Back to Journals » Journal of Pain Research » Volume 19
Reshaping Precision Cancer Pain Management with Multimodal Artificial Intelligence: A Review on Subtyping and Treatment Response Prediction
Authors Wang X ![]() , Tang X, Wei C, Xu J, Sun K
, Tang X, Wei C, Xu J, Sun K ![]() , Zhou G
, Zhou G
Received 26 September 2025
Accepted for publication 24 January 2026
Published 2 February 2026 Volume 2026:19 570481
DOI https://doi.org/10.2147/JPR.S570481
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Amitabh Gulati
Xuexing Wang,1– 3,* Xingxing Tang,4 Chunmei Wei,1 Jinsong Xu,2 Kai Sun,3,* Guozhong Zhou2,*
1Department of Oncology, Anning First People’s Hospital Affiliated to Kunming University of Science and Technology, Anning, People’s Republic of China; 2Pain Medicine Department, Anning First People’s Hospital Affiliated to Kunming University of Science and Technology, Anning, People’s Republic of China; 3Department of Oncology, Ganzhou Cancer Hospital, Ganzhou, People’s Republic of China; 4Cadre Medical Department, Third Affiliated Hospital of Kunming Medical University, Kunming, 650000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guozhong Zhou, Email [email protected] Kai Sun, Email [email protected]
Abstract: The profound heterogeneity of cancer pain renders conventional “one-size-fits-all” analgesic strategies ineffective, creating an urgent need for tools that can accurately subtype pain and predict individual therapeutic responses. This review proposes a transformative solution: a patient-specific “digital twin” for pain, powered by multimodal Artificial Intelligence (AI). This framework leverages advanced AI methodologies, including large foundation models and transformer architectures, to integrate and interpret these complex datasets. By synthesizing diverse data streams—from genomics and digital pathology to clinical text and patient-reported outcomes—the digital twin can uncover complex, non-linear patterns to simultaneously classify pain subtypes (eg, nociceptive, neuropathic, nociplastic) and predict sensitivity to specific analgesic regimens. While promising, we critically assess major translational barriers, including data scarcity, model interpretability, the need for robust prospective validation, and privacy concerns. To bridge the gap from concept to clinic, we outline a concrete research roadmap and a “Hybrid Telemedicine and On-Site Expert” implementation model. This AI-driven framework offers a path toward precise, dynamic, and truly personalized cancer pain management, aiming to tangibly improve outcomes for patients worldwide.
Keywords: cancer pain, multimodal artificial intelligence, digital twin, pain subtyping, individualized treatment prediction
Introduction
Cancer pain is one of the most common and distressing complications for cancer patients, severely impairing their quality of life and posing a significant challenge to clinical treatment.1,2 Although traditional management strategies, such as the World Health Organization (WHO) three-step analgesic ladder, have played a fundamental role in pain relief, their “one-size-fits-all” approach ignores the vast intrinsic heterogeneity of cancer pain, leading to inadequate individualized treatment and leaving many patients with unsatisfactory pain control.1 Therefore, developing innovative strategies that can accurately identify different pain subtypes and predict individual treatment responses has become an urgent need in oncology and pain medicine.
In recent years, biomedical research has entered an era of data-driven precision medicine. The proliferation of multi-omics technologies (eg, genomics, transcriptomics) and breakthroughs in Artificial Intelligence (AI) and Machine Learning (ML) algorithms have provided unprecedented tools for unraveling the complexity of diseases.3–5 Particularly, multimodal Large Models, including Large Language Models (LLMs) and Vision-Language Models (VLMs), have demonstrated exceptional capabilities in integrating and analyzing massive, heterogeneous data (eg, genomic sequences, pathology images, clinical progress notes), suggesting a strong potential to aid in clinical decision-making, predict treatment responses, and optimize cancer management.6 For instance, deep learning can now infer a wide range of genetic mutations and molecular subtypes directly from routine histology slides, demonstrating a powerful link between tissue phenotype and genotype that can be harnessed for precision medicine.7 To address this heterogeneity, a new framework is needed that can synthesize diverse patient data in a holistic and dynamic manner. This review argues for a paradigm shift in cancer pain management, moving away from siloed analyses toward an integrated, AI-driven approach. While the application of such sophisticated multimodal AI in pain medicine is still in its nascent stage, this review proposes a forward-looking conceptual framework centered on creating a “digital twin” of a patient’s pain state by fusing multimodal data. This framework is not merely a static predictive model but a dynamic, longitudinal representation that evolves with the patient. It aims to simultaneously achieve precise pain subtyping and predict individualized treatment responses. We will first delve into the clinical and molecular basis of cancer pain heterogeneity, establishing the necessity for this new paradigm. Subsequently, we will detail the components of our proposed framework, from data integration to advanced AI models. Finally, we will outline a concrete research roadmap and a practical implementation model to translate these cutting-edge technologies into clinical practice, with the goal of providing a theoretical and practical guide for developing the next generation of intelligent pain management systems.
The Heterogeneity of Cancer Pain: Clinical and Molecular Foundations
Cancer pain is not a single entity but a complex syndrome driven by multiple underlying mechanisms. Its high degree of clinical and molecular heterogeneity is the core reason for current therapeutic dilemmas. Therefore, a deep understanding of its subtypes, molecular basis, and phenotypic characteristics is a prerequisite for achieving precision management.
Clinical Subtypes and Their Pathophysiological Features
According to the International Association for the Study of Pain (IASP) classification, cancer pain is primarily divided into three major subtypes based on its pathophysiological mechanisms. These subtypes often coexist in the same patient, increasing the complexity of diagnosis and treatment.
Nociceptive Pain: This type is caused by the direct compression, invasion, or destruction of normal tissues (such as bone, viscera) by the tumor, activating peripheral nociceptors. It often presents clinically as dull, throbbing, or pressure-like pain, such as the severe pain caused by bone metastases.8
Neuropathic Pain: This results from direct tumor invasion of nervous tissue or damage to the nervous system by treatments like chemotherapy, radiotherapy, or surgery.9,10 Typical symptoms include spontaneous burning sensations, stabbing pain, numbness, or allodynia. Chemotherapy-Induced Peripheral Neuropathy (CIPN) is a common form.11,12 Additionally, Perineural Invasion (PNI) is significantly associated with more severe pain in Head and Neck Squamous Cell Carcinoma (HNSCC) and is an important marker of a neuropathic component.13 Chronic Postsurgical Pain (CPSP) also often has neuropathic features.14,15
Nociplastic Pain: This is a newer concept referring to pain that arises from dysfunctional pain processing pathways in the central nervous system (ie, central sensitization) without clear evidence of tissue or nerve damage. In cancer survivors, this pain may be related to long-term post-treatment sequelae and inflammatory states, characterized by altered pain perception and modulation systems.16 Identifying this elusive subtype, which is defined by the absence of clear peripheral drivers or biomarkers, represents a critical diagnostic challenge. The hypothesis that AI-driven pattern recognition on longitudinal clinical and physiological data may offer unique insights requires rigorous investigation, particularly regarding the establishment of a “ground truth” for model training and validation.
Different subtypes respond very differently to treatment. For example, opioids often have limited efficacy for neuropathic pain.17 Therefore, precise subtype diagnosis based on pathophysiological mechanisms is the cornerstone for developing individualized treatment plans.1,18,19
Molecular Basis of Individual Differences in Cancer Pain
Genomic and molecular biology research has provided profound insights into the individual differences in cancer pain, revealing a complex regulatory network from genetic polymorphisms to the tumor microenvironment.
Genetic Susceptibility: An individual’s sensitivity to pain and response to analgesics are significantly influenced by genetic factors. For instance, mutations in the gene encoding the voltage-gated sodium channel Nav1.7 are closely related to pain perception; gain-of-function mutations can cause severe pain, while loss-of-function mutations lead to an inability to feel pain. Nav1.7 is abnormally expressed in various cancer cells and is associated with the development of CIPN, making it a potential analgesic target.12 Similarly, Single Nucleotide Polymorphisms (SNPs) in the ENPP2 gene, which encodes autotaxin, are associated with the severity of neuropathic pain and opioid requirements, with patients carrying specific alleles potentially experiencing more severe pain.20
Regulation by the Tumor Microenvironment (TME): The TME is not composed solely of cancer cells; its components, such as nerve and immune cells, play a key role in the development of cancer pain. Studies have found that a neuron-like subset of Tumor-Associated Macrophages (TAMs) can promote intratumoral neurogenesis and express pain receptors, thereby driving pain behavior.21 In head and neck cancer, a functional “cross-activation circuit” exists between the tumor and surrounding nerves, which co-promotes pain and tumor progression by exchanging pro-nociceptive mediators like Brain-Derived Neurotrophic Factor (BDNF) and Tumor Necrosis Factor-alpha (TNF-α).22
Epigenetics and Inflammation: Epigenetic modifications (eg, DNA methylation, histone modification) and persistent inflammatory states are key mechanisms that link genetic and environmental factors and drive the chronification of pain. The inflammatory factor TNF-α has been identified as a core mediator of nociplastic pain and bone cancer pain, and interventions targeting its expression (eg, using EGCG) have shown analgesic effects.16,23
Phenotypic Assessment of Pain and Its Challenges
Accurate, multidimensional assessment of pain phenotypes is the clinical foundation for achieving precise subtyping.
Standardized Assessment Tools: The Numerical Rating Scale (NRS) is widely used in clinical practice to assess pain intensity.17,24 To more comprehensively capture the multidimensional characteristics of pain, it is necessary to combine tools like the Brief Pain Inventory (BPI) and questionnaires for screening neuropathic components, such as the DN4 or the Leeds Assessment of Neuropathic Symptoms and Signs (LANSS).11,25,26
Challenges in Clinical Diagnosis: Despite various tools, a standardized clinical diagnosis for Neuropathic cancer Pain (NcP) is still lacking. There is limited consistency among different assessment methods (eg, scales, clinical impression, expert consensus), highlighting the importance of establishing more rigorous and unified diagnostic criteria.26
Objective Behavioral Indicators: In preclinical research, non-stimulus-evoked behavioral tests, such as grid climbing, have been developed to more objectively assess pain-related protective behaviors in animal models.27 However, the translation of such findings from preclinical models to human clinical practice remains a significant hurdle in pain research.
Assessing Treatment Adequacy: The Pain Management Index (PMI) is used as an auditable indicator of the adequacy of cancer pain treatment. Studies have found that about a quarter of patients still have a negative PMI, indicating inadequate treatment, which is more common in women and patients whose daily activities are severely disrupted.24
A Digital Twin Framework for Precision Cancer Pain Management
To address the complexity and heterogeneity of cancer pain, the research paradigm must shift from single-data-source analysis to a systematic approach that integrates multidimensional information. We propose a “digital twin” framework, where a computational model serves as a dynamic, in-silico representation of a patient’s pain state, built and updated using multimodal data.
Integration of Multimodal Data: From Genes to Clinical Text
Building a robust cancer pain prediction model requires integrating data from different levels to form a complete picture of the patient (Table 1).
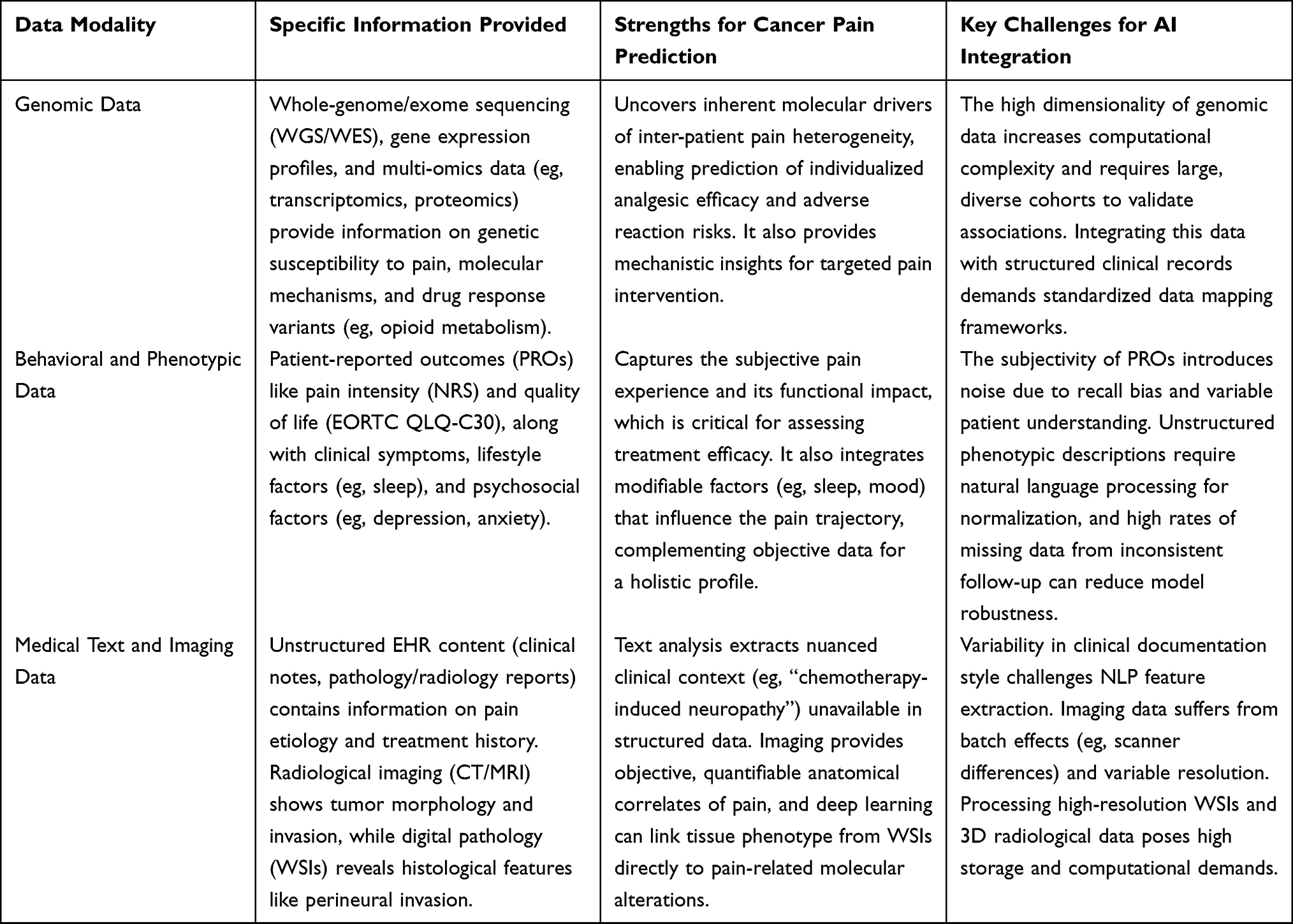 |
Table 1 Comparison of Key Data Modalities for Building a Cancer Pain Digital Twin. This Table Summarizes the Primary Data Types, the Specific Information They Provide, Their Strengths, and Their Key Challenges for Integration into AI Models |
Genomic Data: Includes whole-genome/exome sequencing, gene expression profiles, and multi-omics data, providing underlying information about individual genetic susceptibility, disease molecular mechanisms, and drug responses. Integrating genomic data with Electronic Health Records (EHRs) is key to advancing genomic medicine into clinical practice.28,29
Behavioral and Phenotypic Data: Covers Patient-Reported Outcomes (PROs, eg, pain scores, quality of life), clinical symptoms, lifestyle, and psychosocial factors (eg, depression, anxiety). Research has confirmed that phenotypes such as neuroticism, cognitive function, and sleep patterns are associated with the risk and treatment response of various chronic diseases.30–32
Medical Text and Imaging Data: Unstructured text in EHRs, such as clinical notes, pathology reports, and radiology reports, contains a wealth of clinical information. Natural language processing (NLP) techniques can be used to extract key clinical concepts and phenotypes.29 In addition to radiological imaging, digital pathology, in the form of Whole-Slide Images (WSIs), has emerged as a high-dimensional data source. Deep learning workflows can now predict a wide range of molecular alterations directly from routine H&E-stained histology slides, linking tissue phenotype to genotype.7,33 Combining these with radiomic features from CT, MRI, etc., can provide valuable information about tumor morphology and invasion extent.
However, the integration of these multimodal data presents significant technical and ethical challenges. The “data wrangling” problem—encompassing data acquisition, standardization, cleaning, and linkage across disparate sources—is immense. Real-world clinical data are often characterized by high levels of missingness, noise, and institutional variance, which can severely degrade model performance. Integrating these multimodal data also faces significant challenges in data privacy and security, requiring the development of data sharing and analysis frameworks that protect patient privacy.34
Core AI Technologies: From Machine Learning to Foundation Models
Advanced machine learning algorithms are key to unlocking the value of multimodal data. It is crucial to differentiate between three classes of models: (a) Traditional Machine Learning (ML): Models like random forests, Support Vector Machines (SVMs), and Lasso regression are effective for structured data and have been used for classification and prediction with good performance,35 but they struggle with the complexity of high-dimensional, unstructured data like images or free text. (b) Custom Deep Learning (DL): Models such as Convolutional Neural Networks (CNNs) for images and genomic sequences36 and Recurrent Neural Networks (RNNs) for time-series data (eg, pain trajectories) can learn complex features automatically. Their application in pathology image analysis to detect metastases or predict molecular markers has shown great promise.37,38 (c) Multimodal Foundation Models: This newest class includes large language models (LLMs) and vision-language models (VLMs) pre-trained on massive, general datasets. Their unique capability lies in their ability to perform zero-shot or few-shot learning and to process and fuse diverse data types (eg, text, images, genomics) within a unified architecture, such as a Transformer. Their potential advantage over custom models lies in leveraging in-context learning to reason about rare pain presentations or novel data combinations without requiring explicit retraining. The GestaltMML model, for example, successfully integrated patient facial images and clinical text to improve rare disease diagnosis,39 showcasing a potential architecture for cancer pain.
It is critical, however, to recognize that these models primarily identify correlations, not causal relationships. A key future direction is the integration of causal discovery algorithms to move beyond prediction and toward a more robust understanding of treatment effects.
Privacy-Preserving Computation: To address the challenges of sharing sensitive medical data, technologies like homomorphic encryption, federated learning, and differential privacy have emerged. For instance, the MedCo system uses collective homomorphic encryption to allow multiple institutions to jointly analyze distributed clinical and genomic data without exposing the raw data.40 The OGHE method performs CNN classification directly on encrypted genomic data, ensuring data confidentiality.36
Training and Generalization of Large Models
Training a high-performance, generalizable large model is a systematic engineering effort.
Training Strategy: A “large-scale pre-training + domain-specific fine-tuning” paradigm is commonly adopted. The model is first pre-trained on massive general datasets (eg, general medical texts, public genomic databases) to learn broad feature representations, and then fine-tuned on a specific cancer pain multimodal dataset to adapt to the specific task.
Generalization Ability and Challenges: The model’s generalization ability—its performance on unseen data from different clinical centers or populations—is the ultimate measure of its clinical value. A fundamental tension exists between training a generalizable model on a large population and applying it to create a highly specific, N-of-1 “digital twin”. The inherent heterogeneity and sparsity of medical data, as well as systematic biases between institutions, pose severe challenges to model generalization. These challenges include “dataset shift”, where the statistical properties of the training data differ from the deployment data, and the need for robust domain adaptation techniques. As highlighted in neuro-oncology, robust clinical implementation requires further investigation on a larger, multicenter scale, along with a streamlined and standardized image processing workflow.41 Future research needs to focus on developing more robust model architectures and using techniques like federated learning to integrate diverse data to enhance model generalization and fairness.42,43
Clinical Implementation: The success of a model lies not only in its technical sophistication but also in its smooth integration into the clinical workflow. Incorporating strategies from behavioral economics, such as “nudges”, can help design more user-friendly clinical decision support systems, promoting the adoption of AI-assisted tools by doctors and patients, thereby translating the model’s predictive power into real clinical benefits.44
AI-Driven Precision Subtyping and Response Prediction
Utilizing the “digital twin” framework, AI can move beyond separate analytical steps to perform simultaneous subtyping and treatment response prediction, identifying fine-grained patient subgroups that transcend traditional clinical observations.
The Integrated Workflow: A Conceptual Framework
We propose a conceptual workflow for a multimodal AI system designed to create and leverage a patient’s pain digital twin (Figure 1). The workflow proceeds as follows: Multimodal Data Collection and Integration: Collect and integrate a patient’s genomic data, pain assessment scales (eg, NRS, DN4), digital pathology (WSI) and radiology images, clinical text from EHRs, and proteomics/metabolomics data; Data Preprocessing and Feature Engineering: Clean, standardize, and normalize heterogeneous data. Use specialized encoders for each modality (eg, NLP for text, CNNs for images, bioinformatics tools for omics) to create a unified feature space; Multimodal Fusion and Model Training: A central fusion module, potentially based on a Transformer architecture, integrates the features. The model is trained on a large, high-quality dataset to learn the mapping from input data to a dual output: (a) cancer pain subtype probabilities (eg, neuropathic vs nociceptive vs nociplastic) and (b) predicted efficacy scores for a panel of potential treatments (eg, opioids, gabapentinoids, NSAIDs); Clinical Decision Support Output: For a new patient, the trained model generates a comprehensive report. This report would not be a simple prescription but an actionable summary, including: (1) the most likely pain subtype(s) with confidence scores; (2) a ranked list of recommended treatments with predicted response rates and potential side effects; (3) an interpretability analysis (eg, using SHAP) highlighting the key data features driving the prediction (eg, “High likelihood of neuropathic pain driven by perineural invasion on WSI and specific gene variant X”); and (4) alerts for when model confidence is low or when its prediction conflicts with standard guidelines, prompting clinician review.
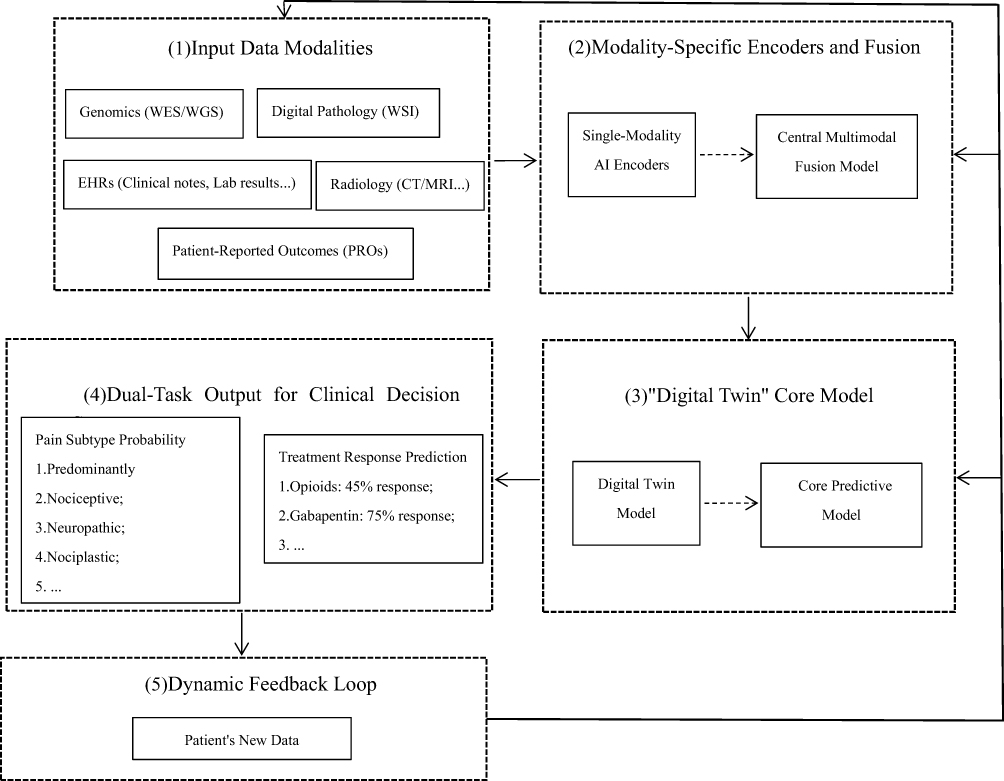 |
Figure 1 Conceptual Framework for a Multimodal AI-Powered “Digital Twin” in Precision Cancer Pain Management. The diagram illustrates the proposed workflow. (1) Input Data Modalities: Data from diverse sources, including Genomics (WES/WGS: whole-exome/whole-genome sequencing), Digital Pathology (WSI: high-resolution whole slide image of tissue samples), Radiology (CT/MRI et al), EHRs (electronic health records, including clinical notes and lab results), and Patient-Reported Outcomes (PROs: patient self-assessed symptoms or quality of life), are collected for an individual patient. (2) Modality-Specific Encoders and Fusion: Each data type is processed by a specialized AI encoder (eg, CNN: convolutional neural network, a model tailored for image analysis; NLP model: natural language processing model, designed to interpret text like clinical notes) to extract high-dimensional features (key patterns in the data). These features are then integrated by a central Multimodal Fusion Module (eg, a Transformer-based architecture: a flexible AI model that can effectively combine different types of data, such as images and text). (3) The “Digital Twin” Core Model: The fused data feeds into a core predictive model, which has been trained to understand the complex relationships between the inputs (eg, how genomic changes link to pain subtypes). (4) Dual-Task Output for Clinical Decision Support: The model simultaneously generates two key outputs: (1) Pain Subtype Probability, classifying the pain as predominantly nociceptive (tissue-damage related), neuropathic (nerve-related), or nociplastic (chronic pain from altered pain processing), and (2) Treatment Response Prediction, providing a ranked list of potential therapies with their predicted efficacy scores (eg, Opioids: 45% response; Gabapentin: 75% response). (5) Dynamic Feedback Loop: The patient’s outcomes and any new data are fed back into the system, allowing the “digital twin” (a patient-specific AI replica) to be dynamically updated for ongoing, adaptive treatment management, reflecting its longitudinal nature. |
Dynamic Updating and Feedback Loop: The digital twin is not static. It is continuously updated with new clinical data (eg, follow-up pain scores, adverse events), often provided directly by the patient via mobile health apps. This allows the model to dynamically re-evaluate and adjust treatment recommendations over time, learning from the individual’s unique response trajectory. The technical requirements for this include robust data pipelines for real-time ingestion and computationally efficient methods for model updating to handle data drift without full retraining.
Addressing Heterogeneity: Technical Innovations to Improve Accuracy
The vast heterogeneity of cancer pain is a major obstacle.45 Technical innovations can address this challenge:
Deep Integration of Multi-omics Data: Moving beyond single-gene analysis, systems biology approaches that integrate genomic, transcriptomic, proteomic, and metabolomic data can build complex models depicting the molecular network of cancer pain. For example, single-cell RNA sequencing has successfully identified a specific neuron-like macrophage subpopulation associated with cancer pain, providing a basis for molecular pathway-based subtyping.21
Fusing Imaging and Biomarkers: Combining functional neuroimaging (eg, fMRI) with peripheral blood or tissue biomarkers (eg, inflammatory factors) provides objective physiological indicators of pain status. For instance, the pain intensity in HNSCC patients is closely related to pathological features in the TME, such as perineural invasion and glial cell activation status,22 all of which can serve as input features for the model.
Applying Advanced Clinical Classification Frameworks: The latest International Classification of Diseases 11th Revision (ICD-11) provides a more refined pathophysiological classification framework for chronic cancer pain, which can guide data annotation and model training.45
Unsupervised and Semi-supervised Learning: In many cases, precise subtype labels are scarce. Unsupervised clustering algorithms (eg, variational autoencoders) can discover new, latent patient subgroups from unlabeled data, revealing unknown dimensions of heterogeneity.
Foundational Evidence and Current Gaps
Recent research, while not yet realizing the full digital twin concept, provides foundational evidence for its components and highlights the specific gaps our proposed framework aims to fill.
The Need for AI-Driven Diagnostic Optimization: A prospective study comparing different methods for diagnosing neuropathic cancer pain (NcP) found significant inconsistencies between the DN4 questionnaire, clinicians’ judgment, and expert committee classification.26 This finding does not merely show a problem; it demonstrates precisely why an AI model that can integrate more rigorous etiological logic and standardized pain features is necessary to surpass existing tools and improve diagnostic accuracy.
The Feasibility of AI-driven Computational Pathology: The power of AI to extract clinically relevant information from images is well-established. Deep learning models have demonstrated performance comparable to or even exceeding that of pathologists in detecting lymph node metastases.37 This success proves the principle that AI can extract meaningful biological signals from histology, providing a crucial data modality for a pain prediction model that links tissue morphology to pain phenotype. The gap remains in connecting these pathological features directly to pain outcomes at scale.
Linking Subtypes to Treatment Response: The known efficacy of methadone against the neuropathic pain component46 and the differential efficacy of non-pharmacological interventions like acupuncture47 or gut microbiota modulation48 provide early evidence for treatment stratification. Our proposed framework would formalize this by learning these links from data, predicting which patients are likely “methadone responders” or “acupuncture responders” based on their complete multimodal profile, a task that currently relies on clinical trial-and-error.
Clinical Translation: A Roadmap and Implementation Model
Bringing advanced predictive models from research to clinical practice is the final mile to realizing their value, a journey filled with both opportunities and challenges.
Critical Challenges in Clinical Translation
Model Generalization and Data Silos: A model trained at one institution may fail at another due to “dataset shift”. Federated learning offers a partial solution by allowing models to be trained across institutions without sharing raw sensitive data, thereby improving model generalization and fairness.43
Model Interpretability (the “Black Box” Problem): Clinicians need to understand why a model makes a certain prediction. While Explainable AI (XAI) methods like SHAP are useful, their fidelity to the model’s actual internal logic is not guaranteed. For highly complex deep learning models, these post-hoc explanations can be superficial or, in some cases, misleading, limiting clinical trust. Developing truly robust and clinically meaningful interpretability is a major research frontier.49
Moreover, a critical examination of AI’s trajectory in other medical fields offers important “cautionary tales” for its application in pain management. A salient example comes from radiology and other specialties, where many AI models, despite stellar performance on training data, are validated in single-center trials, raising significant concerns about their generalizability and performance when deployed in real-world settings across different hospitals and imaging equipment.50 This issue is intrinsically linked to the “black box” problem; a lack of true interpretability undermines clinical trust and complicates accountability, with some experts arguing that current explainability methods may offer a “false hope” of transparency.51 Furthermore, these models can inadvertently perpetuate and even amplify existing societal biases. A stark example is the discovery that deep learning models can accurately predict a patient’s self-reported race from medical images alone—a capability that clinical experts do not possess—creating an enormous risk for entrenching health inequities if not actively mitigated.52 These precedents underscore the imperative to prioritize robust, multi-center validation and algorithmic fairness from the outset of model development.
Rigorous Clinical Validation: Most existing models are retrospective. Their clinical utility must be confirmed through prospective, multicenter Randomized Controlled Trials (RCTs) that demonstrate improved patient outcomes, not just predictive accuracy.53
Causality versus Correlation: AI models excel at identifying complex correlations, but clinical decisions require an understanding of causality. There is a significant risk of acting on spurious correlations. Future work must incorporate methods for causal inference to distinguish predictive markers from causal drivers of pain and treatment response.
Economic and Accessibility Barriers: The proposed framework requires extensive data collection (eg, WGS, serial imaging) that is not currently standard of care and would be prohibitively expensive for most healthcare systems. This raises concerns about cost-effectiveness and the potential for such advanced technologies to exacerbate existing healthcare disparities if not implemented equitably.
Data Privacy and Ethics: Strict adherence to data security and patient privacy regulations is mandatory.54 Regulatory approval and public trust are also essential for widespread adoption.55 Furthermore, the role of the patient in co-creating and governing their own “digital twin” must be considered, moving towards a model of shared decision-making.
A Proposed Research Roadmap
To systematically overcome these barriers, we propose a concrete, three-phase research roadmap:
Phase 1: Establish a Federated Data Network. Create a multi-institutional consortium to build a large-scale, standardized, multimodal cancer pain data repository. This network would use federated learning principles to protect patient privacy while enabling collaborative model development.
Phase 2: Launch a Benchmarking Challenge. Host an open, competitive challenge (analogous to ImageNet) to benchmark different AI models on the standardized tasks of pain subtyping and treatment response prediction using the federated dataset. This will accelerate methodological innovation and identify the most promising architectures.
Phase 3: Conduct a Prospective, AI-Driven Adaptive Clinical Trial. Design and execute an RCT where patients are randomized to either standard-of-care pain management or an AI-guided arm. In the AI arm, the “digital twin” model’s recommendations would guide treatment selection. The trial’s primary endpoint would be a clinically meaningful improvement in pain control.
Implementation via a “Hybrid Telemedicine and On-Site Expert” Model
Beyond technical development, translating AI into practice requires a robust delivery model, especially to bridge the care gap between major medical centers and grassroots institutions. We advocate for a “Hybrid Telemedicine and On-Site Expert” dual-track assistance model:
The “Cloud” Track: A centralized AI decision support system, embodying the trained “digital twin” models, is deployed via a digital health platform. This provides primary care clinics with real-time, expert-level guidance on pain assessment, subtyping, and treatment selection, accessible through remote consultation platforms.56,57 This standardizes care and disseminates expertise.
The “Entity” Track: This involves the physical dispatch of experts from hub hospitals to primary care clinics for periodic on-site training, co-management of complex cases, and quality control. This human-in-the-loop approach builds trust, addresses practical implementation challenges, and ensures the AI tools are used correctly and effectively, overcoming habit-based prescribing patterns.58
This integrated hub-and-spoke model, combining remote AI-driven decision support with on-site expert collaboration, can effectively disseminate high-quality medical resources and promote a tiered healthcare system for cancer pain management, ensuring more equitable access to precision care.
Conclusion and Future Perspectives
Cancer pain management is at a transformative crossroads. We have argued that the traditional “one-size-fits-all” model is obsolete and must be replaced by a precise, individualized strategy. We proposed a “digital twin” conceptual framework, powered by multimodal AI, as the engine for this transformation. This framework integrates genomics, clinical phenotypes, imaging, and medical text to enable simultaneous, precise subtyping and individualized treatment response prediction.
While significant challenges remain, particularly in data acquisition, model validation, and clinical integration, the path forward is becoming clearer. The research roadmap we have outlined—from federated data networks to prospective AI-driven trials—provides a concrete strategy for the field. Furthermore, the “Hybrid Telemedicine and On-Site Expert” implementation model offers a pragmatic solution for deploying these advanced tools to ensure equitable patient access.
Future advances in generative AI and LLMs may further enhance these capabilities, enabling intelligent clinical decision support, automated patient education, and accelerated scientific discovery. However, it is essential to approach this potential with a balanced and critical perspective, acknowledging the history of hype cycles in medical AI. This requires close collaboration among multidisciplinary teams, with a patient-centered approach, to jointly promote technological innovation, clinical validation, and the establishment of ethical frameworks. Ultimately, this paradigm shift will profoundly reshape the future of cancer pain treatment, bringing more effective pain relief and a more dignified life to millions of cancer patients worldwide.
Abbreviations
AI, Artificial Intelligence; ML, Machine Learning; NRS, Numerical Rating Scale; NeuP, Neuropathic Pain; NocP, Nociceptive Pain; NpIP, Nociplastic Pain; CDSS, Clinical Decision Support System; HER, Electronic Health Record; PROs, Patient-Reported Outcomes Measures.
Data Sharing Statement
The data used in this review are derived from publicly available literature and databases. All relevant studies and data sources have been cited in the main text, and the literature search strategy (including databases, time range, and key terms) is detailed in the “Methods” section. No new datasets were generated during the current study.
Ethics Approval and Consent to Participate
This study is a narrative review focusing on the synthesis and analysis of existing published research, without involving human subjects, animal experiments, or the collection/use of any individual-level data (including clinical samples, personal health information, etc.). Therefore, ethical approval from an ethics committee and informed consent from participants are not applicable to this work.
Acknowledgments
We would like to thank Dr. Chao Song (Pain Medicine Department, Anning First People’s Hospital Affiliated to Kunming University of Science and Technology, Anning, China) for his valuable contributions to the revision of this manuscript. As an expert in pain medicine, his critical review and insightful suggestions, particularly concerning the mechanisms of pain/clinical applications, significantly improved the quality of the paper.
Author Contributions
Wang made the primary contribution to this work and is the sole first author. Zhou and Sun are co-corresponding authors.
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that there is no specific funding support for this study.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Wirz S, Keßler J, Hofbauer H. Tumor-associated pain. Schmerz. 2024;38:57–12. doi:10.1007/s00482-023-00782-x
2. Mercadante S, Adile C, Aielli F, et al. Personalized pain goals and responses in advanced cancer patients. Pain Med. 2020;21(2):e215–e221. doi:10.1093/pm/pnz254
3. Ruan X, Lu X, Gao J, et al. Multiomics data reveals the influences of myasthenia gravis on thymoma and its precision treatment. J Cell Physiol. 2020;236(2):1214–1227. doi:10.1002/jcp.29928
4. Abida, Alzahrani AR, Alhuthali HM, et al. Personalized oncology in pheochromocytomas and paragangliomas: integrating genetic analysis with machine learning. Med Oncol. 2024;41(11):290. doi:10.1007/s12032-024-02532-0
5. Shay JW, Homma N, Zhou R. Abstracts from the 3rd international genomic medicine conference (3rd IGMC 2015): Jeddah, Kingdom of Saudi Arabia. 30 November - 3 December 2015. BMC Genomics. 2016;17 Suppl 6(Suppl 6):487. doi:10.1186/s12864-016-2858-0
6. Xiang J, Wang X, Zhang X, et al. A vision-language foundation model for precision oncology. Nature. 2025;638(8051):769–778. doi:10.1038/s41586-024-08378-w
7. Kather JN, Heij LR, Grabsch HI, et al. Pan-cancer image-based detection of clinically actionable genetic alterations. Nat Cancer. 2020;1(8):789–799. doi:10.1038/s43018-020-0087-6
8. Oldenburger E, Brown S, Willmann J, et al. ESTRO ACROP guidelines for external beam radiotherapy of patients with complicated bone metastases. Radiother Oncol. 2022;173:240–253. doi:10.1016/j.radonc.2022.06.002
9. Lee DY, Lee JJ, Richeimer SH. Cancer pain syndromes. Cancer Treat Res. 2021;182:17–25. doi:10.1007/978-3-030-81526-4_2
10. Fleisch J, Dahan A. Pain in cancer. Ned Tijdschr Geneeskd. 2018;161:D1447. PMID: 29424325.
11. Dhawan S, Andrews R, Kumar L, et al. A randomized controlled trial to assess the effectiveness of muscle strengthening and balancing exercises on chemotherapy-induced peripheral neuropathic pain and quality of life among cancer patients. Cancer Nurs. 2020;43(4):269–280. doi:10.1097/NCC.0000000000000693
12. Banderali U, Moreno M, Martina M. The elusive Nav1.7: from pain to cancer. Curr Top Membr. 2023;92:47–69. doi:10.1016/bs.ctm.2023.09.003
13. Santi MD, Zhang M, Asam K, et al. Perineural invasion is associated with function-evoked pain and altered extracellular matrix in patients with head and neck squamous cell carcinoma. J Pain. 2024;25(10):104615. doi:10.1016/j.jpain.2024.104615
14. Martinez V, Lehman T, Lavand’homme P, et al. Chronic postsurgical pain: a European survey. Eur J Anaesth. 2024;41(5):351–362. doi:10.1097/EJA.0000000000001974
15. Etli MU, Sarıkaya C, Onen MR, et al. Spinal hemangioblastomas and neuropathic pain. World Neurosurg. 2021;149:149e780–e784. doi:10.1016/j.wneu.2021.01.100
16. Verspyck E, Attal N. Diagnosing nociplastic pain in cancer survivors: a major step forward. Brit J Anaesth. 2023;130(5):515–518. doi:10.1016/j.bja.2023.02.006
17. Tsai JH, Liu IT, Su PF, et al. Lidocaine transdermal patches reduced pain intensity in neuropathic cancer patients already receiving opioid treatment. BMC Palliat Care. 2023;22(1):4. doi:10.1186/s12904-023-01126-3
18. Swarm RA, Paice JA, Anghelescu DL, et al. Adult cancer pain, version 3.2019, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Ne. 2019;17(8):977–1007. doi:10.6004/jnccn.2019.0038
19. Meeus M. Pain after cancer: time to move towards a mechanism-based approach! Anat Rec. 2023;307(2):243–247. doi:10.1002/ar.25309
20. Tsuchida R, Nishizawa D, Fukuda KI, et al. Genetic polymorphisms of ENPP2 are possibly associated with pain severity and opioid dose requirements in patients with inflammatory pain conditions: clinical observation study. Int J Mol Sci. 2023;24(8):6986. doi:10.3390/ijms24086986
21. Tang PC, Chung JY, Liao J, et al. Single-cell RNA sequencing uncovers a neuron-like macrophage subset associated with cancer pain. Sci Adv. 2022;8(40):eabn5535. doi:10.1126/sciadv.abn5535
22. Ye Y, Jensen DD, Viet CT, et al. Advances in head and neck cancer pain. J Dent Res. 2022;101(9):1025–1033. doi:10.1177/00220345221088527
23. Li Q, Zhang X. Epigallocatechin-3-gallate attenuates bone cancer pain involving decreasing spinal tumor necrosis factor-α expression in a mouse model. Int Immunopharmacol. 2015;29(2):818–823. doi:10.1016/j.intimp.2015.08.037
24. Morais MV, Lopes RA, Oliveira Júnior JO. Cordotomy for pain control and opioid reduction in cancer patients: a cancer center 11-year experience. EJSO-Eur J Surg Onc. 2024;50(10):108571. doi:10.1016/j.ejso.2024.108571
25. Reis-Pina P, Lawlor PG, Barbosa A. Adequacy of cancer-related pain management and predictors of undertreatment at referral to a pain clinic. J Pain Res. 2017;10:2097–2107. doi:10.2147/JPR.S139715
26. Shkodra M, Brunelli C, Zecca E, et al. Neuropathic pain: clinical classification and assessment in patients with pain due to cancer. Pain. 2021;162(3):866–874. doi:10.1097/j.pain.0000000000002076
27. Falk S, Gallego-Pedersen S, Petersen NC. Grid-climbing behaviour as a pain measure for cancer-induced bone pain and neuropathic pain. Vivo. 2017;31(4):619–623. doi:10.21873/invivo.11102
28. Brown SA, Jouni H, Marroush TS, et al. Disclosing genetic risk for coronary heart disease: attitudes toward personal information in health records. Am J Prev Med. 2017;52(4):499–506. doi:10.1016/j.amepre.2016.11.005
29. McCoy TH, Castro VM, Hart KL, et al. Genome-wide association study of dimensional psychopathology using electronic health records. Biol Psychiatry. 2018;83(12):1005–1011. doi:10.1016/j.biopsych.2017.12.004
30. Terracciano A, Luchetti M, Karakose S, et al. Loneliness and risk of parkinson disease. JAMA Neurol. 2023;80(11):1138–1144. doi:10.1001/jamaneurol.2023.3382
31. Wilcox H, Paz V, Saxena R, et al. The role of circadian rhythms and sleep in anorexia nervosa. JAMA Network Open. 2024;7(1):e2350358. doi:10.1001/jamanetworkopen.2023.50358
32. Xu B, Forthman KL, Kuplicki R, et al. Genetic correlates of treatment-resistant depression. JAMA Psychiatry. 2025;82(5):505. doi:10.1001/jamapsychiatry.2024.4825
33. El Nahhas OSM, van Treeck M, Wölflein G, et al. From whole-slide image to biomarker prediction: end-to-end weakly supervised deep learning in computational pathology. Nat Protoc. 2024;20(1):293–316. doi:10.1038/s41596-024-01047-2
34. Luh F, Yen Y. Cybersecurity in science and medicine: threats and challenges. Trends Biotechnol. 2020;38(8):825–828. doi:10.1016/j.tibtech.2020.02.010
35. Salama V, Godinich B, Geng Y, et al. Artificial intelligence and machine learning in cancer related pain: a systematic review. medRxiv. 2023. doi:10.1101/2023.12.06.23299610
36. Colombo AAF, Colombo L, Falcetta A, et al. Enhancing privacy-preserving cancer classification with convolutional neural networks. Pac Symp Biocomput. 2025;30:565–579. doi:10.1142/9789819807024_0040
37. Ehteshami Bejnordi B, Veta M, Johannes van Diest P, et al. Diagnostic assessment of deep learning algorithms for detection of lymph node metastases in women with breast cancer. JAMA-J Am Med Assoc. 2017;318(22):2199–2210. doi:10.1001/jama.2017.14585
38. Wu S, Hong G, Xu A, et al. Artificial intelligence-based model for lymph node metastases detection on whole slide images in bladder cancer: a retrospective, multicentre, diagnostic study. Lancet Oncol. 2023;24(4):360–370. doi:10.1016/S1470-2045(23)00061-X
39. Wu D, Yang J, Liu C, et al. GestaltMML: enhancing rare genetic disease diagnosis through multimodal machine learning combining facial images and clinical texts. ArXiv. 2024. PMID: 38711434.
40. Raisaro JL, Troncoso-Pastoriza JR, Misbach M, et al. MedCo: enabling secure and privacy-preserving exploration of distributed clinical and genomic data. IEEE ACM T Comput Bi. 2018;16(4):1328–1341. doi:10.1109/TCBB.2018.2854776
41. Afridi M, Jain A, Aboian M, et al. Brain tumor imaging: applications of artificial intelligence. Semin Ultrasound CT MR. 2022;43(2):153–169. doi:10.1053/j.sult.2022.02.005
42. Wolf LE, Hammack CM, Brown EF, et al. Protecting participants in genomic research: understanding the “web of protections” afforded by federal and state law. J Law Med Ethics. 2020;48(1):126–141. doi:10.1177/1073110520917000
43. Hauschild AC, Lemanczyk M, Matschinske J, et al. Federated random forests can improve local performance of predictive models for various healthcare applications. Bioinformatics. 2022;38(8):2278–2286. doi:10.1093/bioinformatics/btac065
44. Raper AC, Weathers BL, Drivas TG, et al. Protocol for a type 3 hybrid implementation cluster randomized clinical trial to evaluate the effect of patient and clinician nudges to advance the use of genomic medicine across a diverse health system. Implement Sci. 2024;19(1):61. doi:10.1186/s13012-024-01385-5
45. Chams C, Borda De Agua Reis A, Berna C, et al. Chronic cancer pain: pathophysiology and ICD-11 classification. Rev Med Suisse. 2022;18(787):1259–1263. doi:10.53738/REVMED.2022.18.787.1259
46. Brown P, Ryder A, Robinson C, et al. Methadone for chronic pain: a review of pharmacology, efficacy, and safety concerns. Health Psychol Res. 2025;13(1):129552. doi:10.52965/001c.129552
47. Wang F, Zhao J, Li Y, et al. Acupuncture and acupressure with improved cancer-related depression of retrospective studies. Front Oncol. 2022;12:1036634. doi:10.3389/fonc.2022.1036634
48. Tian TT, Chen G, Sun K, et al. ChanLingGao alleviates intestinal mucosal barrier damage and suppresses the onset and progression of Colorectal cancer in AOM/DSS murine model. Int Immunopharmacol. 2024;143(Pt 1):113193. doi:10.1016/j.intimp.2024.113193
49. Liu Y, Wu Y, Xia Q, et al. An explainable predictive machine learning model for axillary lymph node metastasis in breast cancer based on multimodal data: a retrospective single-center study. J Transl Med. 2025;23(1):892. doi:10.1186/s12967-025-06686-x
50. Han R, Acosta JN, Shakeri Z, et al. Randomised controlled trials evaluating artificial intelligence in clinical practice: a scoping review. Lancet Digit Health. 2024;6(5):e367–e373. doi:10.1016/S2589-7500(24)00047-5
51. Ghassemi M, Oakden-Rayner L, Beam AL. The false hope of current approaches to explainable artificial intelligence in health care. Lancet Digit Health. 2021;3(11):e745–e750. doi:10.1016/S2589-7500(21)00208-9
52. Gichoya JW, Banerjee I, Bhimireddy AR, et al. AI recognition of patient race in medical imaging: a modelling study. Lancet Digit Health. 2022;4(6):e406–e414. doi:10.1016/S2589-7500(22)00063-2
53. Lee TC, Shah NU, Haack A, et al. Clinical implementation of predictive models embedded within electronic health record systems: a systematic review. Informatics. 2020;7(3). doi:10.3390/informatics7030025
54. Ahmed Z. Practicing precision medicine with intelligently integrative clinical and multi-omics data analysis. Hum Genomics. 2020;14(1):35. doi:10.1186/s40246-020-00287-z
55. Waters EA, Taber JM, McQueen A, et al. Translating cancer risk prediction models into personalized cancer risk assessment tools: stumbling blocks and strategies for success. Cancer Epidem Biomar. 2020;29(12):2389–2394. doi:10.1158/1055-9965.EPI-20-0861
56. Zhang X, Qiao S, Zhang R, et al. Construction and application of chain management information system for cancer pain. Pain Manag Nurs. 2023;24(4):e75–e80. doi:10.1016/j.pmn.2023.04.004
57. Gali K, Narode R, Young-Wolff KC, et al. Online patient-provider cannabis consultations. Prev Med. 2020;132:105987. doi:10.1016/j.ypmed.2020.105987
58. Jeong A, Wade K. Dexamethasone prescribing for cancer pain between palliative care and radiation oncology. Support Care Cancer. 2022;30(9):7689–7696. doi:10.1007/s00520-022-07203-2
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.