Back to Journals » Journal of Inflammation Research » Volume 19
Rethinking Corticosteroid Therapy in Pediatric Neurology
Authors Lin WS ![]()
Received 15 October 2025
Accepted for publication 3 March 2026
Published 10 March 2026 Volume 2026:19 568197
DOI https://doi.org/10.2147/JIR.S568197
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Dharmappa Krishnappa
Wei-Sheng Lin1,2
1Department of Pediatrics, Taipei Veterans General Hospital, Taipei, Taiwan; 2School of Medicine, National Yang Ming Chiao Tung University, Taipei, Taiwan
Correspondence: Wei-Sheng Lin, Department of Pediatrics, Taipei Veterans General Hospital, No. 201, Sec. 2, Shipai Road, Beitou District, Taipei, 11217, Taiwan, Tel +886-2-2875-7128ext.127, Email [email protected]
Abstract: Corticosteroids have long been a cornerstone in the management of many pediatric neurological disorders. However, their broad immunomodulatory effects raise concerns in the era of precision medicine, where more targeted approaches are increasingly favored, warranting a critical reappraisal of their roles in pediatric neurology. Of particular importance is the possibility that corticosteroids may potentiate components of the innate immune responses and thereby exacerbate neuroinflammation. Accordingly, disease-specific immunopathogenesis should be considered in therapeutic decision-making. The potential for adverse effects, especially with long-term use, remains a major consideration and underscores the need for careful risk–benefit analysis. Several therapeutic innovations, including selective glucocorticoid receptor modulators (such as vamorolone) and intra-erythrocyte dexamethasone delivery, have shown promising safety profiles in Duchenne muscular dystrophy and ataxia telangiectasia, respectively. Beyond the well-established role of corticosteroids in infantile epileptic spasms syndrome, recent evidence suggests that corticosteroids may benefit a substantial proportion of patients with various forms of epilepsy that are resistant to conventional antiseizure medications. Further research is warranted to define the optimal use of corticosteroids with respect to dosing, formulation, timing, and route of administration in various pediatric neurological disorders.
Keywords: corticosteroids, glucocorticoid receptor modulator, glucocorticoid toxicity, intra-erythrocyte drug delivery, neuroinflammation, vamorolone
Text
Corticosteroids have been a cornerstone in the management of many neuroimmunological disorders. Their broad immunomodulatory properties have justified their widespread use across a range of autoimmune and neuroinflammatory conditions. However, in the era of precision medicine, such relatively nonspecific effects on immune pathways, as well as pleiotropic effects on broader physiological systems, may limit their appeal compared to more targeted therapies. This makes the present moment suitable for a critical reappraisal of the therapeutic role of corticosteroids, as exemplified by a recent opinion piece authored by Chiek Teoh et al.1 Several important issues are discussed in their paper, including disease-specific immunopathogenesis and safety concerns. In my view, additional aspects merit further discussion, especially in the context of pediatric neurology. Corticosteroids have been used across a broad spectrum of pediatric neurological disorders (Table 1); in some conditions, their efficacy is well established, whereas in others their use remains anecdotal or exploratory. Importantly, potential adverse effects unique to the pediatric population, most notably growth suppression, should be carefully weighed when considering corticosteroid therapy.
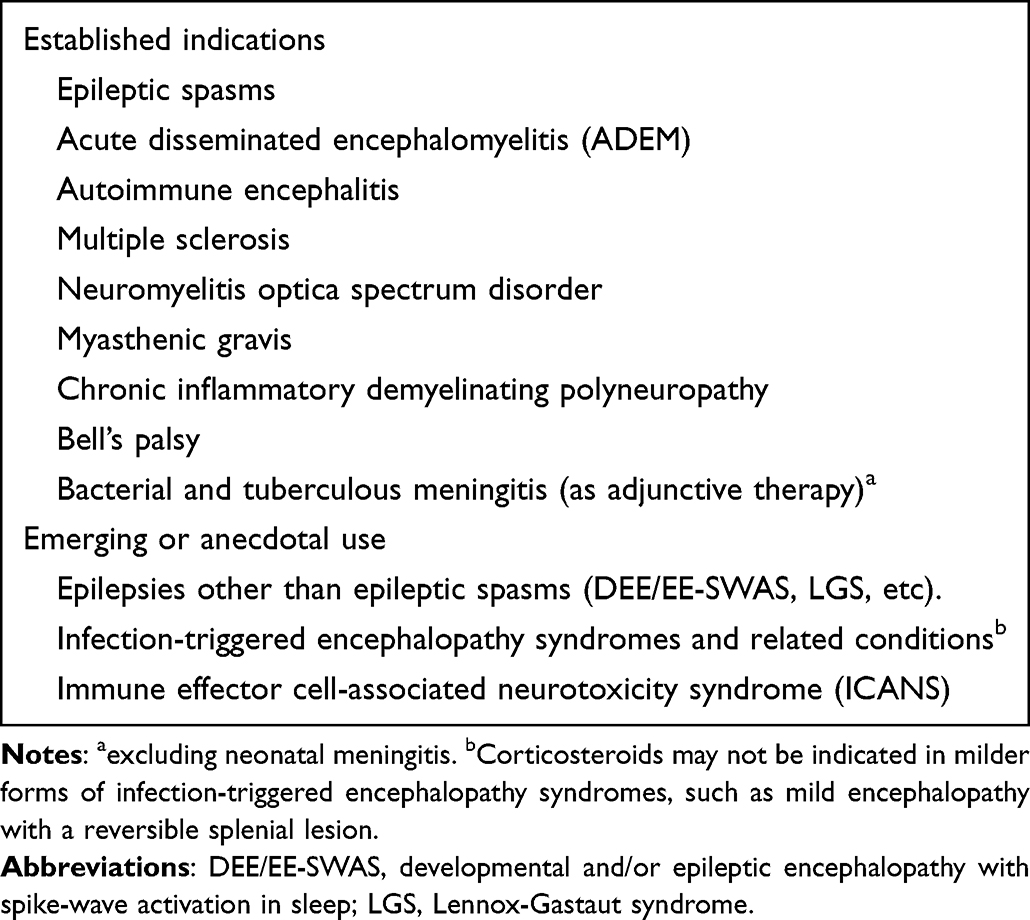 |
Table 1 Corticosteroid Use in Pediatric Neurological Disorders |
Corticosteroids: A Double-Edged Sword
Although corticosteroids are classically regarded as anti-inflammatory and immunosuppressive, they can also potentiate certain elements of innate immunity in the CNS in some contexts. This may not be entirely unexpected, as endogenous corticosteroids have likely evolved to prepare the body, including the immune system, adapt to periods of acute stress. Indeed, endogenous or exogenous corticosteroids can prime microglia for enhanced pro-inflammatory responses upon subsequent immune challenges. This microglial priming has been demonstrated in rodent models exposed to acute stress or chronic corticosterone treatment, with potentiation evidenced by elevated cytokine responses and inflammasome activation.2,3 Notably, blocking glucocorticoid receptor (GR) signaling prevents this priming, supporting the permissive role of corticosteroids in neuroinflammatory sensitization. Given that innate immune processes, such as microglial activation and inflammasome signaling, are implicated in a range of neurological disorders, including multiple sclerosis, N-methyl-D-aspartate (NMDA) receptor encephalitis, Rasmussen encephalitis, and febrile infection-related epilepsy syndrome (FIRES),4 it is essential to re-examine the neuroimmunological effects of corticosteroid therapy in these conditions, particularly with respect to treatment timing and dosage.
Although the context-dependent pro-inflammatory actions of corticosteroids are primarily observed in innate immune processes,5,6 this does not imply that corticosteroids are universally beneficial in autoimmune (ie, adaptive immune-mediated) neurological disorders. A classic example is Guillain-Barré syndrome (GBS), which responds poorly to corticosteroid therapy. Animal studies suggested that corticosteroids may interfere with macrophage-mediated clearance of myelin and axonal debris, thereby impairing remyelination and delaying recovery.7 How this mechanism reconciles with the effectiveness of corticosteroids in chronic inflammatory demyelinating polyneuropathy (CIDP), the chronic counterpart of GBS, remains unresolved. Other causes of corticosteroid resistance, such as GRα phosphorylation, increased GRβ expression, or reduced histone deacetylase (HDAC) 2 expression, may also worth investigation in this context.8 Regardless, these contrasting clinical experiences highlight the importance of tailoring immunotherapy to disease-specific immunopathogenesis.
Enhancing Safety Through Therapeutic Innovations and Steroid Stewardship
Corticosteroid-associated adverse effects are an important consideration when selecting these agents for therapeutic use in children, even when administered for short courses.9 Particular concerns include their potential impact on linear growth and the developing brain,10,11 both of which warrant careful monitoring in the pediatric population. Selective glucocorticoid receptor modulators (SEGRMs) have been proposed as a means of reducing adverse effects through more targeted modulation of GR signaling.12 To date, however, their application remains largely experimental. An encouraging advance in this direction is vamorolone, a dissociative steroid that preserves GR-mediated transrepression while reducing GR-mediated transactivation. Compared with conventional corticosteroids, vamorolone is associated with a more favorable safety profile and has recently been granted regulatory approval for the treatment of Duchenne muscular dystrophy.13,14 An alternative strategy for enhancing the safety of corticosteroid therapy is intra-erythrocyte delivery. This technology encapsulates corticosteroids, specifically dexamethasone sodium phosphate, inside autologous red blood cells, which are then infused back into patients. The novel mode of delivery could be conceived as a sustained-release or long-acting formulation of corticosteroids.15 It has entered Phase 3 clinical trials for pediatric patients with ataxia telangiectasia, demonstrating a better safety profile compared with oral corticosteroids.16,17
When systemic corticosteroids are used to treat central nervous system disorders, their degree of CNS penetration should be considered. For example, dexamethasone may exhibit greater penetration (as reflected by a higher CSF to plasma ratio) and a longer half-life in the CSF compared with prednisolone.18 Alternative routes of drug delivery, such as transnasal brain-targeted strategies, merit exploration as potential methods to bypass systemic limitations.19 Intrathecal corticosteroids have gained increasing attention in recent years for the treatment of various neuroimmunological disorders (Table 2), including those with predominant innate immune involvement (eg, FIRES) and adaptive immune involvement (eg, NMDA receptor encephalitis).20,21 However, the pharmacokinetics and pharmacodynamics of various intrathecal corticosteroid regimens remain insufficiently characterized and require further investigation.22 Intrathecal corticosteroid administration might limit systemic exposure and thereby attenuate some adverse effects; nonetheless, systemic effects may still occur and should be carefully monitored.23 It is essential to evaluate corticosteroid formulations for their suitability for intrathecal administration, as certain excipients and additives may be neurotoxic.24 Intrathecal administration of methylprednisolone has been associated with meningeal thickening and adhesions in canine models; however, the formulation used was not preservative-free, potentially confounding the results.25 Notwithstanding these concerns, current data from both rodent models and human studies suggest that intrathecal delivery of corticosteroids is generally safe.26,27 Regardless of the route of administration, it is advisable to systematically monitor potential adverse effects in clinical practice, for example, through the use of standardized tools such as the Glucocorticoid Toxicity Index (GTI),28 which is now being increasingly used in clinical trials involving corticosteroids. A pediatric version of the GTI is also available.29
 |
Table 2 Intrathecal Corticosteroids for Neuroimmunological Disorders |
The Renaissance of Corticosteroids in Pediatric Epileptology
Although corticosteroids are decades-old agents, their applications in pediatric neurology continue to expand, including in epileptology. Beyond their well-established role in infantile epileptic spasms syndrome, recent empirical evidence suggests that corticosteroids may benefit a substantial proportion of patients with various forms of epilepsy that are resistant to conventional antiseizure medications.39–42 However, these studies were often retrospective in nature and lacked appropriate control groups. Encouragingly, several prospective studies and randomized controlled trials have demonstrated favorable efficacy and acceptable safety profiles of corticosteroids in Lennox-Gastaut syndrome,43 developmental and/or epileptic encephalopathy with spike-wave activation in sleep (DEE/EE-SWAS),44 and other forms of pediatric epileptic encephalopathy.45 These findings align with the growing recognition regarding the roles of inflammation and blood-brain barrier alterations in epilepsy, processes that may be modulated by corticosteroid therapy.46 Existing studies, however, have employed heterogeneous treatment protocols with respect to the choice of corticosteroid, as well as dosing and treatment duration.47 Further rigorous research is needed to more clearly define the optimal regimen of corticosteroids in the management of refractory epilepsy across diverse etiologies.
Concluding Remarks
The complex immunomodulatory effects of corticosteroids are increasingly being elucidated, encompassing both anti-inflammatory and pro-inflammatory actions that are highly context dependent. These mechanistic insights are clinically relevant, as an improved understanding of disease-specific immunopathogenesis may inform more precise and judicious use of corticosteroids and help explain variability in treatment responses.
With continued advances in therapeutic modalities and an increasingly refined understanding of disease pathophysiology, the clinical applications of corticosteroids continue to evolve and expand. Therefore, corticosteroids are likely to remain a cornerstone of therapy for a range of pediatric neurological disorders. The pleiotropic effects of corticosteroids, particularly their potential impact on the developing brain and skeletal maturation in children and adolescents, must be carefully weighed upon prescription. It should also be borne in mind that their effects are highly context-dependent and vary according to dose, timing, and disease stage.5 Continued research is needed to elucidate disease-specific immunopathogenesis and to define the optimal use of corticosteroids and related agents in pediatric neurological practice.
Data Sharing Statement
Data sharing is not applicable to this article as no new data were created in this study.
Author Contributions
Wei-Sheng Lin: Conceptualization, investigation, writing – original draft, writing – review & editing. The author gave final approval of the version to be published; has agreed on the journal to which the article has been submitted; and agrees to be accountable for all aspects of the work.
Funding
This study has no dedicated funding.
Disclosure
The author reports no conflicts of interest in this work.
References
1. Chiek Teoh CS, Dubey SG, Handel AE. Rethinking corticosteroid therapy in autoimmune neurology. Brain. Aug 11, 2025;doi:10.1093/brain/awaf292.
2. Frank MG, Thompson BM, Watkins LR, Maier SF. Glucocorticoids mediate stress-induced priming of microglial pro-inflammatory responses. Brain Behav Immun. 2012;26(2):337–6. doi:10.1016/j.bbi.2011.10.005
3. Frank MG, Hershman SA, Weber MD, Watkins LR, Maier SF. Chronic exposure to exogenous glucocorticoids primes microglia to pro-inflammatory stimuli and induces NLRP3 mRNA in the hippocampus. Psychoneuroendocrinology. 2014;40:191–200. doi:10.1016/j.psyneuen.2013.11.006
4. Tan TH-L, Perucca P, O’Brien TJ, Kwan P, Monif M. Inflammation, ictogenesis, and epileptogenesis: an exploration through human disease. Epilepsia. 2021;62(2):303–324. doi:10.1111/epi.16788
5. Cain DW, Cidlowski JA. Immune regulation by glucocorticoids. Nat Rev Immunol. 2017;17(4):233–247. doi:10.1038/nri.2017.1
6. Desmet SJ, De Bosscher K. Glucocorticoid receptors: finding the middle ground. J Clin Invest. 2017;127(4):1136–1145. doi:10.1172/jci88886
7. Wang Y-Z, Lv H, Shi Q-G, et al. Action mechanism of corticosteroids to aggravate Guillain-Barré syndrome. Sci Rep. 2015;5(1):13931. doi:10.1038/srep13931
8. Lockett J, Inder WJ, Clifton VL. The glucocorticoid receptor: isoforms, functions, and contribution to glucocorticoid sensitivity. Endocr Rev. 2024;45(4):593–624. doi:10.1210/endrev/bnae008
9. Lima JP, Chowdhury SR, Tangamornsuksan W, et al. Adverse events following short-course systemic corticosteroids among children and adolescents: a systematic review and meta-analysis. JAMA Network Open. 2025;8(9):e2534953. doi:10.1001/jamanetworkopen.2025.34953
10. Damsted SK, Born AP, Paulson OB, Uldall P. Exogenous glucocorticoids and adverse cerebral effects in children. Eur J Paediatr Neurol. 2011;15(6):465–477. doi:10.1016/j.ejpn.2011.05.002
11. Drozdowicz LB, Bostwick JM. Psychiatric adverse effects of pediatric corticosteroid use. Mayo Clin Proc. 2014;89(6):817–834. doi:10.1016/j.mayocp.2014.01.010
12. Buttgereit F, Elling C, Jakob F. Design and development of glucocorticoid receptor modulators. Trends Pharmacol Sci. 2025;46(8):771–791. doi:10.1016/j.tips.2025.06.005
13. Dang UJ, Damsker JM, Guglieri M, et al. Efficacy and safety of vamorolone over 48 weeks in boys with duchenne muscular dystrophy: a randomized controlled trial. Neurology. 2024;102(5):e208112. doi:10.1212/wnl.0000000000208112
14. Keam SJ. Vamorolone: first Approval. Drugs. 2024;84(1):111–117. doi:10.1007/s40265-023-01986-2
15. Coker SA, Szczepiorkowski ZM, Siegel AH, et al. A study of the pharmacokinetic properties and the in vivo kinetics of erythrocytes loaded with dexamethasone sodium phosphate in healthy volunteers. Transfus Med Rev. 2018;32(2):102–110. doi:10.1016/j.tmrv.2017.09.001
16. Koenig MK, Leuzzi V, Gouider R, et al. Long-term safety of dexamethasone sodium phosphate encapsulated in autologous erythrocytes in pediatric patients with ataxia telangiectasia. Front Neurol. 2025;15:1526914. doi:10.3389/fneur.2024.1526914
17. Zielen S, Crawford T, Benatti L, et al. Safety and efficacy of intra-erythrocyte dexamethasone sodium phosphate in children with ataxia telangiectasia (ATTeST): a multicentre, randomised, double-blind, placebo-controlled phase 3 trial. Lancet Neurol. 2024;23(9):871–882. doi:10.1016/s1474-4422(24)00220-5
18. Balis FM, Lester CM, Chrousos GP, Heideman RL, Poplack DG. Differences in cerebrospinal fluid penetration of corticosteroids: possible relationship to the prevention of meningeal leukemia. J Clin Oncol. 1987;5(2):202–207. doi:10.1200/jco.1987.5.2.202
19. Drath I, Richter F, Feja M. Nose-to-brain drug delivery: from bench to bedside. Transl Neurodegener. 2025;14(1):23. doi:10.1186/s40035-025-00481-w
20. Wang D, Wu Y, Ji Z, et al. A refractory anti-NMDA receptor encephalitis successfully treated by bilateral salpingo-oophorectomy and intrathecal injection of methotrexate and dexamethasone: a case report. J Int Med Res. 2020;48(10):300060520925666. doi:10.1177/0300060520925666
21. Horino A, Kuki I, Inoue T, et al. Intrathecal dexamethasone therapy for febrile infection-related epilepsy syndrome. Ann Clin Transl Neurol. 2021;8(3):645–655. doi:10.1002/acn3.51308
22. Kroin JS, Schaefer RB, Penn RD. Chronic intrathecal administration of dexamethasone sodium phosphate: pharmacokinetics and neurotoxicity in an animal model. Neurosurgery. 2000;46(1):178–183. doi:10.1093/neurosurgery/46.1.178
23. Hoeflich A, Fitzner B, Walz C, et al. Systemic effects by intrathecal administration of triamcinolone acetonide in patients with multiple sclerosis. Front Endocrinol. 2020;11:574. doi:10.3389/fendo.2020.00574
24. Schlatter J, Nguyen D, Zamy M, Kabiche S, Fontan J-E, Cisternino S. Safety of intrathecal route: focus to methylprednisolone acetate (Depo-Medrol) use. Eur Spine J. 2019;28(1):21–30. doi:10.1007/s00586-017-5387-x
25. Lima RM, Navarro LH, Carness JM, et al. Clinical and histological effects of the intrathecal administration of methylprednisolone in dogs. Pain Physician. 2010;13(5):493–501. doi:10.36076/ppj.2010/13/493
26. Fisher K, Cokley J. Intrathecal steroids: a more targeted approach to central nervous system inflammation. Neurology. 2024;103(7_Supplement_1):S136–S137. doi:10.1212/01.wnl.0001051948.48254.e8
27. Abram SE, Marsala M, Yaksh TL. Analgesic and neurotoxic effects of intrathecal corticosteroids in rats. Anesthesiology. 1994;81(5):1198–1205. doi:10.1097/00000542-199411000-00013
28. Stone JH, McDowell PJ, Jayne DRW, et al. The glucocorticoid toxicity index: measuring change in glucocorticoid toxicity over time. Semin Arthritis Rheum. 2022;55:152010. doi:10.1016/j.semarthrit.2022.152010
29. Brogan P, Naden R, Ardoin SP, et al. The pediatric glucocorticoid toxicity index. Semin Arthritis Rheum. 2022;56:152068. doi:10.1016/j.semarthrit.2022.152068
30. Tatencloux S, Chretien P, Rogemond V, Honnorat J, Tardieu M, Deiva K. Intrathecal treatment of anti- N -Methyl- d -aspartate receptor encephalitis in children. Dev Med Child Neurol. 2015;57(1):95–99. doi:10.1111/dmcn.12545
31. Yarimi JM, Sandweiss AJ, Salazar KP, et al. IT-DEX and B cell depletion in a child with anti-GAD 65 autoimmune encephalitis presenting as NORSE: a case report. J Neuroimmunol. 2024;395:578430. doi:10.1016/j.jneuroim.2024.578430
32. Jordan MB, Allen CE, Weitzman S, Filipovich AH, McClain KL. How I treat hemophagocytic lymphohistiocytosis. Blood. 2011;118(15):4041–4052. doi:10.1182/blood-2011-03-278127
33. Henter J-I, Horne A, Aricó M, et al. HLH-2004: diagnostic and therapeutic guidelines for hemophagocytic lymphohistiocytosis. Pediatr Blood Cancer. 2007;48(2):124–131. doi:10.1002/pbc.21039
34. Shalabi H, Harrison C, Yates B, Calvo KR, Lee DW, Shah NN. Intrathecal hydrocortisone for treatment of children and young adults with CAR T-cell immune-effector cell-associated neurotoxicity syndrome. Pediatr Blood Cancer. 2024;71(1):e30741. doi:10.1002/pbc.30741
35. Shah NN, Johnson BD, Fenske TS, Raj RV, Hari P. Intrathecal chemotherapy for management of steroid-refractory CAR T-cell–associated neurotoxicity syndrome. Blood Adv. 2020;4(10):2119–2122. doi:10.1182/bloodadvances.2020001626
36. Ji Q, Dong Y, Zhang Y, et al. Earlier intrathecal dexamethasone effectively alleviate immune effector cell-associated neurotoxicity syndrome. Int Immunopharmacol. 2024;142(Pt B):113214. doi:10.1016/j.intimp.2024.113214
37. Abu-Mugheisib M, Benecke R, Zettl UK. Repeated intrathecal triamcinolone acetonide administration in progressive multiple sclerosis: a review. Mult Scler Int. 2011;2011:219049. doi:10.1155/2011/219049
38. Li R, Chen L, Rong L, et al. Clinical characteristics and efficacy of intrathecal therapy in pediatric lupus encephalopathy. Lupus. 2025;34(8):844–851. doi:10.1177/09612033251344192
39. Kimizu T, Takahashi Y, Oboshi T, et al. Methylprednisolone pulse therapy in 31 patients with refractory epilepsy: a single-center retrospective analysis. Epilepsy Behav. 2020;109:107116. doi:10.1016/j.yebeh.2020.107116
40. Falsaperla R, Collotta AD, Marino SD, et al. Drug resistant epilepsies: a multicentre case series of steroid therapy. Seizure. 2024;117:115–125. doi:10.1016/j.seizure.2024.02.007
41. Schiller K, Thomas J, Avigdor T, et al. Pulsatile corticoid therapy reduces interictal epileptic activity burden in children with genetic drug-resistant epilepsy. Epilepsia Open. 2024;9(4):1265–1276. doi:10.1002/epi4.12947
42. van Arnhem MML, Vijn LJ, Rubboli G, et al. Clobazam versus corticosteroid for developmental and epileptic encephalopathy with spike-wave activation in sleep ((D)EE-SWAS): results of a multicenter observational study. Epilepsia. 2025;doi:10.1111/epi.18680.
43. Yang D, Na J-H, Kim SH, Kim HD, Lee JS, Kang H-C. Efficacy and prognosis of long-term, high-dose steroid therapy for Lennox–Gastaut syndrome. Epilepsy Res. 2022;179:106847. doi:10.1016/j.eplepsyres.2021.106847
44. van Arnhem MML, van den Munckhof B, Arzimanoglou A, et al. Corticosteroids versus clobazam for treatment of children with epileptic encephalopathy with spike-wave activation in sleep (RESCUE ESES): a multicentre randomised controlled trial. Lancet Neurol. 2024;23(2):147–156. doi:10.1016/s1474-4422(23)00409-x
45. Rangarajan A, Mundlamuri RC, Kenchaiah R, et al. Efficacy of pulse intravenous methylprednisolone in epileptic encephalopathy: a randomised controlled trial. J Neurol Neurosurg Psychiatry. 2022;93(12):1299–1305. doi:10.1136/jnnp-2022-329027
46. Orsini A, Foiadelli T, Costagliola G, et al. The role of inflammatory mediators in epilepsy: focus on developmental and epileptic encephalopathies and therapeutic implications. Epilepsy Res. 2021;172:106588. doi:10.1016/j.eplepsyres.2021.106588
47. Becker -L-L, Kaindl AM. Corticosteroids in childhood epilepsies: a systematic review. Front Neurol. 2023;14:1142253. doi:10.3389/fneur.2023.1142253
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Elusive SLIPPERS Syndrome (Supratentorial Lymphocytic Inflammation with Parenchymal Perivascular Enhancement Responsive to Steroids): A Case Report and Literature Review
Khan A, Khan MM, Al-Bozom IA, Baregzai Y, Ibrahim W, Hammadi F
International Medical Case Reports Journal 2023, 16:357-361
Published Date: 10 June 2023