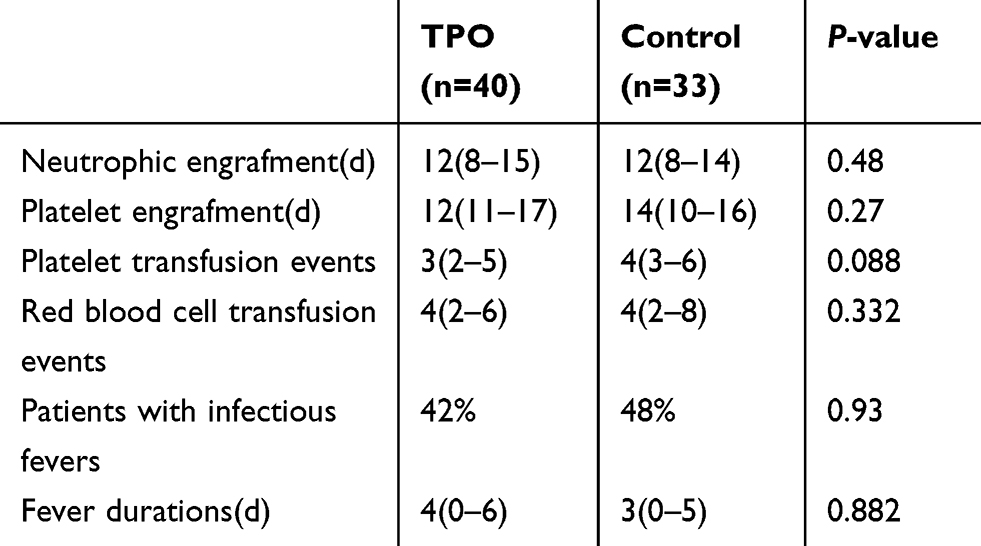 |
Table 3 Results of hematopoietic reconstitution |
Discussion
A successful APBSCT requires the infusion of the minimum amount of hematopoietic stem cells to ensure the completion of continuous hematopoietic reconstruction within a certain amount of time after high-dose chemotherapy. Several studies have shown that the number of hematopoietic stem cells infused and engraftment time are clearly correlated.12–14 The objective of the mobilization process is to collect a sufficient number of stem cells (i.e. a sufficient number of CD34+ cells), which is correlated to rapid haematopoietic recovery. At present, 2×106 CD34+ cells/kg has generally been considered the minimum threshold, and cases with a value lower than this standard may not achieve a fully sustained hematopoietic recovery. However, since the use of ≥5×106 CD34+ cells/kg was correlated to faster neutrophil and platelet recovery with little difference between patients, this number was considered the optimal target for autologous HSCT.15
Although chemotherapy plus G-CSF was effective for stem cell mobilization in most patients, a considerable number of patients still failed the mobilization. The most common cause of mobilization failure was previous chemotherapy with bone marrow toxicity.16,17 Recently, the deepening understanding of the biology of stem cell mobilization has enabled the application of many new strategies to improve the quantity and quality of production of stem cells, and reduce the risk of mobilization failure.18 Plerixafor is the most well-studied mobilization synergist, and is thereby the most widely applied. As an antagonist for chemokine receptors, plerixafor combined with G-CSF is approved by the Food and Drug Administration (FDA) for PBSC mobilization in patients with NHL and multiple myeloma (MM), who failed the mobilization, or are predicted to have poor mobilization. In patients who failed the mobilization, 60% of NHL cases and 71% of MM cases have achieved successful re-mobilization using plerixafor.19–21 However, plerixafor is not yet commercially available in China, and its high price is expected to limit its wide application. Therefore, for patients with poor predicted mobilization efficacy (especially patients with refractory/relapsed NHL), the design of an alternative, efficient and inexpensive mobilization program has become a hotspot of APBSCT research, with the aim of increasing the number of collected hematopoietic stem cells, reducing the failure rate of mobilization, and ensuring that more patients have the opportunity for autologous transplantation.
The rhTPO is a full-length glycosylated thrombopoietin prepared from Chinese hamster by recombinant DNA technology, which has a pharmacological effect similar to endogenous TPO. Both in vitro and in vivo experiments have confirmed that rhTPO not only effectively enhances platelet levels, but also stimulates the growth of hematopoietic progenitor cells to increase their pluripotency.22 Animal experiments have also confirmed that the synergy of TPO and G-CSF greatly shortens the time for platelet, red blood cell and neutrophil generation, and speeds up the recovery of erythroid and megakaryocytic precursor cells in the bone marrow.23 Somlo et al observed for the first time that rhTPO combined with G-CSF for mobilization in breast cancer significantly increased the number of collected CD34+ cells and shortened the platelet and neutrophil engraftment time during the autologous transplantation process, while reducing the amount of red blood cell and platelet transfusions.11 The study conducted by Linker et al, which comprised of 134 patients with hematological malignancies, indicated that rhTPO participation in the mobilization reduced the number of collections.9 The cases included in the present study were all refractory/relapsed NHL patients, and most of them previously received many rounds of repeated cytotoxic chemotherapy, and were considered as a high-risk group with failure in mobilization. It was found that rhTPO was an effective mobilization enhancer that could significantly improve the mobilization effect for peripheral blood stem cells in relapsed/refractory NHL patients when combined with chemotherapy and G-CSF, resulting in an increase in CD34+ cell yield by nearly 50%. Furthermore, the participation of rhTPO allowed a greater proportion of patients to achieve the target collection value. It was particularly important that all patients in the TPO group reached the minimum acquisition threshold, with no mobilization failure cases. All the patients in this group successfully underwent the subsequent high-dose chemotherapy and autologous stem cell transplantation, and the hematopoietic cells were successfully engrafted in all patients, with no cases of delayed engraftment or engraftment failure. In addition, TPO exhibited good safety, and no TPO-related adverse events occurred during the mobilization, such as excessive platelet increase or a thrombotic event.
The time of hematopoietic reconstitution after transplantation is significantly correlated with the number of CD34+ cell infusions. In the present study, although the number of collected CD34+ cells was higher in the TPO group at the transplant stage, the cases in the TPO group did not show a significant advantage in shortening the neutrophil and platelet engraftment time. The possible explanations for this observation are that five patients in the control group failed the mobilization and did not enter the autologous transplantation stage, which “optimized” the control group data, and the size of the included samples was relatively small. Therefore, future studies with a larger number of samples would be conducive to obtain a more objective conclusion. Also, it is important to evaluate the long-term safety of TPO therapy in further investigations, in which the TPO-related adverse events such as secondary carcinogenesis need to be monitored. In conclusion, the present study revealed that the participation of rhTPO, as a synergist of the mobilization of peripheral blood stem cells based on chemotherapy + G-CSF in refractory/relapsed NHL patients, significantly improved mobilization efficacy and safety. High quality mobilization can ensure post-transplantation hematopoietic reconstruction, which is expected to be used to some extent in patients with mobilization failure or a poor predicted mobilization result, as an alternative to plerixafor in China. This approach is worth promoting in clinical application.
Ethical approval
The present study was approved by the Institutional Review Board of Shanghai General Hospital, and is registered under the Chinese Clinical Trial Registry (Trial registry number: ChiCTR-IIR-17010787).
Informed consent
All patients provided a signed informed consent form.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Zahid U, Akbar F, Amaraneni A, et al. A review of autologous stem cell transplantation in lymphoma. Curr Hematol Malig Rep. 2017;12(3):217–226. doi:10.1007/s11899-017-0382-1
2. Sheppard D, Bredeson C, Allan D, Tay J. Systematic review of randomized controlled trials of hematopoietic stem cell mobilization strategies for autologous transplantation for hematologic malignancies. Biol Blood Marrow Transplant. 2012;18(8):1191–1203. doi:10.1016/j.bbmt.2012.01.008
3. Moskowitz CH, Glassman JR, Wuest D, et al. Factors affecting mobilization of peripheral blood progenitor cells in patients with lymphoma. Clin Cancer Res. 1998;4(2):311–316. PMID: 9516916.
4. Devine SM, Flomenberg N, Vesole DH, et al. Rapid mobilization of CD34+ cells following administration of the CXCR4 antagonist AMD3100 to patients with multiple myeloma and non-Hodgkin’s lymphoma. J Clin Oncol. 2004;22(6):1095–1102. doi:10.1200/JCO.2004.07.131
5. To LB, Levesque JP, Herbert KE. How I treat patients who mobilize hematopoietic stem cells poorly. Blood. 2011;118(17):4530–4540. doi:10.1182/blood-2011-06-318220
6. Gisselbrecht C, Glass B, Mounier N, et al. Salvage regimens with autologous transplantation for relapsed large B-cell lymphoma in the rituximab era. J Clin Oncol. 2010;28(27):4184–4190. doi:10.1200/JCO.2010.28.1618
7. van Gorkom G, Finel H, Giebel S, et al. Prospective noninterventional study on peripheral blood stem cell mobilization in patients with relapsed lymphomas. J Clin Apher. 2017;32(5):295–301. doi:10.1002/jca.21506
8. Kaushansky K. Thrombopoietin: understanding and manipulating platelet production. Annu Rev Med. 1997;48:1–11. doi:10.1146/annurev.med.48.1.1
9. Linker C, Anderlini P, Herzig R, et al. Recombinant human thrombopoietin augments mobilization of peripheral blood progenitor cells for autologous transplantation. Biol Blood Marrow Transplant. 2003;9(6):405–413. PMID: 12813449.
10. Wang G, Chen W, Wu Y, Li Y, Leng Y, Liu A. Recombinant human thrombopoietin improves the efficacy of intermediate-dose cyclophosphamide plus granulocyte colony-stimulating factor in mobilizing peripheral blood stem cells in patients with multiple myeloma: a cohort study. Medicine (Baltimore). 2017;96(50):e9302. doi:10.1097/MD.0000000000009302
11. Somlo G, Sniecinski I, Ter Veer A, et al. Recombinant human thrombopoietin in combination with granulocyte colony-stimulating factor enhances mobilization of peripheral blood progenitor cells, increases peripheral blood platelet concentration, and accelerates hematopoietic recovery following high-dose chemotherapy. Blood. 1999;93(9):2798–2806. PMID: 10216073.
12. Haverkos B, Geyer S, McBride A, et al. Mobilization for autologous stem cell transplantation in Hodgkin’s lymphoma (HL) and non-Hodgkin lymphoma: a single institution experience. Biol Blood Marrow Transplant. 2014;20(2):S111–S112. doi:10.1016/j.bbmt.2013.12.160
13. Tomblyn M, Burns LJ, Blazar B, et al. Difficult stem cell mobilization despite adequate CD34+ cell dose predicts shortened progression free and overall survival after autologous HSCT for lymphoma. Bone Marrow Transplant. 2007;40(2):111–118. doi:10.1038/sj.bmt.1705708
14. Canales M, Fernández-Jiménez MC, Martín A, et al. Identification of factors associated with poor peripheral blood progenitor cell mobilization in Hodgkin’s disease. Haematologica. 2001;86(5):494–498. PMID: 11410412.
15. Yoon DH, Sohn BS, Jang G, et al. Higher infused CD34+ hematopoietic stem cell dose correlates with earlier lymphocyte recovery and better clinical outcome after autologous stem cell transplantation in non-Hodgkin’s lymphoma. Transfusion. 2009;49(9):1890–1900. doi:10.1111/j.1537-2995.2009.02202.x
16. Ataca Atilla P, Bakanay Ozturk SM, Demirer T. How to manage poor mobilizers for high dose chemotherapy and autologous stem cell transplantation? Transfus Apher Sci. 2017;56(2):190–198. doi:10.1016/j.transci.2016.11.005
17. Herbert KE, Levesque JP, Mills AK, et al. How we mobilize haemopoietic stem cells. Intern Med J. 2011;41(8):588–594. doi:10.1111/j.1445-5994.2011.02544.x
18. Bensinger W, DiPersio JF, McCarty JM. Improving stem cell mobilization strategies: future directions. Bone Marrow Transplant. 2009;43(3):181–195. doi:10.1038/bmt.2008.410
19. Jantunen E, Varmavuo V, Valtola J. Plerixafor injection: a hematopoietic stem cell mobilizer in non-Hodgkin lymphoma and multiple myeloma. Expert Rev Hematol. 2016;9(8):723–732. doi:10.1080/17474086.2016.1208082
20. Salvino MA, Ruiz J. Hematopoietic progenitor cell mobilization for autologous transplantation-a literature review. Rev Bras Hematol Hemoter. 2016;38(1):28–36. doi:10.1016/j.bjhh.2015.07.011
21. Bilgin YM, de Greef GE. Plerixafor for stem cell mobilization: the current status. Curr Opin Hematol. 2016;23(1):67–71. doi:10.1097/MOH.0000000000000200
22. Wagemaker G, Hartong SC, Neelis KJ, Egeland T, Wognum AW. In vivo expansion of hemopoietic stem cells. Stem Cells. 1998;16:185–191. doi:10.1002/stem.5530160822
23. Wagemaker G, Neelis KJ, Hartong SC, et al. The efficacy of recombinant thrombopoietin in murine and nonhuman primate models for radiation-induced myelosuppression and stem cell transplantation. Stem Cells. 1998;16(6):375–386. doi:10.1002/stem.160375
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.