Back to Journals » Infection and Drug Resistance » Volume 19
Retrospective Study of Pathogen Distribution and Antimicrobial Resistance in 283 Neonates with Bloodstream Infections at a Grade-A Tertiary Hospital in China, 2021–2024
Authors Zhang M, Xia X, Xu M ![]() , Song D, Pan Y, Liang Z
, Song D, Pan Y, Liang Z ![]() , Wang Z
, Wang Z
Received 19 April 2026
Accepted for publication 31 May 2026
Published 11 June 2026 Volume 2026:19 616647
DOI https://doi.org/10.2147/IDR.S616647
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Sandip Patil
Manhui Zhang,1 Xian Xia,1 Mengjiao Xu,2 Danning Song,1 Yue Pan,1 Zhengtong Liang,3 Zhigang Wang1
1Department of Disease Control and Prevention, The Seventh Medical Center of Chinese PLA General Hospital, Beijing, 100700, People’s Republic of China; 2Institute of STD/AIDS Control, Prevention and Research, Sichuan Center for Disease Control and Prevention, Chengdu, Sichuan, 610041, People’s Republic of China; 3Capital Medical University, Beijing, 100069,People’s Republic of China
Correspondence: Zhigang Wang, Email [email protected]
Objective: To characterize pathogen distribution and antimicrobial resistance among neonates with bloodstream infections at a Grade-A tertiary medical center in China.
Methods: This retrospective study reviewed clinical data, culture results, and antimicrobial resistance information from neonates admitted between January 2021 and December 2024. Clinical specimens were collected in accordance with standard protocols for culture. Antimicrobial susceptibility testing was performed using an automated microbial identification system, with results interpreted according to the CLSI standards of the corresponding testing year.
Results: Of 652 neonates admitted within 3 days of life, 283 had blood-culture-proven bloodstream infection; blood-culture positivity was 22.65%. Common bloodstream isolates included Staphylococcus epidermidis and Klebsiella pneumoniae. Staphylococcus epidermidis showed high resistance to penicillin, oxacillin, cefoxitin, and erythromycin, whereas Klebsiella pneumoniae was frequently resistant to cefepime and piperacillin-tazobactam. Among 290 blood-culture isolates, 161 (55.52%) were Gram-positive bacteria, including 109 MDR isolates (67.70%), and 122 (42.07%) were Gram-negative bacteria, including 32 MDR isolates (26.23%). Preterm infants, low-birth-weight infants, and late-onset bloodstream infections accounted for large proportions of the cases.
Conclusion: Local surveillance of pathogen distribution and resistance patterns can support antimicrobial stewardship and infection prevention in neonatal care.
Keywords: neonate, bloodstream infection, pathogen, drug resistance
Healthcare-associated infections (HAIs) remain a severe and widespread threat to in-patient health despite the continuous implementation of multidimensional intervention strategies worldwide. They affect clinical outcomes and patient prognosis and impose a substantial economic burden, further increasing pressure on healthcare systems.1,2 Neonates, particularly preterm infants, are at higher risk of infection than adults because of immune immaturity. Among very low birth weight (VLBW) neonates, HAI rates can exceed 30%.3–6 This vulnerability is related to insufficient maternal antibody transfer, overall immune immaturity,7 compromised skin integrity, prolonged hospitalization, frequent invasive procedures, and the need for long-term broad-spectrum antibiotics and parenteral nutrition.8–10
As the overall level of neonatal care continues to improve, the survival rates of low birth weight and low birth age neonates have increased, whereas the incidence and mortality rates of neonatal bloodstream infections have also shown a gradual upward trend. Healthcare-associated bloodstream infections are the leading causes of infection-related neonatal mortality, particularly in low-birth-weight and severely ill neonates.11 A study7 from the United States revealed that the incidence of early-onset bloodstream infections was 0.98 per 1,000 live births in a national follow-up of approximately 400,000 infants,and among those surviving beyond 3 days, about 21% developed bloodstream infections after 3 days, with an overall mortality rate of 16% in those infected infants.
Globally and regionally, neonatal bloodstream infections remain an important contributor to neonatal morbidity and mortality, particularly among preterm and low-birth-weight infants. Published surveillance studies from different regions show substantial variation in bloodstream-infection incidence, pathogen spectrum, mortality, and antimicrobial resistance, underscoring the need for local data to guide empirical therapy and infection prevention.11–14 In China and East Asia, recent reports have highlighted Coagulase-negative staphylococci (CoNS), Klebsiella pneumoniae, Escherichia coli, and carbapenem-resistant or multidrug-resistant Gram-negative bacteria as clinically important neonatal bloodstream pathogens.13–15
In recent years, with the widespread use and abuse of antibiotics, the drug resistance of bacteria has become an increasingly severe issue. The emergence of multidrug-resistant (MDR) strains has rendered conventional antibiotic therapies gradually ineffective.16 Studies17 indicate that MDR strains exhibit significantly increased resistance to multiple antibiotics, including cephalosporins, aminoglycosides, quinolones, and carbapenems, severely limiting effective treatment options and leading to higher mortality rates and prolonged hospital stays.
Therefore, because recent local surveillance data are needed to clarify pathogen distribution, resistance patterns, and the clinical context of neonatal bloodstream infections in Chinese tertiary care settings, this study retrospectively analyzed clinical data from neonates admitted within 3 days of birth at a Grade-A tertiary medical center between January 2021 and December 2024. The aim was to describe the distribution of bloodstream pathogens and their antimicrobial resistance patterns and to provide evidence that may support antimicrobial selection, antimicrobial stewardship, and infection-prevention strategies in neonatal care.
Subjects and Methods
Object
For the analysis of pathogen detection rates across specimen types, 652 neonatal patients admitted to the Grade-A tertiary medical center from January 1, 2021, to December 31, 2024, were included. The inclusion criteria were: ①admission within 3 days of birth; and ②at least one bacterial, fungal, or mycoplasma culture result during hospitalization.
For the analysis of neonatal bloodstream infections, 283 of the 652 neonates were included because they had a bloodstream-infection diagnosis, blood-culture results, complete birth information, and available medical records. Patient-level analyses used one bloodstream-infection episode per neonate. For isolate-level analyses, the first detection of the same pathogen in a patient was included; repeated detections of the same pathogen were excluded, whereas a subsequently detected different microorganism in the same patient was included as a distinct isolate. This rule yielded 290 isolates from 283 patients.
This retrospective study was approved by the Medical Ethics Committee of the Seventh Medical Center of Chinese PLA General Hospital (approval number: S2026-050-01) and was conducted in accordance with the Declaration of Helsinki. The Ethics Committee approved this retrospective analysis of anonymized clinical data and waived the requirement for written informed consent.
Data Collection
Clinical data were collected through the electronic medical record system, including sex, gestational age, birth weight, number of fetuses, and hospital admission time. The hospital infection-information monitoring system was used to collect microbiological testing data during hospitalization, including specimen type, detection time, pathogen culture results, and antimicrobial resistance results. All clinical specimens, including peripheral blood, sputum, and sterile body fluids such as cerebrospinal fluid, pleural effusion, ascites, and pus, were cultured for bacterial isolation using Thermo Fisher Oxoid series media. Purified single colonies were identified using the bioMérieux VITEK 2 Compact automated microbial identification system and compatible identification cards. Antimicrobial susceptibility testing was performed using the same bioMérieux VITEK 2 Compact platform and compatible susceptibility cards. Results during the study period were interpreted according to the CLSI standards current in the corresponding test year. Specimen collection, transport, cultivation, and antimicrobial resistance testing were conducted in accordance with relevant Chinese clinical and laboratory standards, including WS/T 640–2018 Specimen collection and transport in clinical microbiology and WS/T 805–2022 Basic technical standards for clinical microbiological laboratory.
Neonatal bloodstream infection was defined according to the Chinese neonatal sepsis diagnostic guidance and relevant neonatal-sepsis literature as a positive blood culture in a neonate with compatible clinical evaluation after exclusion of contamination. Because this study focused on microbiologically confirmed bloodstream infection, culture-positive cases were included after contaminant isolates were excluded. Laboratory personnel communicated with clinicians during specimen processing and result review; isolates judged to represent contamination were excluded before analysis. MDR was defined as resistance to at least one agent in each of three or more clinically used antimicrobial categories.
Statistical Methods
The data in this study were analyzed and processed using SAS 9.4. Measurement data were reported as mean±standard deviation (SD) or median (interquartile range), and were tested for comparison in univariate analysis using the Wilcoxon test. Categorical data were presented as case numbers or counts (n) and percentages (%), and were tested for comparison in univariate analysis using the chi-square test (likelihood ratio chi-square test). The significance levels were all set at α=0.05.
Results
Positive Detection Rate of Pathogenic Microorganisms in Neonatal Patients
A total of 6,639 samples, including blood, throat swabs, cerebrospinal fluid, sputum, and other specimens, were collected from 652 neonates. Of these samples, 1,895 were positive for pathogenic microorganisms, yielding an overall detection rate of 28.54% (Table 1). Positive-versus-sterile culture outcomes differed significantly across specimen types (chi-square = 843.659, df = 10, P < 0.001). Among the positive samples, 565 strains of Gram-positive bacteria (29.82%), 836 strains of Gram-negative bacteria (44.12%), 43 strains of fungi (2.27%), and 451 strains of mycoplasma (23.80%) were detected. The positive detection rate of pathogens in blood cultures was 22.65%, which remained relatively low among all types of specimens. Among the positive cultures, a total of 272 strains of Gram-positive bacteria (12.20%), 211 strains of Gram-negative bacteria (9.46%), and 22 strains of fungi (0.99%) were isolated.
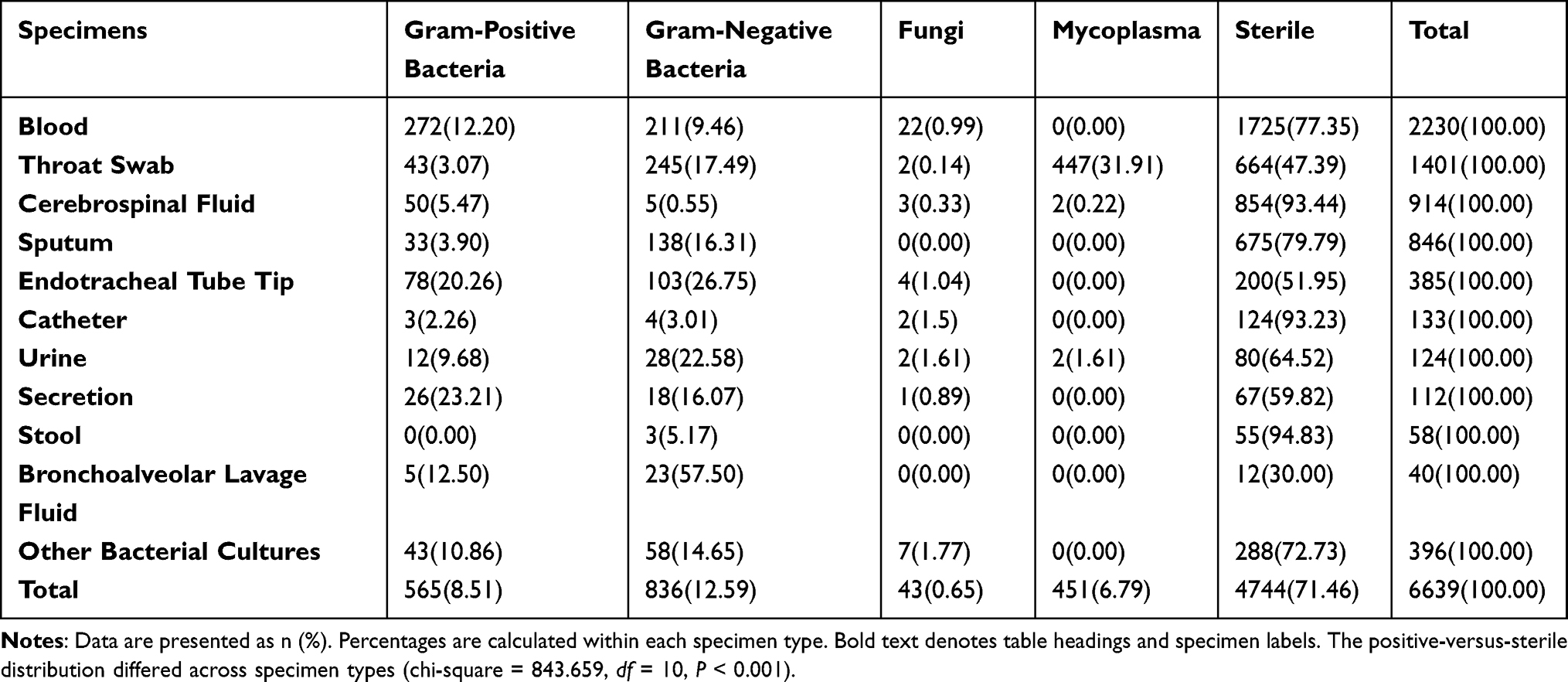 |
Table 1 Positive Detection Rates of Pathogenic Microorganisms from Different Specimen Types in Neonates [n (%)] |
Drug Resistance Characteristics of Pathogens in Blood Stream Infection
Results are reported at both patient and isolate levels. Patient-level summaries describe the 283 neonates with bloodstream infections. Isolate-level pathogen and resistance summaries describe 290 distinct blood-culture isolates recovered under the first-detection reporting rule: repeated detection of the same pathogen in the same patient was excluded, whereas a different microorganism detected later in the same patient was included as a distinct isolate.
At the patient level, 171 of 283 neonates (60.42%) were male and mean birth weight was 1803.15±935.34 g. Preterm infants comprised 81.27% (n = 230) of the enrolled neonates, including 21.55% (n = 61) extremely low birth weight infants, 23.67% (n = 67) very low birth weight infants, and 25.44% (n = 72) low birth weight infants. Small for gestational age was observed in 12.01% of the study population. Early-onset and late-onset infections accounted for 22.26% (n = 63) and 77.74% (n = 220), respectively.
At the isolate level, 161 of 290 bloodstream isolates were Gram-positive bacteria; 109 of these 161 Gram-positive isolates were MDR (67.70%) (Table 2). CoNS, including Staphylococcus epidermidis, Staphylococcus hominis subsp. hominis, Staphylococcus capitis, and Staphylococcus haemolyticus, showed MDR rates above 90% within the corresponding species groups. Among 122 Gram-negative isolates, 32 were MDR (26.23%). Seven isolates were fungi and none was classified as MDR.
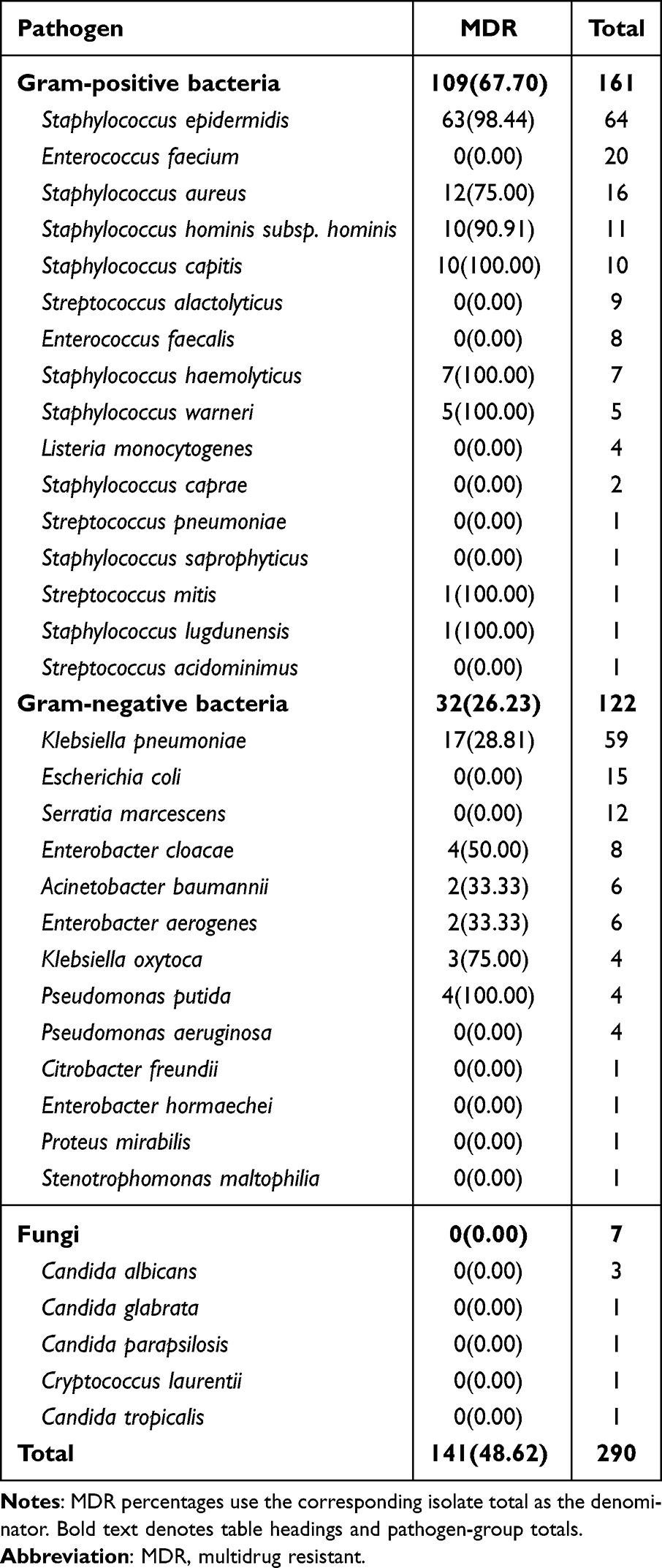 |
Table 2 Multidrug Resistance Patterns of Blood-Culture Isolates |
The predominant Gram-positive pathogens demonstrated variable resistance patterns (Table 3). Staphylococcus epidermidis was highly resistant to penicillin (100.00%), oxacillin (98.44%), and cefoxitin (98.44%), but remained susceptible to linezolid, tigecycline, and vancomycin (no resistance detected). Staphylococcus aureus showed complete resistance to penicillin (100.00%) and high resistance to erythromycin (81.25%), while maintaining low resistance to gentamicin, tigecycline, and vancomycin. Staphylococcus hominis subsp. hominis exhibited resistance to cefoxitin, penicillin, and erythromycin in over 90% of isolates, with preserved susceptibility to tigecycline and vancomycin. Staphylococcus capitis was resistant to oxacillin, penicillin, cefoxitin, and levofloxacin; conversely, tetracycline, tigecycline, and vancomycin demonstrated potential therapeutic efficacy.
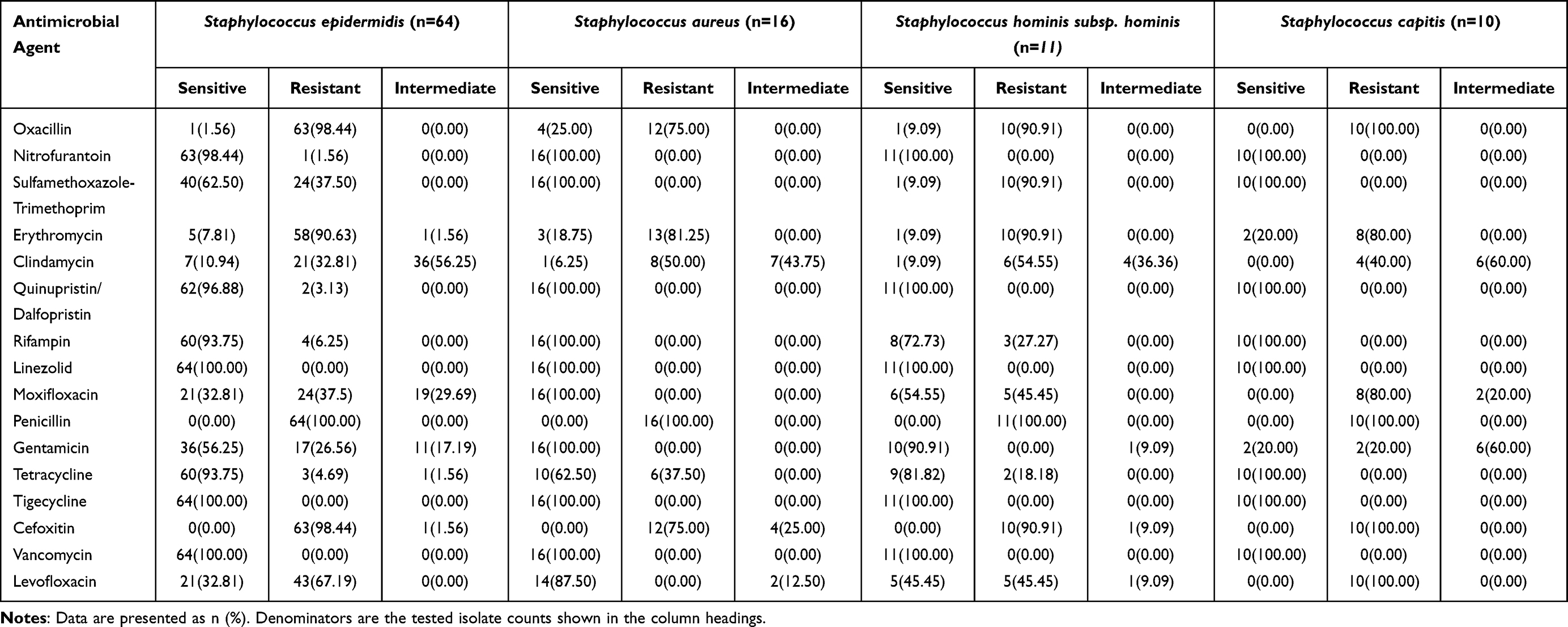 |
Table 3 Resistance Characteristics of Selected Gram-Positive Bacteria [n (%)] |
The predominant Gram-negative pathogen, Klebsiella pneumoniae, exhibited high resistance to cefepime (76.27%) and piperacillin-tazobactam (>50%), but retained susceptibility to amikacin, tobramycin, and levofloxacin (Table 4).
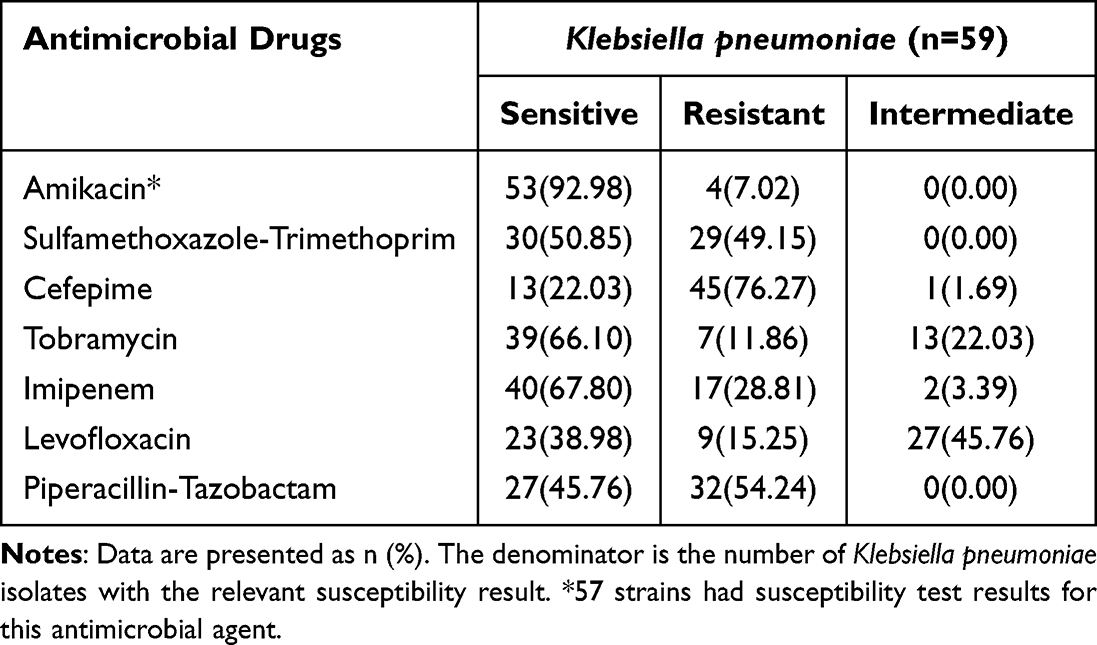 |
Table 4 Resistance Characteristics of Selected Gram-Negative Bacteria [n (%)] |
Demographic Characteristics of Neonates with Bloodstream Infections Caused by Major Pathogenic Bacteria
In this study, pathogenic microorganisms detected in blood cultures with 10 or more strains were defined as major pathogens, including 5 species of Gram-positive bacteria and 3 species of Gram-negative bacteria. We analyzed the demographic characteristics of neonatal patients with bloodstream infections caused by major pathogenic bacteria. Significant differences (P < 0.05, Table 5) were observed among the different pathogens in terms of gestational age classification, birth weight, detection time, gestational weeks, and Apgar scores at 1 and 5 minutes. The bloodstream infections predominantly occurred in preterm infants and low birth weight infants. Pathogens detected 3 days after birth accounted for a large proportion, among which infections caused by Staphylococcus capitis and Serratia marcescens were exclusively late-onset. In contrast, infections caused by Escherichia coli demonstrated a relatively large proportion of early-onset cases (46.67%).
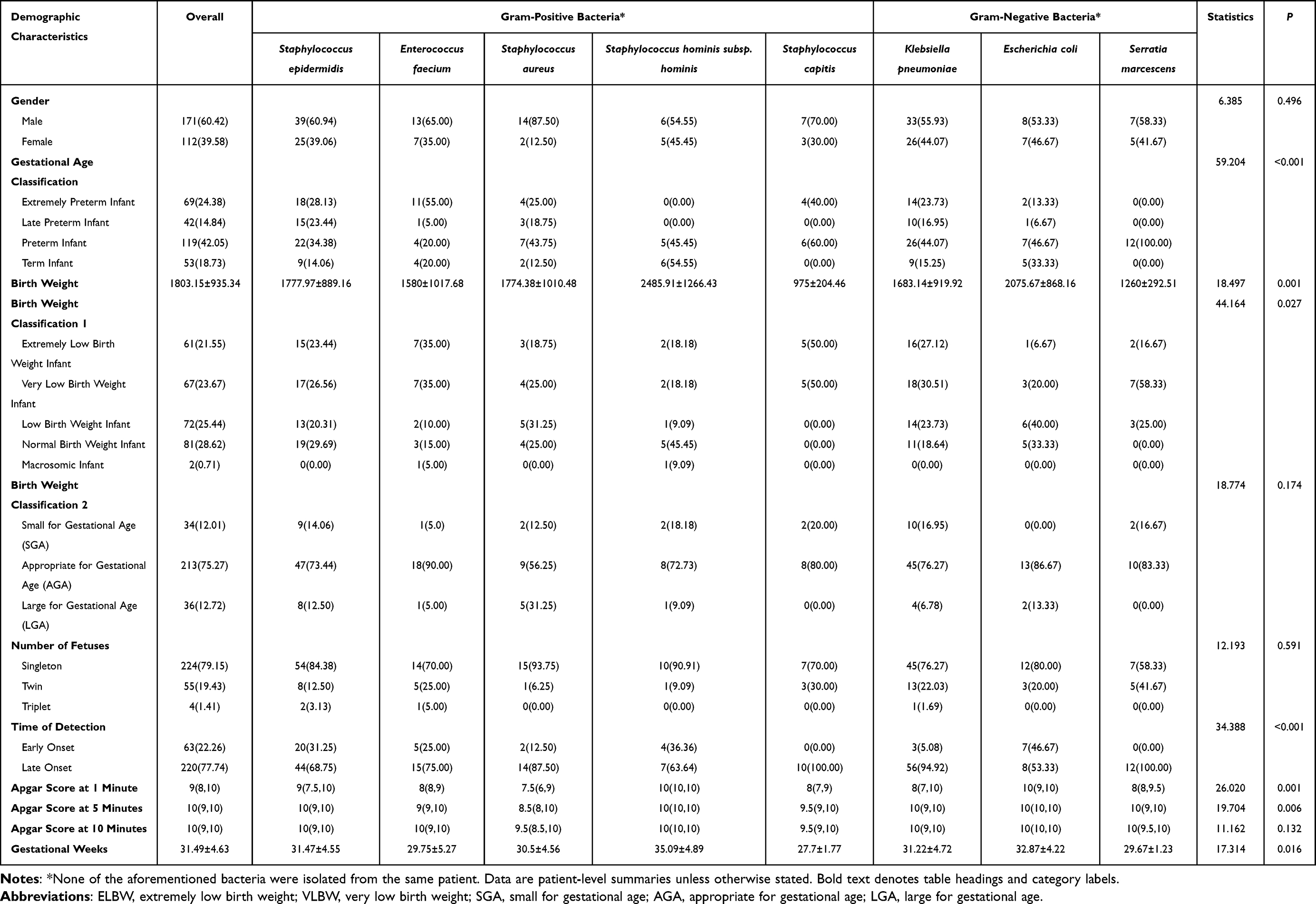 |
Table 5 Demographic Characteristics of Neonates with Major Bloodstream-Infection Pathogens |
Discussion
Neonatal bloodstream infections are one of the leading causes of hospitalization and mortality in newborns. When such infections are attributed to maternal or neonatal treatment or care, they are considered neonatal healthcare-associated infections.18 Healthcare-associated bloodstream infections in neonates can be classified as early-onset and late-onset infections. The definition of early-onset infection varied across many studies, with most researchers defining it as detected positive in a culture of body fluids or site specimens sampled on the 3rd, 7th, or 10th day postpartum. However, in studies on healthcare-associated infections, the optimal sampling time is on the 3rd day postpartum.19 In our study, late-onset infections accounted for 220 cases (77.74%), which was 3.5 times higher than early-onset infections.
Early-onset infections are generally associated with vertical transmission, which may occur through blood-borne transmission or, more commonly, via ascending transmission through the genital tract. The majority of pathogenic microorganisms that cause early-onset infections originate from the maternal body and can be transmitted through the birth canal in several hours preceding or during delivery. Neonates diagnosed with early-onset infections may exhibit a medical history of premature rupture of membranes, preterm birth, chorioamnionitis, or puerperal pyrexia.20 In term infants, the predominant pathogen of early-onset infection is Group B Streptococcus (GBS), whereas in preterm infants it is Escherichia coli.20 In our study, E. coli represented the highest proportion (46.67%) among pathogens causing early-onset infections. Guidelines21 recommend implementing risk assessment tools to identify infants who truly require antibiotic therapy, thereby minimizing unnecessary antibiotic exposure and reducing the risk of antimicrobial resistance and healthcare-associated infections.
Late-onset infections are defined as infections that occur after the 3rd day of birth, caused by pathogenic microorganisms acquired during medical procedures. Late-onset bloodstream infections accounted for a significant proportion in our study. These infection are often associated with factors such as preterm birth, low birth weight, prolonged use of intravascular access, mechanical ventilation, parenteral nutrition, and exposure to broad-spectrum antibiotics.22,23 This finding was most evident in preterm infants, accounting for the predominance of late-onset infections in our study, which likely reflects the high proportion of preterm neonates enrolled. They are one of the important causes of morbidity and mortality in extremely preterm infants and are associated with a higher risk of adverse outcomes such as poor neurodevelopment.24 The distribution of pathogens causing neonatal sepsis varies by geographic region and socioeconomic development. In developed high-income countries, CoNS account for over 50% of late-onset sepsis cases, followed by Gram-negative bacteria such as Escherichia coli and Klebsiella pneumoniae; whereas in low- and middle-income countries, Gram-negative bacteria and fungal infections constitute a significantly higher proportion.12 In addition to bacterial infections, fungal infections (predominantly Candidiasis) represent a major cause of late-onset sepsis, particularly among VLBW infants with high mortality rates.12 In neonatal intensive care units (NICUs) with high rates of fungal infections, prophylactic antifungal agents are recommended. A systematic review demonstrated that prophylactic fluconazole administration reduces the risk of invasive Candidiasis.25 The 2016 Infectious Diseases Society of America (IDSA) guidelines recommend prophylactic fluconazole, administered either intravenously or orally, for infants with birth weight <1000g who are admitted to NICUs with high baseline rates of invasive Candidiasis (>10%).26
Extremely low birth weight (ELBW) and VLBW neonates are also susceptible to infections due to immature immune systems, prolonged hospitalization, and the need for invasive diagnostic and therapeutic procedures.27 Low birth weight infants are associated with lower gestational age, immature immune system development, and often require more frequent intravenous infusions, medications, and parenteral nutrition, making them more susceptible to invasive procedures such as endotracheal intubation and central venous catheterization. These factors collectively render them more vulnerable to infection risks compared with their higher birth weight peers.28 The risk factors of these infections can be modified by measures such as breastfeeding, enhanced hand hygiene, catheter care bundles, and antimicrobial stewardship to reduce the incidence of neonatal bloodstream infections29 and serve as a cost-effective breakthrough in infection prevention and control in NICUs.
In our study, the positive detection rate of pathogenic microorganisms in blood cultures (22.65%) was lower than the overall positive detection rate in all types of specimen cultures (28.54%). Other studies have demonstrated that the positive rates of pathogenic microorganisms in blood cultures vary across different studies, ranging from 10.29% to 28.00%,30–33 which are basically consistent with the results in our study. According to international standard guidelines, blood collection volume for infants and children should follow the manufacturer’s instructions for blood culture bottles, with the maximum feasible volume collected, generally equivalent to 1% of the neonatal body weight. The yield of blood culture depends on the volume of blood cultured; in adults, the detection rate increases by approximately 3% per additional milliliter of blood cultured.34 The relatively low positive detection rates in blood cultures across many studies, with the majority of clinically suspected cases yielding culture-negative results, may be attributed to the relatively thin blood vessels and insufficient blood volumes of neonates, thereby making blood sampling more challenging. Additionally, factors such as the timing of blood sampling, the time of sample submission, and the interpretation of results may also influence the positive detection rates of pathogenic microorganisms in blood cultures, resulting the diagnostic challenges of neonatal bloodstream infections. Despite these limitations, blood culture remains the gold standard for confirming neonatal bloodstream infections. Total blood culture volume and sampling before the use of antibiotics are critical factors affecting the positive detection rate of pathogenic microorganisms in blood culture.35 However, due to the insufficient blood volumes and critical medical conditions of neonates, it is difficult to collect sufficient blood samples to improve blood culture sensitivity. Therefore, enhancing the sensitivity of blood culture and implementing auxiliary screening tests are necessary.
Among the cultured bloodstream isolates, Gram-positive bacteria were the most frequently detected, totaling 161 isolates (55.52%), while Gram-negative bacteria accounted for 122 isolates (42.07%), consistent with related research findings.36 An international neonatal and pediatric bloodstream-infection study also emphasized that pathogen distribution and antimicrobial resistance patterns vary by setting and should inform local empirical-treatment and stewardship decisions.37 Although the proportion of Gram-negative bacteria remained lower than that of Gram-positive bacteria in this study, the observed distribution may reflect differences in reservoirs, transmission pathways, case mix, and laboratory ascertainment and requires further study.38,39
Among the detected Gram-positive bacteria in our study, CoNS accounted for 62.73% of Gram-positive isolates, which is consistent with existing research findings.40 This may be related to the increased number and survival rate of ELBW infants, as well as the widespread use of intravascular devices in high-risk neonates.19 Specifically, Staphylococcus epidermidis was the most frequently detected species (39.75% of Gram-positive isolates), consistently ranking first in neonatal blood cultures and exceeding other pathogens. In a retrospective study by Zhang et al13 on neonatal bloodstream infections from 2016 to 2020 at a hospital, Staphylococcus epidermidis accounted for 31.26% of all isolated bacteria, ranking first among Gram-positive bacteria. Because CoNS can represent either clinically significant infection or blood-culture contamination, interpretation of these findings should be linked to the study’s diagnostic and contamination-control criteria. Staphylococcus epidermidis is common on human skin and mucosal surfaces and may act as an opportunistic infectious agent in NICUs under conditions such as device-associated biofilm formation, antibiotic selection pressure, and host immune immaturity.41 This study found that 98.44% of Staphylococcus epidermidis isolates were MDR, with resistance rates to penicillin, oxacillin, cefoxitin, and erythromycin of 100.00%, 98.44%, 98.44%, and 90.63%, respectively, while no resistance to linezolid, tigecycline, or vancomycin was detected. In addition, Staphylococcus aureus remains a serious pathogen causing neonatal bloodstream infections. Studies42 have shown that approximately 2% of bloodstream infections in ELBW infants are caused by Staphylococcus aureus, with a mortality rate of about 14%. Antimicrobial drug resistance in Staphylococcus aureus is a major global clinical issue and one of the leading causes of deaths associated with antimicrobial drug resistance, of which the proportion of methicillin-resistant Staphylococcus aureus (MRSA) infections continues to rise.43 In this study, Staphylococcus aureus exhibited high resistance to oxacillin, penicillin, and cefoxitin. Among them, 12 isolates were identified as MRSA, accounting for 75.00%.
Our findings indicated that among the detected Gram-negative bacteria, Klebsiella pneumoniae (48.36%) and Escherichia coli (12.30%) were the most prevalent. Similarly, Zelellw et al36 identified Klebsiella pneumoniae and Escherichia coli as the primary pathogens associated with neonatal bloodstream infections in developing countries.32 Infections caused by Klebsiella pneumoniae are often accompanied by high rates of antimicrobial drug resistance and species diversity.15 In recent studies, the proportion of carbapenem-resistant Enterobacteriaceae (CRE), particularly Klebsiella pneumoniae, has been increasing, resulting in limited treatment options and poor prognosis, posing a serious threat to public health.44 In this study, MDR strains accounted for 28.81% of Klebsiella pneumoniae isolates and also exhibited a high rate of resistance to imipenem. Carbapenem resistance in Klebsiella pneumoniae is mediated by two primary mechanisms: non-enzymatic (porin loss plus β-lactamase overexpression) and enzymatic (acquired carbapenemases via plasmids, causing high-level, transmissible resistance).45 As one of the most predominant nosocomial pathogens, Klebsiella pneumoniae is frequently exposed to various classes of antimicrobial agents, subjecting it to intense selective pressure for resistance and resulting in a high prevalence of healthcare-associated infections. A systematic review14 incorporating global multicenter studies demonstrated that the pooled prevalence of CRKP infection among hospitalized neonates was 0.3%, with a mortality rate as high as 22.9%. Notably, the prevalence in Asian countries (0.7%) was significantly higher than that in African countries (0.3%), and the prevalence of CRKP infection in NICUs (0.7%) was significantly higher than that in non-ICU neonatal care unit (0.0%). Due to the extensive drug resistance of CRKP and the numerous restrictions on antimicrobial use during the neonatal period, commonly used agents in adults such as fluoroquinolones and aminoglycosides carry risks of nephrotoxicity or ototoxicity in neonates, rendering the treatment of CRKP a particularly challenging problem. Comprehensive prevention and control measures should be implemented, including strengthening antimicrobial stewardship and restricting carbapenem use to reduce selective pressure, thereby decreasing the incidence and harm of CRKP infection in neonates. To reduce antimicrobial resistance and minimize adverse effects such as neurodevelopmental delay associated with unnecessary antibiotic exposure, strict antimicrobial stewardship protocols should be developed in accordance with evidence-based guidelines and standardized treatment regimens, aiming to decrease the prevalence of MDR bacteria in NICUs and ultimately achieve better therapeutic outcomes for vulnerable neonates.46 Therefore, early and accurate identification of infections and resistance profiles in neonates is also crucial for providing timely and appropriate treatment.
The strong selective pressure from inappropriate and prolonged antimicrobial exposure, particularly broad-spectrum antibacterial therapy, may contribute to fungal selection pressure in NICUs.18 Our analysis detected seven fungal bloodstream isolates, including three Candida albicans isolates (42.86% of fungi). Although no MDR fungal isolates were detected in this dataset, prophylaxis decisions should not be inferred from isolate counts alone. Because local NICU invasive-candidiasis incidence was not available for evaluating the IDSA >10% threshold, antifungal prophylaxis should be guided by ongoing unit-level surveillance, risk assessment, and applicable guidance rather than recommended solely from the present dataset.25,26
Conclusion
This retrospective single-center study described bloodstream pathogens and antimicrobial resistance among 283 neonates with 290 blood-culture isolates. Gram-positive bacteria predominated, especially CoNS and Staphylococcus epidermidis, while Klebsiella pneumoniae was the leading Gram-negative pathogen. High MDR rates among CoNS and clinically important resistance in Klebsiella pneumoniae support continued surveillance, careful review of empiric neonatal antimicrobial regimens, infection-prevention measures, and antimicrobial stewardship. These findings should be interpreted in light of several limitations: culture-negative sepsis cases were excluded; selection bias is possible because analyses focused on culture-positive cases; small blood volumes can reduce blood-culture sensitivity in neonates; some organism-specific resistance estimates are based on small samples; molecular resistance analysis was not performed; multivariable models were not performed because of the limited sample size and small pathogen-specific subgroups. Future work should standardize the laboratory reporting policy for patient-level and isolate-level results, optimize blood-culture collection procedures, and use multicenter surveillance and adjusted analyses where feasible.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Bass LM, de Meireles LHF, Kiriyama EJ, et al. Cost savings of a nationwide project preventing healthcare-associated infections in adult, paediatric and neonatal critical care settings in Brazil: a micro-costing study. BMJ Open. 2025;15(4):e097515. doi:10.1136/bmjopen-2024-097515
2. Allegranzi B, Bagheri Nejad S, Combescure C, et al. Burden of endemic health-care-associated infection in developing countries: systematic review and meta-analysis. Lancet. 2011;377:228–12. doi:10.1016/S0140-6736(10)61458-4
3. Aziz K, McMillan DD, Andrews W, et al. Canadian neonatal network. Variations in rates of nosocomial infection among Canadian neonatal intensive care units may be practice-related. BMC Pediatr. 2005;5:22. doi:10.1186/1471-2431-5-22
4. Gerios L, Rodrigues VHB, Corrente JE, et al. Late-Onset sepsis in very low birth weight premature infants: a 10-Year review of a Brazilian tertiary university hospital-the challenge remains. Am J Perinatol. 2024;41(S 01):e1725–e1731. doi:10.1055/s-0043-1768702
5. Huncikova Z, Vatne A, Stensvold HJ, et al. Norwegian neonatal network. Late-onset sepsis in very preterm infants in Norway in 2009-2018: a population-based study. Arch Dis Child Fetal Neonatal Ed. 2023;108(5):478–484. doi:10.1136/archdischild-2022-324977
6. Agyeman PKA, Schlapbach LJ, Giannoni E, et al. Swiss Pediatric Sepsis Study. Epidemiology of blood culture-proven bacterial sepsis in children in Switzerland: a population-based cohort study. Lancet Child Adolesc Health. 2017;1(2):124–133. doi:10.1016/S2352-4642(17)30010-X
7. Santos RP, Tristram D. A practical guide to the diagnosis, treatment, and prevention of neonatal infections. Pediatr Clin North Am. 2015;62(2):491–508. doi:10.1016/j.pcl.2014.11.010
8. Polin RA, Denson S, Brady MT. Committee on fetus and newborn; committee on infectious diseases. epidemiology and diagnosis of health care-associated infections in the NICU. Pediatrics. 2012;129(4):e1104–9. doi:10.1542/peds.2012-0147
9. Shane AL, Stoll BJ. Neonatal sepsis: progress towards improved outcomes. J Infect. 2014;68:S24–32. doi:10.1016/j.jinf.2013.09.011
10. Wirtschafter DD, Powers RJ, Pettit JS, et al. Nosocomial infection reduction in VLBW infants with a statewide quality-improvement model. Pediatrics. 2011;127(3):419–426. doi:10.1542/peds.2010-1449
11. Dramowski A, Bolton L, Bekker A, et al. Epidemiology of healthcare-associated bloodstream infection in South African neonatal units. BMC Infect Dis. 2024;24(1):1350. doi:10.1186/s12879-024-10219-0
12. Fung PG, Hon EKL, Leung KA. Antibiotic treatment for neonatal sepsis: changing trends and future directions. Drugs Context. 2026;15. doi:10.7573/dic.2025-5-4
13. Zhang X, Li Y, Tao Y, Ding Y, Shao X, Li W. Epidemiology and drug resistance of neonatal bloodstream infection pathogens in east China children’s medical center from 2016 to 2020. Front Microbiol. 2022;13:820577. doi:10.3389/fmicb.2022.820577
14. Hu Y, Yang Y, Feng Y, et al. Prevalence and clonal diversity of carbapenem-resistant Klebsiella pneumoniae causing neonatal infections: a systematic review of 128 articles across 30 countries. PLoS Med. 2023;20(6):e1004233. doi:10.1371/journal.pmed.1004233
15. Wen SCH, Ezure Y, Rolley L, et al. Gram-negative neonatal sepsis in low- and lower-middle-income countries and WHO empirical antibiotic recommendations: a systematic review and meta-analysis. PLoS Med. 2021;18(9):e1003787. doi:10.1371/journal.pmed.1003787
16. Ristori MV, Scarpa F, Sanna D, et al. Multidrug-Resistant Klebsiella pneumoniae strains in a hospital: phylogenetic analysis to investigate local epidemiology. Microorganisms. 2024;12(12):2541. doi:10.3390/microorganisms12122541
17. Soni P, Matoria R, Nagalli MM. Antibiotic strategies for neonatal sepsis: navigating efficacy and emerging resistance patterns. Eur J Pediatr. 2025;184(7):439. doi:10.1007/s00431-025-06271-w
18. De Mello Freitas FT, Viegas APB, Romero GAS. Neonatal healthcare-associated infections in Brazil: systematic review and meta-analysis. Arch Public Health. 2021;79(1):89. doi:10.1186/s13690-021-00611-6
19. Jarvis WR. Bennett & Brachman’s Hospital Infections.
20. Stoll BJ, Puopolo KM, Hansen NI, et al. Early-Onset neonatal sepsis 2015 to 2017, the rise of Escherichia coli, and the need for novel prevention strategies. JAMA Pediatr. 2020;174(7):e200593. doi:10.1001/jamapediatrics.2020.0593
21. Verani JR, McGee L, Schrag SJ. Division of bacterial diseases, national center for immunization and respiratory diseases (CDC) prevention of perinatal group B streptococcal disease: revised guidelines from CDC, 2010. MMWR Recomm Rep. 2010;59(RR–10):1–36.
22. Dong Y, Speer CP. Late-onset neonatal sepsis: recent developments. Arch Dis Child Fetal Neonatal Ed. 2015;100(3):F257–63. doi:10.1136/archdischild-2014-306213
23. Russell N, Barday M, Okomo U, Dramowski A, Sharland M, Bekker A. Early-versus late-onset sepsis in neonates - time to shift the paradigm? Clin Microbiol Infect. 2024;30(1):38–43. doi:10.1016/j.cmi.2023.07.023
24. Flannery DD, Edwards EM, Coggins SA, Horbar JD, Puopolo KM. Late-Onset sepsis among very preterm infants. Pediatrics. 2022;150(6):e2022058813. doi:10.1542/peds.2022-058813
25. Xie J, Zeng J, Zheng S. The efficacy and safety of fluconazole in preventing invasive fungal infection in very low birth weight infants: a systematic review and meta-analysis. Ital J Pediatr. 2023;49(1):51. doi:10.1186/s13052-023-01460-5
26. Pappas PG, Kauffman CA, Andes DR, et al. Clinical practice guideline for the management of candidiasis: 2016 update by the infectious diseases society of America. Clin Infect Dis. 2016;62(4):e1–e50. doi:10.1093/cid/civ933
27. Fleiss N, Tarun S, Polin RA. Infection prevention for extremely low birth weight infants in the NICU. Semin Fetal Neonatal Med. 2022;27(3):101345. doi:10.1016/j.siny.2022.101345
28. Kochanowicz JF, Nowicka A, Al-Saad SR, Karbowski LM, Gadzinowski J, Szpecht D. Catheter-related bloodstream infections in infants hospitalized in neonatal intensive care units: a single center study. Sci Rep. 2022;12(1):13679. doi:10.1038/s41598-022-17820-w
29. Attia hussein Mahmoud H, Parekh R, Dhandibhotla S, et al. Insight into neonatal sepsis: an overview. Cureus. 2023;15(9):e45530. doi:10.7759/cureus.45530
30. Abdelhamid SM. Time to positivity and antibiotic sensitivity of neonatal blood cultures. J Glob Infect Dis. 2017;9(3):102–107. doi:10.4103/jgid.jgid_1_17
31. Bech CM, Stensgaard CN, Lund S, et al. Risk factors for neonatal sepsis in Sub-Saharan Africa: a systematic review with meta-analysis. BMJ Open. 2022;12(9):e054491. doi:10.1136/bmjopen-2021-054491
32. Mohakud NK, Mishra JP, Nayak MK, et al. Bacteriological profile and outcome of culture-positive neonatal sepsis in a special newborn care unit setting, Odisha. Cureus. 2022;14(5):e25539. doi:10.7759/cureus.25539
33. Kartik K, Khan FA, Rathoria E, Srivastava D, Singh SK, Rathoria R. Clinical and microbiological profile of culture-positive neonatal sepsis in a tertiary care center in North India. Cureus. 2025;17(9):e92136. doi:10.7759/cureus.92136
34. Ntusi N, Aubin L, Oliver S, Whitelaw A, Mendelson M. Guideline for the optimal use of blood cultures. S Afr Med J. 2010;100(12):839–843. doi:10.7196/samj.4217
35. Lin PC, Chang CL, Chung YH, Chang CC, Chu FY. Revisiting factors associated with blood culture positivity: critical factors after the introduction of automated continuous monitoring blood culture systems. Medicine. 2022;101(30):e29693. doi:10.1097/MD.0000000000029693
36. Zelellw DA, Dessie G, Worku Mengesha E, Balew Shiferaw M, Mela Merhaba M, Emishaw S. A systemic review and meta-analysis of the leading pathogens causing neonatal sepsis in developing countries. Biomed Res Int. 2021;6626983. doi:10.1155/2021/6626983
37. Crichton H, O’Connell N, Rabie H, Whitelaw AC, Dramowski A. Neonatal and paediatric bloodstream infections: pathogens, antimicrobial resistance patterns and prescribing practice at Khayelitsha District Hospital, Cape Town, South Africa. S Afr Med J. 2018;108(2):99–104. doi:10.7196/SAMJ.2018.v108i2.12601
38. Garcia-Prats JA, Cooper TR, Schneider VF, Stager CE, Hansen TN. Rapid detection of microorganisms in blood cultures of newborn infants utilizing an automated blood culture system. Pediatrics. 2000;105(3 Pt 1):523–527. doi:10.1542/peds.105.3.523
39. Johnson J, Robinson ML, Rajput UC, et al. High burden of bloodstream infections associated with antimicrobial resistance and mortality in the neonatal intensive care unit in Pune, India. Clin Infect Dis. 2021;73(2):271–280. doi:10.1093/cid/ciaa554
40. Greenberg RG, Kandefer S, Do BT, et al. Late-onset sepsis in extremely premature infants: 2000-2011. Pediatr Infect Dis J. 2017;36(8):774–779.
41. Moles L, Gómez M, Moroder E, et al. Staphylococcus epidermidis in feedings and feces of preterm neonates. PLoS One. 2020;15(2):e0227823. doi:10.1371/journal.pone.0227823
42. Knoll RL, Podlesny D, Fortmann I, et al. Staphylococcus aureus colonization and bloodstream infection in very preterm infants. Gut Microbes. 2025;17(1):2592423. doi:10.1080/19490976.2025.2592423
43. Namushi J, Tootla H, Nuttall J, Eley B. Staphylococcus aureus bloodstream infection at a referral children’s hospital in Cape Town, South Africa, 2018-2022. BMC Infect Dis. 2025;26(1):5. doi:10.1186/s12879-025-12162-0
44. Yu Z, Li L, Cheng P, Zhang H, Xu S. Clinical characteristics and mortality risk factors of premature infants with carbapenem-resistant Klebsiella pneumoniae bloodstream infection. Sci Rep. 2024;14(1):29486. doi:10.1038/s41598-024-80974-2
45. Aires-de-Sousa M, Ortiz de la Rosa JM, Gonçalves ML, Pereira AL, Nordmann P, Poirel L. Epidemiology of carbapenemase-producing Klebsiella pneumoniae in a Hospital, Portugal. Emerg Infect Dis. 2019;25(9):1632–1638. doi:10.3201/eid2509.190656
46. Chu M, Lin J, Wang M, et al. Reducing the overall use of broad-spectrum antibiotics in NICU is associated with less prevalence of multi-drug resistant Klebsiella pneumoniae isolation in premature infants. Antimicrob Resist Infect Control. 2025;15(1):15. doi:10.1186/s13756-025-01693-5
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Pathogen Distribution of Neonatal Bacterial Meningitis in the Era of Multidrug-Resistant Bacteria: A Single-Center Experience
Zhu M, Lin J, Zhuge Z, Zheng Y, Ye S, Wang X, Zhu J, Chen S, Lin Z
Infection and Drug Resistance 2024, 17:5277-5286
Published Date: 27 November 2024