Back to Journals » Clinical Ophthalmology » Volume 15
Restructuring Wet Age-Related Macular Degeneration Services During the COVID-19 Pandemic to Allow Social Distancing Outpatient Clinics (SDOC)
Received 7 July 2020
Accepted for publication 3 November 2020
Published 17 February 2021 Volume 2021:15 Pages 651—659
DOI https://doi.org/10.2147/OPTH.S269596
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Markus Groppe,* Mandeep Singh Bindra*
Retina Unit, Buckinghamshire Healthcare NHS Trust, Stoke Mandeville and Amersham Hospital, Aylesbury, HP21 8AL, UK
*These authors contributed equally to this work
Correspondence: Markus Groppe
Retina Unit, Buckinghamshire Healthcare NHS Trust, Stoke Mandeville and Amersham Hospital, Aylesbury, HP21 8AL, UK
Email [email protected]
Background: COVID-19 has had a major impact on health-care provision. Social distancing will impact the organization of outpatient clinics (OCs) and require general restructuring of health care.
Methods: Our retinal team participated in a structured fact-finding session to implement social distancing of patients and staff in wet age-related macular degeneration (wAMD) clinics. Clinic flow and performance were continually reviewed and improved. A retrospective audit of all wAMD follow-up appointments was conducted for 4 weeks from the start of the UK lockdown. A search for clinical guidance regarding retinal services was performed on the homepages of international professional bodies. The guidelines were compared to the implemented changes in our wAMD social distancing OCs (SDOCs) and potential risk examined.
Results: The changes in clinic setup to achieve SDOCs are described. The average total time spent in the clinic area by each patient has reduced by 27%. The audit concluded that 65% of patients needed a treatment interval of 4– 7 weeks after their appointment, 17% at either 8 or 9 weeks, and 18% at 10 weeks or beyond. The UK, Australian–New Zealand, US, and German professional ophthalmology bodies have published divergent guidelines, but all recommended a continuation of anti-VEGF injections.
Conclusion: Health-care provision will change and hospitals and outpatient facilities will have to adapt to the COVID-19 epidemic. We describe a clinic setup (SDOCs) that minimizes risk to patients and staff, while maintaining the ability to treat each patient and their disease individually.
Keywords: age-related macular degeneration, COVID-19, social distancing, SDOC
Introduction
The World Health Organization declared the SARS-CoV-2/COVID-19 outbreak a pandemic and global health emergency on March 11, 2020.1
This pandemic has had a major impact on health-care provision, due to the care of affected patients directly2–10 and indirectly due to changes in provision of care of other patients. While only a small proportion of patients with COVID-19 show ocular involvement, cases of conjunctivitis have been reported and an increase in cases of ocular trauma due to change in patient behavior have been postulated. The major impact of COVID-19 in ophthalmology has been as a result of delayed treatment and will only be fully appreciated in the coming months. Social distancing measures and guidelines will have a major impact on the organization of outpatient (ambulatory) clinics and require general restructuring of health services worldwide to protect health-care staff and patients alike. Ophthalmologists are in a high-risk category for transmission of COVID-19, due to close patient contact during examination and treatment and cumulative exposure to patients from their high-volume eye clinics and theaters. Stringent social distancing and hygiene measures are crucial to prevent further outbreaks of COVID-19 in ophthalmology departments.
There has been published guidance on how to manage ophthalmology patients during the pandemic from various professional bodies, including the Royal Australian and New Zealand College of Ophthalmologists (RANZCO),11 the American Academy of Ophthalmology (AAO),12 the American Society of Retina Specialists (ASRS),13 and the Royal College of Ophthalmologists (RCOphth).14
Recommended strategies include delaying and rebooking appointments,14 virtual clinics,15 teleophthalmology,16 treatment-only clinics,17 and social distancing clinics.18
It is recommended that patients with active wet age-related macular degeneration (wAMD) receive ongoing treatment and hospital visits to avoid visual loss.11–14
This article examines the potential implications for our wAMD patients had we not maintained individual intravitreal treatment regimes. It explains the restructuring of our wAMD services and the introduction of social distancing outpatient clinics (SDOCs).
Methods
For the last 4 years, our wAMD service at Buckinghamshire NHS Trust, Amersham Hospital has been run using a one-stop clinic pathway with a “treat and extend” treatment protocol utilizing anti-VEGF injections (ranibizumab and aflibercept). At each visit, each patient has visual acuity and intraocular pressure measurement, macular ocular coherence tomography (OCT; Nidek Retina Scan Duo), face-to-face consultation with a doctor, and an intravitreal injection if required.
As a response to the COVID-19 pandemic in the UK, all members of our multidisciplinary team, including nurses, nurse injectors, admin staff, doctors, and technicians participated in a structured fact-finding session to discuss and analyze the current clinic setup, clinic flow, and treatment of wAMD patients. The session was followed by an interactive workshop to explore ways to reduce or eliminate unessential close contact, in order to increase safety and social distancing of patients and staff. Particular attention was paid to each step of the patient journey and every staff–patient interaction. All team members made suggestions on how to improve clinic flow and reduce unessential close contact with the patients. The suggested changes were implemented on March 9, 2020, prior to any national ophthalmology guidance being issued. The layout of the unit was altered so that 2m distancing was possible at all times. The team received clear briefings, and standard operating procedures were developed.
Clinic flow and performance were continually reviewed at daily safety meetings and proposed improvements discussed and implemented when indicated, resulting in a rapid evolution of the model.
We also conducted a retrospective audit of all wAMD follow-up appointments using the hospital’s electronic patient-record system (Medway) for 4 weeks from the start of the UK lockdown on March 23, 2020. Appointment dates, average appointment duration, appointment outcome, follow-up date, and number of patients who received intravitreal treatment were recorded. The interval between the appointment and the next requested follow-up was measured in weeks. The analysis window was kept to 4 weeks, which is the minimum interval in our treat-and-extend treatment protocol,19 to avoid analyzing more than one appointment per patient.
The average appointment duration was compared to the 4 weeks prior to introducing the changes. The review of the patient-booking system, canceled and missed appointments, and follow-up times was fully anonymized and in accordance with local and NHS guidelines regarding clinical audit and in compliance with the Declaration of Helsinki. Separate ethics approval was not required.
A search for clinical guidance regarding ophthalmology OCs and retinal services was conducted on the homepages of the RCOphth, AAO, ASRS, RANZCO,11–14and German Society of Ophthalmology (Deutsche Ophthalmologische Gesellschaft [DOG]).20
We reviewed the content of the websites to find any guidance regarding wAMD during COVID-19.
These suggested guidelines were compared to the implemented changes in our wAMD SDOCs, and we examined potential risks to our specific wAMD population if we had not continued with our model.
Results
At the beginning of the COVID-19 pandemic in the UK in early March 2020, our retinal team felt strongly that to prevent sight loss in our patients with wAMD, not only should we continue to see and treat them, but we should try to maintain each patient’s individualized treatment regime if we could do so safely. The wAMD clinic had already previously been relocated to a nonacute hospital (cold) site.
The multidisciplinary workshop produced a number of proposed changes. The initial changes were implemented and then continuously discussed and improved after daily multidisciplinary safety meetings, and are summarized in Table 1.
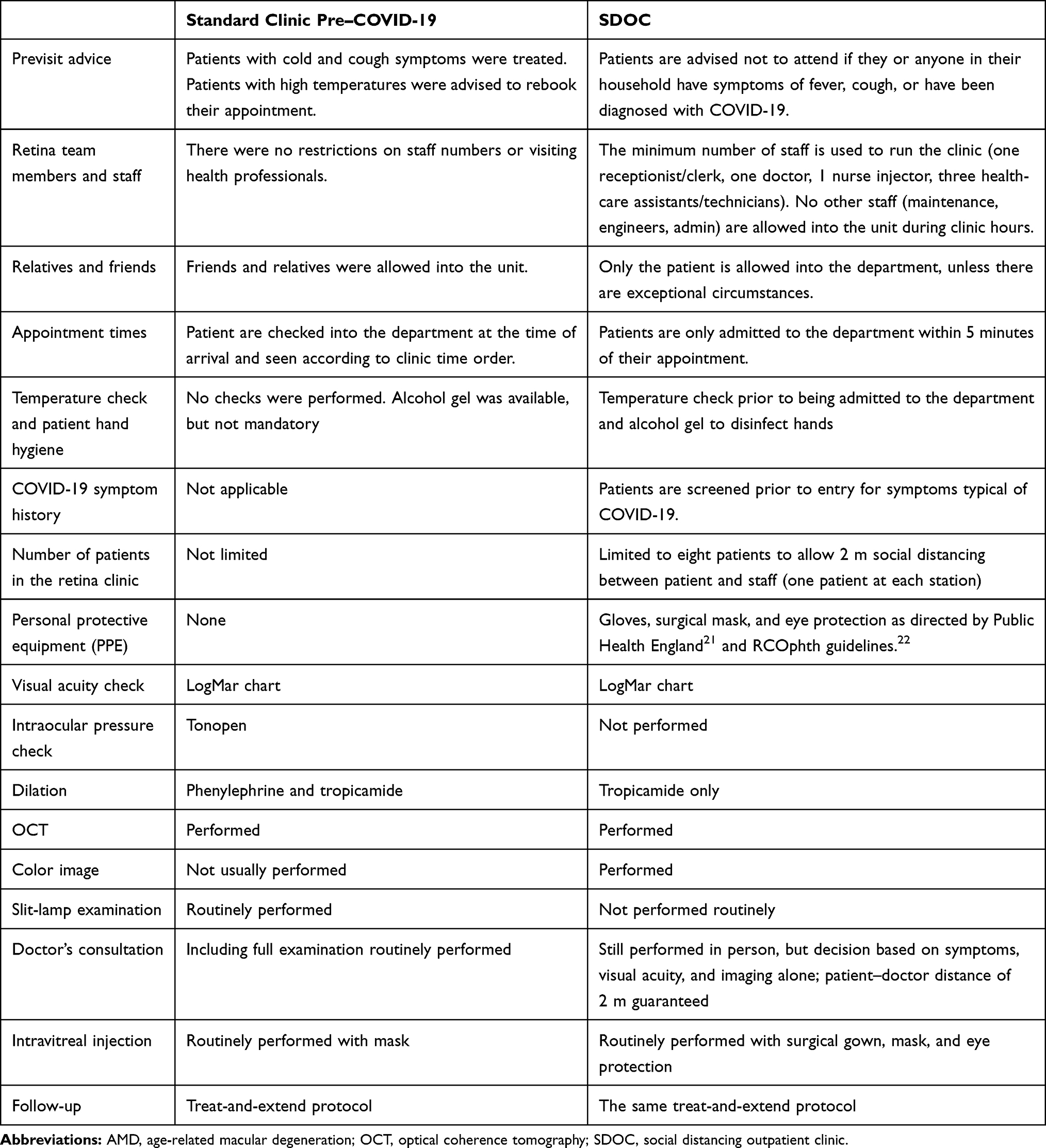 |
Table 1 Changes Introduced to our Wet AMD Clinic to Allow Social Distancing (SDOC) |
All changes were introduced with the aim of minimizing the number of interactions with staff, allowing patients to maintain adequate distance from staff and other patients ideally at all times (SDOCs), and minimizing the time patients spent in the unit.
Social distancing was achieved at check-in, visual acuity measurement, consultation with the doctor, at any waiting time, and at checkout. Contact <2 m was required only during instillation of drops for pupil dilation, during the intravitreal injection procedure, and for OCT and imaging, as our device requires a 1.2 m working distance between technician and patient. Adequate personal protective equipment is worn by staff at each interaction,21,22 and meticulous hand hygiene with soap and water or hand-sanitizing gel is performed between each interaction.
We discussed the necessity of pupil dilation and whether this could be avoided. We concluded that the color-image quality through an undilated pupil using our device did not allow adequate interpretation on a reliable repeatable basis.
Figure 1 illustrates the design of our wAMD unit prior to and after our COVID-19 changes. Originally, patients sat in the waiting area prior to and between each step. Patients are now greeted at the entrance to the unit, rather than reporting to the clinic reception, and are asked about any symptoms of COVID-19. Their temperature is checked, and they disinfect their hands with hand-sanitizing gel prior to entering. The patient is then guided directly to the vision bay, where visual acuity is measured and dilating drops instilled. Once the pupils are adequately dilated, an OCT scan and color image are taken. The patient is then guided to one of three examination bays. The patient’s electronic medical records and images have been preloaded onto the two computer screens in the room by the technician. One doctor rotates between three consulting bays performing strict hand hygiene between each. Clinical management decisions are made after consultation with the patient and reviewing the images. Routine slit-lamp retinal examination is no longer performed, and the rooms are large enough to allow a distance of 2 m between patient and doctor at all times. The patient is then taken directly to the injection room. During this time, the patient’s follow-up appointment is made and they exit the unit directly after receiving their injection.
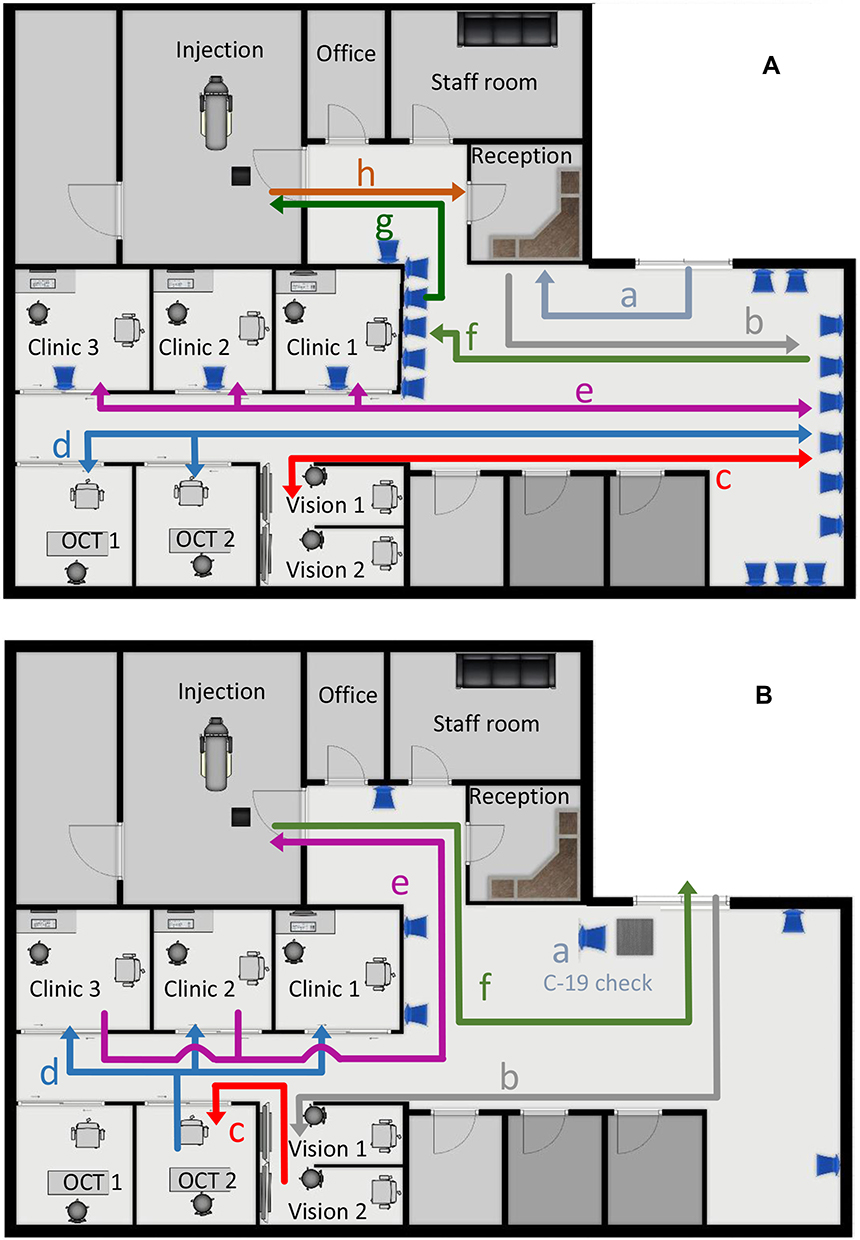 |
Figure 1 (A) Clinic flow prior to COVID-19: a) patient check-in reception desk, b) patient sits in waiting area, c) patient gets a vision check and waits again in the waiting area, d) OCT scan and waiting area, e) consultation and waiting area, f) sub–waiting area injection, g) intravitreal anti-VEGF injection, h) checkout for follow-up appointment. (B) Social distancing outpatient clinic setup. Waiting-room chairs are removed to a minimum and not usually used, and the second chair in clinic rooms for relatives or friends is removed. The clinic rooms are used as waiting areas prior to consultation and injection: a) temperature check and COVID-19 questionnaire, b) direct transfer to vision bays, c) OCT scan, d) patient transfer to clinic room, d) patient transfer to injection room, e) patient leaves the unit via the reception desk with the follow-up appointment. Abbreviation: OCT, optical coherence tomography. |
The total time spent in the clinic by each patient has reduced to a mean of 40 minutes for check-in, visual acuity measurement, pupil dilation, OCT and color imaging, consultation, intravitreal injection, and checkout compared to 55 minutes prior to the changes.
During our 4-week audit period from UK lockdown on March 23, 2020 to April 17, 2020, a total of 661 patients had booked appointments. In sum, 64 of these (9.7%) did not attend their appointment, double our pre-COVID-19 nonattendance rate (4.7%). Of the 597 patients seen in clinic, 508 received intravitreal injections, 583 received a follow-up appointment, and ten were discharged. Figure 2 illustrates the requested follow-up interval following the patient’s appointment: 65% of patients were booked to be seen 4–7 weeks after their appointment, 17% at either 8 or 9 weeks, and 18% at 10 weeks or beyond.
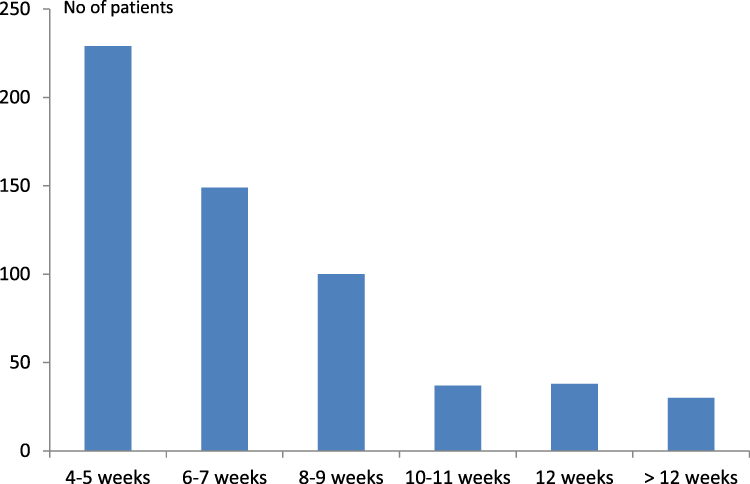 |
Figure 2 Follow-up interval of wet age-related macular degeneration patients who were seen during UK lockdown between March 23, 2020 and April 17, 2020 (n=597). |
All management decisions were made using our treat-and-extend protocols. Of the 508 patients who received an injection, 378 (74%) were booked to receive their next appointment and intravitreal anti-VEGF treatment at a <8-week interval, 72 (14%) at an 8-week interval, and 75 (15%) at an interval >8 weeks (Figure 3).
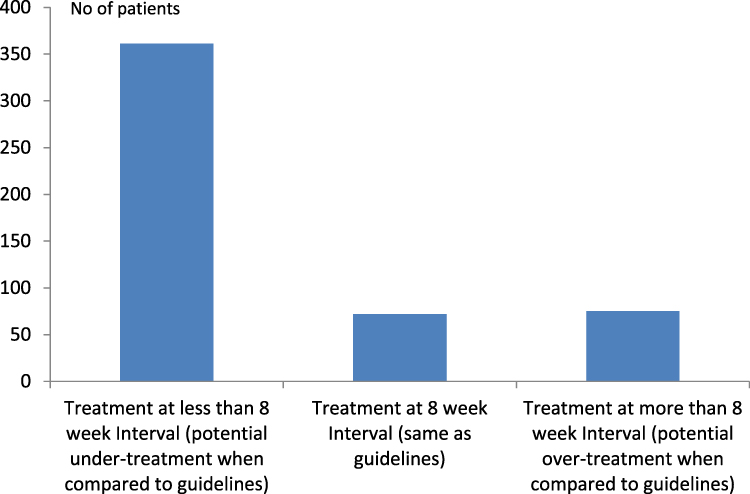 |
Figure 3 Number of patients requiring treatment before 8 weeks, at 8 weeks, and later than 8 weeks and consequence when compared to treatment as per the Royal College of Ophthalmologists COVID-19 age-related macular degeneration guidelines. |
In sum, 75 of 597 (12.6%) patients did not receive an injection, as they were on the monitor-and-extend part of the protocol.
The publicly available guidance for management of wAMD from national professional ophthalmology bodies is summarized in Table 2.
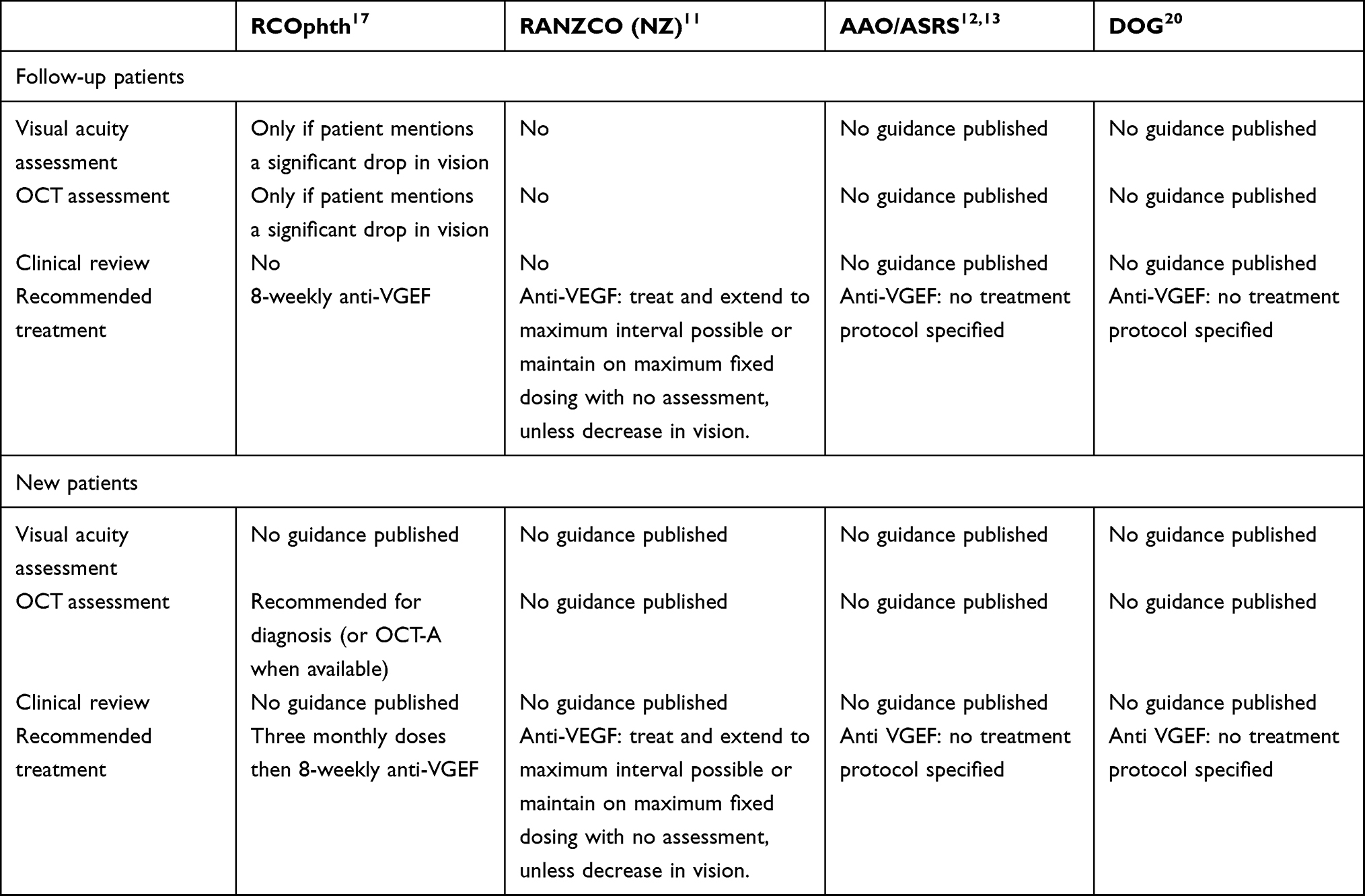 |
Table 2 Summary of Published Guidance for Treatment of wAMD Patients During the COVID-19 Pandemic |
The RCOphth and the New Zealand section of RANZCO have issued detailed guidance. The RCOphth suggests 8-weekly intravitreal injections in treatment only clinics. RANZCO suggests a treat-and-extend regime.
The American and German bodies (AAO, ASRS, DOG) state that anti-VEGF injection should be continued, but do not specify specific treatment regimes.
Discussion
Social distancing due to COVID-19 will need to continue for the foreseeable future.23 Health-care provision is changing, and hospitals and outpatient facilities will have to adapt to meet these requirements.24 Temperature checks and screening questions will become mandatory before entering health-care facilities,25 as will social distancing measures.
It will become mandatory to challenge the traditional methods of service provision to continue to provide long-term high-quality care to wAMD patients and provide a safe environment for both patients and staff. Different models of care provision already exist in wAMD clinics, with the main differences being the treatment protocols (treat and extend vs fixed dosing or as needed)26,27 and the timing of consultation and treatment (one stop vs two stop).
Differences in clinic and treatment protocols are dependent (among others) on the layout and design of the department, health economics,28,29 patient compliance, and individual preferences of treating specialists.
In a COVID-19 era, a one-stop clinic model has clear benefits in terms of reduced clinic visits and thus reduced exposure for patients and staff. We feel treat-and-extend treatment algorithms allow the best combination of treatment and visit burden, outcomes, and costs.30 This is the treatment regimen currently recommended in the RANZCO COVID-19 guidelines.11 Any change to a different treatment regimen needs careful planning, however.19
We feel our clinic setup has minimized risks to patients and staff, while maintaining the ability to treat each patient and their disease individually. Our wAMD clinic is designed to allow seamless, one-way patient flow and efficiency (Figure 1B). The clinic is run by one senior clinician, who sees patients in three rooms. The design of the unit was ideal to allow the introduction of SDOCs with minimal physical changes and no additional costs. We believe that social distancing will become mandatory for all outpatient and ambulatory departments and the need for increased clinical space will become the limiting factor in providing care. It is suggested that patient numbers per clinic need to be reduced to achieve SDOCs.14 We have shown that we can see and treat the same number of patients as we were pre–COVID-19 and reduce visit duration on average by 27% or 15 minutes.
The numbers of patients not attending our clinics initially increased, due to anxiety regarding COVID-19. After an awareness campaign of telephone reassurance and explanation to patients informing them of safety measures introduced, cancelation rates have now reduced to pre–COVID-19 levels.
The published national guidance for wAMD has varied from country to country, and has mostly advocated the approach of maintaining care for those patients who require treatment and weighing their risk of coming to harm through failure to treat serious eye disease against the risk of patients acquiring COVID-19 infection during an ophthalmology appointment.11–14,16,20
Patients with active wAMD require ongoing treatment to avoid visual loss. One approach for these patients has been to maintain all patients on 8-weekly anti-VEGF therapy with no clinic review, unless they mention a significant drop in vision at their injection visit.17,31 Although this might be a workable solution initially for some units, patients will require monitoring of disease activity with OCT scans and fundus examination/imaging for ongoing care.
Whereas other areas of ophthalmology-care provision might lend themselves to the provision of telemedicine32 or virtual clinics,33 direct patient contact is required for imaging and the administration of intravitreal anti-VEGF therapy in patients with wAMD. It is well recognized that direct patient–doctor interaction and communication significantly increases patient satisfaction34 and is of particular importance in AMD clinics.35 We have shown that we can see the same number of patients in a one-stop clinic as in a virtual clinic (20–25 patients per 3-hour session per doctor). We achieve that while maintaining patient–doctor interaction, treating patients with intravitreal therapy at the same visit, and maintaining patient and staff safety with social distancing.
If we had switched all our patients to 8-weekly intravitreal treatments during this period, 71% would have had a treatment interval longer than indicated using an individualized treatment plan with a treat-and-extend protocol, while 15% of patients would have received treatment too early and thus had unnecessary exposure. Furthermore, 14.2% of our patients did not require intravitreal treatment or were discharged and would have received treatment unnecessarily.
While pragmatic simple changes during a time of crisis may be preferred and easier to implement, simplified treatment strategies could lead to inferior outcomes, without necessarily decreasing COVID-19–related risk.
We introduced SDOCs prior to the publication of the RCOphth guidelines, and felt that the social distancing and safety measures we had put in place were sufficient to continue safely with our clinics without changing our individualized treatment protocols.
In summary, COVID-19 will likely require ongoing social distancing and other safety measures in outpatient-care provision. We feel we have demonstrated that this is achievable in one-stop wAMD clinics while maintaining patient numbers and patient satisfaction. Our model may not be suitable or achievable in all units, depending on individual circumstances, but we hope that the steps we have outlined in our SDOCs show that safe and high-quality individual care can be provided without sacrificing clinic numbers or patient–doctor interaction in a COVID-19 era.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest for this work.
References
1. WHO Director-General. WHO Director-General’s opening remarks at the media briefing on COVID- 19: 11 March 2020. Available from: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19—11-march-2020.
2. Arshad Ali S, Baloch M, Ahmed N, Arshad Ali A, Iqbal A. The outbreak of Coronavirus disease 2019 (COVID-19)-an emerging global health threat. J Infect Public Health. 2020;13(4):
3. Lazzerini M, Barbi E, Apicella A, Marchetti F, Cardinale F, Trobia G. Delayed access or provision of care in Italy resulting from fear of COVID-19. Lancet Child Adolesc Health. 2020;4(5):
4. Zhou Y, Duan C, Zeng Y, et al. Ocular Findings and Proportion with Conjunctival SARS-COV-2 in COVID-19 patients [published online ahead of print, 2020 Apr 21]. Ophthalmology. 2020. doi:10.1016/j.ophtha.2020.04.028.
5. Khavandi S, Tabibzadeh E, Naderan M, Shoar S. Corona virus disease-19 (COVID-19) presenting as conjunctivitis: atypically high-risk during a pandemic [published online ahead of print, 2020 Apr 27]. Cont Lens Anterior Eye. 2020;43(3):SS1367. doi:10.1016/j.clae.2020.04.010
6. Hamroush A, Qureshi M, Shah S. Increased risk of ocular injury seen during lockdown due to COVID-19 [published online ahead of print, 2020 Apr 27]. Cont Lens Anterior Eye. 2020;43(3). doi:10.1016/j.clae.2020.04.007
7. Lim LW, Yip LW, Tay HW, et al. Sustainable practice of ophthalmology during COVID-19: challenges and solutions [published online ahead of print, 2020 Apr 21]. Graefes Arch Clin Exp Ophthalmol. 2020;258:
8. WHO. Strengthening the health system response to COVID-19 recommendations for the WHO European Region Policy brief (1 April 2020). Available from: http://www.euro.who.int/en/health-topics/Health-systems/pages/strengthening-the-health-system-response-to-covid-19/strengthening-the-health-system-response-to-covid-19-policy-brief.
9. Qiao C, Zhang H, He M, et al. Symptomatic COVID-19 in Eye Professionals in Wuhan, China [published online ahead of print, 2020 Apr 18]. Ophthalmology. 2020;127(9):SS0161–SS0166. doi:10.1016/j.ophtha.2020.04.026
10. Jørstad ØK, Moe MC, Eriksen K, Petrovski G, Bragadóttir R. Coronavirus disease 2019 (COVID-19) outbreak at the department of ophthalmology, Oslo University Hospital, Norway. Acta Ophthalmol. 2020;98(3):
11. RANZCO: 28/04/2020 RANZCO NZ Branch guidance: change to COVID-19 level 3. Available from: https://ranzco.edu/wp-content/uploads/2020/04/RANZCO-Level-3-NZ-Guidelines-22-April-2020.GS_.pdf.
12. AAO: 18/03/2020 Recommendations for urgent and nonurgent patient care. Available from: https://www.aao.org/headline/new-recommendations-urgent-nonurgent-patient-care.
13. ASRS: 14/04/2020 COVID-19: updates and Resources. Available from: https://www.asrs.org/practice/asrs-member-alert-regarding-covid-19-pandemic.
14. RCOphth: management of ophthalmology services during the Covid pandemic. Available from: https://www.rcophth.ac.uk/wp-content/uploads/2020/03/RCOphth-Management-of-Ophthalmology-Services-during-the-Covid-pandemic-280320.pdf.
15. Williams AM, Kalra G, Commiskey PW, et al. Ophthalmology practice during the Coronavirus disease 2019 pandemic: the University of Pittsburgh experience in promoting clinic safety and embracing video visits [published online ahead of print, 2020 May 6]. Ophthalmol Ther. 2020. doi:10.1007/s40123-020-00255-9
16. Saleem SM, Pasquale LR, Sidoti PA, Tsai JC. Virtual ophthalmology: telemedicine in a Covid-19 Era [published online ahead of print, 2020 Apr 30]. Am J Ophthalmol. 2020;216:237–242. doi:10.1016/j.ajo.2020.04.029
17. RCOphth: 30/03/2020 medical retinal management plans during COVID-19. Available from: https://www.rcophth.ac.uk/wp-content/uploads/2020/03/Medical-Retinal-Management-Plan-during-COVID-19-UPDATED-300320-1-3.pdf.
18. Gupta S, Jangra RS, Gujrathi AV, et al. A novel clinical set up for examining healthy dermatology outpatients in time of Covid-19 [published online ahead of print, 2020 Apr 18]. Clin Exp Dermatol. 2020. doi:10.1111/ced.14246
19. Amoaku W, Balaskas K, Cudrnak T, et al. Initiation and maintenance of a Treat-and-Extend regimen for ranibizumab therapy in wet age-related macular degeneration: recommendations from the UK Retinal Outcomes Group. Clin Ophthalmol. 2018;12:
20. Deutsche Ophthalmologische Gesellschaft. Coronavirus Covid 19. Available from: https://www.dog.org/?cat=288.
21. Public Health England. Recommended PPE for primary, outpatient, community and social care by setting, NHS and independent sector 19. Available from: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/878750/T2_poster_Recommended_PPE_for_primary__outpatient__community_and_social_care_by_setting.pdf.
22. RCOphth PPE and staff protection requirements for ophthalmology. Available from: https://www.rcophth.ac.uk/wp-content/uploads/2020/04/UPDATED-RCOphth-PPE-for-ophthalmology-090420.pdf.
23. European Centre for Disease Prevention and Control. Considerations relating to social distancing measures in response to COVID-19 – second update. Available from: https://www.ecdc.europa.eu/sites/default/files/documents/covid-19-social-distancing-measuresg-guide-second-update.pdf.
24. European Centre for Disease Prevention and Control. Infection prevention and control for COVID-19 in healthcare settings - first update. Available from: https://www.ecdc.europa.eu/sites/default/files/documents/COVID-19-infection-prevention-and-control-healthcare-settings-march-2020.pdf.
25. Liu YA, Hsu YC, Lin MH, et al. Hospital visiting policies in the time of COVID-19: a nationwide website survey in Taiwan [published online ahead of print, 2020 Apr 21]. J Chin Med Assoc. 2020;83:566–570. doi:10.1097/JCMA.0000000000000326
26. Wykoff CC, Ou WC, Croft DE, et al. Neovascular age-related macular degeneration management in the third year: final results from the TREX-AMD randomised trial. Br J Ophthalmol. 2018;102(4):
27. Yang Y, Downey L, Mehta H, et al. Resource use and real-world outcomes for ranibizumab treat and extend for neovascular age-related macular degeneration in the UK: interim results from TERRA. Ophthalmol Ther. 2017;6(1):
28. Hufendiek K, Pielen A, Framme C. Injektionsstrategien bei der anwendung intravitrealer VEGF-inhibitoren: pro re nata versus treat and extend“ [strategies of intravitreal injections with anti-VEGF: “pro re nata versus treat and extend”]. Klin Monbl Augenheilkd. 2018;235(8):
29. Rayat JS, Grewal PS, Whelan J, Tennant MT, Choudhry N. Canadian preference and trends survey results for anti-VEGF treatment of macular edema. Can J Ophthalmol. 2016;51(3):
30. Ghosh W, Wickstead R, Claxton L, et al. The cost-effectiveness of ranibizumab treat and extend regimen versus aflibercept in the UK. Adv Ther. 2016;33(9):
31. NICE Guideline. Age related macular degeneration. Available from: https://www.nice.org.uk/guidance/ng82/chapter/Recommendations#diagnosis-and-referral.
32. Kang S, Thomas PBM, Sim DA, Parker RT, Daniel C, Uddin JM. Oculoplastic video-based telemedicine consultations: Covid-19 and beyond [published online ahead of print, 2020 May 12]. Eye (Lond). 2020;34:1193–1195. doi:10.1038/s41433-020-0953-6
33. Jayaram H, Strouthidis NG, Gazzard G. The COVID-19 pandemic will redefine the future delivery of glaucoma care. Eye (Lond). 2020;34:1203–1205. doi:10.1038/s41433-020-0958-1
34. Greaney ML, Sprunck-Harrild K, Ruddy KJ, et al. Study protocol for Young & Strong: a cluster randomized design to increase attention to unique issues faced by young women with newly diagnosed breast cancer. BMC Public Health. 2015;15:37. doi:10.1186/s12889-015-1346-9
35. Boyle J, Vukicevic M, Koklanis K, Itsiopoulos C, Rees G. Experiences of patients undergoing repeated intravitreal anti-vascular endothelial growth factor injections for neovascular age-related macular degeneration. Psychol Health Med. 2018;23(2):
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.