Back to Journals » Lung Cancer: Targets and Therapy » Volume 17
Response to Selpercatinib in a CCDC6-RET Lung Adenocarcinoma with an Acquired Novel RET p.L730_G731insL After Progression on Pralsetinib: A Case Report
Authors Tian C, Zou Y, Liu J, Zhao J, Tian S, Liu Y, Wang G
Received 28 February 2026
Accepted for publication 30 April 2026
Published 20 May 2026 Volume 2026:17 605845
DOI https://doi.org/10.2147/LCTT.S605845
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sai-Hong Ou
Chunyu Tian,1,* Yang Zou,1,* Jinxin Liu,1,* Jing Zhao,2 Simiao Tian,3 Ying Liu,1,4 Gang Wang1
1Department of Oncology III, Affiliated Zhongshan Hospital of Dalian Medical University, Dalian, Liaoning Province, People’s Republic of China; 2Department of Pharmacy, Affiliated Zhongshan Hospital of Dalian Medical University, Dalian, Liaoning Province, People’s Republic of China; 3Department of Medical Records and Statistics, Affiliated Zhongshan Hospital of Dalian Medical University, Dalian, Liaoning Province, People’s Republic of China; 4The Key Laboratory of Biomarker High Throughput Screening and Target Translation of Breast and Gastrointestinal Tumor, Liaoning, Liaoning Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ying Liu, Email [email protected] Gang Wang, Email [email protected]
Abstract: RET fusion is one of the key driver oncogenes in lung cancer. Selective RET inhibitors have become the standard of care for these patients. However, acquired resistance remains inevitable Among the mechanisms of on-target resistance, solvent front mutations in the RET kinase domain are the most common. In contrast, kinase domain insertion mutations are rarely reported as a mechanism of resistance. This article reports a case of a patient with advanced lung adenocarcinoma. Initial genetic testing at diagnosis revealed a CCDC6-RET fusion. The patient achieved partial response after treatment with pralsetinib, but subsequently developed disease progression. After resistance developed, next-generation sequencing (NGS) was performed. The results showed that the original RET fusion persisted. Additionally, a newly acquired insertion mutation (p.L730_G731insL) was detected in the RET kinase domain. Based on this resistance mechanism, the patient discontinued pralsetinib. Treatment was switched to another selective RET inhibitor, selpercatinib. Follow-up imaging evaluation showed that the pulmonary lesions achieved a partial response (PR).This suggests that selpercatinib has therapeutic activity against the tumor carrying this RET insertion mutation. However, the patient received concurrent brain radiotherapy and radiofrequency ablation of liver lesions; therefore, the response in intracranial and hepatic sites cannot be solely attributed to selpercatinib. The observation is hypothesis-generating rather than proof of sensitivity. This case provides a reference for precision treatment strategies after resistance to RET inhibitors.
Keywords: RET intergenic fusion, lung adenocarcinoma, selpercatinib, novel intergenic, insertion mutation
Introduction
Receptor-tyrosine kinase gene (RET) fusion occurs in 1.4% of non-small cell lung cancer (NSCLC) and 1.7% of lung adenocarcinoma in China.1 In recent years, the introduction of selective RET inhibitors, represented by pralsetinib and selpercatinib, has significantly improved the prognosis of patients with advanced RET fusion-positive NSCLC.2 These agents have become the first-line standard of care recommended by clinical guidelines (NCCN and CSCO guidelines) for this patient population.Although initial treatment usually achieves favorable objective response rates and durable disease control, acquired resistance remains inevitable It has become a major challenge limiting long-term survival in these patients.Currently, solvent front mutations are known to be the most common acquired resistance mechanism to second-generation inhibitors.3 They prevent drug binding through steric hindrance, such as G810C/S/R and others.4 However, the response of selpercatinib to novel RET insertion mutations remains unknown. Here, we report a patient with lung adenocarcinoma who harbored a novel RET insertion mutation (p.L730_G731insL) and showed response to selpercatinib.
Case Representation
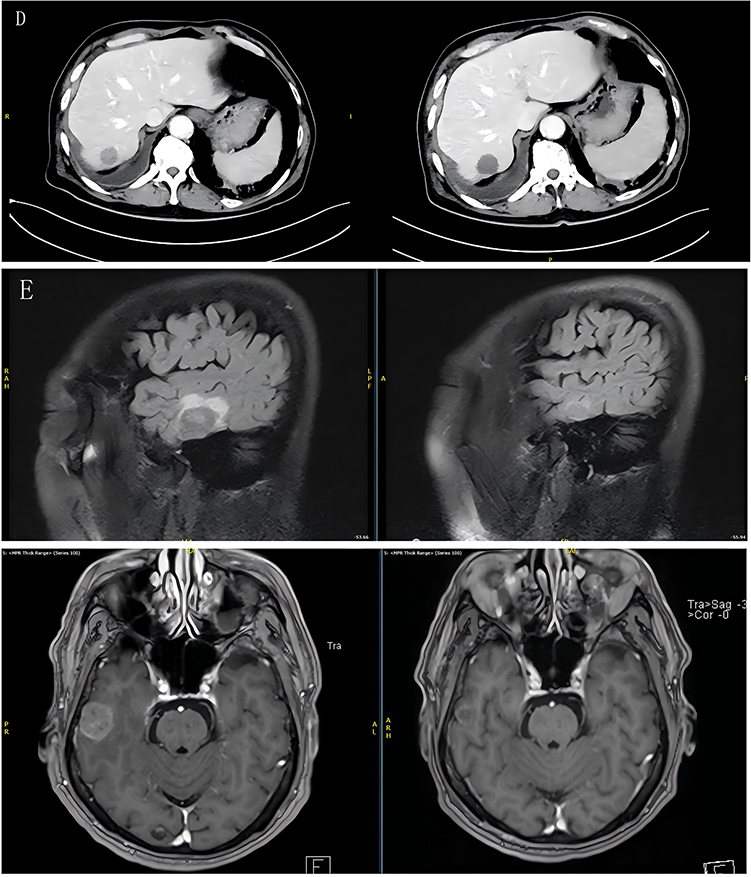
A 66-year-old male with a long-term smoking history presented with progressively worsening symptoms, including right-sided chest pain, cough, and sputum production. Imaging revealed a 2.7 cm × 2.2 cm mass in the right middle lobe. He underwent video-assisted thoracic surgery (VATS) at another hospital, with right middle lobectomy and lymph node sampling. Postoperative histopathological examination confirmed lung adenocarcinoma. The pathological stage was pT2aN2M0, stage IIIA. In December 2018, genetic testing was performed on the surgical tissue using high-throughput next-generation sequencing (NGS:Geneseeq’s Chudekang® Lung 14-gene mutation detection kit). The results detected a CCDC6-RET gene fusion (CCDC6:exon1~RET:exon12, 6.1%). Postoperatively, the patient received adjuvant chemotherapy with pemetrexed plus cisplatin for 6 cycles, followed by maintenance therapy with pemetrexed alone for 4 cycles. During the treatment period, the disease remained stableIn December 2020, follow-up imaging revealed multiple liver metastases. A second NGS (Geneseeq’s Quanjing® Cancer Gene Detection Panel) test was performed on a blood sample, but no clear mutations were detected. Thereafter, the patient received multiple lines of treatment, including another attempt at chemotherapy with pemetrexed plus cisplatin, local radiotherapy to the lung lesions, and treatment with anlotinib. During follow-up, pleural effusion and bone metastases developed (some diagnostic and treatment records from other hospitals were missing).In July 2022, a third NGS (Geneseeq’s Baimaikang® Lung Cancer Gene Panel) test was performed on a blood sample. The results again detected the CCDC6-RET fusion (0.9%), confirming that this driver gene persisted. In March 2023, the patient was transferred to our hospital for further treatment.At that time, both domestic and international clinical guidelines recommended highly selective RET inhibitors as the first-line treatment for advanced non-small cell lung cancer with RET fusion positivity. After evaluation, treatment with pralsetinib was initiated in March 2023.Pralsetinib was administered orally at the standard dose of 400 mg once daily. The patient tolerated the treatment well, and no dose reduction or interruption was required. No grade ≥3 adverse events were observed during pralsetinib therapy. In October 2024, follow-up contrast-enhanced abdominal CT showed enlargement of the liver metastases compared to previous imaging, as well as new metastatic lesions in both lungs and the pleura. Cranial MRI suggested possible intracranial metastases. Based on the comprehensive imaging findings, the patient was determined to have developed acquired resistance to pralsetinib.To clarify the mechanism of resistance, in October 2024, the patient underwent a needle biopsy of a liver metastasis. A fourth NGS (Geneseeq’s Baimaikang® Lung Cancer Gene Panel)test was performed concurrently (during the biopsy, radiofrequency ablation was also performed on some of the liver metastases for local treatment). The test results showed that the original CCDC6-RET fusion (35.17%) persisted, while a newly acquired insertion mutation in the RET kinase domain, p.L730_G731insL (exon12, 24.17%), was detected. Comparison of pre-treatment (July 2022, blood) and post-resistance (October 2024, liver) NGS showed that the only newly emerged alteration was the RET p.L730_G731insL (24.17%), while the original CCDC6-RET fusion persisted (0.9% → 35.17%). No other RET resistance mutations or bypass pathway alterations (MET, KRAS, EGFR, BRAF, PIK3CA) were detected in either sample, confirming that p.L730_G731insL is the sole acquired resistance mechanism. A literature review revealed that this mutation has not been previously reported in populations with resistance to RET inhibitors. Based on the above test results, combined with the 2024 Chinese Society of Clinical Oncology (CSCO) Guidelines for the Diagnosis and Treatment of Non-Small Cell Lung Cancer and relevant evidence-based medicine, a multidisciplinary team (MDT) discussion was conducted. After full communication with the patient and his family, treatment was switched to another highly selective RET inhibitor, selpercatinib,at a dose of 160 mg twice daily orally (160 mg bid po), in November 2024. Concurrently, stereotactic radiotherapy was administered to the intracranial lesions. Given the patient’s history of rapid disease progression on prior therapies and the need for early efficacy assessment to guide subsequent treatment, the first on-treatment imaging was performed at 1 month after selpercatinib initiation. One month after starting selpercatinib, Follow-up imaging evaluation showed that the pulmonary lesions achieved a partial response (PR) (Figure 1).At 3 months after selpercatinib initiation, follow-up CT of the chest confirmed that the pulmonary lesions maintained a partial response (PR).Concurrently, serum CEA levels decreased from 163.82 ng/mL before selpercatinib to 38.72 ng/mL at the 3-month follow-up, consistent with the partial response observed on imaging.The patient’s clinical symptoms also improved, suggesting that selpercatinib has good inhibitory activity against the tumor carrying the p.L730_G731insL insertion mutation. No severe drug-related adverse events occurred during treatment, and the patient tolerated the therapy well. Figure 1 (A) Chest CT before selpercatinib: pulmonary lesions (arrows). (B) Chest CT at 1 month after selpercatinib: partial response. (C) Chest CT at 3 months: maintained PR. (D) Liver lesions before and after radiofrequency ablation. (E) Brain MRI before and after stereotactic radiotherapy. Figure 1 Continued.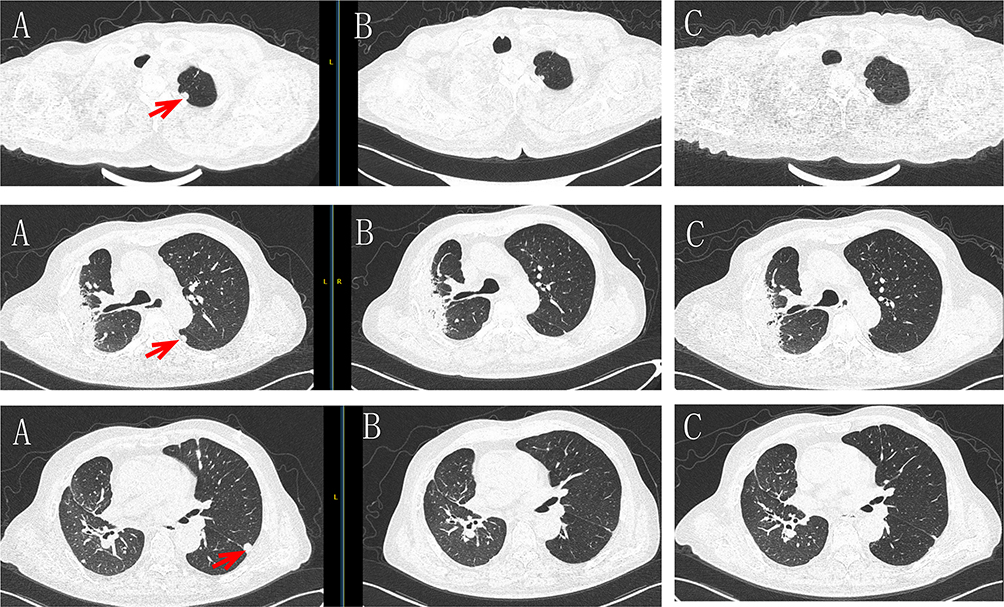
The patient’s complete treatment course, including key clinical events, genetic testing results, treatment decisions, and corresponding efficacy assessments, is visually presented in a timeline format in (Figure 2).
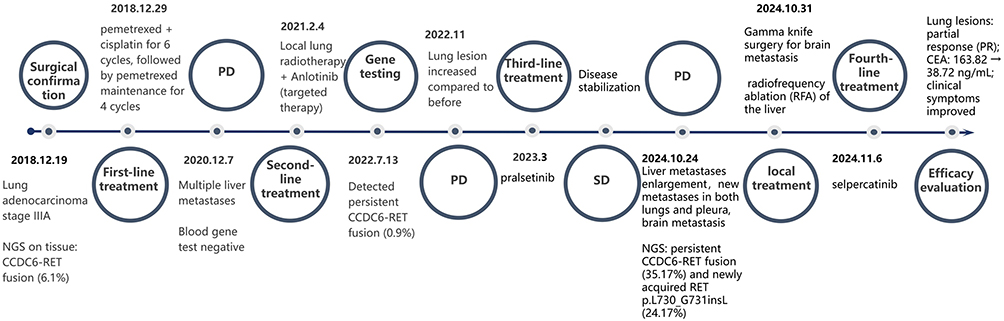 |
Figure 2 Treatment flow chart. The timeline shows key clinical events, NGS results, treatment decisions, and efficacy assessments from diagnosis to 3-month follow-up after switching to selpercatinib. |
Discussion
Although selpercatinib and pralsetinib have shown high response rates and more durable responses in RET-altered cancers,4–7 several recent studies have identified acquired resistance mutations. These mutations are located at the bottom of the RET ATP-binding site (G810C/S/R), the hinge region (Y806C/N), and the β2 strand (V738A).4 In addition, bypass mechanisms have also been reported.8 Among these mutations, G810C/S/R mutations show the strongest resistance.9 This case is the first to report a novel acquired in-frame insertion mutation in the RET kinase domain, p.L730_G731insL. This mutation inserts an additional leucine residue between L730 and G731. We speculate that this may lead to local outward protrusion of the main chain, further increasing spatial occupation in this region.Due to the cyclohexane ring of pralsetinib being closer to residue 730 and having greater structural rigidity, it may cause severe steric clash with the inserted leucine side chain. This could significantly weaken drug binding.In contrast, selpercatinib has a smaller volume and greater spatial allowance in this region. Its flexible chain may avoid the inserted side chain through conformational adjustment. It may even form new interactions with the added hydrophobic residue, thereby maintaining binding capacity.Therefore, we speculate that selpercatinib may maintain inhibitory activity against the L730-G731insL mutation, whereas pralsetinib may develop resistance to this mutation.This finding shares similarity with the previously reported L730V/I (amino acid substitution) mutations.10 The latter have been shown to confer high-level resistance to pralsetinib. Together, these findings suggest that residue 730 plays a critical role in drug binding.However, when evaluating the efficacy of selpercatinib, careful analysis of therapeutic responses across different lesions is required.In this case, the patient received radiotherapy for brain metastases at the time of switching to selpercatinib. Additionally, radiofrequency ablation was performed concurrently with the biopsy of liver metastases after resistance had developed.Therefore, the control of intracranial lesions may be primarily attributed to radiotherapy. Similarly, the local treatment effect of radiofrequency ablation cannot be ruled out as a contributing factor to the changes observed in the liver lesions.However, it is worth noting that the lung lesions showed significant shrinkage after selpercatinib treatment, and this area did not receive any local intervention.This observation provides relatively independent clinical evidence that selpercatinib has inhibitory activity against tumors harboring the p.L730_G731insL mutation.This limitation suggests that future studies with more controlled clinical designs, such as sequentially administered treatment or monotherapy regimens, are needed to further validate the inhibitory activity of selpercatinib against tumors with this type of mutation.
Conclusion
In this case, a potential novel acquired insertion mutation—RET p.L730_G731insL—was detected in a patient with CCDC6-RET fusion-positive lung adenocarcinoma. The patient had developed resistance after treatment with pralsetinib.This finding supports the continued implementation of molecular monitoring during targeted therapy to identify emerging resistance mechanisms.After the detection of this mutation, the treatment strategy was switched to selpercatinib. The patient achieved partial response (PR) in the lung lesions.This observation suggests that, in select cases, selpercatinib may retain therapeutic activity against tumors harboring this mutation.However, as the patient concurrently received cranial radiotherapy and radiofrequency ablation of liver lesions, the results of this study cannot establish a causal relationship. Nor are they sufficient to define a standard treatment regimen.Future prospective studies are needed to further clarify the sensitivity of this mutation to selpercatinib. Such studies will provide evidence to support clinical decision-making in the context of acquired resistance to RET inhibitors.
Data Sharing Statement
Any data and additional information required to reanalyze the data reported in this paper can be made available upon request from the lead contact.
Ethics Approval and Consent to Participate
The research followed the principles outlined in the Declaration of Helsinki. In accordance with the journal’s policy (Consent to publish is a journal requirement and cannot be exempted by an ethics committee), institutional approval was not required for the publication of this single case report. The patient provided written informed consent for the publication of this case report and any related images. The name of the institution is the Affiliated Zhongshan Hospital of Dalian Medical University.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by grants awarded to Gang Wang from the Horizontal Project of China Aging Development Foundation (LJH-XY-20250194-16), and to Ying Liu from the Beijing Science and Technology Innovation Medical Development Foundation (KC2023-JX-0288-FQ17) and the Liaoning Provincial Joint Science and Technology Program (Natural Science Foundation General Project, No.2024-MSLH-006).
Disclosure
Dr Gang Wang reports grants, personal fees, non-financial support from Affiliated Zhongshan Hospital of Dalian Medical University, during the conduct of the study. The authors declare that they have no other known competing financial interests or persona relationships that could have appeared to influence the work reported in this paper.
References
1. Wang SS, Wang F, Zeng Z, et al. Case report: a novel intergenic MIR4299/MIR8070-RET fusion with RET amplification and clinical response to pralsetinib in a lung adenocarcinoma patient. Front Oncol. 2022;12:929763. doi:10.3389/fonc.2022.929763
2. Hu X, Khatri U, Shen T, Wu J. Progress and challenges in RET-targeted cancer therapy. Front Med. 2023;17(2):207–6. doi:10.1007/s11684-023-0985-y
3. Lin JJ, Liu SV, McCoach CE, et al. Mechanisms of resistance to selective RET tyrosine kinase inhibitors in RET fusion-positive non-small-cell lung cancer. Ann Oncol. 2020;31(12):1725–1733. doi:10.1016/j.annonc.2020.09.015
4. Solomon BJ, Tan L, Lin JJ, et al. RET solvent front mutations mediate acquired resistance to selective RET inhibition in RET-driven malignancies. J Thorac Oncol. 2020;15(4):541–549. doi:10.1016/j.jtho.2020.01.006
5. Drilon A, Oxnard GR, Tan DSW, et al. Efficacy of selpercatinib in RET fusion-positive non-small-cell lung cancer. N Engl J Med. 2020;383(9):813–824. doi:10.1056/NEJMoa2005653
6. Subbiah V, Gainor JF, Rahal R, et al. Precision targeted therapy with BLU-667 for RET-driven cancers. Cancer Discov. 2018;8(7):836–849. doi:10.1158/2159-8290.Cd-18-0338
7. Wirth LJ, Sherman E, Robinson B, et al. Efficacy of selpercatinib in RET-altered thyroid cancers. N Engl J Med. 2020;383(9):825–835. doi:10.1056/NEJMoa2005651
8. Subbiah V, Shen T, Terzyan SS, et al. Structural basis of acquired resistance to selpercatinib and pralsetinib mediated by non-gatekeeper RET mutations. Ann Oncol. 2021;32(2):261–268. doi:10.1016/j.annonc.2020.10.599
9. Subbiah V, Shen T, Tetzlaff M, et al. Patient-driven discovery and post-clinical validation of NTRK3 fusion as an acquired resistance mechanism to selpercatinib in RET fusion-positive lung cancer. Ann Oncol. 2021;32(6):817–819. doi:10.1016/j.annonc.2021.02.010
10. Shen T, Hu X, Liu X, Subbiah V, Mooers BHM, Wu J. The L730V/I RET roof mutations display different activities toward pralsetinib and selpercatinib. NPJ Precis Oncol. 2021;5(1):48. doi:10.1038/s41698-021-00188-x
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
LIBRETTO-431: Confirming the Superiority of Selpercatinib to Chemotherapy and the Lack of Efficacy of Immune Checkpoint Inhibitors in Advanced RET Fusion-Positive (RET+) NSCLC, Another Unique Never-Smoker Predominant Molecular Subtype of NSCLC
Lee ATM, Ou SI
Lung Cancer: Targets and Therapy 2024, 15:75-80
Published Date: 23 May 2024