Back to Journals » Open Access Rheumatology: Research and Reviews » Volume 13
Rheumatoid Arthritis Onset from Shoulder Monoarthritis
Authors Ishida K, Nagira K, Hagino H, Enokida M, Hayashi I, Hayashibara M, Takeda C, Nagashima H
Received 26 December 2020
Accepted for publication 19 March 2021
Published 7 May 2021 Volume 2021:13 Pages 103—109
DOI https://doi.org/10.2147/OARRR.S297106
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Chuan-Ju Liu
Koji Ishida,1 Keita Nagira,1 Hiroshi Hagino,2 Makoto Enokida,1 Ikuta Hayashi,1 Masako Hayashibara,1 Chikako Takeda,1 Hideki Nagashima1
1Department of Orhopedic Surgery, Faculty of Medicine, Tottori University, Yonago, Tottori, Japan; 2School of Health Science, Faculty of Medicine, Tottori University, Yonago, Tottori, Japan
Correspondence: Keita Nagira
Department of Orhopedic Surgery, Faculty of Medicine, Tottori University, 36-1 Nishi-cho, Yonago, Tottori, Japan
Tel +81-859-38-6587
Fax +81-859-38-6589
Email [email protected]
Purpose: To investigate the incidence and clinical characteristics of rheumatoid arthritis (RA) presenting with shoulder monoarthritis.
Patients and Methods: Our study included 113 patients (77 females; mean age, 63.0 ± 13.1 years) whom we newly diagnosed with RA in 2012– 2016. We investigated cases with onset from shoulder monoarthritis. Specifically, we examined physical findings, blood test results, radiographic findings, magnetic resonance imaging (MRI) findings, and duration from initial visit to diagnosis. RA was diagnosed based on the 2010 American College of Rheumatology/European League Against Rheumatism (ACR/EULAR) classification criteria.
Results: Overall, mean 2010 ACR/EULAR criteria score was 6.8 ± 1.8, and median duration to diagnosis was 3 days (interquartile range: 0– 14). Two patients (1.8%) were identified as having RA with onset from shoulder monoarthritis. Both were late middle-aged women with MRI findings of rotator cuff tear and remarkable synovial proliferation. However, neither patient fulfilled the 2010 ACR/EULAR criteria. It took 85 and 98 days to make a definitive diagnosis, respectively.
Conclusion: Early diagnosis is difficult when RA synovitis develops from shoulder monoarthritis, especially, in elderly patients who have a rotator cuff tear. In addition to MRI, culture-based and pathological examinations may be helpful for early diagnosis of RA.
Keywords: rheumatoid arthritis, monoarthritis, shoulder, rotator cuff tear
Introduction
Rheumatoid arthritis (RA) presenting with onset from shoulder monoarthritis is uncommon. There are several reports of shoulder joint symptoms caused by RA.1–3 In particular, patients with elderly-onset rheumatoid arthritis have large joint involvement and shoulder symptoms more often than patients with younger-onset rheumatoid arthritis.4–6 However, in these reports shoulder arthritis was one symptom of polyarthritis. There are no reports of RA onset with only shoulder monoarthritis. Therefore, the incidence of RA onset from shoulder monoarthritis remains unclear. We encountered such cases, which were difficult to diagnose. Thus, the aim of this study was to investigate the incidence and clinical characteristics of RA presenting with onset of shoulder monoarthritis, identify causes of diagnostic difficulties, and propose useful methods for early diagnosis.
Patients and Methods
This study involved medical record review. Our study included 113 patients (36 males, 77 females) whom we newly diagnosed with RA from January 2012 to December 2016 in the department of orthopedics at our hospital. Mean age was 63.0 ± 13.1 years; the age range was 18–89 years. The patients were diagnosed with RA based on the 2010 American College of Rheumatology/European League Against Rheumatism (ACR/EULAR) classification criteria for RA (≥6 points).7 Patients who did not fulfill the 2010 ACR/EULAR criteria (<6 points) were diagnosed with RA based on rheumatologist judgment of their clinical course, assessment of synovitis in affected joints based on contrast-enhanced magnetic resonance imaging (MRI) or power Doppler ultrasonography, and exclusion of other diseases that could cause arthritis. We excluded patients with insufficient data or a prior diagnosis of RA at another hospital or department. We identified patients who had chronic (3 months or more) shoulder monoarthritis with no any other joint pain and swelling at the time of diagnosis. We examined their shoulder radiographic and MRI findings. Furthermore, we investigated the duration from initial visit to definitive diagnosis.
Results
Eighty-nine patients were diagnosed with RA because they fulfilled the 2010 ACR/EULAR classification criteria (≥6 points). Twenty-four patients who did not fulfill the criteria (<6 points) were diagnosed with RA based on rheumatologist judgment. RA with onset of shoulder monoarthritis was identified in 2 of 113 (1.8%) patients. The characteristics of all patients and the two patients with shoulder monoarthritis are shown in Table 1. Eighty-nine (78.8%) patients fulfilled the 2010 ACR/EULAR classification criteria. Mean score among all patients was 6.8 ± 1.8 points. Median duration from initial visit to diagnosis was 3 days (interquartile range: 0–14). Both patients with RA onset consisting of shoulder monoarthritis were late middle-aged women and MRI of the shoulder showed rotator cuff (RC) tear and remarkable synovial proliferation. In addition, they did not fulfill the 2010 ACR/EULAR classification criteria (<6 points). They could not be diagnosed with RA at the first visit; duration from initial visit to diagnosis was 85 and 98 days, respectively. Mean ACR/EULAR score among all patients was 6.8 ± 1.8 points. The diagnosis of both patients with RA onset consisting of shoulder monoarthritis was delayed compared to diagnosis for the other patients.
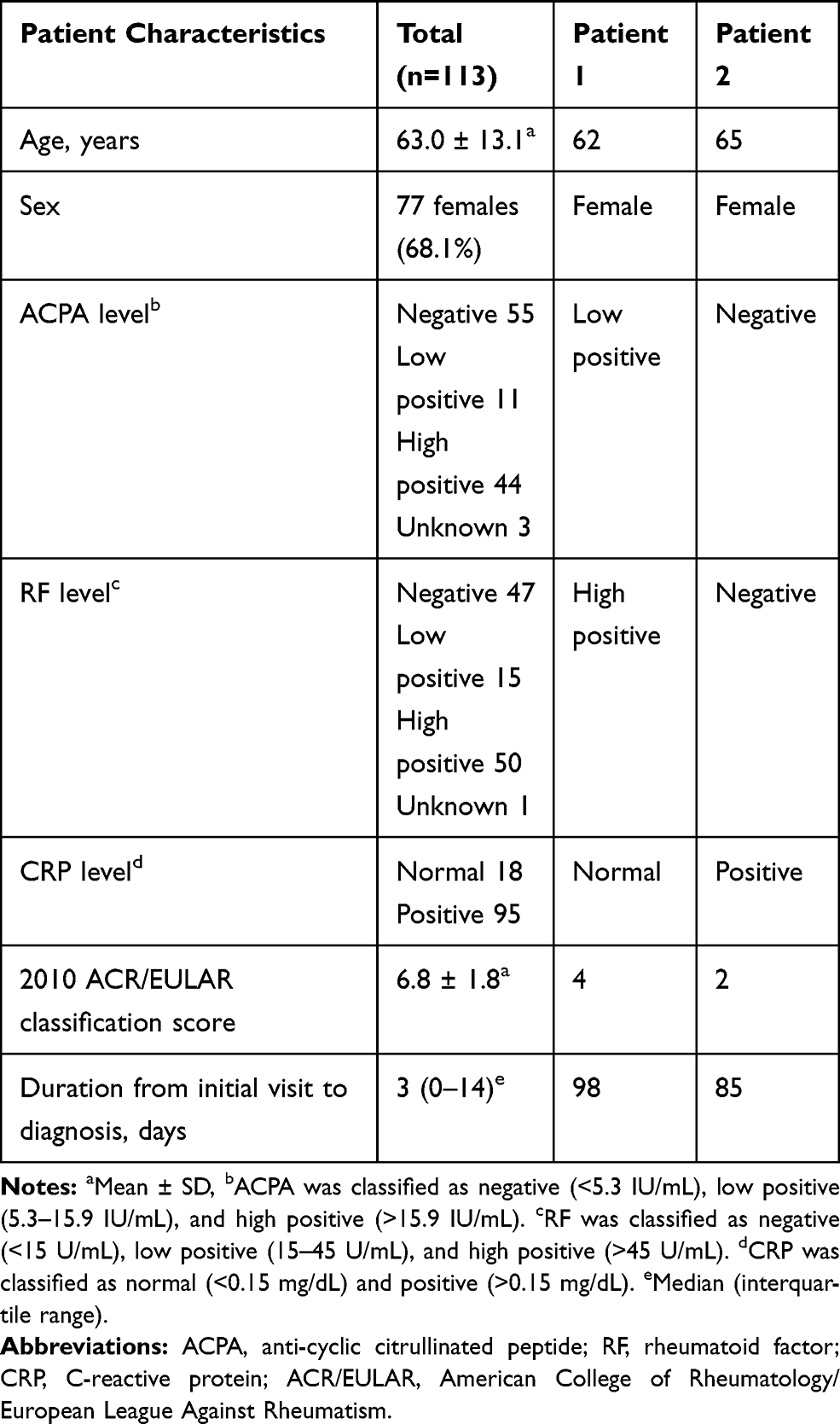 |
Table 1 Characteristics of All Patients Whom We Newly Diagnosed with Rheumatoid Arthritis (RA) and Two Patients with Only Shoulder Monoarthritis at Onset |
Patient 1
A 62-year-old woman with dyslipidemia and no family history of RA presented with right shoulder pain over the past 8 months. She was diagnosed with RC tear at a primary care clinic and sought consultation at our hospital. On physical examination, she had only right shoulder tenderness and swelling. Pain on motion and limited range of motion in the right shoulder were observed at that time. The supraspinatus (SSP) and infraspinatus (ISP) had fair muscle strength during manual muscle test (MMT). Impingement signs were also positive. There was no other joint swelling or tenderness. Radiography of the right shoulder did not show bone atrophy or erosion (Figure 1A). MRI of the right shoulder showed RC tears (SSP and ISP tears); remarkable synovial proliferation in the glenohumeral (GH) joint, subacromial space, bicipital sulcus, and subscapularis bursa (Figure 1B and C); and GH joint effusion. Laboratory tests revealed low levels of inflammatory markers and positive serological markers for RA: C-reactive protein (CRP) was 0.03 mg/dL, rheumatoid factor (RF) was 50.0 U/mL, and anti-cyclic citrullinated peptide (ACPA) was 12.4 IU/mL. She could not be definitively classified with RA because she scored 4 points according to the 2010 ACR/EULAR classification criteria. Therefore, we could not determine whether her synovitis was due to the RC tear or RA. A corticosteroid injection in the GH joint was effective for only a short period. Three months later, her symptoms did not improve and CRP was 1.11 mg/dL. At this time, she was diagnosed with RA based on the clinical course, although she scored 5 points according to the 2010 ACR/EULAR classification criteria. She started oral prednisolone therapy (5 mg daily). Her right shoulder pain decreased. Three months after the start oral prednisolone therapy, CRP decreased to 0.31 mg/dL, but increased to 1.18 mg/dL after another 3 months. MRI showed more severe bone erosion of the humeral head and synovial proliferation. Radiography also showed bone erosion at this time (Figure 1D–F). Therefore, oral salazosulfapyridine (1000 mg daily) was added. One year later, she developed bilateral knee pain and swelling, and methotrexate (MTX) was added at a dose of 8 mg weekly. One month after starting MTX, CRP decreased to 0.06 mg/dL, but then increased again and remained around 1.00 mg/dL. Since her polyarthritis was poorly controlled even with MTX, she was started on the biological disease-modifying antirheumatic drug infliximab at 3 mg/kg. Six months later, the dose of infliximab increased to 6 mg/kg. However, suppression of polyarthritis was temporary. Thus, she was switched to certolizumab pegol 400 mg every 2 weeks. Since the start of treatment with certolizumab pegol, her symptoms decreased and CRP has remained normal.
 |
Figure 1 X-ray and magnetic resonance imaging (MRI) of the right shoulder in Patient 1. At the first visit, X-ray showed no bone erosion (A) and T2-weighted MRI showed synovial proliferation in the glenohumeral joint and rotator cuff tears (B). There were only slight bone signals in the humeral head (C). Nine months later, X-ray showed bone erosions in the humeral head (D) and MRI showed much more remarkable synovial proliferation and numerous bone erosions in the humeral head (E and F). |
Patient 2
A 65-year-old woman with a history of right shoulder periarthritis for approximately 10 years and no family history of RA visited a primary care clinic because her shoulder pain was aggravated 1 month prior. She was diagnosed with RC tear. She sought consultation at our hospital for surgery. On physical examination, she had right shoulder tenderness but no swelling. MMT showed poor SSP, ISP, and subscapularis strength. Impingement signs were also positive. There were no other joint findings. Radiography did not show bone atrophy or erosion (Figure 2A). T2-weighted MRI revealed an RC tear and remarkable synovial proliferation in the GH joint, subacromial space, bicipital sulcus, and subscapularis bursa (Figure 2B and C). Laboratory tests revealed high levels of inflammatory markers and negative serological markers for RA: CRP was 4.09 mg/dL, RF was <5 U/mL, and ACPA was <0.6 IU/mL. She could not be definitively classified with RA because she scored 4 points on the 2010 ACR/EULAR classification criteria. Therefore, we could not determine whether her synovitis was due to the RC tear or RA. Thus, we planned arthroscopic surgery for the RC tear and pathological examination of the synovium. Shoulder arthroscopy revealed RC tear and remarkable synovial proliferation in the GH joint (Figure 3). This patient had severe synovitis that was disproportionate to that of the RC tears. Gram staining of synovium and synovial fluid in the right shoulder revealed no bacteria and cultures were negative. Pathological examination of the joint synovium revealed infiltration by inflammatory cells, which included plasma cells, with blood vessel proliferation (Figure 4), which is a finding consistent with RA. CRP decreased to 0.38 mg/dL 2 weeks after arthroscopic surgery but increased again 1.05 mg/dL 1 month after surgery. Shoulder joint pain persisted. Therefore, she was classified with RA based on the clinical judgment of a rheumatologist. She was started on MTX therapy. The initial dose of MTX was 6 mg/week. It increased to 10 mg/week a month later. CRP was negative. She achieved remission from RA.
 |
Figure 2 X-ray and magnetic resonance imaging (MRI) findings in Patient 2. At the first visit, X-ray showed no bone erosions (A). Fat-suppressed T2-weighted MRI of the right shoulder (B: axial, C: coronal) showed remarkable synovial proliferation in the glenohumeral joint, subacromial space, intertubercular sulcus, and subscapularis bursa and further effusions in the glenohumeral joint and subacromial space. Supraspinatus, infraspinatus, and subscapularis tendons were torn. There were no bone signals. |
 |
Figure 3 Arthroscopic images in Patient 2 (A: rotator interval, B: middle glenohumeral ligament). There was remarkable synovial proliferation in the glenohumeral joint. Biopsy of the synovium was performed. Supraspinatus, infraspinatus, and subscapularis muscle tendons were torn. She underwent arthroscopic repair of only the subscapularis tendon because the supraspinatus and infraspinatus muscle tendons were severely ruptured and difficult to repair. |
 |
Figure 4 Section of the shoulder joint synovium. (A) shows hematoxylin and eosin (H&E) staining at low magnification (× 40). (B) shows H&E staining at high magnification (× 400). The synovium proliferated in the form of villi. There was infiltration by inflammatory cells, which included plasma cells, with blood vessel proliferation. Findings were consistent with nonspecific synovitis with no bacterial phagocytosis. There were no tumor cells. |
Discussion
RA is an inflammatory disease characterized by symptoms especially in small joints. Older patients more frequently have acute onset in both small and large joints.1,4,6,8–12 A previous report showed that 12.6% of patients with RA have shoulder arthritis at onset with or without arthritis in other joints.13 Shoulder symptoms may be more common in patients aged over 60 years at disease onset, although this remains debated.1,6 Polymyalgia rheumatica is also an important cause of shoulder pain, although it does not cause monoarthritis. In addition, there are several reports of abnormal shoulder findings in patients with RA on imaging studies such as radiography, MRI, and ultrasound.14–16 GH joint abnormalities (Larsen grade 2 or more) are visible on radiographs in 48% of patients 15 years after disease onset.1–3 However, there are no reports of RA presenting with onset from shoulder monoarthritis. In our study, the proportion of patients with shoulder monoarthritis at RA onset was 1.8% (2/113 patients). Both patients were late middle-aged women who did not meet the 2010 ACR/EULAR classification criteria (<6 points). MRI of the shoulder revealed an RC tear and remarkable synovial proliferation. It took approximately 3 months to be classified. There are several studies about the relationship between RA and RC tear; 24–52% of patients aged 50 years or over with RA of the shoulder joint have at least one large RC tear.17,18 RA of the shoulder is characterized by proliferative synovitis (pannus), which is capable of degrading bone and cartilage matrix within and around the joint capsule. It results in cartilage thinning and bone loss as well as soft tissue detachment and destruction.17 RA is common in middle-aged and elderly people. RA has several characteristics in common with RC tear and shoulder periarthritis. In middle-aged patients who have chronic unilateral shoulder pain, shoulder periarthritis and RC tear are more common than RA. Therefore, among our patients with chronic shoulder pain, some might actually have RA but are misdiagnosed with periarthritis or RC tear. It is difficult for us to make a diagnosis of RA in a patient with monoarthritis of the shoulder and it is even more difficult if the patient also has a RC tear.
Based on the 2010 EULAR/ACR classification criteria for RA, patients with synovitis of at least one small joint can be classified as having definite RA if other items are satisfied. However, synovitis of one large joint does not exceed 6 points, so it is difficult to classify them as having define RA. ACR/EULAR state that
Although patients with a score <6/10 are not classifiable as having RA, their status can be reassessed and the criteria might be fulfilled cumulatively over time.7
This classification system is the new proposed paradigm for the entity of RA; of note, this is not a classification system for “early” RA.7 Several reports emphasize that this classification is not intended for early diagnosis of RA.19,20 If patients with monoarthritis, for example, in the shoulder or knee, do not fulfill the criteria, we should make the diagnosis by waiting for other joint symptoms to appear. In order to make an early diagnosis, a detailed evaluation of synovitis using MRI or pathological examination is recommended when RA is suspected.
In Patient 1, CRP was negative at the first visit because her shoulder arthritis was mild. There was a paucity of other information such as pathological and culture examination results. Thus, she was initially treated with prednisolone. If we were able to confirm the diagnosis of RA earlier, we could have started MTX earlier and achieved better control of the disease. In Patient 2, we performed culture-based and pathological examination of the synovium and synovial fluid. Although there were no findings specific for RA, these examinations were useful in ruling out other diseases such as tumors and infections. In order to diagnose a patient with chronic unilateral shoulder pain and synovitis on MRI as having probable RA, it is necessary to rule out some other diseases. For example, we need to rule out shoulder periarthritis, RC tear, osteoarthritis, pseudogout, gout, tumors, non-tuberculous and tuberculous mycobacterial infection, and arthritis associated with other autoimmune diseases.
Arthritis is classified as RA or non-RA based on the 2010 ACR/EULAR classification criteria, but it may be appropriate to diagnose patients who do not fulfill the criteria as having unspecified arthritis.21 Few studies have been performed to characterize seronegative RA in the long term. Paalanen et al investigated the 10-year clinical course of patients with seronegative arthritis. They reported that only 13 (13/435 [3%]) patients could be reclassified as having seropositive or erosive RA. Among the 435 seronegative patients, 4 turned seropositive (2 for ACPA and 2 for RF [>2x reference level]) and 9 developed erosions typical for RA.21 The 2010 ACR/EULAR classification criteria stated:
Much like other classification criteria, clinicians may be able to diagnose an individual who has not met the classification criteria definition or who has features that are not a component of the classification criteria.7
We interpreted the classification broadly in order to start treatment early. We classified patients who do not fulfill the classification as having RA based clinician judgment and treated them with DMARDs. The diagnosis of RA in the two patients presented here was also supported by the ruling out of other diseases and the effectiveness of DMARDs. Patient 1 was seropositive and might have fulfilled the classification criteria if arthritis appeared later in other joints. In contrast, Patient 2 was seronegative, and might be classified as having unspecified arthritis. When the patient has an RC tear with remarkable synovial proliferation, RA must be suspected even if the 2010 ACR/EULAR classification criteria are not fulfilled. Additional examinations such as culture-based and pathology should be performed.
Conclusion
In our study, 1.8% (2/113) of patients had RA onset manifesting as shoulder monoarthritis. It is difficult to classify patients who have symptoms in one large joint, such as shoulder monoarthritis, with RA. If patients have a RC tear, it is more difficult to make a diagnosis of RA. RA should be suspected when MRI shows RC tear with remarkable synovial proliferation. Furthermore, pathological examination (biopsy) may be useful for early diagnosis of RA onset with shoulder monoarthritis.
Ethics Approval and Informed Consent
The protocol of this study was approved by the institutional review board of Tottori University Faculty of Medicine (Reference number 19A089). This study has been conducted in accordance with the Declaration of Helsinki. Informed consent was obtained from Patient 1 and Patient 2 for publication of all data including images. Informed consent was obtained from all individual participants included in the study.
Disclosure
Professor Hideki Nagashima reports grants from Shimizu Hospital, Motomachi Hospital, Misasa Onsen Hospital, Tsuyama Daiichi Hospital, Yowakai, Kaken Pharmaceutical Co., Ltd, Pfizer Japan Inc., MSD, K. K., Shionogi & Co., Ltd., Nippon Zoki Pharmaceutical Co., Ltd., Kawashima Corporation, AbbVie GK, Grants-in-Aid for Scientific Research, personal fees for speaker honorarium from Chugai Pharmaceutical Co., Ltd, Asahi Kasei Pharma Co., Taisho Toyama Pharmaceutical Co. Ltd., Eisai Co., Ltd., Astellas Pharma Inc., Teijin Pharma Ltd., Takeda Pharmaceutical Co., Ltd., Daiichi Sankyo Co., Ltd., Stryker Japan KK, AOSpine, Eli Lilly Japan K. K., Hisamitsu Pharmaceutical Co., Inc., Nippon Sigmax Co. Ltd., Globus Medical Japan, Inc, Becton, Dickinson and Company, NuVasive, Inc., Kyocera Co., and Johnson & Johnson K.K., outside the submitted work. Professor Hiroshi Hagino has received lecture fees or grants outside the submitted work from Amgen Inc., Asahi Kasei Pharma Corp., Astellas Pharma Inc., Chugai Pharmaceutical Co., Ltd., Daiichi Sankyo Co., Ltd., Eisai Co., Ltd., Eli Lilly Japan Co., Ltd., Pfizer Japan Inc., Mitsubishi Tanabe Pharma Corp., Mochida Pharma Co., Ltd, Ono Pharmaceutical Co., Ltd., Pfizer Japan Inc., Taisho Pharmaceutical Co., Ltd., Teijin Pharma Ltd., and UCB Japan Co., Ltd. The authors report no other conflicts of interest in this work.
References
1. Thomas T, Noel E, Goupille P, Duquesnoy B, Combe B. The rheumatoid shoulder: current consensus on diagnosis and treatment. Joint Bone Spine. 2006;73(2):139–143. doi:10.1016/j.jbspin.2005.03.013
2. Lehtinen JT, Kaarela K, Belt EA, Kautiainen HJ, Kauppi MJ, Lehto MU. Incidence of acromioclavicular joint involvement in rheumatoid arthritis: a 15 year endpoint study. J Rheumatol. 1999;26(6):1239–1241.
3. Lehtinen JT, Kaarela K, Belt EA, Kautiainen HJ, Kauppi MJ, Lehto MU. Incidence of glenohumeral joint involvement in seropositive rheumatoid arthritis. A 15 year endpoint study. J Rheumatol. 2000;27(2):347–350.
4. Calvo-Alen J, Corrales A, Sanchez-Andrada S, Fernandez-Echevarria MA, Pena JL, Rodriguez-Valverde V. Outcome of late-onset rheumatoid arthritis. Clin Rheumatol. 2005;24(5):485–489. doi:10.1007/s10067-004-1067-4
5. Rexhepi S, Rexhepi M, Sahatçiu-Meka V, Rexhepi B, Bahtiri E, Mahmutaj V. Late onset rheumatoid arthritis an observational study. Reumatizam. 2016;63(1):1–5.
6. El-Labban AS, Omar HA, El-Shereif RR, Ali F, El-Mansoury TM. Pattern of Young and Old Onset Rheumatoid Arthritis (YORA and EORA) among a group of Egyptian patients with rheumatoid arthritis. Clin Med Insights Arthritis Musculoskelet Disord. 2010;3:25–31. doi:10.4137/CMAMD.S4935
7. Aletaha D, Neogi T, Silman AJ, et al. 2010 rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Arthritis Rheum. 2010;62(9):2569–2581. doi:10.1002/art.27584
8. van der Heijde DM, van Riel PL, van Leeuwen MA, van ‘T Hof MA, van Rijswijk MH, van de Putte LB. Older versus younger onset rheumatoid arthritis: results at onset and after 2 years of a prospective follow up study of early rheumatoid arthritis. J Rheumatol. 1991;18(9):1285–1289.
9. Turkcapar N, Demir O, Atli T, et al. Late onset rheumatoid arthritis: clinical and laboratory comparisons with younger onset patients. Arch Gerontol Geriatr. 2006;42(2):225–231. doi:10.1016/j.archger.2005.07.003
10. Lance NJ, Curran JJ. Late-onset, seropositive, erosive rheumatoid arthritis. Semin Arthritis Rheum. 1993;23(3):177–182. doi:10.1016/S0049-0172(05)80038-1
11. Pease CT, Haugeberg G, Morgan AW, Montague B, Hensor EM, Bhakta BB. Diagnosing late onset rheumatoid arthritis, polymyalgia rheumatica, and temporal arteritis in patients presenting with polymyalgic symptoms. A prospective long term evaluation. J Rheumatol. 2005;32(6):1043–1046.
12. Ruta S, Rosa J, Navarta DA, et al. Ultrasound assessment of new onset bilateral painful shoulder in patients with polymyalgia rheumatica and rheumatoid arthritis. Clin Rheumatol. 2012;31(9):1383–1387. doi:10.1007/s10067-012-2016-2
13. Nishiyama S, Aita T, Yoshinaga Y, et al. A study of fhe first site of joint involvement and clinical manifestations in patients with rheumatoid arthritis (RA). Clin Rheumatol. 2010;22(3):326–330.
14. Hermann KG, Backhaus M, Schneider U, et al. Rheumatoid arthritis of the shoulder joint: comparison of conventional radiography, ultrasound, and dynamic contrast-enhanced magnetic resonance imaging. Arthritis Rheum. 2003;48(12):3338–3349. doi:10.1002/art.11349
15. Kanbe K, Chiba J, Inoue Y, Taguchi M, Iwamatsu A. Analysis of clinical factors related to the efficacy of shoulder arthroscopic synovectomy plus capsular release in patients with rheumatoid arthritis. Eur J Orthop Surg Traumatol. 2015;25(3):451–455. doi:10.1007/s00590-014-1570-5
16. Stegbauer J, Rump LC, Weiner SM. Sites of inflammation in painful rheumatoid shoulder assessed by musculoskeletal ultrasound and power Doppler sonography. Rheumatol Int. 2008;28(5):459–465. doi:10.1007/s00296-007-0465-8
17. van de Sande MA, de Groot JH, Rozing PM. Clinical implications of rotator cuff degeneration in the rheumatic shoulder. Arthritis Rheum. 2008;59(3):317–324. doi:10.1002/art.23330
18. Rozing PM, Brand R. Rotator cuff repair during shoulder arthroplasty in rheumatoid arthritis. J Arthroplasty. 1998;13(3):311–319. doi:10.1016/S0883-5403(98)90177-2
19. Schneider M, Kruger K. Rheumatoid arthritis–early diagnosis and disease management. Dtsch Arztebl Int. 2013;110(27–28):477–484. doi:10.3238/arztebl.2013.0477
20. Mjaavatten MD, Bykerk VP. Early rheumatoid arthritis: the performance of the 2010 ACR/EULAR criteria for diagnosing RA. Best Pract Res Clin Rheumatol. 2013;27(4):451–466. doi:10.1016/j.berh.2013.09.001
21. Paalanen K, Rannio K, Rannio T, Asikainen J, Hannonen P, Sokka T. Does early seronegative arthritis develop into rheumatoid arthritis? A 10-year observational study. Clin Exp Rheumatol. 2019;37(1):37–43.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.