Back to Journals » Journal of Inflammation Research » Volume 19
Research Progress on Traditional Chinese Medicine Preparations in Respiratory Inflammatory Diseases
Authors Liu X, Liu B, Wang S, Tian Y, Liu Y, Cui X, Zhang S
Received 10 June 2025
Accepted for publication 8 January 2026
Published 29 January 2026 Volume 2026:19 545874
DOI https://doi.org/10.2147/JIR.S545874
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Cynthia Koziol-White
Xiuli Liu,1 Bo Liu,1 Shengsheng Wang,2 Yang Tian,1 Ying Liu,1 Xiaoli Cui,1 Shuisheng Zhang3
1Department of Rehabilitation, Jilin Academy of Chinese Medicine Sciences, Changchun, 130022, People’s Republic of China; 2Clinical Drug Trial Institution, Jilin Academy of Chinese Medicine Sciences, Changchun, 130022, People’s Republic of China; 3Department of Geriatrics, Jilin Academy of Chinese Medicine Sciences, Changchun, 130022, People’s Republic of China
Correspondence: Shuisheng Zhang, Department of Geriatrics, Jilin Academy of Chinese Medicine Sciences, No. 6426, Ziyou Road, Nanguan District, Changchun, 130022, Jilin Province, People’s Republic of China, Email [email protected]
Abstract: The global burden of respiratory inflammatory diseases, such as asthma, chronic bronchitis, and chronic obstructive pulmonary disease (COPD), continues to rise, highlighting the urgent need for safer and more effective therapeutic strategies. Conventional treatments provide symptomatic relief but remain limited by adverse effects, tolerance, and incomplete resolution of inflammation. In recent years, traditional Chinese medicine (TCM) formulations have gained growing attention as promising complementary or alternative approaches due to their holistic and multi-targeted pharmacological actions. This review summarizes current preclinical and clinical evidence on the application of classical TCM preparations—including Xuebijing, Qingkailing, Xiyanping, Tanreqing, Chuankezhi, Shuanghuanglian, and Yejuhua injections—in the management of respiratory inflammatory diseases. These herbal treatments exhibit significant anti-inflammatory, antioxidative, and immunomodulatory effects through modulation of key signaling pathways such as NF-κB, MAPK, and TLRs. Importantly, clinical studies suggest that these TCM preparations can alleviate respiratory symptoms, reduce disease exacerbations, and enhance patient quality of life, highlighting their potential clinical significance and translational value in managing respiratory inflammatory diseases.
Keywords: traditional Chinese medicine, preparations, respiratory inflammatory disease
Introduction
Respiratory inflammatory diseases comprise a broad spectrum of disorders characterized by acute or chronic inflammation of the airways and pulmonary tissues, including asthma, chronic obstructive pulmonary disease (COPD), bronchitis, pneumonia and coronavirus disease 2019 (COVID-19).1–3 Their pathogenesis involves complex interactions between environmental factors-such as pathogens, pollutants, and allergens-and dysregulated immune responses. Upon exposure to these external stimuli, aberrant immune activation drives excessive production of inflammatory mediators, recruitment of immune cells, and oxidative stress. This pathological cascade disrupts epithelial barriers, promotes airway remodeling, and ultimately leads to tissue injury and progressive impairment of respiratory function.4,5 Globally, respiratory inflammatory diseases impose a substantial health burden. Lower respiratory tract infections alone account for over 2 million deaths annually, while the global prevalence of asthma exceeds 300 million cases.6,7 Clinically, these diseases are commonly manifested by symptoms such as coughing, wheezing, dyspnea, and excessive mucus production. Respiratory inflammatory diseases are also associated with cardiovascular and metabolic comorbidities, potentially linked through shared molecular mechanisms and risk factors, which can further compromise patients’ quality of life and overall prognosis.8
The current treatment strategies predominantly rely on pharmacological interventions, including corticosteroids, nonsteroidal anti-inflammatory drugs (NSAIDs), antibiotics, bronchodilators, and phosphodiesterase-4 (PDE4) inhibitors like roflumilast.9–13 While these therapies provide symptomatic relief and reduce disease exacerbations, they are largely supportive and lack specific targeted treatments, resulting in considerable variability in guidelines across different regions and hospitals regarding the types and dosages of medications used. They often fail to address the underlying pathophysiological mechanisms, particularly in chronic and progressive conditions.13 Additionally, prolonged antibiotic use has led to the emergence of antimicrobial resistance. Novel therapeutic approaches-including gene therapy and cell-based inventions-have demonstrated promise but are still in early developmental stages. For instance, gene therapies targeting respiratory inflammatory diseases like COVID-19 remain largely confined to preclinical or early-phase studies.14 Similarly, mesenchymal stromal cell (MSC) therapy, despite showing immunomodulatory and regenerative potential in preclinical studies, has not yet yielded consistent clinical benefits in trials for COPD and acute respiratory distress syndrome (ARDS). This discrepancy is partly attributable to variability in cell viability, host-microenvironment interactions, and incomplete understanding of the underlying mechanisms of action.15
Traditional Chinese medicine (TCM) has been applied for over two millennia in Asia to treat upper respiratory tract infections and common colds. Detailed accounts of respiratory tract symptoms, complications, treatment strategies, and underlying principles were documented in the ShanghanZabinglun, authored by Zhang Zhongjing during China’s Han Dynasty (150–219 A.D).16 Among its many forms, traditional Chinese medicine preparations represent a critical component and have demonstrated therapeutic efficacy in managing various respiratory conditions.17–19 A “TCM preparation” refers to a formulation prepared under the guidance of TCM theory, and composed of multiple medicinal materials, including plants, animals, or minerals, in defined dosages.20 TCM preparations have played a key role in the prevention and treatment of infectious diseases, such as SARS in 2003 and COVID-19 more recently, where they demonstrated safety and clinical efficacy through anti-inflammatory, antioxidant, and anti-apoptotic effects.18 Despite their extensive use, challenges remain in terms of standardization, quality control, and international recognition, but they continue to represent an important component of modern complementary and alternative medicine. This review aims to systematically summarize the current research progress on the application of TCM preparations in the treatment of respiratory inflammatory diseases, with a focus on their constituents, pharmacological mechanisms, clinical evidence, and potential for integration into modern medical practice.
Common Traditional Chinese Medicine Preparations Against Respiratory Inflammatory Diseases
Xuebijing
Xuebijing (XBJ) is a traditional Chinese patent medicine developed for the management of sepsis. Since its initial approval in 2004, XBJ has been utilized in clinical practice in China for nearly two decades, and in 2020 it received authorization from the National Medical Products Administration for the treatment of severe COVID-19.21,22
Constituents
Xuebijing is a traditional Chinese patent medicine, composed of five medicinal herbs including Paeoniae Radix Rubra (Chishao), Chuanxiong Rhizoma (Chuanxiong), Salviae Militiorrhizae Radix et Rhizuma (Danshen), Carthami Flos (Honghua) and Angelicae Sinensis Radix (Danggui).21,23 Its pharmacological effects are attributed to a diverse array of bioactive constituents derived from these herbs. The main components include Paeoniflorin from Paeoniae Radix Rubra,24 ligustrazine from Chuanxiong Rhizoma,25 Salvianolic acid B and tanshinone IIA from Salviae Militiorrhizae Radix et Rhizuma,26 Safflower yellow from Carthami Flos,27 as well as ligustilide and ferulic acid from Angelicae Sinensis Radix28 (Figure 1 and Table 1). These compounds collectively contribute to its anti-inflammatory, antioxidant, anticoagulant, and immunomodulatory properties of Xuebijing, supporting its widespread use in the management of sepsis and inflammatory respiratory diseases.
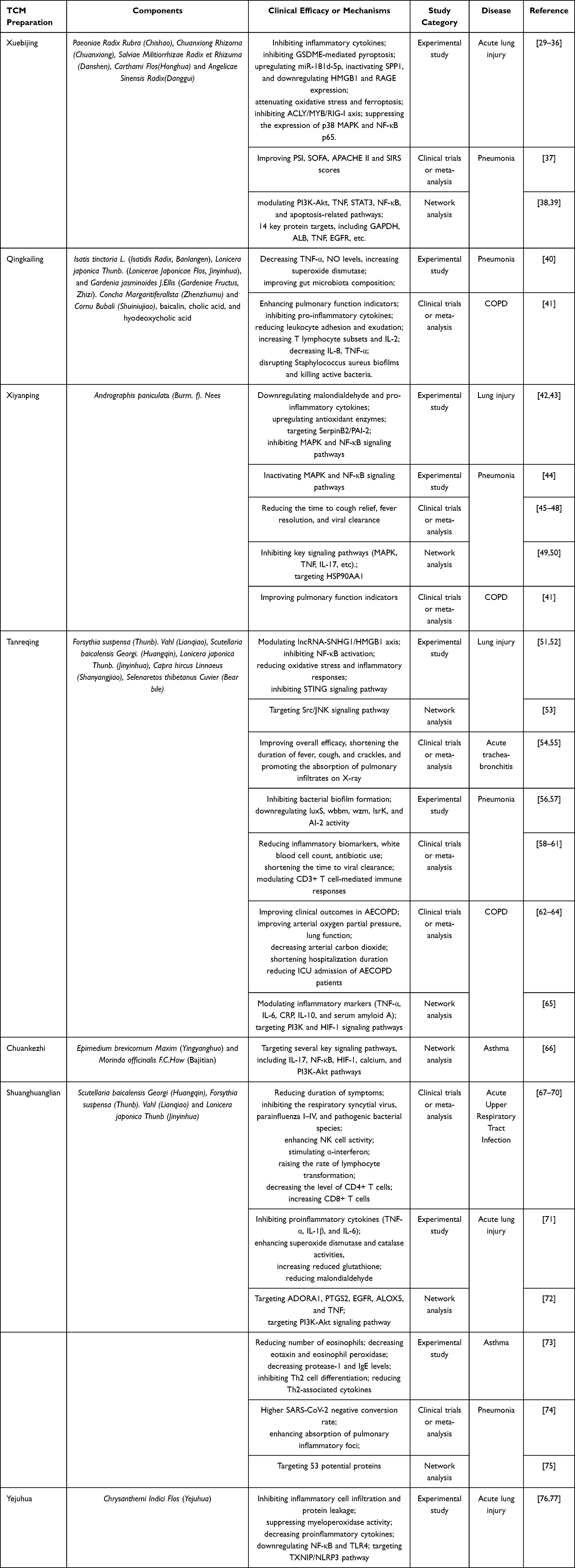 |
Table 1 Components, Clinical Efficacy in Respiratory Inflammatory Diseases, Mechanisms of Traditional Chinese Medicine Preparations |
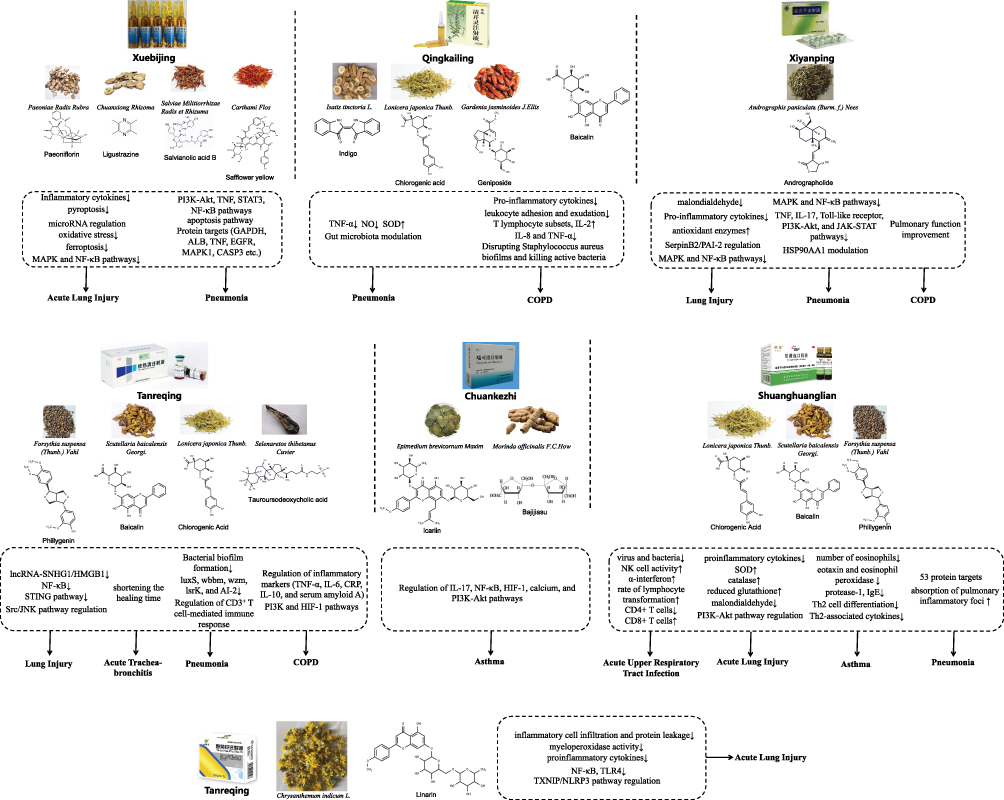 |
Figure 1 Constituents, mechanisms and associated diseases of seven traditional Chinese medicine prepations (Xuebijing, Qingkailing, Xiyanping, Tanreqing, Chuankezhi, Shuanghuanglian, Yejuhua). |
Treatment
Acute Lung Injury
Xuebijing has demonstrated significant therapeutic potential in the treatment of acute lung injury (ALI) by modulating key inflammatory pathways. It inhibits the production of inflammatory cytokines such as tumor necrosis factor-α (TNF-α), interleukin-6 (IL-6) and interleukin-1β (IL-1β), as well as proteins associated with inflammation and pyroptosis.29 One of the mechanisms by which Xuebijing exerts its protective effect involves suppressing TNF-α expression, thereby inhibiting gasdermin E (GSDME)-mediated pyroptosis in pulmonary cells.30 In addition, Xuebijing exerts protective effects against ALI induced by left ventricular ischemia/reperfusion in rabbit models.31 Mechanistically, it alleviates inflammatory response by upregulating miR-181d-5p to inactivate secreted phosphoprotein 1 (SPP1), while downregulating high mobility group box protein 1 (HMGB1) and receptor for advanced glycation end products (RAGE) expression.32,33 Moreover, Xuebijing ameliorated sepsis-induced ALI by reducing oxidative stress and ferroptosis, and by improving endothelial function through inhibition of the ATP citrate lyase (ACLY)/MYB/retinoic acid-inducible gene I (RIG-I) axis.29,34,35 It has also been reported to suppress the expression of p38 mitogen-activated protein kinase (MAPK) and nuclear factor-κB (NF-κB) p65 in paraquat-induced ALI models.36 Despite broad mechanistic activity, most findings are preclinical, and the relative importance of these pathways for actual clinical improvement remains unclear. These uncertainties highlight the need for studies linking pathway modulation with validated ALI outcomes.
Pneumonia
Xuebijing demonstrates notable therapeutic efficacy in patients with severe community-acquired pneumonia (SCAP), particularly in cases characterized by elevated lymphocyte counts and reduced neutrophil levels. A post hoc analysis of a randomized, double-blind, placebo-controlled clinical trial (n = 675) evaluated the efficacy of Xuebijing in severe community-acquired pneumonia (SCAP). Results showed that Xuebijing improved key clinical assessment scores, including the pneumonia severity index (PSI), sequential organ failure assessment (SOFA) score, acute physiology and chronic health evaluation II (APACHE II) score, and systemic inflammatory response syndrome (SIRS) score.37 In the context of COVID-19-induced acute respiratory distress syndrome (ARDS), Xuebijing has shown anti-inflammatory, anti-apoptotic, and immunoregulatory properties by modulating the phosphoinositide 3-kinase (PI3K)-Akt, TNF, signal transducer and activator of transcription 3 (STAT3), NF-κB, and apoptosis-related pathways.38 Proteomic analyses in COVID-19 patients have identified 14 key protein targets of Xuebijing, including glyceraldehyde 3-phosphate dehydrogenase (GAPDH), albumin (ALB), TNF, epidermal growth factor receptor (EGFR), MAPK1, caspase-3 (CASP3), STAT3, MAPK8, prostaglandin-endoperoxide synthase 2 (PTGS2), JUN, interleukin-2 (IL-2), estrogen receptor 1 (ESR1), and MAPK14.39 Furthermore, Xuebijing has also been shown to exert inhibitory effects on radiation-induced pneumonitis.78 However, current evidence mainly reflects improvements in clinical scores, and its impact on hard outcomes (eg, mortality, ventilation duration) remains uncertain. More rigorous trials are needed to clarify its role as an adjunct therapy and identify patients most likely to benefit.
Qingkailing
Qingkailing (QKL) injection was first developed in the 1970s at the Beijing University of Chinese Medicine as a modification of the classical formula Angong Niuhuang pills, which has been employed in China for centuries. At present, QKL is extensively applied in clinical practice for the management of fever, upper respiratory tract infections, pneumonia, and hepatitis, with utility in treating cold and influenza symptoms in pediatric populations.79,80
Constituents
Qingkailing is a traditional Chinese medicine formulation comprising a combination of botanical, animal-derived, and bioactive components. Its primary herbal ingredients include Isatis tinctoria L. (Isatidis Radix, Banlangen), Lonicera japonica Thunb. (Lonicerae Japonicae Flos, Jinyinhua), and Gardenia jasminoides J.Ellis (Gardeniae Fructus, Zhizi). Additionally, it contains two animal-derived substances, Concha Margaritiferallsta (Zhenzhumu) and Cornu Bubali (Shuiniujiao), as well as three bioactive compounds: baicalin (BA), cholic acid (CA), and hyodeoxycholic acid (HA).81 The main pharmacologically active constituents include indigo from Isatis tinctoria L.,82 chlorogenic acid from Lonicera japonica Thunb.,83 Geniposide from Gardenia jasminoides J.Ellis.84 Moreover, Concha Margaritifera and Cornu Bubali provide essential amino acids and trace elements.85 Colletively, these components act synergistically with BA, CA, and HA to confer Qingkailing’s therapeutic properties (Figure 1).
Treatment
Pneumonia
In pneumonia, Qingkailing has been shown to exert anti-inflammatory and antioxidative effects by decreasing TNF-α, nitric oxide (NO) levels, while increasing superoxide dismutase (SOD) level.40 Additionally, Qingkailing improves gut microbiota composition by enhancing the richness and alpha diversity of intestinal flora and restoring multiple intestinal genera associated with inflammation. By significantly enriching beneficial microbiota (eg, Bifidobacterium, Ruminococcus_torques_group, and Dorea) while reducing the abundance of potentially pathogenic bacteria (eg, Staphylococcus, Mucispirillum, and Aerococcus), Qingkailing alleviates pneumonia symptoms. Collectively, these data begin to link Qingkailing’s anti-inflammatory and antioxidative effects with modulation of the gut-lung axis, providing a mechanistic framework for how this formulation may ameliorate pneumonia. Nevertheless, most evidence comes from preclinical or small-scale studies. It remains to be established in larger, well-controlled trials whether microbiota shifts and oxidative stress reduction translate into meaningful improvements in clinical outcomes.
COPD
In the context of COPD, a meta-analysis, which included 57 randomized controlled trials (RCTs), revealed that Qingkailing injection combined with routine treatment was superior to routine treatment alone in treating acute exacerbation COPD (AECOPD). The combination therapy effectively enhances pulmonary function indicators, including forced expiration volume (FEV1), forced vital capacity (FVC) as well as parameters from arterial blood gas analysis index. The therapeutic effects of Qingkailing in COPD are mainly attributed to its multiple pharmacological actions. Specifically, Qingkailing inhibits pro-inflammatory cytokines such as TNF-α and IL-6, reduces leukocyte adhesion and exudation, enhances immune function by increasing T lymphocyte subsets and IL-2 levels while decreasing IL-8 and TNF-α, and exhibits antibacterial effects by disrupting Staphylococcus aureus biofilms and killing active bacteria. These combined mechanisms provide a scientific basis for its clinical efficacy and highlight its potential as an adjunctive therapeutic strategy for COPD management.41 However, it should be noted that most of the included RCTs in this meta-analysis were of small sample size and limited methodological quality, with insufficient reporting of randomization, allocation concealment, and blinding. Therefore, while the findings suggest potential benefits of Qingkailing, they should be interpreted with caution until further high-quality, large-scale RCTs are available. Taken together, the meta-analysis and mechanistic studies support the view that Qingkailing may complement standard AECOPD therapy by simultaneously targeting airway inflammation, immune dysregulation and bacterial persistence. However, given the generally low methodological quality of the available RCTs, these benefits should still be regarded as provisional and require confirmation in rigorously designed, large-scale trials before firm recommendations can be made.
Xiyanping
Xiyanping (XYP) is a proprietary Chinese medicine that has been clinically applied for over three decades in the management of upper respiratory tract infections, viral pneumonia, influenza, and bronchitis. It exhibits notable anti-inflammatory and antiviral properties and is widely utilized in clinical practice for the treatment of respiratory infections and pneumonia.45
Constituents
Xiyanping is a modern Chinese patent medicine derived from andrographolide, the primary active compound extracted from Andrographis paniculata (Burm. f). Nees.86 It exhibits potent antiviral and antibacterial activities, along with a favorable safety profile and minimal risk of inducing antibiotic resistance.87 The mainbioactive constituent of Xiyanping is andrographolide sulfate, a water-soluble derivative that enhances its bioavailability and therapeutic efficacy88 (Figure 1).
Treatment
Lung Injury
Infection with Influenza A virus (IAV) triggers intense inflammatory responses and severe lung injury, contributing substantially to morbidity and mortality. Xiyanping injection has shown clinical efficacy against a range of viral infections. In IAV-infected mice, Xiyanping significantly reduces mortality, lung viral titers, and pathological lung damage. These protective effects are associated with the downregulation of malondialdehyde (MDA) activity and multiple pro-inflammatory cytokines, as well as the upregulation of antioxidant enzymes, including glutathione peroxidase (GSH-Px) and superoxide dismutase (SOD), and the elevation of interferon-γ (IFN-γ) levels.42 Notably, SerpinB2/PAI-2 has been identified as a critical molecular target of Xiyanping. In lipopolysaccharide (LPS)-induced acute lung injury models, andrographolide (the active component of Xiyanping) alleviates inflammatory cell infiltration and histopathological changes in lung tissue. This effect is accompanied by reduced pro-inflammatory cytokines in bronchoalveolar lavage fluid (BALF), serum, and lung tissue through inhibition of the MAPK and NF-κB signaling pathways.43 Both MAPK and NF-κB signaling pathways are considered master regulators of inflammatory responses, as they play critical roles in the evolution as well as the resolution phase of inflammation.89 Collectively, these studies establish a mechanistic framework linking Xiyanping’s antiviral, antioxidative, and anti-inflammatory properties to its lung-protective effects. Nevertheless, the evidence base remains predominantly preclinical, and the relative contribution of each pathway to clinically meaningful outcomes await clarification through rigorously designed human trials.
Pneumonia
A retrospective cohort study reveals that, in patients with community-acquired pneumonia (CAP), Xiyanping injection combined with conventional therapy using cephalosporins and antibiotics is superior to conventional treatment alone.46 In Klebsiella pneumoniae-induced pneumonia, the combination of Xiyanping and azithromycin significantly inhibits bacterial proliferation in lung tissue, improves lung histopathology, and reduces inflammatory mediator levels in lung homogenates and BALF. These effects are primarily attributed to the inactivation of MAPK and NF-κB signaling pathways.44 Evidence from a meta-analysis of 34 studies encompassing 3,111 elderly participants showed that in elderly patients with pneumonia, Xiyanping combined with Western medicine yields better clinical outcomes.47 In a prospective, multicenter, open-label and randomized controlled trial, Zhang et al demonstrated that Xiyanping significantly reduced the time to cough relief, fever resolution, and viral clearance in COVID-19 patients, with no severe adverse events reported.45 A meta-analysis further confirmed the efficacy and safety of Xiyanping, supporting its recommendation as a treatment option for COVID-19.48 Network pharmacology studies have shown that Xiyanping exerts its anti-inflammatory effects by inhibiting key signaling pathways, including MAPK, TNF, IL-17, Toll-like receptor, PI3K-Akt, and JAK-STAT pathways.49 Heat shock protein HSP90AA1 has been identified as a potential target of Xiyanping in COVID-19 therapy.50 These findings collectively suggest that Xiyanping may confer broad-spectrum therapeutic benefits across viral and bacterial pneumonias through modulation of shared inflammatory signaling pathways.
COPD
Similar to Qingkailing, Xiyanping has been reported to significantly improve pulmonary function indicators such as FEV1, FVC and arterial blood gas parameters in patients with AECOPD.41
Tanreqing
Tanreqing (TRQ) injection is widely utilized in clinical practice in China for the treatment of acute upper respiratory tract infections and early-stage pneumonia. It has been approved by the China Food and Drug Administration as a patented Chinese herbal injection. Pharmacological studies have shown that TRQ possesses antiviral activity against multiple respiratory viruses and antibacterial effects against common respiratory pathogens.54
Constituents
Tanreqing injection is a traditional Chinese medicine formulation composed of Forsythia suspensa (Thunb). Vahl (Lianqiao), Scutellaria baicalensis Georgi. (Huangqin), Lonicera japonica Thunb. (Jinyinhua), Capra hircus Linnaeus (Shanyangjiao), and Selenaretos thibetanus Cuvier (Bear bile).90 The primary bioactive constituents of Tanreqing are Phillyrin and Phillygenin derived from Forsythia suspensa (Thunb). Vahl,91 baicalin from Scutellaria baicalensis Georgi., and chlorogenic acid from Lonicera japonica Thunb. Additionally, amino acids from Capra hircus Linnaeus and tauroursodeoxycholic acid from Selenaretos thibetanus Cuvier contribute to the pharmacological profile of the formulation (Figure 1). These compounds collectively confer Tanreqing with anti-inflammatory, antiviral, antibacterial, and immunomodulatory properties, supporting its use in the treatment of respiratory inflammatory diseases.
Treatment
Lung Injury
In LPS-induced ALI, Tanreqing injection mitigates macrophage activation and the inflammatory response by modulating the lncRNA-SNHG1/HMGB1 axis. LncRNA-SNHG1 promotes LPS-induced M1 macrophage activation and inflammatory cytokine production by interacting with HMGB1, and is directly regulated by NF-κB. Tanreqing inhibits NF-κB activation and SNHG1 expression.51 Besides, Tanreqing protects against LPS-induced ALI by reducing oxidative stress and inflammatory responses. This protective effect is associated with inhibition of the STING signaling pathway, which is activated by mtDNA release. The use of a STING agonist (DMXAA) reverses Tanreqing’s effects, confirming the pathway’s key role in its mechanism.52 Network pharmacology analyses further suggest that the Src/JNK signaling pathway plays a pivotal regulatory role in Tanreqing’s therapeutic action against ALI.53 These findings help delineate how Tanreqing targets innate immune signaling and oxidative injury in ALI, offering a mechanistic basis for its multi-pathway efficacy. However, most evidence derives from animal models or in vitro systems, and the clinical relevance of these pathways awaits confirmation in human studies.
Acute Trachea-Bronchitis
Tanreqing has demonstrated clinical efficacy in the management of acute trachea-bronchitis. A meta-analysis including 49 studies with a total of 5131 participants indicated that Tanreqing may have beneficial effects in improving overall efficacy, shortening the duration of fever, cough, and crackles, and promoting the absorption of pulmonary infiltrates on X-ray.54 Moreover, a prospective, multi-center, randomized, double-blinded, parallel-group, placebo-controlled trial, which included 270 acute bronchitis patients, provides evidence-based support for the use of Tanreqing in acute bronchitis management.55 This consistency between meta-analytic and randomized trial data offers supportive evidence for Tanreqing’s symptomatic benefits in acute airway infections.
Pneumonia
Ventilator-associated pneumonia (VAP), a common complication of mechanical ventilation, is effectively managed by Tanreqing through the reduction of inflammatory biomarkers such as C-reactive protein (CRP), procalcitonin, and white blood cell count, while concurrently reducing the need for antibiotic use.58 In Streptococcus pneumoniae-induced pneumonia, Tanreqing combined with antibiotics enhances the overall treatment efficacy compared to Western medicine alone.59 One of its mechanisms involves inhibition of bacterial biofilm formation.56 In Klebsiella pneumoniae infections, Tanreqing suppresses biofilm development by downregulating the expression of luxS, wbbm, wzm, lsrK, and AI-2 activity.57 It also demonstrates potential benefits in severe pneumonia cases.60 A retrospective cohort study including 82 patients revealed that during the COVID-19 pandemic, Tanreqing shortened the time to viral clearance in fecal and pharyngeal samples, potentially by modulating CD3+ T cell-mediated immune responses.61
COPD
A meta-analysis by Zhong et al indicated that Tanreqing plus conventional Western therapy could significantly improve clinical outcomes in AECOPD, with or without respiratory failure, compared to Western medicine alone.62 This combination therapy improves arterial oxygen partial pressure, enhances lung function, decreases arterial carbon dioxide levels, and shortens hospitalization duration.63 In an ongoing, nationwide multicenter registry study, which included 4135 patients, Tanreqing also reduces ICU admission of AECOPD patients.64 Mechanistically, it modulates inflammatory markers such as TNF-α, IL-6, CRP, IL-10, and serum amyloid A, and exerts regulatory effects through the PI3K and hypoxia-inducible factor-1 (HIF-1) signaling pathways.65 These above findings suggest that Tanreqing may complement standard AECOPD management by targeting acute inflammation and hypoxia-related pathways.
Chuankezhi
Chuankezhi is a traditional Chinese medicine derived from two traditional Chinese herbs, both historically used in East Asia for kidney-yang tonification and the management of conditions such as osteoporosis and airway inflammation. In 2001, CKZ was approved by the National Medical Products Administration of China as an injectable formulation for reinforcing kidney-yang. Clinically, it has since been applied in the treatment of respiratory diseases linked to kidney-yang deficiency, including recurrent respiratory infections, asthma, and COPD.92
Constituents
Chuankezhi is a traditional Chinese medicine refined from two classical herbal sources: Epimedium brevicornum Maxim (Yingyanghuo) and Morinda officinalis F.C.How (Bajitian).92 The primary bioactive constituents include icariin, extracted from Epimedium brevicornum Maxim,93 and Bajijiasu, isolated from Morinda officinalis F.C.How (Figure 1).
Treatment
Asthma
Chuankezhi injection serves as an effective adjunctive therapy for bronchial asthma within the framework of traditional Chinese medicine. Studies have shown that its anti-asthmatic effects are primarily mediated through several key signaling pathways, including the IL-17, NF-κB, HIF-1, calcium, and PI3K-Akt pathways.66
Shuanghuanglian
Shuanghuanglian is a classical TCM formula historically documented in ancient medical texts and officially recorded in the Chinese Veterinary Pharmacopoeia. With a clinical application history spanning over 1,800 years, it has demonstrated notable anti-inflammatory properties. Contemporary studies have further validated its efficacy in the management of respiratory diseases of both bacterial and viral etiology.94,95
Constituents
Shuanghuanglian is a classical TCM preparation, composed of Scutellaria baicalensis Georgi (Huangqin), Forsythia suspensa (Thunb). Vahl (Lianqiao) and Lonicera japonica Thunb (Jinyinhua).94,95 Its major chemical compounds are chlorogenic acid, baicalin, Phillygenin and Phillyrin96 (Figure 1). When administered at appropriate doses, Shuanghuanglian has demonstrated a favorable safety profile.97
Treatment
Acute Upper Respiratory Tract Infection
Acute upper respiratory tract infections (AURTIs) refer to illnesses caused by viral or bacterial pathogens affecting the upper respiratory tract, including the common cold, laryngitis, pharyngitis/tonsillitis, acute rhinitis, acute rhinosinusitis, and acute otitis media. Evidence from a randomised single blind trial shows that Shuanghuanglian reduces duration of symptoms, such as fever, cough, wheezing and chest crackles, compared with antibiotics group.67 Additionally, Shuanghuanglian injection demonstrates broad-spectrum antiviral and antibacterial properties, inhibiting the respiratory syncytial virus, parainfluenza I–IV, and up to 23 pathogenic bacterial species, including Staphylococcus aureus and Pseudomonas aeruginosa.68 Immunologically, Shuanghuanglian enhances the natural killer (NK) cell activity, stimulates the production of alpha-interferon, raises the rate of lymphocyte transformation,69 and modulates T-cell by decreasing the level of CD4+ cells and the ratio of CD4+/CD8+ while increasing CD8+.70 By integrating antiviral, antibacterial, and immune-modulating actions, these studies offer a coherent biological rationale for Shuanghuanglian in AURTI management. However, rigorous, placebo-controlled trials remain limited, and its independent therapeutic value beyond symptomatic relief still requires firm clinical validation.
ALI
In LPS-induced ALI models, Shuanghuagnlian significantly reduces the lung wet/dry weight ratio, total cell counts in BALF, and the myeloperoxidase activity in lung tissues. On a molecular level, Shuanghuagnlian inhibits the excessive release of proinflammatory cytokines (TNF-α, IL-1β, and IL-6) in the BALF. Pathologically, it can attenuate interstitial edema, hemorrhage, and neutrophil infiltration in the lung tissue, while enhancing antioxidant defenses such as superoxide dismutase and catalase activities, increasing reduced glutathione content, and reducing malondialdehyde content.71 After oral administration, 92 transitional components in blood were identified, including 28 prototype components and 64 metabolites. Target prediction revealed key anti–acute lung injury targets, including adenosine A1 receptor (ADORA1), prostaglandin-endoperoxide synthase 2 (PTGS2), epidermal growth factor receptor (EGFR), arachidonate 5-lipoxygenase (ALOX5), and TNF. The PI3K-Akt signaling pathway was identified as the central mechanism of action.72
Asthma
Airway hyperresponsiveness is a hallmark of asthma. In a shrimp protein-induced mouse model, Shuanghuanglian administration inhibits inspiratory and expiratory resistance, reduces thickness of airway smooth muscle, and mitigates infiltration of inflammation cells. It also alleviates eosinophilic airway inflammation by reducing the number of eosinophils and decreasing levels of eotaxin and eosinophil peroxidase in the BALF. Furthermore, it suppresses mast cell activity by decreasing protease-1 and IgE levels, inhibits Th2 cell differentiation in mediastinal lymph nodes, and reduces the production of Th2-associated cytokines such as IL-4, IL-5, and IL-13.73
Pneumonia
In cases of Mycoplasma pneumoniae pneumonia, multiple randomized controlled trials have demonstrated that Shuanghuanglian oral preparations combined with azithromycin significantly improves clinical symptoms compared with azithromycin monotherapy. Pharmacological network analysis and molecular docking identified 18 active ingredients in Shuanghuanglian oral liquid and 53 potential protein targets involved in the treatment of M. pneumoniae infection.75 Likewise, in COVID-19 patients, a 14-day Shuanghuanglian treatment regimen resulted in a significantly higher SARS-CoV-2 negative conversion rate in nucleic acid swab tests compared to control groups, as observed in a randomized, open-label, parallel-controlled, multicenter clinical trial including 176 patients. High-dose SHL is also associated with enhanced absorption of pulmonary inflammatory foci.74
Yejuhua
Yejuhua injection, a TCM preparation, was first introduced into clinical practice in 1971. Clinically, YJH injection has been widely employed in the management of upper respiratory tract infections, acute tonsillitis, and pharyngalgia.98
Constituents
Yejuhua is derived from a single botanical source-Chrysanthemi Indici Flos (Yejuhua), which which consists of the dried capitulum (flower head) of Chrysanthemum indicum L., commonly known as feverfew.98 The primary active compound in Yejuhua injection is linarin, a flavonoid with recognized anti-inflammatory and antimicrobial properties99 (Figure 1).
Treatment
ALI
In LPS-induced acute lung injury, Yejuhua significantly alleviates histopathological changes, reduces vascular permeability and pulmonary edema, inhibits inflammatory cell infiltration and protein leakage, suppresses myeloperoxidase activity, decreases the production of proinflammatory cytokines, and downregulates the activation of NF-κB as well as the expression of toll-like receptor 4 (TLR4).76 Moreover, Han et al revealed that the thioredoxin-interacting protein (TXNIP)/NOD-like receptor protein 3 (NLRP3) inflammasome signaling pathway plays a crucial role in the therapeutic effects of linarin—the major active component of Yejuhua—against acute lung injury.77
Comparative Efficacy of Traditional Chinese Medicine Preparations in Respiratory Inflammatory Diseases
AURTI
Guo et al conducted a comprehensive analysis of 81 studies encompassing 11,736 patients to compare the efficacy of Xiyanping, Qingkailing, Reduning, Yanhuning, and Tanreqing injections in the treatment of acute upper respiratory tract infections (AURTIs). The results indicated that Qingkailing was the most effective in alleviating fever and improving overall clinical efficacy. Tanreqing demonstrated the greatest effectiveness in relieving cough, while Yanhuning was superior in reducing sore throat, runny nose, and nasal congestion. Moreover, the overall incidence of adverse effects associated with these herbal injections was low, highlighting their favorable safety profiles in the treatment of AURTIs (Table 2).100 This comparative study helps clarify the differentiated therapeutic niches of each formulation and provide a framework for more tailored TCM selection in AURTIs. However, heterogeneity across trials—including variable diagnostic criteria, outcome definitions, and treatment combinations—limits the certainty of these comparative rankings and highlights the need for standardized, high-quality head-to-head trials. In addition, due to potential batch-to-batch variability and the lack of long-term toxicological studies, the safety of these herbal injections still warrants careful attention.
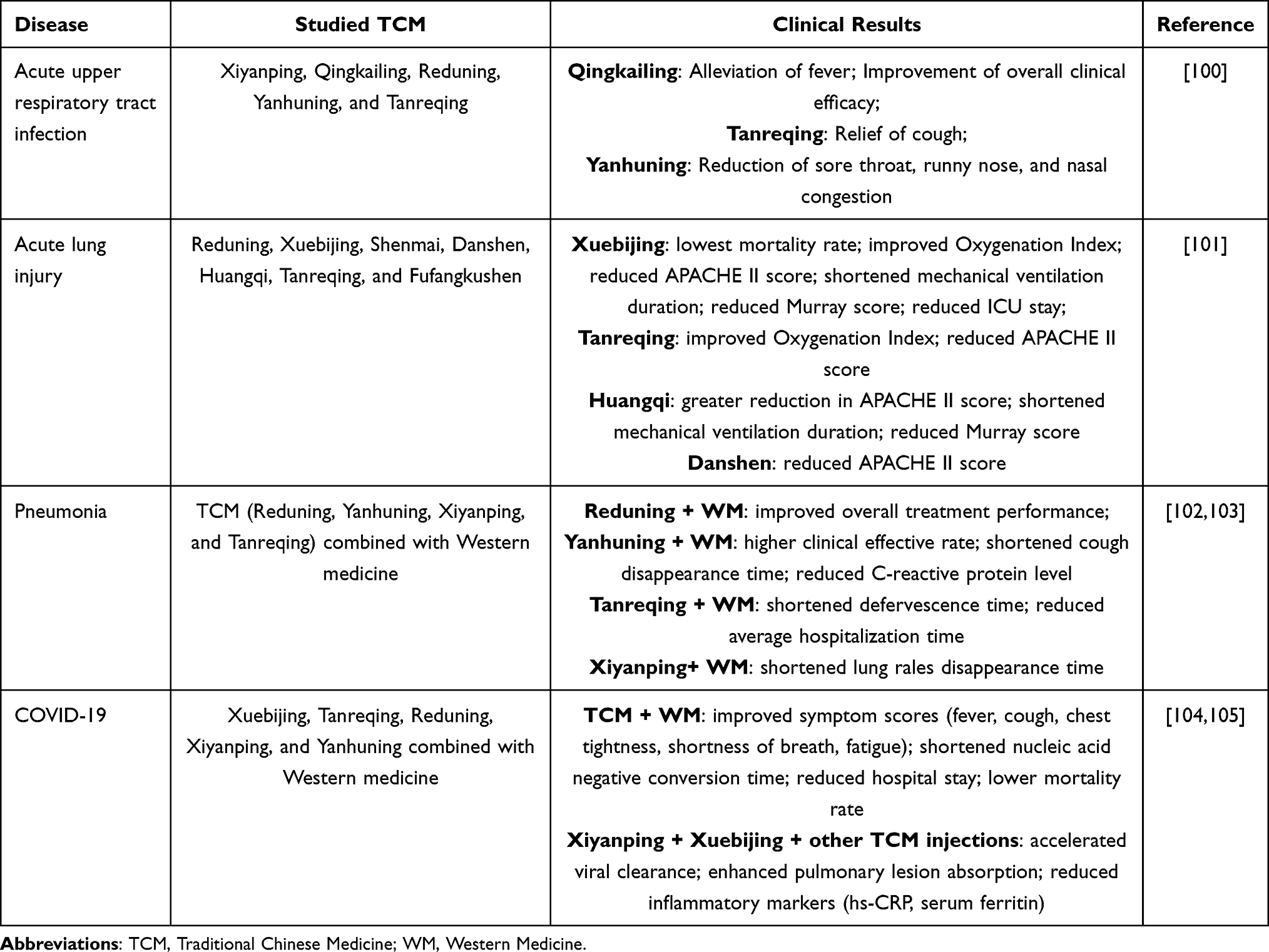 |
Table 2 Comparative Efficacy of Traditional Chinese Medicine Preparations in Respiratory Inflammatory Diseases |
ALI
In another study, Guo et al conducted a comparative analysis of seven Chinese medicine injections—Reduning, Xuebijing, Shenmai, Danshen, Huangqi, Tanreqing, and Fufangkushen—in the treatment of ALI and acute respiratory distress syndrome (ARDS). A total of 26 studies involving 2,073 participants were included. The results revealed that Xuebijing was associated with the lowest mortality rate among the interventions. Both Tanreqing and Xuebijing demonstrated superior efficacy in improving the Oxygenation Index. Additionally, Huangqi, Danshen, Tanreqing, and Xuebijing significantly reduced the APACHE II score, with Huangqi showing a greater effect than Xuebijing. Huangqi and Xuebijing were the most effective in shortening the duration of mechanical ventilation and reducing the Murray score, while Xuebijing was particularly effective in reducing the length of ICU stay.101 By directly comparing multiple herbal injections, this analysis helps delineate the relative strengths of different preparations in ALI/ARDS management—particularly the mortality benefit of Xuebijing and the oxygenation-improving effects of Tanreqing.
Pneumonia
The combination of TCM with conventional Western therapy is increasingly advocated for pneumonia treatment, as it can shorten mechanical ventilation duration, infection control time, and hospital and ICU stays. This integrative approach also improves clinical indicators, including body temperature, respiratory and heart rates, inflammatory markers, and clinical scoring indices such as CPIS, APACHE II, and PSI. Additionally, it enhances pulmonary imaging results, arterial blood gas parameters, and lung function measures such as FVC and FEV1 compared to Western therapy alone. Among the various herbal injections, Tanreqing combined with Western medicine is most advantageous in reducing fever duration and average hospital stay, while Xiyanping is most effective in accelerating the disappearance of lung rales and improving outcomes such as WBC levels, ICU length of stay, and duration of mechanical ventilation. Cluster analysis indicated that Tanreqing and Xiyanping showed comparable benefits across clinical effective rate and key outcome measures. Xuebijing and Tanreqing are the most commonly used in managing severe pneumonia, both of which have been evaluated as “probably beneficial” interventions.19,102,103
COVID-19
For hospitalized patients with COVID-19, the most commonly used Chinese medicine injections are Xuebijing, Tanreqing, Reduning, Xiyanping, and Yanhuning. The integration of TCM with conventional Western medicine has shown significant benefits in improving symptom scores for fever, cough, chest tightness, shortness of breath, and fatigue. The average time to nucleic acid negative conversion was 11.55 ± 5.91 days, with a mean hospital stay of 14.92 ± 6.15 days. The mortality rate was reported to be approximately 1.76%, indicating a potential reduction in mortality.104 Wang et al further compared the efficacy of Chinese medicine treatment (a combination of Xiyanping, Xuebijing, and other TCM preparations injection) with that of standard Western medicine therapy (including antiviral drugs, antibiotics, and corticosteroids). Their findings revealed that the median time to SARS-CoV-2 RNA clearance was significantly shorter in the Chinese medicine group. Additionally, the rate of nucleic acid negative conversion at various follow-up time points was significantly higher than that of the Western medicine group. Chest CT imaging demonstrated greater absorption of pulmonary lesions in the Chinese medicine group. Moreover, inflammatory markers such as high-sensitivity C-reactive protein (hs-CRP) and serum ferritin were significantly reduced in the Chinese medicine group.105 These findings collectively suggest that TCM preparations may offer superior therapeutic efficacy in the treatment of COVID-19, particularly when integrated with Western medical approaches. It should be noted, however, that these findings are primarily based on retrospective studies, which may include confounding factors such as concurrent Western therapies, small sample sizes, and incomplete records. Randomized controlled trials are needed to isolate TCM-specific effects and directly compare TCM with conventional drugs. Therefore, while these data suggest potential benefits of integrating TCM with Western medical approaches for COVID-19, the safety and efficacy of these treatments still require careful evaluation in rigorously designed prospective studies.
Challenges and Future Perspectives
TCM formulations have long been employed in the prevention and treatment of respiratory inflammatory diseases, including asthma, chronic bronchitis, and COPD. These complex herbal combinations exhibit unique therapeutic advantages by targeting multiple pathological pathways simultaneously. In contrast to conventional Western medicines, which often act on single targets, TCM exerts a holistic regulatory effect on the body, modulating immune responses, reducing oxidative stress, alleviating airway inflammation, and promoting tissue repair. Recent pharmacological studies have confirmed the anti-inflammatory, immunomodulatory, and antioxidative properties of many classical TCM formulas.
Clinically, different Chinese medicine injections show distinct advantages across respiratory diseases. Nevertheless, the strength of evidence varies considerably among these preparations, and most studies evaluate them as add-on therapies to standard of care rather than as standalone treatments. For AURTIs, Qingkailing relieves fever, Tanreqing alleviates cough, and Yanhuning reduces nasal symptoms. In ALI and ARDS, Xuebijing lowers mortality and ICU stay, while Tanreqing and Huangqi improve oxygenation and APACHE II scores. For pneumonia, Tanreqing shortens fever and hospitalization, and Xiyanping accelerates lung rale resolution. In COVID-19, Xuebijing, Tanreqing, Reduning, Xiyanping, and Yanhuning improve symptoms, accelerate viral clearance, and reduce inflammation.100–103 Overall, while TCM preparations share broad anti-inflammatory and immune-modulating properties, different preparations provide differentiated therapeutic effects, but the comparative effectiveness between formulations and against guideline-recommended pharmacotherapies remains largely unexplored. These patterns suggest that TCM injections may currently be best positioned as adjunctive or stage-specific options rather than universal therapies for all patients with respiratory inflammatory diseases.
Despite the growing body of supportive evidence, the integration of TCM into mainstream respiratory disease management still faces several obstacles. One major challenge is the unclear material basis of many formulations. Due to the multicomponent nature of TCM, it is often difficult to determine which bioactive ingredients are responsible for the observed therapeutic effects and how potentially conflicting pathways (eg, NF-κB vs PI3K-Akt) are modulated. Although modern technologies such as network pharmacology and metabolomics have been applied to explore potential active components and their interactions with disease targets, these findings remain largely theoretical and require further experimental validation, including knockout models, dose–response assays, and mechanistic in vitro studies.
Another limitation lies in the quality of clinical evidence. While numerous clinical trials have reported the beneficial effects of TCM interventions, many studies are limited by small sample sizes, lack of blinding, inadequate controls, and inconsistent outcome measures. Moreover, the heterogeneity in dosage, formulation, and treatment duration across studies makes it challenging to draw definitive conclusions. Therefore, large-scale, multicenter, randomized controlled trials (RCTs) following rigorous methodologies are urgently needed to validate the efficacy and safety of TCM in treating respiratory inflammatory diseases.
Bioavailability, safety, and potential interactions with conventional Western medicines should also are critical considerations in the clinical translation of TCM preparations. TCM-derived compounds often face challenges such as low water solubility, limited bioavailability, and inadequate target specificity. Recent advances in nanotechnology are expected to overcome these issues, with nanoparticles (NPs) offering benefits including improved bioavailability, controlled drug release, and enhanced targeting precision.106 Owing to possible batch-to-batch inconsistencies and the absence of long-term toxicological data, the safety of these herbal injections requires continued careful evaluation.107 Herb–drug interactions represent a critical factor influencing the clinical efficacy of medical treatments. These interactions can alter the pharmacokinetics or pharmacodynamics of drugs, potentially resulting in therapeutic failure or adverse effects. Although pharmacokinetic interactions have been extensively investigated, pharmacodynamic interactions are less understood, highlighting the need for further research to enhance patient safety and optimize therapeutic outcomes.108
Additionally, issues related to standardization, quality control, and regulatory approval of Chinese herbal products restrict their broader application, particularly in international markets. Variations in raw herb sources, preparation methods, and storage conditions can affect the consistency and reproducibility of therapeutic effects. Addressing these issues requires improved quality assurance systems and unified pharmacopoeia standards.
Despite these challenges, TCM continues to offer promising opportunities for the development of novel respiratory therapies. By combining traditional knowledge with modern scientific approaches, the pharmacological mechanisms of TCM can be more clearly elucidated, and its clinical applications can be better standardized. Furthermore, the synergistic potential of integrating TCM with Western medicine should not be overlooked. In clinical practice, such integration has shown to enhance treatment efficacy, reduce adverse effects, and improve overall patient outcomes.
In summary, TCM formulations hold great promise in the treatment of respiratory inflammatory diseases through their multifaceted pharmacological actions. With advances in research methodologies and a growing emphasis on evidence-based practice, the therapeutic value of TCM is expected to gain greater recognition both in China and globally. Furthermore, these findings provide important insights for guiding clinical practice and open new avenues for basic research into the mechanisms of TCM in respiratory inflammation.
Conclusion
This review highlights the therapeutic potential of traditional Chinese medicine (TCM) formulations in respiratory inflammatory diseases, emphasizing their multi-component, multi-target, and multi-pathway effects, including immune regulation, anti-inflammatory activity, oxidative stress modulation, and mucosal repair. While promising as complementary or alternative therapies for conditions such as asthma, chronic bronchitis, and COPD, challenges remain. Large-scale randomized controlled trials are needed to validate efficacy, and further research is required to clarify the active compounds, molecular mechanisms, and standardized quality control and dosage forms. Addressing these issues could promote the more comprehensive integration of TCM into the clinical management of respiratory inflammatory diseases, thereby enhancing therapeutic efficacy and patient quality of life.
Data Sharing Statement
All source data for this work (or generated in this study) are available from the corresponding author upon reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by Jilin Provincial Natural Science Foundation Project (20200201620JC).
Disclosure
The authors declare no competing interests.
References
1. Komalla V, Mehta M, Achi F, Dua K, Haghi M. The potential for phospholipids in the treatment of airway inflammation: an unexplored solution. Curr Mol Pharmacol. 2021;14:333–19.
2. Bloushi S, Al-Ahmad M. Exploring the immunopathology of type 2 inflammatory airway diseases. Front Immunol. 2024;15(1285598).
3. Royce SG, Le Saux CJ. Role of caveolin-1 in asthma and chronic inflammatory respiratory diseases. Expert Rev Respir Med. 2014;8(3):339–347. doi:10.1586/17476348.2014.905915
4. Ge Y, Tang G, Fu Y, Deng P, Yao R. The impact of environmental factors on respiratory tract microbiome and respiratory system diseases. Eur J Med Res. 2025;30(1):236. doi:10.1186/s40001-025-02517-3
5. Guttenberg MA, Vose AT, Tighe RM. Role of innate immune system in environmental lung diseases. Curr Allergy Asthma Rep. 2021;21(5):34. doi:10.1007/s11882-021-01011-0
6. Chung KF, Dixey P, Abubakar-Waziri H, et al. Characteristics, phenotypes, mechanisms and management of severe asthma. Chinese Medical Journal. 2022;135(10):1141. doi:10.1097/CM9.0000000000001990
7. Anderson R, Feldman C. The global burden of community-acquired pneumonia in adults, encompassing invasive pneumococcal disease and the prevalence of its associated cardiovascular events, with a focus on pneumolysin and macrolide antibiotics in pathogenesis and therapy. Int J Mol Sci. 2023;24(13):11038. doi:10.3390/ijms241311038
8. Grosbois J-M, Détrée A, Pierache A, et al. Impact of cardiovascular and metabolic comorbidities on long-term outcomes of home-based pulmonary rehabilitation in COPD. Int J Chron Obstruct Pulmon Dis. 2023;18:155–167. doi:10.2147/COPD.S381744
9. S SLJ, V R. Scope of adjuvant therapy using roflumilast, a PDE-4 inhibitor against COVID-19. Pulm Pharmacol Ther. 2021;66:101978. doi:10.1016/j.pupt.2020.101978
10. Feleszko W, Rossi GA, Krenke R. Immunoactive preparations and regulatory responses in the respiratory tract: potential for clinical application in chronic inflammatory airway diseases. Expert Rev Respir Med. 2020;14:603–619.
11. Azh N, Barzkar F, Motamed-Gorji N, et al. Nonsteroidal anti-inflammatory drugs in acute viral respiratory tract infections: an updated systematic review. Pharmacol Res Perspect. 2022;10:e00925.
12. Killeen BM, Wolfson AB. Antibiotics for acute bronchitis. Am Fam Physician. 2020;102.
13. Kirolos A, Manti S, Blacow R, et al. A systematic review of clinical practice guidelines for the diagnosis and management of bronchiolitis. J Infect Dis. 2020;222:S672–S679.
14. Harford JB, Kim SS, Pirollo KF, Chang EH. TP53 gene therapy as a potential treatment for patients with COVID-19. Viruses. 2022;14:739.
15. Hezam K, Mo R, Wang C, Liu Y, Li Z. Anti-inflammatory effects of mesenchymal stem cells and their secretomes in pneumonia. Curr Pharm Biotechnol. 2022;23(9):1153–1167. doi:10.2174/1389201022666210907115126
16. Yu J-S, Ho C-H, Hsu Y-C, Wang -J-J, Hsieh C-L. Traditional Chinese medicine treatments for upper respiratory tract infections/common colds in Taiwan. Eur J Integr Med. 2014;6:538–544.
17. Zhuang Z, Wen J, Zhang L, et al. Can network pharmacology identify the anti-virus and anti- inflammatory activities of Shuanghuanglian oral liquid used in Chinese medicine for respiratory tract infection? Eur J Integr Med. 2020;37:101139. doi:10.1016/j.eujim.2020.101139
18. Li P, Hu S, Qian C, et al. The therapeutic effect of traditional chinese medicine on inflammatory diseases caused by virus, especially on those caused by COVID-19. Front Pharmacol. 2021;12:650425. doi:10.3389/fphar.2021.650425
19. Xie K, Guan S, Jing H, et al. Efficacy and safety of traditional Chinese medicine adjuvant therapy for severe pneumonia: evidence mapping of the randomized controlled trials, systematic reviews, and meta-analyses. Front Pharmacol. 2023;14:1227436. doi:10.3389/fphar.2023.1227436
20. Cheng X, Su X, Chen X, et al. Biological ingredient analysis of traditional Chinese medicine preparation based on high-throughput sequencing: the story for Liuwei Dihuang Wan. Sci Rep. 2014;4(1):5147. doi:10.1038/srep05147
21. Zhou W, Lai X, Wang X, Yao X, Wang W, Li S. Network pharmacology to explore the anti-inflammatory mechanism of Xuebijing in the treatment of sepsis. Phytomedicine. 2021;85:153543. doi:10.1016/j.phymed.2021.153543
22. Hu T. Xuebijing injection for sepsis treatment: when will it be approved outside of China? JAMA Intern Med. 2023;183(11):1280–1281. doi:10.1001/jamainternmed.2023.4398
23. Yuan S, Cao Y, Jiang J, et al. Xuebijing injection and its bioactive components alleviate nephrotic syndrome by inhibiting podocyte inflammatory injury. Eur J Pharm Sci. 2024;196:106759. doi:10.1016/j.ejps.2024.106759
24. Ni J, Yang M, Zheng X, et al. Synthesis, antioxidant activity, and molecular docking of novel paeoniflorin derivatives. Chem Biol Drug Des. 2024;104(3):e14629. doi:10.1111/cbdd.14629
25. Chen X, Yang T, Zhou Y, Mei Z, Zhang W. Astragaloside IV combined with ligustrazine ameliorates abnormal mitochondrial dynamics via Drp1 SUMO/deSUMOylation in cerebral ischemia–reperfusion injury. CNS Neurosci Ther. 2024;30(4):e14725. doi:10.1111/cns.14725
26. Xu Z, Cai K, Su S-L, Zhu Y, Liu F, Duan J-A. Salvianolic acid B and tanshinone IIA synergistically improve early diabetic nephropathy through regulating PI3K/Akt/NF-κB signaling pathway. J Ethnopharmacol. 2024;319:117356. doi:10.1016/j.jep.2023.117356
27. Chen L, Ding L, Zhang H, et al. Dynamic microwave-assisted extraction coupled with on-line spectrophotometric determination of safflower yellow in Flos Carthami. Anal Chim Acta. 2006;580(1):75–82. doi:10.1016/j.aca.2006.07.040
28. Song X, Liu C, Zhang Y, et al. Sustainable extraction of ligustilide and ferulic acid from Angelicae SInensis Radix, for antioxidant and anti-inflammatory activities. Ultrason Sonochem. 2023;94:106344. doi:10.1016/j.ultsonch.2023.106344
29. Chen Y, Tong H, Pan Z, et al. Xuebijing injection attenuates pulmonary injury by reducing oxidative stress and proinflammatory damage in rats with heat stroke. Exp Ther Med. 2017;13(6):3408–3416. doi:10.3892/etm.2017.4444
30. Zhang C, Chen X, Wei T, et al. Xuebijing alleviates LPS-induced acute lung injury by downregulating pro-inflammatory cytokine production and inhibiting gasdermin-E-mediated pyroptosis of alveolar epithelial cells. Chin J Nat Med. 2023;21(8):576–588. doi:10.1016/S1875-5364(23)60463-7
31. Ji M, Wang Y, Wang L, Chen L, Li J. Protective effect of Xuebijing injection against acute lung injury induced by left ventricular ischemia/reperfusion in rabbits. Exp Ther Med. 2016;12(1):51–58. doi:10.3892/etm.2016.3275
32. Wang Q, Wu X, Tong X, Zhang Z, Xu B, Zhou W. Xuebijing ameliorates sepsis-induced lung injury by downregulating HMGB1 and RAGE expressions in mice. Evid Based Complement Alternat Med. 2015;2015:860259. doi:10.1155/2015/860259
33. Wu X, Xin R, Zhang Y, et al. Xuebijing improves inflammation and pyroptosis of acute lung injury by up-regulating miR-181d-5p-mediated SPP1 inactivation. Clinics. 2024;79:100336. doi:10.1016/j.clinsp.2024.100336
34. Cui J, Deng Y, Li X, et al. Herbal-based Xuebijing injection ameliorated vascular endothelial dysfunction via inhibiting ACLY/MYB/RIG-I axis in sepsis-associated lung injury. Phytomedicine. 2025;140:156573. doi:10.1016/j.phymed.2025.156573
35. Zou F, Zou J, Du Q, et al. XueBiJing injection improves the symptoms of sepsis-induced acute lung injury by mitigating oxidative stress and ferroptosis. J Ethnopharmacol. 2025;337:118732. doi:10.1016/j.jep.2024.118732
36. Liu M, Su M, Zhang W, et al. Protective effect of Xuebijing injection on paraquat-induced pulmonary injury via down-regulating the expression of p38 MAPK in rats. BMC Complement Altern Med. 2014;14(1):498. doi:10.1186/1472-6882-14-498
37. Zhang C, He H, Chen X, et al. The prediction of lymphocyte count and neutrophil count on the efficacy of Xuebijing adjuvant treatment for severe community-acquired pneumonia: a post hoc analysis of a randomized controlled trial. Phytomedicine. 2023;110:154614. doi:10.1016/j.phymed.2022.154614
38. Tao P, Jiming L. Molecular mechanisms revealed by network pharmacology of Xuebijing on the treatment of acute respiratory distress syndrome caused by novel coronavirus infection. Eur Rev Med Pharmacol Sci. 2022;26(8):2651–2661. doi:10.26355/eurrev_202204_28594
39. Zheng W-J, Yan Q, Ni Y-S, et al. Examining the effector mechanisms of Xuebijing injection on COVID-19 based on network pharmacology. BioData Mining. 2020;13(1):17. doi:10.1186/s13040-020-00227-6
40. Chen H, Li S, Pan B, et al. Qing-Kai-Ling oral liquid alleviated pneumonia via regulation of intestinal flora and metabolites in rats. Front Microbiol. 2023;14:1194401. doi:10.3389/fmicb.2023.1194401
41. Chen X, Kang F, Lai J, Deng X, Guo X, Liu S. Comparative effectiveness of phlegm-heat clearing Chinese medicine injections for AECOPD: a systematic review and network meta-analysis. J Ethnopharmacol. 2022;292:115043. doi:10.1016/j.jep.2022.115043
42. Liu T, Li S, Wang X, et al. Deciphering the therapeutic effects of Xiyanping injection: insights into pulmonary and gut microbiome modulation, SerpinB2/PAI-2 targeting, and alleviation of influenza a virus-induced lung injury. Virol J. 2025;22(1):19. doi:10.1186/s12985-025-02636-7
43. Peng S, Hang N, Liu W, et al. Andrographolide sulfonate ameliorates lipopolysaccharide-induced acute lung injury in mice by down-regulating MAPK and NF-κB pathways. Acta Pharm Sin B. 2016;6(3):205–211. doi:10.1016/j.apsb.2016.02.002
44. Gu X, Gao R, Li Y, Liu J, Wu Y, Xu H. Combination effect of azithromycin with TCM preparation Xiyanping injection against Klebsiella pneumoniae infection in rats. Phytomedicine. 2022;104:154332. doi:10.1016/j.phymed.2022.154332
45. Zhang X-Y, Lv L, Zhou Y-L, et al. Efficacy and safety of Xiyanping injection in the treatment of COVID −19: a multicenter, prospective, open-label and randomized controlled trial. Phytother Res. 2021;35(8):4401–4410. doi:10.1002/ptr.7141
46. Shi H, Guo W, Zhu H, et al. Cost-effectiveness analysis of xiyanping injection (andrographolide sulfonate) for treatment of adult community acquired pneumonia: a retrospective, propensity score-matched cohort study. Evid Based Complement Alternat Med. 2019;2019:4510591. doi:10.1155/2019/4510591
47. Yuan Y, Zheng Q, Si Z, et al. Efficacy of Chinese herbal injections for elderly patients with pneumonia—a bayesian network meta-analysis of randomized control trials. Front Pharmacol. 2021;12:610745. doi:10.3389/fphar.2021.610745
48. Zhou H, Chen D, Zhang Y, et al. Efficacy and safety of Xiyanping for COVID-2019: a protocol for systematic review and meta-analysis. Medicine. 2020;99(46):e22962. doi:10.1097/MD.0000000000022962
49. Li J, Guo S, Tan Y, et al. Integrated network pharmacology analysis and in vitro validation revealed the underlying mechanism of Xiyanping injection in treating coronavirus disease 2019. Medicine. 2023;102(34):e34866. doi:10.1097/MD.0000000000034866
50. Xia L, Zhang L, Yang K, Chen T, Ye X, Yan Z. The pharmacological mechanism of Xiyanping injection for the treatment of novel coronavirus pneumonia (COVID-19): based on network pharmacology strategy. Evid Based Complement Alternat Med. 2022;2022:9152201. doi:10.1155/2022/9152201
51. Hu C, Li J, Tan Y, et al. Tanreqing injection attenuates macrophage activation and the inflammatory response via the lncRNA-SNHG1/HMGB1 axis in lipopolysaccharide-induced acute lung injury. Front Immunol. 2022;13:820718. doi:10.3389/fimmu.2022.820718
52. He Y-Q, Zhou -C-C, Deng J-L, Wang L, Chen W-S. Tanreqing inhibits LPS-induced acute lung injury in vivo and in vitro through downregulating STING signaling pathway. Front Pharmacol. 2021;12:746964. doi:10.3389/fphar.2021.746964
53. Tang B, Xie L, Wang Y, et al. Exploratory research on the effective chemical basis of tanreqing injection for treating acute lung injury: in vivo, in vitro and in silico. J Ethnopharmacol. 2025;337:118780. doi:10.1016/j.jep.2024.118780
54. Wang P, Liao X, Xie Y-M, Chai Y, Li L-H. Tanreqing injection for acute bronchitis disease: a systematic review and meta-analysis of randomized controlled trials. Complement Ther Med. 2016;25:143–158. doi:10.1016/j.ctim.2016.02.008
55. Cheng G, She B, Mao B, Jiang H. Efficacy and safety of Tanreqing oral liquid in treatment of acute bronchitis: study protocol for a randomized controlled trial. Trials. 2022;23(1):373. doi:10.1186/s13063-022-06318-5
56. Wang Y, Wang T, Hu J, et al. Anti-biofilm activity of TanReQing, a traditional Chinese medicine used for the treatment of acute pneumonia. J Ethnopharmacol. 2011;134(1):165–170. doi:10.1016/j.jep.2010.11.066
57. Zhang W, He M, Kong N, Niu Y, Li A, Yan Y. Study on the inhibition activity and mechanism of Tanreqing against Klebsiella pneumoniae biofilm formation in vitro and in vivo. Front Cell Infect Microbiol. 2024;14:1368450. doi:10.3389/fcimb.2024.1368450
58. Li P, Wu Y, Ge D, et al. Effects of Tanreqing injection against ventilator-associated pneumonia: a meta-analysis and systematic review of clinical studies. Front Pharmacol. 2025;16:1545088. doi:10.3389/fphar.2025.1545088
59. Li X, Wei S, Ma X, et al. Efficacy and safety of Tanreqing injection combined with antibiotics against Streptococcus pneumoniae pneumonia: a systematic review and meta-analysis. J Clin Pharm Ther. 2022;47(8):1159–1172. doi:10.1111/jcpt.13706
60. Wang L, Fan Y, Xu J, Deng H, Geng C, Jia B. The efficacy and safety of Tanreqing injection combined with western medicine for severe pneumonia: a protocol for systematic review and meta-analysis. Medicine. 2020;99(35):e22010. doi:10.1097/MD.0000000000022010
61. Zhang X, Xue Y, Chen X, et al. Effects of Tanreqing Capsule on the negative conversion time of nucleic acid in patients with COVID-19: a retrospective cohort study. J Integr Med. 2021;19(1):36–41. doi:10.1016/j.joim.2020.10.002
62. Wang D, Han D, Huang T, Zhou X, Xu Y. Efficacy evaluation and potential pharmacological mechanism of tanreqing injection in the treatment of COPD combined with respiratory failure based on meta-analysis and network pharmacology. Heliyon. 2023;9(2):e13513. doi:10.1016/j.heliyon.2023.e13513
63. Zhong Y, Mao B, Wang G, et al. Tanreqing injection combined with conventional western medicine for acute exacerbations of chronic obstructive pulmonary disease: a systematic review. J Altern Complement Med. 2010;16(12):1309–1319. doi:10.1089/acm.2009.0686
64. Fan G, Wang D, Wu S, et al. Better response to Tanreqing injection in frequent acute exacerbation of chronic obstructive pulmonary disease (AECOPD) patients—real-world evidence from a nationwide registry (ACURE) study. Front Pharmacol. 2023;14:1118143. doi:10.3389/fphar.2023.1118143
65. Han -X-X, Tian Y-G, Liu X-F, et al. Network pharmacology combined with pharmacodynamics revealed the anti-inflammatory mechanism of Tanreqing capsule against acute-exacerbation chronic obstructive pulmonary disease. Sci Rep. 2022;12(1):13967. doi:10.1038/s41598-022-18326-1
66. Zhu H, Shi Y, Jiang S, et al. Investigation of the mechanisms of chuankezhi injection in the treatment of asthma based on the network pharmacology approach. Evid Based Complement Alternat Med. 2021;2021:5517041. doi:10.1155/2021/5517041
67. Kong XT, Fang HT, Jiang GQ, Zhai SZ, O’Connell DL, Brewster DR. Treatment of acute bronchiolitis with Chinese herbs. Arch Dis Child. 1993;68(4):468–471. doi:10.1136/adc.68.4.468
68. Zhang H, Chen Q, Zhou W, et al. Chinese medicine injection shuanghuanglian for treatment of acute upper respiratory tract infection: a systematic review of randomized controlled trials. Evid Based Complement Alternat Med. 2013;2013:987326. doi:10.1155/2013/987326
69. Wang YH, Xu KJ, Jiang WS. Experimental and clinical study of shuanghuanglian aerosol in treating acute respiratory tract infection. Zhongguo Zhong Xi Yi Jie He Za Zhi. 1995;15(6):347–350.
70. Lin G, Liu D, Zhu L. Clinical study on Shuanghuanglian powder in treating children viral myocarditis. Zhongguo Zhong Xi Yi Jie He Za Zhi. 1998;18(10):601–602.
71. Fang L, Gao Y, Liu F, Hou R, Cai R-L, Qi Y. Shuang-huang-lian attenuates lipopolysaccharide-induced acute lung injury in mice involving anti-inflammatory and antioxidative activities. Evid Based Complement Alternat Med. 2015;2015:283939. doi:10.1155/2015/283939
72. Li R, Zhu Y, Yu M, Liu T, Zhao Y, Yu Z. Study on the mechanism of anti-acute lung injury of Shuanghuanglian oral liquid based on identification of transitional components in blood and network pharmacology. J Chromatogr B Analyt Technol Biomed Life Sci. 2022;1212:123498. doi:10.1016/j.jchromb.2022.123498
73. Gao Y, Fei Q, Qi R, et al. Shuang-Huang-Lian attenuates airway hyperresponsiveness and inflammation in a shrimp protein-induced murine asthma model. Evid Based Complement Alternat Med. 2019;2019:4827342. doi:10.1155/2019/4827342
74. Ni L, Wen Z, Hu X, et al. Effects of Shuanghuanglian oral liquids on patients with COVID-19: a randomized, open-label, parallel-controlled, multicenter clinical trial. Front Med. 2021;15(5):704–717. doi:10.1007/s11684-021-0853-6
75. Shi L, Wu Q-G, Zhang J-C, Yang G-M, Liu W, Wang Z-F. Mechanism of Shuang-Huang-Lian oral liquid for treatment of mycoplasmal pneumonia in children on network pharmacology. Comb Chem High Throughput Screen. 2020;23(9):955–971. doi:10.2174/1386207323666200514073428
76. Li C-W, Chen Z-W, Wu X-L, et al. A standardized traditional Chinese medicine preparation named yejuhua capsule ameliorates lipopolysaccharide-induced acute lung injury in mice via downregulating toll-like receptor 4/nuclear factor-κB. Evid Based Complement Alternat Med. 2015;2015:264612. doi:10.1155/2015/264612
77. Han X, Wu Y-C, Meng M, Sun Q-S, Gao S-M, Sun H. Linarin prevents LPS‑induced acute lung injury by suppressing oxidative stress and inflammation via inhibition of TXNIP/NLRP3 and NF‑κB pathways. Int J Mol Med. 2018;42(3):1460–1472. doi:10.3892/ijmm.2018.3710
78. Li Z, Wang D, Zhang Y, et al. The efficacy and safety of Xuebijing injection in the treatment of radiation pneumonitis: a protocol for systematic review and meta-analysis. Medicine. 2021;100(5):e24344. doi:10.1097/MD.0000000000024344
79. Cheng F, Wang X, Lu Y, Zhong X, Zhao Y, Wang Q. Chinese medicine injection qingkailing for treatment of acute ischemia stroke: a systematic review of randomized controlled trials. Evid Based Complement Alternat Med. 2012;2012:213172. doi:10.1155/2012/213172
80. Li T-Y, Li Z, Yang X-Y, et al. Comparative pharmacokinetics of baicalin and geniposide in juvenile and adult rats after oral administration of Qingkailing Granules. Chin Herb Med. 2020;12(4):446–451. doi:10.1016/j.chmed.2020.05.011
81. Li H, Xin G, Zhou Q, et al. Qingkailing granule alleviates pulmonary fibrosis by inhibiting PI3K/AKT and SRC/STAT3 signaling pathways. Bioorg Chem. 2024;146:107286. doi:10.1016/j.bioorg.2024.107286
82. Garcia-Macias P, John P. Formation of natural indigo derived from woad (Isatis tinctoria L.) in relation to product purity. J Agric Food Chem. 2004;52(26):7891–7896. doi:10.1021/jf0486803
83. Mahboob T, Azlan A-M, Tan T-C, et al. Anti-encystment and amoebicidal activity of Lonicera japonica Thunb. and its major constituent chlorogenic acid in vitro. Asian Pac J Trop Med. 2016;9(9):866–871. doi:10.1016/j.apjtm.2016.07.008
84. Qin T, Hasnat M, Wang Z, et al. Geniposide alleviated bile acid-associated NLRP3 inflammasome activation by regulating SIRT1/FXR signaling in bile duct ligation-induced liver fibrosis. Phytomedicine. 2023;118:154971. doi:10.1016/j.phymed.2023.154971
85. Liu R, Wang M, Duan J-A, Guo J-M, Tang Y-P. Purification and identification of three novel antioxidant peptides from Cornu Bubali (water Buffalo horn). Peptides. 2010;31(5):786–793. doi:10.1016/j.peptides.2010.02.016
86. Wu M-N, Zhou L-J-M, Zhou D-M. Xiyanping injection combined with Acitretin for psoriasis vulgaris: a systematic review and meta-analysis. Front Pharmacol. 2022;13:971715. doi:10.3389/fphar.2022.971715
87. Yang Q-W, Li Q, Zhang J, et al. Crystal structure and anti-inflammatory and anaphylactic effects of andrographlide sulphonate E in Xiyanping, a traditional Chinese medicine injection. J Pharm Pharmacol. 2019;71(2):251–259. doi:10.1111/jphp.13028
88. Cui J, Gao J, Li Y, et al. Andrographolide sulfate inhibited NF-κB activation and alleviated pneumonia induced by poly I:C in mice. J Pharmacol Sci. 2020;144(4):189–196. doi:10.1016/j.jphs.2020.08.005
89. Lee I-T, Yang C-M. Inflammatory signalings involved in airway and pulmonary diseases. Mediators Inflamm. 2013;2013:791231. doi:10.1155/2013/791231
90. Yang J, Chen X, He X, et al. Tanreqing injection demonstrates anti-dengue activity through the regulation of the NF-κB-ICAM-1/VCAM-1 axis. Phytomedicine. 2024;130:155764. doi:10.1016/j.phymed.2024.155764
91. Guo J, Tang J-K, Wang B-F, et al. Phillygenin from Forsythia suspensa leaves exhibits analgesic potential and anti-inflammatory activity in carrageenan-induced paw edema in mice. J Food Biochem. 2022;46(12):e14460. doi:10.1111/jfbc.14460
92. Yi-Jun C, Wei-Ya C, Jia-Xing W, Chun-Yu L, Fei-Fei Y, Yong-Hong L. The pulmonary pharmacokinetics and anti-inflammatory effects after intratracheal and intravenous administration of Chuankezhi injection. Biomed Pharmacother. 2022;156:113892. doi:10.1016/j.biopha.2022.113892
93. Wang G, Li X, Li N, et al. Icariin alleviates uveitis by targeting peroxiredoxin 3 to modulate retinal microglia M1/M2 phenotypic polarization. Redox Biol. 2022;52:102297. doi:10.1016/j.redox.2022.102297
94. Zhang C, Ouyang L, Zhang X, et al. Anaphylactoid reactions induced by Shuanghuanglian injection and Shenmai injection and metabolomics analysis. Front Pharmacol. 2023;14:1200199. doi:10.3389/fphar.2023.1200199
95. Zhu L, Zhang H, Xiao X, et al. Shuanghuanglian volatile oil exerts antipyretic, anti-inflammatory, and antibacterial synergistic effects through multiple pathways. J Ethnopharmacol. 2025;337:118795. doi:10.1016/j.jep.2024.118795
96. Zhou W, Di L, Bi X, Chen L, Du Q. [Study on in situ intestinal absorption of active ingredients in Shuanghuanglian oral liquid in rats. Zhongguo Zhong Yao Za Zhi. 2011;36(13):1733–1738.
97. Han R, Ye J-X, Quan L-H, Liu C-Y, Yang M, Liao Y-H. Evaluating pulmonary toxicity of Shuang–Huang–Lian in vitro and in vivo. J Ethnopharmacol. 2011;135(2):522–529. doi:10.1016/j.jep.2011.03.060
98. Lv Y, Fu J, Shi X, Yang Z, Han S. Screening allergic components of Yejuhua injection using LAD2 cell membrane chromatography model online with high performance liquid chromatography-ion trap-time of flight-mass spectrum system. J Chromatogr B Analyt Technol Biomed Life Sci. 2017;1055-1056:119–124. doi:10.1016/j.jchromb.2017.04.045
99. Zhao X, Mao X, Xu X, Li X, Bi K, Jia Y. Determination and pharmacokinetics of linarin in rat plasma after intramuscular administration of linarin solution and Yejuhua injection by HPLC. Biomed Chromatogr. 2015;29(2):164–166. doi:10.1002/bmc.3269
100. Guo X, Liu C, Zhao Q, Huang S. Efficacy of five different traditional Chinese medicine injections in acute upper respiratory tract infection in children: a network meta-analysis and systematic review. Front Pediatr. 2024;12:1358639.
101. Guo J, Zhu J, Wang Q, Wang J, Jia Y. Comparative efficacy of seven kinds of chinese medicine injections in acute lung injury and acute respiratory distress syndrome: a network meta-analysis of randomized controlled trials. Front Pharmacol. 2021;12:627751.
102. Niu L, Xiao L, Zhang X, et al. Comparative efficacy of chinese herbal injections for treating severe pneumonia: a systematic review and Bayesian network meta-analysis of randomized controlled trials. Front Pharmacol. 2021;12:743486.
103. Huang X, Duan X, Zhu Y, Wang K, Wu J, Tian X. Comparative efficacy of Chinese herbal injections for the treatment of community-acquired pneumonia: a Bayesian network meta-analysis of randomized controlled trials. Phytomedicine. 2019;63:153009.
104. Han R, Xie Y, Zhao H, et al. The efficacy of traditional Chinese medicine in the treatment of the COVID-19 pandemic in Henan Province: a retrospective study. Eur J Med Res. 2023;28(1):78. doi:10.1186/s40001-023-01006-9
105. Wang Y, Lu C, Li H, et al. Efficacy and safety assessment of severe COVID-19 patients with Chinese medicine: a retrospective case series study at early stage of the COVID-19 epidemic in Wuhan, China. J Ethnopharmacol. 2021;277:113888. doi:10.1016/j.jep.2021.113888
106. Yang L, Wang Y, Ye X, Liu Q, Qu D, Chen Y. Traditional Chinese medicine-based drug delivery systems for anti-tumor therapies. Chin J Nat Med. 2024;22(12):1177–1192. doi:10.1016/S1875-5364(24)60746-6
107. Fung FY, Linn YC. Developing traditional Chinese medicine in the era of evidence-based medicine: current evidences and challenges. Evid Based Complement Alternat Med. 2015;2015:425037. doi:10.1155/2015/425037
108. Singh A, Zhao K. Herb-drug interactions of commonly used Chinese medicinal herbs. Int Rev Neurobiol. 2017;135:197–232.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.