")
Back to Journals » Research and Reports in Urology » Volume 12
Review of Testicular Tumor: Diagnostic Approach and Management Outcome in Africa
Authors Cassell A , Jalloh M , Ndoye M , Yunusa B, Mbodji M, Diallo A, Gaye O , Labou I, Niang L, Gueye S
Received 14 December 2019
Accepted for publication 11 February 2020
Published 18 February 2020 Volume 2020:12 Pages 35—42
DOI https://doi.org/10.2147/RRU.S242398
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jan Colli
Ayun Cassell,1 Mohamed Jalloh,1 Medina Ndoye,1 Bashir Yunusa,2 Mouhamadou Mbodji,1 Abdourahmane Diallo,1 Omar Gaye,1 Issa Labou,1 Lamine Niang,1 Serigne Gueye1
1Department of Urology and Andrology, Hopital General de Grand Yoff, Dakar, Senegal; 2Department of Surgery, Liberia College of Physicians and Surgeons, Monrovia, Liberia
Correspondence: Ayun Cassell
Department of Urology and Andrology, Hopital General de Grand Yoff, Dakar, Senegal
Tel +221770135805
Email [email protected]
Abstract: Testicular cancer is a common malignancy in young males with higher incidence in developed nations but with the lowest incidence in Africa (0.3– 0.6/100 000). Ironically, the global testicular cancer mortality rate has shown a reverse trend to its incidence with higher rates in low- and middle-income countries (0.5 per 100 000) than in high-income countries. Data from GLOBOCAN 2008 have shown relatively high mortality rates in sub-Saharan countries like Mali, Ethiopia, Niger and Malawi. The prognosis of testicular tumor is good with remarkable chemosensitivity to cisplatin-based regimen. Early diagnosis, careful staging and a multidisciplinary management approach is crucial to achieve this optimal result. These results are achievable in the sub-Saharan region if the relevant resources are appropriated for cancer care and clinical guidelines are formulated in a regional context.
Keywords: germ cell, orchidectomy, testicular cancer
Introduction
Testicular cancer is the commonest solid malignancy in young males.1 Testicular cancer (TC) accounts for 1% of all male cancer and 5% of urological malignancy.2 According to Albers et al the incidence of testicular cancer varies by ethnicity with higher incidence in high-income nations and lower in low-income countries.3 The global incidence has been rising steadily over the past decade.4 The highest incidence of TC was found in Norway (11.8/100 000) and lower in India (0.5 per 100 000) and Thailand (0.4/100 000).5 The exact incidence of testicular in sub-Saharan Africa is unknown but the incidence is lowest in Africa generally is estimated to range from (0.3–0.6/100 000).6 The global TC mortality rate has shown a reverse trend to its incidence with higher rates in low- and middle-income countries (0.5 per 100 000) than in high-income countries.7 Data from GLOBOCAN 2008 has shown relatively high mortality rates in Sub-Saharan countries like Mali, Ethiopia, Niger and Malawi. However, in absence of a national cancer registry, it is difficult to achieve the true incidence at a national level according to Znaor et al.7
Testicular dysgenesis syndrome (hypospadias, cryptorchidism, impaired spermatogenesis) has been substantiated as common risk factors for testicular cancer (TC). Evidence has shown that family history of testicular cancer in first degree relative and the presence of contralateral TC/Germ Cell Neoplasia in Situ (GCNIS) may increase the risk of testicular tumors.1–7
The predominant histological type is Germ Cell Tumor (90–95%) and 1–2% are found to be bilateral at diagnosis. Germ cell tumor are classified as either Seminoma, non-seminoma, teratoma and mixed tumors with the latter being considered as non-seminomas.1,3,5,8 This classification was based on biological, histological and practical reasons. The peak incidence for non-seminomatous tumor is in the third decade while pure seminoma peaks in the fourth decade.3 The risk of occult metastasis for stage I pure seminoma is low. Pure Seminoma is more chemo-sensitive and radio-sensitive compared to NSGCT. Other subtypes of NSGCT are embryonal carcinoma, choriocarcinoma, yolk sac tumor and teratoma. Teratoma is generally chemo-resistant and will require surgical resection. Alpha-Feto Protein (AFP) is produced by both embryonal carcinoma and yolk sac tumors.1,4 Choriocarcinoma and pure seminoma do not produce AFP; therefore, any pure seminoma with elevated AFP is considered a NSGCT. Beta-Human Chorionic Gonadotropin (Beta-HCG) are produced by both pure seminoma and NSGCT. The magnitude of Lactate dehydrogenase (LDH) elevation correlates directly with the tumor bulk. Though LDH is non-specific, it is generally used for prognostic assessment of germ cell tumor at diagnosis and risk stratification of patient with metastatic non-seminomatous germ cell tumor starting chemotherapy.1,4 The Lactate dehydrogenase-1 (LDH-1) isoenzyme is the most frequently elevated for germ cell testicular tumor.1
The prognosis of testicular tumor is good with remarkable chemosensitivity to cisplatin-based regimen.1,3,6,8,9 Early diagnosis, careful staging and a multidisciplinary management approach is crucial to achieve this optimal result. Nevertheless, poor prognosis non-seminomatous germ cell tumor will portend a poor overall survival (OS) and recommendation may be amenable to clinical trials.1,3
The aim of the study is to highlight published diagnostic and therapeutic approaches in the Sub-Saharan region and their impact on outcome in post-pubertal patients with reference to the current international guidelines. We envision that development of a regional guideline on TC and national cancer registry in these regions could be stimulated from this report.
Methodology
A literature review was conducted from 1998 to 2019 using PubMed, African Journal Online, Google and Google Scholar electronic databases. The search strategy included medical search heading (MEsH) and keywords using “Testicular Cancer” appended (Guidelines, Liberia, Senegal, Nigeria, Togo, Benin, Burkina, Ivory Coast, Gambia, Ghana, Mali). Results from the search term included more than 100 articles. Only 23 publications including clinical guidelines, prospective and retrospective studies were included. The Sub-Saharan literature (8 publications) were reviewed for patients’ demographics, study period, age parameters, diagnostic imaging, commonest presentation, commonest clinical staging using either the Tumor-Nodal-Metastasis (TNM) Staging or the Royal Marsden Staging System. The various histological types (germ cell tumors and stromal tumors), serum markers (Alpha-feto Protein, Beta-Human Chorionic Gonadotropin, Lactate dehydrogenase), management options and outcomes were also considered for review. A pooled analysis of some variables in (Tables 1 and 2) was performed as the rest of the data (Tables 1–3) were analyzed qualitatively and demonstrated in the main text of the results and discussion. All the guidelines and recommendations in the discussion are extrapolated from the American Urological Association (AUA) Guideline, European Association of Urologists (EAU) Guideline, National Comprehensive Cancer Network (NCCN) and the Canadian Urological Association (CUA) Guideline.
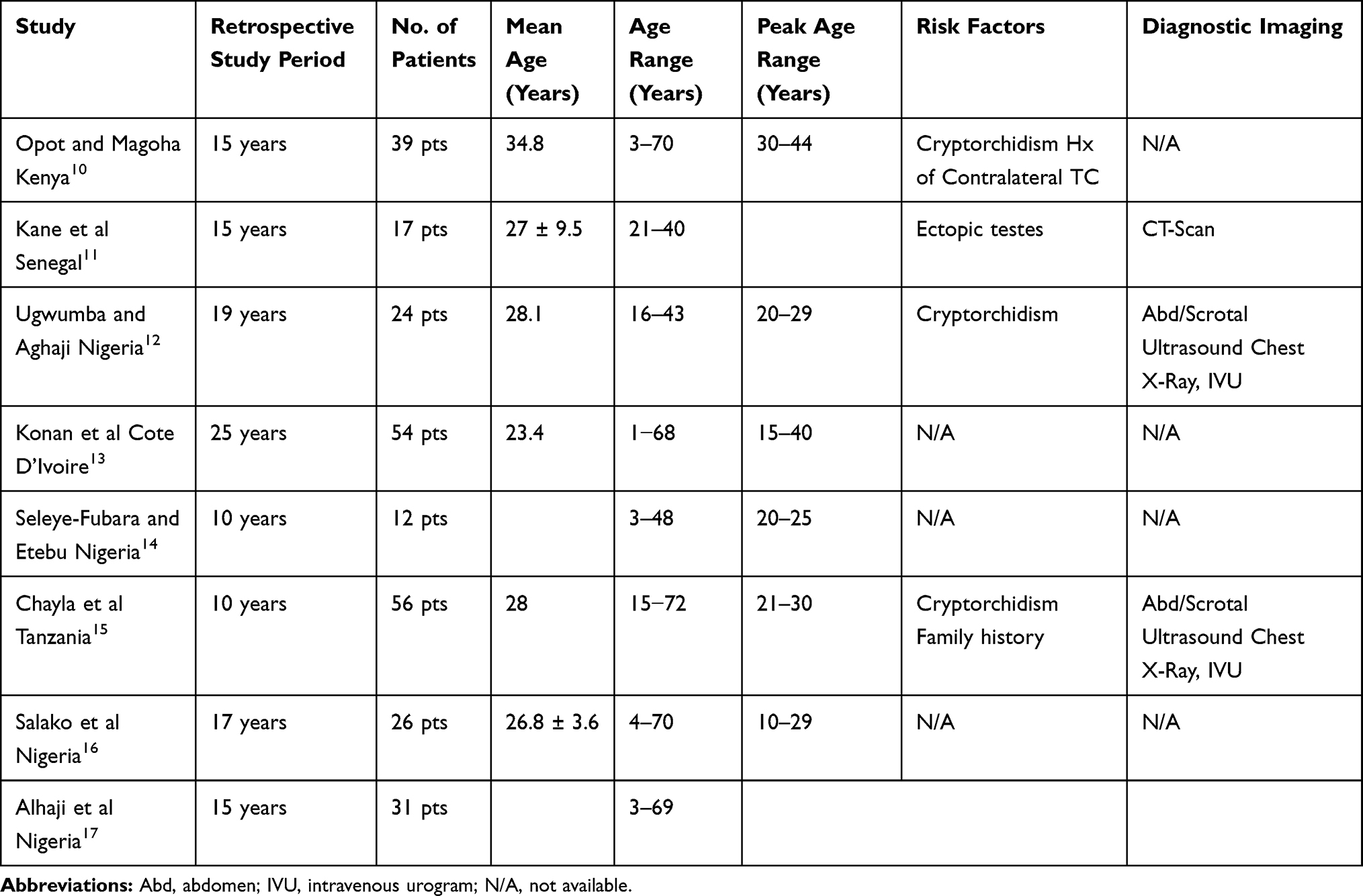 |
Table 1 Study Demographics, Age Parameters, Risk Factors and Diagnostic Imaging |
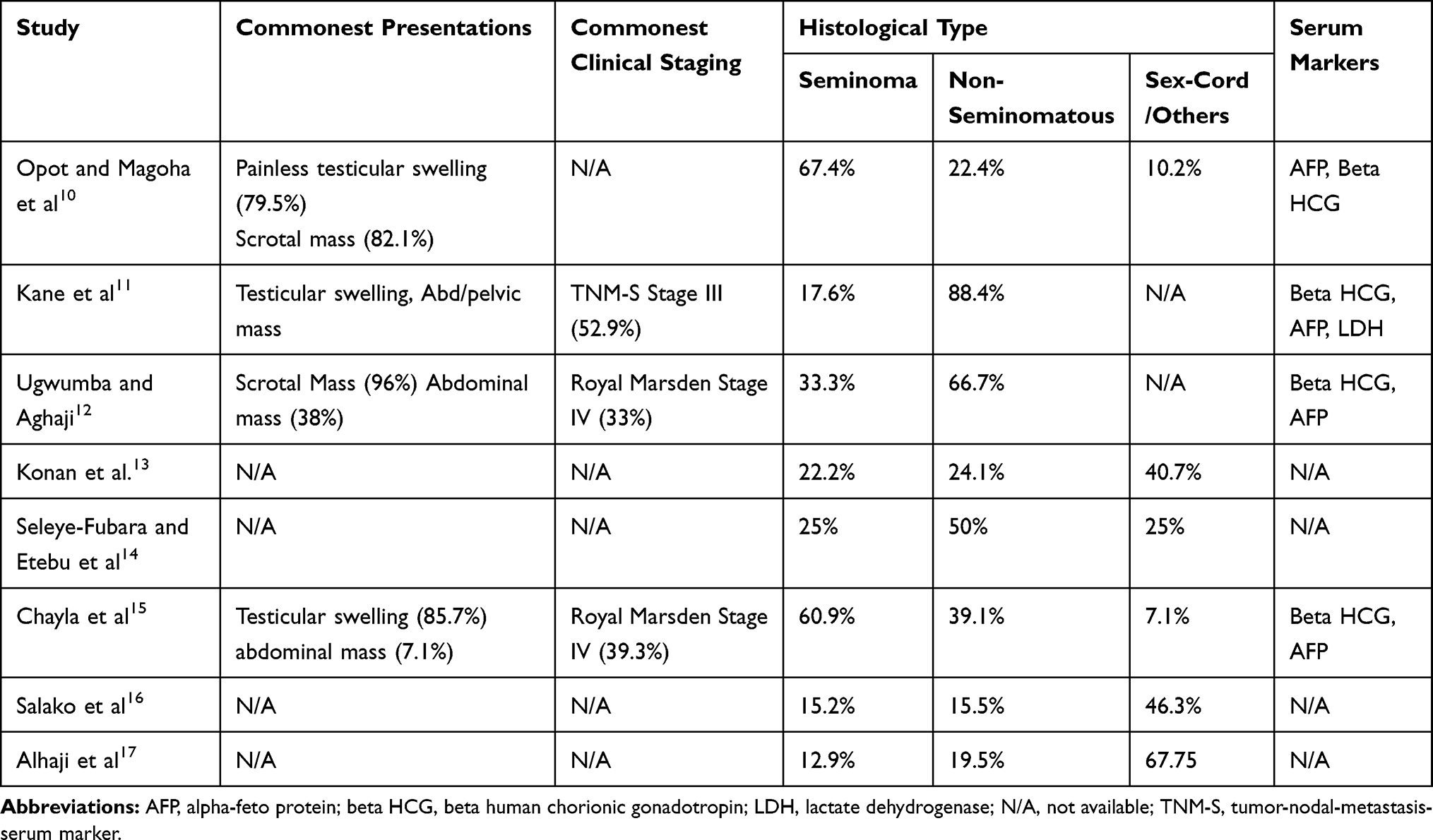 |
Table 2 The Clinical Presentation, Clinical Staging, Histological Types and Serum Markers |
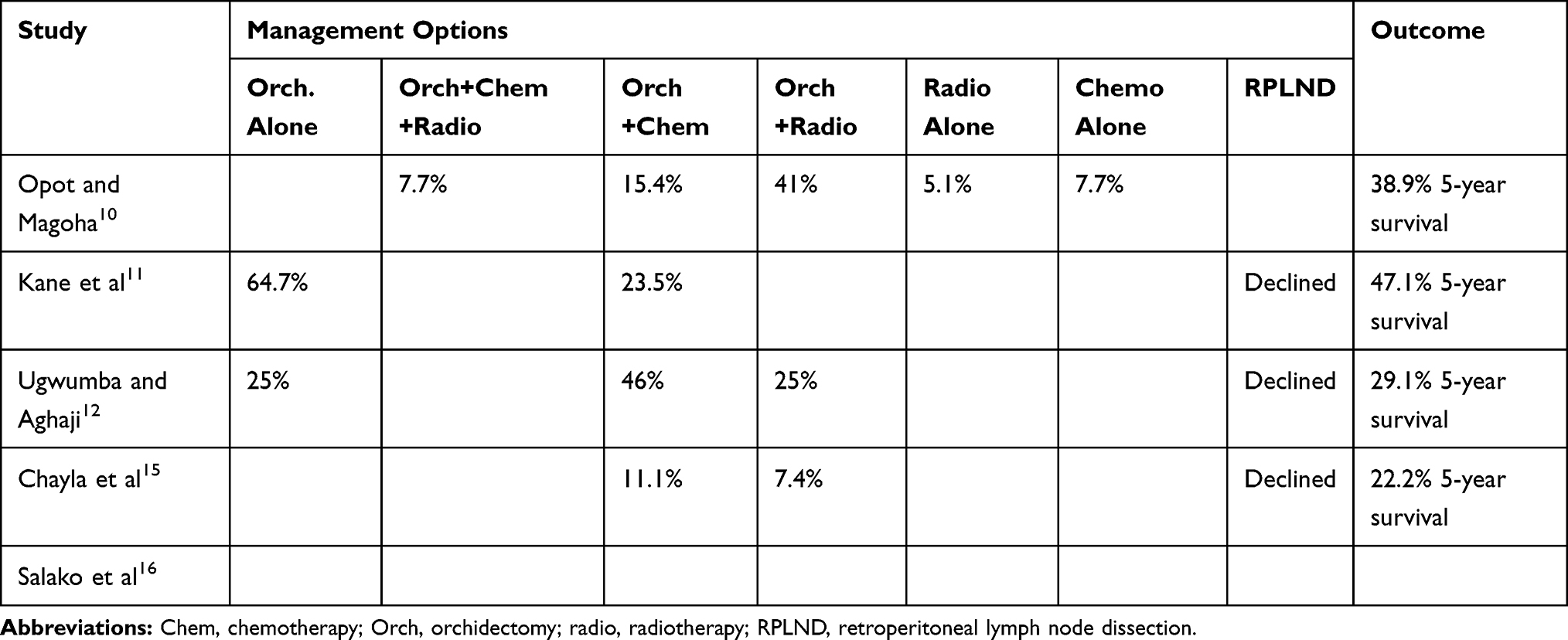 |
Table 3 Management Options and 5-Year Overall Survival of Patients with Testicular Cancer |
Evidence Synthesis
A total of 8 publications from the Sub-Saharan region were reviewed involving a total of 256 patients10–17 with testicular tumor cancer over an average of 15.8 years. The average age range varied from 1 to 70 years with a mean age of 28.1 years. However, the focus of the review has remained on the management of Germ Cell Testicular Cancer in postpubertal males. Cryptorchidism was common risk factors for testicular cancer amongst the publication followed by family history of testicular cancer and ectopic testes. Testicular swelling was the commonest symptom with some patients presenting with scrotal, abdominal or pelvic mass. Diagnostic Computed Tomography Scan (CT-Scan) was not available for clinical staging in most Sub-Saharan institutions except Senegal and Kenya. Most hospitals considered abdomino-scrotal ultrasound as an alternative for clinical staging to access retroperitoneal lymph node involvement and chest X-ray for pulmonary metastasis. Most studies did not report the clinical staging due to the study design and local resource challenge. However, Kane et al clinically staged the patients using the TNM Staging with the aid of testicular serum markers and CT-Scan where 52.9% presented as Stage III. The publications from Nigeria and Tanzania utilized the Royal Marsden Staging System with an average of 36.2% of patients presenting with stage IV testicular cancer. Germ Cell Tumor accounted for 84.2% of all testicular cancer with predominant seminomatous germ cell tumor at 46.8% whereas non-seminoma germ cell testicular cancer accounted for 37.4%. Other sex cord and stromal tumors were highlighted as well during the literature review. Studies by Opot et al, Kane et al, Ugwunba et al and Chayla et al showed that orchidectomy followed by adjuvant chemotherapy was a common treatment. Other treatment modalities included chemotherapy + radiotherapy, orchidectomy + Chemotherapy + radiotherapy, orchidectomy alone, chemotherapy alone or radiotherapy alone. No retroperitoneal lymph node dissection was performed as most patients decline the procedure.11,12,15 The average 5-year survival was 34.3% from four reviews.10–12,15
Discussion and Recommendation
The management of testicular cancer is based on a multidisciplinary team involving Urologist, medical oncologist, radio-oncologist, radiologist and pathologist. When treatment decision is being considered, the histological specimen should be reviewed by an expert pathologist. Over an average of 15.8 years, 256 patients were management for TC from 8 publications in the Sub-Saharan region.10–17 These were all retrospective studies with some limitations in diagnostic imaging, staging and treatment protocols. However, based on the AUA, EAU, CUA, NCCN guidelines,1,3,8 major recommendations were summarized against the available publications in the region. With adequate health financing and prioritization of uro-oncological pathologies, the management of germ cell testicular cancer can be treated in Africa with the latest global recommendation. The guideline recommendation of germ cell TC is relatively less expensive than treatment of other forms of urological cancer.18,19 Secondly, the overall prognosis of germ cell testicular tumor is good after treatment.1,3,8,9
Diagnosis Staging and Initial Management
During physical exam, any solid testicular mass discovered should be considered as testicular cancer until proven otherwise. The workup should include serum tumor markers (AFP, HCG and LDH) before any intervention including orchidectomy. Proper counseling about the possibility of infertility, testicular prothesis and sperm banking should be considered for patients with pathology of the contralateral testes.1–4 A trans-scrotal ultrasound with doppler is recommended for all patients with unilateral or bilateral scrotal mass.1–4,8 A radical inguinal orchidectomy is the standard initial management of suspicious testicular tumor and provides specimen for histological diagnosis.
Patients who are diagnosed newly of germ cell tumor with elevated serum tumor marker (AFP, HCG) should obtain a chest and abdominal computed tomography (CT-scan) for staging. However, a chest x-ray is preferred for stage I Seminoma patients compared to CT-scan.3,8,9 While chest CT-scan has a higher sensitivity to chest X-ray (100% versus 76%), chest X-ray has a superior specificity to Chest CT-scan.1 When testicular tumor markers are in normal range, the rate of skip metastasis is almost zero; therefore, the addition of a chest CT-scan is highly unlikely to alter treatment plan.
All patients should be staged according to the Tumor-Nodal-Metastasis-Serum Tumor Marker (TMN-S) staging. Regardless of age, any post-pubertal male with germ cell testicular tumor should be managed according to the adult guideline. Patient requiring chemotherapy for metastatic disease (stage IIc and III) should be stratified based on the International Germ Cell Cancer Collaborative Group (IGCCCG) which identified three prognostic groups: good, intermediate, and poor risk.1–4
Clinical stage I tumors are clinically confined to the testes, clinical stage II tumors involve the regional retroperitoneal lymph node while stage III tumors represents distant retroperitoneal lymph nodes, pulmonary as well as viscera metastasis. Elevated serum tumor markers have the propensity to upstage any stage of the disease.1,3,9 For example, rising post-orchiectomy levels of AFP in patient (with or without clinical evidence of metastases) may be appropriately managed as metastatic NSGCT.
A publication by Kane et al11 from Senegal involving 17 patients over 15 years reported full clinical staging with the use of trans-scrotal ultrasound, abdominopelvic CT-scan and serum tumor marker thus the TNM-S. Most other studies in the review from the Sub-Saharan region were limited by either the study design, the absence of CT-scan12,15 or serum tumor marker testing.13,14,16,17 As a result, the Royal Marsden Staging system was used by two studies12,15 with the aid of abdomino-scrotal ultrasound while other studies did not report a staging method.10,13,14,16,17 Abdominal scrotal ultrasound is nevertheless limited in assessing retroperitoneal lymph node except for relatively larger lymph nodes. This could induce a subsequent under staging of most testicular tumor in these settings.
Management of Stage I Seminoma
Surveillance after orchidectomy is preferred to adjuvant chemotherapy or radiotherapy. This is recommended to avoid unnecessary side effects of overtreatment with adjuvant carboplatin or radiotherapy as the cancer-specific survival is not better than surveillance.1–4
Management of Stage II Seminoma
Patients with stage IIA or IIB seminoma with lymph node <3 cm should receive adjuvant multiagent cisplatin-based chemotherapy or radiation therapy as the recurrence after both treatments is <10%. The radiation dose ranges from 30 GY to 35 GY to the paraaortic and ipsilateral pelvic nodes.1,8 The patient may require 4 cycles of etoposide and cisplatin (EP) or 3 cycles of bleomycin, etoposide and cisplatin (BEP). A CT-scan is performed 3 months after treatment to monitor treatment response. Treatment response to radiation and chemotherapy in this group is satisfactory.8 Patient should be counseled about the long-term side effects of radiation and chemotherapy could involve the cardiovascular, gastrointestinal and hematological system.
Management of Clinical Stage I Non-Seminoma Germ Cell Tumor
Approximately 30% of patients with clinical stage I NSGCT will have subclinical or occult metastasis. A shared decision-making with the patient about the advantages and disadvantages of (surveillance, adjuvant therapy and retroperitoneal lymph node dissection/RPLND) should be ascertained.1,3,8 Patient with Stage I disease and no lymphovascular invasion (LVI) can be offered surveillance if they can comply follow-ups. There is a 30% cumulative risk of relapse on surveillance; therefore, cisplatin-based adjuvant chemotherapy (with one course of cisplatin, etoposide, bleomycin BEP) and RPLND should be discussed with the patients. However, clinical stage I patients with LVI should receive one cycle of BEP adjuvant therapy according to current evidence.1,3,8 In case of a relapse 3 cycles of BEP are recommended. Patients with clinical stage I NSGCT with associated somatic malignancy (teratoma with malignant potential) should undergo RPLND because these tumors may differentiate into sarcomas that are chemo resistant.
Management of Clinical Stage II Non-Seminoma Germ Cell Cancer: Patients with clinical stage IIA with elevated serum tumor marker and stage IIB with or without elevated markers can benefit from adjuvant cisplatin-based chemotherapy.3,8,9 For stage IIA NSGCT with normal serum tumor marker can be offer surveillance after orchidectomy. Surveillance can continue for tumors that are shrinking. In the presence of a growing retroperitoneal mass and normal serum tumor marker, a teratoma should be suspected and an RPLND should be performed. Patients with Stage IIB NSGCT should undergo RPLND as the histological specimen almost always confirms testicular cancer. Two cycles of post-RPLND chemotherapy are advised due to high rates of relapse if a non-teratoma germ cell cancer is found in the surgical specimen.1 Stage IIB NSGCT is classified as good prognosis risk disease and the recommended chemotherapeutic regimen either 4 cycles of etoposide and cisplatin (EP) or 3 cycles of bleomycin, etoposide and cisplatin (BEP).1,8
Management of Metastatic Disease (Stage IIC and III) (2)
The management of advanced prostate cancer is based on the IGCCCG risk classification as good prognosis risk group, intermediate prognosis risk group and poor prognosis risk group. For good prognosis seminomatous germ cell tumor, the recommended treatment is 3 cycles of BEP or 4 cycles of EP.1–4,8,9 Intermediate seminomatous germ cell tumor should be managed with 4 cycles of BEP or etoposide, cisplatin, ifosfamide (VIP).20,21
The recommended treatment for good prognosis risk group – NSGCT is 3 cycles of BEP or 4 cycles of EP is bleomycin is contraindicated. The five-year survival for intermediate prognosis risk group NSGCT is about 80%. Four cycles of BEP are recommended as the standard treatment. The poor prognosis NSGCT as stratified by the IGCCCG risk classification has a five-year survival of 45% to 50%.18,19 The standard treatment guideline is 4 cycles of BEP.1–3,8,9 Patients who do not respond to first-line chemotherapy can receive high dose carboplatin + etoposide followed by autologous transplant or ifosfamide + paclitaxel followed by high dose etoposide with stem cell support as second-line therapy.4 A salvage resection may be anticipated if the recurrent mass is at an isolated site.
Amongst the 256 patients in the review of 8 Sub-Saharan publications with testicular cancer, germ cell tumor was the commonest 84.2% with non-seminomatous predominance. A few studies from the review10–12,15 outlined their various treatment modalities which included adjuvant chemotherapy (most common treatment), chemotherapy + radiotherapy, orchidectomy + Chemotherapy + radiotherapy, orchidectomy alone, chemotherapy alone or radiotherapy alone. No retroperitoneal lymph node dissection was performed as most patients decline the procedure10,11,14 which is much lower than the poor prognosis NSGCT as stratified by the IGCCCG risk classification (45% to 50%).
However, most these treatment options amongst the regional publications were not matched with their appropriate clinical staging. The average 5-year overall survival from 4 reports in the review of sub-Saharan literature was 34.3%.10–12,15 Cancer research and management remain a challenge in most developing nations as diagnostics and proper documentation make retrospective studies difficult to conduct. The need for improving oncological care and creating a cancer registry cannot be emphasized more.
Follow-Up
The primary objective of follow-up in the first year after treatment of TC is to identify relapse early and treat with curative intent.2,3,21 Follow-ups are individualized to the disease histology, stage, treatment option and response to treatment.1–4 Serum tumor markers, chest x-ray, abdominopelvic CT-scan or MRI are modalities used for monitoring patients treated form germ cell tumor.22 Follow-up after 5 years post-treatment of germ cell tumor is generally not recommended as relapse after this period is rare.
If radiation or chemotherapy was used as a treatment option for germ cell tumor, the patient is advised of the risk of cardiovascular disease and monitored for any component of metabolic syndrome.22,23 These include an active healthy lifestyle and the urgent need to strictly abstain from smoking to reduce their risk. They should also be counseled of the elevated risk of secondary malignancy. Periodic follow-up with their primary care physician is advised. If hypogonadism is observed during follow-up, an early morning serum testosterone test and luteinizing hormone levels can be measured. The risk of infertility is outstanding following orchidectomy + chemotherapy or radiotherapy; therefore, the possibility of semen preservation should be discussed with the patient.22,23
Challenges and Roadmap for Better Outcome of Cancer Care in Sub-Saharan Africa
The Africa continent is challenged by low income and a maigre health allocated budget; therefore, only a minute proportion of the population can afford health care The situation is worsened when these patients may require comprehensive cancer care which entails surgery, expensive chemotherapeutic agents and facilities for radiotherapy. Even, the lack of Urologist, Oncologist and Radiotherapist has been evident for the past decades in most parts of the continent. Reports have shown that only 3% of global drugs are produced in Africa and the rest are imported. A study by Stefan et al revealed that only Morocco and South Africa have managed to produce 70% to 80% of their drug they consume.24
The way forward to improve cancer care in the region is to involve all stakeholders including urologists, oncologists, radiologists, radiotherapists, oncological nurses, and psychotherapists to formulate or adopt a guideline on testicular cancer that is practical in low-income settings, but evidence based.
The African Organization for Research and Training in Cancer in 2012 launched the African Cancer Network Project with hopes to improve partnership amongst various organizations working for cancer control.25 There were approximately 102 cancer centers identified, but mostly located in South Africa. The partnership of National and International Cancer Associations along with local government to support comprehensive cancer care (surgery, chemotherapy, radiotherapy) is a crucial milestone to achieve. Pharmaceutical companies should be engaged for affordable pricing or better local production of essential chemotherapeutical agents. The push for national insurance schemes and financial security has to be emphasized.
Conclusion
Testicular cancer is common in young males and germ cell tumors are predominant histology. All testicular mass should be considered malignant until proven otherwise. Orchidectomy is useful for both treatment and staging. Relevant imaging and serum tumor marker should be used both for diagnosis staging and follow-up. Adjuvant Chemotherapy and radiotherapy are useful adjuncts as these tumors are both chemo-sensitive and radio-sensitive. The 5-year overall survival after treatment of localized testicular cancer is greater than 95%. These results are achievable in the Sub-Saharan region if the relevant resources are appropriated for cancer care.
Acknowledgment
Special thanks to the Department of Urology and Andrology.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Stephenson A, Eggener SE, Bass EB, et al. Diagnosis and treatment of early stage testicular cancer: AUA guideline. J Urol. 2019;20:10–97.
2. Laguna M.P, Albers P.Albrech W, et al. EAU guidelines on testicular cancer EAU; 2019. Available from: http://www.uroweb.org/guideline/testicular-cancer/.
3. Albers P, Albrecht W, Algaba FC. et al. EAU guidelines on testicular cancer, EAU; 2017:1–55. Available from: https://uroweb.org›wp-content›uploads›EAU-Guidelines-Testicular-C.
4. Gilligan T, Lin DW, Aggarwal R, et al. Testicular cancer, version 2.2020, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Ne. 2019;17(12):1529–1554. doi:10.6004/jnccn.2019.0058
5. Curado M, Edwards B, Shin H, et al. Cancer Incidence in Five Continents. Vol IX. IARC Scientific Pub. No. 160. Lyon, France: IARC Press; 2007.
6. Farmanfarma KK, Mahdavifar N, Mohammadian-Hafshejani A, Salehiniya H. Testicular cancer in the world: an epidemiological review. J Canc Res. 2018;5(4):1–5.
7. Znaor A, Lortet-Tieulent J, Jemal A, Bray F. International variations and trends in testicular cancer incidence and mortality. Eur Urol. 2014;65(6):1095–1106. doi:10.1016/j.eururo.2013.11.004
8. Wood L, Kollmannsberger C, Jewett M, et al. Canadian consensus guidelines for the management of testicular germ cell cancer. Can Urol Assoc J. 2010;4(2):e19. doi:10.5489/cuaj.815
9. Honecker F, Aparicio J, Berney D, et al. ESMO consensus conference on testicular germ cell cancer: diagnosis, treatment and follow-up. Ann Oncol. 2018;29(8):1658–1686. doi:10.1093/annonc/mdy217
10. Opot EN, Magoha GA. Testicular cancer at Kenyatta National Hospital. East Afr Med J. 2000;77(2):80–85.
11. Kane R, Zakou AR, Diao B, et al. Cancer du testicule: particularités cliniques et limites thérapeutiques en milieu hospitalier urologique au Sénégal. Afr J of Urol. 2014;20(3):149–153. doi:10.1016/j.afju.2014.04.003
12. Ugwumba FO, Aghaji AE. Testicular cancer: management challenges in an African developing country. S Afr Med J. 2010;100(7):452–455. doi:10.7196/SAMJ.3871
13. Konan PG, Dekou A, Kouame B, et al. Malignant testicular tumors in Côte d’Ivoire-anatomo-pathologic observations on 54 cases. Afr J of Urol. 2005;11(3):191–196.
14. Seleye-Fubara D, Etebu EN. Testicular tumors in port harcourt (a ten-year review). Niger J Clin Pract. 2004;7(2):56–59.
15. Chalya PL, Simbila S, Rambau PF. Ten-year experience with testicular cancer at a tertiary care hospital in a resource-limited setting: a single centre experience in Tanzania. World J Surg Oncol. 2014;12(356):1–8. doi:10.1186/1477-7819-12-356
16. Salako AA, Onakpoya UU, Osasan SA, Omoniyi-Esan GO. Testicular and para-testicular tumors in south western Nigeria. Afr Health Sci. 2010;10(1):14–17.
17. Alhaji SA, Abdulkadir A, Sanusi HM. A 15-year pathologic review of testicular and para-testicular tumours in Kano, Northern Nigeria. Nigerian J of Basic and Clin Sci. 2016;13(2):114–118. doi:10.4103/0331-8540.187360
18. Cassell A, Yunusa B, Jalloh M, et al. A review of localized prostate cancer: an African perspective. World J Oncol. 2019;10(4–5):162–168. doi:10.14740/wjon1221
19. Cassell A, Yunusa B, Jalloh M, et al. Non-muscle invasive bladder cancer: a review of the current trend in Africa. World J Oncol. 2019;10(3):123–131. doi:10.14740/wjon1210
20. Thibault C, Fizazi K, Barrios D, et al. Compliance with guidelines and correlation with outcome in patients with advanced germ-cell tumours. Eur J Cancer. 2014;50(7):1284–1290. doi:10.1016/j.ejca.2014.01.026
21. Beyer J, Bokemeyer C. Chemotherapy for germ cell cancer. Urologe A. 2004;43(12):1507–1513. doi:10.1007/s00120-004-0704-5
22. Beyer J, Albers P, Altena R, et al. Maintaining success, reducing treatment burden, focusing on survivorship: highlights from the third European consensus conference on diagnosis and treatment of germ-cell cancer. Ann Oncol. 2013;24:878–888. doi:10.1093/annonc/mds579
23. Cathomas R, Hartmann M, Krege S, et al. Interdisciplinary evidence-based recommendations for the follow-up of testicular germ cell cancer patients. Onkologie. 2011;34(1–2):59–64. doi:10.1159/000323346
24. Cassell A, Yunusa B, Jalloh M, et al. Management of advanced and metastatic prostate cancer: a need for a Sub-Saharan guideline. J Oncol. 2019;2019:1–9. doi:10.1155/2019/1785428
25. Stefan DC. Cancer care in Africa: an overview of resources. J Glob Oncol. 2015;1(1):30–36. doi:10.1200/JGO.2015.000406
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.