Back to Journals » Clinical Ophthalmology » Volume 14
Retinal Microvasculature Changes After Repair of Macula-off Retinal Detachment Assessed with Optical Coherence Tomography Angiography
Authors McKay KM, Vingopoulos F ![]() , Wang JC, Papakostas TD, Silverman RF, Marmalidou A, Lains I
, Wang JC, Papakostas TD, Silverman RF, Marmalidou A, Lains I ![]() , Eliott D, Vavvas DG, Kim LA
, Eliott D, Vavvas DG, Kim LA ![]() , Wu DM, Miller JB
, Wu DM, Miller JB ![]()
Received 7 May 2019
Accepted for publication 12 May 2020
Published 26 June 2020 Volume 2020:14 Pages 1759—1767
DOI https://doi.org/10.2147/OPTH.S214623
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
K Matthew McKay,1,* Filippos Vingopoulos,1,* Jay C Wang,1 Thanos D Papakostas,1,2 Rebecca F Silverman,1 Anna Marmalidou,1 Inês Lains,1 Dean Eliott,1 Demetrios G Vavvas,1 Leo A Kim,1 David M Wu,1 John B Miller1
1Retina Service, Massachusetts Eye and Ear, Department of Ophthalmology, Harvard Medical School, Boston, MA, USA; 2Retina Service, Weill Cornell Medical College, New York, NY, USA
*These authors contributed equally to this work
Correspondence: John B Miller
Retina Service, Massachusetts Eye and Ear, Harvard Medical School, 243 Charles St, Boston, MA 02114 Tel +1 (617) 573-3750
Fax +1 (617) 573-3698
Email [email protected]
Objective: To characterize the microvascular retinal changes after repair of macula-off rhegmatogenous retinal detachment (RRD) using optical coherence tomography angiography (OCT-A).
Patients and Methods: A retrospective review of patients who underwent repair of macula-off RRD. Fellow unaffected eyes were used as controls. Post-operative OCT-A allowed comparison of vessel density (VD) and foveal avascular zone (FAZ) area in the superficial and deep retinal capillary plexus (DCP) as well as VD in the choriocapillaris layer.
Results: Seventeen eyes of 17 RRD patients were included in the final analysis. There was a reduction in VD of the deep retinal capillary plexus in affected eyes compared to fellow eyes (p = 0.046). RRD eyes with reduced VD in DCP compared with their fellow control eyes had worse visual acuity after repair compared to those without (p = 0.032). No significant microvasculature changes were detected in the FAZ area and VD in the superficial capillary plexus and choriocapillaris compared to fellow eyes.
Conclusion: In macula-off RRD eyes, significant microvascular changes were detected in the DCP using OCT-A even after successful anatomical repair. Decreased VD in the DCP compared to the fellow healthy eyes was correlated with worse visual acuity.
Keywords: microvascular changes, OCT-angiography, macula-off retinal detachment
Background and Objective
While anatomic success for retinal reattachment after macula involving (mac-off) rhegmatogenous retinal detachment (RRD) is reported as near or greater than 90%,1–6 there is a wider range of outcomes for final visual acuity. Most large series demonstrate that approximately 40% of patients will attain visual acuity of 20/50 or better.4,7
A number of studies have utilized optical coherence tomography (OCT) imaging for enhanced evaluation of the retinal microstructure in the post-operative period, identifying features that correlate with visual outcome.8–11 These have included outer retinal layer abnormalities, such as loss of external limiting membrane integrity, disruption of ellipsoid zone (EZ), and decreased photoreceptor outer segment length. Although there have been several older studies on the effect of retinal detachment (RD) on vascular flow,12–17 there is less known about the association between vascular changes and final visual acuity.18–21
OCT-Angiography (OCT-A) provides in vivo, non-invasive imaging of real-time blood flow through the retinal and choroidal vasculature. It has been extensively investigated in macular degeneration, retinal vein occlusion, diabetic retinopathy, posterior uveitis and optic neuropathies.22–27 Recently, few reports investigated OCT-A parameters after mac-on28–30 or mac-off28,29,31,32 RD repair including vascular density (VD) and FAZ area and correlated those with visual function. Building on those reports, we herein employed OCT-A to evaluate microvascular changes in the superficial (SCP) and deep capillary plexuses (DCP), choriocapillaris and the FAZ area and their correlation with final best corrected visual acuity (BCVA) in eyes after mac-off RRD repair using the fellow eyes as controls.
Patients/Materials and Methods
We conducted a retrospective review of consecutive patients with a diagnosis of mac-off RRD with foveal detachment who underwent primary repair with pars plana vitrectomy (PPV) by two surgeons (JBM, DW) from November 2015 to August 2017, and who had been imaged with OCT-A. Institutional Review Board approval was obtained from the Massachusetts Eye and Ear Human Studies Committee and the study adhered to the tenets of the Declaration of Helsinki. Informed consent was waived in the present study due to its retrospective nature and data were de-identified to protect patient confidentiality.
Exclusion criteria were eyes with traumatic or tractional RD, previously diagnosed retinal pathology or poor quality OCT-A imaging data, as assessed by an experienced grader (JCW). Only eyes with single surgery anatomic success were included. The unaffected, fellow eyes were used as controls. From medical records, we collected demographic and clinical data, such as patient age, sex, and systemic comorbidities. Each patient had visual acuity assessment and complete ophthalmic examination pre- and post-operatively. OCT-A imaging was acquired on the Optovue Avanti SD-OCT system (Optovue, Inc, Fremont, CA, USA) in both eyes during post-operative visits after resolution of the intravitreal gas bubble. Final best corrected visual acuity was recorded at the most recent follow-up.
For image analysis, we exported the OCT-A images (3mm x 3mm) of the superficial and deep retinal capillaries, and choriocapillaris; and then imported them into ImageJ (National Institute of Health, Bethesda, Maryland, USA). Using this software, we converted them to 8 bit images, binarized them using the “Otsu” algorithm, and then skeletonized them using ImageJ to control for individual vessel thickness (see Figure 1). Capillary vessel density (VD) was calculated as the percent area occupied by the vessels. The foveal avascular zone (FAZ) of both superficial and deep retinal capillary images was outlined manually with the polygon function, and the FAZ area was subsequently calculated for both layers. Image analysis was conducted by one author who was masked to the affected RRD eye (JCW).
 |
Figure 1 Sample OCT-A images of a control, non-RRD left eye of an affected patient. The top row shows superficial retinal capillary plexus. The bottom row shows deep retinal capillary plexus. Left most images represent raw data. Second column images show manually outlined FAZs. Third column images show binarized images. Right most images show skeletonized data on which vessel density was calculated. |
All statistics were performed using the computing environment R (R Core Team, 2017, Vienna, Austria). Paired T-test analysis was used to compare capillary VD and FAZ in eyes affected by RRD and unaffected control eyes. Wilcoxon rank-sum test analysis was used to compare RRD eyes with and without decreased deep capillary VD. A multivariate analysis with dependent variables the VD OCT-A parameters and independent variables the time interval from the RD repair to OCT-A acquisition and to BCVA measurement was performed.
Results
Demographics
Seventeen eyes of 17 patients with macula-off RRD were included in the final analysis. The respective healthy fellow eyes were used as controls. Demographic characteristics are shown in Table 1. Two patients were excluded from analysis for preexisting retinal pathology, and one for chronic RRD which underwent repair by PPV and scleral buckle (SB). The mean age was 57 years (standard deviation 11 years, range 25 to 69 years) and the average time from presentation with RRD to repair was 3 days (range 0–6). The mean post-operative follow-up was 8 months (range 1 to 23 months), and OCT-A was obtained on average 4 months after repair (range 1 to 16 months). Table 2 provides a summary of the individual RRD eyes data sorted by final visual acuity from best to worst. Of the 17 included RRD eyes, 11 were phakic and 6 were pseudophakic at the time of RD repair. Four of these 11 initially phakic patients had undergone cataract extraction with intraocular lens implantation after RD repair by the time of their OCT-A assessment. Table 3 provides individual data for the fellow unaffected eyes.
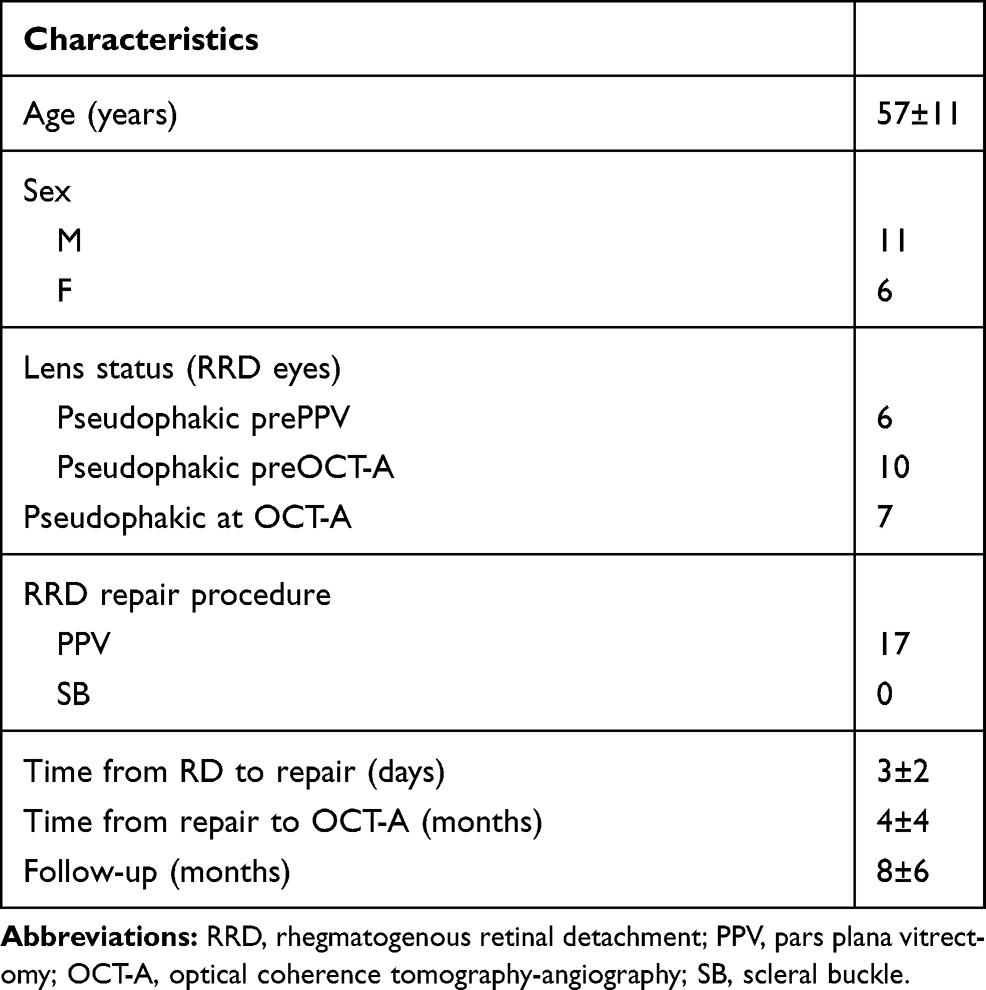 |
Table 1 Demographics and Clinical Characteristics |
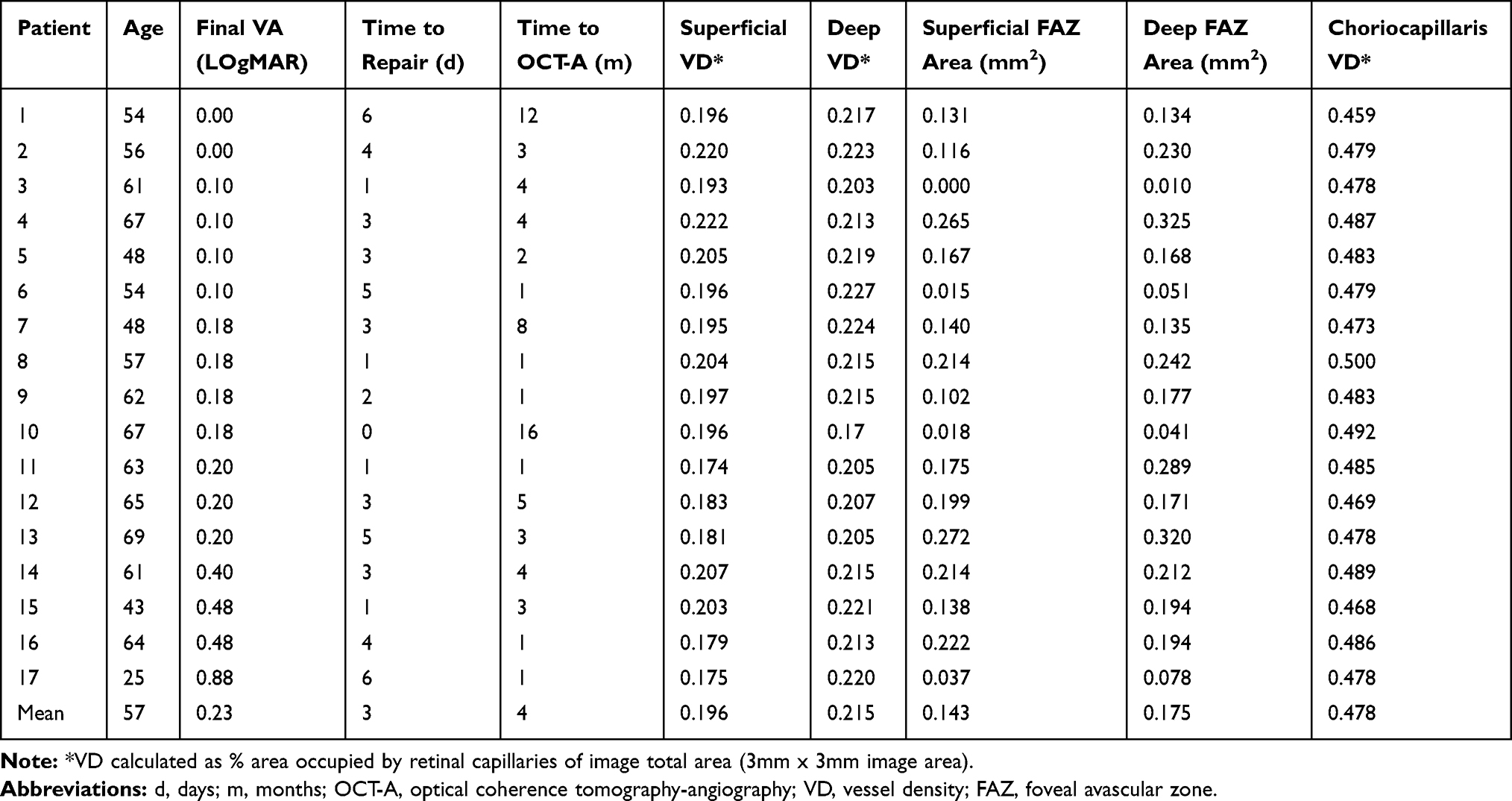 |
Table 2 Data for RRD Eyes |
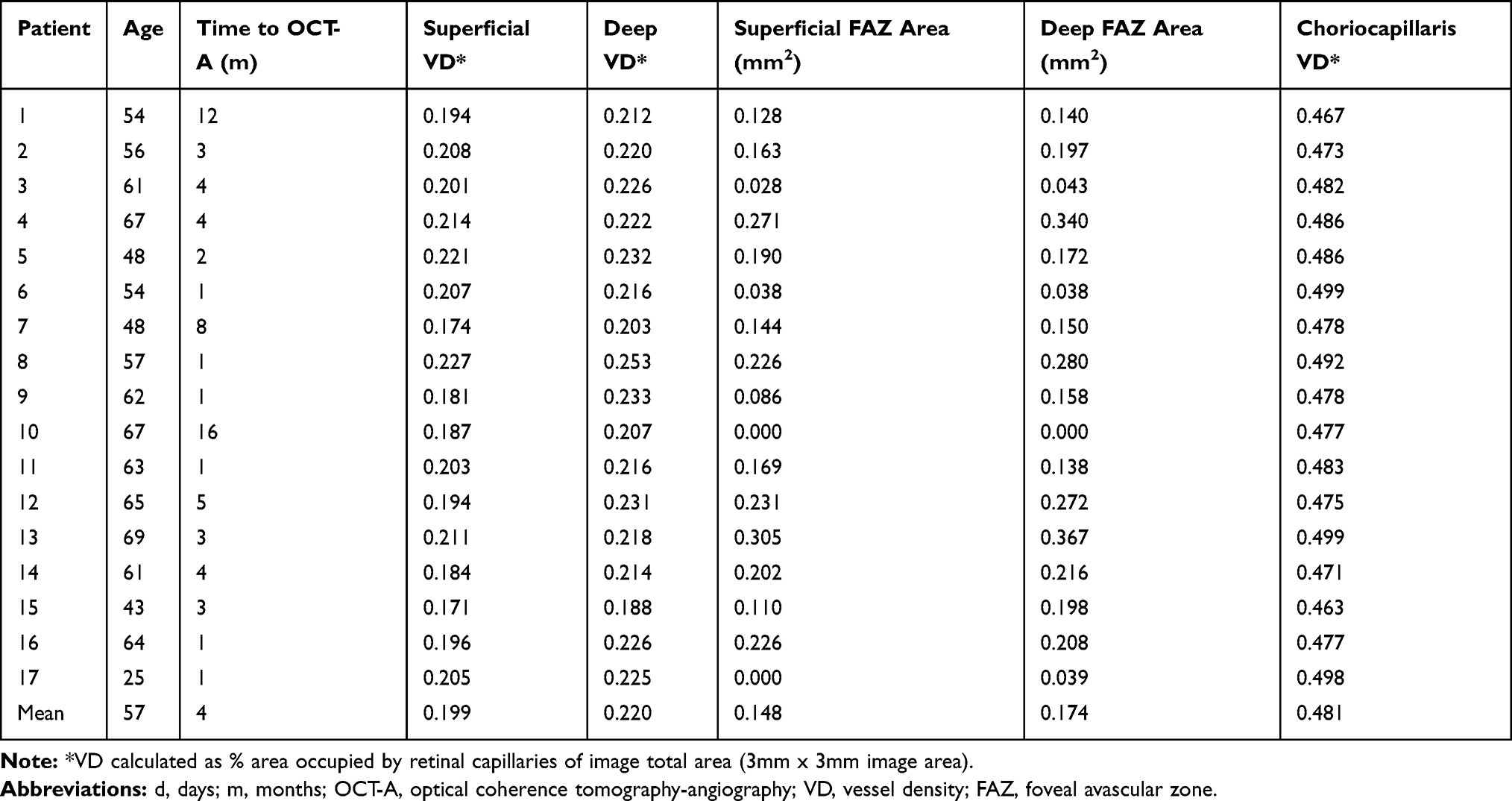 |
Table 3 Data for the Fellow Unaffected Eyes |
Visual Function
Presenting visual acuity ranged from 20/30 to hand motion (HM). After successful repair, the mean final best corrected visual acuity (BCVA) was 20/34. The BCVA in affected eyes ranged from 20/20 to 20/150. Most importantly, there was a high degree of visual recovery with 13 of the 17 eyes achieving a BCVA better than 20/40.
OCT-A Image Analysis
There was a statistically significant reduction in VD of the deep capillary plexus in eyes affected by RRD compared to the fellow control eyes (p = 0.046) (Table 4). This reduction in deep capillary plexus VD was observed in 12 out of the 17 patients included in this analysis and persisted in eyes with follow-up OCT-A as part of their clinical care. These follow-up OCT-A scans were not included in the current study. Additional studies are underway to obtain OCT-As at more standard intervals in a prospective study design. The 12 patients with VD reduction in the deep capillary plexus of the RRD eye compared with the fellow eye had a mean visual acuity 20/39. On the other hand, those five patients with a higher VD of the deep capillary plexus in the eye affected by RRD had a significantly better mean visual acuity of 20/25 (p= 0.03). There was no significant difference in VD of the superficial (p = 0.13) or choriocapillaris (p = 0.28) layers, nor was there a significant difference in the superficial (p = 0.32) or deep (p = 0.62) FAZ areas between eyes affected by RRD and fellow control eyes. All four of the patients with final visual acuity worse than 20/40 demonstrated reduction in deep capillary plexus VD; however, the magnitude of VD reduction in those eyes with worse than 20/40 vision compared with the fellow eye was small. Of the 12 RRD eyes which demonstrated decreased deep capillary plexus VD, 10 also demonstrated EZ loss on OCT.
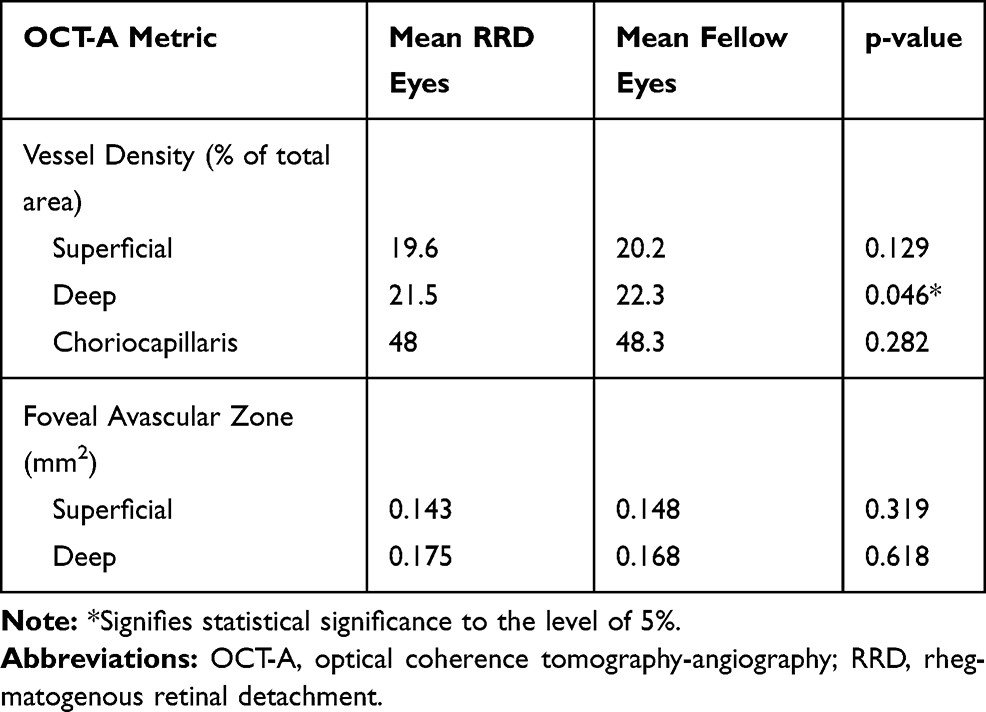 |
Table 4 Mean Vessel Densities and Foveal Avascular Zone Area in RRD Eyes versus Fellow Eyes |
On multivariate regression analysis, there was no statistically significant effect of time internal from RD repair to OCT-A on VD of superficial capillary plexus (p>0.05), deep capillary plexus (p>0.05), choriocapillaris (p>0.05), superficial or deep FAZ (p>0.05). Similarly, there was no statistically significant effect of time from RD repair to BCVA measurement on VD of all the parameters mentioned above except from VD of the deep capillary plexus, where we found a statistically significant effect (p=0.001).
Discussion
In an attempt to elucidate the mechanism by which retinal detachment causes microvascular macular changes, we herein employed OCT-A in mac-off RRD eyes following repair, using the healthy fellow eyes as a control group. Compared to the fellow healthy eyes, a statistically significant reduction in VD of the DCP was identified in mac-off RRD eyes with evidence of correlation with final BCVA after repair. RRD eyes with reduced VD in the DCP had worse BCVA after repair compared to those with no statistically significant reduction compared to the fellow eyes. No significant microvasculature changes were detected in the superficial or deep FAZ area, VD in the superficial capillary plexus and choriocapillaris compared to fellow eyes. Our results build on the few recent reports that have investigated mac-off RRD eyes following repair using OCT-A.28,29,31,32 We herein explore the various suggested mechanisms for the microvascular changes observed even following surgical repair of RRD including the effect of the RD itself, the effect of our surgical intervention for RD repair and the effect of macular detachment on the retinal microvasculature.
A neurosensory RD is thought to lead to outer retinal ischemia, although the exact mechanism is not completely understood. There is animal but not human experimental evidence of transient increase in HIF1α expression33 as well as data suggesting that hyperoxia in animal models of RD may be beneficial.34–36 Separation of the photoreceptors (PR) from retinal pigment epithelium (RPE) leads to a cascade of molecular37 and biochemical changes38,39 that lead to activation of a multitude of pathways including inflammation,40–44 gliosis45,46 and reparative attempts,47,48 however, there is an ensuing neuronal cell death from apoptosis49–52 and necrosis53–55 that contributes to loss of PR cells and decreased visual function.54,56-59 The vascular changes associated with RD have not been investigated in similar detail. Sato et al in 197112 and Tolentino et al in 197613 reported the findings of Fluorescein Angiography (FA) on RD with lattice degeneration focusing mostly in the peripheral changes and reporting flow slowdown, vascular occlusions, arteriovenous shunts and permeability alterations. Picolino in 198314 reported the FA findings of 50 patients with RD confirming the prior peripheral retinal vasculature changes and reporting that central retina vasculature also exhibited diffuse dilatation of the capillary network in the detached retina as well as capillary hyperpermeability. In 1989 Satoh reported that the circulation times were slower in the detached retina compared to the attached areas.15 Recently, Akiyama et al60 employed focal macular ERG and reported ERG responses to be reduced in the attached macula of macula-on RRD eyes compared to the fellow eyes, suggesting that alterations in the retinal microcirculation could be observed even in the attached macula (or retina) of eyes having RRD.
All the above studies focused on vascular changes in the detached retina prior to repair. The selection of surgical technique might also play a role in the ensuing retinal microvascular changes following RD repair. Ohkubo in 1988 reported on FA findings before and after repair in only 2 cases and concluded that the disturbed retinal circulation in the detached retina improved after surgery at least the area which was not indented by an exoplant; whereas an encircling element disturbed the choroidal circulation.16 Sabates et al in 1989 reported on macular changes after repair and reported mostly on the incidence of CME (16%).17 Eshita et al in 2004 reported that the microcirculation in the macular area in macula-on RD was diminished after SB and correlated to the extent of the RD; however, it showed signs of recovery over a month.21 Similar information were provided by Kubicka-Trzaska and Górniak-Bednarz in 2007.20 Sato et al did a similar study comparing PPV/gas versus SB and found similar conclusions to the prior two studies and no major difference between SB and PPV as it relates to macular microcirculation but did conclude that use of gas tamponade might have a subclinical adverse effect on the neuroretinal disk rim circulation.19 In 2011 Kubicka-Trzaska examined the macular microcirculation after repair with the use of silicone oil and reported disturbances in the macular microcirculation that may persist longer than what has been reported before for other types of repair.18 Recently, Tsen et al used OCT-A to compare different surgical techniques for RRD repair and found vitrectomy alone to render a higher post-operative VD in the choriocapillaris, while the combined vitrectomy and SB procedure lead to lower VD in SCP and DCP compared to SB or vitrectomy alone.32
Apart from the effect of RD itself on retinal microvasculature and the effect of the ensuing surgical repair, recently there is growing evidence that macular detachment might further contribute to alterations of the retinal microvasculature. Woo et al used OCT-A to examine the FAZ area in 34 eyes after successful RRD repair28 and found both the post-operative superficial and deep FAZ area to be significantly larger in the 19 mac-off eyes compared to the 15 mac-on eyes and that the deep FAZ zone was larger in the mac-off compared to the fellow eyes. The changes in FAZ zone correlated with visual acuity in their cohort. Recently, Bonfiglio et al29 retrospectively reviewed 37 mac-off eyes with a 12-month follow-up using OCT-A and reported decreased SCP and DCP VD parafoveally and decreased foveal DCP VD with final BCVA being negatively correlated to parafoveal DCP VD and foveal SCP VD. They also studied 56 mac-on RRD eyes and found decreased DCP VD parafoveally that was negatively correlated with final BCVA. When comparing mac-on and mac-off RRD eyes, the group found mac-off eyes to have lower SCP VD parafoveally and decreased foveal and parafoveal DCP VD suggesting macula detachment may contribute to microvasculature changes in RRD eyes. They found no difference in FAZ zone in mac-off or mac-on eyes compared to fellow eyes yet they only measured FAZ in one slab without separating SCP and DCP.
Few more recent studies employed OCT-A in an attempt to study RRD in either mac-off or mac-on RRD albeit without directly comparing mac-off with mac-on eyes. Wang et al retrospectively studied 14 eyes with mac-off RRD using OCT-A during the first 12 weeks post-operatively and found gradual recovery of macular perfusion over time with a significant increase in flow density in SCP DCP and CC over time progressively approximating but never reaching the values of the fellow eye. They found final BCVA to be negatively correlated with CC flow deficits but not with SCP or DCP VD. Of interest, CC perfusion recovery reached plateau before recovery of the retinal circulation in SCP, DCP and matching BCVA recovery curve, suggesting recovery of impaired choroidal circulation was important for the improvements in visual function and outer retinal morphology in retinal diseases.31 Tsen et al prospectively evaluated 28 eyes with mac-off RRD using OCT-A and reported VD to be significantly lower in the SCP and DCP in the RD eyes compared to the fellow eyes32 while Yoshikawa et al investigated 5 eyes with mac-on RRD pre-operatively and reported parafoveal VD and FAZ to be not significantly different between the eyes with RRD and the fellow eye suggesting that the macular microvasculature remains intact.30
In our study of 17 eyes with mac-off RD, we found a reduction of the VD in the DCP employing OCT-A. Furthermore, we report worse visual outcomes in eyes which had reduced VD in the deep capillary plexus compared with those that did not. We found only a small reduction in VD in the superficial capillary plexus that did not reach statistical significance (p=0.13). This might be expected because the superficial capillary plexus supplies the region less affected by the RD. There were no significant differences in the choriocapillaris layer but it should be noted that there are limitations in resolving the individual lobules of the choriocapillaris, which are not always clearly demonstrated with spectral-domain OCT-A.61 This may have limited our ability to detect subtle changes in choriocapillaris perfusion after RRD. Future studies employing Swept-Source OCT-A could potentially improve accuracy and sensitivity for detecting choriocapillaris lesions.62–64 Unlike the prior study by Woo et al,28 we found no statistically significant difference in the superficial or deep FAZ area comparing RRD and fellow eyes.
Our study has limitations related to the small number of eyes, its retrospective nature and lack of longitudinal changes in OCT-A after RD repair. To account for the potential effect of variable time interval form RD repair to OCT-A and BCVA acquisition on OCT-A parameters a multivariate analysis was performed. Our study also did not adjust for the potential effect of axial length on the OCT-A parameters, as with the vast majority (92%) of OCT-A studies.65 Fortunately, we compared our study eyes to the contralateral fellow control eyes for our comparisons so axial lengths disparities should not disrupt our results. Our cohort also had a narrow range of final visual acuity, with 13 out of 17 (76%) achieving better than 20/40 BCVA after RD repair. The unusually high number of patients with good visual outcome in our series may represent an atypical RD repair group that may not be translatable to all populations. Because of the small range of visual acuity outcomes, our ability to statistically correlate VD and FAZ size with visual acuity was limited. More significant differences in macular microvascular structure may only become more apparent in patients with worse visual outcomes, a population not adequately represented in this study. There may also be other functional measures of vision that better correlate with the identified microvascular changes, such as contrast sensitivity and microperimetry. A larger patient cohort, longer duration of follow-up, inclusion of patients with worse visual outcome, and use of swept-source OCT-A may help to further elucidate the role of microvascular changes in eyes affected by RRD.
Disclosure
Dr Thanos D Papakostas is advisory board for Genentech, Thrombogenics, and Alimera, outside the submitted work. Dr John B Miller reports personal fees from Alcon, Heidelberg, Zeiss, and Allergan, outside the submitted work. The authors declare that they have no other conflicts of interest to disclose relevant to the publication.
References
1. Schaal S, Sherman MP, Barr CC, Kaplan HJ. Primary retinal detachment repair: comparison of 1-year outcomes of four surgical techniques. Retina. 2011;31(8):1500–1504. doi:10.1097/IAE.0b013e31820d3f55
2. Chignell AH, Fison LG, Davies EW, Hartley RE, Gundry MF. Failure in retinal detachment surgery. Br J Ophthalmol. 1973;57(8):525–530. doi:10.1136/bjo.57.8.525
3. Rachal WF, Burton TC. Changing concepts of failures after retinal detachment surgery. Arch Ophthalmol. 1979;97(3):480–483. doi:10.1001/archopht.1979.01020010230008
4. Wilkinson CP, Bradford RH
5. Sharma T, Challa JK, Ravishankar KV, Murugesan R. Scleral buckling for retinal detachment. predictors for anatomic failure. Retina. 1994;14(4):338–343. doi:10.1097/00006982-199414040-00008
6. Speicher MA, Fu AD, Martin JP, von Fricken MA. Primary vitrectomy alone for repair of retinal detachments following cataract surgery. Retina. 2000;20(5):459–464. doi:10.1097/00006982-200009000-00005
7. Burton TC. Recovery of visual acuity after retinal detachment involving the macula. Trans Am Ophthalmol Soc. 1982;80:475–497.
8. Nakanishi H, Hangai M, Unoki N, et al. Spectral-domain optical coherence tomography imaging of the detached macula in rhegmatogenous retinal detachment. Retina. 2009;29(2):232–242. doi:10.1097/IAE.0b013e31818bcd30
9. Park DH, Choi KS, Sun HJ, Lee SJ. Factors associated with visual outcome after macula-off rhegmatogenous retinal detachment surgery. Retina. 2017.
10. Schocket LS, Within A, Fujimoto JG, et al. Ultrahigh-resolution optical coherence tomography in patients with decreased visual acuity after retinal detachment repair. Ophthalmology. 2006;113(4):666–672. doi:10.1016/j.ophtha.2006.01.003
11. Shimoda Y, Sano M, Hashimoto H, Yokota Y, Kishi S. Restoration of photoreceptor outer segment after vitrectomy for retinal detachment. Am J Ophthalmol. 2010;149(2):284–290. doi:10.1016/j.ajo.2009.08.025
12. Sato K, Tsunakawa N, Inaba K, Yanagisawa Y. Fluorescein angiography on retinal detachment and lattice degeneration. I. Equatorial degeneration with idiopathic retinal detachment. Nihon Ganka Gakkai Zasshi. 1971;75:635–642.
13. Tolentino FI, Lapus JV, Novalis G, Trempe CL, Gutow GS, Ahmad A. Fluorescein angiography of degenerative lesions of the peripheral fundus and rhegmatogenous retinal detachment. Int Ophthalmol Clin. 1976;16(1):13–29. doi:10.1097/00004397-197601610-00005
14. Cardillo Piccolino F. Vascular changes in rhegmatogenous retinal detachment. Ophthalmologica. 1983;186(1):17–24. doi:10.1159/000309255
15. Satoh Y. Retinal circulation in rhegmatogenous retinal detachment demonstrated by videofluorescence angiography and image analysis. I. The condition of retinal circulation before retinal detachment surgery. Nihon Ganka Gakkai Zasshi. 1989;93(10):1002–1008.
16. Ohkubo H. Fluorescein angiographic findings in the detached and reattached retina. Jpn J Ophthalmol. 1988;32(4):423–428.
17. Sabates NR, Sabates FN, Sabates R, Lee KY, Ziemianski MC. Macular changes after retinal detachment surgery. Am J Ophthalmol. 1989;108(1):22–29. doi:10.1016/S0002-9394(14)73255-6
18. Kubicka-Trzaska A, Kobylarz J, Romanowska-Dixon B. Macular microcirculation blood flow after pars plana vitrectomy with silicone oil tamponade. Klin Oczna. 2011;113(4–6):146–148.
19. Sato EA, Sinoda K, Kimura I, Ohtake Y, Inoue M. Microcirculation in eyes after rhegmatogenous retinal detachment surgery. Curr Eye Res. 2007;32(9):773–779. doi:10.1080/02713680701531108
20. Kubicka-Trzaska A, Gorniak-Bednarz A. Macular microcirculation blood flow changes after conventional surgery for rhegmatogenous retinal detachment. Klin Oczna. 2007;109(4–6):179–182.
21. Eshita T, Shinoda K, Kimura I, et al. Retinal blood flow in the macular area before and after scleral buckling procedures for rhegmatogenous retinal detachment without macular involvement. Jpn J Ophthalmol. 2004;48(4):358–363. doi:10.1007/s10384-004-0096-5
22. Akil H, Falavarjani KH, Sadda SR, Sadun AA. Optical coherence tomography angiography of the optic disc; an overview. J Ophthalmic Vis Res. 2017;12(1):98–105. doi:10.4103/2008-322X.200162
23. de Carlo TE, Bonini Filho MA, Baumal CR, et al. Evaluation of preretinal neovascularization in proliferative diabetic retinopathy using optical coherence tomography angiography. Ophthalmic Surg Lasers Imaging Retina. 2016;47(2):115–119. doi:10.3928/23258160-20160126-03
24. Casselholmde Salles M, Kvanta A, Armen U, Epstein D. Optical coherence tomography angiography in central retinal vein occlusion: correlation between the foveal avascular zone and visual acuity. Invest Ophthalmol Vis Sci. 2016;57(9):Oct242–6. doi:10.1167/iovs.15-18819
25. Ma J, Desai R, Nesper P, Gill M, Fawzi A, Skondra D. Optical coherence tomographic angiography imaging in age-related macular degeneration. Ophthalmol Eye Dis. 2017;9:1179172116686075.
26. Wang JC, Lains I, Sobrin L, Miller JB. Distinguishing white dot syndromes with patterns of choroidal hypoperfusion on optical coherence tomography angiography. Ophthalmic Surg Lasers Imaging Retina. 2017;48(8):638–646. doi:10.3928/23258160-20170802-06
27. de Carlo TE, Romano A, Waheed KA, Duker JS. A review of optical coherence tomography angiography (OCTA). Int J Retin. 2015;1(1):5. doi:10.1186/s40942-015-0005-8
28. Woo JM, Yoon YS, Woo JE, Min JK. Foveal avascular zone area changes analyzed using OCT angiography after successful rhegmatogenous retinal detachment repair. Curr Eye Res. 2018;43(5):674–678. doi:10.1080/02713683.2018.1437922
29. Bonfiglio V, Ortisi E, Scollo D, et al. Vascular changes after vitrectomy for rhegmatogenous retinal detachment: optical coherence tomography angiography study. Acta Ophthalmol. 2019. doi:10.1111/aos.14315
30. Yoshikawa Y, Shoji T, Kanno J, et al. Evaluation of microvascular changes in the macular area of eyes with rhegmatogenous retinal detachment without macular involvement using swept-source optical coherence tomography angiography. Clin Ophthalmol. 2018;12:2059–2067. doi:10.2147/OPTH.S177933
31. Wang H, Xu X, Sun X, et al. Macular perfusion changes assessed with optical coherence tomography angiography after vitrectomy for rhegmatogenous retinal detachment. Graefes Arch Clin Exp Ophthalmol. 2019;257(4):733–740. doi:10.1007/s00417-019-04273-7
32. Tsen CL, Sheu SJ, Chen SC, Wu TT. Imaging analysis with optical coherence tomography angiography after primary repair of macula-off rhegmatogenous retinal detachment. Graefes Arch Clin Exp Ophthalmol. 2019;257(9):1847–1855. doi:10.1007/s00417-019-04381-4
33. Shelby SJ, Angadi PS, Wheng QD, Yao J, Jia L, Zacks DN. Hypoxia inducible factor 1alpha contributes to regulation of autophagy in retinal detachment. Exp Eye Res. 2015;137:84–93. doi:10.1016/j.exer.2015.06.016
34. Mervin K, Valter K, Muslim J, Lewis G, Fisher S, Stone J. Limiting photoreceptor death and deconstruction during experimental retinal detachment: the value of oxygen supplementation. Am J Ophthalmol. 1999;128(2):155–164. doi:10.1016/S0002-9394(99)00104-X
35. Lewis G, Marvin K, Valter K, et al. Limiting the proliferation and reactivity of retinal Muller cells during experimental retinal detachment: the value of oxygen supplementation. Am J Ophthalmol. 1999;128(2):165–172. doi:10.1016/S0002-9394(99)00103-8
36. Sweigard JH, Mastumoto H, Smith KE, et al. Inhibition of the alternative complement pathway preserves photoreceptors after retinal injury. Sci Transl Med. 2015;7(297):297ra116. doi:10.1126/scitranslmed.aab1482
37. Matsumoto H, Murakami Y, Kataola K, et al. Membrane-bound and soluble Fas ligands have opposite functions in photoreceptor cell death following separation from the retinal pigment epithelium. Cell Death Dis. 2015;6(11):e1986. doi:10.1038/cddis.2015.334
38. Matsumoto H, Murakami Y, Kataola K, et al. Mammalian STE20-like kinase 2, not kinase 1, mediates photoreceptor cell death during retinal detachment. Cell Death Dis. 2014;5(5):e1269. doi:10.1038/cddis.2014.218
39. Roh MI, Murakami Y, Thanos A, VAvvas DG, Miller JW. Edaravone, an ROS scavenger, ameliorates photoreceptor cell death after experimental retinal detachment. Invest Ophthalmol Vis Sci. 2011;52(6):3825–3831. doi:10.1167/iovs.10-6797
40. Nakazawa T, Matsubara A, Noda K, et al. Characterization of cytokine responses to retinal detachment in rats. Mol Vis. 2006;12:867–878.
41. Nakazawa T, Hisatomi T, Nakazawa C, et al. Monocyte chemoattractant protein 1 mediates retinal detachment-induced photoreceptor apoptosis. Proc Natl Acad Sci U S A. 2007;104(7):2425–2430. doi:10.1073/pnas.0608167104
42. Nakazawa T, Kawama M, Ryu M, et al. Tumor necrosis factor-alpha mediates photoreceptor death in a rodent model of retinal detachment. Invest Ophthalmol Vis Sci. 2011;52(3):1384–1391. doi:10.1167/iovs.10-6509
43. Kataoka K, Mastumoto H, Kaneko H, et al. Macrophage- and RIP3-dependent inflammasome activation exacerbates retinal detachment-induced photoreceptor cell death. Cell Death Dis. 2015;6(4):e1731. doi:10.1038/cddis.2015.73
44. Takahashi S, Adachi K, Suzuki Y, Maeno A, Nakazawa M. Profiles of inflammatory cytokines in the vitreous fluid from patients with rhegmatogenous retinal detachment and their correlations with clinical features. Biomed Res Int. 2016;2016:4256183. doi:10.1155/2016/4256183
45. Lewis GP, Chapin EA, Byun J, et al. Muller cell reactivity and photoreceptor cell death are reduced after experimental retinal detachment using an inhibitor of the Akt/mTOR pathway. Invest Ophthalmol Vis Sci. 2009;50(9):4429–4435. doi:10.1167/iovs.09-3445
46. Nakazawa T, Takeda M, Lewis GP, et al. Attenuated glial reactions and photoreceptor degeneration after retinal detachment in mice deficient in glial fibrillary acidic protein and vimentin. Invest Ophthalmol Vis Sci. 2007;48(6):2760–2768. doi:10.1167/iovs.06-1398
47. Kayama M, Nakazawa T, Thannos A, et al. Heat shock protein 70 (HSP70) is critical for the photoreceptor stress response after retinal detachment via modulating anti-apoptotic Akt kinase. Am J Pathol. 2011;178(3):1080–1091. doi:10.1016/j.ajpath.2010.11.072
48. Matsumoto H, Kataoki K, Tsoka P, Connor KM, Miller JW, Vavvas DG. Strain difference in photoreceptor cell death after retinal detachment in mice. Invest Ophthalmol Vis Sci. 2014;55(7):4165–4174. doi:10.1167/iovs.14-14238
49. Berglin L, Algvere PV, Seregard S. Photoreceptor decay over time and apoptosis in experimental retinal detachment. Graefes Arch Clin Exp Ophthalmol. 1997;235(5):306–312. doi:10.1007/BF01739640
50. Guerin CJ, Anderson DH, FAriss R, Fisher SK. Retinal reattachment of the primate macula. Photoreceptor recovery after short-term detachment. Invest Ophthalmol Vis Sci. 1989;30(8):1708–1725.
51. Chang CJ, Lai WW, Edward DP, Two MO. Apoptotic photoreceptor cell death after traumatic retinal detachment in humans. Arch Ophthalmol. 1995;113(7):880–886. doi:10.1001/archopht.1995.01100070054025
52. Arroyo JG, YAng L, Bula D, Chen DF. Photoreceptor apoptosis in human retinal detachment. Am J Ophthalmol. 2005;139(4):605–610. doi:10.1016/j.ajo.2004.11.046
53. Trichonas G, Murakami Y, Thanos A, et al. Receptor interacting protein kinases mediate retinal detachment-induced photoreceptor necrosis and compensate for inhibition of apoptosis. Proc Natl Acad Sci U S A. 2010;107(50):21695–21700. doi:10.1073/pnas.1009179107
54. Murakami Y, Notomi S, Hisatomi T, et al. Photoreceptor cell death and rescue in retinal detachment and degenerations. Prog Retin Eye Res. 2013;37:114–140. doi:10.1016/j.preteyeres.2013.08.001
55. Murakami Y, Miller JW, Vavvas DG. RIP kinase-mediated necrosis as an alternative mechanisms of photoreceptor death. Oncotarget. 2011;2(6):497–509. doi:10.18632/oncotarget.286
56. Huckfeldt RM, Vavvas DG. Neuroprotection for retinal detachment. Int Ophthalmol Clin. 2013;53(4):105–117. doi:10.1097/IIO.0b013e31829cf08d
57. Han KJ, Lee YH, Vavvas DG. Optical coherence tomography automated layer segmentation of macula after retinal detachment repair. PLoS One. 2018;13(5):e0197058. doi:10.1371/journal.pone.0197058
58. Park DH, Choi KS, Sun HJ, Lee SJ. Factors associated with visual outcome after macula-off rhegmatogenous retinal detachment surgery. Retina. 2018;38(1):137–147. doi:10.1097/IAE.0000000000001512
59. Dooley I, Traecy M, O’Rourke M, Khalid I, Kilmartin D. Serial spectral domain ocular coherence tomography measurement of outer nuclear layer thickness in rhegmatogenous retinal detachment repair. Curr Eye Res. 2015;40(10):1073–1076. doi:10.3109/02713683.2014.971936
60. Akiyama K, Fujinami K, Watanabe K, et al. Macular dysfunction in patients with macula-on rhegmatogenous retinal detachments. Br J Ophthalmol. 2019;103(3):404–409. doi:10.1136/bjophthalmol-2018-312153
61. Spaide RF. Choriocapillaris flow features follow a power law distribution: implications for characterization and mechanisms of disease progression. Am J Ophthalmol. 2016;170:58–67. doi:10.1016/j.ajo.2016.07.023
62. Spaide RF, Fujimoto JG, Waheed NK, Sadda SR, Staurenghi G. Optical coherence tomography angiography. Prog Retin Eye Res. 2018;64:1–55. doi:10.1016/j.preteyeres.2017.11.003
63. Lane M, Moult EM, Novais EA, et al. Visualizing the choriocapillaris under drusen: comparing 1050-nm swept-source versus 840-nm spectral-domain optical coherence tomography angiography. Invest Ophthalmol Vis Sci. 2016;57(9):OCT585–90. doi:10.1167/iovs.15-18915
64. Miller AR, Roisman L, Zhang Q, et al. Comparison between spectral-domain and swept-source optical coherence tomography angiographic imaging of choroidal neovascularization. Invest Ophthalmol Vis Sci. 2017;58(3):1499–1505. doi:10.1167/iovs.16-20969
65. Llanas S, Linderman RE, Chen FK, Carroll J. Assessing the use of incorrectly scaled optical coherence tomography angiography images in peer-reviewed studies: a systematic review. JAMA Ophthalmol. 2019.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.