Back to Journals » Clinical Ophthalmology » Volume 15
Results of a Glaucoma Shared Care Model Using the Enhanced Glaucoma Staging System and Disc Damage Likelihood Scale with a Novel Scoring Scheme in New Zealand
Authors Buller AJ ![]()
Received 29 October 2020
Accepted for publication 22 December 2020
Published 7 January 2021 Volume 2021:15 Pages 57—63
DOI https://doi.org/10.2147/OPTH.S285966
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Alexander J Buller
The Eye Surgery Hastings, Hastings, Hawkes Bay, New Zealand
Correspondence: Alexander J Buller
The Eye Surgery Hastings, 309 Karamu Road South, Hastings, Hawkes Bay 4122, New Zealand
Tel +6466505798
Fax +6466503593
Email [email protected]
Purpose: To report the results of a scheme sharing follow-up glaucoma consultations between community optometrists and secondary care in a hospital ophthalmic clinic.
Patients and Methods: Optometrists measured intraocular pressure (IOP) with Goldmann Tonometry, graded the optic disc with the Disc Damage Likelihood Score (DDLS) and graded visual field tests with the enhanced Glaucoma Staging Score (eGSS). A scoring system from these tests was applied, and patients were either seen routinely 6 months later within the scheme or returned non-routinely to secondary care. Appointments within the scheme were 6-monthly with the pattern of three community optometrist visits then one hospital clinic visit.
Results: Community optometrists conducted 529 appointments for 285 patients. A total of 114 patients were seen after non-routine return to secondary care, with 61 true positives (53.5%) and 53 false positives (46.5%). Forty-one patients (14.4%) developed glaucoma progression, and 18 patients (6.3%) developed new non-glaucomatous ophthalmic diseases. Fifty-two patients were seen at 2 years after the routine return to secondary care, and three had glaucoma progression, with scheme specificity of 94.2%. The overall false-positive returns to secondary care from eGSS alone was 7.4%, and from the DDLS was 0.01%.
Conclusion: The DDLS and eGSS performed well for this population and would be recommended for use in shared care schemes, and the scoring scheme fulfilled its clinical and clerical purposes. Secondary care appointments are recommended in shared care schemes to manage the expected comorbidities and glaucoma progression, and prevent sight loss from false negatives.
Keywords: collaborative care, optometry, optometrist, primary care
Introduction
The World Glaucoma Association describes glaucoma as a group of eye diseases that cause progressive damage to the optic nerve at the point where it leaves the eye.1 Glaucoma is the second most common cause of blindness worldwide, causing blindness in an estimated 6.9 million persons globally.2 Most types of glaucoma are chronic conditions requiring long term or lifelong follow-up. This means that considerable healthcare resources are required to manage glaucoma, and this has been shown to be difficult in both developed and developing countries alike. The 2015 annual report from Blind Low Vision New Zealand identified glaucoma as the second most common cause of blindness and low vision in New Zealanders over 65, affecting 91,000 New Zealanders.3 The Eye Health Workforce Service Review in New Zealand 2010 identified both a shortage of ophthalmologists and training places for ophthalmologists to meet the required capacity for ophthalmic care, which was estimated to double over the following 10 years.4 It recommended optometrists, eye health nurse specialists and general practitioners could help increase the capacity of eye care services.
Shared care between ophthalmologists and other eye care professionals has become an established model for glaucoma follow-up and monitoring: in 2006 a national survey in England identified 66 schemes operating in 62 departments.5 No established best practice model has been identified, due to variations in types of glaucoma in local populations, availability of differing eye care professionals, local funding mechanisms, geographical constraints, and clinical requirements, for example, between initial and follow-up assessments. There is also no standardisation of the clinical dataset required for glaucoma monitoring. The World Glaucoma Association Consensus Series 8 publication on the Progression of Glaucoma recommends evaluation of both structure and function of the optic nerve for detection of glaucomatous progression, with no specific test regarded as the perfect reference standard.6
Hawke’s Bay is a New Zealand province with a population of 166,368 in the 2018 census.7 An audit of glaucoma patients attending clinic for follow-up appointments at Hawke’s Bay Hospital in 2017 found that patients who had a planned 3, 6 and 12-month follow-up period were getting appointments at an average of 10, 14 and 38 months respectively. This was after the introduction of an in-house nurse-led glaucoma clinic in 2013, which had reached full capacity. The local ophthalmologists had no spare clinical capacity for extra appointments and also identified having no spare clerical capacity to assess and make clinical decisions from reports on patient encounters from a shared care glaucoma scheme. The hospital eye clinic also had no spare infrastructure capacity to support the required increase in clinical activity levels. In Hawke’s Bay community optometry practices are numerous and are geographically well distributed, have existing infrastructure in place and are staffed with highly qualified optometrists. After discussion with local optometrists, it was agreed that a shared care system had the potential to increase publicly funded glaucoma care capacity without requiring an increase in infrastructure. A review of the equipment across the optometric practices identified that six different types of visual field machines were in use in Hawke’s Bay.
Intraocular pressure (IOP) remains the only modifiable risk factor for glaucoma progression.8 Several landmark trials have identified key IOP levels. In ocular hypertension IOP over 28 mmHg has a greater risk of optic nerve damage developing, and treated IOP below 24 mmHg reduces that risk.9 In primary open-angle glaucoma, IOP at or below 18 mmHg is associated with a lower risk of progression,10 and an IOP decrease of 30% from baseline is recommended in treating normal-tension glaucoma.11 With Goldmann tonometry inter-observer error of 2 mmHg being expected12 and diurnal fluctuations of 2–6 mmHg being normal,13 a difference in measurement of 8 mmHg between visits is within the expected range. There can also be differences in measurements expected with different tonometry devices, with Goldmann tonometry being the least variable commonly available device.12
The Disc Damage Likelihood Scale (DDLS) was introduced by Spaeth et al in 2002 as a method of quantifying clinical optic disc examination in glaucoma.14 It grades glaucomatous optic disc changes on a scale from 1 to 10 and takes optic disc size into account. It has good inter- and intra-observer variability,15 good accuracy for glaucomatous progression,16 is low cost and requires no special equipment.
The Enhanced Glaucoma Staging System (eGSS) was published in 2006 and uses the main visual field global parameters of mean deviation and corrected pattern standard deviation or loss variance to plot visual field test result onto a graph with 7 stages representing visual field advancement.17 It can be applied to visual field tests from all machines which report these visual field parameters and produces an event-based classification that can be easily applied and interpreted.
It was decided to introduce a shared care glaucoma scheme with patients being seen by optometrists in the community, with the aims of providing capacity to follow every patient with glaucoma in Hawke’s Bay on time, avoid untreated glaucoma progression leading to significant loss of sight, provide standardised glaucoma assessment across all participating caregivers, allow any community optometrist to participate, and the outcomes of each appointment were identified by the optometrist without ophthalmologist review or input.
Patients and Methods
To enrol glaucoma patients follow-up appointments were identified using the hospital clerical recall system, and their notes reviewed. Patients were included if they had no change to their IOP lowering treatment in the previous 6 months, their DDLS in both eyes was 6 or less, they could reliably perform visual fields and did not have a non-glaucomatous scotoma. Patients were excluded if they required ongoing ophthalmic monitoring or treatment for any non-glaucomatous disease.
Optometrists would see patients every 6 months for three visits, and the fourth appointment would be at the hospital outpatient department 2 years after enrolment into the shared care scheme. Gonioscopy would not be required of the community optometrists, and patients were included if gonioscopy was not required in the next 2 years. This was defined as if, at the patient’s last gonioscopy, the narrowest angle quadrant was Schaffer grade 4 or open 40 degrees then gonioscopy would need to be repeated within 4 years, and Shaffer grade 3 or open 30 degrees then repeat gonioscopy was required within 3 years. It was also considered safe for the patient to be enrolled if they were pseudophakic or patent peripheral iridotomies were present.
The appointments were co-ordinated by the hospital administration team, with patients informed by letter of the scheme and being asked to choose from the list of participating optometrists. A fee of $130 New Zealand dollars was agreed for the optometrist to provide each appointment, including the visual field test. The optometrist was sent a report from the hospital with the patient’s demographics, ophthalmic diagnoses, current treatments, known adverse reactions, and last recorded visual acuity, IOP, DDLS and eGSS.
Optometrist orientation to the scheme and explanation of the eGSS was performed in two group sessions. To assess the application of the DDLS, each optometrist examined a reference set of 20 stereo optic disc photographs providing a disc drawing and DDLS of each. These were then graded by the local glaucoma specialist ophthalmologist and the optometrists’ results compared for acceptable agreement using Cohen’s Kappa, similar to the assessment of graders for the World Health Organisation simplified trachoma grading system.
Optometrists recorded the patient’s Goldmann IOP, DDLS and eGSS from each eye at each visit. The outcome of the visit would be either a routine review within the scheme in 6 months or non-routine referral back to the hospital, either due to a new ophthalmic condition being identified or worsening of the glaucoma testing. To provide autonomous decision-making for the optometrists a scoring system was devised for the glaucoma tests based on the clinical risk of changes in tests. Table 1 shows the scoring system. If the patient was referred back to the hospital early due to glaucomatous changes then possible delay before being seen at the hospital was anticipated, and an additional topical IOP lowering medication was added after the community optometrist visit. A protocol of IOP lowering eyedrops prescribing was in a pre-written letter which was sent to the patient’s GP requesting the next appropriate drop be added to the patient’s prescription.
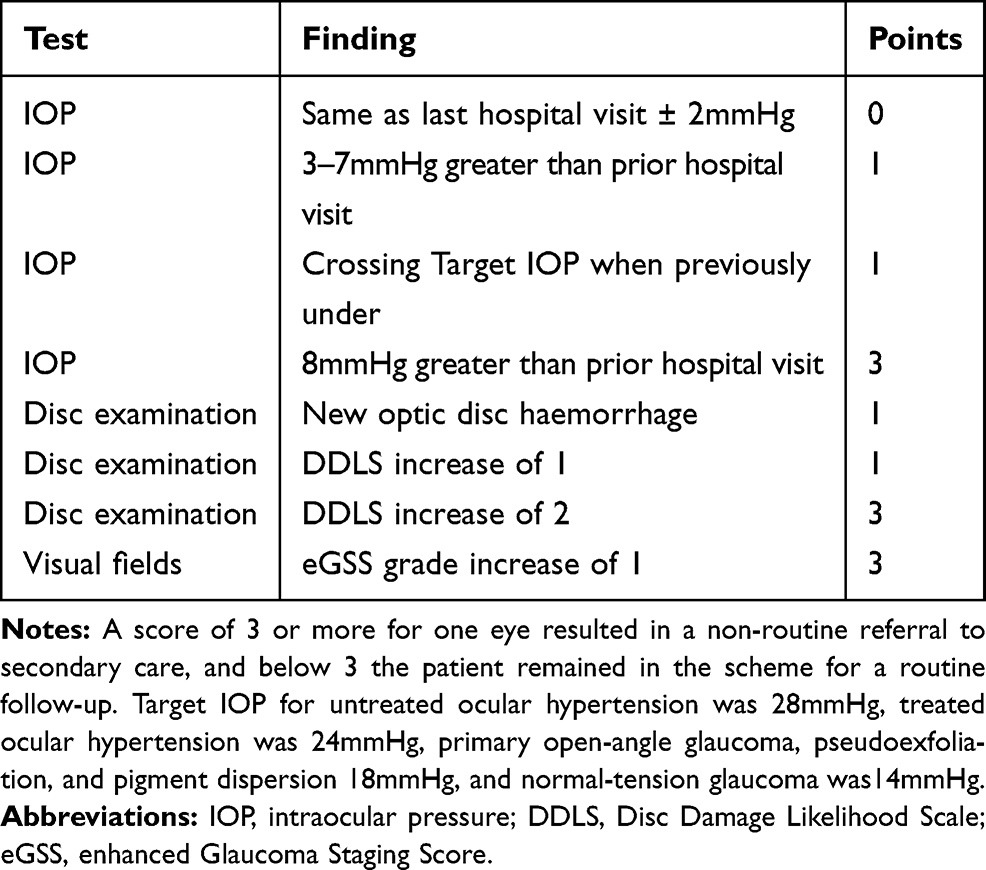 |
Table 1 Shared Care Scheme Scoring System from Glaucoma Follow-Up Appointment |
Statistics were performed using Wizard Statistics and Analysis version 1.9.44 (https://www.wizardmac.com).
This audit is exempt from ethical committee review and approval according to Standard Operating Procedures for Health and Disability Ethics Committees New Zealand section 3 paragraph 30.18 This audit does comply with the Code of Health and Disability Services Consumers’ Rights 199619 and the tenets of the Declaration of Helsinki.
Results
Twenty-three optometrists enrolled to participate. Using Cohen’s Kappa statistic 20 had substantial inter-rater reliability level of agreement (0.61–0.80) with DDLS grading pictures, and 3 achieved this after short further training on the application of the DDLS to their own disc drawings.
The first appointment at a community optometrist was in June 2017 and results were collected in March 2020. The number of patients enrolled was 301. The age range was 41–95 (mean 74).
The total number of community optometrist appointments attended was 529. Patients did not attend 18 appointments, with 16 of these being first appointments, 2 being second appointments, and none third appointments. During the data collection period, 9 patients (3.0%) died and 4 patients (1.3%) moved out of the area. One patient returned to the hospital for follow-up due to no participating optometrist being closer to their rural address.
From 285 first appointments attended 202 patients (70.9%) were booked for routine community optometrist follow-up and 83 (29.1%) were referred non-routinely back to the hospital. The outcomes of 148 second appointments were 112 patients (75.7%) were booked for routine community optometrist follow-up and 36 (24.3%) were referred non-routinely back to the hospital. The outcomes of 86 third appointments were 81 patients (94.2%) booked for routine follow-up and 5 (5.8%) were referred non-routinely back to the hospital.
Fifty-two patients were seen at the hospital clinic following routine return to the clinic 2 years after enrolment into the scheme. Forty-nine (94.2%) of those patients were not found to have glaucoma progression or IOP increase requiring treatment, with 3 (5.8%) of those patients being listed for cataract surgery. Three patients had additional IOP lowering eyedrops added to their regime, two for raised IOP without an optic disc or visual field change, and one patient had DDLS and eGSS progression.
Table 2 shows the reasons for 124 non-routine referrals back to the hospital clinic. Six of these patients either died or moved out of the area, and four had not been seen at the time of data collection. One hundred and fourteen were reviewed and there were 61 true positives (53.5%), and 53 false positives (46.5%).
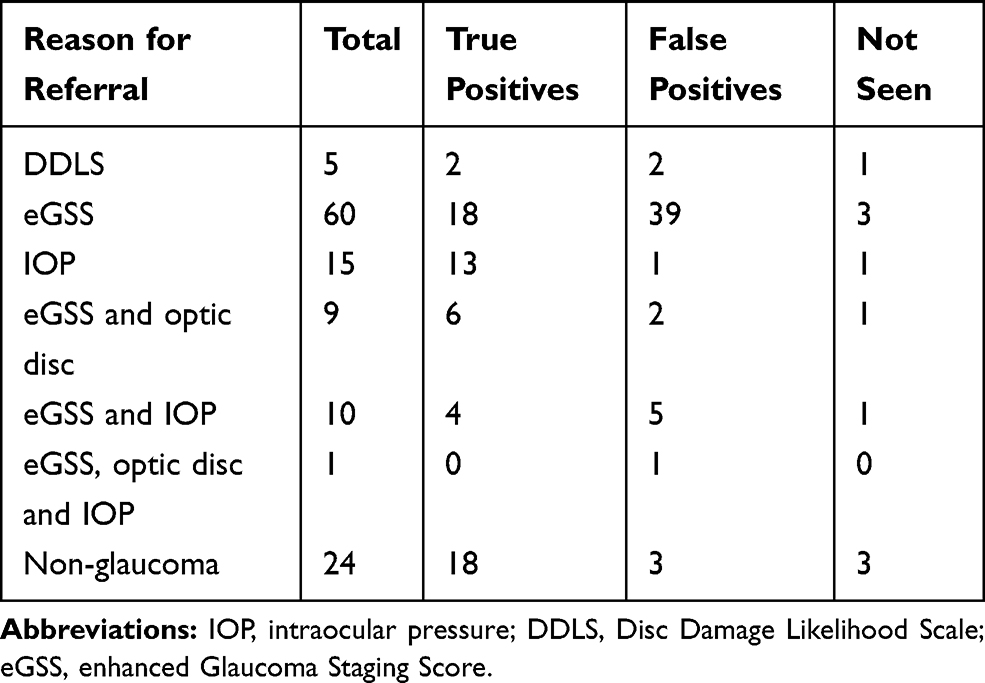 |
Table 2 The Reasons for Non-Routine Referrals to Secondary Care from Community Optometrist Visits and the Outcomes |
Out of 61 confirmed true positive non-routine returns to the hospital clinic 38 (62.3%) were due to uncontrolled IOP or glaucoma progression, 19 (31.1%) were due to the development of non-glaucomatous ophthalmic conditions, and 4 (6.6%) were unable to complete the required testing reliably. From the 285 first community optometrist appointments, 27 cases (9.5%) of confirmed uncontrolled glaucoma or increased IOP were identified, and of 148 second community optometrist appointments 11 cases (7.4%) of confirmed uncontrolled glaucoma or increased IOP were identified.
Out of 83 non-routine referrals from first community optometrist appointments, 43 (51.8%) were true positives, 32 (38.6%) false positives, and 8 (9.6%) either died, moved away or were not seen. From 36 non-routine referrals after second community optometrist appointments, 16 (44.4%) were true positives, 19 (52.8%) false positives, and 1 (2.8%) was not seen, and for third community optometrist appointments, there were 5 total non-routine referrals with 2 true positives, 2 false positives and 1 not seen. A Pearson correlation test shows a positive correlation (p=0.040) between total non-routine referrals and true positive rates for first, second and third community optometrist appointments.
Discussion
The primary aim of this scheme was to create capacity for appointments for glaucoma patients. Twenty-three optometrists volunteered for the scheme. They conducted 529 appointments over a 34-month period averaging one appointment every 1.5 months per optometrist. As such, there is the capacity to increase the number of patients in the scheme without overwhelming individual optometry practices. All second and third appointments with community optometrists were available within the planned 6-month follow-up period.
Another outcome aim was for community optometrists to be able to work independently of secondary care. The report from each eye was in the form of three numbers (IOP, DDLS and eGSS). These event-based numerical data enabled a relatively simple scoring scheme to be used, and simplified communication between primary and secondary care. A Pearson correlation test found a positive correlation between non-routine referral rates from first, second and third community appointments suggesting first appointments did not produce extra non-routine referrals due to a learning curve being needed for the optometrists to use the referral criteria.
Forty-one patients developed confirmed glaucoma progression or required increased IOP lowering therapy giving a glaucoma progression rate of 14.4% in this population during this period. This is in line with figures published in other populations.20 There were also 18 patients (6.3%) who developed new non-glaucomatous ophthalmic diseases requiring management at the hospital ophthalmology clinic, giving a combined 20.7% rate of development of confirmed ophthalmic disease requiring secondary care management. The inclusion criteria for this scheme were designed to include glaucoma cases deemed at low risk for either progression of glaucoma or significant sight loss during the 2-year period. Alterations to the inclusion criteria would alter the expected rates of new problems developing. Gonioscopy was excluded from the scheme as a source of referral back to the hospital clinic. These figures show that disease progression can be expected at high rates in glaucoma follow-up patients and shared care schemes should include secondary care reviews to manage the expected co-morbidities and glaucoma progression, perform other examinations such as gonioscopy at appropriate intervals, and prevent significant sight loss from false negatives within a follow-up system.
A shared care scheme would ideally have a low false-positive return rate and good specificity. Fifty-three false-positive appointments were generated for the hospital clinic (10.0%). Fifty-two patients were seen after routine return to the hospital clinic at 2 years, with three patients being found to have glaucoma progression, yielding a specificity of 94.2%. This progression could have developed between their third community optometrist appointment and return to the hospital clinic (which in most cases was more than 6 months between appointments) and so the overall scheme specificity could be higher. With high specificity and acceptable sensitivities, the scoring scheme performed satisfactorily and adjustments are not planned for the continuation of the scheme.
The use of the DDLS as a method to monitor the glaucomatous optic disc was very successful. The enrolled optometrists were all postgraduate and already experienced with optic disc examination. Training on the DDLS was quick and all optometrists who applied were included in the scheme. The optometrists were supplied with the patients’ DDLS from the latest hospital assessment, with only increases of 2 on the DDLS scale referred back to the hospital non-routinely. From a total of 529 community optometrist appointments there were 5 non-routine referrals to the hospital from DDLS changes alone, and out of 4 seen two were false positives (0.01%). Using optometrists to examine the optic disc to determine the DDLS meant that no costs related to disc imaging were incurred, and 6.3% of patients had their non-glaucomatous pathology identified and referred to the hospital ophthalmic clinic appropriately. Feedback from the optometrists was a request for available optic disc stereo photographs for practice, and this has been developed and published as a website at www.glaucoma4k.org.
Visual fields are a complex and subjective test, and there is an expected rate of short- and long-term fluctuation in results from real-world data. Trend-based analysis is not readily available when comparing results from different machines. There are also logistical problems with visual field databases co-ordinating across multiple sites leading to problems with test results being available at different appointments. The eGSS mitigates these factors by using an event-based scale with seven steps using global visual field parameters. Only increases in eGSS were returned to the hospital, any patients whose eGSS decreased compared to their hospital visual field were kept within the scheme for follow-up routinely. Patients performed visual field testing once only per community optometrist appointment, with no re-testing for changes in the eGSS score. There were 39 (7.4%) false-positive non-routine returns to the hospital clinic generated from changes in the eGSS alone. This is similar to measured fluctuation levels in the eGSS predecessor, the Glaucoma Staging System, published in 1998.21 There were also 18 patients (3.4%) with eGSS progression which was confirmed on re-testing with the hospital’s visual field machine. Of patients seen routinely at 2 years, one out of 52 patients showed eGSS progression along with DDLS progression. These figures give a sensitivity (defined as not producing false-positive returns to the hospital clinic) of 92.6% and a specificity of 98.1% for the performance of the eGSS in these circumstances. Overall the eGSS performed well. It produced measurable results which integrated well between primary and secondary care across six different types of visual field machine with good sensitivity and specificity, and its use for shared care schemes can be recommended.
Several investigations have quantified the clinical examination, test interpretation and the clinical decision-making of optometrists versus ophthalmologists in glaucoma care.22–27 Substantial agreement between ophthalmologists and optometrists on management decisions has been demonstrated in many of these,22–27 with higher levels of training being linked with higher agreement between care providers.25 The results from this scheme align with these findings of good agreement between the optometrists’ clinical examination findings and decisions to return patients non-routinely to the hospital, and the ophthalmologists’ decisions when these patients were seen.
The scheme was introduced in response to an audit which found that glaucoma follow-up appointments were delayed compared to the planned follow-up period. Patients enrolled in the study were from this population, so when attending their first community optometrist appointment were at a larger than planned gap from their last hospital clinic assessment. This could increase the amount of new glaucoma and non-glaucoma problems identified at first appointments in the scheme. It would be helpful to include greater numbers of patients seen routinely after return to hospital clinics; however, in March 2020, most routine hospital ophthalmic outpatient activity was suspended due to the COVID-19 global pandemic, with fewer appointments being conducted over the following months and further delays to routine appointments caused by this. The performance of different visual field machines in the scheme was not assessed, but the overall numbers from each optometric practice are unlikely to provide the statistical power for this. Another drawback is that patients within the scheme perform visual field testing on the hospital machine only once every 2 years, making trend-based analysis of this testing less accurate due to fewer tests being performed less frequently.
Conclusion
The results from this shared care glaucoma scheme support the Disc Damage Likelihood Scale being recommended for optic disc examination reporting in shared care between primary and secondary care.
The Enhanced Glaucoma Staging Score can be recommended for visual field monitoring in shared care.
A shared care scheme should expect glaucoma progression and the development of new ophthalmic diseases in patients with previously stable glaucoma, and have provision for managing these.
Acknowledgments
The author would like to acknowledge Jane Hawthorn for her work in collecting data and coordinating and providing clinical care for patients during the conduction of the shared care scheme.
Disclosure
The author reports no conflicts of interest in this work.
References
1. World Glaucoma Association [homepage on the Internet]. What is Glaucoma?; 2020. Available from: https://wga.one/wga/what-is-glaucoma/.
2. World Health Organization [homepage on the Internet]. Blindness and Visual Impairment; 2019. Available from: https://www.who.int/health-topics/blindness-and-vision-loss#tab=tab_1.
3. Blind Low Vision New Zealand [homepage on the Internet]. Blindness and low vision in New Zealand latest statistics; 2015. Available from: https://blindlowvision.org.nz/information/statistics-and-research/.
4. New Zealand Ministry of Health [homepage on the Internet]. O’Rourke M, Frederikson L, Jacobs R, et al. Eye health workforce service review; 2011. Available from: https://www.health.govt.nz/system/files/documents/pages/eye-health-review-may-2011.pdf.
5. Vernon SA, Adair A. Shared care in glaucoma: a national study of secondary care lead schemes in England. Eye. 2010;24:265–269. doi:10.1038/eye.2009.118
6. Weinreb RN, Garway-Heath DF, Leung C, Crowston JG, Medeiros FA. WGA Consensus Series 8 Progression of Glaucoma. Amsterdam: Kugler Publications; 2011.
7. Stats NZ Tatauranga Aotearoa [homepage on the Internet]. Census population and dwelling counts; 2018. Available from: https://www.stats.govt.nz/information-releases/2018-census-population-and-dwelling-counts.
8. Leske MC, Heijl A, Hussein M, Bengtsson B, Hyman L, Komaroff E; Early Manifest Glaucoma Trial Group. Factors for Glaucoma Progression and the effect of treatment: the Early Manifest Glaucoma Trial. Arch Ophthalmol. 2003;121:48–56. doi:10.1001/archopht.121.1.48
9. Gordon MO, Beiser JA, Brandt JD, et al. The ocular hypertension treatment study baseline factors that predict the onset of primary open-angle glaucoma. Arch Ophthalmol. 2002;120:714–720. doi:10.1001/archopht.120.6.714
10. The AGIS Investigators. The Advanced Glaucoma Intervention Study (AGIS): 7 The relationship between control of intraocular pressure and visual field deterioration. Am J Ophthalmol. 2000;130:429–440. doi:10.1016/S0002-9394(00)00538-9
11. The Collaborative Normal Tension Glaucoma Study Group. Comparison of glaucomatous progression between untreated patients with normal-tension glaucoma and patients with therapeutically reduced intraocular pressures (NTGS). Am J Ophthalmol. 1998;126:487–497. doi:10.1016/S0002-9394(98)00223-2
12. Tonnu P-A, Ho T, Sharma K, White E, Bunce C, Garway-Heath DF. A Comparison of four methods of tonometry: method agreement and interobserver variability. Br J Ophthalmol. 2005;89:847–850. doi:10.1136/bjo.2004.056614
13. Asrani S, Zeimer R, Wilensky J, Geiser D, Vitale S, Lindenmuth K. Large diurnal fluctuations in intraocular pressure are independent risk factor in patients with glaucoma. J Glaucoma. 2000;9:134–142. doi:10.1097/00061198-200004000-00002
14. Spaeth GL, Henderer J, Liu C, et al. The disc damage likelihood scale: reproducibility of a new method of estimating the amount of optic nerve damage caused by glaucoma. Trans Am Ophthalmol Soc. 2002;100:181–185.
15. Henderer JD, Liu C, Kesen M, et al. Reliability of the disc damage likelihood scale. Am J Ophthalmol. 2003;135:44–48. doi:10.1016/S0002-9394(02)01833-0
16. Kara-Jose AC, Melo LAS
17. Brusini P, Filacordia S. Enhanced glaucoma staging system (GSS2) for classifying functional damage in glaucoma. J Glaucoma. 2006;15:40–46. doi:10.1097/01.ijg.0000195932.48288.97
18. Standard Operating Procedures for Health and Disability Ethics Committees [homepage on the Internet]. Auckland: Health and Disability Commissioner; 2019. Available from: https://ethics.health.govt.nz/operating-procedures.
19. Code of Health and Disability Services Consumers’ Rights [homepage on the Internet]. Auckland: Health and Disability Commissioner; 1996. Available from: https://www.hdc.org.nz/your-rights/about-the-code/code-of-health-and-disability-services-consumers-rights/.
20. Saunders LJ, Medeiros FA, Weinreb RN, Zangwill LM. What rates of glaucoma progression are clinically significant? Expert Rev Ophthalmol. 2016;11:227–234. doi:10.1080/17469899.2016.1180246
21. Kocak I, Zulauf M, Bergamin O. Evaluation of the Brusini glaucoma staging system for typing and staging of perimetric results. Ophthalmologica. 1998;212:221–227. doi:10.1159/000027296
22. Ho S, Vernon SA. Decision making in chronic glaucoma - optometrists vs ophthalmologists in a shared care service. Ophthalmic Physiol Opt. 2011;31:168–173. doi:10.1111/j.1475-1313.2010.00813.x
23. Banes MJ, Culham LE, Bunce C, Xing W, Viswanathan A, Garway-Heath D. Agreement between optometrists and ophthalmologists on clinical management decisions for patients with glaucoma. Br J Ophthalmol. 2006;90:579–585. doi:10.1136/bjo.2005.082388
24. Marks JR, Harding AK, Harper RA, et al. Agreement between specially trained and accredited optometrists and glaucoma specialist consultant ophthalmologists in their management of glaucoma patients. Eye. 2012;26:853–861. doi:10.1038/eye.2012.58
25. Scheetz J, Koklanis K, Long M, Lawler K, Karimi L, Morris ME. Validity and reliability of eye healthcare professionals in the assessment of glaucoma - a systematic review. Int J Clin Pract. 2015;69:689–702. doi:10.1111/ijcp.12600
26. Ho K, Stapleton F, Wiles L, et al. Systematic review of the appropriateness of eye care delivery in eye care practice. BMC Health Serv Res. 2019;19:646. doi:10.1186/s12913-019-4493-3
27. Ford BK, Angell B, Liew G, White AJR, Keay LJ. Improving patient access and reducing costs for glaucoma with integrated hospital and community care: a case study from Australia. Int J Integr Care. 2019;19:5. doi:10.5334/ijic.4642
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.