Back to Journals » Psychology Research and Behavior Management » Volume 15
Resilience Among Residents from the Areas First Affected by COVID-19 in South Korea
Received 1 March 2022
Accepted for publication 9 April 2022
Published 22 April 2022 Volume 2022:15 Pages 1033—1041
DOI https://doi.org/10.2147/PRBM.S364323
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Eunhee Nam,1 Yujeong Kim2
1College of Nursing, Kyungpook National University, Daegu, Republic of Korea; 2College of Nursing, Research Institute of Nursing Science, Kyungpook National University, Daegu, Republic of Korea
Correspondence: Yujeong Kim, College of Nursing, Research Institute of Nursing Science, Kyungpook National University, 680 Gukchabosangro, Jung-gu, Daegu, 41944, Republic of Korea, Tel +82-53-420-4921, Fax +82-53-425-1258, Email [email protected]
Purpose: This study aimed to identify the factors affecting the resilience of residents of South Korea, from areas where the coronavirus disease of 2019 outbreak first occurred.
Methods: A cross-sectional design was used, with a convenience sample of 212 residents from Daegu and Gyeongbuk, areas that were first affected by COVID-19 in South Korea. Data were collected through a structured self-administered survey from September 3 to September 5, 2020. The questionnaire included general characteristics, post-traumatic stress, perceived health status, family history, and resilience. The data were analyzed using descriptive analysis, t-test, ANOVA, Pearson’s correlation coefficient, and multiple linear regression.
Results: Resilience was correlated with post-traumatic stress, perceived health status, and family hardiness. Factors influencing resilience were family hardiness, economic status, and residence.
Conclusion: There is a need for strategies and intervention programs that aim to improve family resilience and reduce the impact of economic losses caused by pandemics.
Keywords: COVID-19, resilience, post-traumatic stress, family relations, disease outbreaks
Introduction
The coronavirus disease of 2019 (COVID-19), a respiratory infection caused by severe acute respiratory syndrome coronavirus 2, has spread across the globe since its initial outbreak in Wuhan, China, in December 2019.1 In South Korea, the first COVID-19 case was confirmed in January 2020, and the first wave originated from two places. One was a religious organization in Daegu and the other was a hospital in Gyeongbuk.2 With 5279 and 969 confirmed cases in Daegu and Gyeongbuk, respectively, as of March 15, 2020, these two regions were declared special disaster areas in relation to COVID-19.3
A novel infectious disease triggers a greater stress response in individuals, than what is experienced daily and may result in mood disorders, such as depression and anxiety.4 According to a national survey, exploring the mental health of people during the COVID-19 pandemic, performed on 1500 Koreans in April 2020,5 the level of stress caused by COVID-19 was 1.5 times higher than the stress caused during the Middle East Respiratory Syndrome (MERS) outbreak. In particular, 65.3% and 47.2% of the residents from Daegu and Gyeongbuk, respectively, were found to suffer from anxiety.5
However, resilience helps to overcome such stressful events.6 According to the research,7 resilience refers to the ability to respond flexibly to stressful environmental or situational demands based on appropriate self-regulation and successful adaptation to the environment. Low resilience hinders a person’s ability to adapt to a changing environment, this emphasizes its importance. Therefore, the level of resilience and its predictors among residents of Daegu and Gyeongbuk need to be investigated to develop prompt interventions for people facing similar situations in the future.
Bonanno8 identified four factors of resilience: severity of exposure, individual factors, family factors, and community features. In this study, variables falling under each factor was selected through an extensive literature review. In relation to severity of exposure, prolonged or severe exposure to a traumatic event can lead to mental disorders, like post-traumatic stress disorder (PTSD).9 PTSD can be understood as the mental and physical symptoms experienced after being exposed to a disaster or shocking event, such as physical injuries and death.10 Regarding the relationship between infectious diseases and PTSD, nurses who provided care for patients with SARS displayed a higher level of PTSD than nurses who did not.11 Patients involved in disaster-related or industrial accidents had lower resilience with increasing levels of post-traumatic stress,10 suggesting that PTSD from a disaster influences resilience. As Daegu and Gyeongbuk were impacted by the first wave of COVID-19 in South Korea and are still battling the virus, residents of these regions may suffer from more severe PTSD symptoms than those from other regions.
An example of a variable this study considers as part of the individual factors is perceived health status, which represents the subjective level of one’s health.12 Studies on disaster victims reported that residents of a region affected by the sinking of a passenger ship showed poorer perceived health after the accident than before the accident.13 Another study found that older adults with better perceived health, who engage in physical activity are more resilient than those who do not.14 These findings suggest that perceived health status can affect a person’s level of resilience.
Family hardiness is an example of a variable that falls under the family factors and includes resistance to family stress, resources for adjustment, and learning abilities pertaining to new experiences.15 Studies on patients with breast cancer16 and gynecological cancer17 observed that patients with greater family hardiness were more resilient, highlighting the relationship between the two elements.
In terms of community features, previous studies have explored the relationship between the variables of community and disaster. For instance, students living in New York, who were affected by the 9/11 terrorist attacks suffered double the level of PTSD than their counterparts in other areas.18 Ozbay et al19 reported that people with more social support are able to maintain better physical and mental health with a greater ability to recover from stress. These findings suggest that community systems or policies affect individuals’ resilience.
Therefore, this study aimed to identify the influence of post-traumatic stress disorder, perceived health status, and family hardiness on resilience among residents in the areas first affected by the COVID-19 outbreak in South Korea. Through this study, we intend to prepare basic data for establishing a program that can enhance the resilience of community residents in a similar disaster situation.
Methods
Study Design
This study used a cross-sectional survey to investigate the relationships between variables such as PTSD, perceived health status, family strength, and resilience among residents in the areas first affected by the COVID-19 outbreak in South Korea. The STROBE guidelines for observational research were followed in the reporting of this study.
Participants
Adults aged 19–64 years who lived in the Daegu or Gyeongbuk regions from January 2020 (the start of the COVID-19 outbreak in South Korea) to September 2020 (when the survey was distributed) were enrolled in the study. Individuals who moved to a different region after the outbreak of COVID-19 were excluded. The appropriate sample size required for regression analysis was computed using the G*Power 3.1.9.2 software. For an effect size of 0.10, significance (α) of 0.05, power (1 − β) of 0.80, and 15 predictor variables, the minimum required sample size was 201. However, the questionnaire was distributed to 240 participants in consideration of potential dropouts. After excluding 28 questionnaires with missing responses, a total of 212 questionnaires were included in the final analysis.
Data Collection
Data collection took place from September 3 to September 5, 2020, via an online survey to minimize direct contact with the participants, thus respecting the safety requirements and requests for social distancing during the COVID-19 pandemic. The participants were recruited on internet communities for the targeted regions and through social media (eg, Instagram). Before the start of the questionnaire, they were informed that the questionnaire was only for residents of Daegu and Gyeongbuk. After reading the online recruitment advertisements, volunteers who accessed the questionnaire link were requested to read the study information sheet to understand the inclusion criteria, purpose, and method of the study and the contents of the survey before they were allowed to begin the questionnaire.
Study Instruments
Post-Traumatic Stress Disorder (PTSD)
This was assessed using the Impact Event Scale-Revised-Korea, which is an adapted and validated Korean version of the Impact Event Scale-Revised,20 originally developed by Horowitz, Wilner, and Alvarev21 and modified by Weiss and Marmar.22 The researchers obtained permission from the authors to use this tool. It consists of 22 items, each rated on a five-point Likert scale ranging from 0 (“never”) to 4 (“frequently”). A higher score indicates greater PTSD. Cronbach’s α was 0.83 in Eun et al’s study, and 0.93 in this study.
Perceived Health Status
The Short-Form Health Survey validated by Ware, Kosinski, and Keller,23 assessed this factor, but only after permission to use the Korean version from OPTUM.COM, was obtained. This tool consists of 12 items in two domains: physical - and mental health. A scoring program was downloaded from OPTUM.COM to convert the scores on a 100-point scale. A higher score indicated a better perceived health status. Cronbach’s α was 0.91 in Ware et al’s23 study and 0.84 in this study.
Family Hardiness
This was assessed using the Family Hardiness index developed by McCubbin, Patterson, and Thompson,24 and adapted into Korean by Sim.25 We obtained permission to use this tool from the authors. It comprises 20 items rated on a four-point Likert scale ranging from 1 (“strongly disagree”) to 4 (“strongly agree”). Negatively worded items are reverse-scored, and a higher score indicates greater family hardiness. Cronbach’s α was 0.82 in McCubbin et al’s study24 and 0.85 in this study.
Resilience
Resilience was measured using the Korean version of the Connor-Davidson Resilience Scale,26 originally developed by Connor, Kathryn, Jonathan, and Davidson.27 The researchers obtained permission to use the tool after paying a fee to the original authors. It has 25 items rated on a five-point Likert scale ranging from 1 (“strongly disagree”) to 5 (“strongly agree”). A higher score shows a person may possess greater resilience. Cronbach’s α was 0.89 in Connor et al’s study27 and 0.93 in this study.
Data Analysis
The collected data were analyzed using the following procedures using the IBM SPSS 25.0 software tool. First, participants’ general characteristics were analyzed using the frequency, percentage, mean, and standard deviation. Second, participants’ PTSD, perceived health status, family hardiness, and resilience were analyzed using the mean, standard deviation, minimum - and maximum values. Third, differences in resilience according to participants’ general characteristics were analyzed using a t-test and a one-way ANOVA. This was followed by Scheffe’s test for post-hoc comparisons. Fourth, the correlations between participants’ PTSD, perceived health status, family hardiness, and resilience were analyzed using Pearson’s correlation coefficient. Fifth, the predictors of resilience were identified using multiple linear regression.
Ethical Considerations
This study was carried out in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board of Kyungpook National University (no. KNU-2020-0031) before data collection. The participants were informed that their anonymity was guaranteed, that they were free to withdraw from the study at any time, and that the data would only be used for research purposes. Only participants who voluntarily indicated their consent to participate by checking “I agree” were allowed to proceed with the questionnaire. The collected data were encoded and stored at the researchers’ laboratory. Participants who completed the questionnaire were given a small reward.
Results
Participants’ General Characteristics
Participants were predominantly women (63.7%), between the ages of 20–29 years (65.2%), with a mean age of 26.79 years. The majority lived in Daegu (74.5%) and had an education level of a college graduate or higher (79.2%). Regarding marital status, 70.3% of the participants were single, divorced, or widowed, and 74.1% lived with their family. More than half (72.2%) of the participants said that they were employed. Most of the participants described themselves as middle-class (74.1%) and did not have an underlying disease (88.7%). The vast majority of the participants (94.8%) did not personally know anyone who tested positive for COVID-19, including themselves. A total of 58% of participants had no financial loss as a result of the COVID-19 pandemic and 97.2% did not suffer any physical damage from it (Table 1).
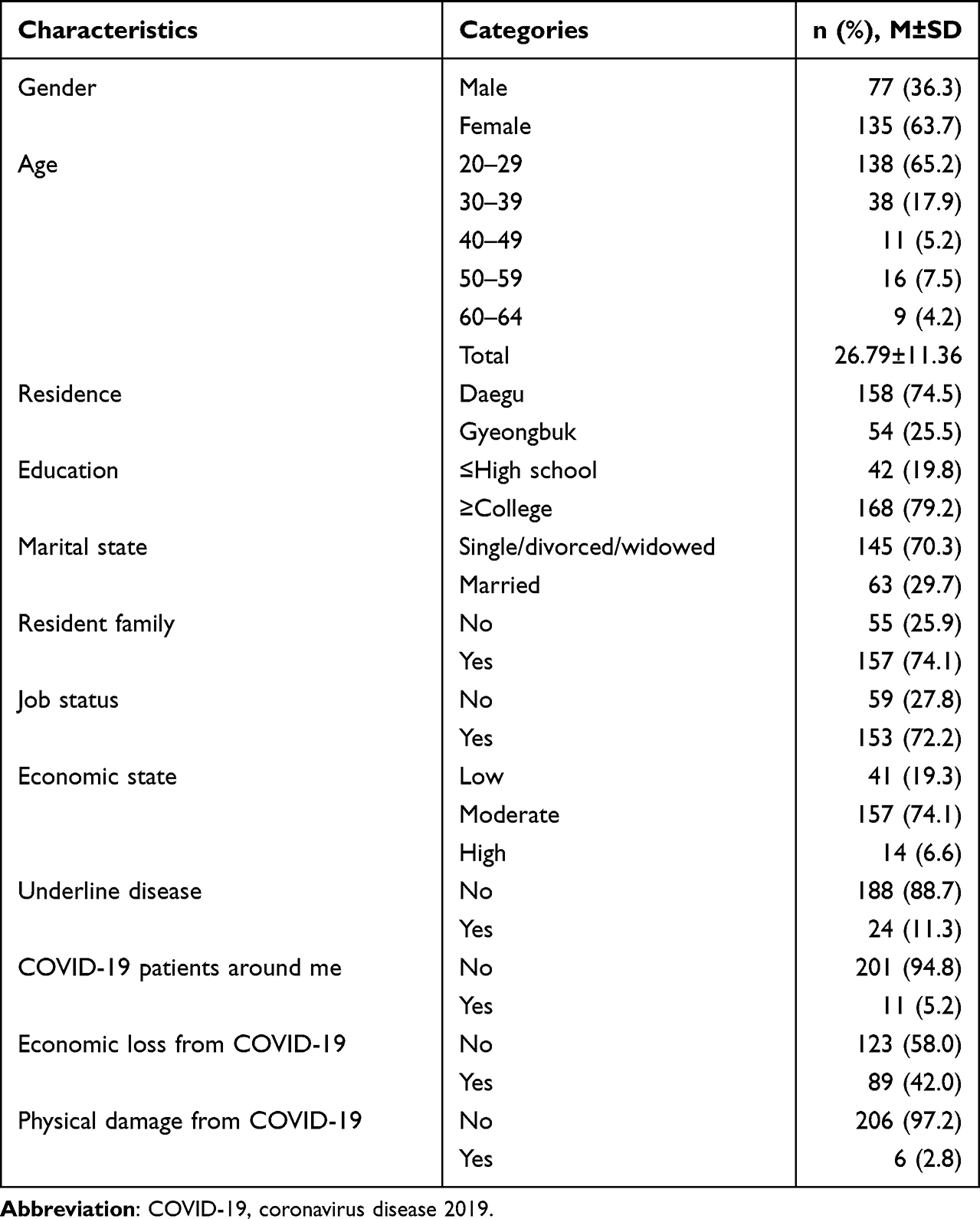 |
Table 1 General Characteristics of the Subjects (N=212) |
Descriptive Statistics of the Study Variables
Table 2 shows the minimum, maximum, and mean scores of the study variables. The mean PTSD score was 1.01 ± 0.70, the mean perceived health status was 57.09 ± 8.08, the mean family hardiness score was 2.96 ± 0.35, and the mean resilience score was 2.59 ± 0.56.
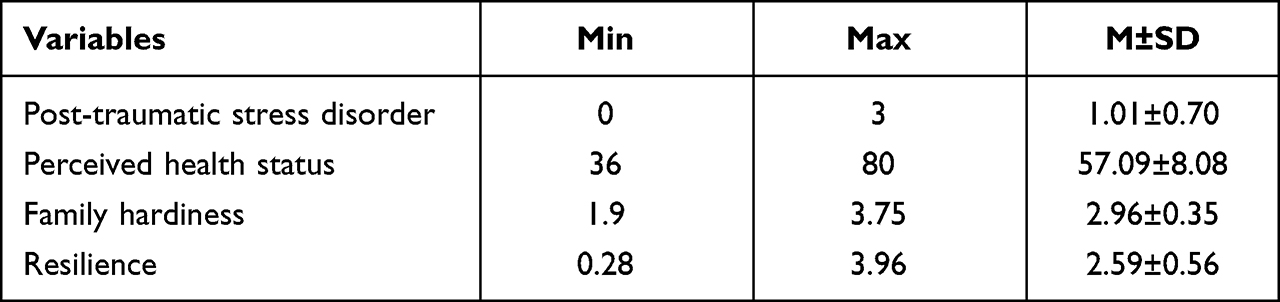 |
Table 2 Post-Traumatic Stress Disorder, Perceived Health Status, Family Hardiness, and Resilience (N=212) |
Differences in Resilience According to General Characteristics
Table 3 shows the participants’ resilience according to their general characteristics. Resilience significantly differed according to area of residence, financial status, and financial loss from COVID-19. Daegu residents had lower resilience than Gyeongbuk residents; participants with lower financial status and financial loss from COVID-19 had lower resilience than those with higher financial status and no financial loss, respectively.
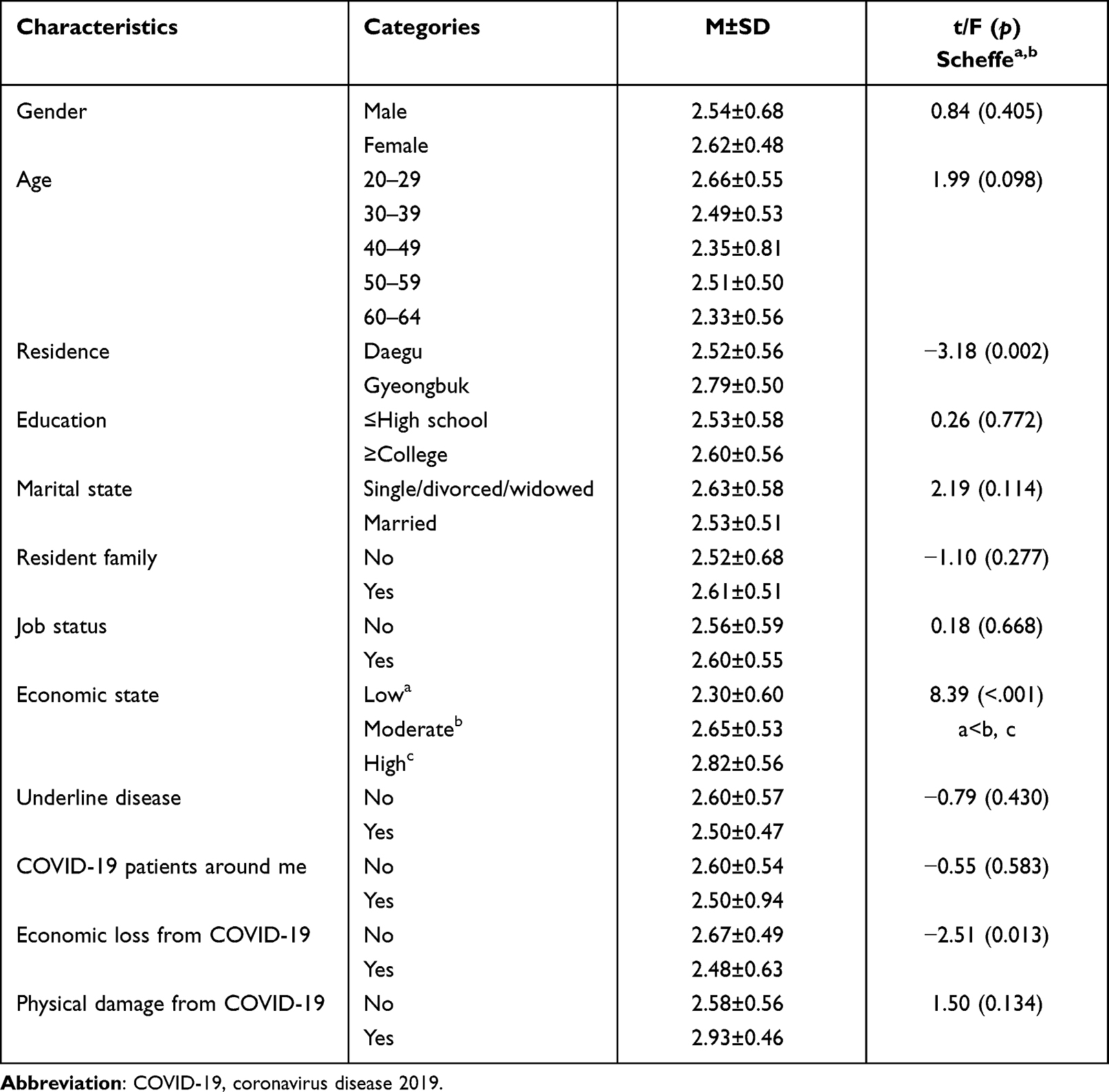 |
Table 3 Resilience According to General Characteristics (N=212) |
Correlations Between Variables
Table 4 shows the correlations between PTSD, perceived health status, family hardiness, and resilience. Resilience was negatively correlated with PTSD and significantly positively correlated with perceived health status and family hardiness.
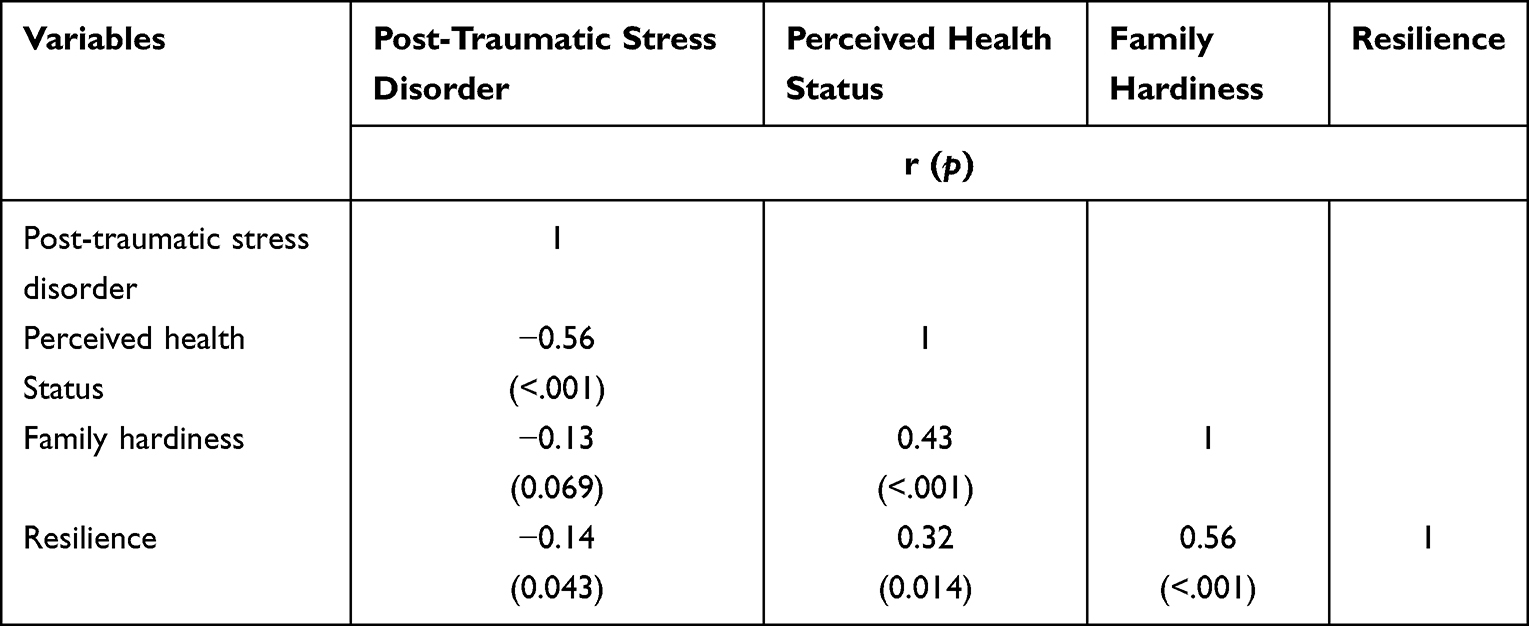 |
Table 4 Correlations Between Post-Traumatic Stress Disorder, Perceived Health Status, Family Hardiness, and Resilience |
Predictors of Resilience
The factors affecting resilience are displayed in Table 5. The regression assumptions were tested to help identify predictors of resilience. The Durbin-Watson index was 2.11, confirming the absence of autocorrelation and independence of residuals. The variance inflation factor was below 10, at 1.12–1.84, with tolerance above 0.1 at 0.54–0.88, confirming the absence of multicollinearity. The general characteristics that significantly differed in resilience and where the parameters correlated with resilience were entered as independent variables. Categorical variables were dummy coded. The results showed that the area of residence, middle-class financial status, high-class financial status, and family hardiness significantly influenced resilience. Resilience was higher among Gyeongbuk residents than Daegu residents; the middle and high-classes had higher levels of resilience than the lower class. Participants with greater family hardiness had higher resilience. The most potent predictor of resilience was family hardiness, and all the predictors explained 36% of resilience.
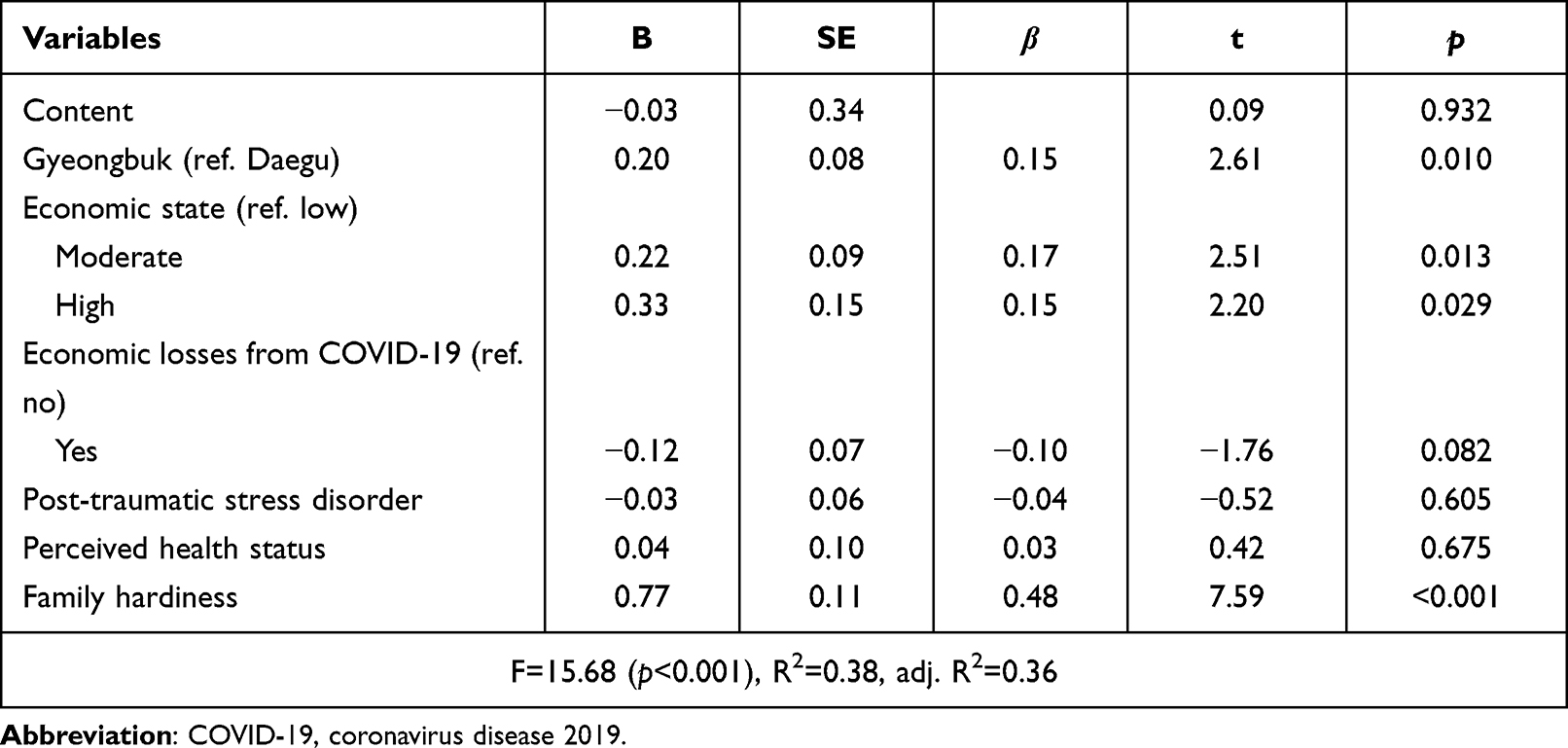 |
Table 5 Factors Affecting Resilience (N=212) |
Discussion
This study aimed to examine the level of resilience among residents of communities affected by the first wave of COVID-19 in South Korea and to investigate the associations between the variables and predictors of resilience. Resilience was lower in residents of Daegu and Gyeongbuk when compared to those in ostomates (2.67 points)28 and workers involved in an industrial accident (2.86 points).10 The fact that the COVID-19 pandemic is still ongoing and returning to everyday life is uncertain due to the emergence of several mutated viruses seems to have negatively impacted the participants’ resilience.
In this study, family hardiness, area of residence, and financial status were identified as significant predictors of resilience. Of these, family hardiness most potently influenced a participant’s resilience, which is in line with previous findings.17,25 Family hardiness acts as a buffer that protects the individual from stress and enables them to adjust when faced with adversities.29 They handle it better because they are able to actively deal with threats. In other words, having greater family hardiness means that an individual is able to deal appropriately with and adjust flexibly to a situation, thereby increasing their overall resilience.30 Therefore, family support - or family relationship-enhancement programs, such as couples and family counseling, should be implemented in communities to provide an opportunity for families to develop the skills to understand and support one another.
Daegu residents in this study showed significantly lower resilience than Gyeongbuk residents. This discrepancy may be because the percentage of COVID-19 patients at the time of data collection in September 2020 was higher in Daegu (7065; 0.29%) than in Gyeongbuk (1426; 0.05%) (Daegu Metropolitan City, 2020). In addition, Daegu has a greater proportion of moving population than Gyeongbuk. This translates to greater uncertainty regarding the potential exposure to the infection, and the consequent anxiety and fear might have affected resilience.
This study found that people who identified as middle or high-classes had greater resilience than those who identified as lower class. As the COVID-19 pandemic is prolonged, the suicide rate has also increased due to worsening financial conditions such as income decline, unemployment, falling social class, and poverty. Further, a study found that poor disaster victims indicated that they have more concerns and more anxiety about how they would be able to return to their pre-disaster standard of living and economic activities.31 This anxiety, caused by disaster-related financial problems, adversely impacted their resilience.32 Poorer individuals may have displayed higher anxiety levels because they lack the material resources and support systems to adjust to adverse situations. This observation reflects the sentiments from previous findings that resilience decreases as the financial status declines.17 Thus, policies that provide support to low-income individuals and aim to boost their resilience during various disasters, including infectious disease outbreaks, should be a focal point for policymakers.
In this study, PTSD did not significantly influence resilience. The severity of mental health problems due to PTSD increases as the rate of exposure increases.33 Thus, the fact that most of the participants (94.8%) did not personally know anyone, including themselves, confirmed as positive for COVID-19 may explain the study’s results. As PTSD levels and mental health problems may differ according to the level of exposure to a traumatic event,34 subsequent studies should take into consideration that the results may depend on the number of positive COVID-19 diagnoses among the individuals participating in the study and the people around them. Meanwhile, a study on adolescents reported that PTSD was not a significant influencing factor of resilience after disasters, but was a mediating factor between protective factors and risk factors of resilience.35 Therefore, a comparative study by age groups is needed, and a study to verify the mediating effect of PTSD is also needed.
Perceived health status did not significantly influence resilience as initially suspected. This is presumably because most of the participants were younger without any major health problems, as indicated by the high percentage of participants between the ages 20–29 years and the low mean age of the study sample. According to the 2020 Statistics in a report from Korea based on gender- and age-specific perceived health status, individuals between the ages of 20–29 years showed the highest perceived health status (69.5%), while those who are 60 years or older had the lowest perceived health status (28.5%) among the sample of adults aged 19–64 years, which was the age criterion for the study.36 Considering that younger individuals regard their health more positively, the fact that most of the participants were young may have contributed to the study’s results.
This study is significant because it identified some predictors of resilience among the residents of the communities affected by the first wave of COVID-19 in South Korea. Findings may be useful in developing emotional support and programs aimed at overcoming challenges for the residents of the communities who may face similar disasters in the future. The results of this study show that when providing a support program to enhance resilience after a disaster, it is necessary to prioritize the level of support within the family, the regional characteristics of the disaster, and the socioeconomic level of local residents. However, the study also has some limitations. First, the findings have limited generalizability because the participants were conveniently sampled from the target regions. Second, subsequent studies should consider that an individuals’ resilience can be influenced by knowing someone who has been confirmed as positively diagnosed with COVID-19. Third, this study is mainly a descriptive survey; consequently, the causality among the parameters cannot be determined. Finally, resilience may have been under- or over-estimated due to the nature of self-reported data.
During the COVID-19 pandemic, the Korean government launched a trauma center and a psychological support organization to provide psychological and emotional support to help citizens. In addition to this, services that check and link negative physical and mental health using health questionnaires are needed at public health centers and community centers so that local residents can easily use them. In a long-term disaster situation, a system must be established to quickly assess people’s resilience and mental health through the correct clinical assessment tools and provide optimal interventions.37 Further, there is a lack of programs to promote family unity, a key factor affecting resilience. Therefore, various systematic programs that increase family strength should be developed.
Conclusions
This study examined the relationships between PTSD, perceived health status, family hardiness, and resilience and tried to identify the predictors of resilience among Daegu and Gyeongbuk residents. The government and local organizations should develop diverse programs for community residents to improve their members’ family hardiness, which contributes to the development of resilience. Moreover, the level of resilience in communities from special disaster regions that are strongly affected by disasters must be examined and the policymakers should focus on prevention and intervention programs aimed at boosting their resilience to promote a prompt return to their everyday lives.
Acknowledgments
This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (No. NRF-2020R1I1A3068740). We would like to thank the NRF.
Disclosure
The authors report no actual or potential conflicts of interest in this work.
References
1. Center for Disease Control and Prevention. CDC science agenda for COVID-19, 2020–2023 (Online); 2021. Available from: https://www.cdc.gov/coronavirus/2019-ncov/science/science-agenda-covid19.html.
2. Son MA. Coronavirus infection-19 and the deepening contradiction of capitalism. Radic Rev. 2020;83:223–225.
3. Central disaster management headquarters. Coronavirus outbreak Gov Briefs; 2020. Available from: http://ncov.mohw.go.kr/tcmBoardView.do?brdId=3&brdGubun=31&dataGubun=&ncvContSeq=1241&contSeq=1241&board_id=311&gubun=BDC.
4. Yuan K, Gong YM, Liu L, et al. Prevalence of posttraumatic stress disorder after infectious disease pandemics in the twenty-first century, including CODI-19: a meta-analysis and systematic review. Mol Psychiatry. 2021;27(1):1–17. doi:10.1038/s41380-021-01117-x
5. Gyeonggi Research Institute national. Mental health survey due to corona. Statistics Korea. 19 (Online); 2020. Available from: https://www.gri.re.kr/%EC%9D%B4%EC%8A%88-%EC%A7%84%EB%8B%A8/?brno=14489&prno=20200231.
6. Gloria CT, Steinhardt MA. Relationships among positive emotions, coping, resilience and mental health. Stress Health. 2016;32(2):145–156. doi:10.1002/smi.2589
7. Fullerton DJ, Zhang LM, Kleitman S, Sudzina F. An integrative process model of resilience in an academic context: resilience resources, coping strategies, and positive adaptation. PLoS One. 2021;16(2):e0246000. doi:10.1371/journal.pone.0246000
8. Bonanno GA. Loss, trauma, and human resilience. Have we underestimated the human capacity to thrive after extremely aversive events? Am Psychol. 2004;59(1):20–28. doi:10.1037/0003-066X.59.1.20
9. Bonanno GA, Brewin CR, Kaniasty K, La Greca AM. Weighing the costs of disaster: consequences, risks, and resilience in individuals, families, and communities. Am Psychol. 2010;11(1):1–49.
10. Han JW, Lee BS. The effect of post-traumatic stress on quality of life in industrial accident patients: effect of recovery resilience. J Korea Acad-Ind Coop Soc. 2018;19(4):167–177.
11. Su TP, Lien TC, Yang CY, et al. Prevalence of psychiatric morbidity and psychological adaptation of the nurses in a structured SARS caring unit during outbreak: a prospective and periodic Assessment study in Taiwan. J Psychiatr Res. 2007;41(1–2):119–130. doi:10.1016/j.jpsychires.2005.12.006
12. Â L, Ramires A, Moura AD, Souto T, Marôco J. Psychological well-being and health perception: predictors for past, present and future. Arch Clin Psychiatry. 2019;46(3):53–60. doi:10.1590/0101-60830000000194
13. Lee JS. A comparative study on the mental health and health-related quality of life in victimized community residences before and after Sewol ferry disaster. Asia Pac J Multimedia Serv Converg Art Humanit Sociol. 2018;8(10):895–903.
14. Eifert EK, Hall M, Smith PH, Wideman L. Quality of life as a mediator of leisure activity and perceived health among older women. J Women Aging. 2019;31(3):248–268. doi:10.1080/08952841.2018.1444937
15. Damayant IL, Annatagia L. Family hardiness and caregiver burden among the family of stroke patients. In:
16. Huang Y, Huang Y, Bao M, Zheng S, Du T, Wu K. Psychological resilience of women after breast cancer surgery: a cross-sectional study of associated influencing factors. Psychol Health Med. 2019;24(7):866–878. doi:10.1080/13548506.2019.1574353
17. Cho HM, Yoo EK. Effects of depression, family support on resilience in patients with gynecological cancer. J Korean Soc Wellness. 2015;10(4):183–195.
18. Schlenger WE, Caddell JM, Ebert L, et al. Psychological reactions to terrorist attacks: findings from the National Study of Americans’ Reactions to September 11. JAMA. 2002;288(5):581–588. doi:10.1001/jama.288.5.581
19. Ozbay F, Johnson DC, Dimoulas E, Morgan CA, Charney D, Southwick S. Social support and resilience to stress: from neurobiology to clinical practice. Psychiatry. 2007;4(5):35–40.
20. Eun HJ, Kwon TW, Lee SM, Kim TH, Cho MR, Cho SJ. A study on reliability and validity of the Korean version of impact of event scale-revised. J Korean Neuropsychiatr Assoc. 2005;44(3):303–310.
21. Horowitz M, Wilner N, Alvarez W. Impact of event scale: a measure of subjective stress. Psychosom Med. 1979;41(3):209–218. doi:10.1097/00006842-197905000-00004
22. Weiss DS, Marmar CR. The impact of event scale-revised. In: Wilson J, Keane TM, editors. Assessing Psychological Trauma and PTSD. New York: Guilford Press; 1996:399–411.
23. Ware JE, Kosinski M, Keller SD. A 12-item short-form health survey: construction of scales and preliminary tests of reliability and validity. Med Care. 1996;34(3):220–233. doi:10.1097/00005650-199603000-00003
24. McCubbin HI, Patterson J, Thompson EA. Family hardiness index. In: McCubbin HI, Thompson AI, editors. Family Assessment for Research and Practice. Madison: University of Wisconsin Press; 1991.
25. Sim MK. Influence of resiliency factors on adaptation in families of children with cancer. J Korean Acad Child Health Nurs. 2004;10(4):383–394.
26. Baek HS, Lee KU, Joo EJ, Lee MY, Choi KS. Reliability and validity of the Korean version of the Connor-Davidson Resilience Scale. Psychiatry Investig. 2010;7(2):109–115. doi:10.4306/pi.2010.7.2.109
27. Connor KM, Davidson JR. Development of a new resilience scale: the Connor-Davidson Resilience Scale (CD-RISC). Depress Anxiety. 2003;18(2):76–82. doi:10.1002/da.10113
28. Shin JH, So HS, Kim EA. Influence of post-traumatic stress disorders on quality of life among patients with ostomy: focused on the mediating effect of resilience. Korean J Adult Nurs. 2017;29(6):657–666. doi:10.7475/kjan.2017.29.6.657
29. Costanza A, Amerio A, Aguglia A, et al. From “the interpersonal theory of suicide” to “the interpersonal trust”: an unexpected and effective resource to mitigate economic crisis-related suicide risk in times of covid-19? Acta Biomedica. 2021;92:e2021417. doi:10.23750/abm.v92iS6.12249
30. Maurović I, Liebenberg L, Ferić M. A review of family resilience: understanding the concept and operationalization challenges to inform research and practice. Child Care Pract. 2020;26(4):337–357. doi:10.1080/13575279.2020.1792838
31. Wen J, Shi YK, Li YP, Yuan P, Wang F, García O. Quality of life, physical diseases, and psychological impairment among survivors 3 years after the Wenchuan earthquake, a population-based survey. PLoS One. 2012;7(8):e43081. doi:10.1371/journal.pone.0043081
32. Skalski S, Uram P, Dobrakowski P, Kwiatkowska A. The link between ego-resiliency, social support, SARS-CoV-2 anxiety and trauma effects. Polish adaptation of the coronavirus Anxiety Scale. Pers Individ Dif. 2021;171:110540. doi:10.1016/j.paid.2020.110540
33. Kim SI. Influence of fear about Middle East Respiratory Syndrome event of hospital worker and general public on socio-psychological health: mediating effect of posttraumatic stress. Anxiety Mood. 2019;15(1):45–52.
34. Sareen J. Posttraumatic stress disorder in adults: impact, comorbidity, risk factors, and treatment. Can J Psychiatry. 2014;59(9):460–467. doi:10.1177/070674371405900902
35. Laksmita OD, Chung MH, Liao YM, Haase JE, Chang PC. Predictors of resilience among adolescent disaster survivors: a path analysis. J Adv Nurs. 2020;6(8):2060–2071. doi:10.1111/jan.14396
36. Statistics Korea. Government. Subjective health status by Gender and Age Group, 2020. Statistics Korea; 2020. Available from: https://www.index.go.kr/unify/idx-info.do?idxCd=8082.
37. Baertschi M, Costanza A, Canuto A, Weber K. The dimensionality of suicidal ideation and its clinical implications. Intl J Methods in Psychiatr Res. 2019;28(1):e1755. doi:10.1002/mpr.1755
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Resilience and Prosocial Behavior Among Chinese University Students During COVID-19 Mitigation: Testing Mediation and Moderation Models of Social Support
Xue S, Kaufman MR, Zhang X, Xia S, Niu C, Zhou R, Xu W
Psychology Research and Behavior Management 2022, 15:1531-1543
Published Date: 16 June 2022
Resilience and Depressive Symptoms Mediated Pathways from Social Support to Suicidal Ideation Among Undergraduates During the COVID-19 Campus Lockdown in China
Zhang X, Liu X, Mi Y, Wang W, Xu H
Psychology Research and Behavior Management 2022, 15:2291-2301
Published Date: 23 August 2022
Resilience as a Source of Easement to Health-Related Worries in Women at Increased Risk for Breast or Ovarian Cancer During the COVID-19 Pandemic
Schwab R, Droste A, Stewen K, Elger T, Theis S, Heimes AS, Peters K, Schmidt M, Brenner W, Hasenburg A
International Journal of General Medicine 2022, 15:7039-7052
Published Date: 5 September 2022
How Interpersonal Sensitivity Affects Depression Under the COVID-19 Lockdown Among College Students in South China: A Moderated Mediation Model
Zhang Y, Sun Q
Psychology Research and Behavior Management 2023, 16:1271-1282
Published Date: 18 April 2023
The Relationship Between Social Media Use and Negative Emotions Among Chinese Medical College Students: The Mediating Role of Fear of Missing Out and the Moderating Role of Resilience
Chen S, Li H, Pang L, Wen D
Psychology Research and Behavior Management 2023, 16:2755-2766
Published Date: 19 July 2023