")
Back to Journals » International Journal of Women's Health » Volume 14
Respectful Maternity Care in South Asia: What Does the Evidence Say? Experiences of Care and Neglect, Associated Vulnerabilities and Social Complexities
Authors Kaphle S , Vaughan G , Subedi M
Received 3 December 2021
Accepted for publication 3 March 2022
Published 7 July 2022 Volume 2022:14 Pages 847—879
DOI https://doi.org/10.2147/IJWH.S341907
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Sabitra Kaphle,1 Geraldine Vaughan,2 Madhusudan Subedi3
1Central Queensland University, School of Health, Medical and Applied Sciences, Melbourne, VIC, 3000, Australia; 2Central Queensland University, School of Health, Medical and Applied Sciences, Sydney, NSW, 2000, Australia; 3School of Public Health, Patan Academy of Health Sciences, Kathmandu, Nepal
Correspondence: Sabitra Kaphle, Central Queensland University, School of Health, Medical and Applied Sciences, Melbourne, VIC, 3000, Australia, Email [email protected]
Background: Respectful maternity care encompasses the right to continuity of care and dignified support for women during the reproductive period, enabling informed choice. However, the evidence is limited in the context of South Asia region where maternal, perinatal and newborn mortality is still a critical challenge to health systems. Evidence is required to better understand the context of respectful maternity care to inform directions for appropriate policy and practice.
Objective: The objective of this scoping review was to explore facilitators and barriers of respectful maternity care practice in South Asia.
Design: CINAHL, EMBASE, PubMed, Medline, SCOPUS and Cochrane databases were used to identify related studies. Data were systematically synthesized and analysed thematically.
Findings: There was considerable heterogeneity in the 61 included studies from seven South Asian countries, with most of the research conducted in Nepal and India. While the experience of abuse and neglect was common, 10 critical themes emerged related to neglected choices and compromised quality of care (particularly where there were health inequities) in the context of institutional care experiences; and the imperative for improved investment in training and significant policy and legislative change to enforce equitable and respectful maternity care practice.
Conclusions and Implications for Practice: Evidence about respectful maternity care in South Asia indicates that women accessing professional and facility-based services experienced high levels of disrespect, abuse and maltreatment. Women from vulnerable, socially disadvantaged and economically poor backgrounds were more likely to experience higher level abuse and receive poor quality of care. There is an urgent need for a well-resourced, sustained commitment to mandate and support the provision of respectful and equitable maternity care practice in South Asia.
Keywords: maternal health, respect, pregnancy, maternity care, health service, South Asia
Introduction
Around 810 women die globally each day from preventable causes related to pregnancy and childbirth, 94% of which occur in low resource settings (World Health Organisation, 2019). Reducing maternal, perinatal and neonatal mortality in developing countries has been a concerted focus of both Millennium Development Goals (MDGs) and Sustainable Development Goals (SDGs) with efforts to address underlying mortality risks by promoting institutional births, increasing skilled professional support and ensuring that every woman has access to basic maternal health care.1
However, the challenge remains high for sub-Saharan Africa and South Asia in particular to tackle the complex factors contributing to higher mortality.2 In resource-limited settings, a range of social, cultural, economic and structural barriers consistently impact on women’s access to care during pregnancy and childbirth,3,4 thus reductions in related deaths remain a critical challenge for health systems. Furthermore, significant disparities exist within the regions and countries in which the burden of maternal, perinatal and neonatal mortality is highest, concentrated among women who experience disproportionate health inequities and poorer health outcomes associated with structural deficiencies and discrimination.1,5
The South Asia region includes eight countries – Afghanistan, Bangladesh, Bhutan, India, Nepal, Maldives, Pakistan, and Sri Lanka – where maternal, perinatal and newborn mortality has been an ongoing challenge for the health system. With concerted efforts of all sectors, South Asia has demonstrated a significant reduction in maternal mortality ratio (MMR) from 384 per 100,000 live births in 2000 to 157 in 2017 (World Health Organisation, 2019), underpinned by improved access to skilled providers and quality maternity care.6,7 These figures contrast to MMRs of 10–18 per 100,000 live births in high-income countries and there is work to be done to continue (and sustain) decreased MMRs.
A critical aspect of continued progress in better maternal outcomes is having access to respectful maternity care (RMC). Based on human rights principles, RMC ensures that every woman receives dignified, equitable care without coercion or discrimination, including the right to her choice of care and preferences during the childbirth to support positive experiences. These rights are violated when a woman experiences disrespect, abuse, refusal or mistreatment by care providers or professionals during pregnancy and childbirth.8,9 A growing recognition of the extent of mistreatment, abuse, disrespect and neglect of women during childbirth has in turn led to demands for an urgent response to address these concerns.10,11 Experiences of abuse and disrespect among women giving birth in health institutions create barriers for women seeking health care during pregnancy and birth-related complications, as well as being a serious human rights concern.12,13
Provision of respectful maternal care requires collaborative efforts across disciplines, systems and stakeholders, including women, families, care providers, health services and health care systems.14 The increased utilisation of pregnancy-related services by women in South Asia offers an opportunity to demonstrate the impacts of quality care in the further reduction of maternal, perinatal and neonatal mortality. In turn, this supports services to operationalise the concept of respectful maternity care fully in practice, improving positive experiences for women seeking professional services and promoting choice and agency for women. A better understanding of the context of existing practice, barriers and enablers is required to inform RMC practice in South Asia. A scoping review was determined as the appropriate method to map and explore current practice and perspectives in South Asian countries, examining evidence of RMC experiences to women who attend services during pregnancy, childbirth and postnatal period.
Methods
The review used the framework and Preferred Reporting Items for Systematic Reviews and Meta-Analysis extension for scoping reviews (PRISMA-ScR) guidelines.15,16
The following questions guided the review process.
- What is respectful maternity care and how it is defined?
- What are current practices around respectful maternity care in South Asia?
- What facilitators and barriers exist in maintaining respectful maternity care in South Asia?
- Which populations are at a higher risk of not receiving respectful maternity care in South Asia?
- What actions and policies are required to support improvements in respectful maternity care in South Asia?
Eligibility and Search Strategy
Eligibility criteria comprised peer-reviewed research published in English from 2010 to 2020 that focused on experiences of women, their families, service providers, stakeholders and community (see Table 1).
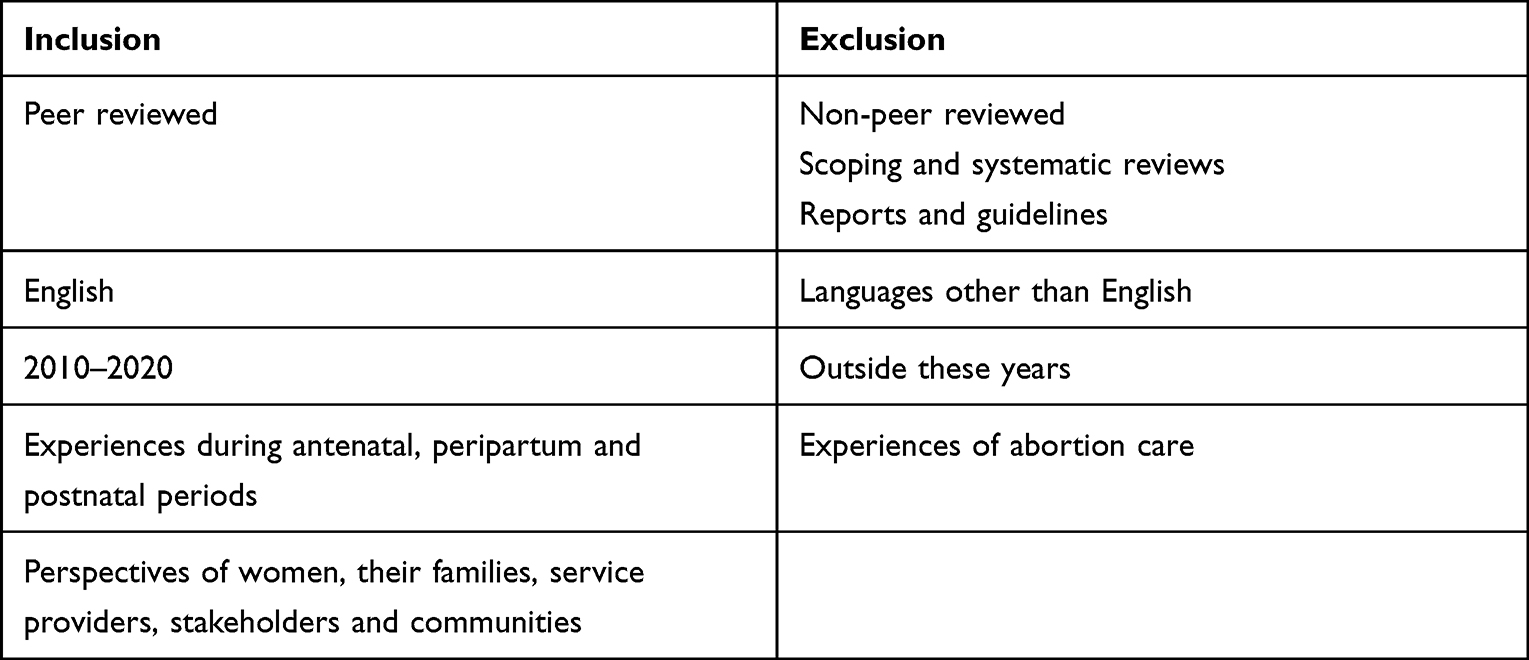 |
Table 1 Inclusion and Exclusion Criteria of Studies |
An initial limited search of MEDLINE and CINAHL was conducted, followed by a brief analysis of the text words contained in the title and abstract of retrieved papers. A second search using identified keywords and index terms was undertaken across all included databases. Thirdly, the reference list of identified reports and articles from full-text sources included in the screening review was then searched for additional sources. Search terms for CINAHL, EMBASE, PubMed, Medline, SCOPUS and Cochrane databases related to pregnancy and childbirth; professional and other birth support role; attributes of care; and country location and included maternity OR maternal OR pregnant* OR childbirth OR birth* OR antenatal OR perinatal OR postnatal AND midwife* OR midwives OR obstetric* OR “healthcare provider” OR “health care provider” OR “healthcare professional” OR “health care professional” OR “health volunteer” OR “birth attendant” AND “health services” OR “models of care” OR “health system” OR “health practice” OR community OR healthcare OR “health care” OR “health practice” AND respect* OR dignity OR woman-centred OR “woman centred” OR “client centred” OR “person centred” OR “culturally safe” OR quality OR compassion* OR holistic OR disrespect* OR abuse OR discrimination OR stigma AND “South Asia” OR “South Asian” OR Afghanistan* OR Bangladesh* OR Bhutan* OR India* OR Maldives OR Nepal* OR Pakistan* OR “Sri Lanka” OR Sri Lanka*.
The searches were conducted in November and December 2020, resulting in 1157 articles.
Study Selection
Two reviewers (SK and GV) independently reviewed the titles of identified articles (1157) and those clearly not relevant to the topic were excluded. Abstracts of all articles were reviewed for inclusion using the screening checklist developed with criteria for this review. The full texts of potentially eligible papers (155) were retrieved and reviewed by two reviewers (SK and GV) based on the criteria with a primary focus on respectful maternity care during pregnancy, childbirth and up to six weeks’ postpartum in the South Asia region. During the screening, disagreement between reviewers were resolved by discussion with a third reviewer (MS). See Figure 1.
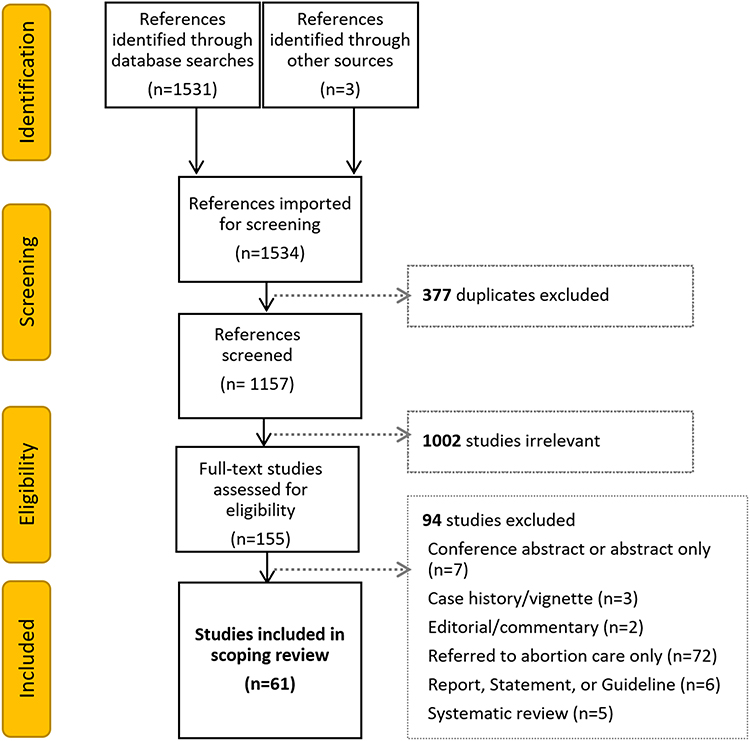 |
Figure 1 PRISMA reporting framework for study selection. Notes: Adapted from: Tricco AC, Lillie E, Zarin W et al PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann Intern, Med. 2018;169(7):467–473. doi:10.7326/M18-0850.16 Copyright © 2018, The American College of Physicians. Creative Commons Attribution License (https://creativecommons.org/about/cclicenses/). |
Quality Assessment
Two reviewers (SK and GV) conducted assessment independently and discussed together until the consensus was reached in the case of discrepancies. This appraisal process helped to refine and interpret the findings of the review.
Data Extraction
Population and study characteristics, data collection and analysis, themes, author’s interpretations including the data around current practice, barriers, enablers of respectful care, characteristics of abuse and study recommendations were extracted to a standardised table developed for this review (see Table 2).
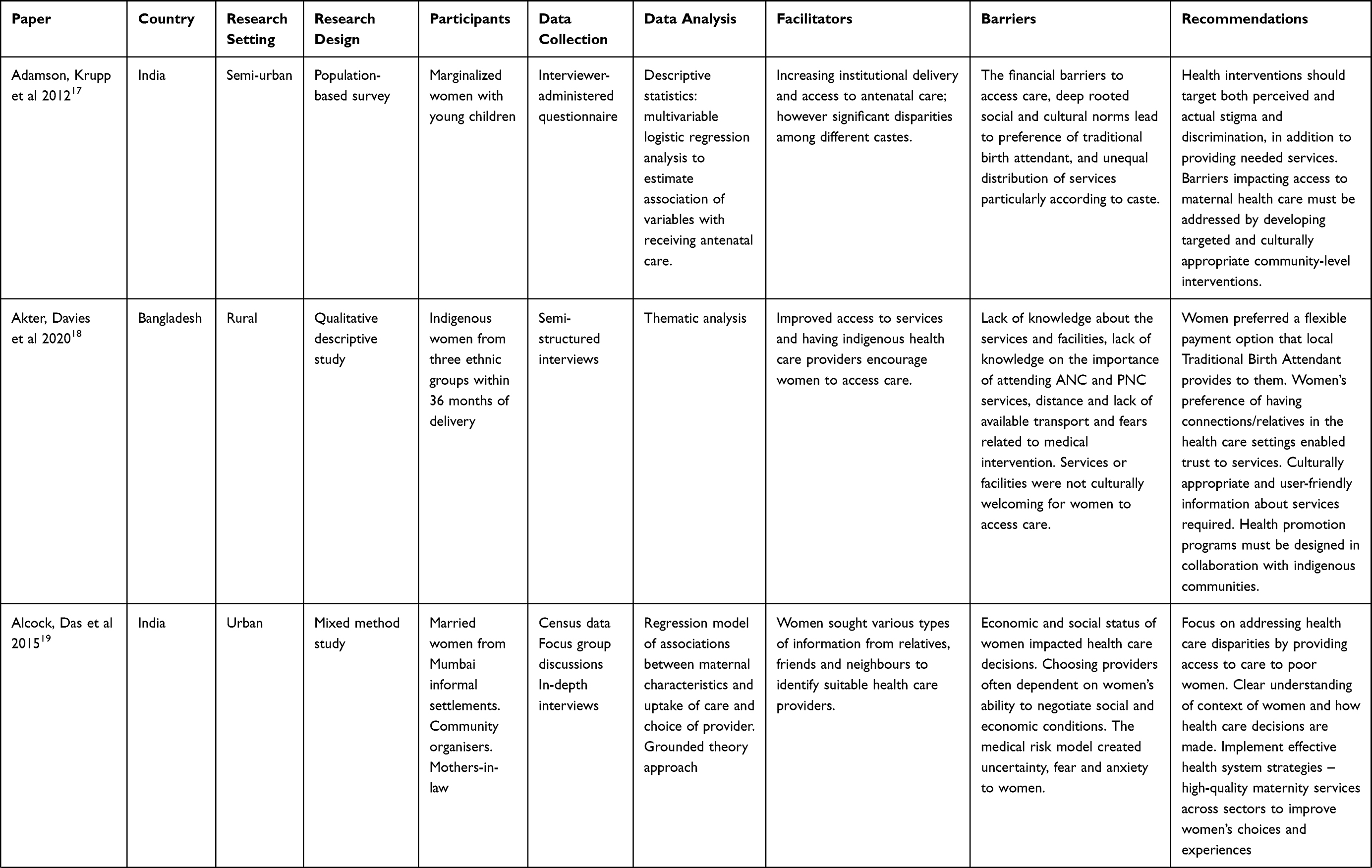 | 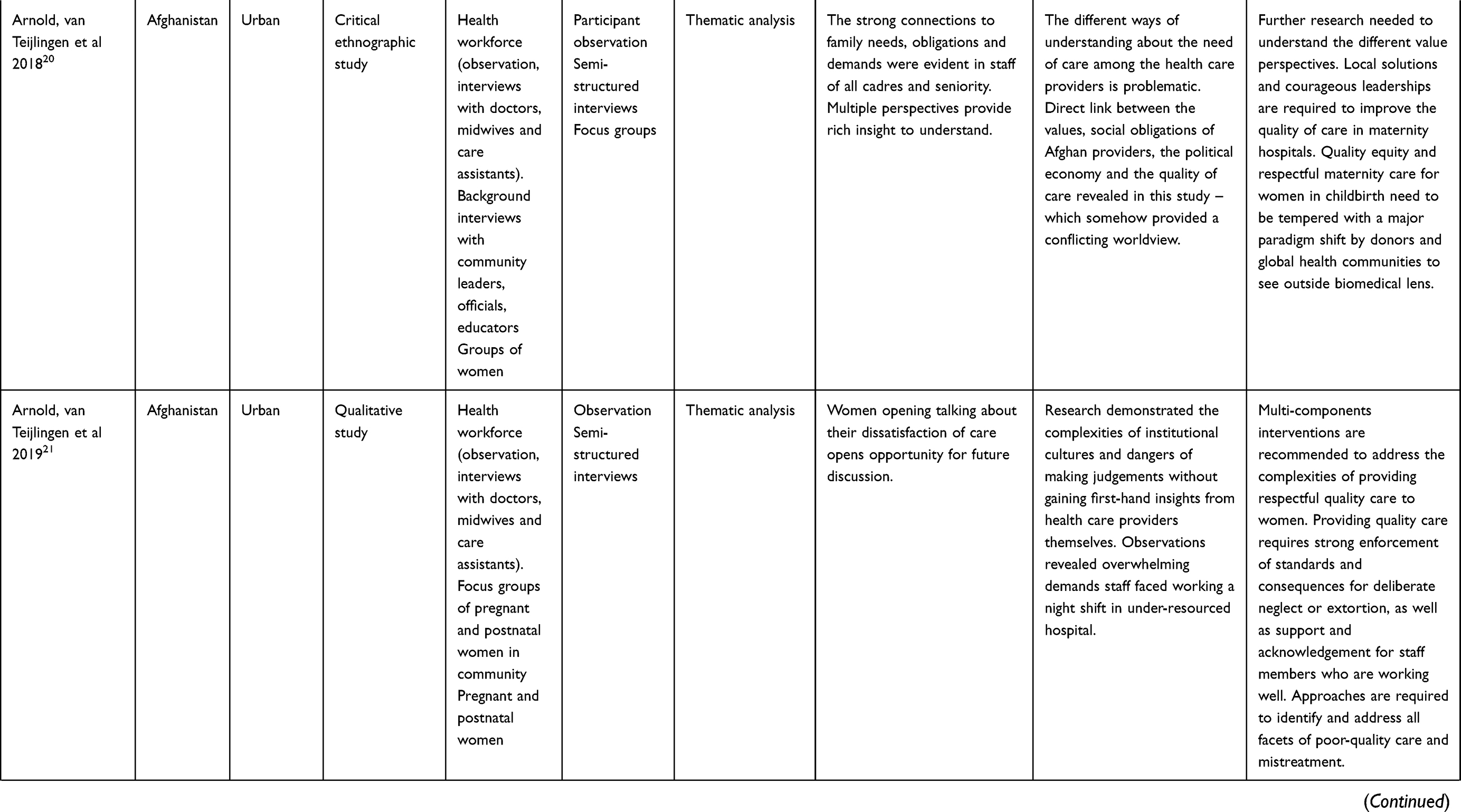 | 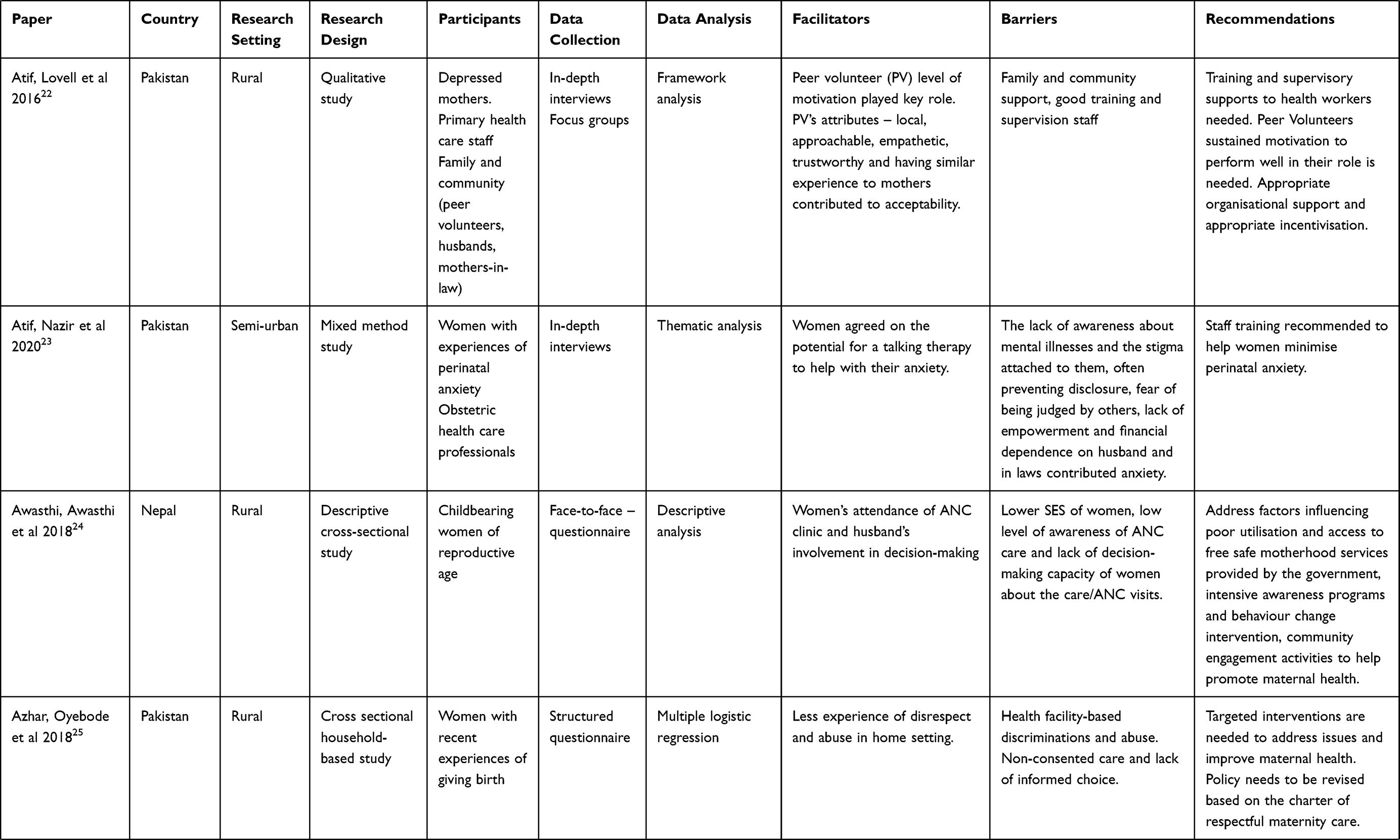 | 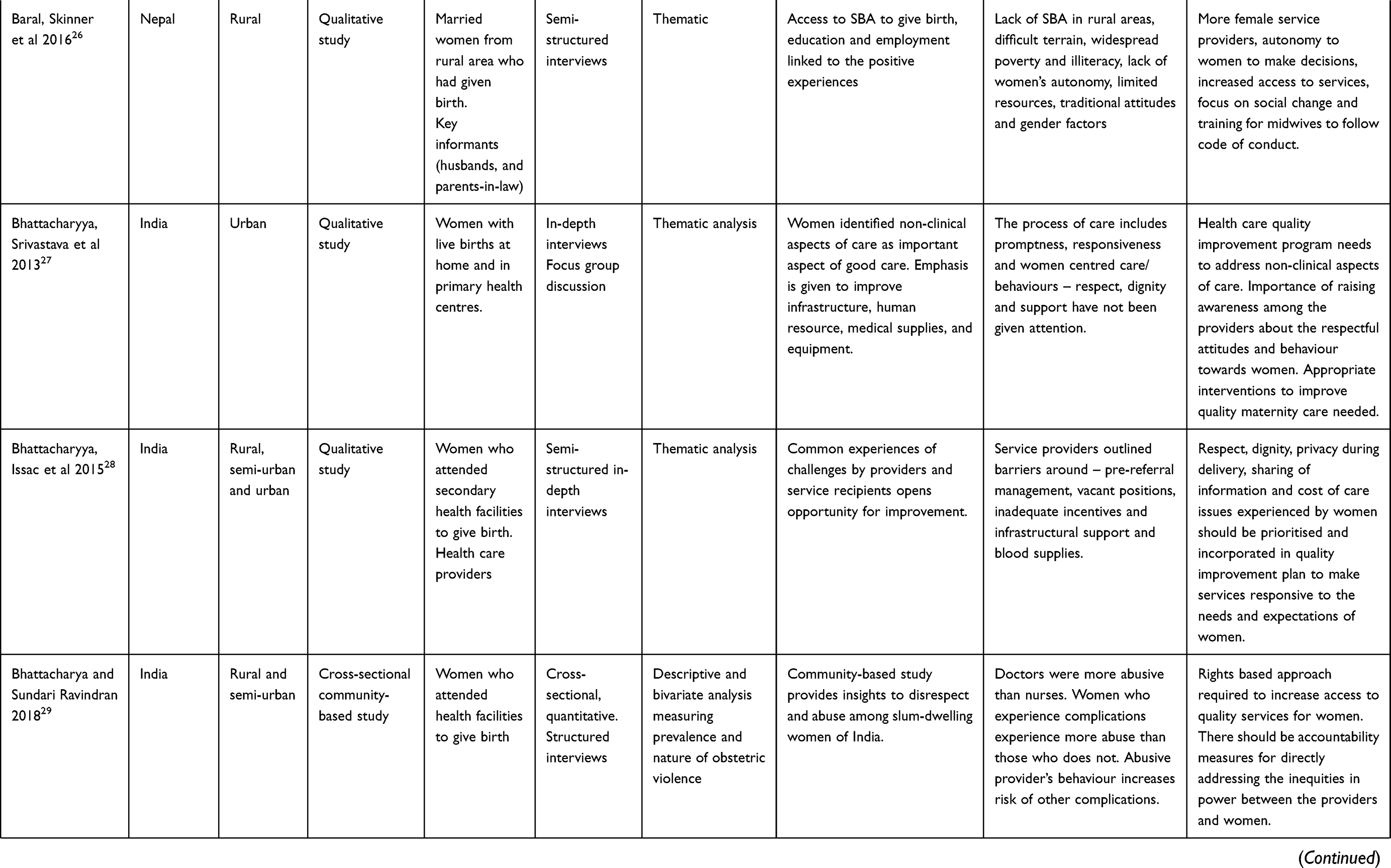 | 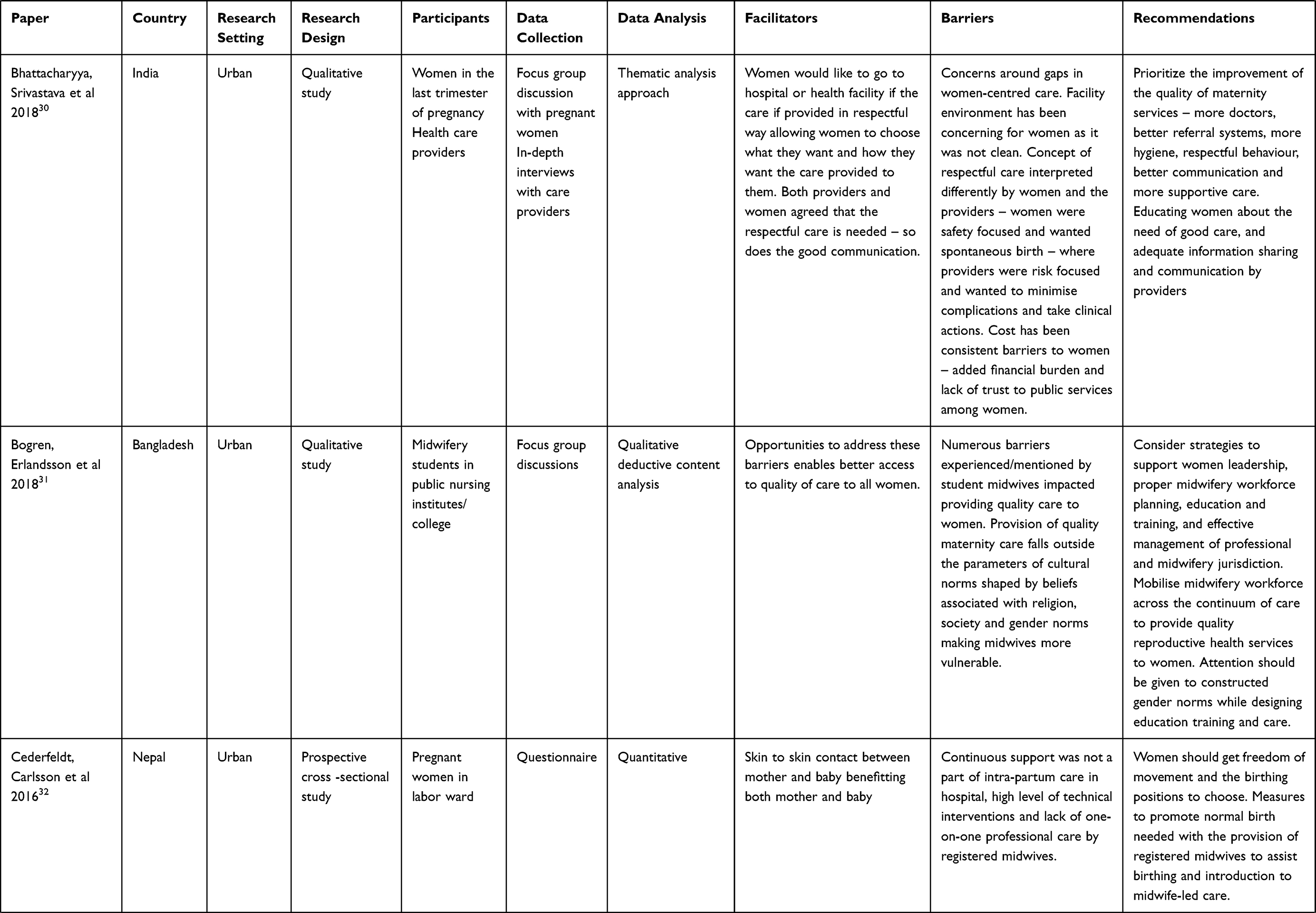 | 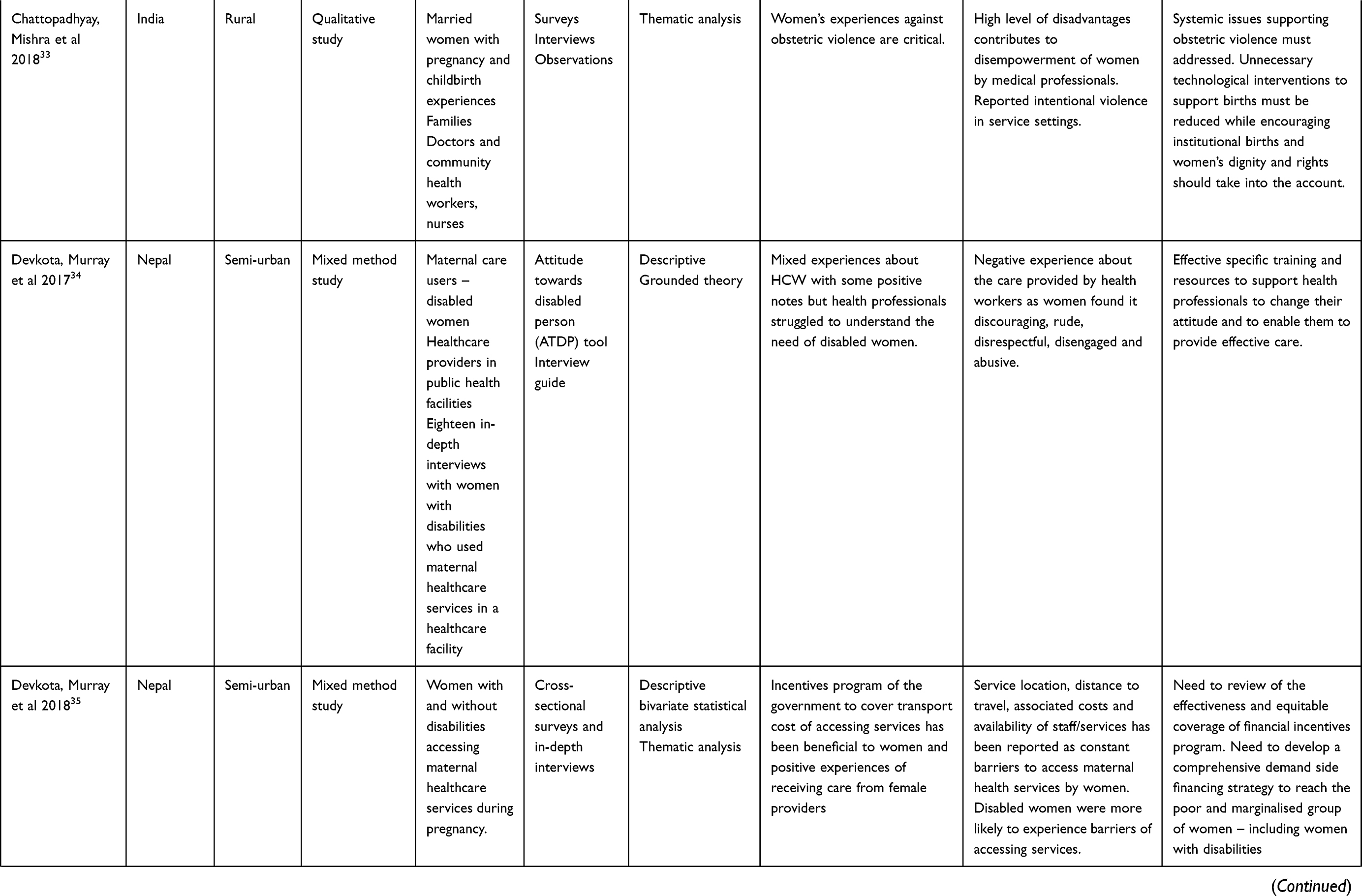 | 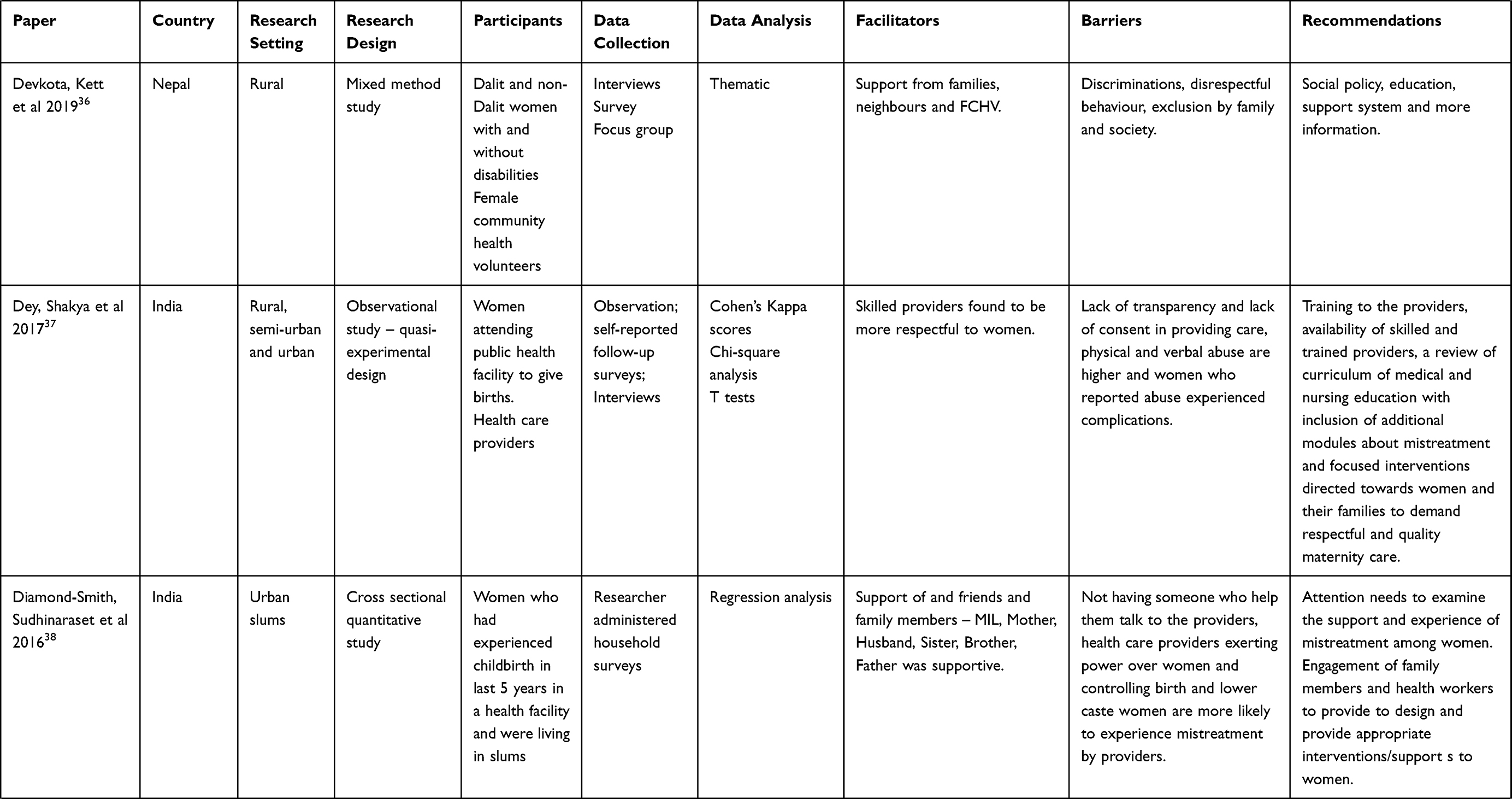 | 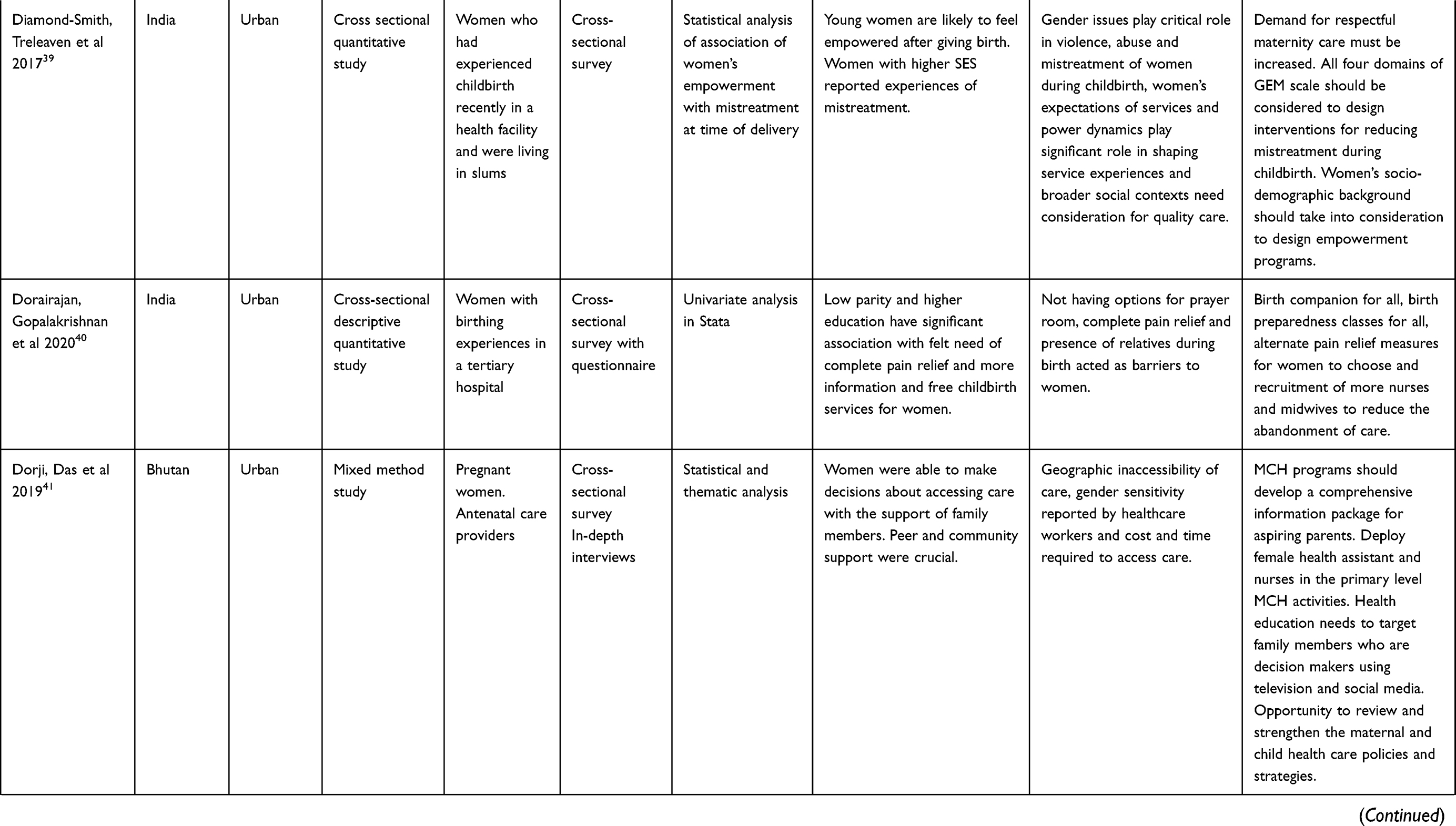 | 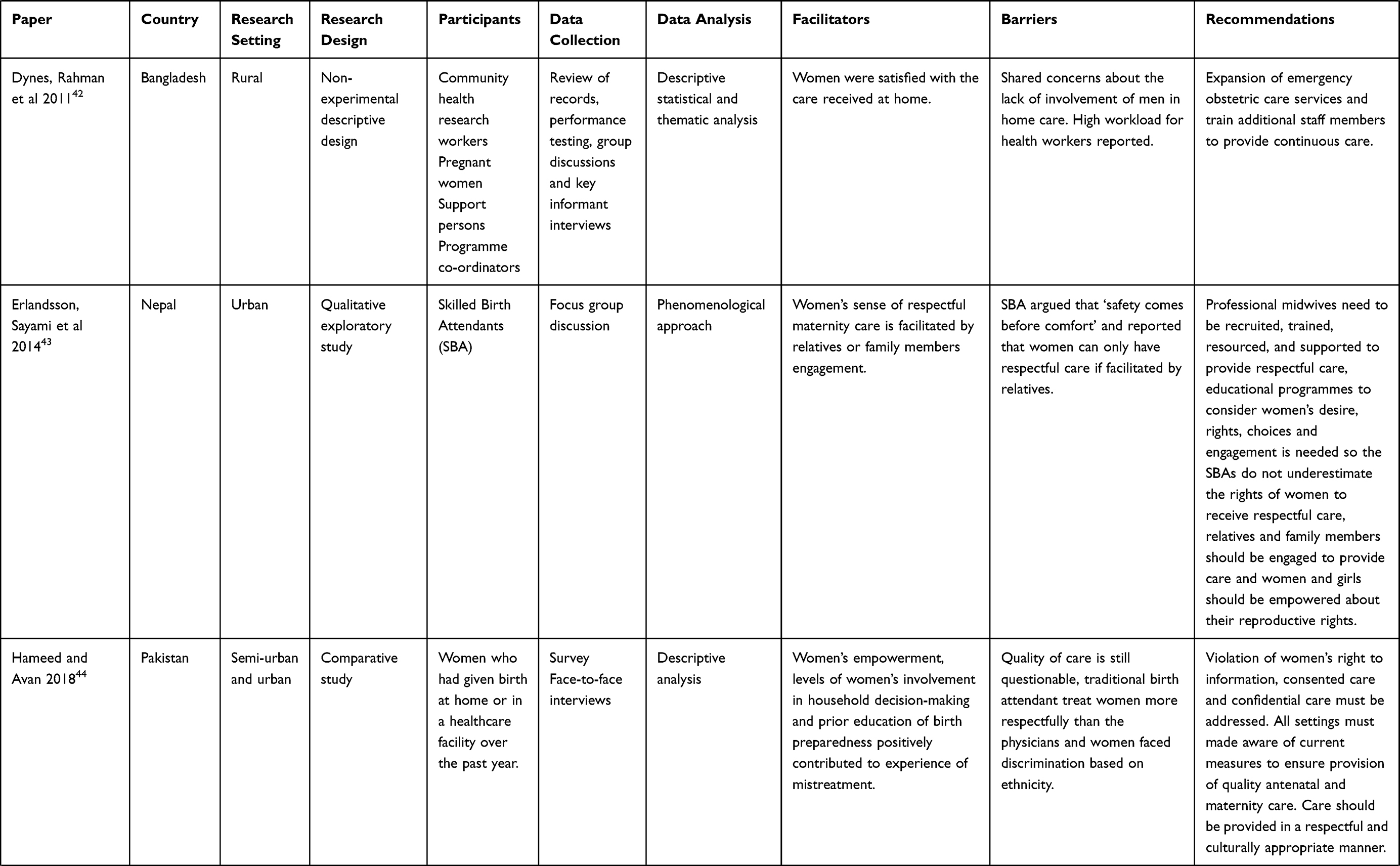 | 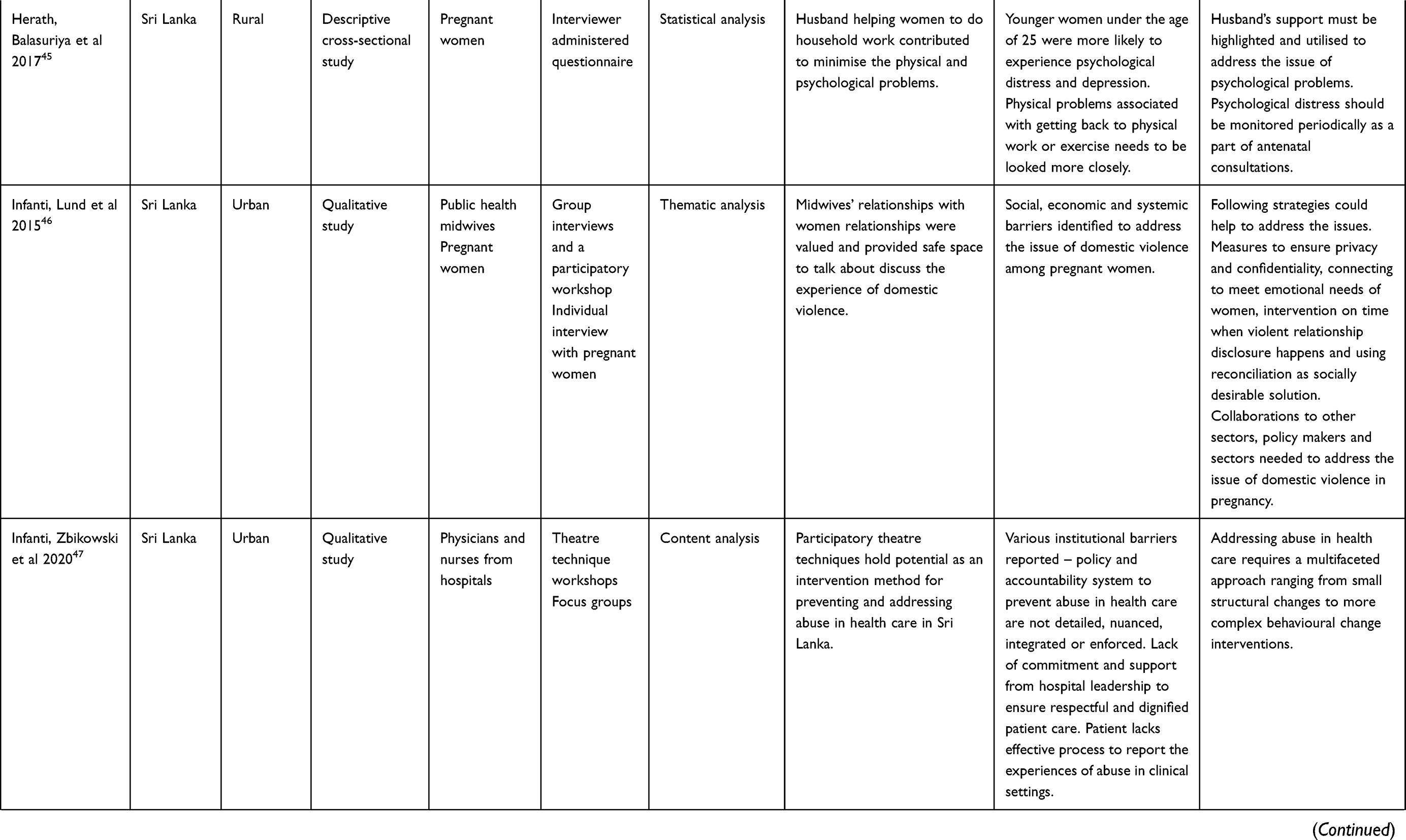 | 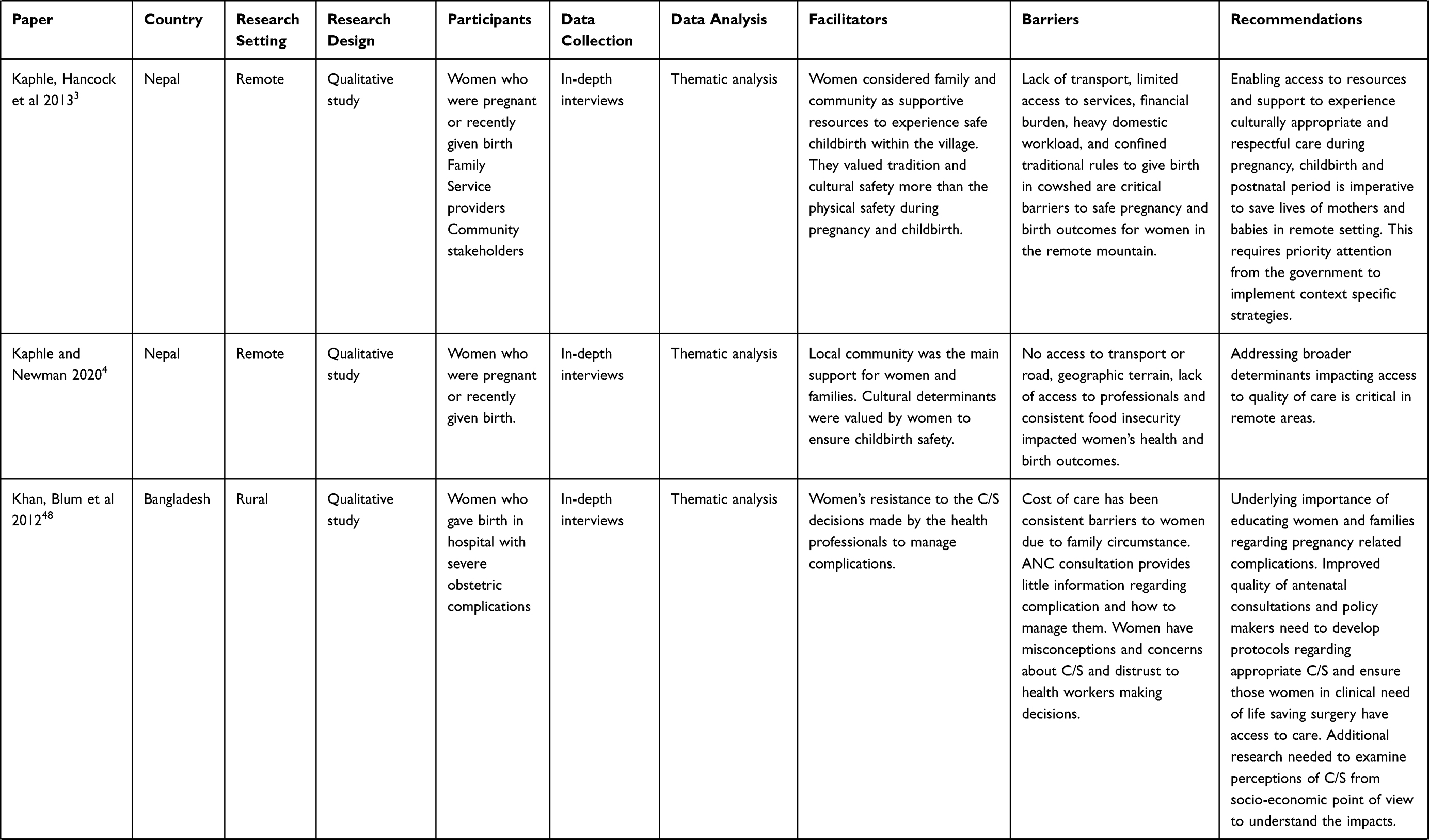 | 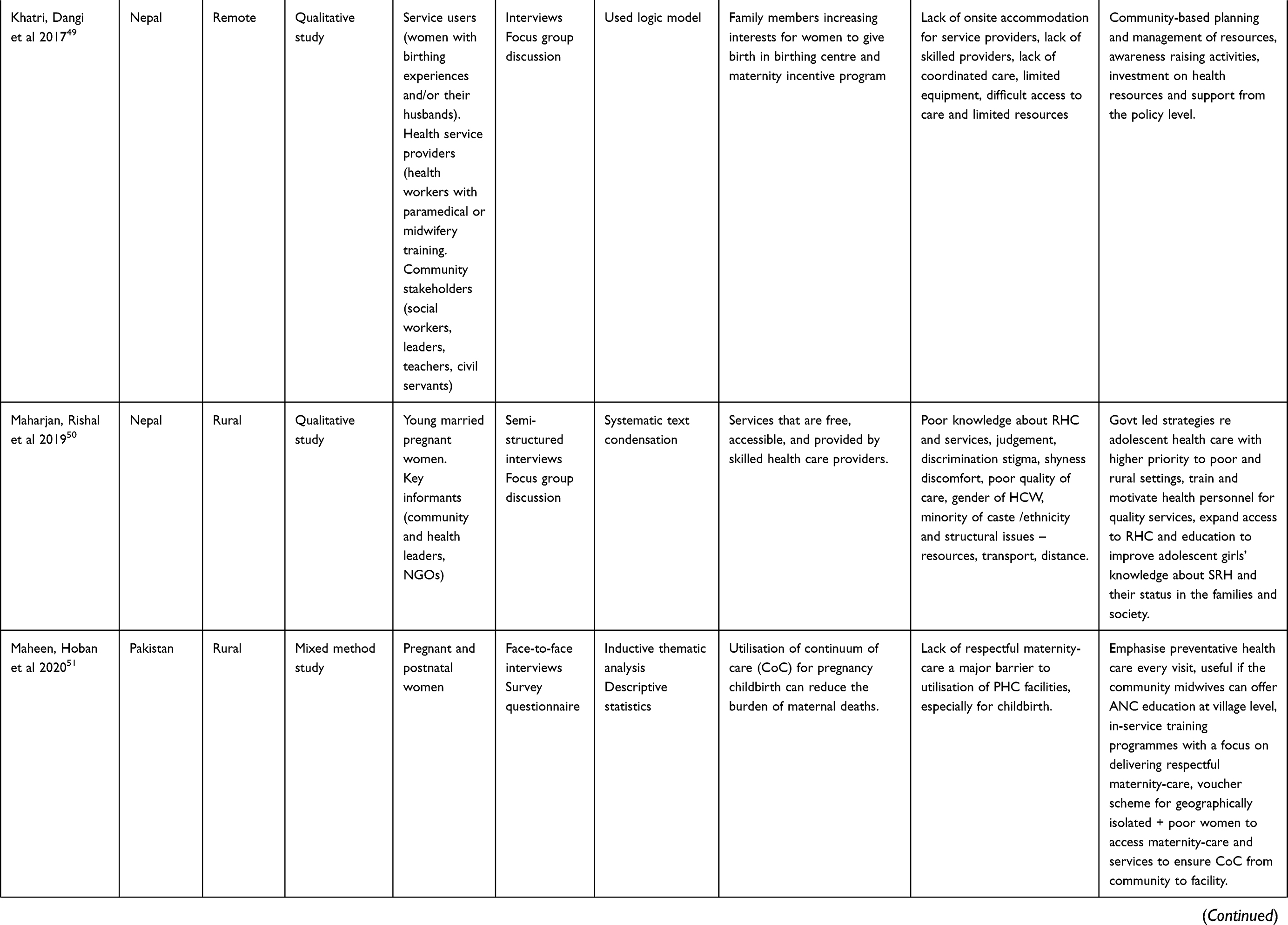 | 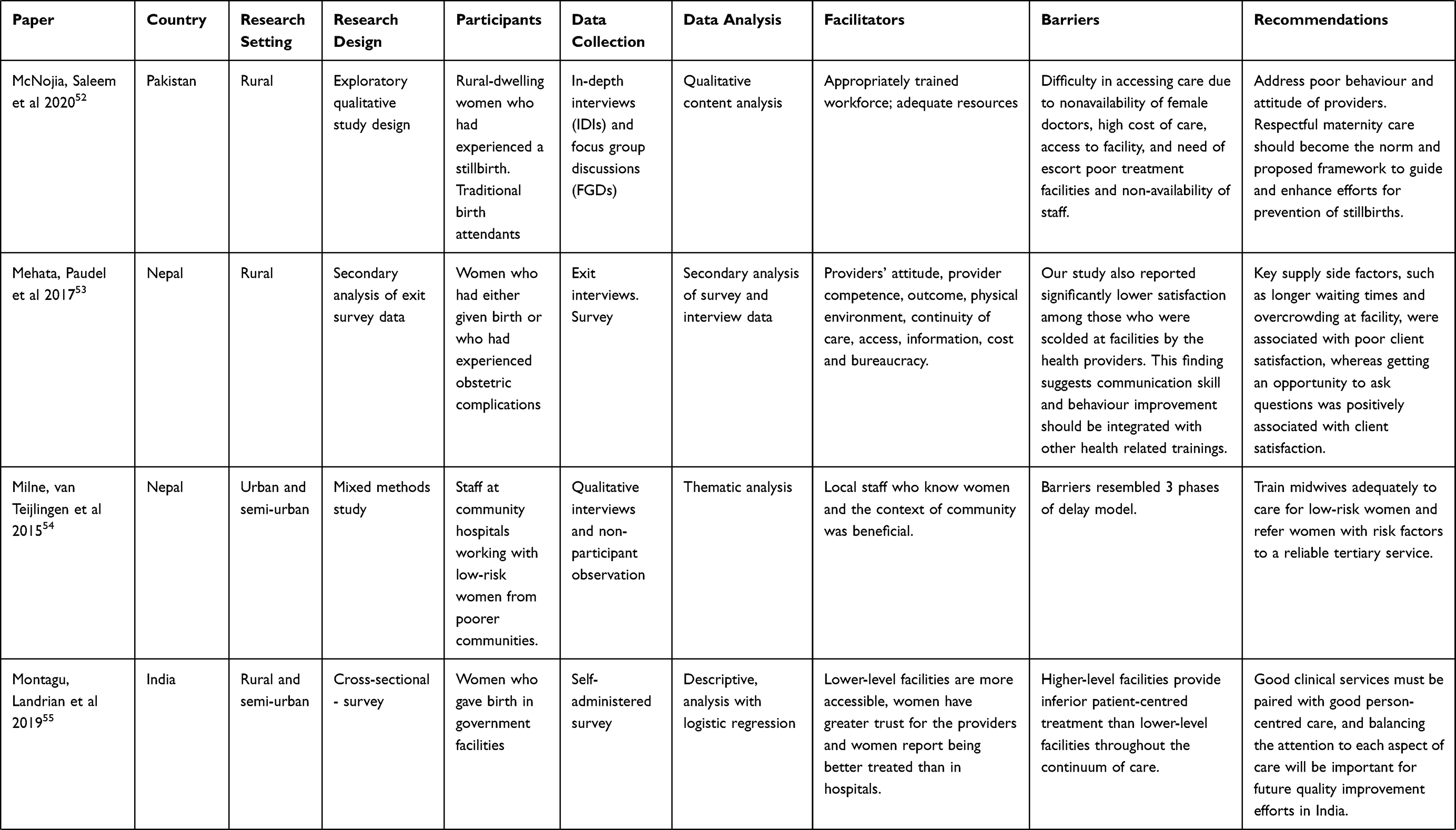 | 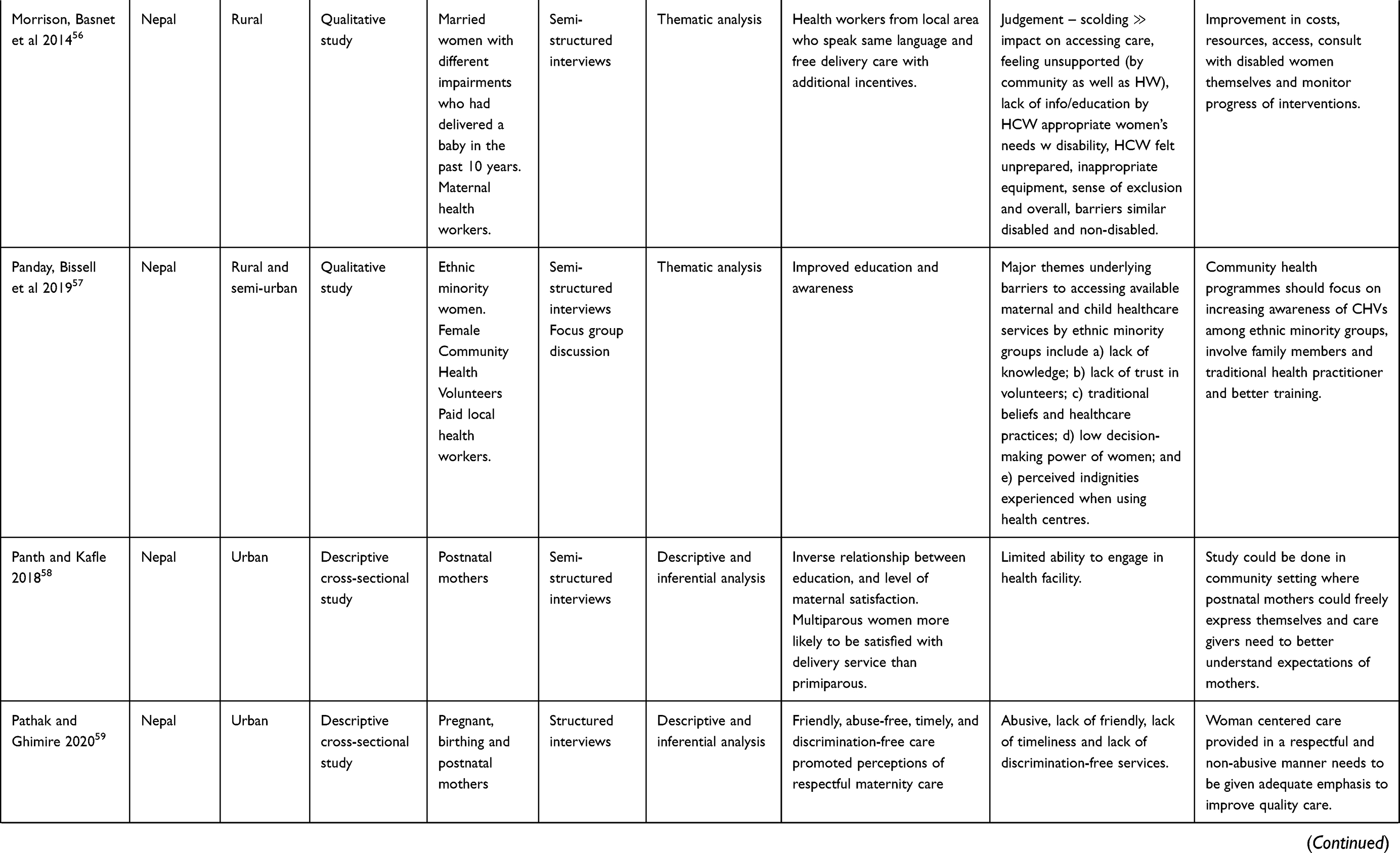 | 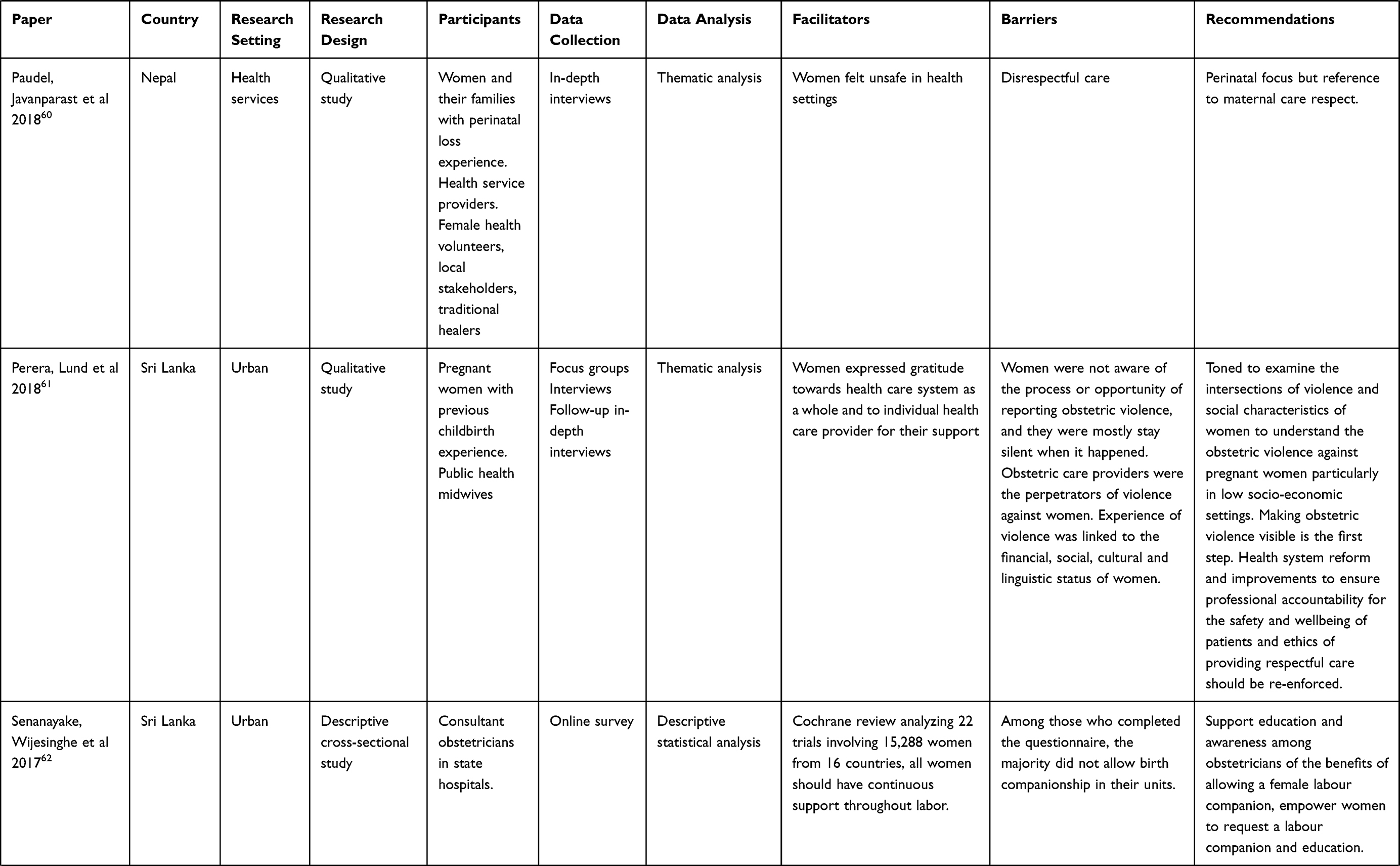 | 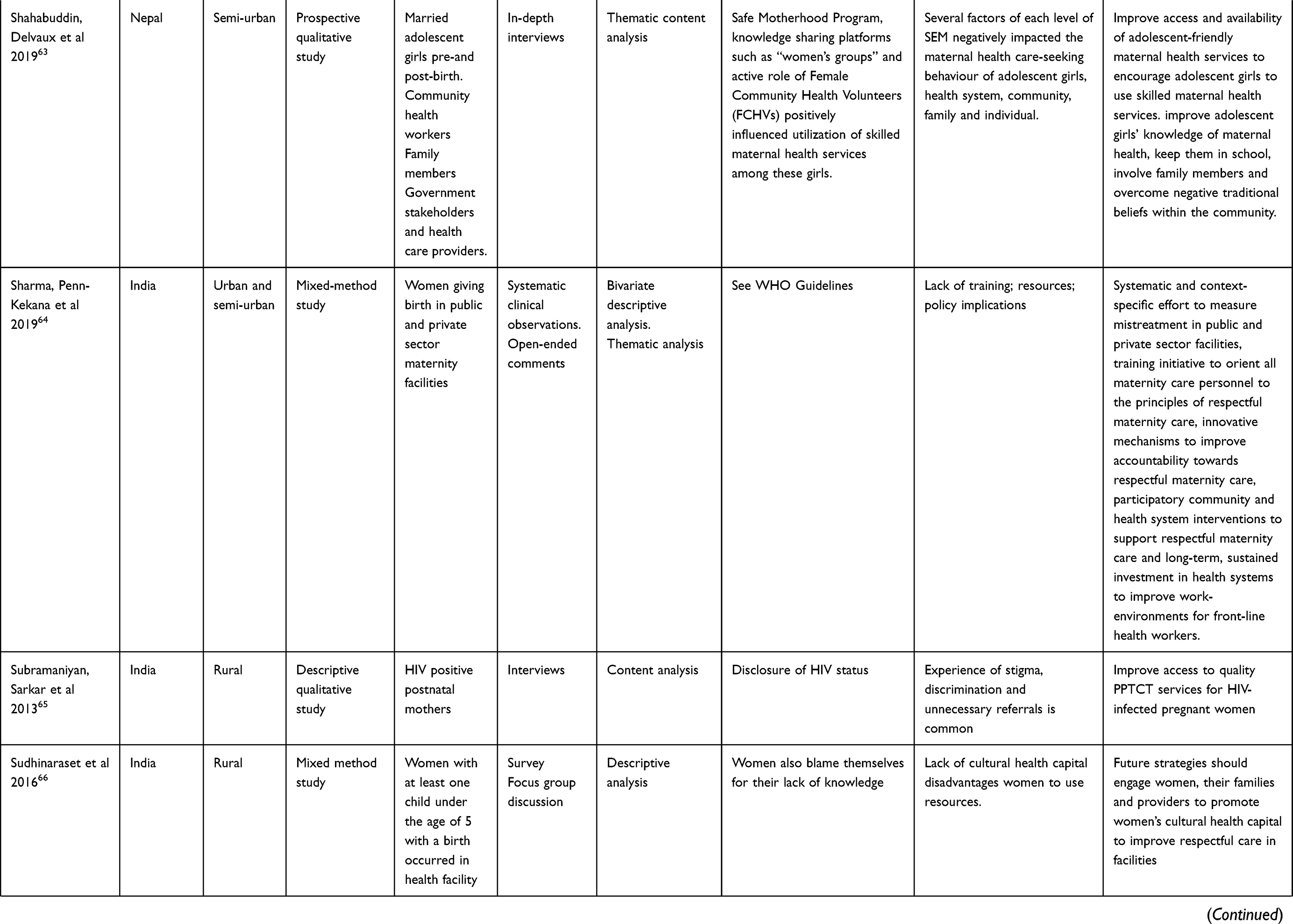 |  | 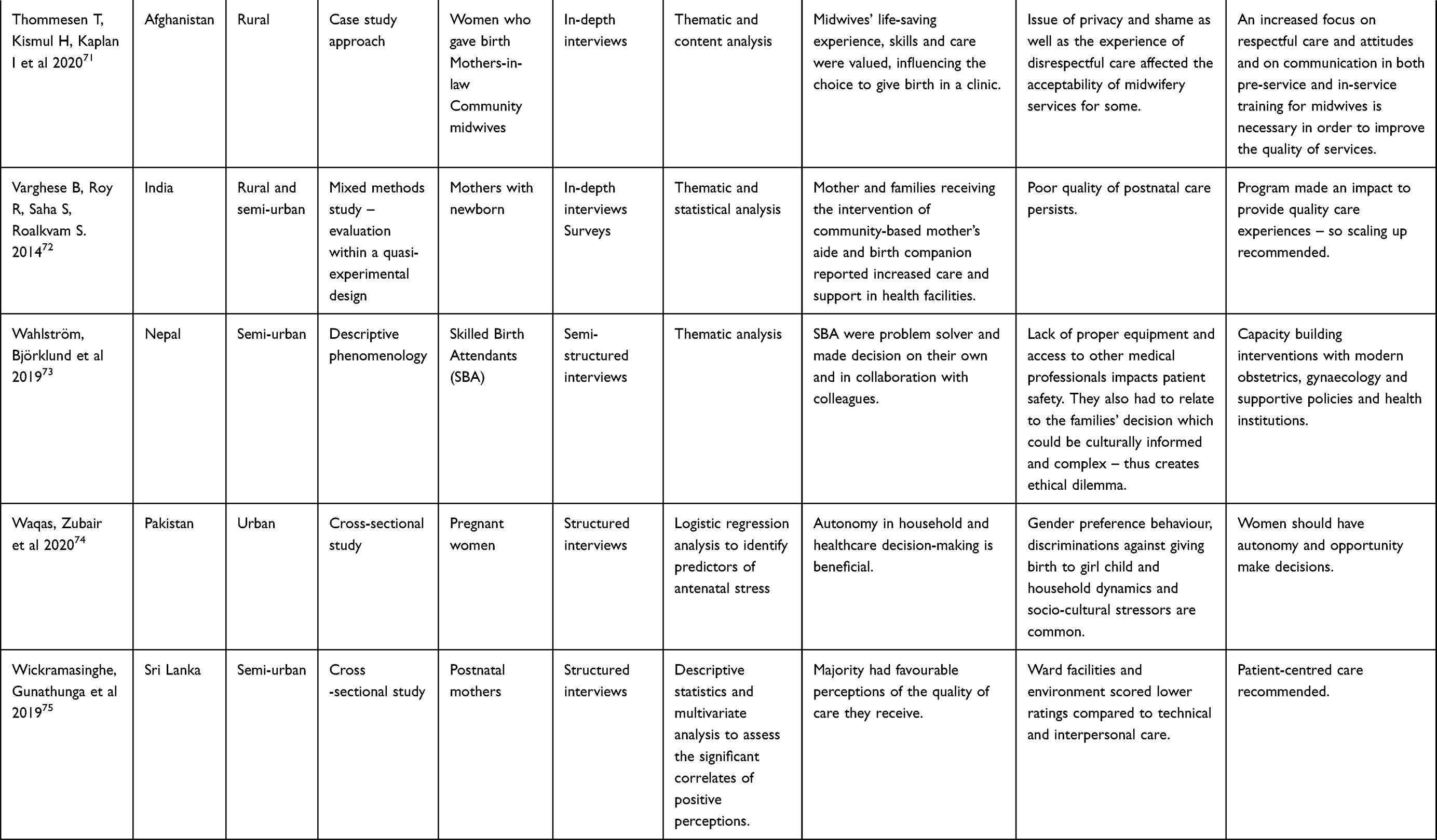 |
Table 2 Characteristics of Included Papers |
Data Synthesis
A combined inductive and deductive thematic analysis approach was employed, where initial open coding on each relevant text unit elicited key themes emerging from the data. We developed the preliminary coding framework with main domains drawn from the literature and checked against the studies selected for inclusion. All included studies were reviewed until no new themes emerged and the co-researchers agreed on the definition, scope and interpretation of each theme. During the synthesis process, we revised some codes and merged some sub-themes. Based on the initial coding, repeated review of codes and emerging themes, 10 broad themes were developed to provide focused interpretations of the results.
Results
The analysis synthesised findings from 61 studies conducted across seven countries: Afghanistan, Bangladesh, Bhutan, India, Nepal, Pakistan, and Sri Lanka (Figure 2). No eligible papers from the Maldives were sourced. Most studies explored the experiences of women, with some including perspectives of family members, midwives, obstetricians, midwifery students, hospital officials, community stakeholders and community-based care providers. The research included a mix of quantitative (21), qualitative (29) and mixed methods (11) study designs.
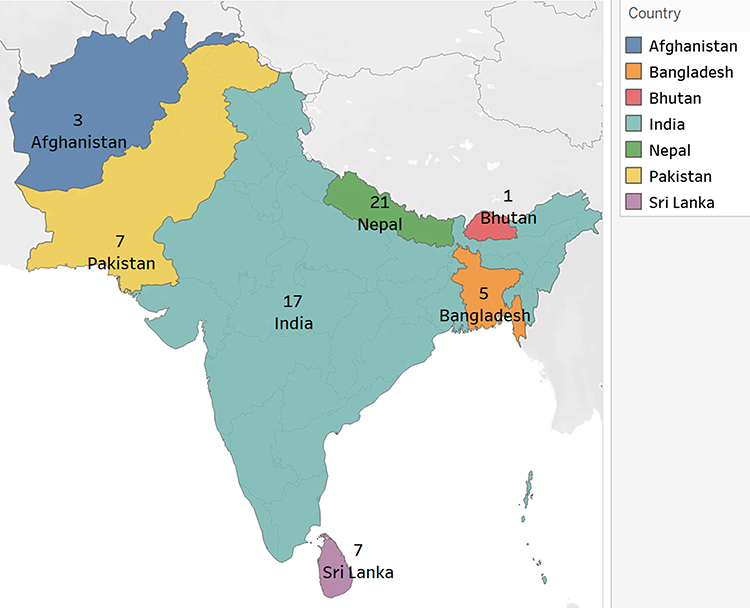 |
Figure 2 A map of included studies in the review by country. |
Table 2 describes the characteristics of included studies. Table 3 summarises the preliminary codes and categories from included studies that addressed the scoping review research questions and guided the development of themes. Ten themes emerged that described issues in the provision of respectful maternity care for women in South Asia. These in turn were grouped, reflecting the focus on two broad overlapping domains that described deficits of care and influencing factors (Compromised quality of care, Context and inequities influencing experiences); and calls for change (Responses and needs, and System level changes – policy, education, funding). Themes and domains were related according to how they were referenced by women, family and community, and workforce (see Figure 3).
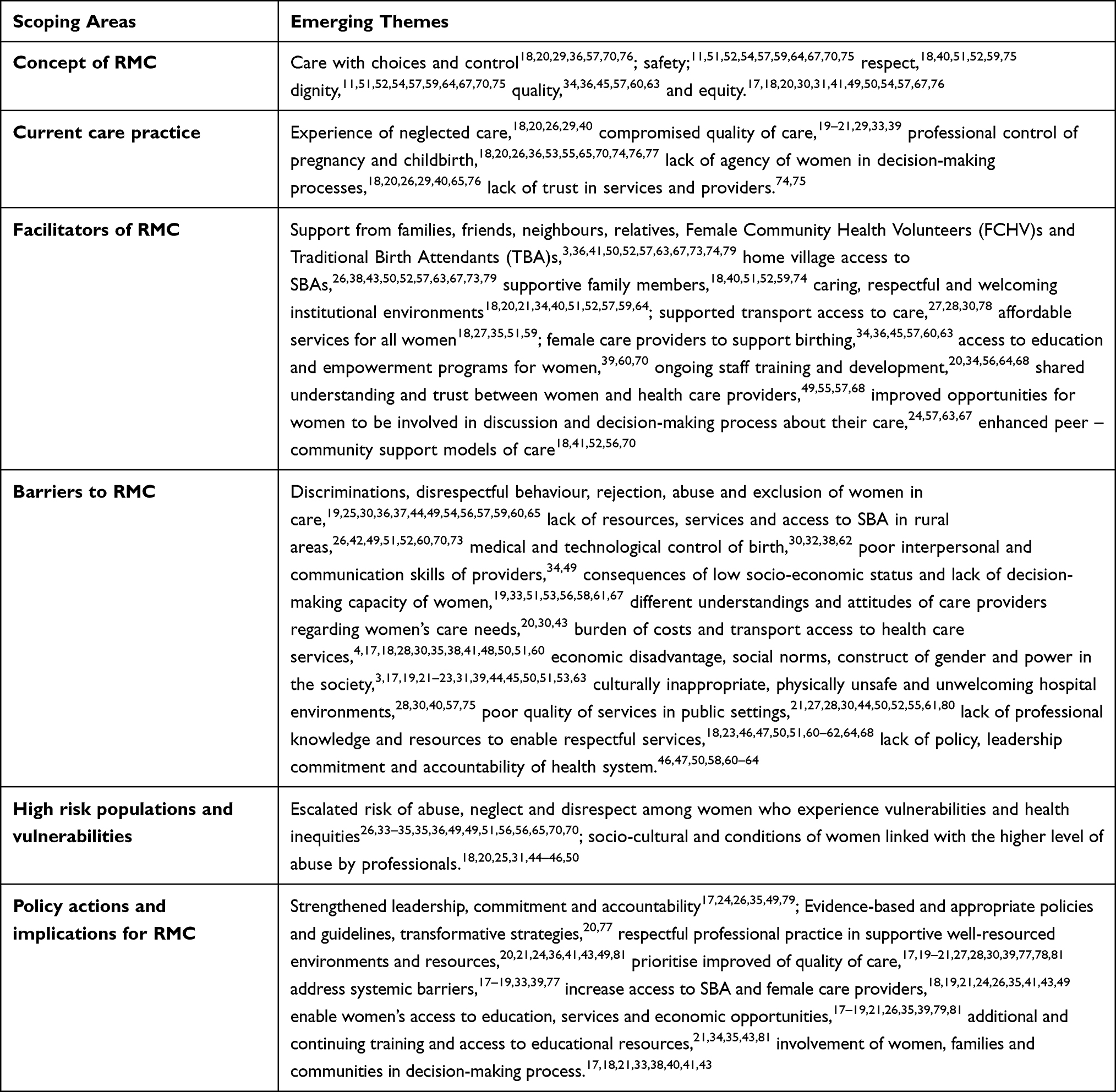 |
Table 3 Aspects of Respectful Maternity Care |
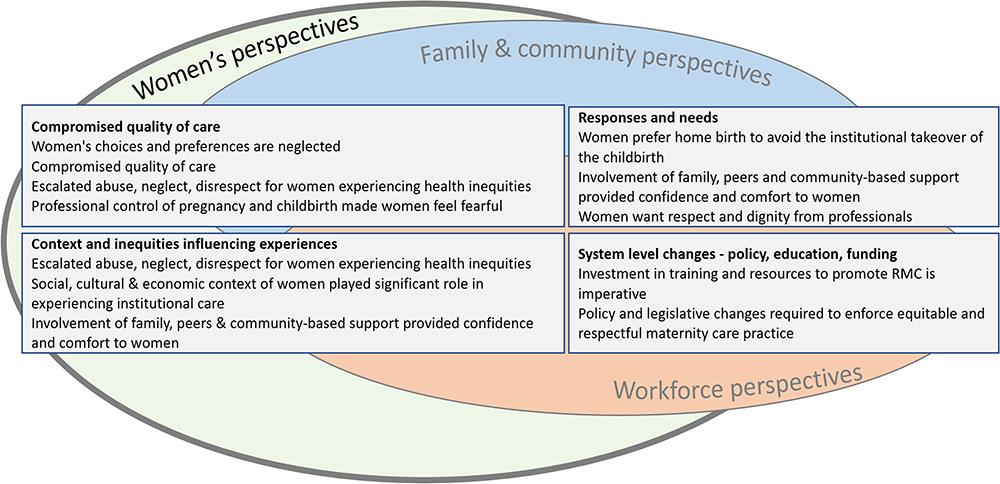 |
Figure 3 A diagram of reported themes from the scoping review. |
The 10 themes are described after Table 2.
Women’s Choices and Preferences are Neglected
Women and family members described being neglected by health care professionals when their choices and preferences to manage pregnancy, childbirth and postnatal care.18,20,26,29,40 Women found that professionals took control of their birth and employed routine procedures without including them in decision-making processes65,76 and that this resulted in a lack of trust in the services provided to women.74,75
Within in the context of family relationships, power dynamics, and the way decisions are made about the services and care within South Asian society, the roles of husband and (in particular) mothers-in-law in making childbirth decisions and expectations regarding practice was critical, with mixed acceptance by women.3,39,52,71,74 This signifies the hidden oppression of women within the social construct of power of patriarchal society and how women are often excluded in making decisions about childbirth.4
Compromised Quality of Care
Women who utilised the facility-based professional care shared their negative experiences and questioned the quality of care provided to them.29,39 Limited access to services was described, ranging from medicines, proper equipment, competent, skilled health care and food supplies. These factors all diminished the quality of services in an environment where women felt they had little agency in the choice of services or health care providers.19,29,33 Women felt their pregnancy and birth was medicalised within the controlled clinical environment of the hospital and reflected on their experience of a lack of basic respect and kindness to women.20,21
Escalated Abuse, Neglect and Disrespect Among Women Who Experience Health Inequities
Women who already experienced health inequities and compromised health outcomes due to underlying social determinants and discrimination experienced more serious forms of abuse, neglect and disrespect from health professionals.35,49,51,56,65,70 This further marginalised and silenced women and their families who felt unable to speak about their negative experiences with health services.26,33,34,36,51,56,65,70 Studies questioned the effectiveness of attempts to address inequities in maternity care in socially vulnerable communities.26,33–36,49 These women are more likely to experience more frequent and significant maternal, perinatal and neonatal morbidity with an associated increased risk of mortality.
Professional Control of Pregnancy and Childbirth Made Women Feel Fearful
Several studies described women’s experience of professional control of pregnancy and childbirth, which left women with little or no perceived ability to make any decisions about the services.20,36,55,65,70,76,77 Women felt they were not involved in decisions about prescribed medicines or procedures and why they were required.26,53,74 This lack of involvement and communication about procedures resulted in further uncertainties, fear and anxiety for women.18,36 Women expressed a preference for access to and choices of medical and technological interventions while giving birth.33,38,41,59,63,64
Women Prefer Home Birth to Avoid the Institutional Takeover of the Childbirth
In this context of professional control and institutional takeover of birth, studies described women’s preference to stay away from the hospital environment in order to exercise some freedom of choice.18,20,29,36,57,70,76 They were more likely to stay home to give birth and seek assistance from family members and community-based care providers to manage problems they experienced during pregnancy, childbirth and postnatal period.26
Where previous experiences of abuse, disrespect, unnecessary clinical procedures, lack of empathy by midwives and doctors and mistreatment created fear, this aversion increased.27,49,56,63,64,67,78 Consequent delays resulted in an increased risk of emergency hospital attendance during pregnancy and childbirth.36,49,56,62,67,70,76
Social, Cultural and Economic Context of Women Played Significant Role in Experiencing Institutional Care
Studies described the social, cultural and economic contexts that impacted on women’s experiences of disrespect, abuse and poor quality of care in the hospital environment. This was heightened for younger women, women from lower socio-economic background, women with disability, women living in rural and remote areas and women from minority religious backgrounds.25,44,46,50,69 In South Asian societies women’s needs, choices and preferences were often neglected during pregnancy and childbirth,31 leading to psychological distress and anxiety, particularly for those women who lacked support from family and health institutions.45 Women and families also spoke about the burden of hidden and unofficial costs required to manage transport, food and other supplies while accessing services in the hospital.18 One study described an interesting pattern between providers and women regarding their cultural and social background in terms of understanding, empathy, trust and provision of respectful care.20
Involvement of Family, Peers and Community-Based Support Provided Confidence and Comfort to Women
Women described being happy to receive the care, support and respect from family, peers, and community-based care providers,41 although the family relationships and power dynamics described in the first theme were influencing factors.3 They tended to seek advice and support from families, relatives, friends and neighbours to make decisions about the types of services and the care providers within their socio-economic circumstances.18,19,72 The collective decisions made about the services for women were based on the intention of gaining positive experiences and minimising the risks of poor birth outcomes. In most cases, women expressed a preference to use traditional birth attendants to support birthing17,52 and female community health volunteers to seek information before or after childbirth.56
Women Want Respect and Dignity from Professionals
Women from diverse settings described hospital environments that created feelings of uncertainties, discrimination, abandonment and neglect by health care providers.11,51,52,54,57,59,64,67,70,75 They shared expectations of having health care providers who would listen and understand their concerns, problems and preferences while providing care with a kind attitude.18,40,51,52,59,75 Women wanted to be treated with respect and dignity without judgement about their social, cultural and economic backgrounds.11,51,52,54,57,59,64,67,70,75
Women preferred to have female doctors and midwives from their cultural and linguistic background to support positive experiences.34,36,45,57,60,63 These findings were congruent with health care providers who agreed about the importance of respect; however, they also highlighted various barriers limiting capacity to do so in their institutional role.17,18,20,30,31,41,49,50,54,57,67,76
Investment in Training and Resources to Promote RMC is Imperative
Health care providers emphasised the need to provide more resources to health care institutions and provide continuous training in respectful maternity care to enable appropriate practice environments.20,34,56,64,68 Studies described an urgent need for improved resourcing – including medicine, equipment and other essential items – to provide quality maternity care to all women.19,26,28,35,49 Public health care facilities were typically more challenged compared to private based on the available infrastructure, resources, support to staff and knowledge of respectful practice.28,49 Women and family members further highlighted the issue of cleanliness, better food, medical supplies, promptness of providing care and attitude of the doctors and midwives.35,53,59,64,74,75
Policy and Legislative Changes Required to Enforce Equitable and Respectful Maternity Care Practice
Most studies reinforced the obligation of providing quality maternity care to all women with equity and respect regardless of age, ethnicity, religion, culture, socio-economic background and physical ability.20,36,50,60,73,76 Providing women an opportunity to make choices about their childbirth was significant but not understood or practiced by the health care professionals.19,59 Women and families believed that government has accountability to provide respectful care, but health care providers constantly highlighted the barriers to provide quality of care to women.29,33,43,54,55,70
It was clear that women’s preference was dismissed in the institutional setting and women subsequently became victim of unnecessary clinical interventions.17,29,43,54,67 Women from low socio-economic background received little attention from health care providers while receiving care.17,21,31,35,50,59 The need for strong policy efforts were recommended as the way to mandate equitable and respectful care in a South Asian context.20,36,60,62,78
Facilitators and Enablers for RMC
Facilitators and enablers to enhance positive experiences to women in South Asia were identified as including support from families, friends, neighbours, relatives, Female Community Health Volunteers (FCHV)s and Traditional Birth Attendants (TBA)s,3,36,41,50,52,57,63,67,73,74,79 having access to SBAs in the village,26,38,43,50,52,57,63,67,73,79 supporting family members to take women to the birthing centre,18,40,51,52,59,74 the provision of a caring, respectful and welcoming institutional environments;18,20,21,34,40,51,52,57,59,64 economic support to women to attend care,27,28,30,78 involvement of female care providers to support birthing,34,36,45,57,60,63 access to education and empowerment programs for women,39,60,70 affordable services to all women;18,27,35,51,59 shared understanding and trust between women and health care providers,49,55,57,68 improved opportunities for women to be involved in discussion and decision-making process about their care,24,57,63,67 enhancing peer-community support models of care;18,41,52,56,70 ongoing training for staff on emerging issues.20,34,56,64,68 The roles of midwives and FCHVs were seen as influential in determining women’s experiences and ensuring their access to community-based services.21,26,31,34,43,70,74,75
Barriers to RMC
In summary, barriers to the provision of respectful maternity care included discriminations, disrespectful behaviour, rejection, abuse and exclusion of women in care,19,25,30,36,37,44,49,54,56,57,59,60,65 lack of resources, services and access to SBA in rural areas,26,42,49,51,52,60,70,73 medical and technological control of birth,30,32,38,62 poor interpersonal and communication skills of providers,34,49 consequences of low socio-economic status and lack of decision-making capacity of women,19,24,33,51,53,56,58,61,67 different understandings and attitudes of care providers regarding women’s care needs,20,30,43 the burden of costs and transport access to health care services,4,17,18,28,30,35,38,41,48,50,51,60 economic disadvantage, social norms, construct of gender and power in the society,3,17,19,21–23,31,39,44,45,50,51,53,63 culturally inappropriate, physically unsafe and unwelcoming hospital environments,28,30,40,57,75 poor quality of services in public settings,21,27,28,30,44,50,52,55,61,80 lack of knowledge and resources to enable respectful services,18,23,46,47,50,51,60–62,64,68 and lack of policy, leadership commitment and accountability of health system.46,47,50,58,60–64
Implications for Policy and Practice
Several studies discussed implications of their findings for evidence-based policies, transformative strategies and respectful professional practice.20,77 The imperative of appropriate social policies, guidelines, supportive environment and resources to raise awareness about the concept of respectful maternity care was consistently highlighted.20,21,24,36,41,43,49,81 Attention to prioritise the improvement of quality of care in health facilities was described.17,19–21,27,28,30,39,77,78,81 Addressing systemic barriers requires considering the socio-cultural contexts of women while designing and providing care.17–19,33,39,77
Similarly, investment should be made to increase access to SBA and female care providers18,19,21,24,26,35,41,43,49 with parallel efforts to enable women’s access to education, services and economic opportunities.17–19,21,26,35,39,79,81
Several studies argued for improved leadership, commitment and accountability at the government level in order to improve the infrastructure, human resources, social capital and equitable coverage of services.17,24,26,35,49,79
The need for additional and continuing training and access to educational resources for health care providers about respectful maternity care was described as a crucial priority.21,34,35,43,81 It was also recommended to involve women, families and communities in health service planning, policy development, service delivery and other decision-making process.17,18,21,33,38,40,41,43
Discussion
The findings of this scoping review draw voices of women, health care professionals, family members and other stakeholders to explore the current practice, facilitators, barriers and policy implications of providing respectful maternity care in South Asian countries. The review found consistent negative experiences of abuse, neglect and disrespect in institutional settings.
Emerging themes captured the experiences of women during pregnancy and childbirth and described the critical complexities of maintaining quality of care within often resource-limited circumstances. Health care providers felt unable to adhere with the norms of providing respectful maternity care to women due to gaps in their own knowledge and skills, resources, institutional supports, policy direction and clinical guidelines.
Vulnerable women and marginalised families experienced higher levels of abuse and discrimination while coming to hospital to receive care. Given the focus of maternity care now is on women centred model where decisions are made valuing the choices and preference that women make,82–87 this puts women at further risks of marginalisation and raises a serious human rights issue of receiving equitable, quality and respectful care.
Studies in our review consistently described women avoiding institutional pregnancy care due to the fear of being misjudged, mistreated and abused in health care settings. Studies described examples of women lacking agency in decision-making processes about their care, where their choices or preferences were dismissed by the professionals who took control of the birthing process. This suggests a medical domination of care and oppression of women seeking care when fight to survival is critical. The impact of choice and control on women’s childbirth experiences to determine safety has been consistently discussed from the perspective of giving power back to women to decide where and how they would like to give birth.88–92 However, a lack of trust in health care provision was described where women had a fear of being victimised by their behaviour and actions. While hospitals took actions to ensure the physical safety of women and the newborn, the emotional safety of women needs further attention.93,94
Social, economic and cultural differences all played influential roles in the experience and provision of care. When women found providers shared similar cultural and religious backgrounds, their experiences of receiving care were typically positive. Similarly, influences of families, friends, neighbours and community-based lay care providers helped women to feel safe, supported and well looked after. The critical role that socio-economic factors play in determining pregnancy and birth outcomes has been the ongoing challenge for disadvantaged settings where maternal and perinatal mortality is still high.95–99 The findings of this review strongly emphasise the significance of involving women, families, communities and service providers from the similar backgrounds to design and deliver culturally appropriate model of care.
The notion of care that women want and need to experience respectful maternity care in South Asia aligns well with the concept of collaborative care that many countries adopted to provide responsive services to their diverse and culturally rich community settings.100–105 This review reaffirms that enforcing respectful maternity care practice in South Asia requires systematic actions across all levels of health care system. Health care providers mostly agreed on the principles and necessity of providing respectful maternity care, however it was often described as impractical in the current health system, social practice, institutional resources and policy environment. Other studies confirm that without taking appropriate policy actions, the challenges that each country is facing to ensure the safe pregnancy and birth outcomes will remain longer and women from diverse social and cultural backgrounds will continue face the barriers of accessing respectful and quality maternity care.106–111
In the context of limited supplies of resources including basic medicine, equipment, staff and lower benefits to the midwives providing care, maintaining welcoming hospital environment and providing quality care to women was considered not possible.
Strengths and Limitations
There is a lack of evidence to understand the current practice of respectful maternity care as a region in South Asia and the significance of enabling the respectful approach to ensure quality of care has not yet got enough attention. This review used a rigorous method for gathering evidence, synthesising data and assessing the validity of findings. The barriers and enablers drawn from experiences of women and others involved in providing care can be instrumental to strengthen relevant policies and respectful maternity care practice across the countries.
These findings cannot be generalised in all contexts of pregnancy, childbirth and postnatal experiences even in South Asia, as the culture, social and structural issues that women experience differ from one place to another. Given that most studies focused on health facility-based experiences from urban and semi-urban settings, there is a lack of insight specific to remote dwelling and other women who are disproportionately affected by social and health inequities. There were no studies found that that met the inclusion criteria from the Maldives, and limited information from Bhutan; thus, insights from these countries are limited and call for resourced research.
Our review focused on respectful maternity care within the context of health services: we acknowledge other factors that profoundly impact on decision-making, childbirth experience and maternal outcomes, particularly familial norms associated with husband and mothers-in-law relations, which in turn is mediated by gender equity (including intimate partner and in-law violence) and social determinants such as economic status and education.112–117
Conclusion
The provision of respectful maternity care is an imperative factor in supporting improved maternal and perinatal outcomes. Concerns and principles that challenge the provision of RMC in South Asian nations are associated with resource-challenged environments (particularly in rural settings), gender equity, educational status, health workforce awareness, education and resourcing, culture, economy and other social determinants. Many of these factors are consistent with other settings; however, they are experienced and expressed diversely in South Asian contexts related to the specific characteristics of individual countries, cultures, and economies.
Sustained improvements in RMC demand strong policy actions, political will and appropriate well-funded programs to provide a well-educated and adequately resourced health workforce and counter economic disadvantage and gender inequities, privileging women’s choices and preferences.
Ethical Approval
Not applicable for review article.
Funding
No funding received.
Disclosure
The authors report no conflicts of interest in relation to this work.
References
1. Howell EA. Reducing disparities in severe maternal morbidity and mortality. Clin Obstet Gynecol. 2018;61(2):387–399. doi:10.1097/GRF.0000000000000349
2. Miller S, Abalos E, Chamillard M, et al. Beyond too little, too late and too much, too soon: a pathway towards evidence-based, respectful maternity care worldwide. Lancet. 2016;388(10056):2176–2192. doi:10.1016/S0140-6736(16)31472-6
3. Kaphle S, Hancock H, Newman LA. Childbirth traditions and cultural perceptions of safety in Nepal: critical spaces to ensure the survival of mothers and newborns in remote mountain villages. Midwifery. 2013;29(10):1173–1181. doi:10.1016/j.midw.2013.06.002
4. Kaphle S, Newman L. Critical social determinants of childbirth outcomes in remote mountains: voices of women from Nepal. J Asian Midwives. 2020;7(2):16–32.
5. Afulani PA, Moyer CA. Accountability for respectful maternity care. Lancet. 2019;394(10210):1692–1693. doi:10.1016/S0140-6736(19)32258-5
6. Hossain J, Laterra A, Paul RR, Islam A, Ahmmed F, Sarker BK. Filling the human resource gap through public-private partnership: can private, community-based skilled birth attendants improve maternal health service utilization and health outcomes in a remote region of Bangladesh? PLoS One. 2020;15(1):e0226923. doi:10.1371/journal.pone.0226923
7. Woldegiorgis MA, Hiller J, Mekonnen W, Meyer D, Bhowmik J. Determinants of antenatal care and skilled birth attendance in sub‐Saharan Africa: a multilevel analysis. Health Serv Res. 2019;54(5):1110–1118. doi:10.1111/1475-6773.13163
8. Sacks E, Kinney MV. Respectful maternal and newborn care: building a common agenda. Reprod Health. 2015;12(1):1–4. doi:10.1186/s12978-015-0042-7
9. Freedman LP, Ramsey K, Abuya T, et al. Defining disrespect and abuse of women in childbirth: a research, policy and rights agenda. Bull World Health Organ. 2014;92:915–917. doi:10.2471/BLT.14.137869
10. Bohren MA, Vogel JP, Hunter EC, et al. The mistreatment of women during childbirth in health facilities globally: a mixed-methods systematic review. PLoS Med. 2015;12(6):e1001847. doi:10.1371/journal.pmed.1001847
11. Mannava P, Durrant K, Fisher J, Chersich M, Luchters S. Attitudes and behaviours of maternal health care providers in interactions with clients: a systematic review. Global Health. 2015;11:36. doi:10.1186/s12992-015-0117-9
12. Ansari H, Yeravdekar R. Respectful maternity care during childbirth in India: a systematic review and meta-analysis. J Postgrad Med. 2020;66(3):133–140. doi:10.4103/jpgm.JPGM_648_19
13. Alliance WR. Respectful maternity care charter: universal rights of mothers and newborns. WRA. Available from: https://www.whiteribbonalliance.org/respectful-maternity-care-charter/.
14. White Ribbon Alliance. Pulling Back the Curtain on Disrespect and Abuse: The Movement to Ensure Respectful Maternity Care. Washington, DC: WRA; 2015.
15. Peters MDJ GC, McInerney P, Munn Z, Tricco AC, Khalil H. Chapter 11: scoping Reviews (2021 version). In: Aromataris EMZ, editor. JBI Manual for Evidence Synthesis; 2021. doi:10.46658/JBIMES-20-12
16. Tricco AC, Lillie E, Zarin W, et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): checklist and explanation. Ann Intern, Med. 2018;169:467–473. doi:10.7326/M18-0850
17. Adamson PC, Krupp K, Niranjankumar B, Freeman AH, Khan M, Madhivanan P. Are marginalized women being left behind? A population-based study of institutional deliveries in Karnataka, India. BMC Public Health. 2012;12(1):30. doi:10.1186/1471-2458-12-30
18. Akter S, Davies K, Rich JL, Inder KJ. Barriers to accessing maternal health care services in the Chittagong Hill Tracts, Bangladesh: a qualitative descriptive study of Indigenous women’s experiences. PLoS One. 2020;15(8):e0237002. doi:10.1371/journal.pone.0237002
19. Alcock G, Das S, More NS, et al. Examining inequalities in uptake of maternal health care and choice of provider in underserved urban areas of Mumbai, India: a mixed methods study. BMC Pregnancy Childbirth. 2015;15(1):1–11. doi:10.1186/s12884-015-0661-6
20. Arnold R, van Teijlingen E, Ryan K, Holloway I. Parallel worlds: an ethnography of care in an Afghan maternity hospital. Soc Sci Med. 2018;216:33–40. doi:10.1016/j.socscimed.2018.09.010
21. Arnold R, van Teijlingen E, Ryan K, Holloway I. Villains or victims? An ethnography of Afghan maternity staff and the challenge of high quality respectful care. BMC Pregnancy Childbirth. 2019;19(1):307. doi:10.1186/s12884-019-2420-6
22. Atif N, Lovell K, Husain N, Sikander S, Patel V, Rahman A. Barefoot therapists: barriers and facilitators to delivering maternal mental health care through peer volunteers in Pakistan: a qualitative study. Article. Int J Ment Health Syst. 2016;10(1). doi:10.1186/s13033-016-0055-9
23. Atif N, Nazir H, Zafar S, et al. Development of a psychological intervention to address anxiety during pregnancy in a low-income country. Front Psychiatry. 2020;10. doi:10.3389/fpsyt.2019.00927
24. Awasthi MS, Awasthi KR, Thapa HS, Saud B, Pradhan S, Khatry RA. Utilization of antenatal care services in dalit communities in Gorkha, Nepal: a cross-sectional study. J Pregnancy. 2018;2018:3467308. doi:10.1155/2018/3467308
25. Azhar Z, Oyebode O, Masud H. Disrespect and abuse during childbirth in district Gujrat, Pakistan: a quest for respectful maternity care. PLoS One. 2018;13(7):e0200318. doi:10.1371/journal.pone.0200318
26. Baral YR, Skinner J, van Teijlingen E, Lyons K. The uptake of skilled birth attendants’ services in rural Nepal: a qualitative study. J Asian Midwives. 2016;3(2):7–25.
27. Bhattacharyya S, Srivastava A, Avan BI. Delivery should happen soon and my pain will be reduced: understanding women’s perception of good delivery care in India. Glob Health Action. 2013;6:22635. doi:10.3402/gha.v6i0.22635
28. Bhattacharyya S, Issac A, Rajbangshi P, Srivastava A, Avan BI. “Neither we are satisfied nor they”-users and provider’s perspective: a qualitative study of maternity care in secondary level public health facilities, Uttar Pradesh, India. BMC Health Serv Res. 2015;15(1):1–13. doi:10.1186/s12913-015-1077-8
29. Bhattacharya S, Sundari Ravindran TK. Silent voices: institutional disrespect and abuse during delivery among women of Varanasi district, northern India. BMC Pregnancy Childbirth. 2018;18(1):338. doi:10.1186/s12884-018-1970-3
30. Bhattacharyya S, Srivastava A, Saxena M, Gogoi M, Dwivedi P, Giessler K. Do women’s perspectives of quality of care during childbirth match with those of providers? A qualitative study in Uttar Pradesh, India. Glob Health Action. 2018;11(1):1. doi:10.1080/16549716.2018.1527971
31. Bogren M, Erlandsson K, Byrskog U. What prevents midwifery quality care in Bangladesh? A focus group enquiry with midwifery students. BMC Health Serv Res. 2018;18(1):
32. Cederfeldt J, Carlsson J, Begley C, Berg M. Quality of intra-partum care at a university hospital in Nepal: a prospective cross-sectional survey. Sex Reprod Healthc. 2016;7:52–57. doi:10.1016/j.srhc.2015.11.004
33. Chattopadhyay S, Mishra A, Jacob S. “Safe”, yet violent? Women’s experiences with obstetric violence during hospital births in rural Northeast India. Cult Health Sex. 2018;20(7):815–829. doi:10.1080/13691058.2017.1384572
34. Devkota HR, Murray E, Kett M, Groce N. Healthcare provider’s attitude towards disability and experience of women with disabilities in the use of maternal healthcare service in rural Nepal. Reprod Health. 2017;14(1). doi:10.1186/s12978-017-0330-5
35. Devkota HR, Murray E, Kett M, Groce N. Are maternal healthcare services accessible to vulnerable group? A study among women with disabilities in rural Nepal. PLoS One. 2018;13(7):e0200370. doi:10.1371/journal.pone.0200370
36. Devkota HR, Kett M, Groce N. Societal attitude and behaviours towards women with disabilities in rural Nepal: pregnancy, childbirth and motherhood. BMC Pregnancy Childbirth. 2019;19(1):20. doi:10.1186/s12884-019-2171-4
37. Dey A, Baker Shakya H, Chandurkar D, et al. Discordance in self-report and observation data on mistreatment of women by providers during childbirth in Uttar Pradesh, India. Reprod Health. 2017;14:1–13. doi:10.1186/s12978-017-0409-z
38. Diamond-Smith N, Sudhinaraset M, Melo J, Murthy N. The relationship between women’s experiences of mistreatment at facilities during childbirth, types of support received and person providing the support in Lucknow, India. Midwifery. 2016;40:114–123. doi:10.1016/j.midw.2016.06.014
39. Diamond-Smith N, Treleaven E, Murthy N, Sudhinaraset M. Women’s empowerment and experiences of mistreatment during childbirth in facilities in Lucknow, India: results from a cross-sectional study. BMC Pregnancy Childbirth. 2017;17(Suppl 2):335. doi:10.1186/s12884-017-1501-7
40. Dorairajan G, Gopalakrishnan V, Chinnakali P, Balaguru S. Experiences and felt needs of women during childbirth in a tertiary care center: a hospital-based cross-sectional descriptive study. J Obstet Gynecol India. 2020. doi:10.1007/s13224-020-01359-9
41. Dorji T, Das M, Van den Bergh R, et al. “If we miss this chance, it’s futile later on” - late antenatal booking and its determinants in Bhutan: a mixed-methods study. BMC Pregnancy Childbirth. 2019;19(1):
42. Dynes M, Rahman A, Beck D, et al. Home-based life saving skills in Matlab, Bangladesh: a process evaluation of a community-based maternal child health programme. Midwifery. 2011;27(1):15–22. doi:10.1016/j.midw.2009.07.009
43. Erlandsson K, Sayami JT, Sapkota S. Safety before comfort: a focused enquiry of Nepal skilled birth attendants’ concepts of respectful maternity care. Evid Based Midwifery. 2014;12(2):59–64.
44. Hameed W, Avan BI. Women’s experiences of mistreatment during childbirth: a comparative view of home- and facility-based births in Pakistan. PLoS One. 2018;13(3):e0194601. doi:10.1371/journal.pone.0194601
45. Herath INS, Balasuriya A, Sivayogan S. Physical and psychological morbidities among selected antenatal females in Kegalle district of Sri Lanka: a cross sectional study. J Obstet Gynaecol. 2017;37(7):849–854. doi:10.1080/01443615.2017.1306697
46. Infanti JJ, Lund R, Muzrif MM, Schei B, Wijewardena K. Addressing domestic violence through antenatal care in Sri Lanka’s plantation estates: contributions of public health midwives. Soc Sci Med. 2015;145:35–43. doi:10.1016/j.socscimed.2015.09.037
47. Infanti JJ, Zbikowski A, Wijewardene K, Swahnberg K. Feasibility of participatory theater workshops to increase staff awareness of and readiness to respond to abuse in health care: a qualitative study of a pilot intervention using forum play among Sri Lankan health care providers. Int J Environ Res Public Health. 2020;17(20):1–14. doi:10.3390/ijerph17207698
48. Khan R, Blum LS, Sultana M, Bilkis S, Koblinsky M. An examination of women experiencing obstetric complications requiring emergency care: perceptions and sociocultural consequences of caesarean sections in Bangladesh. J Health Popul Nutr. 2012;30(2):159–171. doi:10.3329/jhpn.v30i2.11309
49. Khatri RB, Dangi TP, Gautam R, Shrestha KN, Homer CSE. Barriers to utilization of childbirth services of a rural birthing center in Nepal: a qualitative study. PLoS One. 2017;12(5):e0177602. doi:10.1371/journal.pone.0177602
50. Maharjan B, Rishal P, Svanemyr J. Factors influencing the use of reproductive health care services among married adolescent girls in Dang District, Nepal: a qualitative study. BMC Pregnancy Childbirth. 2019;19(1):
51. Maheen H, Hoban E, Bennett C. Factors affecting rural women’s utilisation of continuum of care services in remote or isolated villages or Pakistan – a mixed-methods study. Women Birth. 2020;34:257–265. doi:10.1016/j.wombi.2020.04.001
52. McNojia SZ, Saleem S, Feroz A, et al. Exploring women and traditional birth attendants’ perceptions and experiences of stillbirths in district Thatta, Sindh, Pakistan: a qualitative study. Reprod Health. 2020;17(1):3. doi:10.1186/s12978-020-0852-0
53. Mehata S, Paudel YR, Dariang M, et al. Factors determining satisfaction among facility-based maternity clients in Nepal. BMC Pregnancy Childbirth. 2017;17(1):319. doi:10.1186/s12884-017-1532-0
54. Milne L, van Teijlingen E, Hundley V, Simkhada P, Ireland J. Staff perspectives of barriers to women accessing birthing services in Nepal: a qualitative study. BMC Pregnancy Childbirth. 2015;15:142. doi:10.1186/s12884-015-0564-6
55. Montagu D, Landrian A, Kumar V, et al. Patient-experience during delivery in public health facilities in Uttar Pradesh, India. Health Policy Plan. 2019;34(8):574–581. doi:10.1093/heapol/czz067
56. Morrison J, Basnet M, Budhathoki B, et al. Disabled women’s maternal and newborn health care in rural Nepal: a qualitative study. Midwifery. 2014;30(11):1132–1139. doi:10.1016/j.midw.2014.03.012
57. Panday S, Bissell P, Teijlingen EV, Simkhada P. Perceived barriers to accessing Female Community Health Volunteers’ (FCHV) services among ethnic minority women in Nepal: a qualitative study. PLoS One. 2019;14(6):e0217070. doi:10.1371/journal.pone.0217070
58. Panth A, Kafle P. Maternal satisfaction on delivery service among postnatal mothers in a government hospital, Mid-Western Nepal. Obstet Gynecol Int. 2018;1–11. doi:10.1155/2018/4530161
59. Pathak P, Ghimire B. Perception of women regarding respectful maternity care during facility-based childbirth. Obstet Gynecol Int. 2020;2020:1–8. doi:10.1155/2020/5142398
60. Paudel M, Javanparast S, Newman L, Dasvarma G. Health system barriers influencing perinatal survival in mountain villages of Nepal: implications for future policies and practices. J Health Popul Nutr. 2018;37(1):16. doi:10.1186/s41043-018-0148-y
61. Perera D, Lund R, Swahnberg K, Schei B, Infanti JJ; on behalf of the Ast. When helpers hurt’: women’s and midwives’ stories of obstetric violence in state health institutions, Colombo district, Sri Lanka. BMC Pregnancy Childbirth. 2018;18(1):
62. Senanayake H, Wijesinghe RD, Nayar KR. Is the policy of allowing a female labor companion feasible in developing countries? Results from a cross sectional study among Sri Lankan practitioners. BMC Pregnancy Childbirth. 2017;17(1). doi:10.1186/s12884-017-1578-z
63. Shahabuddin A, Delvaux T, Nöstlinger C, et al. Maternal health care-seeking behaviour of married adolescent girls: a prospective qualitative study in Banke District, Nepal. PLoS One. 2019;14(6):e0217968. doi:10.1371/journal.pone.0217968
64. Sharma G, Penn-Kekana L, Halder K, Filippi V. An investigation into mistreatment of women during labour and childbirth in maternity care facilities in Uttar Pradesh, India: a mixed methods study. Reprod Health. 2019;16(1):7. doi:10.1186/s12978-019-0668-y
65. Subramaniyan A, Sarkar S, Roy G, Lakshminarayanan S. Experiences of HIV positive mothers from rural South India during intra-natal period. J Clin Diagn Res. 2013;7(10):2203–2206. doi:10.7860/JCDR/2013/5782.3471
66. Sudhinaraset M, Treleaven E, Melo J, Singh K, Diamond-Smith N. Women’s status and experiences of mistreatment during childbirth in Uttar Pradesh: a mixed methods study using cultural health capital theory. BMC Pregnancy Childbirth. 2016;16(1):332. doi:10.1186/s12884-016-1124-4
67. Sudhinaraset M, Beyeler N, Barge S, Diamond-Smith N. Decision-making for delivery location and quality of care among slum-dwellers: a qualitative study in Uttar Pradesh, India. BMC Pregnancy Childbirth. 2016;16:148. doi:10.1186/s12884-016-0942-8
68. Swahnberg K, Zbikowski A, Wijewardene K, et al. Can forum play contribute to counteracting abuse in health care? A pilot intervention study in Sri Lanka. Int J Environ Res Public Health. 2019;16(9):1616. doi:10.3390/ijerph16091616
69. Taleb F, Perkins J, Ali NA, et al. Transforming maternal and newborn health social norms and practices to increase utilization of health services in rural Bangladesh: a qualitative review. BMC Pregnancy Childbirth. 2015;15:75. doi:10.1186/s12884-015-0501-8
70. Thapa P, Bangura AH, Nirola I, et al. The power of peers: an effectiveness evaluation of a cluster-controlled trial of group antenatal care in rural Nepal. Reprod Health. 2019;16(1):150. doi:10.1186/s12978-019-0820-8
71. Thommesen T, Kismul H, Kaplan I, Safi K, Van den Bergh G. “The midwife helped me … otherwise I could have died”: women’s experience of professional midwifery services in rural Afghanistan - a qualitative study in the provinces Kunar and Laghman. BMC Pregnancy Childbirth. 2020;20(1):140. doi:10.1186/s12884-020-2818-1
72. Varghese B, Roy R, Saha S, Roalkvam S. Fostering maternal and newborn care in India the Yashoda way: does this improve maternal and newborn care practices during institutional delivery? Article. PLoS One. 2014;9(1):e84145. doi:10.1371/journal.pone.0084145
73. Wahlström S, Björklund M, Munck B. The professional role of skilled birth attendants’ in Nepal – a phenomenographic study. Sexual Reprod Healthcare. 2019;21:60–66. doi:10.1016/j.srhc.2019.05.003
74. Waqas A, Zubair M, Zia S, et al. Psychosocial predictors of antenatal stress in Pakistan: perspectives from a developing country. BMC Res Notes. 2020;13(1):160. doi:10.1186/s13104-020-05007-3
75. Wickramasinghe SA, Gunathunga MW, Hemachandra D. Client perceived quality of the postnatal care provided by public sector specialized care institutions following a normal vaginal delivery in Sri Lanka: a cross sectional study. BMC Pregnancy Childbirth. 2019;19(1):485. doi:10.1186/s12884-019-2645-4
76. Iftikhar Ul Husnain M, Rashid M, Shakoor U. Decision-making for birth location among women in Pakistan: evidence from national survey. BMC Pregnancy Childbirth. 2018;18(1):226. doi:10.1186/s12884-018-1844-8
77. Khan MA, Mirza S, Ahmed M, et al. Making birthing safe for Pakistan women: a cluster randomized trial. BMC Pregnancy Childbirth. 2012;12:67. doi:10.1186/1471-2393-12-67
78. Bhattacharyya S, Srivastava A, Roy R, Avan BI. Factors influencing women’s preference for health facility deliveries in Jharkhand state, India: a cross sectional analysis. BMC Pregnancy Childbirth. 2016;16:1–9. doi:10.1186/s12884-016-0839-6
79. Smith BM, Duncan FE, Ataman L, et al. The national physicians cooperative: transforming fertility management in the cancer setting and beyond. Future Oncol. 2018;14(29):3059–3072. doi:10.2217/fon-2018-0278
80. Arambepola C, Rajapaksa LC, Galwaduge C. Usual hospital care versus post-abortion care for women with unsafe abortion: a case control study from Sri Lanka. BMC Health Serv Res. 2014;14:470. doi:10.1186/1472-6963-14-470
81. Bhatnagar N, Khandekar J, Singh A, Saxena S. The silent epidemic of reproductive morbidity among ever married women (15–49 years) in an urban area of Delhi. J Community Health. 2013;38(2):250–256. doi:10.1007/s10900-012-9607-3
82. Berg M, Olafsdottir O, Lundgren I. A midwifery model of woman-centred childbirth care - In Swedish and Icelandic settings. Sex Reprod Healthc. 2012;3:79–87. doi:10.1016/j.srhc.2012.03.001
83. Gebreyesus SH, Endris BS, Hanlon C, Lindtjørn B. Maternal depression symptoms are highly prevalent among food-insecure households in Ethiopia. Public Health Nutr. 2018;21(5):849–856. doi:10.1017/s1368980017003056
84. Hunter A, Devane D, Houghton C, Grealish A, Tully A, Smith V. Woman-centred care during pregnancy and birth in Ireland: thematic analysis of women’s and clinicians’ experiences. BMC Pregnancy Childbirth. 2017;17:322. doi:10.1186/s12884-017-1521-3
85. Leap N. Woman-centred or women-centred care: does it matter? Br J Midwifery. 2009;17:12–16. doi:10.12968/bjom.2009.17.1.37646
86. Maputle S. A woman-centred childbirth model. Health SA Gesondheid. 2010;15. doi:10.4102/hsag.v15i1.450
87. Maputle MS, Donavon H. Woman-centred care in childbirth: a concept analysis (Part 1). Curationis. 2013;36(1). doi:10.4102/curationis.v36i1.49
88. Cook K, Loomis C. The impact of choice and control on women’s childbirth experiences. J Perinat Educ. 2012;21(3):158–168. doi:10.1891/1058-1243.21.3.158
89. Jomeen J. Choice, Control and Contemporary Childbirth: Understanding Through Women’s Stories. Radcliffe Publishing; 2010.
90. Malacrida C, Boulton T. Women’s perceptions of childbirth “choices”. Gender Society. 2012;26(5):748–772. doi:10.1177/0891243212452630
91. Meyer S. Control in childbirth: a concept analysis and synthesis. J Adv Nurs. 2012;69:218–228. doi:10.1111/j.1365-2648.2012.06051.x
92. Snowden A, Martin C, Jomeen J, Hollins Martin C. Concurrent analysis of choice and control in childbirth. BMC Pregnancy Childbirth. 2011;11:40. doi:10.1186/1471-2393-11-40
93. Dejong J, Akik C, El-Kak F, Osman H, El-Jardali F. The safety and quality of childbirth in the context of health systems: mapping maternal health provision in Lebanon. Midwifery. 2010;26:549–557. doi:10.1016/j.midw.2010.06.012
94. Lothian JA. Risk, safety, and choice in childbirth. J Perinat Educ. 2012;21(1):45–47. doi:10.1891/1058-1243.21.1.45
95. Blumenshine P, Egerter S, Barclay C, Cubbin C, Braveman P. Socioeconomic disparities in adverse birth outcomes: a systematic review. Am J Prev Med. 2010;39:263–272. doi:10.1016/j.amepre.2010.05.012
96. Campbell E, Gilliland J, Dworatzek P, Vrijer B, Penava D, Seabrook J. Socioeconomic status and adverse birth outcomes: a population-based Canadian sample. J Biosoc Sci. 2017;50:1–12. doi:10.1017/S0021932017000062
97. Dominguez TP. Adverse birth outcomes in African American women: the social context of persistent reproductive disadvantage. Soc Work Public Health. 2011;26(1):3–16. doi:10.1080/10911350902986880
98. Magadi M, Madise N, Diamond I. Factors associated with unfavourable birth outcomes in Kenya. J Biosoc Sci. 2001;33:199–225. doi:10.1017/S0021932001001997
99. Meng G, Thompson M, Hall G. Pathways of neighbourhood-level socio-economic determinants of adverse birth outcomes. Int J Health Geogr. 2013;12:32. doi:10.1186/1476-072X-12-32
100. Downe S, Finlayson K, Fleming A. Creating a collaborative culture in maternity care. J Midwifery Women’s Health. 2010;55:250–254. doi:10.1016/j.jmwh.2010.01.004
101. Harris S, Janssen P, Saxell L, Carty E, Macrae G, Petersen K. Effect of a collaborative interdisciplinary maternity care program on perinatal outcomes. CMAJ. 2012;184(17):1885–1892. doi:10.1503/cmaj.111753
102. Kaphle S. Socio-Cultural Insights of Childbirth in South Asia: Stories of Women in the Himalayas. Routledge; 2021.
103. Kermode M, Morgan A, Nyagero J, et al. Walking together: towards a collaborative model for maternal health care in pastoralist communities of Laikipia and Samburu, Kenya. Matern Child Health J. 2017;21(10):1867–1873. doi:10.1007/s10995-017-2337-5
104. Pecci C, Mottl-Santiago J, Culpepper L, Heffner L, McMahan T, Lee-Parritz A. The birth of a collaborative model obstetricians, midwives, and family physicians. Obstet Gynecol Clin North Am. 2012;39:323–334. doi:10.1016/j.ogc.2012.05.001
105. Vogt SE, Silva K, Dias MAB. Comparison of childbirth care models in public hospitals, Brazil. Rev Saude Publica. 2014;48(2):304–313. doi:10.1590/s0034-8910.2014048004633
106. Barclay L, Kornelsen J, Longman J, et al. Reconceptualising risk: perceptions of risk in rural and remote maternity service planning. Midwifery. 2016;38:63–70. doi:10.1016/j.midw.2016.04.007
107. Douglas V. The Rankin Inlet birthing centre: community midwifery in the Inuit context. Int J Circumpolar Health. 2011;70:178–185. doi:10.3402/ijch.v70i2.17803
108. Kildea S, Hickey S, Barclay L, et al. Implementing birthing on country services for aboriginal and torres strait islander families: RISE framework. Women Birth. 2019;32(5):466–475. doi:10.1016/j.wombi.2019.06.013
109. Kildea S, Hickey S, Nelson C, et al. Birthing on Country (in Our Community): a case study of engaging stakeholders and developing a best-practice Indigenous maternity service in an urban setting. Aust Health Rev. 2018;42(2):230–238. doi:10.1071/ah16218
110. Olson R, Couchie C. Returning birth: the politics of midwifery implementation on First Nations reserves in Canada. Midwifery. 2013;29(8):981–987. doi:10.1016/j.midw.2012.12.005
111. Roe Y, Briggs M, Buzzcott C, Hartz DL, Sherwood J, Kildea S. Returning birthing services to communities and Aboriginal control: aboriginal women of Shoalhaven Illawarra region describe how Birthing on Country is linked to healing. J Indig Wellbeing. 2020;5:58–71.
112. Sapkota S, Kobayashi T, Kakehashi M, Baral G, Yoshida I. In the Nepalese context, can a husband’s attendance during childbirth help his wife feel more in control of labour? BMC Pregnancy Childbirth. 2012;12(1):49. doi:10.1186/1471-2393-12-49
113. Sapkota S, Kobayashi T, Takase M. Impact on perceived postnatal support, maternal anxiety and symptoms of depression in new mothers in Nepal when their husbands provide continuous support during labour. Midwifery. 2013;29(11):1264–1271. doi:10.1016/j.midw.2012.11.010
114. Simkhada B, Porter MA, van Teijlingen ER. The role of mothers-in-law in antenatal care decision-making in Nepal: a qualitative study. BMC Pregnancy Childbirth. 2010;10(1):34. doi:10.1186/1471-2393-10-34
115. Hodnett ED, Gates S, Hofmeyr GJ, Sakala C, Weston J. Continuous support for women during childbirth. Cochrane Database Syst Rev. 2011;(2):Cd003766. doi:10.1002/14651858.CD003766.pub3
116. Lewis S, Lee A, Simkhada P. The role of husbands in maternal health and safe childbirth in rural Nepal: a qualitative study. BMC Pregnancy Childbirth. 2015;15(1):162. doi:10.1186/s12884-015-0599-8
117. WHO, UNICEF, UNFPA, World Bank Group, and the United Nations Population Divisions. Trends in Maternal Mortality: 2000 to 2017. Geneva: World Health Organisation; 2019.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.