Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
Research Progress on Coronavirus Prevention and Control in Animal-Source Foods
Authors Gan Y ![]() , Tan F, Yi R, Zhou X, Li C, Zhao X
, Tan F, Yi R, Zhou X, Li C, Zhao X ![]()
Received 29 May 2020
Accepted for publication 21 July 2020
Published 4 August 2020 Volume 2020:13 Pages 743—751
DOI https://doi.org/10.2147/JMDH.S265059
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Yi Gan,1– 3 Fang Tan,4 Ruokun Yi,1– 3 Xianrong Zhou,1– 3 Chong Li,1– 3 Xin Zhao1– 3
1Chongqing Collaborative Innovation Center for Functional Food, Chongqing University of Education, Chongqing, People’s Republic of China; 2Chongqing Engineering Research Center of Functional Food, Chongqing University of Education, Chongqing, People’s Republic of China; 3Chongqing Engineering Laboratory for Research and Development of Functional Food, Chongqing University of Education, Chongqing, People’s Republic of China; 4Department of Public Health, Our Lady of Fatima University, Valenzuela, Philippines
Correspondence: Xin Zhao No. 9, Xuefu Road, Nan’an District, Chongqing Collaborative Innovation Center for Functional Food
Chongqing University of Education Chongqing 400067, People’s Republic of China
Tel +86-23-6265-3650
Email [email protected]
Abstract: Coronaviruses (CoVs) are common pathogens that can infect both animals and humans, thereby posing a threat to global public health. CoV infection mostly occurs during winter and spring in temperate countries; the virus has high transmission efficiency and may have severe infection outcomes. The recent SARS-CoV-2 outbreak exhibited transboundary transmission due to international transportation, trade, and economic exchange. Animal hosts provide a persistent source for CoVs and their recombination. Domestic camels have been shown to be one of the hosts of CoVs, while livestock, poultry and other warm-blooded animals may act as intermediate hosts for CoVs. This paper outlines the biological and epidemiological characteristics and diagnosis of CoVs and describes the origin, transmission route, animal-source food risk, and control measures for CoVs. Such knowledge can be used to prevent CoVs from harming consumers through animal-sourced foods and can help to prevent new zoonoses from occurring. This work will provide a reference for strengthening the controls on the production process in meat production companies, thereby improving food safety.
Keywords: coronavirus, meat, food safety, prevention and control
Introduction
Coronaviruses (CoVs), systemically classified as Coronaviridae, are enveloped viruses that can infect poultry, domestic animals, and humans. The Coronaviridae, which belongs to the order Nidovirales, was first isolated from chickens in 1937 and from humans in 1965.1,2 Phylogenetic evidence has shown that bats and rodents serve as the gene source of most alpha-CoVs and beta-CoVs, while birds are the main reservoir of gamma-CoVs and delta-CoVs. Animal-animal transmission occurs for most CoVs, while only a few CoVs can infect humans through intermediate hosts. Human infections result in diverse symptoms and diseases of the respiratory tract, digestive tract, and nervous system. For example, the Middle East respiratory syndrome coronavirus (MERS-CoV) caused Middle East respiratory syndrome after infecting dromedary camels. Currently, there are seven known CoVs that can infect humans, HCoV-229E, HCoV-NL63, HCoV-OC43, HCoV-HKU1, SARS-CoV, MERS-CoV, and the newly discovered SARS-CoV-2 that causes coronavirus disease 2019 (COVID-19).3 CoVs usually cause self-limiting and mild respiratory tract infections; the main symptoms include fever, coughing, runny nose, and wheezing. Therefore, these infections are often misdiagnosed as pneumonia.4,5 SARS-CoV, MERS-CoV, and SARS-CoV-2 have infected many people, resulting in thousands of deaths. SARS-CoV and SARS-CoV-2 are designated as category B infectious diseases by the National Health Commission, and prevention and control are carried out according to measures used for category a infectious diseases.6
CoV outbreaks mostly occur during winter and spring in temperate regions. Domestic camels have been shown to be one of the hosts for CoVs. Other species of livestock, poultry and warm-blooded animals may be intermediate hosts for CoVs.7 Currently, CoVs with high mortality rate mainly infect humans through intermediate hosts and “host jumps.” In addition, there is no specific drug or vaccine available for CoVs, and thus only symptomatic treatments are used. Increasing movement of people and international commerce has led to global dissemination and epidemics of CoVs that severely affect human health and the global economy.8 The present paper outlines the biological, epidemiological, and diagnostic characteristics of CoVs and describes the control and prevention measures for CoVs. The overall goal is to prevent CoVs from harming public health through animal-source foods.
Biological Characteristics of Coronaviruses
CoVs are divided into 4 genera, namely Alphacoronavirus (α-CoV), Betacoronavirus (β-CoV), Gammacoronavirus (γ-CoV), and Deltacoronavirus (δ-CoV), of which β-CoV pose the greatest threat to human health.9,10 In 2017, the International Committee on Taxonomy of Viruses (ICTV) further divided β-CoV into five subgenera: Embecovirus, Sarbecovirus, Merbecovirus, Nobecovirus, and Hibecovirus.11
Morphology and Genome Structure
Mature CoVs are spherical, oval, or polygonal particles with a diameter of 60–220 nm and a helical and symmetrical nucleocapsid. CoVs are coated with a lipid membrane and appear corona-shaped or crown-shaped under the microscope. A large amount of nucleocapsid protein (N protein) is attached to the viral RNA, and the surface of the virus particle contains spike protein (S protein), membrane protein (M protein), and envelope protein (E protein). A few viruses possess the hemagglutinin-esterase protein (HE protein).12 The N protein has a low degree of polymerization; it can induce cellular immunity and bind to viral RNA to form the nucleocapsid.13 The S protein recognizes specific receptors (N-acetyl-neuraminic acid) on the cell surface during infection to penetrate and lyse the cell membrane so that viral nucleic acid can be injected into cells and induce cellular immunity.14 During infection, the M protein enables transmembrane nutrient transportation, determines virus budding sites, and triggers virus particle assembly and the formation of new viral envelopes.15 The E protein is smaller and is mainly bound to the envelope. The E protein can trigger the assembly of virus particles and can induce apoptosis.16 The HE protein can cause erythrocyte aggregation.17 In addition, the virus particle also contains the Nsp3 protein (multi-domain protein), Nsp5 protein (cysteine protease), Nsp2 protein, ORFb, and ORF3a, but the functions of those proteins are still unknown.
CoVs are single-strand, unsegmented positive RNA viruses, and the genome size is 27–32 kb, making it one of the largest RNA virus genomes that is currently known.18 The 5ʹ end of the CoV genome contains a methylation cap followed by a 65–98 bp guide sequence (loader RNA) and a 209–528 bp 5ʹ untranslated region (UTR). The 3ʹ end also contains a 288–506 bp UTR and a poly A tail. Both UTRs are extremely important for the translation and replication of viral RNA in the host. The remaining middle sequence contains 7–9 open reading frames (ORFs) that encode for various structural proteins, non-structural proteins, and accessory proteins.19,20 There are 2–4 genes that encode for RNA polymerase and 4–5 genes that encode for structural proteins in CoVs. The gene fragments encoding RNA polymerases account for two-thirds of the entire genome; these comprise two open reading frame fragments (ORF1a and ORF1b), while the remaining third of the genome encodes for structural proteins and accessory proteins.21 The genome structure of CoVs from the 5ʹ end to 3ʹ consists of the 5ʹ end-RNA polymerase-(HE protein-S protein-E protein-M protein-N protein-3ʹ end).22
Physicochemical Properties
CoVs show high robustness and survival under suitable temperature and relative humidity (30–50%) conditions and a slow decay rate that mainly involves nucleic acid changes.23 MERS-CoV is still infectious after 60 minutes of aerosolization at 25°C and 79% RH.24 Under room temperature conditions, SARS-CoV can survive in feces/sputum for 1–5 d, 10–19 days in urine, 15 d in blood, and 3 d on surfaces; SARS-CoV can survive for around 21 d at 4°C and for a long period of time at −70°C.25 These viruses are extremely heat-sensitive and can be effectively inactivated by 56°C for 30 min or 70°C for 15 min.26
In addition, CoVs are sensitive to ultraviolet rays, X-rays, γ rays and other ionizing radiation. Ultraviolet radiation can cause RNA to form uracil dimers, while ionizing radiation can cause nucleic acid strand breakage and inhibit viruses. Enveloped viruses are sensitive to lipid solvents and phenols, aldehydes, strong oxidizing agents, and halogenic detergents. Therefore, the CoV can be easily eliminated by 75% ethanol, ether, and chlorine-containing disinfectants. Peracetic acid, chloroform, and other lipid solvents are associated with effective virus destruction.27
Infection Process
The main target cells of CoVs include macrophages, endocrine cells, ganglion cells, dendritic cells, and astrocytes. Recognition of cell surface receptors and adhesion to cells is the first step in infection. The S protein is a transmembrane glycoprotein formed by the S1 subunit at the N terminal and the S2 subunit at the C terminal that are the major antigenic sites on the virus. The S1 subunit contains the receptor binding domain allowing the S protein to bind to host cells. The S2 subunit contains HR1 and HR2 domains that are two α-helix peptides. The S1 subunit binds to the receptor, enabling the S2 fusion peptide to be inserted into the cell membrane, while HR1 and HR2 bind to each other to form a hexamer that completes the fusion between the virus outer membrane and the host cell membrane and allows the injection of genetic materials.28 Currently, receptors that have been found to be used by CoVs include APN/CD13,29 ACE2,30 and CEACAM1.31 After virus entry into the host cell, RNA is used as a template for translation of two polyproteins (1a and 1ab) that are encoded by ORF1. The 3C-like protease and the papain-like protease in polyproteins will hydrolyze polyproteins into 15–16 non-structural proteins, including proteases, RNA replicase, RNA helicase, endonuclease and exonuclease. Following this, the virus RNA forms a replication/transcription complex and completes the synthesis of the negative strand subgenomic RNA, transcription of subgenomic mRNA, and replication of virus genomic gRNA.32 After virus infection of host cells, dendritic cells (DC) will recognize these cells and secrete type I interferons (IFN-α and IFN-β) and inflammatory factors such as IL-1β, IL-6, IL-8, and TNF-α. This will activate downstream signaling pathways and induce natural killer (NK) cells and macrophages to kill or phagocytose infected cells.33,34 The chemokine CCL3 recruits and activates neutrophils, while CCL recruits leukocytes to inflammation sites and induces NK cell proliferation and activation.35,36 However, the immune evasion mechanisms of CoVs can inhibit signaling pathways related to the secretion of type I interferons and chemokines and can impair the function of DCs, NK cells, and neutrophils, thereby interfering with the body’s antiviral response and causing the body to be unable to generate persistent and effective immunity after infection.37 In addition, dissemination to neighboring cells is one of the ways by which CoVs evade immune responses.38
Epidemiological Characteristics of Coronavirus
CoV infections are distributed globally but show regional differences. Humans are generally susceptible and can develop self-limiting acute or chronic persistent infections and can suffer repeated infection and coinfection by multiple respiratory viruses. CoV infections mainly occur during winter and spring. HCoV-229E and HCoV-OC43 are among the most common CoVs, accounting for 10–30% of common colds. Outbreaks occur once every 2–4 years during winter and spring, but pandemics are rare. The infection rate of HCoV-HKU1 is 0.3–4.4%. HCoV-NL63 mainly cause epidemics during summer and autumn. The virus can infect people of all age groups, although infants, elderly people, immunosuppressed patients, and patients with underlying disease are most susceptible. The incidence is around 2%, while the detection rate is higher than for other human CoVs, and epidemics occur yearly. Serological studies have shown that almost everyone will be infected with HCoV-229E, HCoV-NL63, or HCoV-OC43 in childhood. However, repeated infections may occur throughout life due to reduction in antibody titers and viral mutation.39,40 Although human CoV infections often cause mild upper respiratory tract infections, deaths still occur when patients suffer from certain underlying diseases. In 2002, SARS-CoV appeared in southern China before spreading to the rest of the world. Ultimately, SARS-CoV resulted in 8096 infections and 774 deaths in 32 countries, with a mortality rate of 9.56%.41 MERS-CoV first appeared in Saudi Arabia in 2012, causing epidemics in the Middle East. Subsequently, 2494 people were infected, and 858 deaths occurred in 27 countries for a mortality rate of 34.4%.42 There are 203 countries, areas or territories and more than 13876441 confirmed cases of coronavirus disease 2019 (COVID-19) caused by SARS-CoV-2, where the virus infects all age group. There have been 593 087 of deaths from this virus. The crude mortality rates in males, females, and people aged more than 80 years are 2.8%, 1.7%, and 14.8%, respectively. The mortality rate is higher in patients with cardiovascular disease, diabetes, chronic respiratory diseases, or hypertension.3
Clinical Symptoms and Diagnosis of Coronavirus Pneumonia
Symptoms of Coronavirus Infection
The incubation period of human CoV infection41 is around 2–5 days, and the disease course is 6–7 days. CoV infection mainly causes fever, runny nose, cough, and headaches, while gastrointestinal symptoms occur in some cases. However, symptoms are normally mild. Bronchitis, pneumonia, or severe respiratory diseases may result in infants, elderly people, and immunocompromised people. HCoV-229E has a higher proportion of runny nose symptoms compared with other common respiratory diseases. HCoV-OC43 often causes more severe symptoms than HCoV-229E, but asymptomatic infections and occasional severe lower respiratory tract infections may be present. HCoV-HKU1 does not have specific characteristic symptoms and is often diagnosed as bronchiolitis or pneumonia, but infants tend to develop convulsions and febrile seizures. HCoV-NL63 may cause severe cold symptoms and acute respiratory symptoms in infants and immunocompromised adults.
The incubation period of SARS-CoV infection43 is 2–14 days, of which 3–5 days is the most common. Fever is the first symptom to occur, with a temperature of more than 38°C accompanied by headaches, muscle aches, malaise, and diarrhea. Subsequently, pneumonia, frequent coughing, and dyspnea occur. The incubation period of MERS-CoV infection44 is 2–14 days and normally lasts for 5–6 days. Classical symptoms include fever, coughing, and/or shortness of breath, diarrhea, and other gastrointestinal symptoms. The disease rapidly progresses to severe pneumonia and causes respiratory failure, thrombocytopenia, and coagulation disorder. MERS-CoV infection tends to lead to renal failure or septic shock in immunocompromised people. The incubation period of SARS-CoV-23 infection is 1–14 days, of which 3–7 days is the most common incubation period. The main symptoms of SARS-CoV-2 infection include fever, fatigue, and dry cough along with ground-glass opacities and infiltration shadows in both lungs. A minority of patients develop nasal congestion, runny nose, sore throat, and diarrhea. Severely affected patients will experience dyspnea and/or hypoxemia, and critical patients will develop acute respiratory distress syndrome, septic shock, refractory metabolic acidosis, and coagulation disorders. Some SARS-CoV, MERS-CoV, and SARS-CoV-2 patients may be asymptomatic or have only mild symptoms.
Coronavirus Diagnosis
When one or more symptoms are present, the patient should be considered a suspected case for quarantine and clinical diagnosis. This should be combined with the patient’s epidemiological history and clinical symptoms for integrated analysis, and a clinical diagnosis should be made. Respiratory tract samples or blood samples should be used for immunofluorescence assay (IFA), reverse transcription polymerase chain reaction (RT-PCR), enzyme-linked immunosorbent assay (ELISA), or virus cell culture for identification. Additional stool samples can be used for virus isolation and testing to supplement data on digestive tract infection.43
Prevention and Control of Coronavirus in Animal-Source Foods
CoVs are common zoonotic pathogens. Studies have shown that SARS-CoV, MERS-CoV, SARS-CoV-2, HCoV-NL63, and HCoV-229E may originate from bats,44,45 while HCoV-OC43 and HCoV-HKU1 may have originated from rodents and bats46,47 (Table 1). The high population density and widespread distribution of bats provide opportunities for pathogen infection and rapid transmission. When there is frequent contact between bats and humans, companion animals, and livestock, the possibility of cross-species transmission increases. Carnivorous bats may acquire other pathogens from insects or birds and may transmit viruses to predators that prey on bats.48
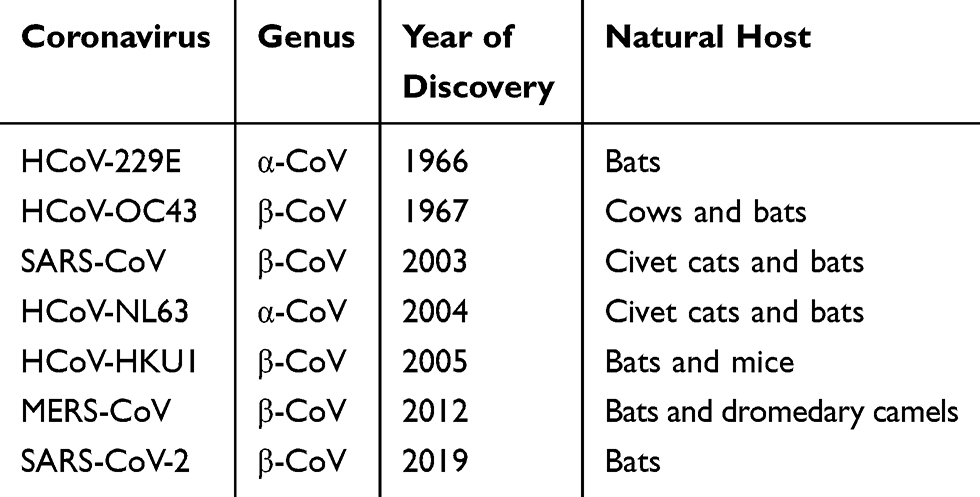 |
Table 1 Discovery, Classification and Natural Host of the Coronaviruses |
The emergence of many zoonotic human diseases, which intimately associated with contact between animal species and with humans, as well as with human diet, has climbed during these decades. For example, SARS, Marburg hemorrhagic fever, and Ebola hemorrhagic fever are associated with human consumption of wildlife. And Public Health England (PHE) also indicated that 60% to 80% of emerging infections are derived from an animal source. And “Bush meat” harvested from remote forested areas remains a risk for animal-derived emerging infections.49 One study suggested that pangolins may be an intermediate host for SARS-CoV-2.50 Consumption of pangolins, illegal but frequent, is present throughout the world that might be an infection pathway of COVID-19. In addition, excessive emphasis on food freshness has resulted in the prevalence of cold foods, raw foods and other consumption methods. However, most bacteria and viruses (eg Ebola virus, SARS-CoV) have strong infectivity under room temperature and refrigeration conditions, causing possible food poisoning or foodborne infections in humans and providing conditions for viral and bacterial outbreaks in human societies. Therefore, China has revised the Wild Animal Conservation Law and adjusted the list of “animal sources of epidemics” to ban the consumption of wildlife. Evidently, CoVs can infect humans, and positive test results for serum antibodies have been attained in civet cats, wild boars, pheasants, cats, rabbits, frogs, camels, and birds. Therefore, it is a high risk of infection from uncooked animal-source foods such as milk and meat.
Even there are some unknown reservoirs, current studies indicate that bats are the main reservoir for CoVs (Figure 1). The virus detection rates of intestinal and stool samples are higher than for respiratory tract or urine samples, indicating that before entering the human population the virus might be easier to infect animals through food residues and stools than other pathways.51 Human are probably infected through direct contact with infected animals, droplets, and excreta. Subsequent direct contact with infected humans, aerosols, and the fecal-oral route enable the spread of CoVs in human populations.52 Serum epidemiological surveys of people involved in game activities have shown that these people have extremely high antibody seroconversion rates.53
 |
Figure 1 Cross-species transmission of human-related coronaviruses. The dashed line indicates potential but unknown transmission. The question mark means potential but no evidence of transmission. |
Although there are limited intermediate hosts for CoV transmission from bats to humans, certain bats can migrate for long distances, thereby increasing the possibility of contact with livestock and increasing the distribution range of CoVs.54 Existing studies have shown that compared with other livestock, pigs tend to promote cross-species transmission of viruses and are more susceptible to bat CoVs (Figure 1). SeACoVs isolated from pig guts are different from known porcine CoVs and are phylogenetically close to the bat CoV HKU2.55,56 In addition, studies have shown that pigs are susceptible to SARS-CoV57 and MERS-CoV.58 The sequence similarity between porcine and human CD26 receptors is 94.5%, which is sufficient for cross-species transmission to occur. In addition, CoVs have been shown to have the potential for recombination in animals.59 Therefore, preventing bat invasion of animal farms should be implemented in addition to monitoring viruses in bats.
Coronavirus Control During Production of Animal-Source Foods
Like wet markets, squalid abattoirs, meat factories and meat markets are known to be hotbeds for disease for deadly pathogens like the ones behind COVID-19, SARS, bird flu, and more (PHE).49 Due to the risk of virus transmission in raw material procurement, slaughter, division, processing, storage, and transportation in processing companies and the foodborne transmission nature of CoVs, residual viruses may be present in raw materials, intermediate products, and finished products. And coronavirus’ apparent ability to thrive in cold, humid air, infection control should be strengthened in the processing of animal-source foods to prevent meat and meat products from becoming vectors for viruses and entering the market. As a large number of people staying in close quarters and sharing limited space, measures should be adopted to prevent infection in company staff.
Routine Control Measures in Foodstuff Manufacturing Companies
A personnel health management system should be established, and annual physical examinations should be conducted. Personnel should only be employed after a health certificate has been obtained. Staff with dysentery, hepatitis A and other digestive tract diseases, pulmonary tuberculosis, or exudative or purulent skin diseases should not be employed.60 During CoV epidemics, foodstuff companies should monitor the temperatures of staff every day, and make some steps to protect workers. For instance, the federal Centers for Disease Control (CDC) and the Occupational Health and Safety Administration (OHSA) recommended providing clean face coverings for employers, rearranging facilities so that workers can remain six feet apart and providing short breaks to allow workers to wash their hands more frequently. When outbreaks occur near the factory, staff should stay home and avoid entering/exiting the factory; personnel movement should be reduced; dormitories should be disinfected daily, and the health status of staff should be recorded. When staff with suspected symptoms occur, work must be immediately stopped; consultation should be carried out at a suitable time, and medical quarantine should be initiated for close contacts.
For CoVs with weak resistance to bacteriocidal substances, staff should wash both hands with detergent before entering the workplace followed by disinfection with 75% alcohol or disinfection with 50 ppm of available chlorine. Operators must disinfect themselves hourly and must wear clean attire in the workplace.
Inspection and quarantine tests should be carried out before animals enter the slaughterhouse, and pre-slaughter testing should be done. Abnormal livestock and poultry should be quarantined and observed. Relevant regulations must be followed for management of livestock and poultry that are not suitable for normal slaughter. When animals that have died due to disease are discovered, they should be processed according to the relevant requirements, and site cleaning and disinfection should be performed. Before the end of the workday, the slaughterhouse should be thoroughly cleaned, and tools should be cleaned and disinfected.
Meat and poultry processing facilities have been linked to a number of coronavirus outbreaks in many counties, such as Germany and America. Processing facilities and equipment need to be periodically cleaned and disinfected. Processing tools should not touch the ground or unclean surfaces. Tools should be immediately cleaned and disinfected after use by each shift and should be placed in designated clean and well-ventilated zones. Moreover, some plants have implemented thermal scanning and installed plexiglass barriers on production floors and in break rooms.
The factory should be kept clean and free of insects and rodents, and the factory and workshop should be disinfected in a timely manner. Ultraviolet irradiation for 30 min and above can be used. Chlorine dioxide (20 g/m3, 100–200 mg/kg), 0.1% benzalkonium bromide + 3% bleach powder, 3% sodium hydroxide or NaClO (400–500 mg/kg) solution should be used for spray disinfection.
Raw materials should be procured from healthy animals in non-epidemic regions, and the supplier must provide Animal Health Certificates and related documents. Supplies from unknown sources should not be allowed. Effective protection measures should be employed during the transportation of raw materials to ensure against contamination. Raw materials that have passed the acceptance check should be quickly warehoused. In addition, a management system should be established, and designated staff should manage and periodically conduct quality and health checks, clear expired or spoiled raw materials, and prevent cross-contamination between raw materials and finished products.59
Control Measures for Coronaviruses
During CoV outbreaks, an epidemic control emergency response team should be established based on the above measures. The members of the team would include CoV testing staff, basic medical staff, company directors, and disease prevention and control center monitors who will test and monitor company staff, raw materials, finished products, and the factory.
The emergency plan will be immediately adopted once positive results are detected among the staff. Confirmed cases should be treated promptly, and quarantine should be implemented for close contacts. When the raw material tests positive for CoV, that batch of raw materials should not be allowed to enter the company and must be disposed of and reported to the local disease prevention and control center and the National Medical Products Administration, and pathogen tracing of the upstream production chain should be carried out.
In food supply chain, actions also need to be taken for coronavirus has been detected on the packing surface of meat and shrimp, on the chopping board of salmon. CoVs are sensitive to heat, while they could survive in cold and wet conditions for weeks to months that animal-source foods may be contaminated by CoVs when comes into contact with infected people during storage and transportation. And people might be infected for CoVs could regain its activity with the gradual rise of temperature. Even these viruses may lose the ability to infect people, for its pathogenicity, consumers afraid to buy these products with viruses on the packages. Thus, strict disinfections should be taken through the supply chain, including vehicles, refrigerated warehouses, shelves and more. Once stuffs in supply chain are confirmed, they need to be quarantine and stricter disinfections should be taken. If an intermediate product or finished product tests positive, the local disease prevention and control center must be notified, the product must be destroyed, and the company must be thoroughly disinfected.
Conclusion
Currently, CoVs have caused three major global epidemics (SARS, MERS, and COVID-19) that have affected the lives and health of tens of thousands of people. Progress has enabled humans to improve methods for acquiring animal-source foods, from hunting and domestication to modern farming. This has resulted in massive increases in the quantity and quality of animal-source foods. At the same time, human hunting of wildlife and consumption of raw animal-source foods has continued to increase, resulting in epidemics caused by viruses. For there are currently no effective vaccines or drugs for CoVs, deviant consumption mentality should be curbed. Meat is an indispensable nutrient source for humans. As viruses can infect livestock and cause a potential threat, pathogen transmission from food sources requires food safety measures during processing to control virus transmission.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Tyrrell DAJ, Bynoe ML. Cultivation of a novel type of common-cold virus in organ cultures. Br Med J. 1965;1:1467–1470. doi:10.1136/bmj.1.5448.1467
2. Drexler JF, Gloza-Rausch F, Glende J, et al. Genomic characterization of severe acute respiratory syndrome-related coronavirus in European bats and classification of coronaviruses based on partial RNA-dependent RNA polymerase gene sequences. J Virol. 2010;84:11336–11349. doi:10.1128/JVI.00650-10
3. World experts and funders set priorities for COVID-19 research. WHO; February 12, 2020. Available from: https://www.who.int/news-room/detail/12-02-2020-world-experts-and-funders-set-priorities-for-covid-19-research.
4. Woo PC, Lau SK, Chu CM, et al. Characterization and complete genome sequence of a novel coronavirus, coronavirus HKU1, from patients with pneumonia. J Virol. 2005;79:884–895. doi:10.1128/JVI.79.2.884-895.2005
5. Woo PC, Yuen KY, Lau SK. Epidemiology of coronavirus-associated respiratory tract infections and the role of rapid diagnostic tests: a prospective study. Hong Kong Med J. 2012;18:22–24.
6. Pneumonia caused by the novel coronavirus is placed under the control of infectious disease statutory. National Health Commission of the People’s Republic of China; January 20, 2020. Available from: http://www.nhc.gov.cn/jkj/s7915/202001/e4e2d5e6f01147e0a8df3f6701d49f33.shtml.
7. Lee P, Hsueh P. Emerging threats from zoonotic coronaviruses-from SARS and MERS to 2019-nCoV. J Microbiol Immunol. 2020. doi:10.1016/j.jmii.2020.02.001
8. Li G, de Clercq E. Therapeutic options for the 2019 novel coronavirus. Nat Rev Drug Discov. 2020;19:149–150. doi:10.1038/d41573-020-00016-0
9. Cui J, Li F, Shi Z. Origin and evolution of pathogenic coronaviruses. Nat Rev Microbiol. 2019;17:181–192. doi:10.1038/s41579-018-0118-9
10. Johnson BA, Graham RL, Menachery VD. Viral metagenomics, protein structure, and reverse genetics: key strategies for investigating coronaviruses. Virol. 2018;517:30–37. doi:10.1016/j.virol.2017.12.009
11. International Committee on Taxonomy of Viruses. Taxonomy history: cornidovirineae. ICTV; February 18, 2017. Available from: https://talk.ictvonline.org/taxonomy/p/taxonomy-history?taxnode_id=20186105.
12. Baudoux P, Carrat C, Besnardeau L, et al. Coronavirus pseudoparticles formed with recombinant M and E proteins induce alpha interferon synthesis by leukocytes. J Virol. 1998;72:8636–8643. doi:10.1128/JVI.72.11.8636-8643.1998
13. Huang C, Hsu Y, Chiang W, et al. Elucidation of the stability and functional regions of the human coronavirus OC43 nucleocapsid protein. Protein Sci. 2009;18:2209–2218. doi:10.1002/pro.225
14. Sanchez CM, Izeta A, Sanchez-morgado JM, et al. Target recombination demonstrates the spike gene of transmissible gastroenteritis coronavirus is a determination of its tropism and virulence. J Virol. 1999;73:7607–7618. doi:10.1128/JVI.73.9.7607-7618.1999
15. Escor D, Oetego J, Laud H, et al. The membrane M protein carboxy terminal bind to transmissible gastroenteritis coronavirus core and contribute to core stability. J Virol. 2001;75:1312–1324. doi:10.1128/JVI.75.3.1312-1324.2001
16. Corse E, Machamer CE. Infectious bronchitis virus E protein is targeted to the golgi complex and directs release of virus-like particles. J Virol. 2000;74:4319–4326. doi:10.1128/JVI.74.9.4319-4326.2000
17. Monto AS. Medical reviews, Coronaviruses. Yale J Biol Med. 1947;47:234–251.
18. Sturman LS, Holmes KV. The molecular biology of coronaviruses. Adv Virus Res. 1983;28:35–122.
19. Izeta A, Smerdou C, Alonso S, et al. Replication and packaging of transmissible gastroenteritis coronavirus-derived synthetic minigenomes. J Virol. 1999;73:1535–1545. doi:10.1128/JVI.73.2.1535-1545.1999
20. Spaan WJM, Delius H, Skinner M, et al. Coronavirus mRNA synthesis involves fusion of non-contiguous sequences. EMBO J. 1983;2:1839–1844. doi:10.1002/j.1460-2075.1983.tb01667.x
21. Sawichi SG, Sawicki DL. A new model for coronavirus transcription. Boston: coronavirus and arterviruses. Adv Exp Med Biol. 1998;440:215–219.
22. Enjuanes L, Sola I, Almazan F, et al. Coronavirus derived expression systems. J Biotech. 2001;88:183–204. doi:10.1016/S0168-1656(01)00281-4
23. Khan RM, Al-Dorzi HM, Al Johani S, et al. Middle East respiratory syndrome coronavirus on inanimate surfaces: a risk for health care transmission. Am J Infect Control. 2016;44:1387–1389. doi:10.1016/j.ajic.2016.05.006
24. Pyankov OV, Bodnev SA, Pyankova OG, et al. Survival of aerosolized coronavirus in the ambient aid. J Aerosol Sci. 2018;115:158–163. doi:10.1016/j.jaerosci.2017.09.009
25. Otter JA, Donskey C, Yezli S, et al. Transmission of SARS and MERS coronaviruses and influenza virus in healthcare settings: the possible role of dry surface contamination. J Hosp Infect. 2016;92:235–250. doi:10.1016/j.jhin.2015.08.027
26. Leclercq I, Batejat C, Burguiere AM, et al. Heat inactivation of the Middle East respiratory syndrome coronavirus. Influenza Other Respir. 2014;8:585–586. doi:10.1111/irv.12261
27. Zhang C, Wang G, Yao Y. Resistance and stability capacity of SARS-CoV against physicochemical factors in environment. Mod Prev Med. 2004;31:1–3.
28. Du L, He Y, Zhou Y, et al. The spike protein of SARS-CoV - a target for vaccine and therapeutic development. Nat Rev Microbiol. 2009;7:226–236. doi:10.1038/nrmicro2090
29. Yeager CL, Ashmun RA, Williams RK, et al. Human aminopeptidase N is a receptor for human coronavirus 229E. Nature. 1992;357:420–422. doi:10.1038/357420a0
30. Li W, Moore MJ, Vasilieva N, et al. Angiotensin-converting enzyme 2 is a functional receptor for the SARS coronavirus. Nature. 2003;426:450–454. doi:10.1038/nature02145
31. Williams RK, Jiang GD, Holmes KM. Receptor for mouse hepatitis virus is a member of the carcinoembryonic antigen family of glycoproteins. Proc Natl Acad Sci U S A. 1991;88:5533–5536. doi:10.1073/pnas.88.13.5533
32. Wang H, Ding C, Liao Y. Cell entry pathway of coronavirus. Chin J Virol. 2019;35:964–971.
33. Stetson DB, Medzhitov R. Type I interferons in host defense. Immunity. 2006;25:373–381. doi:10.1016/j.immuni.2006.08.007
34. Fensterl V, Sen GC. Interferons and viral infections. Biofactors. 2009;35:14–20. doi:10.1002/biof.6
35. Sherry B, Tekamp-Olson P, Gallegos C, et al. Resolution of the two components of macrophage inflammatory protein 1, and cloning and characterization of one of those components, macrophage inflammatory protein 1 beta. J Exp Med. 1988;168:2251–2259. doi:10.1084/jem.168.6.2251
36. Maghazachi AA, Al-Aoukaty A, Schall TJ. CC chemokines induce the generation of killer cells from CD56+ cells. Eur J Immunol. 1996;26:315–319. doi:10.1002/eji.1830260207
37. Yang Q, Tuo J, Huang X, et al. Preliminary mechanism study of HCoV-OC43 escape from human dendritic cell immune elimination. Chin J Immunol. 2017;33:488–493.
38. Dominguez SR, Travanty EA, Qian Z, et al. Human coronavirus HKU1 infection of primary human type II alveolar epithelial cells: cytopathic effects and innate immune response. PLoS One. 2013;8:e70129. doi:10.1371/journal.pone.0070129
39. Dong C. Advances in human coronavirus 229E. Occup Health. 2014;30:3625–3628.
40. Zhang Y. Molecular Epidemiology and Phylogenetic Dynamics of Human Coronavirus OC43. Beijing: Peking Union Medical College; 2014.
41. WHO SARS risk assessment and preparedness framework October 2004. WHO; 2004. Available from: https://www.who.int/csr/resources/publications/WHO_CDS_CSR_ARO_2004_2/en/.
42. WHO MERS global summary and assessment of risk. WHO; 2019. Available from: https://www.who.int/csr/disease/coronavirus_infections/archive_updates/en/.
43. Trivedi S, Miao C, Al-Abdallat MM, et al. Inclusion of MERS-spike protein ELISA in algorithm to determine serologic evidence of MERS-CoV infection. J Med Virol. 2017;90:367–371. doi:10.1002/jmv.24948
44. Su S, Wong G, Shi W, et al. Epidemiology, genetic recombination, and pathogenesis of coronaviruses. Trends Microbiol. 2016;24:490–502. doi:10.1016/j.tim.2016.03.003
45. Zhu N, Zhang D, Wang W, et al. A novel coronavirus from patients with pneumonia in China. N Engl J Med. 2020;382:727–733. doi:10.1056/NEJMoa2001017
46. Forni D, Cagliani R, Clerici M, et al. Molecular evolution of human coronavirus genomes. Trends Microbiol. 2016;25:35–48. doi:10.1016/j.tim.2016.09.001
47. Wu Z, Yang L, Ren X, et al. Deciphering the bat virome catalog to better understand the ecological diversity of bat viruses and the bat origin of emerging infectious diseases. ISME J. 2016;10:609–620. doi:10.1038/ismej.2015.138
48. Rodhain E. Bats and viruses: complex relationships. B Soc Pathol Exot. 2015;108:272–289. doi:10.1007/s13149-015-0448-z
49. Emerging infections: how and why they arise. Public Health England; February 27, 2019. Available from: https://www.gov.uk/government/publications/emerging-infections-characteristics-epidemiology-and-global-distribution/emerging-infections-how-and-why-they-arise.
50. Cyranoski D. Did pangolins spread the china coronavirus to people. Nature. 2020. doi:10.1038/d41586-020-00364-2
51. Subudhi S, Papin N, Bollinger TK, et al. A persistently infecting coronavirus in hibernating Myotis lucifugus, the North little brown bat. J Gen Virol. 2017;98:2297–2309. doi:10.1099/jgv.0.000898
52. Alloacati N, Petrucci AG, Giovanni PD, et al. Bat-man disease transmission: zoonotic pathogens from wildlife reservoirs to human populations. Cell Death Discov. 2016;2:16048. doi:10.1038/cddiscovery.2016.48
53. Xiong L, Jiang L, Jiang Q. Prevalence and control of human diseases caused by beta coronavirus (β-CoVs). Shanghai J Prev Med. 2020;32:1–12.
54. Wang L, Su S, Bi Y, et al. Bat-origin coronaviruses expand their host range to pig. Trends Microbiol. 2018;26:466–470. doi:10.1016/j.tim.2018.03.001
55. Gong L, Li J, Zhou Q, et al. A new bat-HKU2-like coronavirus in swine, China, 2017. Emerg Infect Dis. 2017;23:1607–1609. doi:10.3201/eid2309.170915
56. Pan YF, Tian XY, Qin P, et al. Discovery of a novel swine enteric alphacoronavirus (SeACoV) in southern China. Cell Death Discov. 2017;211:15–21.
57. Chen WJ, Yan MH, Yang L, et al. SARS-associated coronavirus transmitted from human to pig. Emerg Infect Dis. 2005;11:446–448. doi:10.3201/eid1103.040824
58. Vergara-Alert J, van de Brand JMA, Widagdo W, et al. Livestock susceptibility to infection with Middle East respiratory syndrome coronavirus. Emerg Infect Dis. 2017;23:232–240. doi:10.3201/eid2302.161239
59. Sabir JSM, Lam TT, Ahmed MM, et al. Co-circulation of three camel coronavirus species and recombination of MERS-CoVs in Saudi Arabia. Science. 2016;351:81–84. doi:10.1126/science.aac8608
60. Standardization Administration.GB 14881-2013 National Standard for Food Safety: General Hygienic Standard for Food Production. China standard press; 2014.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.