Back to Journals » Clinical Ophthalmology » Volume 20
Retrospective Evaluation of Successive Biovance® Decellularized Basement Membrane Tissue Grafts for the Management of Chronic Subclinical and Stage 1 Neurotrophic Keratitis
Authors Ayres BD, Fram NR ![]() , Wu HK, Feulner L, Desai NR
, Wu HK, Feulner L, Desai NR
Received 12 February 2026
Accepted for publication 12 May 2026
Published 19 May 2026 Volume 2026:20 599498
DOI https://doi.org/10.2147/OPTH.S599498
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sotiria Palioura
Brandon D Ayres,1 Nicole R Fram,2 Helen K Wu,3 Lisa Feulner,4 Neel R Desai5
1Cornea Service, Wills Eye Hospital, Philadelphia, PA, USA; 2Advanced Eye Care, Los Angeles, CA, USA; 3Newton Wellesley Eye Associates, Wellesley, MA, USA; 4Advanced Eye Care & Aesthetics, Bel Air, MD, USA; 5Eye Institute of West Florida, Largo, FL, USA
Correspondence: Brandon D Ayres, Cornea Service, Wills Eye Hospital, 840 Walnut Street, Philadelphia, Pennsylvania, 19107, USA, Email [email protected]
Purpose: To evaluate the clinical outcomes of serial placement of an amniotic decellularized basement membrane (DBM) graft (Biovance®) in patients with subclinical or Mackie Stage 1 neurotrophic keratitis (NK). The primary objective was to assess changes in corneal fluorescein staining and functional corneal sensitivity, with tear osmolarity and metalloproteinase-9 (MMP-9) used as adjunctive indicators of ocular surface stability.
Methods: This retrospective study included eyes with reduced corneal sensitivity (Brill esthesiometry Levels 3– 5), epithelial staining, and positive MMP-9, consistent with subclinical or Mackie Stage 1 NK. Each eye underwent serial DBM graft placement guided by clinical response over an average of 7 weeks. Corneal fluorescein staining, Brill esthesiometry, tear osmolarity, and MMP-9 status were assessed at each visit. Follow-up occurred every 1– 2 weeks, with treatment advanced upon improvements in corneal staining and stabilizing biomarker trends. Outcomes included clinician-documented resolution of epithelial staining, changes in corneal sensitivity, and normalization of tear osmolarity and MMP-9.
Results: A total of 936 eyes from 488 patients met enrollment criteria. Mean DBM utilization increased with disease severity (Brill 3: 3.70; Brill 4: 3.08; Brill 5: 4.30 grafts). Corneal epithelial resolution occurred in all eyes with complete follow-up. Functional corneal sensitivity improved in 0.7% of Brill 3, 31.6% of Brill 4, and 77.5% of Brill 5 eyes. Among eyes with abnormal baseline osmolarity, 70– 82% normalized following treatment. MMP-9 positivity decreased across all severity groups, with 56– 66% converting to negative, corresponding with improved ocular surface stability.
Conclusion: Serial DBM grafting was associated with improvements in corneal staining, functional corneal sensitivity, ocular surface inflammation, and tear-film homeostasis, supporting its role in early-stage NK management. These findings suggest DBM promotes epithelial and neurosensory recovery through host–matrix interactions within the preserved basement membrane and that early intervention may help mitigate disease progression.
Keywords: amniotic membrane tissue, decellularized basement membrane, neurotrophic keratitis, biovance, ocular surface disease, corneal sensitivity
Introduction
Neurotrophic keratitis (NK) is a degenerative corneal neuropathy characterized by impaired trigeminal innervation, leading to epithelial instability, inflammation, and risk of progressive corneal ulceration.1,2 Loss of corneal sensation disrupts epithelial proliferation, blink reflexes, trophic factor signaling, and maintenance of ocular surface homeostasis, predisposing the cornea to punctate epithelial keratopathy, persistent epithelial defects (PED), stromal ulceration, and perforation (clinically classified as Mackie Stages 1–3).3,4
Subclinical NK has been increasingly recognized as an early disease state, characterized by early epithelial breakdown, elevated tear osmolarity, or inflammatory biomarkers, even in the absence of frank epithelial defects.3,5
Patients with diabetes, chronic glaucoma‑medication exposure, and prior corneal surgery may demonstrate early corneal neurosensory dysfunction despite subtle clinical findings.6–8 Identification of subclinical and early NK is thus a critical opportunity for therapeutic intervention before irreversible epithelial and nerve damage occurs.
Objective assessment of corneal sensation has become increasingly important in detecting early neurotrophic dysfunction. Non-contact corneal esthesiometry allows reproducible quantification of sensory thresholds and facilitates stratification of disease severity. Reduced corneal sensitivity has been shown to correlate with epithelial instability and risk of progression, and sensory impairment may precede overt clinical ulceration. Accordingly, corneal sensitivity testing serves as a clinically meaningful surrogate marker of corneal nerve health in early and established NK.
Conventional therapeutic management of NK includes intensive lubrication, therapeutic contact lenses, punctal occlusion, and tarsorrhaphy. Cenegermin, a recombinant human nerve growth factor, represents a targeted neuroregenerative therapy for neurotrophic keratitis. In contrast, amniotic basement membrane–based therapies provide a biologic scaffold that supports epithelial repair and suppresses inflammation, while indirectly facilitating neurosensory recovery. Biovance, a decellularized basement membrane (DBM), has emerged as a unique biologic platform distinguished by complete decellularization, preservation of extracellular matrix (ECM) architecture, enhanced recipient corneal epithelial interaction, and suitability for repeated office-based application.9,10 Mechanical, non-thermal decellularization removes the pro-inflammatory chorion and residual donor cellular debris, reducing immunogenicity while preserving key extracellular matrix proteins such as collagen and elastin, which support a matrix for cellular migration. Additionally, this processing enhances cell attachment, reduces graft slippage and promotes the downstream production of anti-inflammatory cytokines and growth factors, providing a stable scaffold for epithelial cell regeneration.9 In NK and advanced dry eye disease (DED) complicated by persistent corneal epithelial defects, DBM has demonstrated effectiveness in promoting epithelial defect resolution.10
Although DBM has demonstrated efficacy in promoting epithelial healing in ocular surface disease, data describing its role in subclinical and early-stage NK, particularly when applied serially and guided by neurosensory and biomarker response, remain limited. The present retrospective study evaluates the clinical outcomes of serial DBM placement in eyes with subclinical or Mackie Stage 1 NK, using corneal fluorescein staining, corneal sensitivity testing, tear osmolarity, and metalloproteinase-9 (MMP-9) as complementary measures of epithelial integrity, neurosensory function, and ocular surface stability.
Methods
Study Design and Oversight
This study was a retrospective, observational cohort analysis of patients treated for subclinical or early-stage neurotrophic keratitis (NK) in a multi-doctor, multi-office clinical practice. The study protocol was reviewed by Advarra Institutional Review Board, reference number Pro00091817, which determined that the research met criteria for exemption from informed consent due to its retrospective design, minimal risk, and use of de-identified data.
Furthermore, the research adhered to the ethical standards outlined in the Declaration of Helsinki, ensuring compliance with guidelines for conducting research involving human participants.
Study Population and Data Source
Electronic medical records were queried for clinical encounters between June 2024 and March 2025. The analytic cohort consisted of adult patients who underwent serial placement of a decellularized amniotic basement membrane (DBM) graft for management of subclinical or Mackie Stage 1 NK and who had complete baseline and follow-up diagnostic testing.
All analyses were performed at the eye level, with each eye considered an independent observational unit.
Inclusion Criteria
Eyes were included in the study if all of the following criteria were met:
- Age ≥17 years at the time of treatment.
- Presence of persistent corneal epithelial staining on slit-lamp examination despite initial standard therapy, including lubrication, lid hygiene, and topical anti-inflammatory treatment.
- Diagnosis of subclinical NK or Mackie Stage 1 NK, defined as:
- Subclinical NK:
- Brill non-contact corneal esthesiometry Level 3,
- Presence of corneal epithelial fluorescein staining, and
- At least one abnormal tear biomarker, defined as tear osmolarity ≥308 mOsm/L and/or a positive qualitative metalloproteinase-9 (MMP-9) assay.
- Clinical NK (Mackie Stage 1):
- Brill esthesiometry Levels 4–5, and
- Presence of corneal epithelial fluorescein staining.
- Subclinical NK:
4. Availability of complete baseline and final follow-up data, including:
○ Corneal fluorescein staining assessment.
○ Brill corneal esthesiometry.
○ Tear osmolarity testing.
○ Tear MMP-9 testing.
5. Treatment was with serial single layer DBM placements during the study period until resolution of corneal staining.
6. Once the epithelial staining resolved, patients were followed at 1 month, 3 months, and 6 months.
Systemic and ocular risk factors for NK (including diabetes mellitus, chronic glaucoma medication use, or prior corneal surgery) were not required for inclusion but were recorded to characterize the study population.
Exclusion Criteria
Eyes were excluded if any of the following were present:
- Evidence of active ocular infection, corneal perforation, or stromal ulceration consistent with Mackie Stage 2 or 3 NK.
- Ocular surgery within 3 months prior to initiation of DBM treatment.
- Introduction of new topical medications, systemic therapies affecting the ocular surface, or lid-based procedures during the DBM treatment period.
- Incomplete diagnostic data, including missing baseline or follow-up assessments of corneal staining of at least 1 month post treatment protocol, Brill esthesiometry, tear osmolarity, or MMP-9 status.
Clinical Assessments and Diagnostic Testing
At baseline and during follow-up testing every 1–2 weeks, all eyes underwent standardized ocular surface evaluation, including slit-lamp examination with corneal fluorescein staining, non-contact corneal esthesiometry using the Brill esthesiometer (Brill Engines S.L., Barcelona, Spain), tear osmolarity testing (Trukera Medical, Inc., Escondido CA, USA; cutoff ≥308 mOsm/L), and qualitative tear MMP-9 assessment using the InflammaDry assay (QuidelOrtho, San Diego, CA), performed according to manufacturers’ instructions. Any degree of punctate epithelial fluorescein staining was classified as abnormal. Corneal staining was graded on a scale of 1 to 4, with grade 1 representing trace staining and grade 4 representing dense, confluent central corneal staining.
DBM Treatment Protocol
Eligible eyes received serial placement of a decellularized amniotic basement membrane (DBM) graft (Biovance®, DefEYE, Inc., Sarasota, FL) in the clinic setting. DBM application was performed under topical anesthesia. The corneal surface was gently dried using a cellulose sponge, after which the DBM graft was positioned and smoothed into place using a damp cellulose sponge.
Following placement, graft stabilization was achieved using one of the following clinician-selected methods: a 24-hour eyelid pressure patch, a dissolvable collagen shield, or a high–water content (≥50%) bandage contact lens. The majority of patients received a pressure patch. No new topical medications or lid-based procedures were initiated during the treatment period.
Patients were evaluated at approximately weekly intervals. Repeat DBM application was performed at the discretion of the treating clinician based on incomplete epithelial resolution and/or persistence of abnormal neurosensory or biomarker findings. Treatment was continued until resolution of corneal staining accompanied by symptomatic improvement and stabilization or normalization of tear biomarkers. DBM utilization was quantified as the total number of graft placements per eye over the treatment course, including repeat applications at follow-up visits. Once the epithelial staining resolved, patients were followed at 1 month, 3 months, and 6 months.
Statistical Analysis
All statistical analyses were performed at the eye level, with each eye treated as an independent observational unit. Descriptive statistics were used to summarize baseline characteristics and outcomes. Continuous variables are reported as mean ± standard deviation (SD) or median with interquartile range (IQR), as appropriate, and categorical variables are presented as counts and percentages.
Analyses were restricted to eyes with complete baseline and final follow-up data for Brill corneal esthesiometry, tear osmolarity, and MMP-9 status.
Corneal Sensitivity Outcomes
Changes in corneal sensitivity from baseline to final follow-up were assessed using the Wilcoxon signed-rank test, treating Brill esthesiometry levels as an ordinal variable. Improvement in corneal sensitivity was defined as a decrease in Brill level at final follow-up compared with baseline. The proportion of eyes demonstrating any improvement in Brill level was compared across baseline Brill severity groups (Levels 3, 4, and 5) using-χ2 tests.
Tear Osmolarity and MMP-9 Outcomes
Tear osmolarity was dichotomized as normal versus abnormal using a threshold of ≥308 mOsm/L. MMP-9 status was classified as positive versus negative based on the qualitative InflammaDry assay. For both outcomes, changes in the proportion of abnormal eyes between baseline and final follow-up were assessed using McNemar’s χ2-test with continuity correction, both in the overall cohort and stratified by baseline Brill level. Among eyes with abnormal baseline osmolarity or positive baseline MMP-9, the proportion achieving normalization at final follow-up was calculated descriptively.
Statistical Thresholds and Software
All statistical tests were two-sided, and a p-value <0.05 was considered statistically significant. Statistical analyses were performed using R (R Foundation for Statistical Computing, Vienna, Austria).
Methodologic Considerations
Because some patients contributed both eyes, inter-eye correlation was not adjusted for, which may result in underestimation of variance and inflation of statistical significance. This limitation is acknowledged given the retrospective nature of the study and the large sample size.
Results
Study Cohort
A total of 936 eyes from 488 patients met all inclusion criteria and were included in the final analytic cohort. All included eyes had baseline Brill esthesiometry levels 3–5, corneal epithelial fluorescein staining, and complete baseline and final follow-up testing (including pretreatment osmolarity, metalloproteinase-9 (MMP-9), and Brill level). Outcomes were assessed longitudinally over the decellularized basement membrane (DBM) treatment course.
Patients returned weekly for clinical evaluations, and repeated DBM applications were performed based on the patient’s clinical therapeutic response, inclusive of a complete resolution of corneal staining in combination with symptomatic relief and biomarker normalization. All patients within the treatment cohort achieved resolution of their epitheliopathy and concomitant corneal fluorescein staining.
Baseline Characteristics
Baseline demographic and clinical characteristics stratified by Brill corneal sensitivity level are summarized in Table 1. Across all Brill severity groups, patients were predominantly female (64.7–67.7%). Diabetes mellitus was highly prevalent, affecting 85–90% of patients across all groups. Use of chronic topical glaucoma medications ranged from 6.5% to 13.4%, with the highest prevalence in Brill Level 4 eyes. Prior corneal refractive surgery (LASIK/PRK) was uncommon overall and was not observed in Brill Level 4 or 5 eyes.
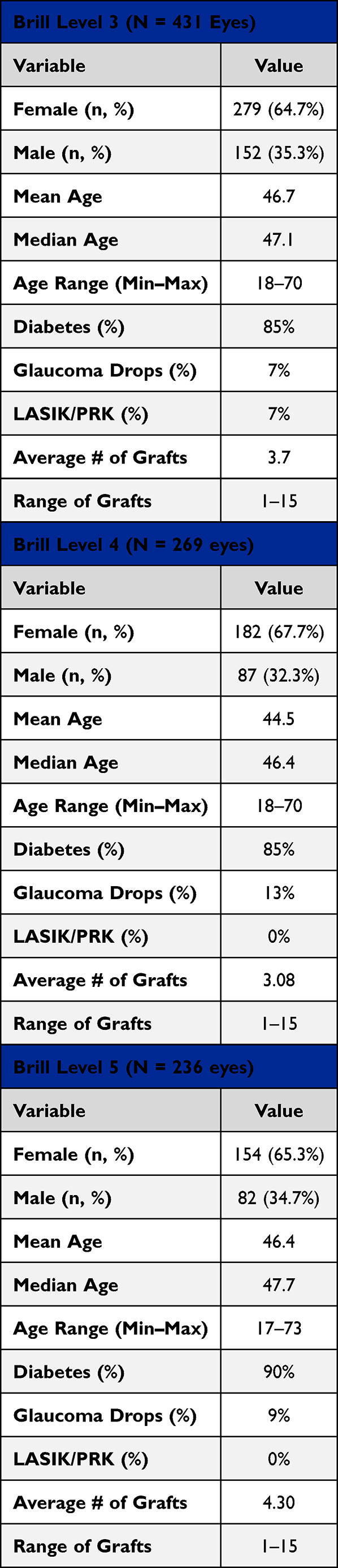 |
Table 1 Patient Demographics, Risk Factors, and DBM Applications |
Mean age across Brill severity groups ranged from the mid-40s to late-40s, reflecting a broad adult population with ocular surface disease and systemic comorbidities.
DBM Treatment Exposure
All included eyes underwent serial placement of a DBM graft during the study period. DBM utilization was defined as the total number of graft placements per eye over the treatment course, including repeat applications at follow-up visits.
Higher DBM utilization was observed in eyes with more severe baseline corneal sensitivity impairment. The distribution of DBM utilization across baseline Brill severity groups is summarized in Table 1.
Corneal Epithelial Outcomes
Once the epithelial staining resolved, patients were seen in routine follow up at approximately 1 month, 3 months, and 6 months. The mean post treatment follow up time was 114.5 days with a range of 35 to 255 days. At final treatment follow-up, complete resolution of corneal epithelial fluorescein staining was observed in all eyes included in the final analytic cohort.
No eyes developed persistent epithelial defects, stromal ulceration, or corneal perforation during the observed follow-up period.
DBM utilization patterns demonstrated that disease severity corresponded with increasing graft burden, with Brill 5 eyes requiring the greatest number of grafts (mean 4.30, range 1–15), followed by Brill 3 (mean 3.70) and Brill 4 (mean 3.08).
Brill Level 3 (N = 431 Eyes)
Patients with baseline Brill 3 corneal sensitivity demonstrated a mean age of 46.7 years and the widest range of ages (18–71). This group consisted of 64.7% (269/431) females. Diabetes was present in 85.2% (367/431) of individuals, while use of glaucoma drops and prior refractive surgery remained relatively low 6.5% (28/431) and 7.4% (32/431) respectively). DBM utilization averaged 3.70 grafts per eye, reflecting a substantial but moderate treatment burden. Despite the lower baseline severity relative to Brill 4–5, a subset of eyes still required extensive grafting, with a range from 1 to 15 grafts.
Brill Level 4 (N = 269 Eyes)
Eyes with corneal sensitivity Brill 4 exhibited the youngest mean age of the cohort (44.5 years) and the highest proportion of patients on glaucoma medications 13.4% (36/269). Diabetes prevalence remained high 85.1% (229/269) while prior LASIK/PRK was not observed in this group. The mean number of grafts was 3.08, slightly lower than Brill 3 and substantially lower than Brill 5, with a similar wide range (1–15).
Brill Level 5 (N = 236 Eyes)
Eyes with Level Brill 5, the most severe corneal sensitivity impairment showed a mean age of 46.4 years and the highest rate of diabetes 90.3% (213/236). Females accounted for 65.3% (154/236) of eyes in this group, similar to other Brill levels. No LASIK/PRK was reported. This group had the highest AMT burden, requiring an average of 4.30 grafts per eye, with a range extending up to 15 grafts per eye.
Corneal Sensitivity Outcomes
Changes in corneal sensitivity following serial DBM placement are summarized in Table 2. Across the entire cohort, there was a statistically significant improvement in corneal sensitivity from baseline to final follow-up (Wilcoxon signed-rank test, p < 0.0001). The median Brill level improved from 4.0 (IQR 3.0–5.0) at baseline to 3.0 (IQR 3.0–4.0) at final follow-up.
 |
Table 2 Corneal Sensitivity Changes After Serial DBM Placement |
The proportion of eyes demonstrating any improvement in Brill level differed by baseline severity:
Brill Level 3 (n = 431 Eyes)
Corneal sensitivity remained largely stable, with 0.7% (3/431) of eyes demonstrating improvement. No eyes showed worsening of corneal sensitivity. A small subset (0.7%) achieved Brill Levels 1–2 at final follow-up.
Brill Level 4 (n = 263 Eyes)
31.6% (83/263) of eyes demonstrated improvement in corneal sensitivity, with 0.8% (2/263) achieving Brill Levels 1–2.
Brill Level 5 (n = 236 Eyes)
77.5% (183/236) of eyes demonstrated improvement in corneal sensitivity, and 0.8% (2/236) achieved Brill Levels 1–2.
The proportion of eyes demonstrating improvement in corneal sensitivity differed significantly across baseline Brill severity groups (χ2 = 440.6, p < 0.0001).
Tear Osmolarity Outcomes
Baseline tear osmolarity status and changes following DBM therapy are summarized in Table 3. Across all baseline Brill severity groups, the majority of eyes demonstrated normal tear osmolarity at baseline.
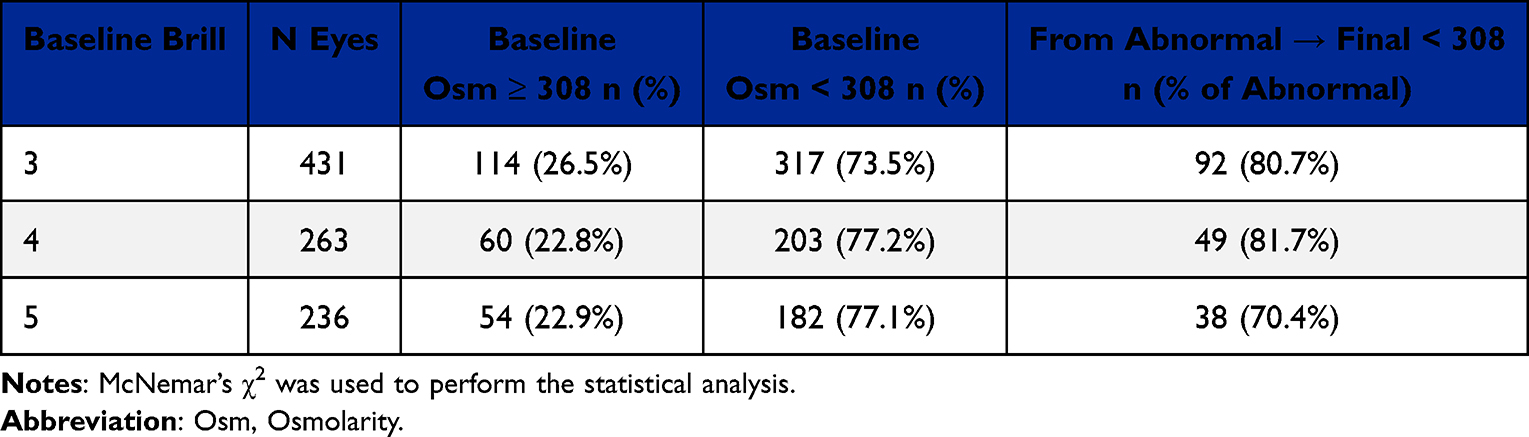 |
Table 3 Tear Osmolarity Changes After Serial DBM Placement |
Among eyes with abnormal baseline tear osmolarity (≥308 mOsm/L), normalization at final follow-up was observed in:
- 80.7% (92/114) of Brill Level 3 eyes
- 81.7% (49/60) of Brill Level 4 eyes
- 70.4% (38/54) of Brill Level 5 eyes
Across the entire cohort, the prevalence of abnormal tear osmolarity decreased from 24.4% at baseline to 20.1% at final follow-up, representing a statistically significant change (McNemar’s test, p = 0.029).
MMP-9 Outcomes
Baseline and final follow-up MMP-9 status are summarized in Table 4. Elevated MMP-9 was common at baseline across all Brill severity groups.
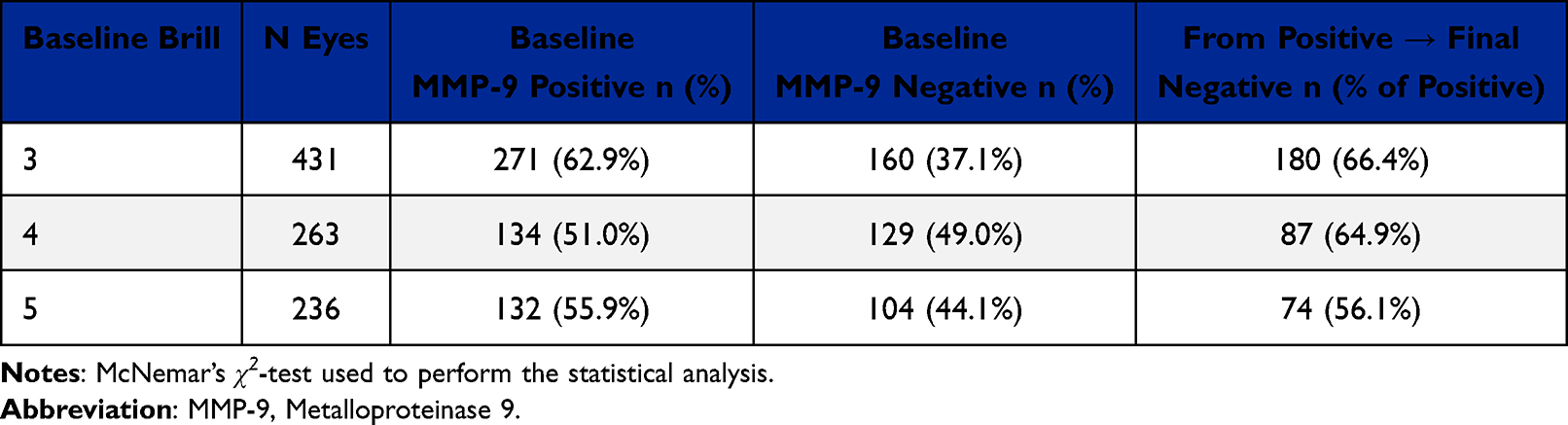 |
Table 4 MMP-9 Changes After Serial DBM Placement |
Among eyes with positive baseline MMP-9, conversion to a negative result at final follow-up was observed in:
- 66.4% (180/271) of Brill Level 3 eyes
- 64.9% (87/134) of Brill Level 4 eyes
- 56.1% (74/132) of Brill Level 5 eyes
Across the entire cohort, the prevalence of MMP-9 positivity decreased from 58.0% at baseline to 35.3% at final follow-up, representing a statistically significant change (McNemar’s test, p < 0.0001).
Statistical Results
Statistical results are summarized in Table 5.
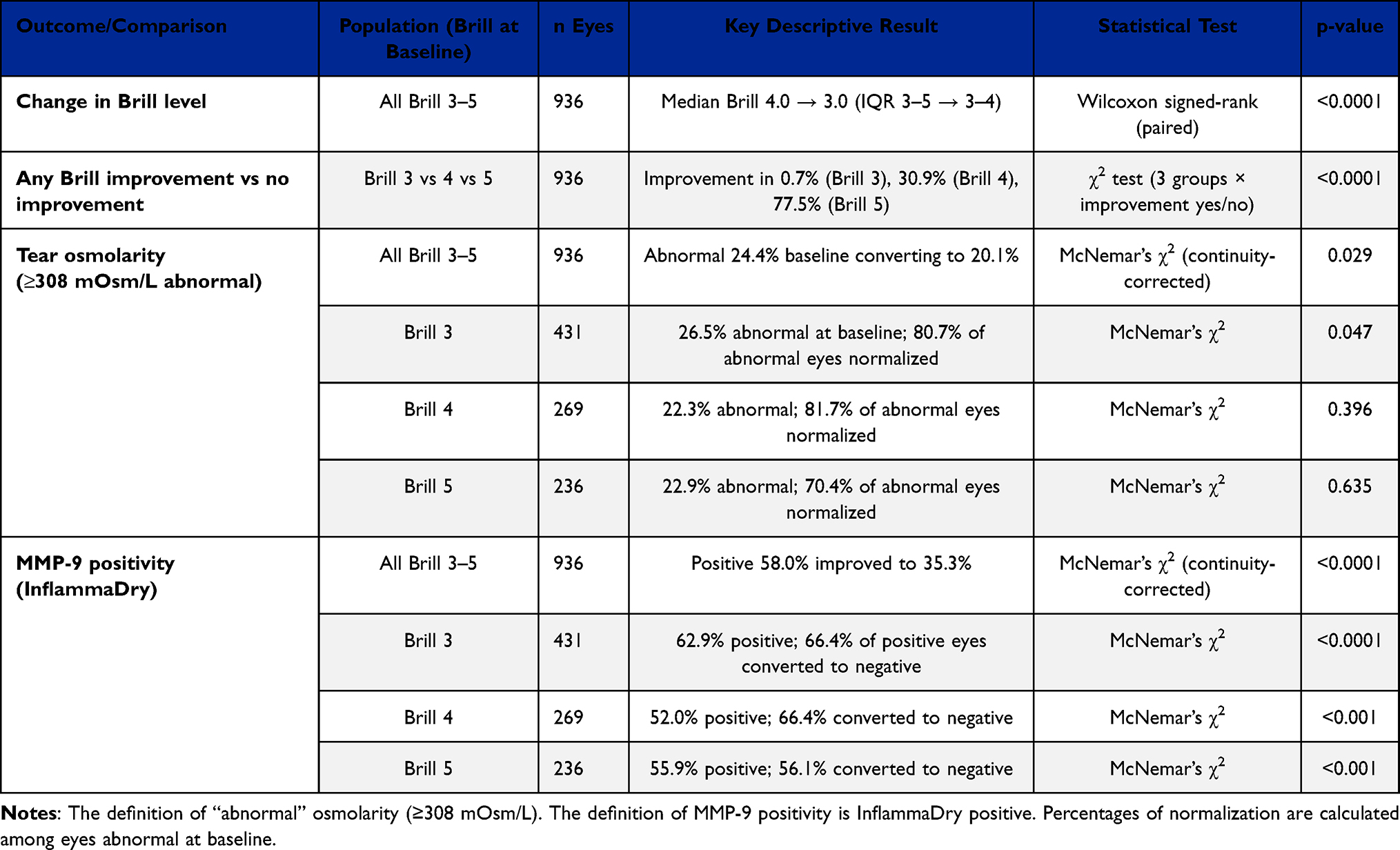 |
Table 5 Summary of Statistical Tests for Primary and Secondary Outcomes |
Discussion
In this large retrospective observational cohort, serial placement of a decellularized amniotic basement membrane (DBM) was associated with consistent resolution of corneal epithelial staining and statistically significant changes in corneal sensitivity and tear biomarkers in eyes with subclinical or Mackie Stage 1 neurotrophic keratitis (NK). These findings extend existing literature on amniotic membrane–based therapies by demonstrating that DBM, when applied serially and guided by clinical response, is associated with measurable improvements across epithelial, neurosensory, and ocular surface biomarker domains in early-stage neurotrophic disease.
Suboptimal nerve plexus (SBNP) loss often precedes measurable sensitivity decline, making early intervention at Brill Level 3, particularly when accompanied by epitheliopathy or abnormal tear biomarkers, a key strategy for preventing progression to overt neurotrophic keratopathy (NK).1,2 Early dysfunction of sub-basal corneal nerves is well-documented in diabetes, dry eye disease, glaucoma, and aging, and frequently precedes overt clinical ulceration.5–8 The concept of “subclinical NK” has emerged to describe patients with underlying risk factors, epithelial disease, tear hyperosmolarity, or elevated inflammatory biomarkers who have not yet developed persistent epithelial defects but demonstrate measurable sensory impairment.1,11
The most striking observation in this study was the severity-dependent pattern of corneal sensitivity change. Eyes with more advanced baseline sensory impairment (Brill Levels 4–5) demonstrated substantially higher rates of measurable improvement compared with eyes classified as Brill Level 3. This pattern likely reflects both biological and measurement-related factors. In early or subclinical NK, corneal sensitivity may be relatively preserved, limiting the capacity for detectable improvement using threshold-based testing. On the other hand, eyes that start with more significant impairment often have a wider range in which improvement can be measured, making it easier to observe their recovery.
Notably, corneal sensitivity in Brill Level 3 eyes did not deteriorate and stayed consistent throughout the treatment period. Though significant improvement was rare for this group, maintaining stability is important for patients who are vulnerable to progressive neuroepithelial issues. These findings underscore the importance of stratifying treatment response by baseline neurosensory status and caution against interpreting lack of measurable improvement in early disease as lack of therapeutic effect. Confocal microscopy may inform future evaluations of the basal nerve plexus following serial DBM placements.
All eyes included in the final analytic cohort demonstrated resolution of corneal epithelial fluorescein staining by the end of the treatment period. Although this study did not employ a graded epithelial staining scale, the uniform resolution of staining suggests that serial DBM placement was effective in supporting epithelial surface restoration in this selected population. Notably, no eyes developed persistent epithelial defects or stromal ulceration during the observed follow-up period. Although this observation does not demonstrate disease prevention without a control group, it does align with clinical stability throughout the treatment period.
Changes in tear osmolarity and MMP-9 concentrations offer complementary insight into ocular surface behavior during DBM therapy. Proteomic analyses of tears from patients with NK identify MMP-9 as one of the most abundant inflammatory proteins associated with this disease.12 Experimental studies further demonstrate that MMP-9 overexpression disrupts re-epithelialization and promotes chronic corneal ulceration, whereas MMP-9 inhibition improves basement membrane integrity and wound healing.13 Together, these findings support the view that elevated MMP-9 may represent a clinically relevant risk factor for persistent epithelial instability and may contribute directly to NK progression.
In contrast, tear osmolarity abnormalities were observed in only a minority of eyes at baseline, consistent with the predominantly neurotrophic rather than evaporative pathophysiology of early NK. Among eyes with elevated baseline osmolarity, a substantial proportion normalized by final follow-up, resulting in a modest but statistically significant reduction in abnormal osmolarity at the cohort level. This pattern suggests that restoration of epithelial integrity may secondarily promote stabilization of tear-film homeostasis in selected patients.
Elevated MMP-9, however, was prevalent across all baseline severity groups and showed a marked reduction following serial DBM placement. As a proteolytic enzyme implicated in epithelial barrier disruption and delayed wound healing, the high baseline prevalence of MMP-9 underscores the inflammatory burden present even in early stages of neurotrophic disease. The observed post-treatment reduction in MMP-9 positivity aligns with the known anti-inflammatory properties of amniotic membrane–derived tissues and supports the role of DBM as an active modulator of the ocular surface environment.
Finally, the convergence of improved corneal sensitivity and reduced MMP-9 positivity suggests that DBM’s clinical benefits extend beyond passive epithelial coverage. These findings support that DBM may promote neuroepithelial recovery through a meaningful suppression of ocular surface inflammation in addition to mechanical support of epithelial healing.
Conventional management of NK begins with conservative therapies such as preservative-free artificial tears, lid hygiene, and topical anti-inflammatory agents to stabilize the ocular surface. However, these measures often provide insufficient support for epithelial recovery in the setting of impaired corneal innervation. AMT has therefore emerged as an important therapeutic modality, offering biologic scaffolding and anti-inflammatory effects that address deficits unmet by conventional treatments.
Cryopreserved AMT has previously been shown to support corneal nerve regeneration and improve corneal sensory function in NK.4,6 However, the present study represents the first evidence that a non-cryopreserved DBM graft can also produce complete resolution of corneal epitheliopathy and clinically meaningful improvements in corneal sensitivity, including measurable improvement in corneal sensitivity, even among patients with advanced NK. This is particularly notable given that DBM lacks viable cellular components or growth factors.9 These findings reflect an evolving understanding that the therapeutic impact of AMT is driven less by the passive transfer of retained biologic factors such as pentraxin or high chain hyaluronic acid, and more by the recipient’s efficient cellular engagement with the preserved basement membrane matrix, which in turn amplifies anti-inflammatory signaling and promotes epithelial and neural recovery.9,10
The observed improvements align with DBM’s capacity to downregulate pro-inflammatory cytokines such as tumor necrosis factor-α (TNF-α) while upregulating interleukin-8 (IL-8), promoting epithelial cell adhesion and migration through its preserved extracellular matrix scaffold.9 Mechanical, non-thermal decellularization removes the pro-inflammatory chorion and donor cellular debris while preserving critical extracellular matrix proteins such as collagen, laminin, and fibronectin, which facilitate epithelial adhesion, migration, and cytokine signaling.9 Preservation of these ECM scaffolding elements enhances epithelial anchoring and promotes a favorable biochemical milieu for anti-inflammatory cytokine release and early neuroepithelial recovery. The sensory restoration documented across all Brill levels, most prominently in severe NK aligns with a host-driven regenerative response induced by DBM in addition to passive surface barrier effects. Serial DBM placement may therefore be particularly advantageous in more advanced NK, where prolonged exposure to a pro-regenerative microenvironment is necessary to achieve durable neurosensory recovery.
Multiple clinical trials and reviews support AMT as an effective escalated therapy for refractory NK, demonstrating high rates of epithelial closure and relatively low complication rates.14–16 However, emerging evidence and contemporary NK management algorithms increasingly underscore the importance of early therapeutic escalation, rather than prolonged reliance on lubricants, lid hygiene, or topical anti-inflammatory agents alone. In patients with subclinical or Mackie stage 1 disease, where sensory impairment and early epithelial instability are present but overt defects have not yet developed, timely initiation of regenerative therapies such as AMT or cenegermin may prevent progression to persistent epithelial defects, stromal breakdown, and advanced neurotrophic disease. This shift toward earlier intervention reflects a growing understanding that addressing the neuroepithelial deficit before structural compromise occurs offers a more favorable pathway for long-term corneal healing and nerve recovery.
Cenegermin, a recombinant human nerve growth factor, represents a targeted neuroregenerative therapy for NK and remains the only FDA-approved pharmacologic treatment for this condition. In contrast, DBM-based therapy provides a biologic scaffold that supports epithelial repair and may indirectly facilitate neurosensory recovery through restoration of the corneal surface environment. These therapeutic approaches are mechanistically distinct and should be viewed as complementary rather than competitive.
DBM offers practical advantages in terms of in-office application, storage, and flexibility of use, particularly in patients with subclinical or early-stage disease who may not yet meet criteria for pharmacologic neuroregenerative therapy or in whom access or tolerability is a concern. The present findings suggest that serial DBM placement may represent a pragmatic escalated therapy option within a stepwise NK management strategy, particularly when guided by objective neurosensory testing and biomarker assessment.
The findings in this study support earlier identification and more proactive treatment of subclinical NK, including patients with mild sensory impairment and non-healing superficial punctate keratitis associated with biomarker abnormalities, especially elevated MMP-9. Early intervention may reduce the risk of persistent epithelial defects and accelerate neuroepithelial recovery.2 Given its accessibility, safety profile, and biologic activity, serial DBM may represents an effective and scalable strategy for treating both early and advanced NK. Although the use of tri-layer DBM constructs, which incorporate additional structural and biochemical support was not performed in this study, it may further enhance epithelial healing, prolong growth-factor retention, provide greater duration of impact, and provide greater scaffold rigidity for stromal remodeling.11,17
The concept of subclinical NK has gained increasing recognition as clinicians identify patients with early epithelial instability and reduced corneal sensitivity prior to development of persistent epithelial defects. The current study supports the feasibility of identifying and treating this population using objective diagnostic tools and suggests that early intervention with regenerative surface therapy may help stabilize the ocular surface during a vulnerable disease phase. While definitive conclusions regarding disease modification cannot be drawn, these findings reinforce the importance of early detection and proactive management.
Limitations
This study has several important limitations. Its retrospective design precludes causal inference and introduces potential selection bias. Outcomes were analyzed at the eye level without adjustment for inter-eye correlation, which may underestimate variance. The study was limited to only subclinical and Mackie stage 1 NK and therefore the outcomes do not necessarily translate directly to Mackie stage 2–3 NK. The absence of a comparator group limits conclusions regarding relative efficacy, and the lack of a standardized epithelial staining scale restricts quantitative assessment of epithelial improvement. In addition, follow-up duration was limited to the treatment period, and longer-term durability of observed changes could not be assessed.
Conclusions
In this large, real-world cohort of eyes with subclinical and early-stage neurotrophic keratitis (NK), serial placement of decellularized basement membrane (DBM) was associated with consistent epithelial surface resolution over an average of approximately 4 months post procedure follow-up, severity-dependent improvements in corneal sensitivity, and reductions in abnormal tear biomarkers. These findings support the role of DBM as an effective clinical management modality to be used for subclinical and Mackie stage 1 NK and emphasize the importance of incorporating objective neurosensory testing and biomarker assessment, particularly MMP-9, into clinical decision-making. Prospective, controlled studies employing standardized outcome measures are warranted to further delineate the role of DBM within established treatment paradigms across all stages of neurotrophic keratopathy.
Acknowledgements
The authors thank Eric Rubinfeld, OD for facilitating access to de-identified clinical data obtained from the electronic medical record system, which supported the analyses presented in this study.
Disclosure
Brandon Ayres and Nicole Fram have no conflicts of interest in this work. Helen Wu and Lisa Feulner are consultants to DefEYE, Inc. Neel R. Desai is both an equity holder and consultant to DefEYE, Inc. He is also an equity holder to Biotissue. The authors report no other conflicts of interest this work.
References
1. Villalba N, Hamrah P, Cruzat A, et al. Detection of early corneal nerve dysfunction using non-contact esthesiometry. Ophthalmol Ther. 2023;12:1251–13. doi:10.1007/s40123-023-00676-2
2. Stolz A, Ramirez-Miranda A, Cortina-Camarillo J, et al. Advances in the understanding and diagnosis of neurotrophic keratitis. Clin Ophthalmol. 2025;19:45–58. doi:10.2147/OPTH.S498122
3. Ayoubi A, Briceño A, Fernández A, et al. Neurotrophic keratitis: emerging diagnostic markers and updated management strategies. Ann Eye Sci. 2025;10(1):15–27.
4. Di Zazzo A, Kheirkhah A, Abud T, Dana R. Management of neurotrophic keratitis. Ocul Surf. 2021;19:322–339. doi:10.1016/j.jtos.2020.11.002
5. Mansoor H, Tan HC, Lin MTY, Mehta JS. Corneal nerve regeneration after treatment of neurotrophic keratopathy. J Clin Med. 2020;9:E3548.
6. Bikbova G, Oshitari T. Corneal nerve morphology and ocular surface status in patients with diabetes mellitus: a review. Clin Ophthalmol. 2018;12:287–294.
7. Cousen P, Cackett P, Bennett H, Swa K, Dhillon B. Tear production and corneal sensitivity in diabetes. Eye. 2007;21(6):694–698.
8. Murphy PJ, Patel S, Kong N, et al. Non-invasive assessment of corneal sensitivity using a new aesthesiometer. Invest Ophthalmol Vis Sci. 2004;45:112–116.
9. Mao J, Protzman NM, John N, et al. An in vitro comparison of human corneal epithelial cell activity and inflammatory response on differently designed ocular amniotic membranes and a clinical case study. J Biomed Mater Res B Appl Biomater. 2023;111(3):684–700.
10. Linsey K. Use of an eyelid pressure patch concomitantly with a decellularized dehydrated amniotic membrane for ocular surface disease management. Ophthalmol Ther. 2025;14:573–584. doi:10.1007/s40123-025-01094-2
11. NaPier L, Buse K, Belin M, et al. Subclinical neurotrophic keratitis: identifying early disease using multimodal diagnostics. Acta Ophthalmol. 2022;100:e1085–e1093.
12. Pieragostino D, Lanzini M, Cicalini I, et al. Tear proteomics reveals the molecular basis of the efficacy of human recombinant nerve growth factor treatment for neurotrophic keratopathy. Sci Rep. 2022;12:1229. doi:10.1038/s41598-022-05229-4
13. Jadczyk-Sorek K, Garczorz W, Bubała-Stachowicz B, et al. Matrix metalloproteinases and the pathogenesis of corneal epithelial wound healing and chronic ulceration. Biol. 2023;12(9):1263. doi:10.3390/biology12091263
14. Khokhar S, Somerville TF, Allan BD. Amniotic membrane transplantation in refractory neurotrophic corneal ulcers. Br J Ophthalmol. 2005;89:420–423. doi:10.1136/bjo.2004.049684
15. Park JH, Kim JK, Kim JC. Amniotic membrane transplantation for management of neurotrophic ulcers and other severe keratopathies. Cornea. 2008;27:592–597.
16. Baig N, Smith MF, O’Brien TP. Efficacy of amniotic membrane transplantation in refractory corneal epithelial defects: a comprehensive review. Eye Vis. 2023;10:24.
17. Denton M. Comparison of effectiveness of biovance single and triple layer decellularized basement membranes for treatment of ocular surface disease: a retrospective study. Clinical Optometry. 2026;18:1–8. doi:10.2147/OPTO.S571568
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.