Back to Journals » Journal of Inflammation Research » Volume 19
Retrospective Analysis of Inflammatory Parameters and Vitamins’ Levels in Psoriasis Patients: A Case-Control Study
Authors Murshidi R ![]() , Bani Hamad S
, Bani Hamad S ![]() , Al Refaei A, Shewaikani N, Al-Nusair DA, Abu Tawileh HB, Murshidi M, Alzeerelhouseini HIA
, Al Refaei A, Shewaikani N, Al-Nusair DA, Abu Tawileh HB, Murshidi M, Alzeerelhouseini HIA ![]()
Received 29 December 2025
Accepted for publication 17 March 2026
Published 11 April 2026 Volume 2026:19 587983
DOI https://doi.org/10.2147/JIR.S587983
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Anish R. Maskey
Rand Murshidi,1 Salsabiela Bani Hamad,1 Assem Al Refaei,2 Nour Shewaikani,2 Dina A Al-Nusair,2 Hind B Abu Tawileh,2 Muayyad Murshidi,3 Hussam I A Alzeerelhouseini1
1Department of Dermatology, School of Medicine, The University of Jordan, Amman, Jordan; 2School of Medicine, The University of Jordan, Amman, Jordan; 3Department of Dermatology, The Jordanian Royal Medical Services, Amman, Jordan
Correspondence: Salsabiela Bani Hamad, University of Jordan Hospital, Department of Medicine, Division of Dermatology, Queen Rania Al-Abdullah Street – Aljubeiha / P.O. Box: 13046, Amman, 11942, Jordan, Email [email protected]
Introduction: Psoriasis is a chronic immune-mediated inflammatory disorder affecting both adults and children worldwide, with an average prevalence of approximately 2%. Recent evidence suggests that several hematological inflammatory parameters and vitamin levels may serve as accessible biomarkers for disease activity and severity assessment.
Methods: This single-center retrospective case–control study was conducted at Jordan University Hospital using electronic medical record data from January 2019 to December 2023. The study included 142 patients with psoriasis and 277 age- and sex-matched controls. Psoriasis severity was assessed using the Psoriasis Area and Severity Index (PASI). Hematological inflammatory indices—including neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), and systemic immune-inflammation index (SII)—as well as vitamin D and vitamin B12 levels were evaluated.
Results: The mean age ± standard deviation was 43.76 ± 16.78 years, with no significant differences between psoriasis cases and controls. Females accounted for 54.93% of psoriasis cases compared with 54.41% of controls. The mean PASI score was 9.02 ± 9.00. Approximately 51.79% of psoriasis patients were vitamin D deficient, while 17.82% had vitamin B12 deficiency. No significant differences in psoriasis severity categories were observed across vitamin B12 or vitamin D levels (p = 0.808 and p = 0.184, respectively). The mean NLR, PLR, and SII were 2.21, 124.6, and 588,441.8, respectively. These inflammatory indices did not demonstrate statistically significant differences between psoriasis patients and controls (p > 0.05).
Conclusion: No significant associations were observed between psoriasis severity and inflammatory hematological indices (NLR, PLR, SII) or vitamin deficiencies. These findings suggest limited standalone utility of these biomarkers for routine assessment of psoriasis severity in this retrospective cohort.
Keywords: psoriasis, inflammatory parameters, PASI score, vitamin deficiencies
Introduction
Psoriasis is a chronic inflammatory immune-mediated disorder that affects adults and children worldwide, with an average prevalence of 2%.1–5 It is a multisystemic disease and is associated with multiple comorbidities,6,7 consequently imposing detrimental effects on patients’ physical and psychological well-being.8,9 The Psoriasis Area and Severity Index (PASI) is still considered the clinical gold standard for measuring disease severity.10,11 However, there is growing interest in using real-world evidence to confirm the value of objective, routinely available laboratory parameters that can supplement these clinical scores, particularly for monitoring subclinical systemic inflammation.
The pathophysiology of psoriasis is complex and still not fully understood;8 several factors play an important role in the pathogenesis of the disease, including immune dysregulation, environmental factors, and genetic susceptibility.8,12,13
Psoriasis can present with various degrees of severity, which can be assessed using the PASI score, an essential tool that enables us to assess disease severity by evaluating the degree of erythema, infiltration, and desquamation in the involved skin areas.10,11
Emerging evidence is demonstrating the potential use of several hematological parameters as diagnostic and prognostic markers.14 The neutrophil-to-lymphocyte ratio (NLR); platelet-to-lymphocyte ratio (PLR); and the systemic immune-inflammatory index (SII) are possible cost-effective markers that we could rely on as an important part of psoriasis investigations.14–16 Multiple studies established a positive association between several hematological parameters and disease severity, yet some studies failed to detect this positive correlation.14,15,17,18 This discrepancy underscores the need for further investigation to determine the true clinical utility of these markers. Although clinical scores are considered the gold standard for assessment, there is a growing demand for real-world evidence to validate routinely available laboratory parameters as objective supplements in daily practice. Such biomarkers may offer an objective complement to clinical assessment, particularly in monitoring the systemic inflammatory burden in patients treated with biologic agents, where traditional clinical signs may not fully reflect underlying disease activity.
In addition to inflammatory indices, this study investigates the correlation between PASI-determined disease severity and serum vitamin D and B12 levels. By combining these inflammatory and nutritional markers, we hope to determine whether they serve as useful biomarkers and whether regular lab tests or targeted vitamin supplements provide real clinical benefits for people with psoriasis.
Materials and Methods
Study Design and Setting
This is a single-center retrospective case–control study conducted at Jordan University Hospital. Clinical and laboratory data were extracted from the electronic medical records (EMR) for the period from January 2019 to December 2023. Investigators had full access to the EMR. No linkage with external databases was performed. Because this study was based on retrospective electronic medical record data, laboratory testing was performed according to clinical indications rather than a standardized research protocol, and residual confounding may remain.
Study Population and Participant Selection
A total of 663 patients with a diagnosis of psoriasis were initially identified in the EMR. Inclusion criteria for cases were a confirmed diagnosis of chronic plaque psoriasis and the availability of complete clinical and laboratory data. Patients with other psoriasis subtypes or incomplete data were excluded, resulting in 142 patients included in the final analysis. Age- and sex-matched controls were selected from the same EMR database at an approximate 2:1 ratio (n = 277). Controls had no history of psoriasis or other autoimmune diseases. Patients were categorized into treatment groups based on their status at the initial clinical visit. To ensure baseline accuracy, only patients who had completed their laboratory evaluations prior to the initiation of medical therapy at our center were enrolled. Controls were selected based on the absence of psoriasis and other autoimmune diseases; however, detailed chronic disease data for controls were not systematically extracted for this specific analysis.
Data regarding psoriasis disease duration were not consistently available in the electronic medical records and were therefore not included in the analysis.
Bias
Selection bias was minimized by including all eligible chronic plaque psoriasis patients with complete data and selecting age- and sex-matched controls from the same EMR. Measurement bias was reduced by using standardized PASI scoring during clinic visits and laboratory values collected prior to systemic treatment. Potential confounders, including age and sex were addressed through matching.
Variables and Data Sources
Psoriasis severity was assessed using the PASI score, a validated scoring system that evaluates erythema, induration, scaling, and affected body surface area. PASI scores were calculated during dermatology clinic visits. Severity was categorized as mild (PASI <7), moderate (PASI 7–12), and severe (PASI >12), according to previously published clinical thresholds.10,11
Laboratory variables included vitamin D, vitamin B12, and complete blood count (CBC). Vitamin D deficiency was defined as serum 25-hydroxyvitamin D levels <20 ng/mL, vitamin D insufficiency as 20–29 ng/mL, and vitamin D sufficiency as ≥30 ng/mL according to Endocrine Society guidelines. Vitamin B12 deficiency was defined according to the hospital laboratory reference range.
From the CBC results, hematological inflammatory indices were calculated. The NLR was calculated as the absolute neutrophil count divided by the absolute lymphocyte count, the PLR as platelet count divided by absolute lymphocyte count, and the SII as (neutrophil count × platelet count) divided by lymphocyte count.
Potential confounders included age, sex, and comorbidities. All variables were extracted directly from the EMR. Laboratory measurements were obtained prior to initiation of systemic therapy and were assessed using uniform methods for cases and controls.
Vitamin D and vitamin B12 measurements were performed based on clinical indications as determined by the treating physicians, rather than systematic screening. To minimize potential confounding, patients with documented hematologic disorders, chronic gastrointestinal malabsorption syndromes, or active malignancy were excluded where identifiable in the electronic records. However, due to the retrospective design, residual confounding related to unrecorded clinical indications cannot be entirely excluded.
Data Cleaning and Management
Data were reviewed for completeness and accuracy. Patients with missing clinical or laboratory data were excluded from the analyses. No formal validation of diagnostic codes was performed.
Statistical Analysis
Continuous variables were summarized as means ± standard deviations, and categorical variables as frequencies and percentages. PASI scores and vitamin levels were analyzed as continuous variables and categorized based on standard thresholds. Comparisons between cases and controls were performed using independent samples t-tests or chi-square tests, as appropriate. Odds ratios with 95% confidence intervals were calculated where applicable. Subgroup analyses were conducted according to psoriasis severity and vitamin D and B12 status. No interaction or sensitivity analyses were performed. Statistical analyses were conducted using IBM SPSS version 23 (IBM Corp., Armonk, NY, USA).
Results
Characteristics of Cases and Controls
Our study included 142 patients with psoriasis and 277 age- and gender-matched controls. The average age and standard deviation were 43.76±16.78 with insignificant differences between cases and controls (p = 0.881, Cohen’s d = - 0.02). Regarding gender, 54.93% of cases were females, compared to 54.41% of controls (p = 1, odds ratio (OR) = 1.02, [95% CI, 0.66–1.56]). The distribution of vitamin B12 levels, vitamin D levels, and recorded comorbidities among psoriasis patients is presented in Table 1. About half (51.79%) of cases were vitamin D deficient, while 17.82% were deficient in vitamin B12. Furthermore, 60% of psoriasis patients had no recorded comorbidities, with diabetes being the most common co-morbidity in 17.86% of patients.
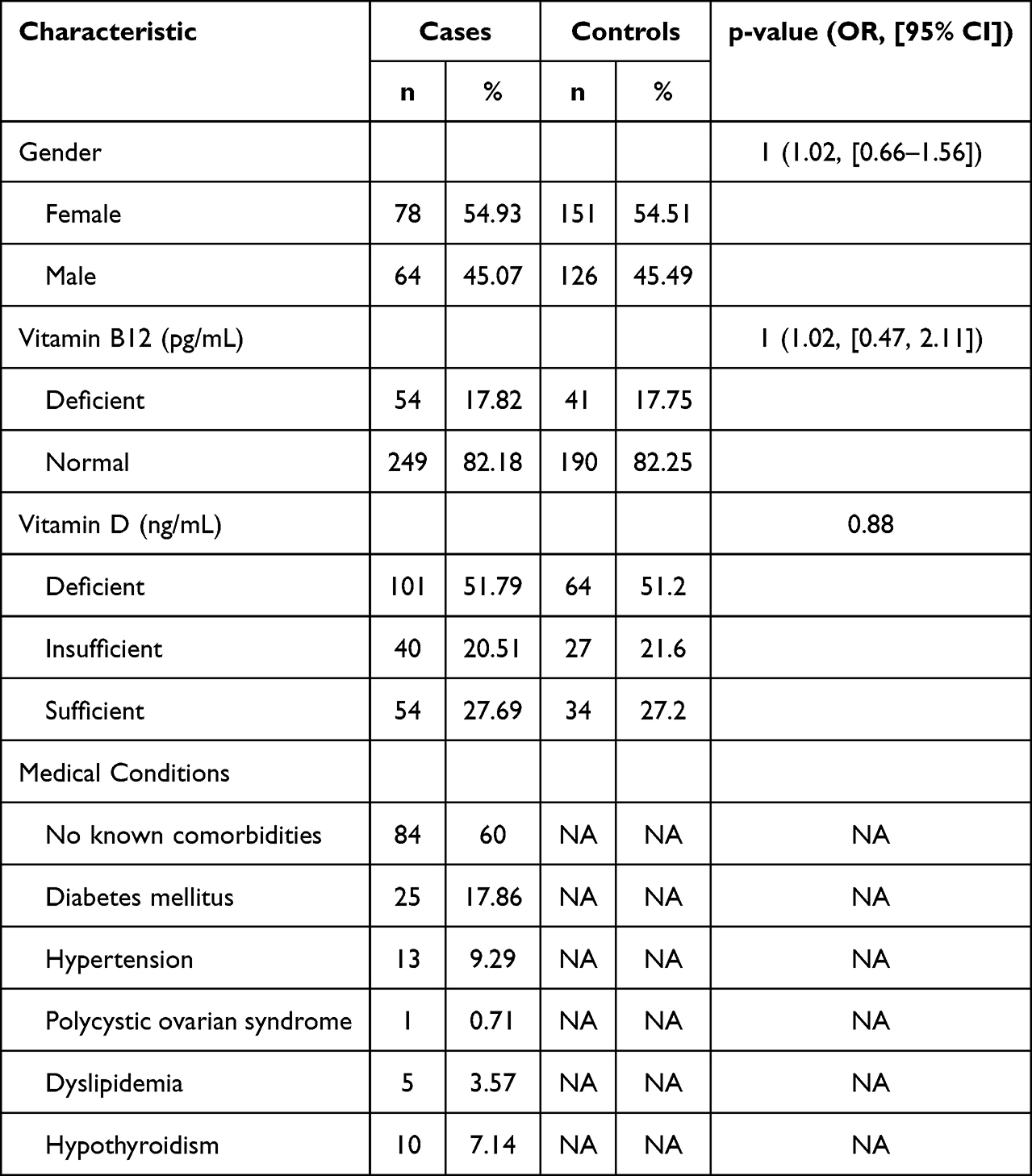 |
Table 1 Gender, Vitamin Levels, and Medical Conditions in Psoriasis Patients |
Features of Psoriasis and Clinical Predictors of Disease Severity
Among psoriasis patients, 36.43% and 23.57% were receiving topical and systemic therapy, respectively (Figure 1A). The average PASI score and standard deviation were 9.02±9.00, with 42.14% experiencing a moderate-to-severe disease (Figure 1B). Less than one in ten (7.09%) of psoriasis patients had psoriatic arthritis (Figure 1C). Gender was not associated with PASI scores or severity categories (p > 0.05).
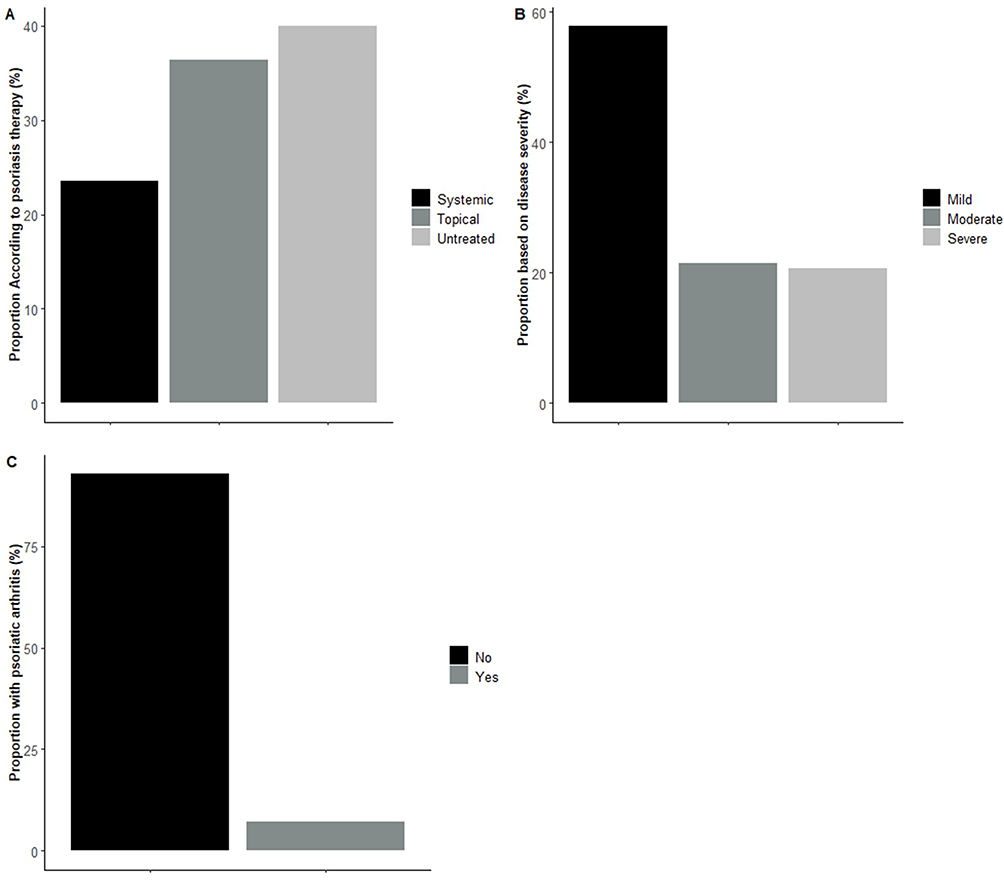 |
Figure 1 Psoriasis characteristics among participants. (A) Distribution of psoriasis treatment modalities (systemic, topical, and untreated). (B) Distribution of psoriasis severity (mild, moderate, and severe). (C) Presence of psoriatic arthritis among participants (yes or no). |
Independent t-test highlighted a significant association between hypertension and PASI scores (p = 0.024, Cohen’s d = 0.58), with a lower mean score in hypertensive people compared to others. Chi-square analysis based on categories of severity was insignificant with hypertension (p = 0.08). Additionally, both mean-based and category-based analyses revealed non-significant variations in PASI scores among individuals who had no recorded comorbidities or patients who had conditions such as diabetes mellitus, hypertension, dyslipidemia, hypothyroidism, or psoriatic arthritis (p > 0.05, Table 2).
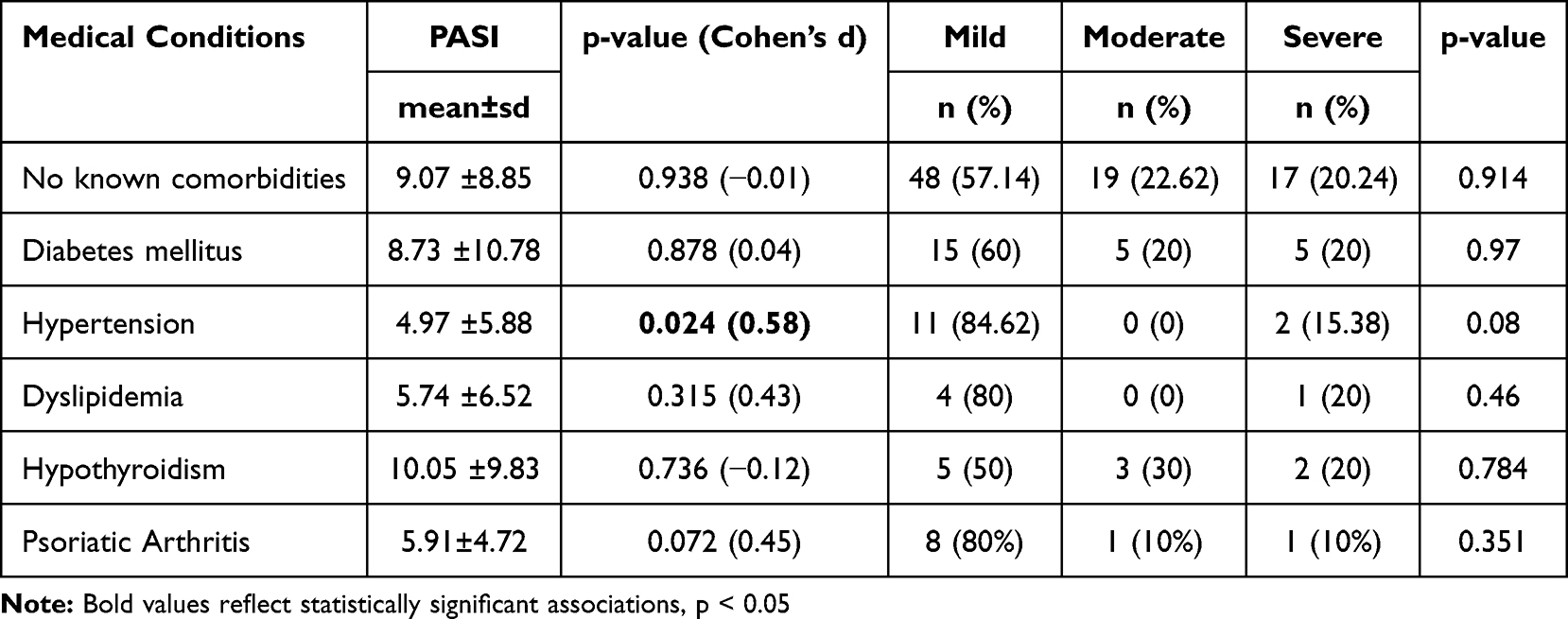 |
Table 2 The Impact of Medical Conditions on Psoriasis Severity |
Among patients with deficient vitamin B12 levels, 25% had severe psoriasis compared to 17.2% of patients with normal vitamin B12 levels (Figure 2A). In terms of vitamin D levels, 27.8% of patients with deficient levels, 15.4% with insufficient levels, and 5.26% with sufficient levels exhibited severe psoriasis (Figure 2B). Chi-square analysis showed insignificant differences in severity category across vitamin B12 and vitamin D levels (p = 0.808 and p = 0.184, respectively). In line, pairwise independent t-test revealed insignificant differences in mean measurements of vitamin B12 and vitamin D across severity categories (p > 0.05).
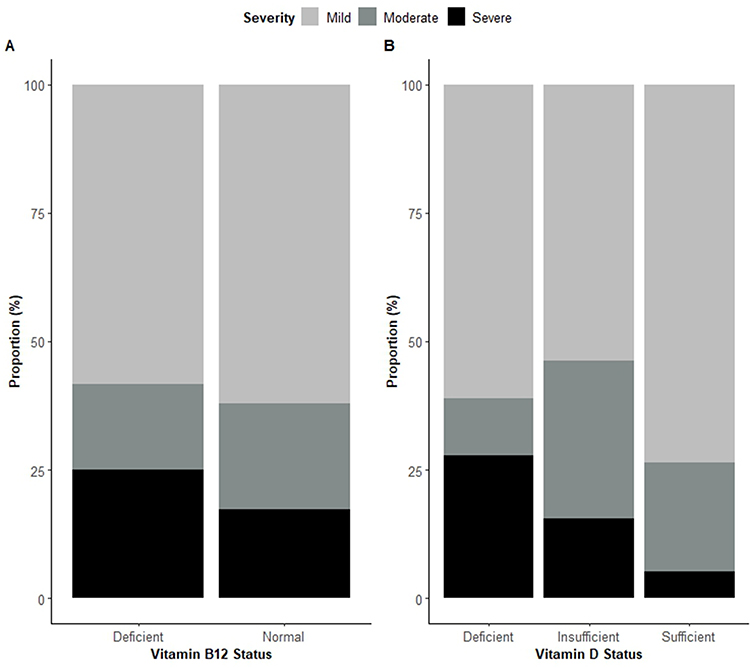 |
Figure 2 Vitamin deficiencies and psoriasis severity. (A) Distribution of psoriasis severity according to Vitamin B12 status (deficient vs normal). (B) Distribution of psoriasis severity according to Vitamin D status (deficient, insufficient, and sufficient). |
Immune Cell Counts and Ratios Correlation with Case Status and Psoriasis Severity
The mean neutrophil and lymphocyte counts were 4604.77 cells/µL and 2350.73 cells/µL, respectively. However, these parameters exhibited no significant differences when comparing cases and controls (p > 0.05). When examining the neutrophil counts in untreated patients compared to patients receiving topical or systemic therapy, insignificant differences were observed (p = 0.897 and p = 0.994, respectively). On the other hand, lower lymphocytes counts were observed in untreated patients when compared to patients receiving topical treatment (p = 0.047, Cohen’s d = −0.47).
The mean NLR, PLR, and SII were found to be 2.21, 124.6, and 588441.8, respectively. However, these parameters exhibited no significant statistical differences between cases and controls (p > 0.05, Figure 3). Similarly, both pairwise t-tests and ROC analyses failed to reveal any correlation between NLR, PLR, SII, and PASI scores. Additionally, CRP and ESR showed no significant differences between cases and controls, nor did they demonstrate variation across PASI severity categories. The lack of association with disease severity was also observed after subsetting by treatment category (p > 0.05, Figure 4).
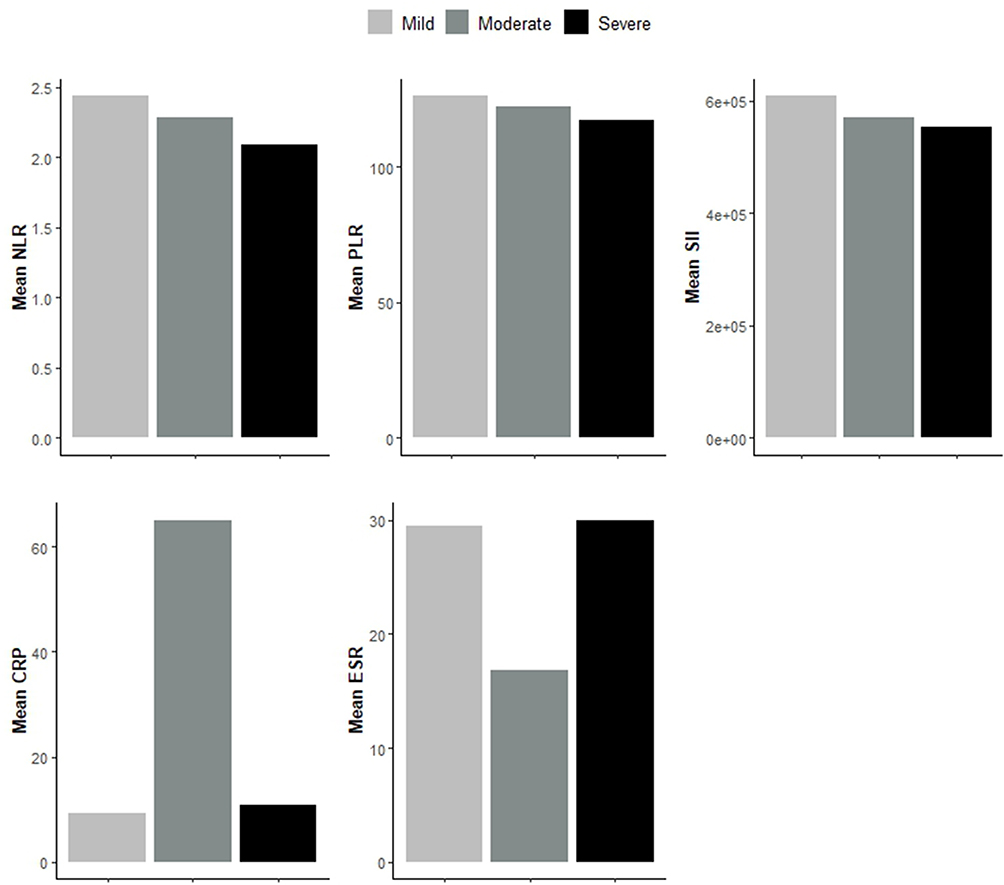 |
Figure 3 Average immune cell ratios and inflammatory markers in cases and controls. |
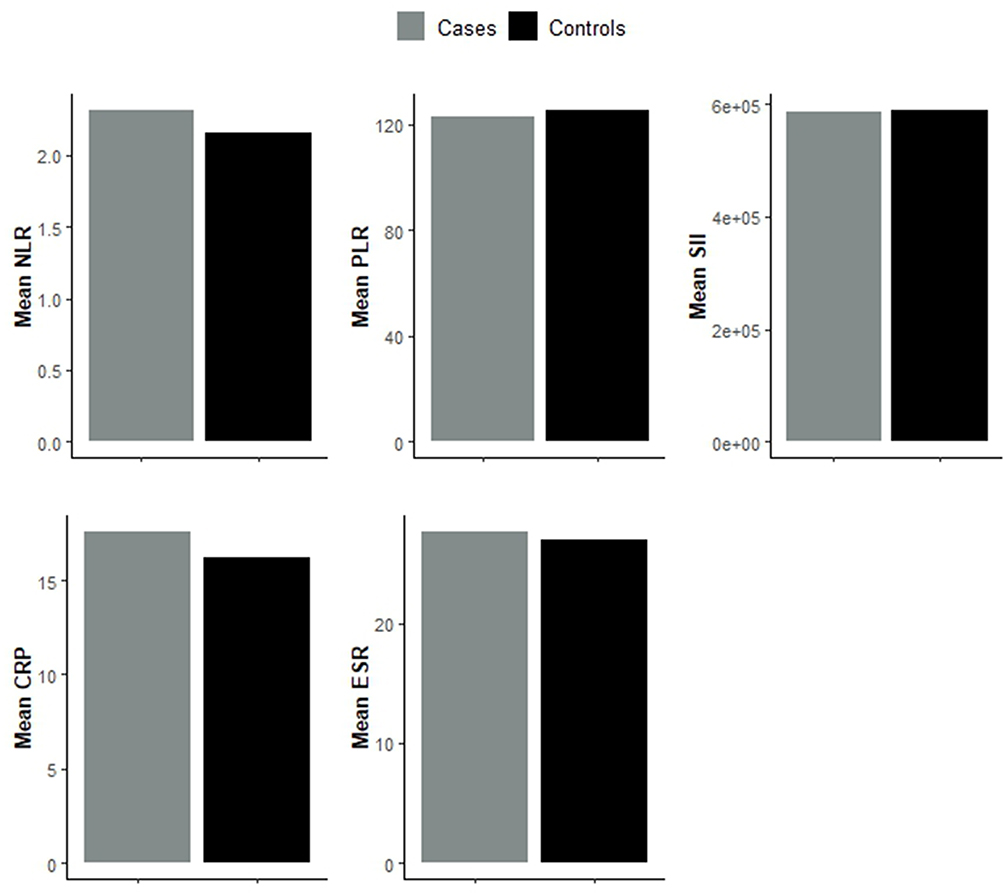 |
Figure 4 Average immune cell ratios and inflammatory markers according to disease severity. |
Immune Cell Ratios Correlation with Vitamin B12 and Vitamin D Deficiency
The correlation between immune cell ratios and vitamin B12 and vitamin D deficiency was examined. In both the total sample and cases, no significant differences in immune cell ratios were found across categories of vitamin D levels (all p > 0.05). Similarly, neither PLR nor SII showed associations with vitamin B12 deficiency in either the overall sample or cases (all p > 0.05). However, NLR was notably higher in vitamin B12-deficient cases compared to those with normal vitamin B12 levels (2.32±1.67 vs 2.02±1.31, p = 0.044, Cohen’s d = 0.2).
Discussion
Psoriasis is a chronic inflammatory multisystemic immune-mediated disorder, that is associated with multiple comorbidities.6,7,19,20 Although the exact etiology of the disease is complex and remains unclear, it was proven that multiple factors significantly contribute to the pathogenesis including autoimmune mechanisms, genetic susceptibility, and environmental factors.3,8,12,13 Chronic inflammation plays a pivotal role in psoriasis pathogenesis.12,21,22 The inflammatory mediators can extend beyond the skin, affecting various organ systems, including the hematopoietic system.23
Elevated white blood cell counts, particularly neutrophilia, have been frequently observed in psoriasis patients.24 Neutrophils are key players in the inflammatory cascade, contributing to tissue damage and exacerbating psoriatic lesions.25 In a study conducted by Rodriguez-Rosales et al, it was mentioned that there is a unique neutrophil profile in the circulation of psoriasis patients, and it highlighted the dominant contribution of neutrophil-mediated inflammation, which can be a valuable target for future therapeutic interventions.26 Moreover, it was proven that T lymphocytes have a crucial part in the development of the disease.27 Nevertheless, the prevalence of lymphopenia was higher in patients with psoriasis compared to healthy patients in a hospital-based cross-sectional study conducted by Wang et al.27
Recently, multiple studies investigated the correlation between inflammatory parameters and psoriasis.14–16,18,28 Some divergent and inconsistent results were obtained, but the majority of the literature signified a positive association between the aforementioned parameters. An observational study that was conducted in the US, analyzed data from a large cohort of participants,14 and denoted the presence of a positive correlation between NLR and disease severity.14 Furthermore, a significant positive correlation between NLR and PASI score was found in a case-control study carried out in Ho Chi Minh City Hospital.28 However, a meta-analysis conducted by Paliogiannis et al suggested that there is a significant correlation between NLR, PLR, and the presence of psoriasis, but not its severity18 Another study failed to detect a positive association between PASI scores and NLR or PLR, this discrepancy was thought to be due to the fact NLR and PLR reflect the inflammatory status of the patient, not the severity.15
Concerning SII, multiple studies found significantly higher values in psoriasis patients.29–31 Moreover, it was identified as a prognostic inflammatory indicator for psoriasis and psoriatic arthritis based on a study conducted by Yorulmaz et al, where a positive correlation was found between SII and both PASI scores and psoriatic arthritis.16 Another study found significantly higher values of SII among patients with PASI ≥ 4.5, and also among patients with involvement of nails and genitalia.32 Additionally, SII values were significantly higher among pustular psoriasis when compared to other subtypes in a study conducted by Ibrahim et al.33 On the other hand, a study conducted in China found a higher level of SII among psoriasis patients, but no significant correlation between its level and psoriasis severity.31 In our study, NLR, PLR, and SII exhibited no significant statistical differences between cases and controls, and no correlation between the aforementioned parameters and PASI scores. Recent real-world studies have also evaluated routinely available hematological indices as potential predictors of treatment response and safety in biologic-treated psoriasis cohorts. In particular, analyses involving monoclonal antibodies such as guselkumab and bimekizumab have explored whether baseline inflammatory markers may help predict therapeutic outcomes or adverse events. These findings suggest that although simple inflammatory indices may not consistently correlate with baseline disease severity, their potential role in longitudinal monitoring and treatment stratification warrants further investigation. Therefore, the clinical utility of these markers may depend more on dynamic assessment over time rather than cross-sectional severity evaluation alone.34,35
The association between psoriasis severity and vitamin D level was also investigated in numerous studies.36,37 A case-control study reported that serum vitamin D levels were significantly lower in psoriasis patients, in addition to finding a significant negative correlation between vitamin D level and PASI score.36 Similarly, a meta-analysis that was conducted by Hollis et al identified that psoriasis patients have lower levels of vitamin D, yet their PASI scores failed to improve after vitamin D supplementation.37 Additionally, vitamin B12 levels among psoriasis patients were assessed in multiple studies.38–42 Most of the studies did not find significant differences between psoriasis patients and controls, which aligns with our study findings.38,40,41 Moreover, a trial of vitamin B12 injections did not show any benefit among psoriasis patients.43 On the other hand, some studies found a significantly lower vitamin B12 level among psoriasis patients,39,42 but there was no significant correlation with psoriasis severity.39 Our study revealed insignificant differences in mean measurements of vitamin B12 and vitamin D between cases and controls, nor across psoriasis severity categories. The NLR correlation with vitamin D and vitamin B12 deficiencies was studied in multiple inflammatory and metabolic conditions.44–47 Multiple studies found a significant negative correlation between vitamin D level and NLR.44,46,47 Baş et al found the rate of NLR higher in vitamin D deficiency patients,44 and Wang et al found the NLR ratio significantly higher among diabetic and prediabetic patients who are vitamin D deficient.46 Additionally, a study in Turkey found no significant correlation between vitamin B12 deficiency and NLR.45 Interestingly, NLR was notably higher in vitamin B12-deficient but not vitamin D-deficient psoriasis patients compared to those with psoriasis patients who have normal vitamin levels in our study.
Limitation
This is a single-center retrospective study, and the study sample was small. Routinely collected EMR data were used, which were not originally created to answer our research question, potentially introducing misclassification, unmeasured confounding, and missing data. Future iterations of the study could include a prospective design with a larger sample among multiple hospitals to clarify the association between these hematological parameters and disease severity, reflected in the PASI score. This will consequently provide valuable evidence for potential improvements in the diagnostic and therapeutic monitoring of the disease.
Conclusion
In conclusion, the hematological and nutritional markers we studied showed limited ability to predict psoriasis severity on their own in our real-world group. However, this does not mean they lack clinical value. Our results show that these biomarkers are complex and may be more useful when combined with other clinical and laboratory measures in broader assessment models. More prospective studies are needed to better understand their role in different patient groups and to see how they can support current treatment monitoring, especially for patients on systemic and biologic therapies.
Data Sharing Statement
The study protocol and SPSS analysis code are available from the corresponding author upon request. Raw patient-level EMR data cannot be shared due to privacy regulations. Aggregated data supporting the findings are included in the article.
Ethical Considerations
The Institutional Review Board of Jordan University Hospital, The University of Jordan, Amman, Jordan (IRB No. 10/2023/17426) approved this study. The study was conducted in accordance with the ethical standards of the Declaration of Helsinki. Given the retrospective case–control design of the study and the use of anonymized patient data, the requirement for written informed consent was waived by the IRB.
Author Contributions
Rand Murshidi – Conceptualization, Supervision, Validation, Writing – Review & Editing.
Salsabiela Bani Hamad – Data Curation, Investigation, Writing – Original Draft, Writing – Review & Editing.
Assem Al Refaei – Methodology, Formal Analysis, Software, Writing – Original Draft, Writing – Review & Editing.
Nour Shewaikani – Methodology, Formal Analysis, Software, Writing – Original Draft, Writing – Review & Editing.
Dina A. Al-Nusair – Investigation, Data Curation, Writing – Original Draft.
Hind B. Abu Tawileh – Investigation, Data Curation, Writing – Original Draft.
Muayyad Murshidi – Validation, Supervision, Writing – Review & Editing.
Hussam I. A. Alzeerelhouseini – Investigation, Writing - Original Draft, Writing – Review & Editing.
All authors took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that they have not received any funding for this work.
Disclosure
The authors declare that they have no competing interests.
References
1. Zhou G, Ren X, Tang Z, et al. Exploring the association and causal effect between white blood cells and psoriasis using large-scale population data. Front Immunol. 2023;14:1043380. doi:10.3389/fimmu.2023.1043380
2. Boehncke WH, Schön MP. Psoriasis. Lancet. 2015;386(9997):983–11. doi:10.1016/S0140-6736(14)61909-7
3. Dopytalska K, Ciechanowicz P, Wiszniewski K, Szymańska E, Walecka I. The role of epigenetic factors in psoriasis. Int J Mol Sci. 2021;22(17):9294. doi:10.3390/ijms22179294
4. Griffiths CEM, Armstrong AW, Gudjonsson JE, Barker JNWN. Psoriasis. Lancet. 2021;397(10281):1301–1315. doi:10.1016/S0140-6736(20)32549-6
5. Parisi R, Iskandar IYK, Kontopantelis E, Augustin M, Griffiths CEM, Ashcroft DM. National, regional, and worldwide epidemiology of psoriasis: systematic analysis and modelling study. BMJ. 2020;m1590. doi:10.1136/bmj.m1590
6. Lotti T, Hercogova J, Prignano F. The concept of psoriatic disease: can cutaneous psoriasis any longer be separated by the systemic comorbidities? Dermatol Ther. 2010;23(2):119–122. doi:10.1111/j.1529-8019.2010.01305.x
7. Kim N, Thrash B, Menter A. Comorbidities in psoriasis patients. Semin Cutan Med Surg. 2010;29(1):10–15. doi:10.1016/j.sder.2010.01.002
8. Armstrong AW, Read C. Pathophysiology, clinical presentation, and treatment of psoriasis. JAMA. 2020;323(19):1945. doi:10.1001/jama.2020.4006
9. Blackstone B, Patel R, Bewley A. Assessing and improving psychological well-being in psoriasis: considerations for the clinician. Psoriasis. 2022;12:25–33. doi:10.2147/PTT.S328447
10. Papp KA, Lebwohl MG, Kircik LH, et al. The proposed PASI-HD provides more precise assessment of plaque psoriasis severity in anatomical regions with a low area score. Dermatol Ther. 2021;11(4):1079–1083. doi:10.1007/s13555-021-00572-2
11. Pasic L, Dzananovic N, Gojak R, et al. Psoriasis area and severity index (PASI) objectivisation by flow cytometry analysis of major lymphocytes subsets. Acta Inform Med. 2023;31(3):206. doi:10.5455/aim.2023.31.206-210
12. Nestle FO, Kaplan DH, Barker J. Psoriasis. N Engl J Med. 2009;361(5):496–509. doi:10.1056/NEJMra0804595
13. Rendon A, Schäkel K. Psoriasis pathogenesis and treatment. Int J Mol Sci. 2019;20(6):1475. doi:10.3390/ijms20061475
14. Hong J, Lian N, Li M. Association between the neutrophil-to-lymphocyte ratio and psoriasis: a cross-sectional study of the national health and nutrition examination survey 2011–2014. BMJ Open. 2023;13(12):e077596. doi:10.1136/bmjopen-2023-077596
15. Wang WM, Wu C, Gao YM, Li F, Yu XL, Jin HZ. Neutrophil to lymphocyte ratio, platelet to lymphocyte ratio, and other hematological parameters in psoriasis patients. BMC Immunol. 2021;22(1):64. doi:10.1186/s12865-021-00454-4
16. Yorulmaz A, Hayran Y, Akpinar U, Yalcin B. Systemic immune-inflammation index (SII) predicts increased severity in psoriasis and psoriatic arthritis. Curr Health Sci J. 2020;46(4):352–357. doi:10.12865/CHSJ.46.04.05
17. Şener G, Inan Yuksel E, Gökdeniz O, Karaman K, Canat HD. The relationship of hematological parameters and C-reactive protein (CRP) with disease presence, severity, and response to systemic therapy in patients with psoriasis. Cureus. 2023. doi:10.7759/cureus.43790
18. Paliogiannis P, Satta R, Deligia G, et al. Associations between the neutrophil-to-lymphocyte and the platelet-to-lymphocyte ratios and the presence and severity of psoriasis: a systematic review and meta-analysis. Clin Exp Med. 2019;19(1):37–45. doi:10.1007/s10238-018-0538-x
19. Griffiths CE, Barker JN. Pathogenesis and clinical features of psoriasis. Lancet. 2007;370(9583):263–271. doi:10.1016/S0140-6736(07)61128-3
20. Machado-Pinto J, Dos S Diniz M, Bavoso NC. Psoriasis: new comorbidities. An Bras Dermatol. 2016;91(1):8–14. doi:10.1590/abd1806-4841.20164169
21. Gisondi P, Bellinato F, Girolomoni G, Albanesi C. Pathogenesis of chronic plaque psoriasis and its intersection with cardio-metabolic comorbidities. Front Pharmacol. 2020;11. doi:10.3389/fphar.2020.00117
22. Campanati A, Marani A, Martina E, Diotallevi F, Radi G, Offidani A. Psoriasis as an immune-mediated and inflammatory systemic disease: from pathophysiology to novel therapeutic approaches. Biomedicines. 2021;9(11):1511. doi:10.3390/biomedicines9111511
23. Ahlehoff O, Gislason GH, Lindhardsen J, et al. Psoriasis carries an increased risk of venous thromboembolism: a Danish nationwide cohort study. PLoS One. 2011;6(3):e18125. doi:10.1371/journal.pone.0018125
24. Lowes MA, Suárez-Fariñas M, Krueger JG. Immunology of Psoriasis. Annu Rev Immunol. 2014;32(1):227–255. doi:10.1146/annurev-immunol-032713-120225
25. Alavi A, Sajic D, Cerci FB, Ghazarian D, Rosenbach M, Jorizzo J. Neutrophilic dermatoses: an update. Am J Clin Dermatol. 2014;15(5):413–423. doi:10.1007/s40257-014-0092-6
26. Rodriguez-Rosales YA, Langereis JD, Gorris MAJ, et al. Immunomodulatory aged neutrophils are augmented in blood and skin of psoriasis patients. J Allergy Clin Immunol. 2021;148(4):1030–1040. doi:10.1016/j.jaci.2021.02.041
27. Hawkes JE, Chan TC, Krueger JG. Psoriasis pathogenesis and the development of novel targeted immune therapies. J Allergy Clin Immunol. 2017;140(3):645–653. doi:10.1016/j.jaci.2017.07.004
28. Nguyen HT, Vo LDH, Pham NN. Neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios as inflammatory markers in psoriasis: a case-control study. Dermatol Reports. 2022. doi:10.4081/dr.2022.9516
29. Melikoglu M, Pala E. Systemic immune-inflammation index as a biomarker of psoriasis severity. Archiv Basic Clin Res. 2023. doi:10.5152/ABCR.2023.22124
30. Zhao X, Li J, Li X. Association between systemic immune-inflammation index and psoriasis: a population-based study. Front Immunol. 2024;15:1305701. doi:10.3389/fimmu.2024.1305701
31. Ma R, Cui L, Cai J, et al. Association between systemic immune inflammation index, systemic inflammation response index and adult psoriasis: evidence from NHANES. Front Immunol. 2024;15:1323174. doi:10.3389/fimmu.2024.1323174
32. Dincer Rota D, Tanacan E. The utility of systemic-immune inflammation index for predicting the disease activation in patients with psoriasis. Int J Clin Pract. 2021;75(6). doi:10.1111/ijcp.14101
33. Ibrahim SH, Guan M, Li S. Systemic immune inflammatory index is associated with pustular psoriasis: a single center retrospective study. J Cosmet Dermatological Sci Appl. 2022;12(04):174–186. doi:10.4236/jcdsa.2022.124015
34. Fratton Z, Bighetti S, Bettolini L, et al. Real-world experience of guselkumab in the elderly population. Psoriasis. 2025;15:581–601. doi:10.2147/PTT.S549502
35. Fratton Z, Bighetti S, Bettolini L, et al. Real-world experience of bimekizumab in a cohort of 109 patients over 48 weeks and identification of predictive factors for an early super response and risk of adverse events. Psoriasis. 2025;15:145–158. doi:10.2147/PTT.S514249
36. Pokharel R, Agrawal S, Pandey P, Lamsal M. Assessment of vitamin D level in patients with psoriasis and its correlation with disease severity: a case–control study. Psoriasis. 2022;12:251–258. doi:10.2147/PTT.S369426
37. Formisano E, Proietti E, Borgarelli C, Pisciotta L. Psoriasis and vitamin D: a systematic review and meta-analysis. Nutrients. 2023;15(15):3387. doi:10.3390/nu15153387
38. Tsai T-Y, Yen H, Huang Y-C. Serum homocysteine, folate and vitamin B 12 levels in patients with psoriasis: a systematic review and meta-analysis. Br J Dermatol. 2019;180(2):382–389. doi:10.1111/bjd.17034
39. Sharaf ESFA, Ghanem BM, Marzouk HF, Abd El Aziz YEM. Serum homocysteine, folic acid and vitamin B12 levels in patients with psoriasis vulgaris. Egypt J Hosp Med. 2022;88(1):3304–3309. doi:10.21608/ejhm.2022.248195
40. Abedini R, Goodarzi A, Saeidi V, et al. Serum homocysteine level, vitamin B12 levels, and erythrocyte folate in psoriasis: a case-control study. Int J Womens Dermatol. 2019;5(3):171–174. doi:10.1016/j.ijwd.2018.12.004
41. Uslu M, Şendur N, Şavk E, et al. Blood homocysteine, folic acid, vitamin B12 and vitamin B6 levels in psoriasis patients. Turkderm. 2017:92–97. doi:10.4274/turkderm.22566
42. Brazzelli V, Grasso V, Fornara L, et al. Homocysteine, vitamin B 12 and folic acid levels in psoriatic patients and correlation with disease severity. Int J Immunopathol Pharmacol. 2010;23(3):911–916. doi:10.1177/039463201002300327
43. Baker H, Comaish JS. Is vitamin B12 of value in psoriasis? BMJ. 1962;2(5321):1729–1730. doi:10.1136/bmj.2.5321.1729
44. Yildirim Baş F, Arslan B. The association between the neutrophil lymphocyte ratio and vitamin D levels. Turkish J Fam Med Prim Care. 2018;12(2):88–91. doi:10.21763/tjfmpc.432455
45. Durmaz A. Evaluation of whole blood, mean platelet volume (MPV) and neutrophil-lymphocyte ratios (NLR) in people with B12 vitamin deficiency. Family Pract Palliative Care. 2022;7(2):30–35. doi:10.22391/fppc.1032712
46. Wang S, Shen T, Xi B, Shen Z, Zhang X. Vitamin D affects the neutrophil-to-lymphocyte ratio in patients with type 2 diabetes mellitus. J Diabetes Investig. 2021;12(2):254–265. doi:10.1111/jdi.13338
47. Akbas EM, Gungor A, Ozcicek A, Akbas N, Askin S, Polat M. Vitamin D and inflammation: evaluation with neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio. Arch Med Sci. 2016;4:721–727. doi:10.5114/aoms.2015.50625
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.