Back to Journals » Journal of Inflammation Research » Volume 19
Rewiring the Lung–CNS Axis After Spinal Cord Injury
Authors Wu H ![]() , Li X, Zhao W
, Li X, Zhao W ![]() , Li Y, Zhang H, Yin H, Gu X
, Li Y, Zhang H, Yin H, Gu X
Received 23 May 2025
Accepted for publication 6 November 2025
Published 8 January 2026 Volume 2026:19 542308
DOI https://doi.org/10.2147/JIR.S542308
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Cynthia Koziol-White
HaiRong Wu,1 Xiaolong Li,1 Wenjun Zhao,1 Yihan Li,1 Hang Zhang,1 Heng Yin,1,2 Xiaofeng Gu3
1Wuxi Affiliated Hospital of Nanjing University of Chinese Medicine., Wuxi, 214071, People’s Republic of China; 2Jiangsu CM Clinical Innovation Center of Degenerative Bone & Joint Disease, Wuxi, 210046, People’s Republic of China; 3Department of Orthopedics, The Affiliated Wuxi People’s Hospital of Nanjing Medical University, Wuxi, 214023, People’s Republic of China
Correspondence: Xiaofeng Gu, Email [email protected]
Abstract: Spinal cord injury (SCI) is a catastrophic disorder of the central nervous system, most commonly resulting from traumatic events such as motor vehicle collisions or falls, but it can also arise from non-traumatic causes including neoplastic, infectious, or degenerative diseases. Respiratory complications are among the most frequent and life-threatening sequelae of SCI. In the acute phase, up to 80% of patients experience respiratory dysfunction, including pneumonia, atelectasis, and respiratory failure. These issues are particularly pronounced in individuals with high cervical injuries, where diaphragmatic and intercostal muscle paralysis impairs effective ventilation and clearance of secretions, substantially increasing the risk of infection. Emerging evidence underscores the bidirectional interplay between pulmonary pathology and central nervous system injury. SCI-induced autonomic dysfunction alters immune regulation, heightening susceptibility to pulmonary infections. Conversely, pulmonary complications can amplify systemic inflammatory responses, which may exacerbate neurological deterioration. Understanding the complex interactions between respiratory complications and SCI pathophysiology is essential for improving patient outcomes. This review therefore focuses on elucidating the mechanisms of pulmonary complications post-SCI and exploring therapeutic strategies to mitigate their impact on neurological recovery.
Keywords: spinal cord injury, neuroimmune interaction, pulmonary microenvironment, lung–CNS axis
Introduction
Spinal cord injury (SCI) is a devastating neurological condition that can result from traumatic events—such as traffic accidents or falls—or non-traumatic causes, including vascular malformations, tumors, infections, transverse myelitis, and syringomyelia.1,2 Although traumatic SCI (tSCI) accounts for the majority of cases, non-traumatic SCI (ntSCI) also constitutes a significant proportion, particularly among elderly populations.3 According to the Global Burden of Disease Study 2019, the annual incidence of SCI is estimated at 900,000 [95% uncertainty interval (UI), 700,000 to 1200,000] cases worldwide, with a global prevalence reaching 20.6 million (95% UI: 18.9–23.6 million).4 Due to its high burden of disability, SCI is currently the sixth leading neurological cause of disability worldwide and ranks seventh in Asia, severely impacting quality of life and imposing substantial socioeconomic costs.5
Beyond motor impairment, SCI frequently leads to multi-organ complications involving neurological, cardiovascular, urological, gastrointestinal, and particularly respiratory systems.6,7 Respiratory complications—such as pneumonia, atelectasis, and respiratory failure—remain leading contributors to morbidity and mortality, especially in individuals with cervical and upper thoracic SCI.6,8 Reports indicate that these complications occur in 40–80% of SCI patients, underscoring their clinical importance.9,10
Recent research has increasingly focused on the lung-brain axis, highlighting bidirectional interactions between the pulmonary microenvironment and the central nervous system (CNS).11,12 After SCI, disruptions in respiratory muscle function and autonomic regulation not only predispose patients to infections and inadequate ventilation but also profoundly alter immune homeostasis, vascular permeability, and local inflammatory responses within the lung.13 In turn, pulmonary complications may exacerbate systemic inflammation and immune dysregulation, worsening neurological damage and impeding repair processes.14,15 Mechanistic studies have identified neural reflex circuits, circulating cytokines, extracellular vesicles, and the pulmonary microbiome as crucial mediators in this intricate interplay.16–19
Despite advances in acute respiratory care, current interventions mainly rely on mechanical ventilation and infection management, with limited strategies directly targeting modulation of the pulmonary microenvironment.20,21 Growing evidence suggests that optimizing lung health is critical not only for preventing respiratory failure but also for facilitating neurological recovery following SCI.14,15,22 This review synthesizes current understanding of pulmonary microenvironment remodeling after SCI, elucidates its regulatory role in CNS repair, and explores emerging therapeutic approaches. By advancing our understanding of the lung-CNS axis, this review aims to guide the development of integrated clinical strategies to enhance pulmonary and neurological outcomes in SCI patients.
Survey Methodology
Literature searches were conducted in the PubMed, Web of Science, and Embase databases. In addition to articles published since 2015, earlier seminal studies were also considered. The keywords used were as follows: spinal cord injury, respiratory complications, pneumonia, atelectasis, respiratory failure, pulmonary embolism, sleep-disordered breathing, lung–CNS axis, lung–brain axis, neuroimmune interaction, vagus nerve stimulation, respiratory muscle training, diaphragm pacing, extracellular vesicles, and pulmonary microbiota. As our work gradually unfolded, we then searched literature by combined keywords such as spinal cord injury and pneumonia, spinal cord injury and respiratory muscle training, lung–CNS axis and neuroinflammation, vagus nerve stimulation and spinal cord injury, extracellular vesicles and lung injury, microbiota and spinal cord injury. After removing duplicate and irrelevant records, 186 articles were finally selected for this review.
Spinal Cord Injury and Respiratory Complications
Respiratory Complications
Respiratory complications are among the most critical challenges in SCI and are strongly influenced by injury level and severity.23 Patients may develop respiratory muscle weakness, diaphragmatic dysfunction, impaired ventilation, secretion retention, and recurrent infections, substantially increasing the risk of pneumonia, respiratory failure, and chronic pulmonary dysfunction24 (Table 1).8,9,25–41 Incidence rates reach 40–70% in cervical or upper thoracic SCI42 and are higher in complete versus incomplete injuries.43,44 According to the ASIA scale, grade A lesions carry the greatest risk.29,45 These complications peak within the first year but may persist long-term, leading to acute decompensation and impaired quality of life.46,47
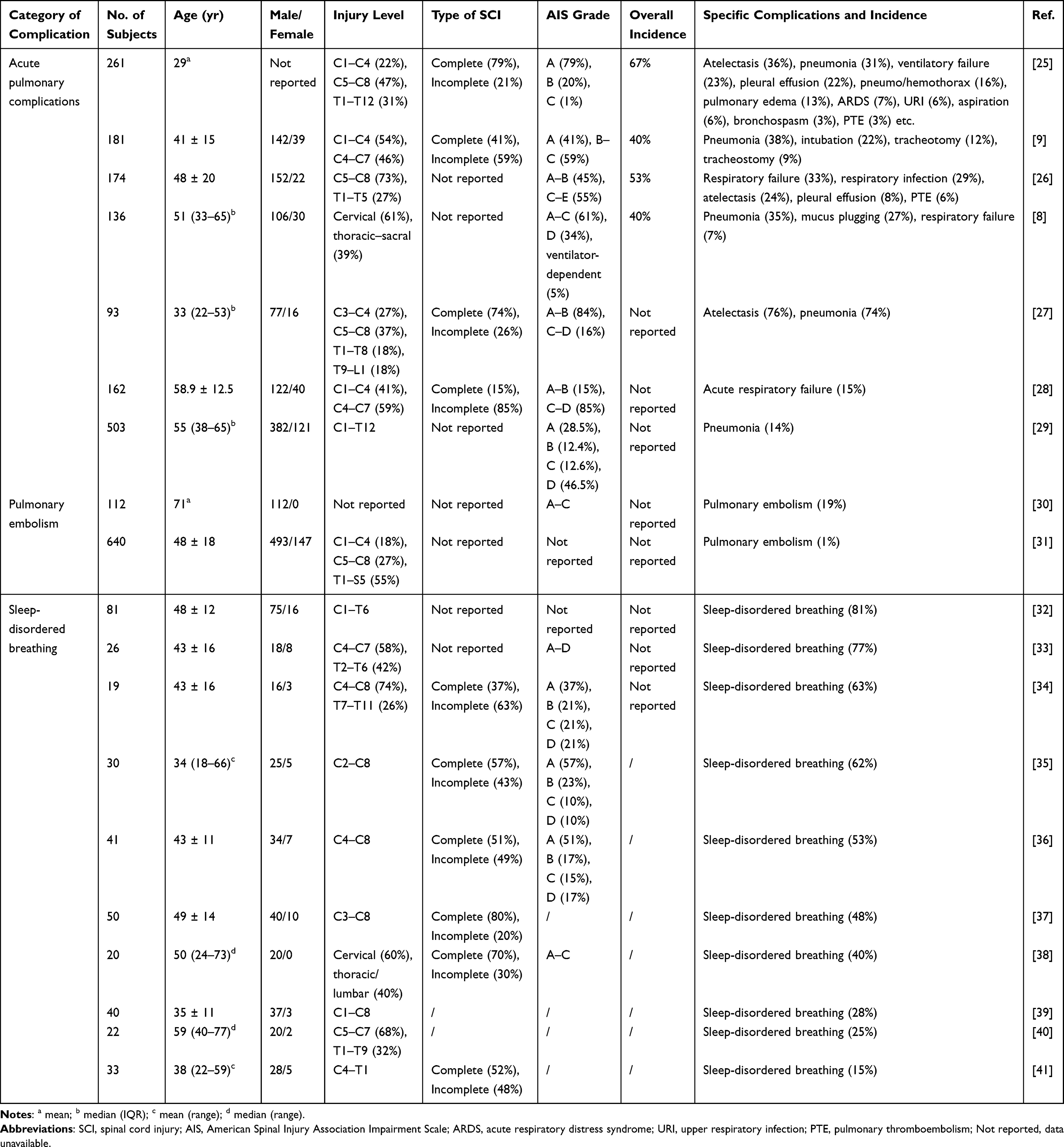 |
Table 1 Incidence and Spectrum of Respiratory Complications After Spinal Cord Injury Across Representative Cohorts |
Respiratory Failure
Respiratory failure is a major cause of morbidity and mortality, particularly in cervical or high thoracic SCI.26,48 It reflects inadequate gas exchange with hypoxemia and/or hypercapnia,49 and is classified as type I (V/Q mismatch, eg, pneumonia or edema)50 or type II (reduced ventilation, eg, muscle fatigue),45,51 and injuries at C3 or higher usually abolish spontaneous breathing, necessitating continuous mechanical ventilatory support. Lesions above C5 often cause diaphragmatic paralysis.10
Pneumonia
Pneumonia is a leading cause of death after SCI,52 with mortality risk markedly increased in the first year.53 Its incidence is highest in cervical and upper thoracic injuries,54 largely due to impaired cough and mucociliary clearance.55,56 These deficits promote secretion retention, bacterial colonization, and infection. Beyond mortality, pneumonia prolongs hospitalization and increases healthcare costs.49
Atelectasis
Atelectasis occurs in up to 36% of acute SCI,10 driven by impaired inspiration, weak cough, and secretion retention.23,57 Its severity correlates with neurological level, with vital capacity (VC) decreasing by 20–50% in high cervical injuries49 and by 30–50% in C5–C6 lesions.10,49,58 Chronic SCI is further complicated by chest-wall stiffness, abdominal muscle laxity, and spasticity, contributing to persistent ventilatory impairment.20 Longitudinal studies confirm progressive declines in FEV1, reductions in functional residual capacity, and stabilization of VC at ~60% of predicted values.49,59
Pulmonary Embolism
PE is the second leading cause of death within the first year after SCI,60 with an incidence of ~4.5% and mortality of ~3.5%.31 Risk factors include immobility, impaired venous return, hypercoagulability, and autonomic dysfunction.61,62 Prophylactic anticoagulation and close monitoring are therefore essential.
Pulmonary Edema
Pulmonary edema is underrecognized in SCI and arises from venous congestion, immobility, and autonomic dysregulation.23,63,64 Case reports illustrate its association with autonomic dysreflexia and acute permeability edema.65 Experimental data suggest VEGF upregulation after SCI enhances vascular permeability and fluid leakage.66
Sleep-Disordered Breathing
OSA develops in 64–83% of tetraplegic patients within months of injury.67 Mechanisms include reduced ventilatory drive, diaphragmatic overload during REM sleep, and upper airway instability.68,69 Clinical features range from nocturnal awakenings and night sweats to excessive daytime sleepiness and impaired cognition. Daytime PaO2 <45 mmHg or base excess <4 mEq indicates nocturnal hypoventilation.70
Mechanisms of Respiratory Complications
Respiratory complications following SCI arise from complex interactions among multiple pathophysiological mechanisms (Figure 1). At their core lies respiratory muscle dysfunction due to disrupted neural pathways controlling the diaphragm, intercostal, and accessory muscles, resulting in impaired ventilation and ineffective airway clearance.23,49 Autonomic dysfunction further exacerbates respiratory impairment by altering bronchial muscle tone, mucociliary clearance, and vascular permeability.23,71 Concurrently, immune dysregulation—characterized by impaired innate and adaptive immune responses—increases susceptibility to pulmonary infections.14 Additionally, disruptions in circulatory regulation, including venous congestion and altered pulmonary blood flow, lead to ventilation-perfusion mismatch and elevate risks for pulmonary edema and embolism.23,71 Collectively, these interrelated mechanisms highlight the multifaceted nature of respiratory disorders following SCI.
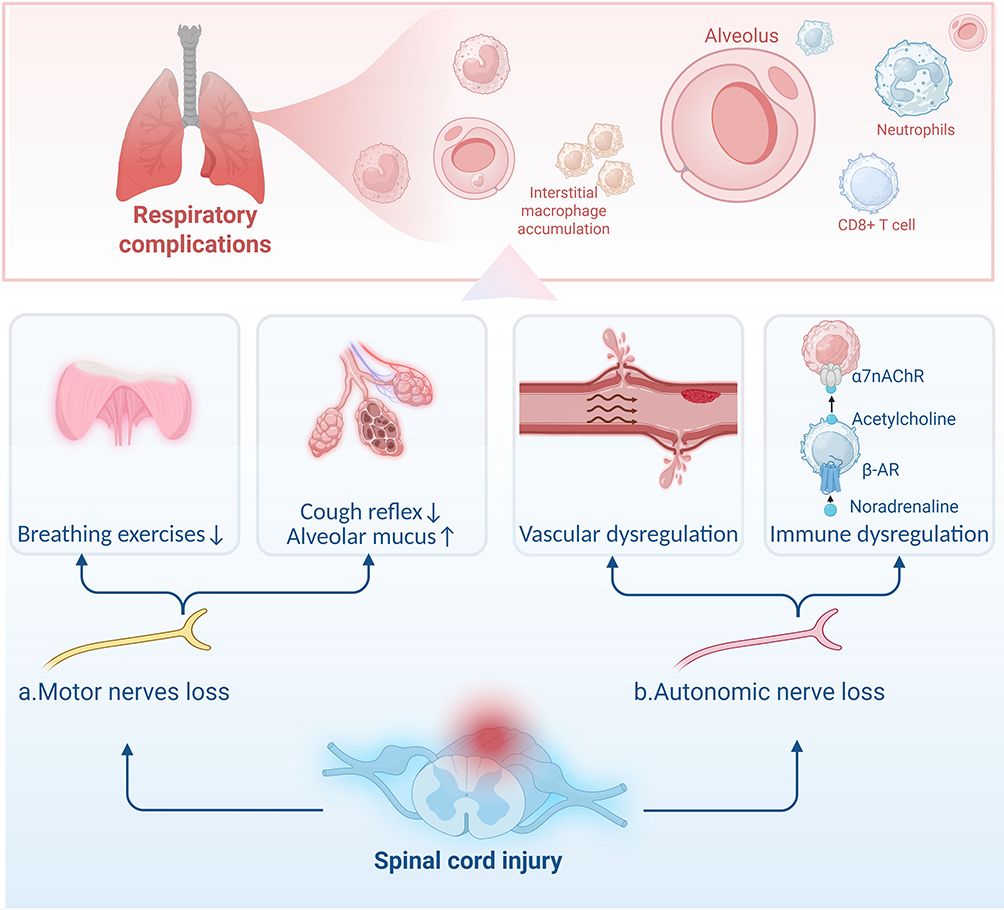 |
Figure 1 Pathophysiological Mechanisms Linking SCI to Pulmonary Complications. SCI can induce a pulmonary inflammatory response, characterized by the accumulation of interstitial macrophages and the infiltration of immune cells, including neutrophils and CD8+ T cells. Concurrently, SCI leads to (a) motor nerve loss, which subsequently causes reduced respiratory effort and an impaired cough reflex combined with increased alveolar mucus. (b) Autonomic nerve loss, also induced by SCI, leads to vascular dysregulation and immune dysregulation, involving α7 nicotinic acetylcholine receptor (α7 nAChR) and β-adrenergic receptor (β-AR) signaling pathways. |
Motor Nerves Loss
Respiratory muscle dysfunction is a significant complication following SCI, primarily caused by paralysis associated with spinal shock below the level of injury.23 The diaphragm, innervated by the phrenic nerve originating from spinal segments C3–C5, is the primary inspiratory muscle and contributes approximately 65% of tidal volume. Intercostal muscles, essential for efficient breathing, are innervated by segments T1–T11, while abdominal muscles, critical for effective expiration and coughing, are innervated by T6–L1.72,73 SCI at levels C1–C3 typically results in complete diaphragmatic paralysis, rendering patients fully dependent on mechanical ventilation.74 Injuries at C4–C5 levels usually cause partial diaphragmatic dysfunction, significantly reducing vital capacity to approximately 20–50% of predicted values.49 Patients with lower cervical injuries (C6–C8) generally retain diaphragm function but experience paralysis of intercostal and abdominal muscles, often presenting with paradoxical breathing, characterized by inward chest wall movement during inspiration due to rib cage instability.59 Thoracic-level SCI (T1–L1) patients typically exhibit impaired respiratory function secondary to compromised innervation of intercostal and abdominal muscles.
Mechanical respiratory dysfunction after SCI involves paradoxical breathing patterns and reduced chest wall compliance, promoting distal airway collapse and micro-atelectasis.23,55 Inspiratory muscle weakness limits deep breathing, resulting in impaired gas exchange, reduced lung compliance, and atelectasis.23,75 Similarly, expiratory muscle weakness reduces coughing effectiveness, exacerbating mucus retention and persistent airway obstruction.76,77 Consequently, mucus accumulation within airways creates a favorable environment for bacterial colonization, increasing susceptibility to respiratory infections such as pneumonia.53
Autonomic Dysfunction
In addition to motor innervation of respiratory muscles, integrity of the autonomic nervous system (ANS) is critical for maintaining respiratory function and airway protection after SCI. The ANS comprises sympathetic and parasympathetic branches, each with distinct anatomical origins and functional roles. Sympathetic preganglionic neurons originate from the intermediolateral cell column of spinal segments T1 to L2/L3 and synapse with postganglionic neurons in paravertebral ganglia.62 In contrast, parasympathetic neurons primarily arise from the brainstem (cranial nerves III, VII, IX, and particularly X—the vagus nerve), as well as sacral spinal segments S2–S4. Notably, parasympathetic innervation from the vagus nerve significantly influences pulmonary function by regulating bronchial smooth muscle tone and mucus secretion.78 Disruption of ANS control after SCI leads to profound autonomic imbalance, manifesting clinically as vasodilation, bradycardia, and systemic hypotension—a condition collectively termed neurogenic shock.79 The resultant hypotension reduces perfusion to vital organs, including the lungs, compromising tissue oxygenation and metabolism. Concurrent respiratory muscle paralysis further diminishes venous return and cardiac output, exacerbating systemic hypoperfusion.79 Enhanced functional connectivity between the nucleus tractus solitarius and the rostral ventrolateral medulla following SCI may potentiate sympathetic activation, increasing pulmonary vascular permeability.80 Moreover, the loss of sympathetic vasomotor control results in persistent hypotension, complicating fluid management in approximately 50% of acute tetraplegic patients and increasing pulmonary edema risk.81
In acute cervical and high thoracic SCI, disruption of sympathetic output (originating from segments T1–L2) severely shifts autonomic balance.62 Loss of sympathetic control results in unopposed parasympathetic (vagal) activity, markedly elevating airway resistance through bronchoconstriction and excessive mucus production.82 Such autonomic imbalance leads to airway obstruction, impaired gas exchange, hypoxemia, and hypercapnia, frequently necessitating tracheal intubation for ventilation support and mucus clearance during acute management.83
Additionally, patients with SCI at or above the T6 level may experience episodes of autonomic dysreflexia (AD), characterized by exaggerated sympathetic responses triggered by noxious stimuli below the injury level (eg, bladder distension or constipation). During AD episodes, massive catecholamine release—including norepinephrine and epinephrine—can precipitate acute severe hypertension, with systolic pressures often surpassing 200 mmHg.84 These hypertensive crises may induce permeability pulmonary edema, severely compromising respiratory function and exacerbating respiratory distress. Sympathetic activation during AD also causes pulmonary venous constriction, further elevating pulmonary capillary pressure. Elevated capillary pressure and endothelial shear stress disrupt endothelial tight junctions, increasing vascular permeability and facilitating protein-rich fluid leakage into alveolar spaces.85 Furthermore, excessive catecholamine release activates the NF-κB signaling pathway in alveolar macrophages, stimulating pro-inflammatory cytokines such as TNF-α and IL-6. These cytokines upregulate intercellular adhesion molecule-1 (ICAM-1) expression on endothelial cells, promoting leukocyte adhesion, infiltration, and subsequent protease release, further impairing pulmonary vascular integrity.86 Moreover, increased pulmonary capillary hydrostatic pressure mechanically stretches endothelial cells, activating mechanosensitive ion channels such as TRPV4. This mechanical stress induces cytoskeletal rearrangements in endothelial cells, while aquaporin-1 (AQP1) channel dysfunction further aggravates fluid leakage into alveoli.87 Collectively, these mechanisms lead to severe, permeability-driven pulmonary edema, characterized by marked proteinaceous exudation.
Thus, autonomic dysfunction after SCI significantly contributes to respiratory complications via multiple mechanisms, including altered airway physiology, excessive mucus secretion, and severe vascular responses.
Immune Dysfunction
Immune dysfunction is a prominent yet frequently overlooked consequence of SCI. Several mechanisms contribute to impaired immune responses, including disruptions in sympathetic and vagal cholinergic pathways innervating lymphoid organs and dysregulation of the hypothalamic-pituitary-adrenal (HPA) axis.88,89 Collectively, these alterations significantly increase susceptibility to infections.
SCI-induced dysregulation of the HPA axis results in abnormal cortisol secretion.90 Elevated cortisol levels suppress immune cell function, notably reducing the activity of critical immune effector cells such as T lymphocytes and natural killer (NK) cells.91 Additionally, SCI is associated with early impairment of hematopoiesis, leading to bone marrow dysfunction and diminished immune cell production, further compromising host defenses.88 The vagus nerve plays a crucial role in regulating pulmonary inflammation via the cholinergic anti-inflammatory pathway (CAP). Efferent vagal fibers release acetylcholine (ACh), inhibiting nuclear factor κB (NF-κB) activation in alveolar macrophages, thereby reducing pro-inflammatory cytokine (eg, TNF-α, IL-6) production by up to 40%.92–94 Proper vagal stimulation facilitates resolution of inflammation, whereas vagotomy or deficiency of α7-nicotinic acetylcholine receptors (α7nAChR) exacerbates pulmonary infection, inflammation, tissue injury, and systemic cytokine release.95 Thus, either excessive or inadequate vagal responses following SCI can worsen pulmonary infections or chronic inflammatory lung conditions.92 Specifically, vagal efferent fibers release ACh, which suppresses NF-κB signaling via α7nAChR, effectively reducing the secretion of pro-inflammatory mediators such as TNF-α.93
Following SCI, sympathetic innervation to lymphoid organs, particularly the spleen, is disrupted. This disruption results in splenic atrophy and impaired lymphocyte function, thereby diminishing the host’s capacity to mount effective immune responses.96,97 Moreover, norepinephrine (NE), a key neurotransmitter of the sympathetic nervous system (SNS), significantly modulates immune responses in the context of SCI. Elevated NE levels inhibit maturation and activation of type 1 helper T cells (Th1), suppressing immune reactivity and increasing vulnerability to infections.89,98 Experimental evidence indicates that excessive SNS activation—characterized by increased catecholamine release—reduces TNF-α production and increases interleukin-10 (IL-10) via β-adrenergic receptors on immune cells.99 Conversely, blockade of β-adrenergic receptors can mitigate infection risks, including pneumonia.99,100
Intervention Strategies
Mechanical Ventilation and Tracheostomy
Patients with complete cervical SCI at or above the C3 level frequently require long-term mechanical ventilation support.101 In the acute phase, tracheostomy reduces airway resistance, lowers aspiration risk, and facilitates mucus clearance.102 However, prolonged use of tracheostomy tubes may lead to speech difficulties, swallowing impairments, increased infection risk, and diminished quality of life.103 For patients with high-level SCI (particularly cervical injuries), respiratory dysfunction can be severe enough to necessitate mechanical ventilation.104,105 Intubation and mechanical ventilation are critical for patients with complete cervical SCI above the C5 level, who experience diaphragmatic paralysis and require ventilatory support.102,104 Early tracheostomy is generally recommended, as it reduces mechanical ventilation duration, shortens ICU stays, and enhances patient comfort and tolerance.106 Early tracheostomy has also been associated with lower mortality and reduced respiratory complications in severe cervical SCI.74,104
Respiratory Muscle Training (RMT)
Respiratory muscle training (RMT) represents an active rehabilitation strategy aimed at improving inspiratory and expiratory muscle strength in individuals with SCI. Unlike passive interventions such as mechanical ventilation, RMT seeks to restore voluntary respiratory capacity by targeting diaphragmatic, intercostal, and accessory respiratory muscles.
Several randomized controlled trials and systematic reviews have demonstrated that inspiratory muscle training (IMT) significantly enhances maximal inspiratory pressure (MIP), vital capacity (VC), and forced expiratory volume in one second (FEV1) in both acute and chronic SCI patients.107,108 Similarly, expiratory muscle training (EMT) improves maximal expiratory pressure (MEP) and cough efficiency, thereby facilitating airway clearance and reducing the risk of atelectasis and recurrent pneumonia.109 When combined with mechanically assisted coughing techniques, RMT further augments mucus clearance and decreases pulmonary infection rates.110
The clinical benefits of RMT extend beyond pulmonary mechanics. By enhancing respiratory strength and endurance, RMT contributes to earlier weaning from mechanical ventilation, shortens intensive care unit stays, and improves long-term quality of life.111–113 In chronic SCI, regular RMT also alleviates sleep-disordered breathing and enhances exercise tolerance, underscoring its role in long-term rehabilitation.107,108,114
Despite these promising findings, RMT remains underutilized in clinical practice. Variability in training protocols, duration, and intensity across studies limits standardization and widespread adoption. Future work should focus on defining optimal RMT regimens and integrating them with multimodal respiratory care frameworks to maximize clinical outcomes in SCI patients.
Non-Invasive Ventilation (NIV)
Non-invasive ventilation (NIV) delivers positive-pressure ventilation via interfaces such as mouthpieces, nasal masks, or oronasal masks, and is suitable for conscious patients who maintain spontaneous breathing.115 Studies indicate that NIV serves as a viable alternative to long-term invasive ventilation, reducing the need for tracheostomy, lowering infection risks, and enhancing speech and swallowing functions.116,117 Intermittent positive-pressure breathing (IPPB), delivered through mouthpieces, masks, or tracheostomy connectors, helps increase inspiratory volume before assisted coughing, preventing atelectasis and improving ventilation.118 Furthermore, combining NIV with mechanically assisted coughing techniques, such as mechanical insufflation-exsufflation, effectively clears airway secretions and reduces pneumonia risk.119,120 Although tracheostomy remains common in patients requiring long-term ventilatory support, various non-invasive approaches—including mouthpiece and mask ventilation—offer effective alternatives.121
Diaphragm Pacing Systems (DPS)
Patients with high cervical SCI may be candidates for diaphragm pacing systems (DPS).122 In individuals with preserved phrenic nerve function, DPS provides an alternative ventilatory strategy by electrically stimulating the phrenic nerves to induce diaphragmatic contractions, facilitating autonomous breathing.123 Early DPS implantation significantly improves the likelihood of weaning from mechanical ventilation and enhances respiratory mechanics and quality of life.124 However, long-term outcomes and precise indications for DPS still require further research.124 DPS can be implemented through direct intrathoracic phrenic nerve pacing (traditional approach) or via laparoscopic insertion of electrodes at the diaphragm’s insertion points of the phrenic nerve.125 In carefully selected patients with restored diaphragm function, tidal volumes can increase sufficiently to allow tracheostomy removal.126 Nevertheless, current evidence regarding long-term DPS efficacy in SCI patients remains limited.
Assisted Breathing Techniques
During the acute phase of SCI, employing abdominal binders or adjusting body positioning (eg, supine position) can enhance diaphragm function and increase vital capacity, especially following acute high cervical injury.127 For patients with lower cervical or thoracic SCI, NIV combined with assisted coughing methods (such as the quad-cough technique) effectively improves respiratory function.128 The use of abdominal binders and supine positioning optimizes diaphragmatic mechanics, increasing lung volumes in patients immediately following SCI.127,129 Similarly, in lower cervical and thoracic injuries, integrating NIV and assisted coughing techniques significantly benefits respiratory management.23,128
Respiratory Complications and CNS Interactions
Emerging research has revealed an important and intricate bidirectional communication network between the lungs and the CNS.130 Strong evidence indicates that pulmonary injury can trigger neuroinflammation, which in turn worsens neurological function.131,132 For instance, acute lung injury (ALI) and acute respiratory distress syndrome (ARDS) are closely associated with cognitive impairment in survivors, suggesting lung dysfunction significantly affects CNS function.131–133 The biological basis of this lung–CNS interaction primarily involves three mechanisms: neural signaling pathways, inflammatory mediators, and microbial factors.130,133 Recent studies further highlight extracellular vesicles, including exosomes, as potential mediators that drive neuroinflammation following pulmonary injury.134,135 (Figure 2).
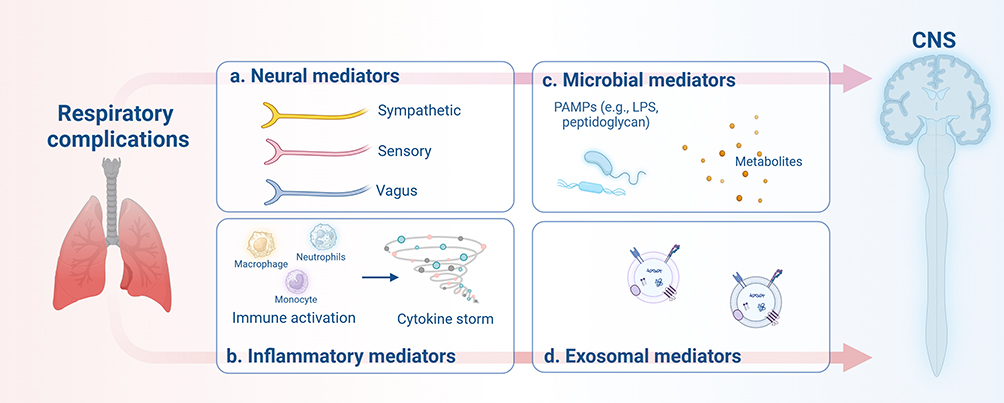 |
Figure 2 Multimodal lung-to-CNS signalling after respiratory complications. Pulmonary injury induces four principal classes of mediators that interact with the central nervous system: (a) Neural—sympathetic efferents, vagal afferent/efferent fibres, and spinal pulmonary afferents; (b) Inflammatory—systemic cytokines released by activated macrophages, neutrophils, and monocytes; (c) Microbial—pathogen-associated molecular patterns (eg, LPS, peptidoglycan) and bacterial metabolites; (d) Exosomal—extracellular vesicles conveying nucleic acids and proteins. These mediators act in parallel rather than sequentially, collectively contributing to neuroinflammation and secondary neurological damage. |
Neural Pathways
The vagus nerve (the tenth cranial nerve), composed of approximately 80% afferent and 20% efferent fibers, constitutes the primary neural pathway of the lung-brain axis.130 Recent findings suggest that pulmonary vagal afferent fibers transmit signals from the pulmonary microenvironment to the nucleus tractus solitarius (NTS) in the medulla, subsequently activating serotonin (5-HT) neurons in the dorsal raphe nucleus (DRN) of the midbrain.136,137 Sensory nerve terminals of vagal afferents are widely distributed in alveoli and bronchial epithelium, transmitting peripheral signals via the nodose ganglion to the NTS, which forms synaptic connections with brainstem nuclei, including the DRN.138 Experimental data have demonstrated that intravenously administered mesenchymal stem cells (MSCs) primarily localize to the lungs, where they activate VGLUT2-positive vagal afferent fibers.137 This activation induces increased c-Fos expression in the NTS and subsequently activates serotonergic neurons in the DRN, significantly improving depressive-like behaviors. Lung injury similarly activates pulmonary sensory receptors (eg, stretch and chemoreceptors), which transmit signals via vagal afferents to the brainstem.136,139 For example, ALI triggers vagus nerve-mediated activation of the hypothalamic-pituitary-adrenal (HPA) axis, thereby amplifying systemic inflammation.139
Additionally, sensory nerves from the lungs directly communicate with the brain, akin to nociceptive signaling.140 Such direct neural communication allows rapid CNS detection of pulmonary infections, triggering sickness behaviors such as fatigue and anorexia.141 This pathway might explain why severe lung injuries can occur with minimal subjective symptoms, potentially due to bacterial biofilms evading immune detection.142
Immune Pathways
Pulmonary disorders such as acute lung injury (ALI) and acute respiratory distress syndrome (ARDS) cause extensive release of inflammatory cytokines (eg, TNF-α, IL-1β, IL-6).143,144 Lung inflammation facilitates the entry of cytokines into systemic circulation. Persistent systemic inflammation can downregulate tight junction proteins (such as Claudin-5 and ZO-1) in blood-brain barrier (BBB) endothelial cells, enhancing BBB permeability.131,145 Increased permeability enables inflammatory cytokines to infiltrate brain parenchyma, leading to neuroinflammation and cognitive dysfunction.19 Animal studies show that lipopolysaccharide (LPS)-induced ALI causes a threefold increase in microglial activation in the hippocampus, accompanied by a 50% decline in spatial memory performance. The strong association between ALI/ARDS, neuroinflammation, and cognitive dysfunction in survivors provides new avenues for targeted neuromodulatory therapies addressing neuropsychiatric complications following spinal cord injury.131,146
Lung Flora
Emerging evidence highlights a critical role of the lung microbiota in regulating CNS health, analogous to the well-established gut-brain axis.147 For example, mouse infection with Bordetella pertussis is associated with inflammation and β-amyloid deposition, whereas colonization by Klebsiella pneumoniae correlates with increased Alzheimer’s disease risk. In healthy individuals, the lung microbiota predominantly comprises Firmicutes (38%), Bacteroidetes (29%), and Proteobacteria (18%).148 Following SCI, conditions such as neurogenic pulmonary edema and ventilator-associated pneumonia facilitate colonization by Gram-negative bacteria.149 Lipopolysaccharide (LPS) released by these bacteria may enter the CNS through a compromised blood-spinal cord barrier, triggering neuroinflammation via Toll-like receptor 4 (TLR4) signaling pathways and serving as a direct mediator of lung-brain communication.150,151 Interestingly, experimental autoimmune encephalomyelitis (EAE) models demonstrated that antibiotic-induced lung microbiome dysbiosis (eg, via neomycin) reduced CNS T-cell infiltration by approximately 70% and downregulated MHC-II expression on microglia by about 50%. This immunomodulatory effect was mediated by LPS from Prevotella species, activating type I interferon responses via TLR4 in microglia, consequently suppressing pro-inflammatory cytokine production.151,152 Similarly, respiratory infections with aerosolized Bordetella pertussis alleviated EAE severity through IL-10-mediated regulatory T-cell responses and downregulation of VLA-4 and LFA-1 on CD4⁺ T cells.153,154
Metabolites from lung microbiota also contribute to lung-brain interactions.155 Short-chain fatty acids (SCFAs) produced by pulmonary bacteria can cross the blood-brain barrier via monocarboxylate transporters.155 For example, systemic propionate administration increased brain-derived neurotrophic factor (BDNF) expression by 30% in the prefrontal cortex, improving cognitive performance.156 Conversely, kynurenine—a tryptophan metabolite generated by lung macrophage indoleamine 2,3-dioxygenase-1 (IDO1)—is linked to depressive behaviors due to elevated CNS levels.157–159
Pulmonary microbiota dysbiosis may also predispose the CNS to direct infections. Cryptococcus neoformans, an inhaled fungal pathogen, initially causes pneumonia and subsequently disseminates to the CNS, resulting in meningoencephalitis. This pathogen accesses the CNS via transmigration of infected macrophages.160 Additionally, certain respiratory viruses may invade the CNS through retrograde axonal transport along the vagus nerve, reaching brainstem respiratory centers and exacerbating respiratory symptoms such as respiratory distress.161,162
Extracellular Vesicles Mediators
Exosomes and other extracellular vesicles (EVs) released by pulmonary cells during inflammation carry bioactive molecules, such as microRNAs and proteins.163 These EVs can cross the blood-brain barrier, influencing cellular functions within the CNS and promoting neuroinflammation.163,164 Recent studies have identified EVs as potential mediators of lung-brain communication, capable of transmitting signals that induce neuroinflammation following pulmonary injury. For instance, ventilator-induced lung injury (VILI) activates pyroptosis pathways in spinal cord microglia via circulating exosomes.165,166 Experimental research demonstrated that lung-derived exosomes released during VILI carry activated caspase-1, causing a three-fold increase in Gasdermin-D (GSDMD) expression within the spinal cord, subsequently promoting neuronal apoptosis.148,167
Challenges and Prospects
Current Limitations
Respiratory complications—rather than the neurological level alone—largely determine length of stay and cost during the index admission for cervical and high‑thoracic SCI, underscoring the need for proactive pulmonary management.168 Contemporary care is mainly supportive: endotracheal intubation, tracheostomy, bronchodilators, airway‑clearance devices and empirical antibiotics. Although life‑saving, conventional mechanical ventilation (MV) is neuromuscularly uncoupled; prolonged passive inflation precipitates ventilator‑induced diaphragmatic dysfunction (VIDD) through disuse atrophy, oxidative stress and proteolysis.169 VIDD, together with baro‑/volutrauma and ventilator‑associated pneumonia, prolongs weaning, reduces survival and degrades quality of life. Extended MV also perturbs the central nervous system: deep sedation and immobility promote ICU‑acquired weakness, and the loss of afferent feedback from paralysed respiratory muscles may impair neuroplasticity in medullary and pontine networks.95 Indeed, the ability to wean from MV is one of the strongest predictors of long‑term survival after cervical SCI.170–172 Repeated antibiotic courses foster dysbiosis and resistance, while chronic infection perpetuates lung injury, leaving many patients ventilator‑dependent with recurrent pneumonia. These shortcomings highlight the urgent need to reactivate or replace central respiratory circuits and to rebalance post‑injury immune dysfunction; without addressing the neurogenic basis of ventilatory failure and its immunological sequelae, durable improvements in pulmonary and neurological outcomes will remain elusive.
A major limitation in managing respiratory complications after SCI is the absence of reliable biomarkers for guiding and monitoring therapeutic interventions.173 Patients with SCI exhibit substantial heterogeneity in neurological deficits, immune status, and susceptibility to pulmonary complications.174 Identifying biomarkers to stratify patients and predict therapeutic responses is therefore essential for effective personalized medicine.175,176 I Pro-inflammatory cytokines (such as IL-6 and TNF-α) and anti-inflammatory cytokines (such as IL-10), stress hormones (eg, cortisol), and microbial metabolites are candidate biomarkers that can help define a patient’s immune status and predict vulnerability to complications like pneumonia or SCI-induced immune depression (SCI-IDS).15,175,177,178 Similarly, biomarkers of neural damage or repair—including neurofilament proteins and growth factors—might indicate the efficacy of systemic treatments in promoting central nervous system (CNS) recovery.179 However, currently there are no validated biomarkers specifically reflecting lung-spinal cord crosstalk.15 For instance, the ratio of pro-inflammatory to anti-inflammatory cytokines in cerebrospinal fluid (CSF) or bronchoalveolar lavage fluid (BALF) could serve as indicators of neuroimmune interactions after SCI.15,177 The development of these biomarkers could enable clinicians to quickly identify patients at heightened risk for SCI-IDS or severe pulmonary complications, thus allowing early initiation and tailored dosing of interventions.15 Identifying these critical therapeutic windows through biomarker monitoring or advanced imaging is an ongoing research priority.180
Future Prospects
Immune‑stimulation Pre‑conditioning
Immune-stimulation pre-conditioning (IS-PC) utilizes sub-clinical doses of immune activators, such as Toll-like receptor (TLR) agonists, to induce protective immune tolerance and limit subsequent inflammatory responses following spinal cord injury (SCI). Recent preclinical studies demonstrate that systemic administration of ultra-low, non-pyrogenic doses of TLR ligands—including lipopolysaccharide (LPS; TLR4 agonist), CpG oligodeoxynucleotide (TLR9 agonist), or polyinosinic:polycytidylic acid (poly-I:C; TLR3 agonist)—24 to 72 hours before or shortly after SCI can significantly attenuate neuronal apoptosis and improve functional outcomes.181 The underlying mechanisms involve initial transient activation of NF-κB signaling, followed by induction of negative regulatory factors (A20, SOCS1, IRAK-M), enhanced expression of antioxidant transcription factors (Nrf2–HO-1 pathway), and promotion of protective autophagy.182 In rodent SCI models, pre-conditioning with low-dose LPS (eg, 0.1–0.2 mg/kg intraperitoneally) effectively reduces inflammatory cytokines and neuronal death, translating into meaningful improvements in locomotor function.183 Parallel research in acute lung injury models supports the concept, showing that intravenous administration of ultra-low-dose LPS (approximately 10 µg/kg) prior to lung ischemia–reperfusion injury significantly reduces pulmonary edema, cytokine release, neutrophil infiltration, and alveolar-capillary barrier disruption. These data collectively indicate a narrow therapeutic window: carefully controlled doses confer protection, whereas slightly higher doses exacerbate lung injury and inflammation.184
From a translational perspective, aerosolized delivery of low-dose immune stimulants is particularly appealing, given rapid pulmonary uptake with minimal systemic effects.185 Although aerosolized ultra-low-dose LPS inhalation has been used safely in healthy volunteers to model inflammation for drug testing, no clinical trials to date have evaluated IS-PC as a therapeutic strategy in SCI or ARDS patients.186 Importantly, the dysregulated immune environment post-SCI could alter responses to such immunostimulatory approaches, necessitating careful titration and monitoring.187
Emerging non-invasive transcutaneous VNS devices, feasible even in acute intensive care settings, are currently under investigation.188 Although further clinical validation is required, these preliminary findings underscore VNS as an attractive therapeutic option for addressing the neuroimmune dysfunction that links pulmonary complications and neurological injury after SCI.189,190
Vagus-Nerve Stimulation (VNS)
VNS acts via both cholinergic and adrenergic pathways to modulate inflammation, offering a promising adjunctive approach for SCI-associated respiratory complications.191,192 Physiologically, VNS activates the cholinergic anti-inflammatory pathway through α7 α7nAChR, thereby reducing pro-inflammatory cytokines such as IL-6 and TNF-α.192,193 Concurrently, VNS promotes adrenal epinephrine release, which exerts anti-inflammatory effects via β2-adrenergic receptors, further inhibiting NF-κB-mediated inflammatory signaling in alveolar macrophages.139,194
Clinical studies in ARDS patients have shown that VNS significantly decreases systemic IL-6 levels (by approximately 40%) and concurrently improves cognitive outcomes.195 Preclinical studies using a T9-level SCI rodent model demonstrated that VNS effectively reduces lipopolysaccharide-induced acute lung injury, indicating its critical role in modulating pulmonary inflammation after SCI.196,197 Thus, VNS potentially confers dual benefits in SCI: peripheral suppression of pulmonary inflammation, which may mitigate complications such as pneumonia or ARDS, and central modulation of neuroinflammation, potentially facilitating spinal cord repair.15
Conclusions
Pulmonary interventions after SCI are shifting from passive respiratory support toward targeted therapies that address the neuroimmune dysfunction central to SCI-related complications. As mounting evidence supports the bidirectional crosstalk between the lung and CNS, novel therapeutic strategies are emerging to modulate this interaction. These include VNS, immune-stimulation pre-conditioning with toll-like receptor agonists. Each aims not only to reduce respiratory morbidity and mortality but also to promote neurological recovery by rebalancing systemic immunity and enhancing CNS plasticity. However, several challenges remain—most notably, patient heterogeneity, a lack of robust biomarkers for patient stratification, and uncertainties in optimal intervention timing. Translating these experimental insights into clinical standards will require multimodal therapeutic frameworks, individualized protocols, and rigorous trials. Ultimately, this paradigm shift—from stabilizing respiration alone to therapeutically leveraging pulmonary-CNS interactions—offers the potential to improve both survival and neurological function in patients with SCI.
Data Sharing Statement
No datasets were generated or analyzed during the current study. The data that support the findings of this study are available from the corresponding author upon reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The National Natural Science Foundation (81973878),Top Talent Support Program for young and middle-aged people of Wuxi Health Committee (BJ2023069); Jiangsu CM Clinical Innovation Center of Degenerative Bone & Joint Disease (Jiangsu science and education of traditional Chinese medicine(2021)No. 4).
Disclosure
The authors declare that they have no competing interests.
References
1. Migliorini CE, New PW, Tonge BJ. Comparison of depression, anxiety and stress in persons with traumatic and non-traumatic post-acute spinal cord injury. Spinal Cord. 2009;47(11):783–19. doi:10.1038/sc.2009.43
2. New PW, Sundararajan V. Incidence of non-traumatic spinal cord injury in Victoria, Australia: a population-based study and literature review. Spinal Cord. 2008;46:406–411. doi:10.1038/sj.sc.3102152
3. Khadour FA, Khadour YA, Meng L, XinLi C, Xu T. Epidemiology features of traumatic and non-traumatic spinal cord injury in China, Wuhan. Sci Rep. 2024;14:1640. doi:10.1038/s41598-024-52210-4
4. Ding W, Hu S, Wang P, et al. Spinal cord injury: the global incidence, prevalence, and disability from the global burden of disease study 2019. Spine. 2022;47:1532–1540. doi:10.1097/BRS.0000000000004417
5. Liu Y, Yang X, He Z, et al. Spinal cord injury: global burden from 1990 to 2019 and projections up to 2030 using Bayesian age-period-cohort analysis. Front Neurol. 2023;14:1304153. doi:10.3389/fneur.2023.1304153
6. Sezer N, Akkuş S, Uğurlu FG. Chronic complications of spinal cord injury. World J Orthop. 2015;6:24–33. doi:10.5312/wjo.v6.i1.24
7. Sun X, Jones ZB, Chen XM, et al. Multiple organ dysfunction and systemic inflammation after spinal cord injury: a complex relationship. J Neuroinflammation. 2016;13:260.
8. Josefson C, Rekand T, Lundgren-Nilsson Å, Sunnerhagen KS. Respiratory complications during initial rehabilitation and survival following spinal cord injury in Sweden: a retrospective study. Spinal Cord. 2021;59:659–664. doi:10.1038/s41393-020-00549-6
9. Yang X-X, Huang Z-Q, Li Z-H, Ren D-F, Tang J-G. Risk factors and the surgery affection of respiratory complication and its mortality after acute traumatic cervical spinal cord injury. Medicine. 2017;96:e7887. doi:10.1097/MD.0000000000007887
10. Tollefsen E, Fondenes O. Respiratory complications associated with spinal cord injury. Tidsskr nor Laegeforen. 2012;132(9):1111–1114. doi:10.4045/tidsskr.10.0922
11. Hosang L, Canals RC, van der Flier FJ, et al. The lung microbiome regulates brain autoimmunity. Nature. 2022;603:138–144. doi:10.1038/s41586-022-04427-4
12. Bajinka O, Simbilyabo L, Tan Y, Jabang J, Saleem SA. Lung-brain axis. Crit Rev Microbiol. 2022;48:257–269. doi:10.1080/1040841X.2021.1960483
13. Araneda OF, Rosales-Antequera C, Contreras-Briceño F, et al. Systemic and pulmonary inflammation/oxidative damage: implications of general and respiratory muscle training in chronic spinal-cord-injured patients. Biology. 2023;12. doi:10.3390/biology12060828
14. Mifflin KA, Brennan FH, Guan Z, et al. Spinal cord injury impairs lung immunity in mice. J Immunol. 2022;209:157–170. doi:10.4049/jimmunol.2200192
15. Berk BC, Pereira A, Vizcarra VS, Pröschel C, Hsu CG. Spinal cord injury enhances lung inflammation and exacerbates immune response following exposure to LPS. Front Immunol. 2024;15:1483402. doi:10.3389/fimmu.2024.1483402
16. Mumaw CL, Levesque S, McGraw C, et al. Microglial priming through the lung-brain axis: the role of air pollution-induced circulating factors. FASEB J. 2016;30:1880–1891. doi:10.1096/fj.201500047
17. Greve HJ, Dunbar AL, Lombo CG, et al. The bidirectional lung brain-axis of amyloid-β pathology: ozone dysregulates the peri-plaque microenvironment. Brain. 2023;146. doi:10.1093/brain/awac113
18. Starke N, Challa NV, Yuan H, et al. Extracellular vesicle ASC: a novel mediator for lung-brain axis in preterm brain injury. Am J Respir Cell Mol Biol. 2024;71:464–480. doi:10.1165/rcmb.2023-0402OC
19. Park H, Lee CH. The impact of pulmonary disorders on neurological health (lung-brain axis). Immune Netw. 2024;24:e20. doi:10.4110/in.2024.24.e20
20. Xie Y, Zhang L, Guo S, et al. Changes in respiratory structure and function after traumatic cervical spinal cord injury: observations from spinal cord and brain. Front Neurol. 2023;14:1251833. doi:10.3389/fneur.2023.1251833
21. Michel-Flutot P, Lane MA, Lepore AC, Vinit S. Therapeutic strategies targeting respiratory recovery after spinal cord injury: from preclinical development to clinical translation. Cells. 2023;12. doi:10.3390/cells12111519
22. DiSabato DJ, Marion CM, Mifflin KA, et al. System failure: systemic inflammation following spinal cord injury. Eur J Immunol. 2024;54:e2250274. doi:10.1002/eji.202250274
23. Berlowitz DJ, Wadsworth B, Ross J. Respiratory problems and management in people with spinal cord injury. Breathe. 2016;12:328–340. doi:10.1183/20734735.012616
24. Hagen EM, Eide GE, Rekand T, Gilhus NE, Gronning M. A 50-year follow-up of the incidence of traumatic spinal cord injuries in Western Norway. Spinal Cord. 2010;48:313–318. doi:10.1038/sc.2009.133
25. Jackson AB, Groomes TE. Incidence of respiratory complications following spinal cord injury. Arch Phys Med Rehabil. 1994;75:270–275.
26. Sampol J, González-Viejo MÁ, Gómez A, et al. Predictors of respiratory complications in patients with C5-T5 spinal cord injuries. Spinal Cord. 2020;58:1249–1254. doi:10.1038/s41393-020-0506-7
27. Agostinello J, Battistuzzo CR, Batchelor PE. Early clinical predictors of pneumonia in critically ill spinal cord injured individuals: a retrospective cohort study. Spinal Cord. 2019;57:41–48. doi:10.1038/s41393-018-0196-6
28. Xie Y, Wang Y, Zhou Y, et al. A nomogram for predicting acute respiratory failure after cervical traumatic spinal cord injury based on admission clinical findings. Neurocrit Care. 2022;36:421–433. doi:10.1007/s12028-021-01302-4
29. Mueller G, Berlowitz DJ, Raab AM, et al. Incidence and risk factors of pneumonia in individuals with acute spinal cord injury: a multi-national, multi-center, prospective cohort study. Arch Phys Med Rehabil. 2024;105:884–891. doi:10.1016/j.apmr.2023.11.002
30. Frisbie JH, Sharma GVRK. Right bundle branch block as a screening test for pulmonary embolism in chronic spinal cord injury. Arch Phys Med Rehabil. 2009;90:1241–1244. doi:10.1016/j.apmr.2009.01.013
31. Alabed S, De Heredia LL, Naidoo A, et al. Incidence of pulmonary embolism after the first 3 months of spinal cord injury. Spinal Cord. 2015;53:835–837. doi:10.1038/sc.2015.105
32. Bauman KA, Kurili A, Schotland HM, et al. Simplified approach to diagnosing sleep-disordered breathing and nocturnal hypercapnia in individuals with spinal cord injury. Arch Phys Med Rehabil. 2016;97:363–371. doi:10.1016/j.apmr.2015.07.026
33. Sankari A, Bascom A, Oomman S, Badr MS. Sleep disordered breathing in chronic spinal cord injury. J Clin Sleep Med. 2014;10:65–72. doi:10.5664/jcsm.3362
34. Castillo-Escario Y, Kumru H, Ferrer-Lluis I, Vidal J, Jané R. Detection of sleep-disordered breathing in patients with spinal cord injury using a smartphone. Sensors. 2021;21. doi:10.3390/s21217182
35. Berlowitz DJ, Brown DJ, Campbell DA, Pierce RJ. A longitudinal evaluation of sleep and breathing in the first year after cervical spinal cord injury. Arch Phys Med Rehabil. 2005;86:1193–1199.
36. Leduc BE, Dagher JH, Mayer P, Bellemare F, Lepage Y. Estimated prevalence of obstructive sleep apnea-hypopnea syndrome after cervical cord injury. Arch Phys Med Rehabil. 2007;88:333–337.
37. Stockhammer E, Tobon A, Michel F, et al. Characteristics of sleep apnea syndrome in tetraplegic patients. Spinal Cord. 2002;40:286–294.
38. Burns SP, Little JW, Hussey JD, Lyman P, Lakshminarayanan S. Sleep apnea syndrome in chronic spinal cord injury: associated factors and treatment. Arch Phys Med Rehabil. 2000;81:1334–1339.
39. McEvoy RD, Mykytyn I, Sajkov D, et al. Sleep apnoea in patients with quadriplegia. Thorax. 1995;50:613–619.
40. Short DJ, Stradling JR, Williams SJ. Prevalence of sleep apnoea in patients over 40 years of age with spinal cord lesions. J Neurol Neurosurg Psychiatry. 1992;55:1032–1036.
41. Klefbeck B, Sternhag M, Weinberg J, et al. Obstructive sleep apneas in relation to severity of cervical spinal cord injury. Spinal Cord. 1998;36:621–628.
42. Consortium for Spinal Cord Medicine. Respiratory management following spinal cord injury: a clinical practice guideline for health-care professionals. J Spinal Cord Med. 2005;28:259–293.
43. Linn WS, Adkins RH, Gong H, Waters RL. Pulmonary function in chronic spinal cord injury: a cross-sectional survey of 222 southern California adult outpatients. Arch Phys Med Rehabil. 2000;81:757–763. doi:10.1016/s0003-9993(00)90107-2
44. Casha S, Christie S. A systematic review of intensive cardiopulmonary management after spinal cord injury. J Neurotrauma. 2011;28:1479–1495. doi:10.1089/neu.2009.1156
45. Mourelo Fariña M, Salvador de la Barrera S, Montoto Marqués A, Ferreiro Velasco ME, Galeiras Vázquez R. Update on traumatic acute spinal cord injury. Part 2. Med Intensiva. 2017;41:306–315. doi:10.1016/j.medin.2016.10.014
46. van den Berg ME, Castellote JM, de Pedro-Cuesta J, Mahillo-Fernandez I. Survival after spinal cord injury: a systematic review. J Neurotrauma. 2010;27:1517–1528. doi:10.1089/neu.2009.1138
47. Waddimba AC, Jain NB, Stolzmann K, et al. Predictors of cardiopulmonary hospitalization in chronic spinal cord injury. Arch Phys Med Rehabil. 2009;90:193–200. doi:10.1016/j.apmr.2008.07.026
48. Sengupta D, Bindra A, Kumar N, et al. Respiratory morbidity and mortality of traumatic cervical spinal cord injury at a level I trauma center in India. Spinal Cord Ser Cases. 2021;7(36). doi:10.1038/s41394-020-00371-5
49. Brown R, DiMarco AF, Hoit JD, Garshick E. Respiratory dysfunction and management in spinal cord injury. Respir Care. 2006;51.
50. Chen L, Rackley CR. Diagnosis and epidemiology of acute respiratory failure. Crit Care Clin. 2024;40:221–233. doi:10.1016/j.ccc.2023.12.001
51. Juniper M. NEWS2, patient safety and hypercapnic respiratory failure. Clin Med Lond. 2022;22:518–521. doi:10.7861/clinmed.2022-0352
52. Raab AM, Mueller G, Elsig S, et al. Systematic review of incidence studies of pneumonia in persons with spinal cord injury. J Clin Med. 2021;11. doi:10.3390/jcm11010211
53. Burns SP. Acute respiratory infections in persons with spinal cord injury. Phys Med Rehabil Clin N Am. 2007;18.
54. Cotton BA, Pryor JP, Chinwalla I, et al. Respiratory complications and mortality risk associated with thoracic spine injury. J Trauma. 2005;59:1400–1407;discussion1407–1409. doi:10.1097/01.ta.0000196005.49422.e6
55. Galeiras Vázquez R, Rascado Sedes P, Mourelo Fariña M, Montoto Marqués A, Ferreiro Velasco ME. Respiratory management in the patient with spinal cord injury. Biomed Res Int. 2013;168757. doi:10.1155/2013/168757
56. Krassioukov A. Autonomic function following cervical spinal cord injury. Respir Physiol Neurobiol. 2009;169:157–164. doi:10.1016/j.resp.2009.08.003
57. Zeng C, Lagier D, Lee J-W, Vidal Melo MF. Perioperative pulmonary atelectasis: Part I. Biol Mech Anesthesiol. 2022;136:181–205. doi:10.1097/ALN.0000000000003943
58. Chen CF, Lien IN, Wu MC. Respiratory function in patients with spinal cord injuries: effects of posture. Paraplegia. 1990;28:81–86.
59. Baydur A, Adkins RH, Milic-Emili J. Lung mechanics in individuals with spinal cord injury: effects of injury level and posture. J Appl Physiol. 2001;90:405–411. doi:10.1152/jappl.2001.90.2.405
60. Chhabra HS, Sharawat R, Vishwakarma G. In-hospital mortality in people with complete acute traumatic spinal cord injury at a tertiary care center in India-a retrospective analysis. Spinal Cord. 2022;60:210–215. doi:10.1038/s41393-021-00657-x
61. Lv B, Wang H, Li W, et al. Admission prevalence and risk factors of deep vein thrombosis in patients with spinal cord injury complicated with cervical fractures. Clin Appl Thromb Hemost. 2022;28:10760296221108969. doi:10.1177/10760296221108969
62. Wulf MJ, Tom VJ. Consequences of spinal cord injury on the sympathetic nervous system. Front Cell Neurosci. 2023;17:999253. doi:10.3389/fncel.2023.999253
63. He B, Nan G. Pulmonary edema and hemorrhage after acute spinal cord injury in rats. Spine J. 2016;16:547–551. doi:10.1016/j.spinee.2015.11.065
64. Šedý J, Kuneš J, Zicha J. Pathogenetic mechanisms of neurogenic pulmonary edema. J Neurotrauma. 2015;32:1135–1145. doi:10.1089/neu.2014.3609
65. Calder KB, Estores IM, Krassioukov A. Autonomic dysreflexia and associated acute neurogenic pulmonary edema in a patient with spinal cord injury: a case report and review of the literature. Spinal Cord. 2009;47:423–425. doi:10.1038/sc.2008.152
66. Šedý J, Zicha J, Kunes J, Jendelová P, Syková E. Mechanisms of neurogenic pulmonary edema development. Physiol Res. 2008;57:499–506. doi:10.33549/physiolres.931432
67. Reyes MRL, Elmo MJ, Menachem B, Granda SM. A primary care provider’s guide to managing respiratory health in subacute and chronic spinal cord injury. Top Spinal Cord Inj Rehabil. 2020;26:116–122. doi:10.46292/sci2602-116
68. Aboussouan LS. Sleep-disordered breathing in neuromuscular disease. Am J Respir Crit Care Med. 2015;191:979–989. doi:10.1164/rccm.201412-2224CI
69. Bourke SC, Gibson GJ. Sleep and breathing in neuromuscular disease. Eur Respir J. 2002;19:1194–1201.
70. Mohammadieh AM, Chan A, Cistulli PA. Sleep-disordered breathing - clinical spectrum. Aust Dent J. 2024;69(Suppl 1):S45–S52. doi:10.1111/adj.13043
71. Cardozo CP. Respiratory complications of spinal cord injury. J Spinal Cord Med. 2007;30:307–308.
72. Schilero GJ, Bauman WA, Radulovic M. Traumatic spinal cord injury: pulmonary physiologic principles and management. Clinics Chest Med. 2018;39:411–425. doi:10.1016/j.ccm.2018.02.002
73. Terson de Paleville DG, McKay WB, Folz RJ, Ovechkin AV. Respiratory motor control disrupted by spinal cord injury: mechanisms, evaluation, and restoration. Transl Stroke Res. 2011;2:463–473. doi:10.1007/s12975-011-0114-0
74. Berney S, Bragge P, Granger C, Opdam H, Denehy L. The acute respiratory management of cervical spinal cord injury in the first 6 weeks after injury: a systematic review. Spinal Cord. 2011;49:17–29. doi:10.1038/sc.2010.39
75. Sheel AW, Reid WD, Townson AF, Ayas NT, Konnyu KJ. Effects of exercise training and inspiratory muscle training in spinal cord injury: a systematic review. J Spinal Cord Med. 2008;31:500–508.
76. Kang SW, Shin JC, Park CI, et al. Relationship between inspiratory muscle strength and cough capacity in cervical spinal cord injured patients. Spinal Cord. 2006;44:242–248.
77. Shank CD, Walters BC, Hadley MN. Current topics in the management of acute traumatic spinal cord injury. Neurocrit Care. 2019;30:261–271. doi:10.1007/s12028-018-0537-5
78. Undem BJ, Kollarik M. The role of vagal afferent nerves in chronic obstructive pulmonary disease. Proc Am Thorac Soc 2. 2005.
79. Popa C, Popa F, Grigorean VT, et al. Vascular dysfunctions following spinal cord injury. J Med Life. 2010;3:275–285.
80. Schappe MS, Brinn PA, Joshi NR, et al. A vagal reflex evoked by airway closure. Nature. 2024;627:830–838. doi:10.1038/s41586-024-07144-2
81. Andrade MJ, Quintas FL, Silva AM, Cruz P. Is autonomic dysreflexia a cause of respiratory dysfunction after spinal cord injury? Spinal Cord Ser Cases. 2021;7:4. doi:10.1038/s41394-020-00372-4
82. Grimm DR, Arias E, Lesser M, Bauman WA, Almenoff PL. Airway hyperresponsiveness to ultrasonically nebulized distilled water in subjects with tetraplegia. J Appl Physiol. 1999;86:1165–1169.
83. Henke AM, Billington ZJ, Gater DR. Autonomic dysfunction and management after spinal cord injury: a narrative review. J Pers Med. 2022;12. doi:10.3390/jpm12071110
84. Kiker JD, Woodside JR, Jelinek GE. Neurogenic pulmonary edema associated with autonomic dysreflexia. J Urol. 1982;128:1038–1039. doi:10.1016/s0022-5347(17)53334-0
85. Davison DL, Terek M, Chawla LS. Neurogenic pulmonary edema. Crit Care. 2012;16(212). doi:10.1186/cc11226
86. Parinandi N, Gerasimovskaya E, Verin A. Editorial: molecular mechanisms of lung endothelial permeability. Front Physiol. 2022;13:976873. doi:10.3389/fphys.2022.976873
87. King LS, Nielsen S, Agre P, Brown RH. Decreased pulmonary vascular permeability in aquaporin-1-null humans. Proc Natl Acad Sci U S A. 2002;99:1059–1063. doi:10.1073/pnas.022626499
88. Rodgers KA, Kigerl KA, Schwab JM, Popovich PG. Immune dysfunction after spinal cord injury - A review of autonomic and neuroendocrine mechanisms. Curr Opin Pharmacol. 2022;64:102230. doi:10.1016/j.coph.2022.102230
89. Allison DJ, Ditor DS. Immune dysfunction and chronic inflammation following spinal cord injury. Spinal Cord. 2015;53:14–18. doi:10.1038/sc.2014.184
90. Herman JP, McKlveen JM, Ghosal S, et al. Regulation of the hypothalamic-pituitary-adrenocortical stress response. Compr Physiol. 2016;6:603–621. doi:10.1002/cphy.c150015
91. Carpenter RS, Marbourg JM, Brennan FH, et al. Spinal cord injury causes chronic bone marrow failure. Nat Commun. 2020;11(3702). doi:10.1038/s41467-020-17564-z
92. Kelly MJ, Breathnach C, Tracey KJ, Donnelly SC. Manipulation of the inflammatory reflex as a therapeutic strategy. Cell Rep Med. 2022;3:100696. doi:10.1016/j.xcrm.2022.100696
93. Han X, Li W, Li P, et al. Stimulation of α7 nicotinic acetylcholine receptor by nicotine suppresses decidual M1 macrophage polarization against inflammation in lipopolysaccharide-induced preeclampsia-like mouse model. Front Immunol. 2021;12:642071. doi:10.3389/fimmu.2021.642071
94. Zhu X, Dai S, Xia B, Gong J, Ma B. Activation of the alpha 7 nicotinic acetylcholine receptor mitigates osteoarthritis progression by inhibiting NF-κB/NLRP3 inflammasome activation and enhancing autophagy. PLoS One. 2021;16:e0256507. doi:10.1371/journal.pone.0256507
95. Pereira MR, Leite PE. The involvement of parasympathetic and sympathetic nerve in the inflammatory reflex. J Cell Physiol. 2016;231:1862–1869. doi:10.1002/jcp.25307
96. Zhen-Gang L, Fan Y, Jingwei S, et al. Revisiting the immune landscape post spinal cord injury: more than black and white. Front Aging Neurosci. 2022;14:963539. doi:10.3389/fnagi.2022.963539
97. Held KS, Lane TE. Spinal cord injury, immunodepression, and antigenic challenge. Semin Immunol. 2014;26(5):415–420. doi:10.1016/j.smim.2014.03.003
98. Lucin KM, Sanders VM, Jones TB, Malarkey WB, Popovich PG. Impaired antibody synthesis after spinal cord injury is level dependent and is due to sympathetic nervous system dysregulation. Exp Neurol. 2007;207(1):75–84. doi:10.1016/j.expneurol.2007.05.019
99. Al-Kuraishy HM, Al-Gareeb AI, Mostafa-Hedeab G, et al. Effects of β-blockers on the sympathetic and cytokines storms in Covid-19. Front Immunol. 2021;12(749291). doi:10.3389/fimmu.2021.749291
100. Sykora M, Siarnik P, Diedler J. β-blockers, pneumonia, and outcome after ischemic stroke: evidence from virtual International Stroke Trials Archive. Stroke. 2015;46(5):1269–1274. doi:10.1161/STROKEAHA.114.008260
101. Balas M, Jaja BNR, Harrington EM, et al. Earlier tracheostomy reduces complications in complete cervical spinal cord injury in real-world practice: analysis of a multicenter cohort of 2001 patients. Neurosurgery. 2023;93(6):1305–1312. doi:10.1227/neu.0000000000002575
102. Long -P-P, Sun D-W, Zhang Z-F. Risk factors for tracheostomy after traumatic cervical spinal cord injury: a 10-year study of 456 patients. Orthop Surg. 2022;14(1):10–17. doi:10.1111/os.13172
103. Wang Y, Lu H, Teng H, et al. Efficacy and safety of early tracheotomy in acute cervical spinal cord injury. J Coll Physicians Surg Pak. 2020;30(9):956–960. doi:10.29271/jcpsp.2020.09.956
104. Beom J-Y, Seo H-Y. The need for early tracheostomy in patients with traumatic cervical cord injury. Clin Orthop Surg. 2018;10(2):191–196. doi:10.4055/cios.2018.10.2.191
105. Foran SJ, Taran S, Singh JM, Kutsogiannis DJ, McCredie V. Timing of tracheostomy in acute traumatic spinal cord injury: a systematic review and meta-analysis. J Trauma Acute Care Surg. 2022;92(1):223–231. doi:10.1097/TA.0000000000003394
106. Khan M, Prabhakaran K, Jehan F, et al. Early tracheostomy in patients with cervical spine injury reduces morbidity and improves resource utilization. Am J Surg. 2020;220(3):773–777. doi:10.1016/j.amjsurg.2020.01.054
107. Tran DH, Le HT, Chu TTQ, Pham HTC, Le ANV. The effects of inspiratory muscle training in individuals with cervical spinal cord injuries: a systematic review and meta-analysis. Ann Rehabil Med. 2025;49:152–163. doi:10.5535/arm.250013
108. El-Sayed Attalla AF, Ahmed KT, Abd El Monem M. Effects of inspiratory muscle training on clinical predictors of respiratory muscle strength and lung function in burned patients with inhalation injury. J Burn Care Res. 2023;44:140–145. doi:10.1093/jbcr/irac163
109. Allen J, Astin R, Smith C, Banks D, Turner C. Expiratory muscle strength training improves measures of pressure generation and cough strength in a patient with myotonic dystrophy type 1. Neuromuscul Disord. 2020;30:750–755. doi:10.1016/j.nmd.2020.07.003
110. Hung T-Y, Wu WL, Kuo HC, et al. Effect of abdominal weight training with and without cough machine assistance on lung function in the patients with prolonged mechanical ventilation: a randomized trial. Crit Care. 2022;26:153. doi:10.1186/s13054-022-04012-1
111. Elkins M, Dentice R. Inspiratory muscle training facilitates weaning from mechanical ventilation among patients in the intensive care unit: a systematic review. J Physiother. 2015;61:125–134. doi:10.1016/j.jphys.2015.05.016
112. Ahmed S, Daniel Martin A, Smith BK. Inspiratory muscle training in patients with prolonged mechanical ventilation: narrative review. Cardiopulm Phys Ther J. 2019;30:44–50. doi:10.1097/CPT.0000000000000092
113. Villelabeitia-Jaureguizar K, Calvo-Lobo C, Rodríguez-Sanz D, et al. Low intensity respiratory muscle training in COVID-19 patients after invasive mechanical ventilation: a retrospective case-series study. Biomedicines. 2022;10. doi:10.3390/biomedicines10112807
114. Liu F, Jones AYM, Tsang RCC, Yam TTT, Tsang WWN. Effects of inspiratory muscle training on respiratory function, diaphragmatic thickness, balance control, exercise capacity and quality of life in people after stroke: a randomized controlled trial protocol. PLoS One. 2025;20:e0319899. doi:10.1371/journal.pone.0319899
115. Wong SL, Shem K, Crew J. Specialized respiratory management for acute cervical spinal cord injury:: a retrospective analysis. Top Spinal Cord Inj Rehabil. 2012;18:283–290. doi:10.1310/sci1804-283
116. Girou E, Schortgen F, Delclaux C, et al. Association of noninvasive ventilation with nosocomial infections and survival in critically ill patients. JAMA. 2000;284:2361–2367.
117. Robert D, Argaud L. Clinical review: long-term noninvasive ventilation. Crit Care. 2007;11:210.
118. Pratiwi SH. Effectiveness of respiratory muscle training interventions in patients with spinal cord injury; a literature review. JIKO. 2023;7:43–50. doi:10.46749/jiko.v7i1.120
119. Chen T-H, Hsu J-H. Noninvasive ventilation and mechanical insufflator-exsufflator for acute respiratory failure in children with neuromuscular disorders. Front Pediatr. 2020;8(593282). doi:10.3389/fped.2020.593282
120. Ren S, Li W, Wang L, et al. Numerical analysis of airway mucus clearance effectiveness using assisted coughing techniques. Sci Rep. 2020;10:2030. doi:10.1038/s41598-020-58922-7
121. Annunziata A, Coppola A, Polistina GE, et al. Daytime alternatives for non-invasive mechanical ventilation in neuromuscular disorders. Acta Myol. 2021;40:51–60. doi:10.36185/2532-1900-042
122. Wijkstra PJ, van der Aa H, Hofker HS, et al. Diaphragm pacing in patients with spinal cord injury: a European experience. Respiration. 2022;101:18–24. doi:10.1159/000517401
123. Bezdudnaya T, Lane MA, Marchenko V. Paced breathing and phrenic nerve responses evoked by epidural stimulation following complete high cervical spinal cord injury in rats. J Appl Physiol. 2018;125:687–696. doi:10.1152/japplphysiol.00895.2017
124. Onders RP, Elmo M, Kaplan C, et al. Long-term experience with diaphragm pacing for traumatic spinal cord injury: early implantation should be considered. Surgery. 2018;164:705–711. doi:10.1016/j.surg.2018.06.050
125. Tedde ML, Vasconcelos Filho P, Hajjar LA, et al. Diaphragmatic pacing stimulation in spinal cord injury: anesthetic and perioperative management. Clinics. 2012;67:1265–1269.
126. DiMarco AF, Onders RP, Kowalski KE, et al. Phrenic nerve pacing in a tetraplegic patient via intramuscular diaphragm electrodes. Am J Respir Crit Care Med. 2002;166:1604–1606.
127. Shin JC, Han EY, Cho KH, Im SH. Improvement in pulmonary function with short-term rehabilitation treatment in spinal cord injury patients. Sci Rep. 2019;9:17091. doi:10.1038/s41598-019-52526-6
128. Bach JR. Noninvasive respiratory management of high level spinal cord injury. J Spinal Cord Med. 2012;35:72–80. doi:10.1179/2045772311Y.0000000051
129. Abdallah SJ, Chan DS, Glicksman R, et al. Abdominal binding improves neuromuscular efficiency of the human diaphragm during exercise. Front Physiol. 2017;8(345). doi:10.3389/fphys.2017.00345
130. Li C, Chen W, Lin F, et al. Functional two-way crosstalk between brain and lung: the brain-lung axis. Cell Mol Neurobiol. 2023;43. doi:10.1007/s10571-022-01238-z
131. Sahu B, Sandhir R, Naura AS. Two hit induced acute lung injury impairs cognitive function in mice: a potential model to study cross talk between lung and brain. Brain Behav Immun. 2018;73:633–642. doi:10.1016/j.bbi.2018.07.013
132. Hopkins RO, Weaver LK, Collingridge D, et al. Two-year cognitive, emotional, and quality-of-life outcomes in acute respiratory distress syndrome. Am J Respir Crit Care Med. 2005;171:340–347.
133. Ziaka M, Exadaktylos A. Pathophysiology of acute lung injury in patients with acute brain injury: the triple-hit hypothesis. Crit Care. 2024;28:71. doi:10.1186/s13054-024-04855-w
134. Lanyu Z, Feilong H. Emerging role of extracellular vesicles in lung injury and inflammation. Biomed Pharmacother. 2019;113(108748). doi:10.1016/j.biopha.2019.108748
135. Zhang C-N, Li F-J, Zhao Z-L, Zhang J-N. The role of extracellular vesicles in traumatic brain injury-induced acute lung injury. Am J Physiol Lung Cell Mol Physiol. 2021;321:L885–L891. doi:10.1152/ajplung.00023.2021
136. Kubin L, Alheid GF, Zuperku EJ, McCrimmon DR. Central pathways of pulmonary and lower airway vagal afferents. J Appl Physiol. 2006;101:618–627.
137. Huang J, Huang W, Yi J, et al. Mesenchymal stromal cells alleviate depressive and anxiety-like behaviors via a lung vagal-to-brain axis in male mice. Nat Commun. 2023;14:7406. doi:10.1038/s41467-023-43150-0
138. Chang RB, Strochlic DE, Williams EK, Umans BD, Liberles SD. Vagal Sensory Neuron Subtypes that Differentially Control Breathing. Cell. 2015;161:622–633. doi:10.1016/j.cell.2015.03.022
139. Murray K, Cremin M, Tay E, et al. Inhibition of acute lung inflammation by a neuroimmune circuit induced by vagal nerve stimulation. bioRxiv. 2025. doi:10.1101/2025.02.12.637880
140. Su Y, Barr J, Jaquish A, et al. Identification of lung innervating sensory neurons and their target specificity. Am J Physiol Lung Cell Mol Physiol. 2022;322:L50–L63. doi:10.1152/ajplung.00376.2021
141. Krapić M, Kavazović I, Wensveen FM. Immunological mechanisms of sickness behavior in viral infection. Viruses. 2021;13. doi:10.3390/v13112245
142. Granton E, Brown L, Defaye M, et al. Biofilm exopolysaccharides alter sensory-neuron-mediated sickness during lung infection. Cell. 2024;187:1874–1888e1814. doi:10.1016/j.cell.2024.03.001
143. Cross LJM, Matthay MA. Biomarkers in acute lung injury: insights into the pathogenesis of acute lung injury. Crit Care Clin. 2011;27:355–377. doi:10.1016/j.ccc.2010.12.005
144. Zhou K, Lu J. Progress in cytokine research for ARDS: a comprehensive review. Open Med. 2024;19:20241076. doi:10.1515/med-2024-1076
145. Wang X, Wang Y, Pan H, Yan C. Dimethyl fumarate prevents acute lung injury related cognitive impairment potentially via reducing inflammation. J Cardiothorac Surg. 2021;16:331. doi:10.1186/s13019-021-01705-6
146. Zong T, Li N, Han F, et al. Microglial depletion rescues spatial memory impairment caused by LPS administration in adult mice. Peer J. 2024;12:e18552. doi:10.7717/peerj.18552
147. Albaiceta GM, Brochard L, Dos Santos CC, et al. The central nervous system during lung injury and mechanical ventilation: a narrative review. Br J Anaesth. 2021;127:648–659. doi:10.1016/j.bja.2021.05.038
148. Chavez L, Meguro J, Chen S, et al. Circulating extracellular vesicles activate the pyroptosis pathway in the brain following ventilation-induced lung injury. J Neuroinflammation. 2021;18:310. doi:10.1186/s12974-021-02364-z
149. Bietar B, Lehmann C, Stadnyk AW. Effects of CNS injury-induced immunosuppression on pulmonary immunity. Life. 2021;11. doi:10.3390/life11060576
150. Wang L, Botchway BOA, Liu X. The repression of the HMGB1-TLR4-NF-κB signaling pathway by Safflower Yellow may improve spinal cord injury. Front Neurosci. 2021;15:803885. doi:10.3389/fnins.2021.803885
151. Batista CRA, Gomes GF, Candelario-Jalil E, Fiebich BL, de Oliveira ACP. Lipopolysaccharide-induced neuroinflammation as a bridge to understand neurodegeneration. Int J Mol Sci. 2019;20. doi:10.3390/ijms20092293
152. Kalyan M, Tousif AH, Sonali S, et al. Role of endogenous lipopolysaccharides in neurological disorders. Cells. 2022;11. doi:10.3390/cells11244038
153. McGuirk P, McCann C, Mills KHG. Pathogen-specific T regulatory 1 cells induced in the respiratory tract by a bacterial molecule that stimulates interleukin 10 production by dendritic cells: a novel strategy for evasion of protective T helper type 1 responses by Bordetella pertussis. J Exp Med. 2002;195:221–231.
154. Mikhak Z, Strassner JP, Luster AD. Lung dendritic cells imprint T cell lung homing and promote lung immunity through the chemokine receptor CCR4. J Exp Med. 2013;210:1855–1869. doi:10.1084/jem.20130091
155. Gao Y, Wang K, Lin Z, et al. The emerging roles of microbiome and short-chain fatty acids in the pathogenesis of bronchopulmonary dysplasia. Front Cell Infect Microbiol. 2024;14:1434687. doi:10.3389/fcimb.2024.1434687
156. Dombi ZB, Szendi I, Burnet PWJ. Brain derived neurotrophic factor and cognitive dysfunction in the Schizophrenia-bipolar spectrum: a systematic review and meta-analysis. Front Psychiatry. 2022;13:827322. doi:10.3389/fpsyt.2022.827322
157. Huang Y-S, Ogbechi J, Clanchy FI, Williams RO, Stone TW. IDO and Kynurenine metabolites in peripheral and CNS disorders. Front Immunol. 2020;11:388. doi:10.3389/fimmu.2020.00388
158. Dantzer R. Role of the Kynurenine metabolism pathway in inflammation-induced depression: preclinical approaches. Curr Top Behav Neurosci. 2017;31:117–138. doi:10.1007/7854_2016_6
159. Kim H, Chen L, Lim G, et al. Brain indoleamine 2,3-dioxygenase contributes to the comorbidity of pain and depression. J Clin Invest. 2012;122:2940–2954. doi:10.1172/JCI61884
160. Denham ST, Brown JCS. Mechanisms of pulmonary escape and dissemination by Cryptococcus neoformans. J Fungi. 2018;4. doi:10.3390/jof4010025
161. Förster M, Weyers V, Küry P, et al. Neurological manifestations of severe acute respiratory syndrome coronavirus 2-a controversy ‘gone viral’. Brain Commun. 2020;2:fcaa149. doi:10.1093/braincomms/fcaa149
162. Bohmwald K, Gálvez NMS, Ríos M, Kalergis AM. Neurologic alterations due to respiratory virus infections. Front Cell Neurosci. 2018;12:386. doi:10.3389/fncel.2018.00386
163. Osaid Z, Haider M, Hamoudi R, Harati R. Exosomes interactions with the blood-brain barrier: implications for cerebral disorders and therapeutics. Int J Mol Sci. 2023;24. doi:10.3390/ijms242115635
164. Balusu S, Van Wonterghem E, De Rycke R, et al. Identification of a novel mechanism of blood-brain communication during peripheral inflammation via choroid plexus-derived extracellular vesicles. EMBO Mol Med. 2016;8:1162–1183. doi:10.15252/emmm.201606271
165. Gu J, Wu J, Wang C, et al. BMSCs-derived exosomes inhibit macrophage/microglia pyroptosis by increasing autophagy through the miR-21a-5p/PELI1 axis in spinal cord injury. Aging. 2024;16:5184–5206. doi:10.18632/aging.205638
166. Wang Y, Jia L, Wei M, et al. Circulating exosomes mediate neurodegeneration following hepatic ischemia-reperfusion through inducing microglial pyroptosis in the developing hippocampus. Transplantation. 2023;107:2364–2376. doi:10.1097/TP.0000000000004664
167. Mahida RY, Matsumoto S, Matthay MA. Extracellular vesicles: a new frontier for research in acute respiratory distress syndrome. Am J Respir Cell Mol Biol. 2020;63:15–24. doi:10.1165/rcmb.2019-0447TR
168. Petrof BJ, Jaber S, Matecki S. Ventilator-induced diaphragmatic dysfunction. Curr Opin Crit Care. 2010;16:19–25. doi:10.1097/MCC.0b013e328334b166
169. Schreiber AF, Garlasco J, Vieira F, et al. Separation from mechanical ventilation and survival after spinal cord injury: a systematic review and meta-analysis. Ann Intensive Care. 2021;11:149. doi:10.1186/s13613-021-00938-x
170. Bassi T, Taran S, Girard TD, Robba C, Goligher EC. Ventilator-associated brain injury: a new priority for research in mechanical ventilation. Am J Respir Crit Care Med. 2024;209:1186–1188. doi:10.1164/rccm.202401-0069VP
171. Ziaka M, Exadaktylos A. Brain-lung interactions and mechanical ventilation in patients with isolated brain injury. Crit Care. 2021;25:358. doi:10.1186/s13054-021-03778-0
172. Bassi TG, Rohrs EC, Fernandez KC, et al. Brain injury after 50 h of lung-protective mechanical ventilation in a preclinical model. Sci Rep. 2021;11:5105. doi:10.1038/s41598-021-84440-1
173. Leister I, Haider T, Mattiassich G, et al. Biomarkers in traumatic spinal cord injury-technical and clinical considerations: a systematic review. Neurorehabil Neural Repair. 2020;34. doi:10.1177/1545968319899920
174. Stukas S, Cooper J, Gill J, et al. Association of CSF and serum neurofilament light and glial fibrillary acidic protein, injury severity, and outcome in spinal cord injury. Neurology. 2023;100:e1221–e1233. doi:10.1212/WNL.0000000000206744
175. Alostaz H, Cai L. Biomarkers from secondary complications in spinal cord injury. Curr Pharmacol Rep. 2022;8:20–30. doi:10.1007/s40495-021-00268-3
176. Albayar AA, Roche A, Swiatkowski P, et al. Biomarkers in spinal cord injury: prognostic insights and future potentials. Front Neurol. 2019;10:27. doi:10.3389/fneur.2019.00027
177. Elizei SS, Kwon BK. The translational importance of establishing biomarkers of human spinal cord injury. Neural Regen Res. 2017;12:385–388. doi:10.4103/1673-5374.202933
178. Noushad S, Ahmed S, Ansari B, et al. Physiological biomarkers of chronic stress: a systematic review. Int J Health Sci. 2021;15:46–59.
179. Wang L, Gu S, Gan J, et al. Neural stem cells overexpressing nerve growth factor improve functional recovery in rats following spinal cord injury via modulating microenvironment and enhancing endogenous neurogenesis. Front Cell Neurosci. 2021;15:773375. doi:10.3389/fncel.2021.773375
180. Gumbel JH, Yang CB, Hubscher CH. Timeline of changes in biomarkers associated with spinal cord injury-induced polyuria. Neurotrauma Rep. 2021;2:462–475. doi:10.1089/neur.2021.0046
181. Sangaran PG, Ibrahim ZA, Chik Z, Mohamed Z, Ahmadiani A. Lipopolysaccharide pre-conditioning attenuates pro-inflammatory responses and promotes cytoprotective effect in differentiated PC12 cell lines via pre-activation of toll-like Receptor-4 signaling pathway leading to the inhibition of Caspase-3/nuclear factor-κappa B pathway. Front Cell Neurosci. 2021;14:–2020. doi:10.3389/fncel.2020.598453
182. Hu J, Huang K, Bao F, et al. Low-dose lipopolysaccharide inhibits spinal cord injury-induced neuronal apoptosis by regulating autophagy through the lncRNA MALAT1/Nrf2 axis. PeerJ. 2023;11:e15919. doi:10.7717/peerj.15919
183. Li W, Jiang D, Li Q, et al. Lipopolysaccharide–induced preconditioning protects against traumatic spinal cord injury by upregulating Nrf2 expression in rats. Life Sci. 2016;162:14–20. doi:10.1016/j.lfs.2016.08.008
184. Ochando J, Mulder WJM, Madsen JC, Netea MG, Duivenvoorden R. Trained immunity - basic concepts and contributions to immunopathology. Nat Rev Nephrol. 2023;19:23–37. doi:10.1038/s41581-022-00633-5
185. Sudduth ER, Trautmann-Rodriguez M, Gill N, Bomb K, Fromen CA. Aerosol pulmonary immune engineering. Adv Drug Deliv Rev. 2023;199:114831. doi:10.1016/j.addr.2023.114831
186. Möller W, Heimbeck I, Hofer TP, et al. Differential inflammatory response to inhaled lipopolysaccharide targeted either to the airways or the alveoli in man. PLoS One. 2012;7:e33505. doi:10.1371/journal.pone.0033505
187. McAuley DF, Laffey JG, O’Kane CM, et al. Simvastatin in the acute respiratory distress syndrome. N Engl J Med. 2014;371:1695–1703. doi:10.1056/NEJMoa1403285
188. Austelle CW, Cox SS, Wills KE, Badran BW. Vagus nerve stimulation (VNS): recent advances and future directions. Clin Auton Res. 2024;34:529–547. doi:10.1007/s10286-024-01065-w
189. Fang Y-T, Lin YT, Tseng WL, et al. Neuroimmunomodulation of vagus nerve stimulation and the therapeutic implications. Front Aging Neurosci. 2023;15:1173987. doi:10.3389/fnagi.2023.1173987
190. Zhang S, Zhao Y, Qin Z, et al. Transcutaneous auricular vagus nerve stimulation for chronic insomnia disorder: a randomized clinical trial. JAMA Network Open. 2024;7:e2451217. doi:10.1001/jamanetworkopen.2024.51217
191. Pavlov VA, Wang H, Czura CJ, Friedman SG, Tracey KJ. The cholinergic anti-inflammatory pathway: a missing link in neuroimmunomodulation. Mol Med. 2003;9:125–134.
192. Liu F-J, Wu J, Gong L-J, Yang H-S, Chen H. Non-invasive vagus nerve stimulation in anti-inflammatory therapy: mechanistic insights and future perspectives. Front Neurosci. 2024;18:1490300. doi:10.3389/fnins.2024.1490300
193. Wang X, Yang Z, Xue B, Shi H. Activation of the cholinergic antiinflammatory pathway ameliorates obesity-induced inflammation and insulin resistance. Endocrinology. 2011;152:836–846. doi:10.1210/en.2010-0855
194. Cremin M, Schreiber S, Murray K, Tay EXY, Reardon C. The diversity of neuroimmune circuits controlling lung inflammation. Am J Physiol Lung Cell Mol Physiol. 2023;324:L53–L63. doi:10.1152/ajplung.00179.2022
195. Wang W, Li R, Li C, Liang Q, Gao X. Advances in VNS efficiency and mechanisms of action on cognitive functions. Front Physiol. 2024;15:1452490. doi:10.3389/fphys.2024.1452490
196. Janssen HJB, Geraedts TC, Fransen LF, et al. Electrical vagus nerve stimulation is a promising approach to reducing pulmonary complications after an esophagectomy: an experimental rodent model. Immunol Res. 2024;72:1247–1258. doi:10.1007/s12026-024-09523-3
197. Li S, Qi D, Li J-N, Deng X-Y, Wang D-X. Vagus nerve stimulation enhances the cholinergic anti-inflammatory pathway to reduce lung injury in acute respiratory distress syndrome via STAT3. Cell Death Discov. 2021;7:63. doi:10.1038/s41420-021-00431-1
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.