Back to Journals » Clinical Interventions in Aging » Volume 20
Respiratory Microbiome in Elderly Patients on Prolonged Mechanical Ventilation: A Prospective Multi-Center Observational Study
Authors Wang Y, Wu J, Wang Y, Jiang W, Wang D, Zhao J, Qin X, Yuan Y, Zhang H, Wang J, Zhen J, Du Y, Mu X, Li L, Wang T, Zou L, Fang X, Sun B, Li H ![]()
Received 21 August 2025
Accepted for publication 13 December 2025
Published 27 December 2025 Volume 2025:20 Pages 2705—2716
DOI https://doi.org/10.2147/CIA.S553377
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Yang Wang,1,* Jionghe Wu,1,2,* Yajuan Wang,1,* Wei Jiang,1 Dan Wang,1 Jing Zhao,1 Xuebing Qin,1 Yaping Yuan,1,2 Hongyun Zhang,1 Jing Wang,3 Jie Zhen,4 Yuguo Du,5 Xiangdong Mu,6 Li Li,6 Ting Wang,7 Lin Zou,1 Xiangqun Fang,1 Baojun Sun,1 Hongxia Li1
1Department of Pulmonary and Critical Care Medicine, the Second Medical Center, National Clinical Research Center for Geriatric Diseases, Chinese PLA General Hospital, Beijing, 100000, People’s Republic of China; 2Chinese PLA Medical School, Beijing, 100000, People’s Republic of China; 3Emergency Department, Xuanwu Hospital, Capital Medical University, Beijing, 100000, People’s Republic of China; 4Intensive Care Unit, Beijing Shijitan Hospital, Capital Medical University, Beijing, 100000, People’s Republic of China; 5Geriatrics Department, the Seventh Medical Center, Chinese PLA General Hospital, Beijing, 100000, People’s Republic of China; 6Department of Pulmonary and Critical Care Medicine, Beijing Tsinghua Changgung Hospital, Beijing, 100000, People’s Republic of China; 7Department of Pulmonary and Critical Care Medicine, Beijing Tiantan Hospital, Capital Medical University, Beijing, 100000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Baojun Sun, Email [email protected] Hongxia Li, Email [email protected]
Purpose: The purpose of this study was to explore dynamic changes of respiratory microbiome in elderly patients undergoing prolonged mechanical ventilation (PMV) by isothermal microfluidic amplification chip technology (IAMC).
Methods: The study enrolled patients in six general hospitals in Beijing. Patients who developed Ventilator-associated pneumonia (VAP) within the observation period were enrolled in the VAP group, while those without VAP were categorized in non-VAP group. The study adopted IAMC technology to dynamically monitor the differences in the detection rates of bacteria, fungi, and viruses in the two groups. The conventional microbiological tests (CMT) were performed to clarify the correlation between KPC and drug resistance phenotype of K. pneumoniae.
Results: Among 218 patients, 78 were diagnosed with VAP. The pulmonary microbiota composition of patients without VAP was relatively stable. Compared with the non-VAP group, the detection rates of Enterococcus faecalis, Epstein–Barr virus, and Herpes simplex virus were significantly increased in the VAP group, whereas those of Haemophilus influenzae and Serratia marcescens were significantly reduced. In the VAP group, the detection rates of Enterococcus faecalis and Epstein–Barr virus were higher after the occurrence of VAP than before. A high correlation was observed between the KPC genotype of K. pneumoniae and its resistance phenotype.
Conclusion: Viruses and Gut microbes might be closely related to the development of VAP in elderly undergoing PMV. The detection of the KPC gene of K. pneumoniae can guide antibiotic selection, and IAMC can aid in quickly identifying pathogens and facilitate targeted treatment.
Clinical Trial Registration Number: ChiCTR2100051343.
Keywords: respiratory microbiome, elderly patients, VAP, PMV
Introduction
Mechanical ventilation is an important modality for saving the lives of critically ill patients, and up to 10%–50% of mechanically ventilated patients require prolonged mechanical ventilation (PMV) (≥21 days).1–3 Elderly patients receiving mechanical ventilation generally experience immune senescence caused by aging, the coexistence of multiple diseases, and the repeated application of broad-spectrum antibiotics 3 months before diagnosis. Consequently, they are prone to chronic respiratory failure, and they often require PMV. The incidence of PMV is highest in patients older than 85 years.4–6
The incidence of ventilator-associated pneumonia (VAP) ranges 5%–60%, and the fatality rate ranges 15%–76%.7–10 PMV carries a higher risk of VAP. Studies have illustrated that microbes in the lower respiratory tract in mechanically ventilated patients are widely involved in the development of VAP, and dynamic microbial changes in the lower respiratory tract are associated with VAP.11–14 However, most studies only focused on the bacterial changes in the lower respiratory tract in patients receiving short-term mechanical ventilation, and they rarely focused on the dynamic changes of bacteria, fungi, and viruses.13,14 Recent research on PMV also emphasized the importance of standardized weaning and rehabilitation management, but limited attention was given to alterations in the lower respiratory microbiota, particularly among elderly patients. According to 2023 CHINET surveillance data in China, Klebsiella pneumoniae was the predominant pathogen isolated from respiratory specimens (17.1%), with a significant drug resistance burden.15
This prospective, multicenter study employed isothermal microfluidic amplification chip (IAMC) technology, which was based on the loop-mediated isothermal amplification (LAMP) technology and microfluidic chip. The objective of the study was to (1) compare pathogen profiles between VAP and non-VAP groups, (2) characterize longitudinal microbial shifts preceding and following VAP diagnosis, and (3) validate the concordance of KPC genotype with carbapenem resistance phenotypes in Klebsiella pneumoniae isolates, contrasting IAMC with conventional microbiological methods.
Methods
Research Design
This prospective, multicenter, observational study enrolled patients who received PMV between September 2021 and October 2023 at six institutions in Beijing, China: The Second Medical Center and the Seventh Medical Center of Chinese People’s Liberation Army General Hospital; Xuanwu Hospital, Capital Medical University; Beijing Shijitan Hospital, Capital Medical University; Beijing Tiantan Hospital, Capital Medical University; and Beijing Tsinghua Changgung Hospital.
The inclusion criteria were as follows: age ≥ 65 years; receipt of invasive mechanical ventilation ≥21 days; absence of pneumonia (confirmed by X-ray or CT); and no use of antibiotics within 72 h prior to enrollment. Enrollment was defined as the first ventilation event within one year of study entry. The exclusion criteria were as follows: terminal stage of disease (survival time < 7 days); presence of tracheal stenosis or malformation or tracheoesophageal fistula; active tumor within 3 months or undergoing chemotherapy; extrapulmonary organ infection after enrollment; or novel coronavirus infection within 3 weeks before or during enrollment. The study followed the guidelines of the Declaration of Helsinki, and the protocol was approved by the Ethics Committee of the Chinese People’s Liberation Army General Hospital. Written informed consent was obtained from all participants or their legal agents (Informed consent was obtained from legal agents because the elderly participants undergoing prolonged mechanical ventilation were often critically ill or cognitively impaired, rendering them unable to provide consent themselves).
Definition and Specimen Retention and Collection
The expert consensus from the US National Association for Medical Direction of Respiratory Care (NAMDRC) defines prolonged mechanical ventilation as requiring continuous mechanical ventilation for ≥21 days, with a daily duration of ≥6 hours.2 The diagnostic criteria for VAP are as follows: 1. Chest X-ray or CT showing new infiltrative shadows, consolidation shadows, or ground glass shadows, excluding diseases such as atelectasis, heart failure (pulmonary edema), and pulmonary embolism; 2. At least two of the following criteria must be met simultaneously: 1) Fever, body temperature >38°C; 2) Purulent airway secretions; 3) The peripheral blood white blood cell count is higher than 10 × 109/L or less than 4 × 109/L.12
The observation period without VAP was 28 days. Lower respiratory tract aspirates were taken at 1–3 and 7–10 days after enrollment, as well as at other times at the discretion of the medical staff. The observation period for VAP lasted until 2 weeks after VAP was diagnosed. Lower respiratory tract aspirates were taken at 1–3 days after the diagnosis of VAP, as well as at other times at the discretion of the medical staff. Tracheal aspirates were collected per clinical guidelines. Specimen quality was assessed using sputum smear microscopy, with acceptability defined as: squamous epithelial cells <10 per low-power field (LPF); leukocytes >25 per LPF; or squamous epithelial cell/leukocyte ratio <1:2.5 under LPF.16,17 Five milliliters of lower respiratory aspirate samples were retained each time. The qualified lower respiratory tract aspiration samples were divided into two parts, with one used for conventional microbiological tests (CMT) (sputum culture, combining drug susceptibility test, et al) and one applied for IAMC technology.16,17
CMT was performed in clinical laboratories of tertiary hospitals, with results independently validated by a certified microbiologist and a senior physician holding the rank of associate chief physician or higher.
The IAMC detection process was conducted by CapitalBio Technology (Beijing, China), encompassing nucleic acid extraction, sample loading, isothermal amplification, data analysis, and result interpretation. Specimens were transported at 4°C and delivered to the laboratory within 72 hours. The workflow of IAMC detection is illustrated in Supplementary Figure S1, and the comprehensive list of detectable pathogens is provided in Supplementary Table S1.
Identification of Pathogens and Their Potential Clinical Impact
The IAMC detection results were combined with the traditional microbial detection results, and then the clinical, imaging, and laboratory findings were used to make an assessment. The specific implementation was first determined by two deputy chief physicians in the research team and then discussed by four chief physicians, including one microbiology expert and one microfluidic chip technical expert, to determine the final result (presence of pathogenic bacteria, bacterial infection, Candida or virus colonization, and mixed infection; need to adjust the antibiotic regimen).
Dynamic Comparison of Results from the IAMC Method in the Non-VAP and VAP Groups
The IAMC method was employed to analyze and compare the differences in pathogens between VAP patients and non-VAP patients; For VAP patients, microbial changes before and after the occurrence of VAP were compared.
Statistical Analysis
Based on the occurrence of VAP during the observation period, patients were divided into the non-VAP and VAP groups. Clinical characteristics including pre-existing pulmonary comorbidities (COPD, bronchiectasis) and immunosuppressive conditions (long-term corticosteroid use >0.5 mg/kg/day, chemotherapy within 6 months) were documented for baseline assessment. To address multiple comparisons, the Benjamini–Hochberg procedure was applied with a false discovery rate (FDR) threshold of <0.05 for all inter-group pathogen comparisons. Missing data were handled through complete-case analysis, with <5% missingness in baseline variables confirmed by Little’s MCAR test. Statistical analysis was performed using IBM SPSS Statistics 23.0 (IBM, Armonk, NY, USA). Normally distributed measurement data were expressed as the mean ± standard deviation, and comparisons between the groups were performed using the independent-samples t-test. Non-normally distributed measurement data were expressed as the median (interquartile range), and comparisons between the groups were performed using the non-parametric Mann–Whitney U-test. Countable data were expressed as percentages, and comparisons were performed using the χ2 test. P < 0.05 indicated statistical significance.
Results
The study included 218 patients. The inclusion process is presented in Figure 1. The demographic data and clinical characteristics of the cohort are presented in Table 1. The median patient age was 94 (91, 98) years, and the median duration of invasive mechanical ventilation was 249.50 (106.75, 747.00) days. The cohort included 212 (97.25%) men and six (2.75%) women. Seventy-eight (35.78%) patients were diagnosed with VAP during the observation period. There were no significant differences in age, sex, the duration of invasive mechanical ventilation, the prevalence of common diseases, and the history of drug use between the groups (all P > 0.05).
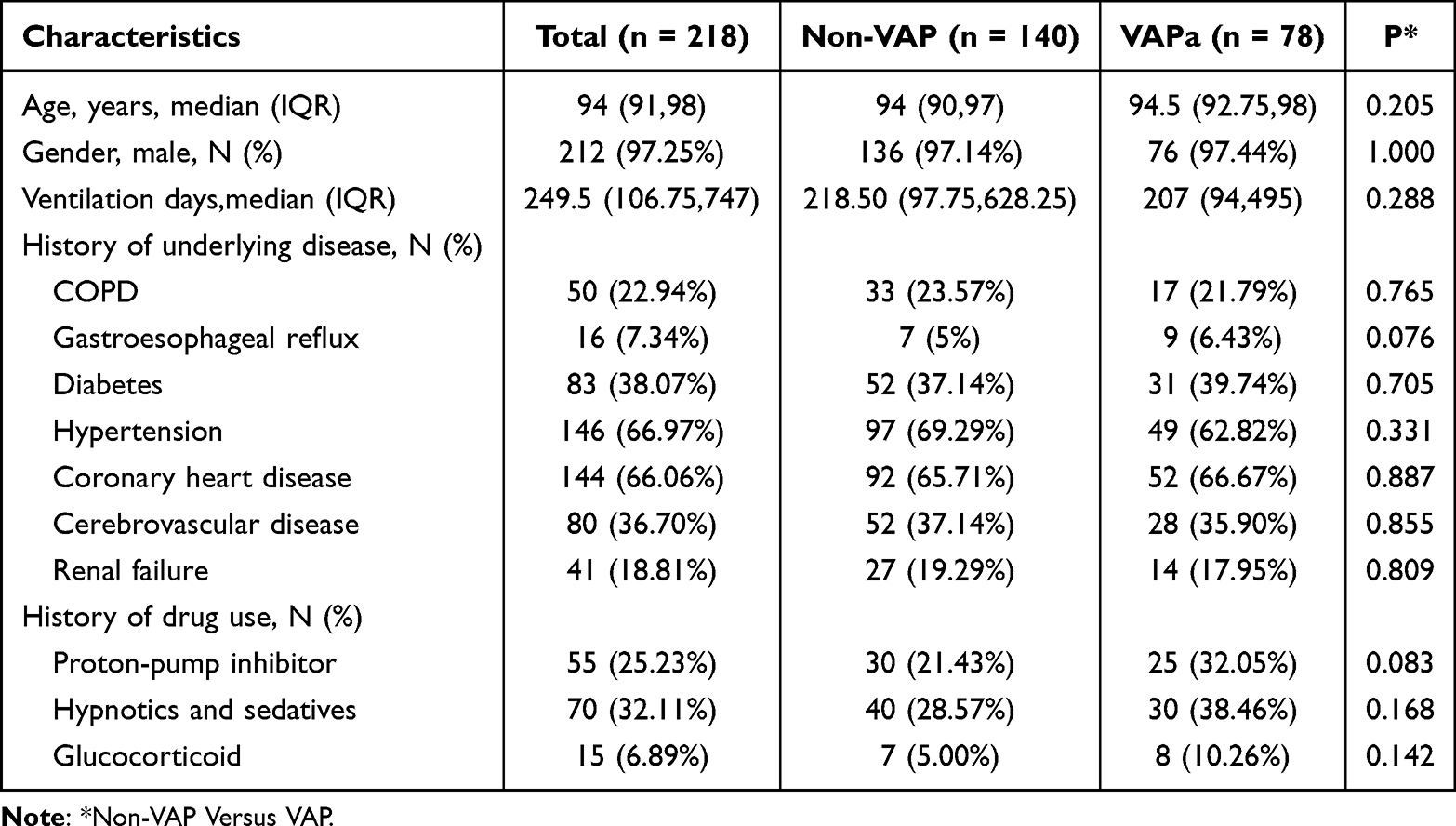 |
Table 1 Clinical Characteristics and Laboratory Findings of 218 Older Adult Patients |
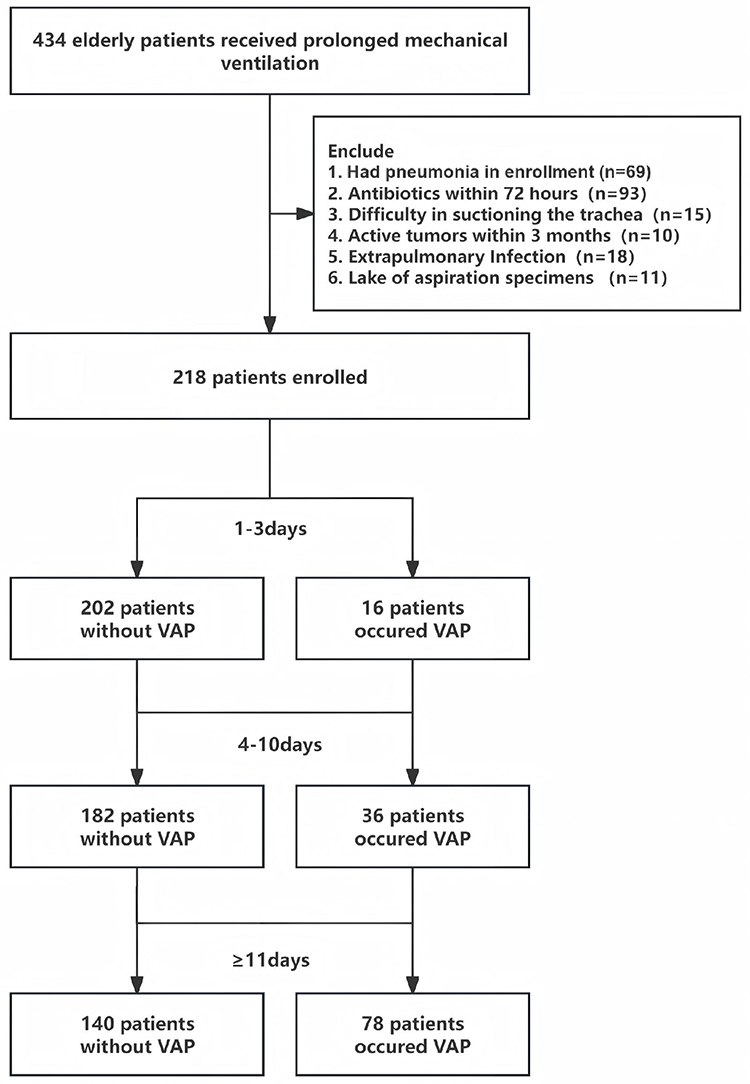 |
Figure 1 Screening of patients receiving prolonged mechanical ventilation the study period. |
Comparison of the Diagnostic Performance of the Test methods
One hundred and thirty-eight lower airway aspirate samples were collected from 78 patients in the VAP group, and 245 samples were obtained from 140 patients in the non-VAP group, as presented in Figure 1. The lower respiratory tract aspirates were tested by CMT and IAMC (Tables 2–3). In total, 314 (81.98%) samples were positive in both tests (18 complete, 59 inconsistent, and 237 partially consistent with at least one pathogen), and 22 (5.74%) were negative in both tests. Thirty-seven (9.66%) samples were positive only in the IAMC test, and 10 (2.61%) samples were positive only in CMT (Supplementary Table S2). The ability of IAMC to detect Klebsiella pneumoniae, Stenotrophomonas maltophilia, Pseudomonas aeruginosa, Enterococcus, Viruses and other pathogens was stronger than CMT (all P < 0.05, Figure 2, Supplementary Table S3).
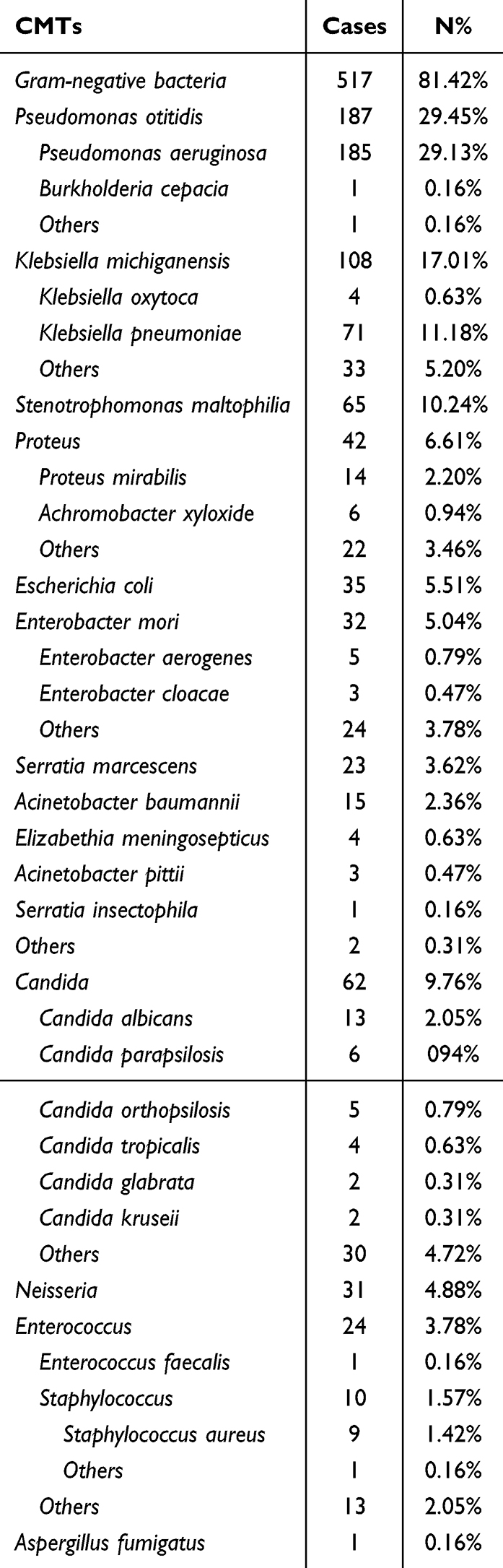 |
Table 2 Results of CMTs of 635 Pathogens in 383 Lower Respiratory Tract Aspirated Samples from 218 Patients |
 |
Table 3 Results of IAMC of 1312 Pathogens in 383 Lower Respiratory Tract Aspirated Samples from 218 Patients |
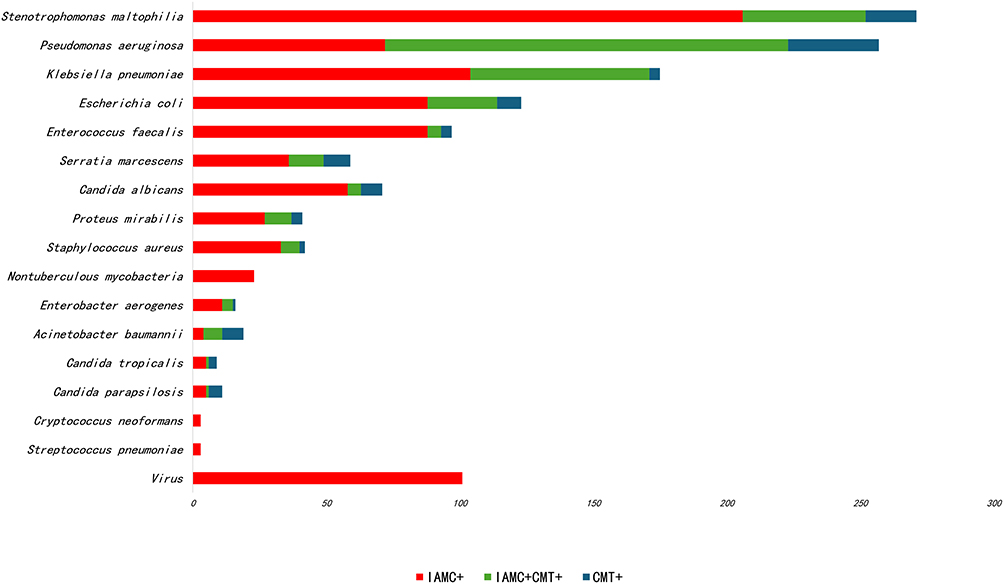 |
Figure 2 Comparison of the ability of CMT and IAMC to detect microorganisms in 383 lower respiratory tract aspirated samples from 218 patients. |
IAMC analysis of lower respiratory tract aspirates from elderly PMV patients revealed a predominance of Gram-negative bacilli, accounting for 67.92% of all detected microorganisms. The top four isolates were Stenotrophomonas maltophilia (19.21%), Pseudomonas aeruginosa (17%), Klebsiella pneumoniae (13.03%), and Escherichia coli (8.69%). Gram-positive cocci constituted 11.36%, viruses 7.42%, fungi 6.58%, and other organisms 6.72% (Table 3).
Effect of Antibiotics on the Detection Method
In the VAP group, the most commonly used antibiotics were β-lactams, prescribed to 51 patients (65.4%), followed by quinolones in 8 patients (10.3%), macrolides in 4 patients (5.1%), and aminoglycosides in 3 patients (3.8%). We collected 58 lower respiratory tract aspirate samples in which the antibiotics were used for more than 3 days. Pathogens were detected by the IAMC and CMT in 53 and 45 samples, respectively (91.4% vs 77.6%, P < 0.001).
Potential Impact of IAMC on Treatment
Analysis of the IAMC results of the first lower airway aspirate samples obtained after 1–3 days in the VAP group signaled a potential change in the antibiotic management strategy in 17 patients (21.79%, Supplementary Table S4).
Dynamic Comparison of Results from the IAMC Method in the Non-VAP and VAP Groups
Stable-phase samples were collected from 74 of 140 patients in the non-VAP group at both 1–3 and 7–10 days. Longitudinal comparison of the results revealed no statistical difference in the proportion of microorganisms detected in the two groups (P > 0.05, Figure 3a). Compared with samples obtained at 1–3 days in the non-VAP group, Enterococcus faecalis, Epstein–Barr virus, and Herpes simplex virus were detected more frequently in the VAP group (all P < 0.05), whereas the detection rates of Haemophilus influenzae and Serratia marcescens were significantly decreased (both P < 0.05, Figure 3b). Meanwhile, stable-phase samples were collected before the occurrence of VAP in 50 patients in the VAP group. Compared with the findings before the occurrence of VAP, the positivity rates of E. faecalis and Epstein–Barr virus at 1–3 days after the occurance of VAP were significantly increased (both P < 0.05), whereas the positivity rates of H. influenzae and S. marcescens were significantly decreased (both P < 0.05, Figure 3c). No significant differences were observed in the detection rate of Klebsiella pneumoniae between the VAP and non-VAP groups, or before and after the onset of VAP (Figure 3).
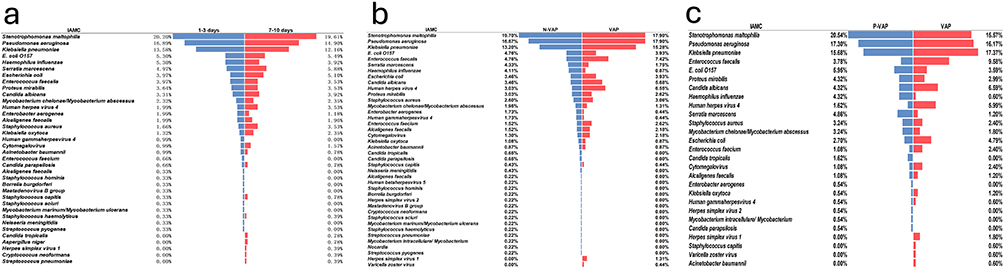 |
Figure 3 (a) IAMC microbial results distribution of 148 lower respiratory aspirate samples from non-VAP group. (b) IAMC microbial results distribution of 140 non-VAP and 78 VAP lower respiratory aspirate samples. (c) IAMC microbial results distribution of 50 pre-VAP and 50 post-VAP lower respiratory aspirate samples. |
Drug Resistance Genotype and Phenotype of K. pneumoniae
In total, 171 K. pneumoniae strains were detected using IAMC technology, among which 98 (57.31%) expressed KPC, OMPK35, or other resistance genes (Figure 4). Seventy-four strains (43.27%) expressed KPC. Using the results of CMT, the sensitivity of the KPC gene for determining carbapenem resistance in K. pneumoniae was 69.09%, and the specificity was 68.97% (Supplementary Table S5). Thirty-eight strains of carbapenem-resistant K. pneumoniae (CRKP) expressing KPC were further typed as KPC-2.
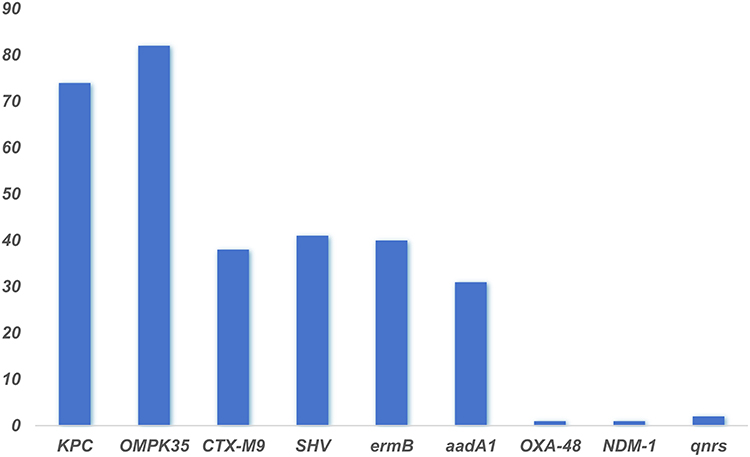 |
Figure 4 Distribution of Klebsiella pneumoniae antibiotic resistance genes detected by IAMC. |
Discussion
This study longitudinally investigated the dynamic changes in the bacterial, fungal, and viral flora in elderly patients undergoing PMV in real-world settings. We found that the lung microbial composition in elderly patients without VAP was relatively stable. Some studies found that the microbial composition of the lower respiratory tract of mechanically ventilated patients changes greatly because of the influence of endotracheal intubation.16,17 These studies usually enrolled patients intubated within 2 weeks, and the damaged airway barrier was not significantly repaired yet. Oropharyngeal microorganisms were extensively inhaled into the lower respiratory tract during endotracheal intubation, leading to sharp changes in its microbial composition. However, the duration of mechanical ventilation duration exceeded 21 days in this study, and the impact of invasive procedures gradually waned.
The study also compared the microbial composition of the lower respiratory tract between the VAP group and the non-VAP group, and found significantly higher detection rates of Enterococcus faecalis, EB virus, and Herpes simplex virus in the VAP group (P < 0.05). The detection rate of common bacteria such as Haemophilus influenzae and Serratia marcescens in community-acquired pneumonia18 was significantly reduced (P < 0.05). Some studies19,20 have also found that the microbiota structure of VAP patients differs significantly compared to non-VAP patients. They suggested that the pathogen spectrum of early-onset VAP (mechanical ventilation less than 5 days) is closer to community-acquired pneumonia, while the pathogen spectrum of late-onset VAP (mechanical ventilation greater than or equal to 5 days) is similar to hospital acquired pneumonia. Yet, the population enrolled in this study is clearly late-onset VAP. The higher detection rates of Epstein–Barr virus and Herpes simplex virus in the VAP group suggested a potential link between viral infections and the development of VAP. Viral reactivation was a well-documented phenomenon in critically ill patients. Particular attention has been paid to the frequent detection of non-respiratory viruses in individuals under invasive mechanical ventilation. Meta-analysis showed that antiviral therapy might result in lower hospital and 30-day all-cause mortality in mechanically ventilated ICU patients.21,22 A study of critically ventilated patients found that 21% of patients with worsening respiratory conditions during mechanical ventilation had evidence of Herpes simplex virus pneumonia on histopathological examination.23 Shorr et al found that the most common viral infections in mechanically ventilated patients are rhinovirus, influenza A virus, and Epstein–Barr virus.24 In our study, the positivity rate of E. faecalis was also significantly higher in the VAP group. The connection between the gut and lung microbiomes is termed the “gut–lung axis”.25 Research has found that in healthy individuals, the lungs and intestines contain significantly different microbiomes. However, in critically ill patients such as sepsis, severe trauma, or ARDS, the permeability of the intestines and alveoli increases, and potential pathogens may transfer from the intestines into the lungs. The resulting microbial dysbiosis further promotes inflammation and acute lung injury.26,27 E. faecalis is a normal microbe present in the intestine, and some studies have isolated this microbe from the lower respiratory tract specimens of patients with VAP.28,29 A prior study found a close association between enterococci and VAP, leading to prolonged ventilation.30 Together with the current results, we suggest that VAP is associated with the displacement of the intestinal microflora.
The stable presence of Klebsiella pneumoniae in the lower respiratory tract indicates a high rate of background colonization in this patient population. In this study, 171 K. pneumoniae strains were detected using an IAMC, of which 55 (32.16%) were CRKP. In China and Singapore, the majority of highly virulent K. pneumoniae strains that exhibit resistance to carbapenems expressed KPC.31 Our study initially investigated the contribution of the KPC gene to resistance in CRKP using sputum culture and drug sensitivity tests; further genetic typing of 38 KPC-carrying isolates demonstrated that all were KPC-2. Zhang et al reported that KPC-2 strains are resistant to all β-lactams and that they are only sensitive to ceftazidime/avibactam.32 According to the expert consensus, when the sequencing depth is sufficient, it is advised to use resistance gene, with species specificity, prediction for antibiotic-resistant phenotype.33 To date, most studies initially used traditional culture techniques to identify carbapenemase-producing K. pneumoniae, followed by confirmation of the presence of KPC through genetic testing, which is time-consuming. This study discovered that KPC is highly specific and sensitive, enabling clinicians to identify CRKP and select appropriate antibiotics within a few hours.
The IAMC test used in this study is a novel method for the efficient and rapid amplification of DNA under isothermal conditions. In this study, IAMC technology was applied to an elderly population requiring PMV. Compared with sputum culture, the IAMC test had higher ability to detect pathogens such as K. pneumoniae, Enterococcus, S. maltophilia, fungi, and viruses in 2 hours, consistent with the results of related studies.34 The study also found that the IAMC was less affected by antibiotic treatment, maintaining detection rates exceeding 90% for pathogenic bacteria when antibiotics were used for more than 3 days. By combining traditional sputum culture and IAMC technology, the study results illustrated that 21.7% of elderly patients with VAP needed adjustment, which is crucial for the precise treatment of antibiotics.
Strengths and Limitations
The median duration of mechanical ventilation in this study cohort was 249.5 days, and the median age at enrollment was 94 years. Additionally, this was the largest multicenter, prospective study of elderly patients requiring PMV to date. In previous researches on PMV, normally the patients enrolled were below 60 years of age or within 3 months of mechanical ventilation.35,36 This study fills a gap in the microbiological study of the lower respiratory tract in super-elderly patients requiring PMV. However, some limitations must be acknowledged. First, although the microbial species was determined, the microbial load was not assessed. In addition, the cohort had a male predominance, indicating selection bias.
Conclusion
The four most frequently detected organisms in the tracheal aspirates of elderly PMV patients were the Gram-negative bacilli Stenotrophomonas maltophilia, Pseudomonas aeruginosa, Klebsiella pneumoniae and Escherichia coli. This study observed the dynamic changes in the microbial composition in different stages in elderly patients requiring PMV. The findings suggested that virus and gut microorganisms might be closely related to VAP. In addition, KPC-positive can guide antibiotic selection. IAMC technology was helpful for the rapid diagnosis of pathogens and administration of targeted therapy.
Data Sharing Statement
We will provide all relevant de-identified participant data underlying this article, including but not limited to patient demographics, group allocation, sampling time, and test results from lower respiratory tract sputum specimens. The underlying data is deposited at https://www.nbsdc.cn/. Other study documents that will be made available include study protocol and clinical study report, which can be found at https://www.ncmi.cn/. Both are available from the 1st author, Dr. Yang WANG (email: [email protected]), upon reasonable request. The data and the study documents are available immediately and to be shared indefinitely.
Ethics Approval and Consent to Participate
The study protocol was approved by the Ethics Committee of Chinese People’s Liberation Army (PLA) General Hospital (ethical approval number: S2021-374-01), and written informed consent was obtained from all the participants or legal representatives.
Acknowledgment
To clarify, we don’t have a sponsor for this study. The study was funded by the National Key Research and Development Program (2020YFC2005402), the National Clinical Research Center Project for Geriatric Diseases (NCRCG-PLAGH-2023002).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research is supported by the National Key Research and Development Program (2020YFC2005402), the National Clinical Research Center Project for Geriatric Diseases (NCRCG-PLAGH-2023002).
Disclosure
The authors declare no conflict of interests.
References
1. Windisch W, Dellweg D, Geiseler J, et al. Prolonged weaning from mechanical ventilation. Dtsch Arztebl Int. 2020;117(12):197–204. doi:10.3238/arztebl.2020.0197
2. MacIntyre NR, Epstein SK, Carson S, et al. Management of patients requiring prolonged mechanical ventilation: report of a NAMDRC consensus conference. Chest. 2005;128(6):3937–3954. doi:10.1378/chest.128.6.3937
3. Shen X, Sun J, Hong L, et al. Decreased triiodothyronine (T3) as a predictor for prolonged mechanical ventilation in critically ill patients with cardiac surgery. BMC Anesthesiol. 2022;22(1):66. doi:10.1186/s12871-022-01608-6
4. Hung MC, Lu HM, Chen L, et al. Life expectancies and incidence rates of patients under prolonged mechanical ventilation: a population-based study during 1998 to 2007 in Taiwan. Crit Care. 2011;15(2):R107. doi:10.1186/cc10128
5. Chin-Yee N, D’Egidio G, Thavorn K, Heyland D, Kyeremanteng K. Cost analysis of the very elderly admitted to intensive care units. Crit Care. 2017;21(1):109. doi:10.1186/s13054-017-1689-y
6. Goligher EC, Dres M, Fan E, et al. Mechanical ventilation-induced diaphragm atrophy strongly impacts clinical outcomes. Am J Respir Crit Care Med. 2018;197(2):204–213. doi:10.1164/rccm.201703-0536OC
7. Reignier J, Mercier E, Le Gouge A, et al. Effect of not monitoring residual gastric volume on risk of ventilator-associated pneumonia in adults receiving mechanical ventilation and early enteral feeding: a randomized controlled trial. JAMA. 2013;309(3):249–256. doi:10.1001/jama.2012.196377
8. Seguin P, Laviolle B, Dahyot-Fizelier C, et al. Effect of oropharyngeal povidone-iodine preventive oral care on ventilator-associated pneumonia in severely brain-injured or cerebral hemorrhage patients: a multicenter, randomized controlled trial. Crit Care Med. 2014;42(1):1–8. doi:10.1097/CCM.0b013e3182a2770f
9. Zimlichman E, Henderson D, Tamir O, et al. Health care-associated infections: a meta-analysis of costs and financial impact on the US health care system. JAMA Intern Med. 2013;173(22):2039–2046. doi:10.1001/jamainternmed.2013.9763
10. Zilberberg MD, Nathanson BH, Puzniak LA, Shorr AF. Descriptive epidemiology and outcomes of nonventilated hospital-acquired, ventilated hospital-acquired, and ventilator-associated bacterial pneumonia in the United States, 2012-2019. Crit Care Med. 2022;50(3):460–468. doi:10.1097/CCM.0000000000005298
11. Fromentin M, Ricard JD, Roux D. Respiratory microbiome in mechanically ventilated patients: a narrative review. Intensive Care Med. 2021;47(3):292–306. doi:10.1007/s00134-020-06338-2
12. Torres A, Niederman MS, Chastre J, et al. International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital-acquired pneumonia and ventilator-associated pneumonia: guidelines for the management of hospital-acquired pneumonia (HAP)/ventilator-associated pneumonia (VAP) of the European Respiratory Society (ERS), European Society of Intensive Care Medicine (ESICM), European Society of Clinical Microbiology and Infectious Diseases (ESCMID) and Asociacion Latinoamericana del Torax (ALAT). Eur Respir J. 2017;50(3).
13. Lamarche D, Johnstone J, Zytaruk N, et al. Microbial dysbiosis and mortality during mechanical ventilation: a prospective observational study. Respir Res. 2018;19(1):245. doi:10.1186/s12931-018-0950-5
14. Lozupone CA, Stombaugh JI, Gordon JI, Jansson JK, Knight R. Diversity, stability and resilience of the human gut microbiota. Nature. 2012;489(7415):220–230. doi:10.1038/nature11550
15. Hu F, Pan Y, Li H, et al. Carbapenem-resistant Klebsiella pneumoniae capsular types, antibiotic resistance and virulence factors in China: a longitudinal, multi-centre study. Nat Microbiol. 2024;9(3):814–829. doi:10.1038/s41564-024-01612-1
16. Mohan A, Madan K, Hadda V, et al. Guideline for diagnostic flexible bronchoscopy in adults. Zhonghua Jie He He Hu Xi Za Zhi. 2019;42(8):573–590.
17. Du Rand IA, Blaikley J, Booton R, et al. British thoracic society guideline for diagnostic flexible bronchoscopy in adults: accredited by NICE. Thorax. 2013;68(Suppl 1):i1–i44. doi:10.1136/thoraxjnl-2013-203618
18. Niederman MS, Torres A. Severe community-acquired pneumonia. Eur Respir Rev. 2022;31(166):220123. doi:10.1183/16000617.0123-2022
19. De Pascale G, De Maio F, Carelli S, et al. Staphylococcus aureus ventilator-associated pneumonia in patients with COVID-19: clinical features and potential inference with lung dysbiosis. Crit Care. 2021;25(1):197. doi:10.1186/s13054-021-03623-4
20. Xiao T, Guo Q, Zhou Y, et al. Comparative respiratory tract microbiome between carbapenem-resistant acinetobacter baumannii colonization and ventilator associated pneumonia. Front Microbiol. 2022;13:782210. doi:10.3389/fmicb.2022.782210
21. Klompas M. New insights into the prevention of hospital-acquired pneumonia/ventilator-associated pneumonia caused by viruses. Semin Respir Crit Care Med. 2022;43(2):295–303. doi:10.1055/s-0041-1740582
22. Hagel S, Scherag A, Schuierer L, et al. Effect of antiviral therapy on the outcomes of mechanically ventilated patients with herpes simplex virus detected in the respiratory tract: a systematic review and meta-analysis. Crit Care. 2020;24(1):584. doi:10.1186/s13054-020-03296-5
23. Luyt CE, Combes A, Deback C, et al. Herpes simplex virus lung infection in patients undergoing prolonged mechanical ventilation. Am J Respir Crit Care Med. 2007;175(9):935–942. doi:10.1164/rccm.200609-1322OC
24. Shorr AF, Ilges DT, Micek ST, Kollef MH. The importance of viruses in ventilator-associated pneumonia. Infect Control Hosp Epidemiol. 2023;44(7):1137–1142. doi:10.1017/ice.2022.223
25. Wang L, Cai Y, Garssen J, Henricks P, Folkerts G, Braber S. The bidirectional gut-lung axis in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2023;207(9):1145–1160. doi:10.1164/rccm.202206-1066TR
26. Narayana JK, Aliberti S, Mac AM, et al. Microbial dysregulation of the gut-lung axis in bronchiectasis. Am J Respir Crit Care Med. 2023;207(7):908–920. doi:10.1164/rccm.202205-0893OC
27. Mu S, Xiang H, Wang Y, et al. The pathogens of secondary infection in septic patients share a similar genotype to those that predominate in the gut. Crit Care. 2022;26(1):68. doi:10.1186/s13054-022-03943-z
28. Nesseler N, Mansour A, Schmidt M, et al. Healthcare-associated infections in patients with severe COVID-19 supported with extracorporeal membrane oxygenation: a nationwide cohort study. Crit Care. 2024;28(1):54. doi:10.1186/s13054-024-04832-3
29. Kharel S, Bist A, Mishra SK. Ventilator-associated pneumonia among ICU patients in WHO Southeast Asian region: a systematic review. PLoS One. 2021;16(3):e0247832. doi:10.1371/journal.pone.0247832
30. Grasselli G, Scaravilli V, Mangioni D, et al. Hospital-acquired infections in critically ill patients with COVID-19. Chest. 2021;160(2):454–465. doi:10.1016/j.chest.2021.04.002
31. Wang M, Earley M, Chen L, et al. Clinical outcomes and bacterial characteristics of carbapenem-resistant Klebsiella pneumoniae complex among patients from different global regions (CRACKLE-2): a prospective, multicentre, cohort study. Lancet Infect Dis. 2022;22(3):401–412. doi:10.1016/S1473-3099(21)00399-6
32. Zhang P, Shi Q, Hu H, et al. Emergence of ceftazidime/avibactam resistance in carbapenem-resistant Klebsiella pneumoniae in China. Clin Microbiol Infect. 2020;26(1):124.e1–124.e4. doi:10.1016/j.cmi.2019.08.020
33. In OM, Moderate TP, Chinese PC, et al. Expert consensus for the application of metagenomic next generation sequencing in the pathogen diagnosis in clinical moderate and severe infections (first edition). Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2020;32(5):531–536. doi:10.3760/cma.j.cn121430-20200228-00095
34. Wei S, Wang L, Shi M, et al. Rapid, accurate, and novel diagnostic technique for respiratory pathogens: clinical application of loop-mediated isothermal amplification assay in older patients with pneumonia, a multicenter prospective observational study. Front Microbiol. 2022;13:1048997. doi:10.3389/fmicb.2022.1048997
35. Bissett B, Gosselink R, van Haren F. Respiratory muscle rehabilitation in patients with prolonged mechanical ventilation: a targeted approach. Crit Care. 2020;24(1):103. doi:10.1186/s13054-020-2783-0
36. Colleti JJ, Azevedo RT, de Oliveira CF, de Araujo OR. Prolonged mechanical ventilation in children: review of the definition. Pediatr Crit Care Med. 2021;22(11):e588–e593. doi:10.1097/PCC.0000000000002773
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.