")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
Response of Psoriasis with Systemic Lupus Erythematosus to Secukinumab: A Case Report and Review of the Literature
Authors Dai B, Bai Y, Yu H, Huang Q, Wang L
Received 19 September 2023
Accepted for publication 7 December 2023
Published 15 December 2023 Volume 2023:16 Pages 3589—3594
DOI https://doi.org/10.2147/CCID.S440977
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Rungsima Wanitphakdeedecha
Bowen Dai,1,2 Yanping Bai,2 HongDa Yu,1,2 Qiuchen Huang,1,2 Lei Wang2
1Graduate School, Beijing University of Chinese Medicine, Beijing, 100029, People’s Republic of China; 2Department of Dermatology and Venerology, China-Japan Friendship Hospital, Beijing, 100029, People’s Republic of China
Correspondence: Lei Wang, Department of Dermatology and Venereology, China-Japan Friendship Hospital, No. 2, Yinghua East Street, Chaoyang District, Beijing, 100029, People’s Republic of China, Email [email protected]
Abstract: Although psoriasis and systemic lupus erythematosus are both immune abnormalities, there are few reports on Ps combined with SLE in China and abroad. We present a case of a 23-year-old female with a 10-year history of psoriasis, who had a relapse with significant joint symptoms and a PASI score of 35.6, along with several positive antibodies, including antinuclear antibodies, elevated CRP and ESR, and was diagnosed with psoriasis and SLE. She has been treated with secukinumab 300 mg subcutaneously, improving her condition. She is currently being followed up. The PubMed, SCOPUS, and ISI Web of Science databases were thoroughly searched for English studies reporting psoriasis with systemic lupus erythematosus and treated using biologics. Three case reports/series were included after the screening. Our case report provides a reference for clinicians using secukinumab to treat psoriasis combined with SLE. However, further research is needed to determine whether it can be widely used or if there are common signaling pathways that can be interfered with the pathogenesis of the diseases.
Keywords: psoriasis, systemic lupus erythematosus, secukinumab
Introduction
Psoriasis is a common, chronic, and relapsing form of erythematous, a scaly skin disease encompassing a wide spectrum of morbidity, which imposes a heavy burden on the lives and psychological well-being of patients.1 Systemic lupus erythematosus is a chronic autoimmune disease of unknown etiology that affects almost all organs and can produce large amounts of antinuclear antibodies.2 Psoriasis combined with Systemic lupus erythematosus is clinically rare. We report a case of 23-year-old female patient with psoriasis and systemic lupus erythematosus. Sikulchizumab is a fully human monoclonal antibody of high affinity that was expressed in a Chinese hamster ovary cell line, which selectively binds IL-17A and neutralizes the biological activity of this cytokine. Several studies have shown that IL-17 expression and secretion in SLE patients and Ps patients tend to be elevated.3,4 This patient improved after receiving secukinumab treatment. The article concludes that this case informs clinicians on the use of secukinumab for the treatment of psoriasis combined with systemic lupus erythematosus, but further research is needed to determine if it can be widely used or if there are common signaling pathways that can intervene in the pathogenesis of the disease.
Case Report
A 23-year-old woman presented in 2020 with a 10-year history of psoriasis. Ten years ago, she developed scattered red papules with itching on her upper extremities and back. She used a folk prescription of Chinese herbal medicine (specific medication unknown) without relief from the lesions. Nine years ago, the lesions spread to her head, and she received a diagnosis of “psoriasis” at an external hospital. There, she was treated orally with Salvia tablets and Chinese patent drugs, and topically with mometasone furoate cream and calcipotriol scalp solution, which relieved her skin lesions. In May 2019, the patient developed interphalangeal joint stiffness after running a marathon, which was heaviest in the morning and improved with activity. Later, she gradually developed swelling and discomfort in her shoulder, knee, and hip joints. In October 2019, her skin lesions worsened, and she received treatment with oral and topical herbal medicine (specific medication unknown) at another hospital. However, the skin lesions did not improve, and laboratory findings showed an erythrocyte sedimentation rate of 70mm/h. In January 2020, her joint symptoms worsened after skiing, leading to limited movement of the knee and hip joints, accompanied by swelling and pain. She experienced slight pain relief with Voltaren and ibuprofen. It was at this point that she sought treatment in our department (Figure 1). The patient had no significant medical history, but there was a family history of psoriasis, with her mother having erythrodermic psoriasis.
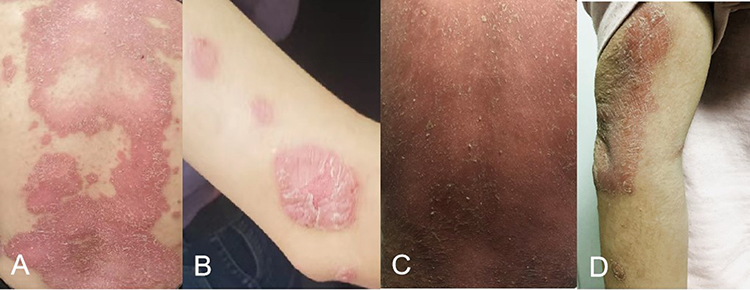 |
Figure 1 Clinical manifestations of the patient’s back and upper extremities 1 month prior to treatment, PASI:25.4 (A and B). Clinical manifestations of the patient’s back and upper limbs in this visit, PASI:35.6 (C and D). |
The physical examination revealed that the patient was fully alert with normal vital signs, thorax, and abdominal examinations. However, in regards to her dermatological conditions, there were dark red hypertrophic plaques fused into patches on the trunk and extremities, covered with a large number of furfuraceous scales, especially on the back (Psoriasis Area and Severity Index (PASI):35.6). If arthralgia, potentially attributed to Psoriatic Arthritis (PsA), were considered as originating from Systemic Lupus Erythematosus (SLE) activity, the SLE Disease Activity Index (SLEDAI) score would be 12. The laboratory findings revealed no significant abnormalities in the routine blood test, liver and kidney function, or tuberculosis screening. However, the urine routine showed a significant elevation in erythrocytes, with a count of 97.4 uL (normal range 0–25). There was also a decrease in complement C3 levels, measured at 41.4 mg/dl (70–128), and complement C4 levels, which were 14.2 mg/dl (16–47). Other abnormal laboratory results included a rheumatoid factor of 138 IU/mL (<20), rapid C-reactive protein of 27.4 mg/L (<=10), and an elevated erythrocyte sedimentation rate of 84 mm/h (0–20). Furthermore, several autoantibodies were detected, including anti-nuclear antibody 1:640 cytoplasmic granular type, positive anti-RNP antibody, positive anti-Sm antibody, anti-dsDNA antibody >200 IU/mL (<20), anti-β2 glycoprotein antibody 25 U/mL (<24), and anti-cardiolipin antibody IgG 18 PL/mL (<10).
Based on the patient’s clinical symptoms, laboratory test results, positive Auspitz sign, and family history, we consider the diagnosis to be psoriasis combined with systemic lupus erythematosus. Unfortunately, we were unable to obtain any pathological data due to the patient’s refusal to undergo hist-path examination. After obtaining informed consent from the patient, treatment began with a weekly subcutaneous injection of 300 mg of secukinumab. After one week of treatment, the patient reported substantial relief from symptoms, such as stiffness and pain in the joints of the hands, reduction of diffuse erythema on the back, the disappearance of skin swelling, and reduction of scaling. After four weeks of treatment, the PASI score was 1.2, with no significant skin lesion present on the back, and the joint symptoms were significantly reduced. After five weeks of treatment, C-reactive protein rapidly returned to the normal range of <2.5 mg/L, blood sedimentation was 67 mm/h (0–20) lower than it was before, and anti-dsDNA antibodies decreased to 87 IU/mL (<20) (Table 1). Essentially, all clinical symptoms improved, and there were no adverse events noted during the subsequent follow-up (Figure 2).
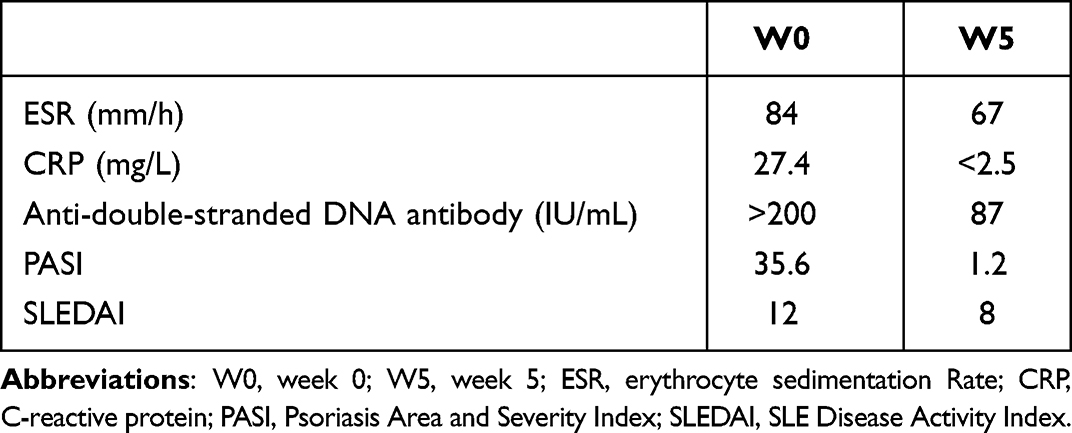 |
Table 1 Comparison of Laboratory Findings Before and After Treatment |
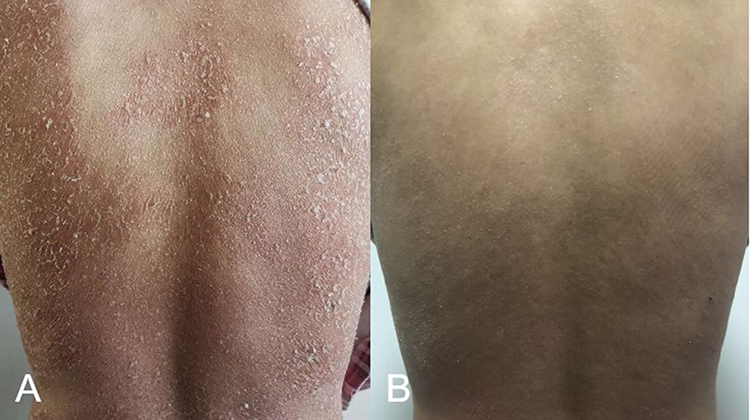 |
Figure 2 Clinical manifestations in the patient’s back after 1 week (A) and 5 weeks of treatment (B). |
Discussion
In this case, the patient’s initial visit was dominated by erythrodermic psoriasis. The calculated PASI score of 35.6 indicated severe psoriasis. The lesions did not improve significantly with previous treatment regimens and gradually worsened. Given the heavy joint symptoms, tests related to the anti-nuclear antibody profile and rheumatoid arthritis antibody profile were also performed. The results revealed that the patient was positive for various anti-nuclear antibodies, including anti-RNP antibodies, anti-Sm antibodies, anti-dsDNA antibodies, anti-β2 glycoprotein antibodies, and anti-cardiolipin antibodies. Additionally, the patient exhibited elevated ESR and CRP levels. Consequentially, the diagnosis of erythrodermic psoriasis combined with SLE was established by integrating clinical signs and ancillary tests.
Ps combined with SLE is clinically rare. Zalla et al5 discovered this coexistence occurred in only 0.69% of patients with psoriasis and 1.1% of patients with LE. Although the causes of Ps and SLE are unknown, they are closely related to genetics, immunity, and infection. Genome-wide association studies have found that SLE and Ps share common genetic susceptibility loci, such as MHC genes, and non-MHC, such as PTPN22, STAT4, and TNIP1.6–12 Two common susceptibility genes, NFKBIA and IL28RA for psoriasis and SLE, were newly identified by national scholars through case-control differential analysis.13 These studies have confirmed the possibility of the co-occurrence of Ps and SLE. Although the combined patients are still a minority, they share common factors that may initiate the pathogenesis. This case provides clinical information for this purpose. During the treatment of SLE, the use of hydroxychloroquine and reduction or discontinuation of glucocorticosteroids can induce or worsen PS. On the other hand, phototherapy used to treat PS may also induce or worsen SLE, making it challenging to decide on a treatment plan when both conditions are present. Therefore, the focus should not only be on addressing the acute condition but also on achieving a balance between the two conditions as much as possible.
Biologic agents are currently an important treatment option for patients with moderate to severe psoriasis,14–18 and the available biologic agents have excellent short- and long-term efficacy. They are well tolerated in the treatment of psoriasis. Recent research suggests that psoriasis and lupus share a common pathogenic mechanism characterized by the overactivation of the Th17 pathway, which results in elevated levels of IL-17, IL-22, and IL-23.19 The most serious distress of this patient at the time of consultation was the skin lesions and joint symptoms. Therefore, the best option for controlling skin lesions and improving joint symptoms is to use secukinumab, which targets IL-17A and has a rapid onset of action, significant long-term efficacy, and high safety.20 We summarised case reports of using biologics to treat psoriasis with SLE (Table 2). Unfortunately, we were unable to obtain the patient’s histopathological samples. In clinical practice, some patients with subacute cutaneous lupus erythematosus may present with a psoriasis-like rash, which requires differentiation from psoriasis combined with lupus by direct immunofluorescence, serological antibodies, and other methods.
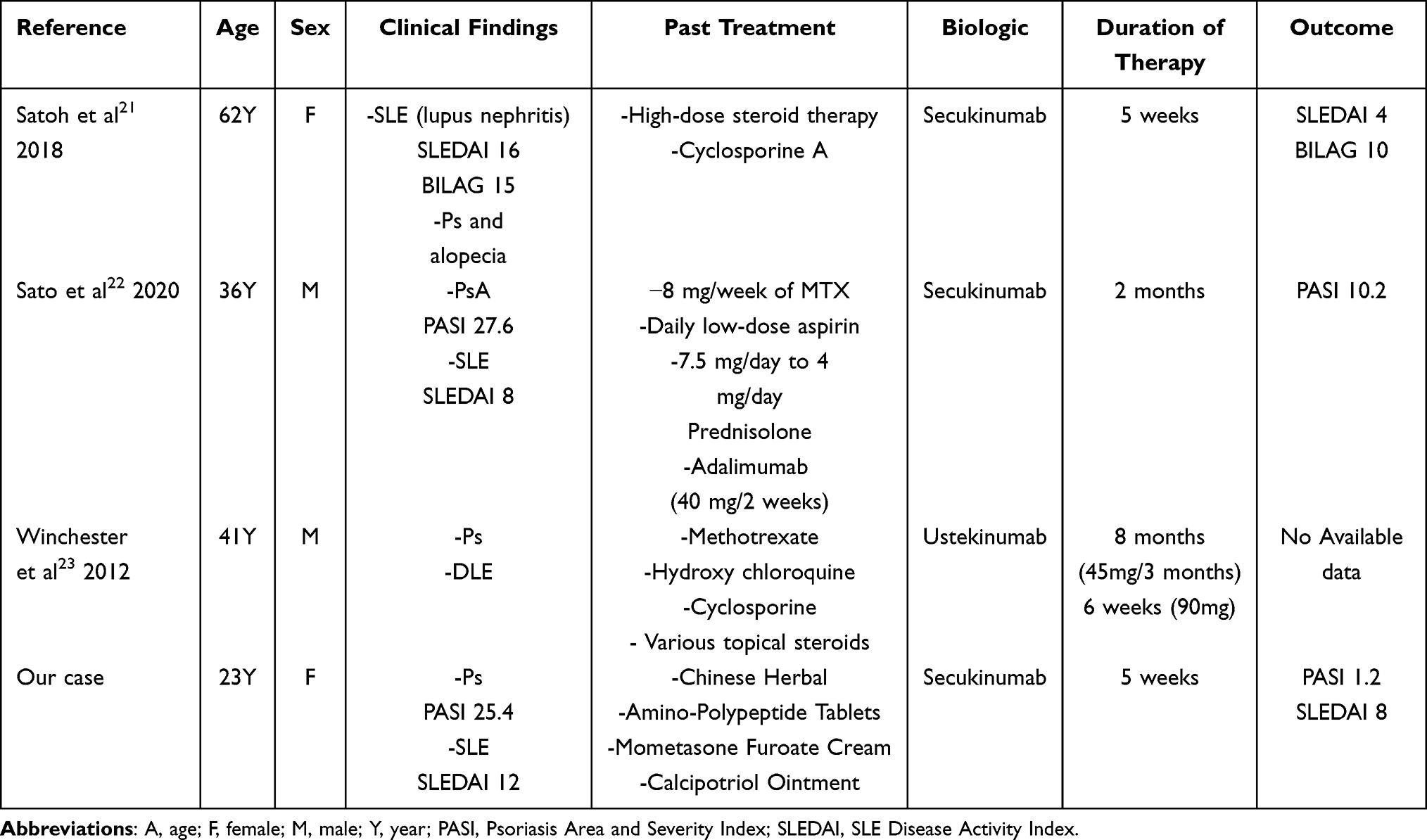 |
Table 2 Psoriasis and Systemic Lupus Erythematosus Treated with Biologics |
Conclusion
Overall, the therapeutic efficacy of secukinumab in psoriasis is beyond doubt, but its efficacy in SLE needs further testing. The present case of Ps combined with SLE was fortunately controlled by secukinumab. However, whether it can be widely used or there are common signalling pathways that can be intervened in the pathogenesis of both diseases needs further investigation.
Ethical Approval
The ethical committee of the hospital gave the agreement to report this case.
Consent Statement
A formal written informed consent has been provided by the patient to have the case details and any accompanying images published.
Acknowledgments
We would like to express our gratitude to the patient and the hospital for providing permission to publish the case details.
Funding
This study was supported financially by the China’s national high-level hospital clinical research funding (2022-NHLHCRF-LX-02-0122).
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Griffiths CEM, Armstrong AW, Gudjonsson JE, Barker JNWN. Psoriasis. Lancet. 2021;397(10281):1301–1315. doi:10.1016/S0140-6736(20)32549-6
2. Lau CS, Yin G, Mok MY. Ethnic and geographical differences in systemic lupus erythematosus: an overview. Lupus. 2006;15(11):715–719. doi:10.1177/0961203306072311
3. Yang Y, Yan C, Yu L, et al. The star target in SLE: IL-17. Inflamm Res. 2023;72(2):313–328. doi:10.1007/s00011-022-01674-z
4. Ghoreschi K, Balato A, Enerbäck C, Sabat R. Therapeutics targeting the IL-23 and IL-17 pathway in psoriasis. Lancet. 2021;397(10275):754–766. doi:10.1016/S0140-6736(21)00184-7
5. Zalla MJ, Muller SA. The coexistence of psoriasis with lupus erythematosus and other photosensitive disorders. Acta Derm Venereol Suppl (Stockh). 1996;195:1–15. doi:10.2340/00015555195115
6. Li Y, Liao W, Chang M, et al. Further genetic evidence for three psoriasis-risk genes: ADAM33, CDKAL1, and PTPN22. J Invest Dermatol. 2009;129(3):629–634. doi:10.1038/jid.2008.297
7. Harley JB, Alarcón-Riquelme ME, et al.; International Consortium for Systemic Lupus Erythematosus Genetics (SLEGEN). Genome-wide association scan in women with systemic lupus erythematosus identifies susceptibility variants in ITGAM, PXK, KIAA1542 and other loci. Nat Genet. 2008;40(2):204–210. doi:10.1038/ng.81
8. Nair RP, Duffin KC, Helms C, et al. Genome-wide scan reveals association of psoriasis with IL-23 and NF-kappaB pathways. Nat Genet. 2009;41(2):199–204. doi:10.1038/ng.311
9. Zhang XJ, Huang W, Yang S, et al. Psoriasis genome-wide association study identifies susceptibility variants within LCE gene cluster at 1q21. Nat Genet. 2009;41(2):205–210. doi:10.1038/ng.310
10. Han JW, Zheng HF, Cui Y, et al. Genome-wide association study in a Chinese Han population identifies nine new susceptibility loci for systemic lupus erythematosus. Nat Genet. 2009;41(11):1234–1237. doi:10.1038/ng.472
11. Remmers EF, Plenge RM, A.t L, et al. STAT4 and the risk of rheumatoid arthritis and systemic lupus erythematosus. N Engl J Med. 2007;357(10):977–986. doi:10.1056/NEJMoa073003
12. Zervou MI, Goulielmos GN, Castro-Giner F, Tosca AD, Krueger-Krasagakis S. STAT4 gene polymorphism is associated with psoriasis in the genetically homogeneous population of Crete, Greece. Hum Immunol. 2009;70(9):738–741. doi:10.1016/j.humimm.2009.05.008
13. Li Y, Cheng H, Zuo XB, et al. Association analyses identifying two common susceptibility loci shared by psoriasis and systemic lupus erythematosus in the Chinese Han population. J Med Genet. 2013;50(12):812–818. doi:10.1136/jmedgenet-2013-101787
14. Kupper TS. Immunologic targets in psoriasis. N Engl J Med. 2003;349(21):1987–1990. doi:10.1056/NEJMp038164
15. Boehncke WH, Prinz J, Gottlieb AB. Biologic therapies for psoriasis. A systematic review. J Rheumatol. 2006;33(7):1447–1451.
16. Sbidian E, Chaimani A, Afach S, et al. Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis. Cochrane Database Syst Rev. 2020;1(1):CD011535. doi:10.1002/14651858.CD011535.pub3
17. Smith CH, Yiu ZZN, Bale T, et al. British Association of Dermatologists guidelines for biologic therapy for psoriasis: a rapid update. Br J Dermatol. 2020;183(4):628–637. doi:10.1111/bjd.19039
18. Callen JP. New psoriasis treatments based upon a deeper understanding of the pathogenesis of psoriasis vulgaris and psoriatic arthritis: a personal appraisal of their use in practice. J Am Acad Dermatol. 2003;49(2):351–356. doi:10.1067/s0190-9622(03)01149-6
19. Yuying Q, Li D, Liu W, et al. Molecular consideration relevant to the mechanism of the comorbidity between psoriasis and systemic lupus erythematosus (Review). Exp Ther Med. 2023;26(4):482. doi:10.3892/etm.2023.12181
20. Langley RG, Sofen H, Dei-Cas I, et al. Secukinumab long-term efficacy and safety in psoriasis through to year 5 of treatment: results of a randomized extension of the Phase III ERASURE and FIXTURE trials. Br J Dermatol. 2023;188(2):198–207. doi:10.1093/bjd/ljac040
21. Satoh Y, Nakano K, Yoshinari H, et al. A case of refractory lupus nephritis complicated by psoriasis vulgaris that was controlled with secukinumab. Lupus. 2018;27(7):1202–1206. doi:10.1177/0961203318762598
22. Sato K, Aizaki Y, Yoshida Y, Mimura T. Treatment of psoriatic arthritis complicated by systemic lupus erythematosus with the IL-17 blocker secukinumab and an analysis of the serum cytokine profile. Mod Rheumatol Case Rep. 2020;4(2):181–185. doi:10.1080/24725625.2020.1717741
23. Winchester D, Duffin KC, Hansen C. Response to ustekinumab in a patient with both severe psoriasis and hypertrophic cutaneous lupus. Lupus. 2012;21(9):1007–1010. doi:10.1177/0961203312441982
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.