Back to Journals » OncoTargets and Therapy » Volume 19
Research Advances on Targets and Mechanisms in Cancers Complicated by Cardiovascular Diseases
Received 15 November 2025
Accepted for publication 27 January 2026
Published 7 February 2026 Volume 2026:19 581768
DOI https://doi.org/10.2147/OTT.S581768
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Sanjay Singh
Jianing Li,1 Peili Wang2
1Graduate School, Heilongjiang University of Chinese Medicine, Harbin, People’s Republic of China; 2Xiyuan Hospital, China Academy of Chinese Medical Sciences, Beijing, People’s Republic of China
Correspondence: Peili Wang, Email [email protected]
Purpose: Cancers complicated by cardiovascular diseases (CVDs) are increasingly becoming major limiting factors affecting patients’ long-term quality of life and clinical outcomes. Systematic identification of therapeutic targets and their clinical development status is crucial for optimizing treatment strategies. Therefore, this study aimed to establish a target-based analytical framework to systematically map the distribution, developmental stage, maturity, and mechanistic characteristics of clinical trials investigating tumors co-occurring with CVD, thereby identifying potential therapeutic targets.
Patients and Methods: We analyzed clinical trial data on treatments for cancers complicated by CVDs. A total of 58 clinical trials were included and examined across multiple dimensions, including target distribution, development stage, and disease relevance.
Results: Forty-five therapeutic targets were identified, with coagulation Factor X, thrombin, and serpin family C member 1 (SERPINC1) emerging as high-frequency core targets. Most studies focused on coagulation, inflammation, and endothelial pathways. Significant variations were observed in completion status and research phase across different targets, with some demonstrating dual therapeutic and cardiovascular regulatory potentials.
Conclusion: Coagulation and endothelium-related targets emerged as key links between cancer progression and cardiovascular complications. SERPINC1 and 3-hydroxy-3-methylglutaryl-CoA reductase showed potential for synergistic therapy. This study provides a comprehensive overview of targeted therapies for tumors with concomitant CVD, revealing key pathways and under-explored mechanisms. It offers data-driven insights and directional guidance for precision treatment design.
Keywords: cardiovascular disease, therapeutic target, cancer, clinical trial, cardiovascular complication
Introduction
The overall survival rate of patients with cancer has recently improved with continuous advancements in early screening technology for tumors and the widespread application of diverse treatment strategies.1 However, the extending lifespan also introduces new challenges. For example, cardiovascular toxicity resulting from anti-tumor therapy and cancer-induced cardiovascular complications are increasingly becoming key limiting factors that affect patients’ long-term quality of life and clinical outcomes.2 Epidemiological evidence indicates that cardiovascular disease has become one of the leading non-cancer causes of morbidity and mortality among cancer survivors. According to estimates, up to 20%–30% of patients with cancer may develop cardiovascular complications, including cardiomyopathy, arrhythmia, and ischemic heart disease.3 Moreover, venous thromboembolism (VTE) represents the second leading cause of death in patients with cancer after cancer itself. VTE necessitates long-term anticoagulant therapy, carries an annual risk of bleeding complications at 12%, and presents a substantial annual recurrence risk of 21% even with anticoagulation treatment.4
Anti-tumor medications can cause damage to the cardiovascular system through various mechanisms. For example, anthracycline drugs can cause dose-dependent myocardial injury and reduced ejection fraction; human epidermal growth factor receptor 2 (HER2) inhibitors may lead to myocardial dysfunction by inhibiting the HER2 signaling pathway, disrupting mitochondrial function, and inducing oxidative stress in cardiomyocytes; and vascular endothelial growth factor pathway inhibitors are strongly associated with the risks of hypertension and thrombosis.5–7 While the widespread use of immune checkpoint inhibitors (ICIs) has significantly improved the efficacy of treatment for various tumors, it has also been associated with serious adverse reactions, such as immune-related myocarditis, pericarditis, and malignant arrhythmia, indicating that their potential cardiotoxicity should not be ignored.8
Moreover, even in the absence of anticancer treatment, certain cancers can directly or indirectly impair the cardiovascular system through multiple mechanisms. For example, some cancers continuously induce systemic chronic inflammation, leading to a sustained elevation of inflammatory mediators and contributing to cardiovascular pathologies such as atherosclerosis, endothelial dysfunction, and myocardial remodeling, thereby markedly increasing the risk of cardiovascular events.9 Tumor-induced hypercoagulability is another common condition, characterized by the overexpression of coagulation factors, platelet activation, and inhibition of fibrinolysis—all of which predispose patients to VTE, pulmonary embolism, and arterial thrombosis.10 Importantly, this prothrombotic state can occur even in patients who have not received radiotherapy or chemotherapy. In addition, tumors originating from or adjacent to the heart may directly invade the pericardium, myocardium, or coronary arteries, or cause cardiac involvement via hematogenous metastasis, resulting in severe complications such as pericardial effusion, cardiac tamponade, malignant arrhythmia, and congestive heart failure.11 Although these non-treatment-related cardiovascular abnormalities are often underestimated in clinical practice, they have a profound impact on patient prognosis, treatment selection, and therapeutic timing. Therefore, it is urgent to establish more sensitive detection approaches and integrated management strategies, and to incorporate them into research frameworks of tumor-related cardiovascular comorbidities for systematic evaluation.
In response to the complex clinical needs of patients with concomitant cancer and cardiovascular disease, cardio-oncology has emerged as an interdisciplinary field dedicated to optimizing therapeutic strategies, preventing adverse cardiac events, and developing personalized cardioprotective interventions. Systematically understanding the characteristics and distribution patterns of molecular targets currently under development or experimentation, within the context of the rapid development of precision medicine, is essential for identifying global research priorities, revealing development trends, and optimizing clinical decisions. Currently, the lack of standardization in treatment protocols and the fragmented nature of drug development efforts have led to a diversity of therapeutic approaches, posing significant challenges for both patients and clinicians. Moreover, balancing therapeutic efficacy against cardiac toxicity remains a critical challenge in drug development. While some novel therapies show promise, consistent guidelines on reconciling these benefits with side effects are still lacking. These challenges reinforce the rationale to target analysis and clinical trial maturity, underscoring the necessity for further research. Specifically, little is known about the distribution of therapeutic targets, clinical trial stages, completion status, safety assessments, and monitoring settings among populations with cancers complicated by cardiovascular diseases. This knowledge gap hampers the evaluation of whether current research disproportionately focuses on particular cancer types or molecular targets and whether opportunities for therapeutic synergy or overlooked cardiovascular toxicity pathways exist.
Therefore, the present study takes the target as the core analysis unit and relies on the Trialtrove clinical trial database to comprehensively organize and analyze registered research related to “cancer combined with cardiovascular disease” from multiple dimensions, covering target distribution, clinical development progress, temporal evolution trends, regional layout, mechanism of action, safety monitoring settings, and existing research blind spots. We aim to depict a panoramic map of the field and provide data-driven support and decision-making reference for the design of precise treatment strategies, safety control of combination therapy, and future research priorities in oncology cardiology.
Materials and Methods
Data Source and Selection Criteria
Data on clinical trials within the therapeutic areas of cardiovascular and oncology were retrieved from the Trialtrove database (https://clinicalintelligence.citeline.com/). All relevant studies registered up to November 1, 2025, were considered. The search was conducted using the following keywords: Therapeutic area: “Cardiovascular” and “Oncology.” To ensure precision and clinical relevance, only randomized controlled trials were included in the final analysis.
Inclusion and Exclusion Criteria
To maintain the methodological integrity of this review, well-defined inclusion and exclusion criteria were applied. Studies were included if they (i) addressed both cardiovascular and oncology therapeutic areas, (ii) investigated a specific therapeutic mechanism or molecular target, and (iii) were structured as clinical trials. The exclusion criteria were (i) the absence of clearly defined mechanisms or targets; (ii) insufficient or incomplete datasets; and (iii) non-interventional designs such as observational studies, lacking the rigor necessary to evaluate therapeutic efficacy. Additional evaluation was undertaken in cases where the therapeutic target was ambiguously or partly described to determine eligibility. Studies lacking sufficient information to definitively identify therapeutic mechanisms were excluded from the final dataset.
Handling Incomplete Data
A stringent methodological approach was employed to identify and evaluate gaps within the dataset, thereby enhancing the overall reliability and precision of this review. Clinical trials lacking critical outcome information, particularly those without clearly defined primary or secondary endpoints, were excluded from consideration. Studies with ambiguous therapeutic intent underwent additional assessment and were included only if their molecular targets could be clearly identified through external sources or validated databases. Furthermore, studies presenting clearly articulated therapeutic objectives and comprehensive datasets were prioritized, ensuring analytical consistency and supporting more robust comparative insights.
Results
Overall Research Overview
This study analyzed 58 clinical trials focusing on cancer combined with cardiovascular disease. The included studies span Phase I–IV clinical trials and involve multiple systemic disease combinations. Notably, the overall number of clinical trials focusing on cancer combined with cardiovascular disease has been steadily increasing since 1995, with a particularly significant rise in the frequency of trial initiation observed since 2021. In the early stages, clinical trials were relatively rare and mostly concentrated within a single phase of research. Between 2000 and 2010, only a few clinical trials were initiated annually, with some years showing no relevant records. Phase I clinical studies have demonstrated notable activity from 2021 to 2023, with approximately five trials initiated annually, indicating a continuous increase in research efforts focused on exploring pathological mechanisms and evaluating novel treatment strategies within this field. Meanwhile, the number of joint phase trials such as phase I/II, Phase II/III, and later stage trials including phases III and IV has also increased. This trend reflects that some intervention measures have advanced from the initial validation stage to the efficacy evaluation and application stage. Clinical studies on tumors combined with cardiovascular disease are gradually evolving into a continuous research and development pathway, progressing from early-stage exploration to late-stage clinical validation. The research system is continually improving, and the stage structure is becoming more well-organized (Figure 1).
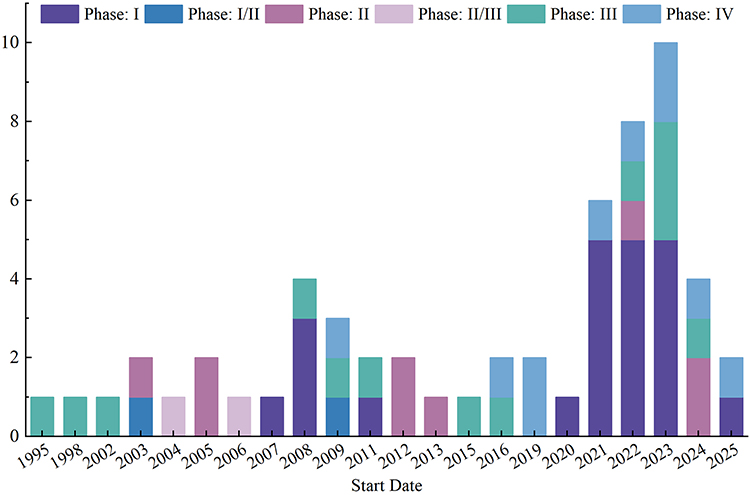 |
Figure 1 Trial phase and trial status distribution of clinical trials for cancers complicated by cardiovascular diseases. |
Target Analysis in Clinical Trials
This study examined 45 distinct therapeutic targets, highlighting the broad application and evolving trends in target-based research across diverse comorbidity contexts. Building on the overall landscape of comorbidity research, the analysis subsequently focused on identifying the most frequently investigated molecular targets. Ten high-frequency research targets were identified across all studies, representing current hotspots in the field. These targets include coagulation factor X (Factor X), coagulation factor II (thrombin), serpin family C member 1 (SERPINC1), estrogen receptor (ER), IKAROS family zinc finger 1 (IKZF1), cereblon (CRBN), KRAS proto-oncogene (GTPase), 3-hydroxy-3-methylglutaryl-CoA reductase (HMGCR), Bruton tyrosine kinase (BTK) and endothelin receptor type B (EDNRB). Among these targets, Factor X was the most frequently investigated, featured in 22 studies, followed by thrombin and SERPINC1, each appearing in 18 studies (Figure 2). These 10 high-frequency targets were mentioned 89 times, accounting for 67% of all recorded target frequencies. This underscores their significant role in disease mechanism studies and targeted drug development within comorbidity-focused research.
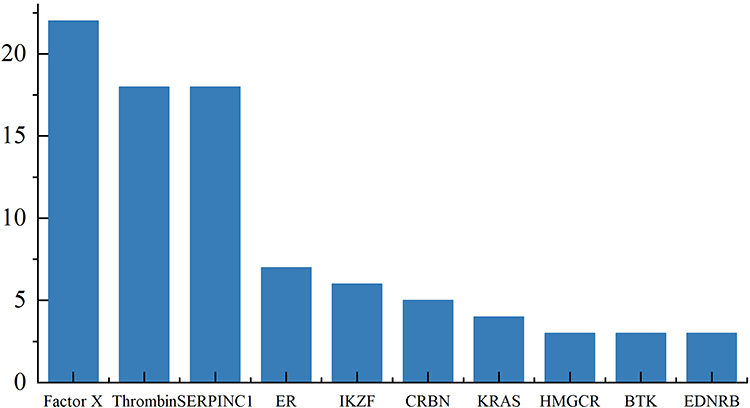 |
Figure 2 Targets distribution of clinical trials for cancers complicated by cardiovascular diseases. |
Completion Level and Development Stage of Target Research
To systematically evaluate the maturity of different targets in clinical development pathways, we selected 10 representative drug targets and comprehensively analyzed their trial completion ratios and stage distributions. The convergence of the studies was assessed using the completion rate (percentage of completed trials) and reflected their stage maturity by the proportion of Phase III+IV trials. Additionally, the joint evaluation of two indicators helps identify targets that have stabilized during the research and development process, along with potential targets that remain in the early stages of validation. Figure 3 presents the detailed parameters.
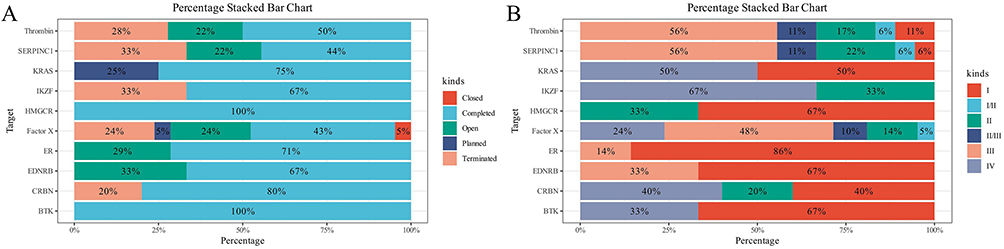 |
Figure 3 Trial status and phase status of targets in clinical trials of cancer combined with cardiovascular disease. (A) Trial status of targets in clinical trials of cancer combined with cardiovascular disease. (B) Trial phase of targets in clinical trials of cancer combined with cardiovascular disease. |
Regarding trial completion status, the completion rates of BTK and HMGCR reached 100%, while those of CRBN, KRAS, and ER were 80%, 75%, and 71%, respectively, indicating smooth progress in their clinical research. The completion rates of EDNRB, IKZF1, Factor X, SERPINC1, and Thrombin were 67%, 67%, 43%, 44%, and 50%, respectively. Notably, the results indicate that although some target projects have advanced to the mid-to-late clinical stages, many trials remain open, planned, or terminated, and overall progress remains insufficient. Figure 4 presents the detailed parameters.
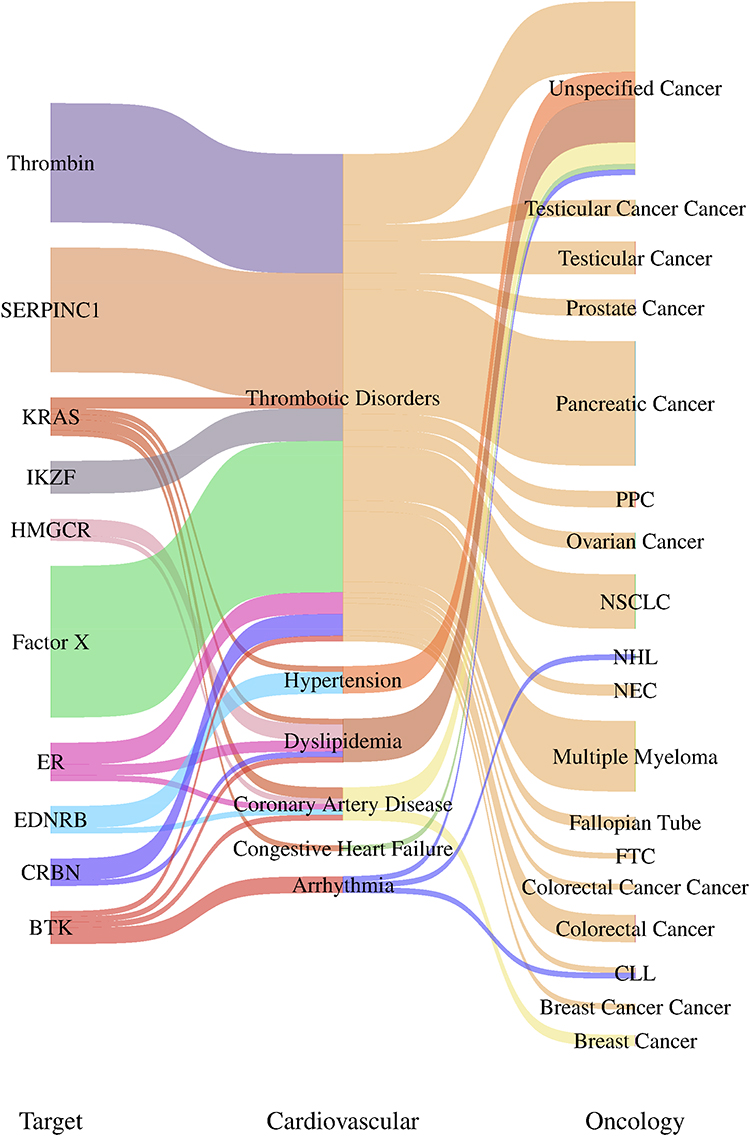 |
Figure 4 Sankey diagram of targets and diseases. |
According to the stage distribution analysis results, the proportion of phase III+IV trials for Factor X, SERPINC1, and thrombin was 72%, 56%, and 56%, respectively. This indicates that most of their studies have progressed to the mid-to-late stages and demonstrate high clinical maturity. The proportion of phase III+IV trials for KRAS was 50%, indicating that half of the research has advanced to the later stage; however, some projects focused on the early stages are still ongoing. For BTK and CRBN, the proportion of phase III+IV trials was 33% and 40% respectively, with relatively lagging stage advancement. The proportion of late-stage trials for ER was only 14%, implying that although its completion rate is high, most research remains in the early stages. All trials involving HMGCR were confined to phases I and II, with no phase III+IV studies identified. This suggests that its development pathway converged on early-stage indications or that no expanded studies have been conducted following pre-market evaluation. IKZF1 and EDNRB have not yet progressed to Phase IV, indicating that their overall development remains in the early stage of clinical validation.
Each target can be categorized based on the dual dimensional indicators of completion and stage maturity, as follows: (i) targets with high completion rates and stage maturity, such as KRAS, SERPINC1, Factor X, and thrombin, which have strong conversion potential; (ii) those with high completion but limited stage advancement, such as BTK and CRBN, where strengthening later-phase research design and accumulating additional evidence is recommended; (iii) those with medium to low completion and maturity levels, such as IKZF1 and EDNRB, which remain in the validation phase; and (iv) those with high completion rates but early-phase research, such as HMGCR and ER, where subsequent indications expansion or post-market real-world studies should be considered.
Distribution of Targets in Tumor and Cardiovascular Disease Types
Figure 4 shows the target network connecting cardiovascular disease and tumors. Each node represents a molecular target, cardiovascular phenotype, or tumor. These connections describe the comorbidity or mechanism correlations found in recent clinical and transformation studies.
In tumor indications, KRAS and HMGCR demonstrated a strong association with solid tumors. BTK and CRBN were mainly limited to hematological malignancies, including chronic lymphocytic leukemia (CLL), non-Hodgkin lymphoma, and multiple myeloma, reflecting their targeted roles in B-cell receptor (BCR) signaling and proteasome regulation therapies. ER signal transduction is still mainly limited to hormone-dependent cancers, including breast cancer and fallopian tube cancer.
In the cardiovascular phenotype, Factor X and Thrombin showed a strong correlation with thrombotic diseases, highlighting their clinical relevance in anticoagulant therapy trials. The key enzyme HMGCR targeted by statins was mainly associated with dyslipidemia and coronary artery disease, which is consistent with its lipid-lowering and pleiotropic vascular effects. EDNRB and BTK were associated with arrhythmia and hypertension, indicating potential off-target cardiovascular responsibility or shared signaling mechanisms, particularly through endothelial and inflammatory pathways. SERPINC1 was also a key regulatory factor in coagulation, located at the interface between thrombosis and cancer, emphasizing its role in tumor-associated coagulation disorders.
Notably, the Sankey network revealed that thrombosis and hypertension phenotypes are the most common cardiovascular complications among all tumor types. Thrombosis-related targets, such as Thrombin, SERPINC1, and Factor X, were related not only to pancreatic and ovarian cancers, but also to hematological malignancies. Meanwhile, dyslipidemia-related targets and vascular signaling mediators appeared to bridge cardiac metabolic disorders and breast or prostate cancer, indicating a potential two-way interaction driven by systemic inflammation and metabolic remodeling.
Discussion
This study systematically analyzed the landscape of clinical trials involving patients with concomitant cardiovascular disease and cancer using data retrieved from the Trialtrove database. We mapped the evolution of research activity, target distribution, and developmental maturity within this interdisciplinary domain by organizing and comparing 58 randomized controlled trials across multiple phases and therapeutic areas. The analysis revealed a steady increase in clinical trial volume since 1995, with a marked surge after 2021, indicating growing clinical and research attention to cardio-oncology comorbidities. To further enrich the landscape analysis, we incorporated a detailed examination of geographical or funding source distribution. Across different regions, the conduct of drug research and clinical trials is significantly influenced by funding availability, policy environments, and clinical needs. For instance, drug development in Europe and North America typically relies on large-scale pharmaceutical companies and government funding, whereas research in certain emerging markets may depend more heavily on local government or regional funding sources. Among the 45 identified molecular targets, Factor X, thrombin, and SERPINC1 were the most frequently investigated, reflecting the central role of coagulation and vascular pathways in tumor progression and cardiovascular complications. Importantly, this study provides a unique contribution by systematically characterizing research trends, maturity levels, and knowledge gaps through a target-based analytical framework. It offers new insights into the current state and future direction of clinical research on cancer-related cardiovascular disease.
In-depth analysis revealed that coagulation and endothelial signaling pathways predominate among high-frequency therapeutic targets, emphasizing their dual relevance to both tumor biology and cardiovascular pathology.12 Specifically, Factor X and Thrombin are closely associated with thrombotic disorders and are recurrently implicated across multiple tumor types.13 Hypercoagulable states are linked to both the neoplasm and its treatment modalities throughout tumor initiation and progression.14 The tumor microenvironment (TME) upregulates multiple components of the coagulation cascade, forming a procoagulant network centered on tissue factor and cancer procoagulants (CPs). CP is a uniquely expressed serine protease in numerous malignancies that directly activates Factor X independent of Factor VII, thereby accelerating prothrombin conversion to thrombin. This mechanism has been validated in experimental tumor models and human tumor tissues, providing a molecular basis for the elevated thrombin generation observed in patients with cancer.15
Thrombin is an effective signaling molecule that not only plays a classical role in fibrin formation but also acts as an effective signaling molecule via protease-activated receptors (PARs). It amplifies the release of inflammatory cytokines, platelet aggregation, cell adhesion, and disruption of the vascular endothelial barrier.16–18 These multifaceted effects not only contribute to tumor cell proliferation, invasion, and metastasis but also lead to vascular dysfunction through endothelial barrier disruption, increased permeability, and maladaptive remodeling.19 Clinical and translational evidence consistently demonstrates that patients with active malignancies exhibit heightened thrombin generation potential. This is driven by tumor cells directly releasing procoagulant factors and indirectly activating platelets, leukocytes, extracellular vesicles, and neutrophil extracellular traps.20 Notably, this forms a self-reinforcing hemostasis−inflammation−tumor cycle that increases the risk of VTE and arterial cardiovascular events. Randomized controlled trials support the clinical significance of this self-reinforcing cycle. Direct oral anticoagulants (DOACs) targeting Factor X have demonstrated superior efficacy in managing cancer-associated thrombosis (CAT). Clinical studies show that DOACs effectively prevent and manage CAT; reduce VTE recurrence; and offer advantages over traditional vitamin K antagonists, including rapid onset of action, less frequent monitoring, and fewer drug interactions.21,22
SERPINC1, which encodes antithrombin III (ATIII), acts as a key endogenous inhibitor within the coagulation cascade in contrast to the procoagulant mechanisms driven by Factor X and thrombin. Antithrombin effectively inhibits the coagulation process by forming irreversible complexes with thrombin and activated Factor Xa, thereby playing a central role in maintaining blood fluidity and preventing thrombosis.23 Deficiency or impaired function of SERPINC1 is strongly associated with an elevated risk of VTE,24 rendering it a critical protective factor in the regulation of coagulation. However, this natural anticoagulant system is frequently subjected to persistent disruption by the TME in patients with malignant tumors.25 The TME typically exhibits characteristics such as chronic inflammation, heightened protease activity, and metabolic dysregulation, factors which synergistically impair the expression and function of ATIII.26–28 For instance, cancer cells can induce oxidative stress-related apoptosis in head and neck squamous cell carcinoma, thereby disrupting hemostatic equilibrium. Tumor cell-secreted proteases may not only directly cleave ATIII but also alter its glycosylation modifications, diminishing its inhibitory capacity against thrombin and Factor Xa.29 Substantial clinical data support this perspective. An observational cohort study revealed significant associations between ATIII activity levels and cancer-related VTE, arterial thromboembolism risk, and all-cause mortality.30
Further investigations revealed that the TME can directly suppress SERPINC1 expression through upstream regulatory pathways. Tumor cell-secreted proteases can directly cleave ATIII or disrupt its glycosylation structure, reducing its binding efficiency to thrombin and Factor Xa.31 However, vascular endothelial damage induced by chronic inflammation within the TME inhibits the primary synthetic source of SERPINC1, further diminishing systemic ATIII levels.32 When SERPINC1 function declines and ATIII inhibition weakens, the thrombin-activated PARs signaling pathway undergoes sustained amplification. This leads to inflammation, endothelial dysfunction, and vascular remodeling, forming a vicious cycle that promotes cancer progression and thrombosis.33,34 Additionally, this mechanism explains why many patients with tumors experience multisystemic vascular lesions and cardiovascular events during disease progression, providing molecular-level support for combined anti-tumor and anti-thrombotic therapies. Recombinant human ATIII is currently approved for treating congenital ATIII deficiency and has demonstrated potential in reducing thrombotic risk in specific tumor populations, such as high-risk groups during pregnancy or postoperatively.35 Within the cancer treatment context, supplementing ATIII or activating SERPINC1 expression holds promise as a novel intervention pathway for hypercoagulable states. This strategy carries a lower bleeding risk and offers more precise targeting than traditional anticoagulants.
HMGCR is another high-frequency therapeutic target that plays a pivotal role in regulating lipid metabolism, inflammatory responses, and cardiovascular homeostasis.36 Its role in tumor biology has recently garnered increasing attention. Cancer cells typically exhibit abnormal lipid metabolic reprogramming to sustain rapid proliferation and survival.37–39 Previous studies have demonstrated that HMGCR is upregulated in hepatocellular carcinoma tissues, with its elevated expression associated with poor prognosis.40 Concurrently, alterations in cholesterol metabolism within pancreatic ductal adenocarcinoma (PDAC) cells significantly impact tumor progression and therapeutic resistance. HMGCR inhibition has been shown to suppress PDAC cell proliferation and survival rates.41 As HMGCR inhibitors, statins exert multifaceted effects beyond reducing hepatic cholesterol synthesis and circulating low-density lipoprotein cholesterol levels via upregulating low-density lipoprotein receptors, including anti-inflammatory, antioxidant, and endothelium-protective actions.42,43 Studies have shown that statins may alleviate anthracycline- or ICI-induced cardiac toxicity.44 Meanwhile, the use of statins may also be associated with a decrease in mortality rates for some cancer types.45 A study on prostate cancer cells revealed that statins, when combined with HMGCR gene silencing, significantly reduced cancer cell viability, inhibited clonogenic formation, and induced apoptosis.46 Concurrently, research linking the risk of breast cancer to lipid-related genes suggests a significant association between HMGCR and breast cancer risk.47 A clinical trial (NCT0442804) is systematically evaluating the efficacy of statins as adjunctive cardioprotective agents in cancer therapy. This study aims to clarify the dual benefits of statins in cancer treatment: reducing cardiovascular event risk while exerting synergistic regulatory effects on tumor biology.48 However, therapeutic responses to statins vary across tumor types, suggesting that their potential benefits require further validation. For instance, breast cancer cells exhibit therapeutic resistance to lipid metabolism remodeling. Although statins inhibit HMGCR, overcoming this resistance may necessitate combination with other drugs or targets.37
Beyond the abovementioned targets, high-frequency targets, such as KRAS, BTK, and ER, exhibit significant fusion characteristics in the mechanisms of cancer and cardiovascular comorbidity, primarily manifested in the complex interplay of immune, metabolic, and vascular pathways.49–51 These targets drive tumor initiation and progression and play pivotal roles in cardiovascular homeostasis. Their dysregulation usually leads to a mutually reinforcing relationship between tumor progression and cardiovascular injury.52–54
KRAS ranks among the most frequently mutated oncogenes in human cancers, with mutations occurring at high frequencies in pancreatic, colorectal, and non-small cell lung cancers, among others.55 The metabolic reprogramming driven by oncogenic KRAS mutations is pivotal for sustaining tumor cell viability and promoting proliferation.56 This metabolic reprogramming primarily manifests as enhanced glycolysis and increased lipid synthesis.57 Cancer cells prioritize aerobic glycolysis, predominantly generating energy through this pathway even under normoxic conditions. This provides the energy and biomolecular precursors required for rapid tumor cell proliferation.58 A potential link exists between KRAS activity and cardiovascular health. KRAS-driven metabolic alterations can induce oxidative stress and suppress endothelial nitric oxide (NO) synthase (eNOS) function, thereby impairing NO signaling. NO is a crucial regulator of vascular endothelial function, responsible for maintaining vascular tone, inhibiting platelet aggregation, and reducing inflammation.59 Impaired NO signaling further compromises vascular compliance and endothelial function, suggesting that KRAS activation correlates with heightened atherosclerotic risk.60 Consequently, strategies targeting KRAS remain crucial for tumor therapy and necessitate consideration of their potential cardiovascular implications.
BTK is a pivotal effector molecule within the BCR signaling pathway, playing a crucial role in B-cell development and lymphoma pathogenesis.61 Ibrutinib, as a first-generation BTK inhibitor, has demonstrated significant therapeutic efficacy in CLL and other B-cell malignancies.62 However, the clinical application of BTK inhibitors is associated with cardiovascular adverse events, such as atrial fibrillation and hypertension.63 This may relate to ibrutinib’s off-target effects. Research indicates that cardiovascular adverse events occurring during BTK inhibitor therapy are linked to non-targeted regulation of myocardial phosphatidylinositol 3-kinase (PI3K)-AKT and calcium ion signaling pathways.64 The PI3K-AKT signaling pathway serves as a pivotal regulator of cellular growth, proliferation, metabolism, and survival.65 Its dysregulated activation is prevalent across multiple cancers and is also implicated in cardiovascular disease pathophysiology.66 BTK activates the PI3K-AKT signaling pathway via multiple receptors, including B-cell activating factor receptor, BCR, and CD40, thereby influencing cellular survival and proliferation.67
ER exhibits a unique bidirectional role in tumor biology and cardiovascular regulation.49 Its activation is a key driver of proliferation in hormone-dependent tumors such as breast and ovarian cancers. In breast cancer, ER positivity represents the most common subtype, with endocrine therapy serving as the primary treatment modality.54 Upon binding to its ligand, ER recruits coactivators to regulate gene transcription and promote cell proliferation.68 ER signaling also mediates vascular protection by upregulating eNOS expression and suppressing inflammatory factors. Estrogens enhance NO production, thereby improving endothelial function and maintaining vascular health.59 This vasoprotective effect plays a crucial role in women’s cardiovascular health.51 However, ER-targeting endocrine therapies, such as aromatase inhibitors, suppress estrogen production, thereby undermining these vasoprotective mechanisms. This effect correlates with dyslipidemia and increased atherosclerosis risk in post-menopausal female patients. For instance, tamoxifen resistance mechanisms involving ligand-independent activation of ER and gene silencing may exacerbate cardiovascular risk.68
Collectively, the cross-integration of KRAS, BTK, and ER in tumor biology and cardiovascular regulation constitutes a shared pathophysiological framework where tumor progression and cardiovascular injury mutually reinforce each other. A deeper understanding of these mechanisms holds significant implications for future clinical trial design, with the goal of balancing anti-cancer efficacy with cardiovascular safety to develop more effective and safer therapeutic strategies.
Beyond conventional targets, we identified several emerging therapeutic categories that remain underrepresented among high-frequency targets. For instance, FXI inhibitors have demonstrated unique advantages in anticoagulant therapy, particularly in preventing thrombosis among patients with atrial fibrillation, though they may introduce novel cardiotoxicity concerns warranting further scrutiny and investigation.69 The application of poly ADP ribose polymerase (PARP) inhibitors in certain cancer treatments has also introduced novel cardiotoxicity risks, which may be particularly pronounced in specific patient cohorts.70 Furthermore, combination immunotherapy regimens are increasingly emerging as a significant therapeutic direction. While their cardiotoxic potential remains under-evaluated, their promise within cancer immunotherapy cannot be overlooked.71
In summary, this study presents a comprehensive overview of therapeutic targets, mechanistic pathways, and clinical research maturity in the field of cancer-related cardiovascular disease. By systematically analyzing randomized clinical trials, we identified coagulation and endothelial dysfunction as central axes linking tumor progression and cardiovascular complications, with Factor X, thrombin, and SERPINC1 emerging as pivotal targets. The dual role of several targets in both oncogenic and cardiovascular pathways underscores the necessity of integrated therapeutic strategies that balance anti-tumor efficacy with cardiovascular safety.
However, this study has some limitations. In addition to vascular-related genes and pathways, fibrosis represents a critical and often underappreciated mechanism underlying drug-induced cardiovascular toxicity. Accumulating evidence indicates that several anticancer agents, including anthracyclines such as doxorubicin, induce cardiomyopathy predominantly through pro-fibrotic remodeling rather than purely vascular injury. This process involves the activation of cardiac fibroblasts, excessive extracellular matrix deposition, and dysregulation of transforming growth factor-β (TGF-β)-related signaling pathways. Importantly, fibrosis-associated pathways may intersect with vascular and inflammatory mechanisms, jointly contributing to long-term cardiac dysfunction. In the future, integrating fibrosis-related targets into the current analytical framework could provide a more comprehensive understanding of drug-related cardiotoxicity and uncover additional therapeutic opportunities. The analysis relied on trial registration data, which may not fully reflect real-world treatment outcomes or unpublished negative results. Additionally, the heterogeneity of trial designs and endpoints could introduce interpretation bias. Despite these constraints, the findings provide valuable insights into current research gaps and therapeutic opportunities. Future studies should focus on validating the translational relevance of dual-pathway targets in real-world settings, exploring their mechanistic crosstalk in preclinical models, and designing next-generation clinical trials that integrate cardiotoxicity risk assessment into oncology drug development.
Specifically, first, an in-depth investigation into the crosstalk and underlying biological mechanisms of the selected targets is required, particularly those that simultaneously modulate cancer progression and cardiovascular disease pathways. Elucidating how these shared targets coordinate signaling across oncogenic, vascular, inflammatory, and fibrotic processes will be essential for mechanistic interpretation. Second, expanding validation using real-world evidence, such as electronic health records, pharmacovigilance databases, and large-scale clinical cohorts, would substantially enhance the robustness and generalizability of the findings beyond controlled experimental settings. Third, future studies should focus on advancing clinical translation by integrating and optimizing combination therapies that concurrently suppress tumor growth while protecting cardiovascular tissues. Such strategies may include co-administration of cardioprotective agents or pathway-guided therapeutic optimization. Finally, the analytical framework developed in this study holds potential for providing predictive insights into the cardiovascular risk profiles of currently used anticancer drugs. Further refinement of this approach may facilitate risk stratification, drug repurposing, and personalized therapeutic decision-making in cardio-oncology practice.
Conclusion
This study systematically organized the distribution of targets and research maturity in tumors combined with cardiovascular disease based on the Trialtrove database. It identified the dominant role of coagulation and endothelium-related targets in clinical research, highlighting their bridging function in tumor progression and cardiovascular complications. Targets such as SERPINC1 and HMGCR demonstrated potential for synergistic therapy, suggesting broader value in integrating mechanisms. However, limitations include the reliance on database information and impact of clinical trial heterogeneity on analytical precision. Research on some targets remains at an early stage, precluding broadly generalizable conclusions. Therefore, future studies should delve deeper into the cross-mechanistic effects of dual-pathway targets, expand real-world data validation, and advance the integration and optimization of anti-tumor and cardiovascular protection strategies.
Abbreviations
SERPINC1, Serpin Family C Member 1; ER, Estrogen Receptor; IKZF1, IKAROS Family Zinc Finger 1; CRBN, Cereblon; HMGCR, 3-Hydroxy-3-Methylglutaryl-CoA Reductase; BTK, Bruton Tyrosine Kinase; EDNRB, Endothelin Receptor Type B; ICIs, Immune Checkpoint Inhibitors; HER2, Human Epidermal Growth Factor Receptor 2; CVD, Cardiovascular Disease; BCR, B-cell Receptor; CP, Cancer Procoagulants; TME, Tumor Microenvironment; VTE, Venous Thromboembolism; eNOS, Endothelial Nitric Oxide Synthase; PI3K, Phosphatidylinositol 3-Kinase; ATIII, Antithrombin III; PDAC, Pancreatic Ductal Adenocarcinoma; DOACs, Direct Oral Anticoagulants; NO, Nitric Oxide; CAT, Cancer-Associated Thrombosis; PARs, Protease-Activated Receptors; CLL, Chronic Lymphocytic Leukemia; PARP, Poly ADP Ribose Polymerase.
Data Sharing Statement
Data will be made available upon request from Jianing Li.
Ethics Approval
This study does not involve human participants, laboratory animals, or histological research. It solely concerns the use of anonymized human imaging data obtained from publicly accessible databases, from which all personally identifiable information has been removed. Pursuant to national legislative guidelines, it is exempt from approval, specifically under Article 32, Items 1 and 2 of the Measures for the Ethical Review of Life Sciences and Medical Research in China, dated February 18, 2023: Research involving life sciences and the use of human information data or biological samples may be exempt from ethical review to alleviate unnecessary burdens on researchers and facilitate such studies. This applies to studies that do not cause harm to human subjects, do not involve sensitive personal information, or commercial interests. Examples include research utilizing publicly available data obtained lawfully, studies based on data generated from observation without interfering with public conduct, and research using anonymized data. Consequently, this study does not require approval from an Institutional Review Board.
Acknowledgments
We extend our gratitude to all participants and the consortia for their valuable contributions.
Author Contributions
All authors made significant contributions to the work reported, whether in study conception, design, and execution; acquisition of data; data analysis and interpretation; or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Innovative Research Program, Heilongjiang University of Chinese Medicine (2024yjscx106).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Wagle NS, Nogueira L, Devasia TP, et al. Cancer treatment and survivorship statistics, 2025. CA Cancer J Clin. 2025;75(4):308–14. doi:10.3322/caac.70011
2. Lee EM, Jiménez-Fonseca P, Galán-Moral R, et al. Toxicities and quality of life during cancer treatment in advanced solid tumors. Curr Oncol. 2023;30(10):9205–9216. doi:10.3390/curroncol30100665
3. Alshahrani AA, Kontopantelis E, Morgan C, Ravindrarajah R, Martin GP, Mamas MA. Cardiovascular diseases in patients with cancer: a comprehensive review of epidemiological trends, cardiac complications, and prognostic implications. Chin Med J. 2025;138(2):143–154. doi:10.1097/CM9.0000000000003419
4. Khorana AA, DeSancho MT, Liebman H, Rosovsky R, Connors JM, Zwicker J. Prediction and prevention of cancer-associated thromboembolism. Oncologist. 2021;26(1):e2–e7. doi:10.1002/onco.13569
5. Camilli M, Cipolla CM, Dent S, Minotti G, Cardinale DM. Anthracycline cardiotoxicity in adult cancer patients: JACC: cardioOncology state-of-the-art review. JACC CardioOncol. 2024;6(5):655–677. doi:10.1016/j.jaccao.2024.07.016
6. Li C, Dai H, Guo X, Zhou L, Jiang M. Comprehensive review of non-invasive-treatment-related cardiovascular toxicity in breast cancer. iScience. 2025;28(4):111759. doi:10.1016/j.isci.2025.111759
7. Mäki-Petäjä KM, McGeoch A, Yang LL, et al. Mechanisms underlying vascular endothelial growth factor receptor inhibition-induced hypertension: the HYPAZ trial. Hypertension. 2021;77(5):1591–1599. doi:10.1161/HYPERTENSIONAHA.120.16454
8. Ball S, Ghosh RK, Wongsaengsak S, et al. Cardiovascular toxicities of immune checkpoint inhibitors: JACC review topic of the week. J Am Coll Cardiol. 2019;74(13):1714–1727. doi:10.1016/j.jacc.2019.07.079
9. Gallucci G, Turazza FM, Inno A, et al. Atherosclerosis and the bidirectional relationship between cancer and cardiovascular disease: from bench to bedside-part 1. Int J Mol Sci. 2024;25(8):4232. doi:10.3390/ijms25084232
10. Odat RM, Alshwayyat S, Nguyen D, et al. Atherosclerosis as a cause of death in patients with cancer: a cohort study. Cardiooncology. 2025;11(1):52. doi:10.1186/s40959-025-00353-2
11. Lichtenberger JP 3rd, Reynolds DA, Keung J, Keung E, Carter BW. Metastasis to the heart: a radiologic approach to diagnosis with pathologic correlation. AJR Am J Roentgenol. 2016;207(4):764–772. doi:10.2214/AJR.16.16148
12. Rak J, Milsom C, May L, Klement P, Yu J. Tissue factor in cancer and angiogenesis: the molecular link between genetic tumor progression, tumor neovascularization, and cancer coagulopathy. Semin Thromb Hemost. 2006;32(1):54–70. doi:10.1055/s-2006-933341
13. Walter J, Handel LL, Brodhun M, et al. Expression of coagulation factors and their receptors in tumor tissue and coagulation factor upregulation in peripheral blood of patients with cerebral carcinoma metastases. J Cancer Res Clin Oncol. 2012;138(1):141–151. doi:10.1007/s00432-011-1078-x
14. Dogan M, Demirkazik A. Venous thromboembolism in patients with cancer and its relationship to the coagulation cascade and vascular endothelial growth factor. Support Cancer Ther. 2005;3(1):28–34. doi:10.3816/SCT.2005.n.022
15. Peng Q, Zhu J, Zhang Y, Jing Y. Blood hypercoagulability and thrombosis mechanisms in cancer patients-A brief review. Heliyon. 2024;10(19):e38831. doi:10.1016/j.heliyon.2024.e38831
16. Liu Y, Pelekanakis K, Woolkalis MJ. Thrombin and tumor necrosis factor alpha synergistically stimulate tissue factor expression in human endothelial cells: regulation through c-Fos and c-Jun. J Biol Chem. 2004;279(34):36142–36147. doi:10.1074/jbc.M405039200
17. Li S, Lu Z, Wu S, et al. The dynamic role of platelets in cancer progression and their therapeutic implications. Nat Rev Cancer. 2024;24(1):72–87. doi:10.1038/s41568-023-00639-6
18. Spronk HM, De Jong AM, Verheule S, et al. Hypercoagulability causes atrial fibrosis and promotes atrial fibrillation. Eur Heart J. 2017;38(1):38–50. doi:10.1093/eurheartj/ehw119
19. Mäder J, Rolling CC, Voigtländer M, et al. Effect of factor XI inhibition on tumor cell-induced coagulation activation. J Thromb Haemost. 2024;22(1):199–212. doi:10.1016/j.jtha.2023.09.015
20. Kobayashi M, Wada H, Fukui S, et al. A clot waveform analysis showing a hypercoagulable state in patients with malignant neoplasms. J Clin Med. 2021;10(22):5352. doi:10.3390/jcm10225352
21. Esmon CT. Targeting factor Xa and thrombin: impact on coagulation and beyond. Thromb Haemost. 2014;111(4):625–633. doi:10.1160/TH13-09-0730
22. Spronk HM, de Jong AM, Crijns HJ, Schotten U, Van Gelder IC, Ten Cate H. Pleiotropic effects of factor Xa and thrombin: what to expect from novel anticoagulants. Cardiovasc Res. 2014;101(3):344–351. doi:10.1093/cvr/cvt343
23. Sánchez-Navarro A, González-Soria I, Caldiño-Bohn R, Bobadilla NA. An integrative view of serpins in health and disease: the contribution of SerpinA3. Am J Physiol Cell Physiol. 2021;320(1):C106–C118. doi:10.1152/ajpcell.00366.2020
24. Bhatti UF, Dhillon NK, Mason R, et al. Antithrombin III levels in critically ill surgical patients: do they correlate with VTE? Trauma Surg Acute Care Open. 2023;8(1):e001009. doi:10.1136/tsaco-2022-001009
25. Boedtkjer E, Pedersen SF. The acidic tumor microenvironment as a driver of cancer. Annu Rev Physiol. 2020;82(1):103–126. doi:10.1146/annurev-physiol-021119-034627
26. Natu J, Nagaraju GP. Gemcitabine effects on tumor microenvironment of pancreatic ductal adenocarcinoma: special focus on resistance mechanisms and metronomic therapies. Cancer Lett. 2023;573:216382. doi:10.1016/j.canlet.2023.216382
27. Chen S, Xu Y, Zhuo W, Zhang L. The emerging role of lactate in tumor microenvironment and its clinical relevance. Cancer Lett. 2024;590:216837. doi:10.1016/j.canlet.2024.216837
28. Johnston CD, Bullman S. The tumour-associated microbiome. Nat Rev Gastroenterol Hepatol. 2022;19(6):347–348. doi:10.1038/s41575-022-00609-7
29. Gao L, Zhao X, Lang L, Shay C, Andrew Yeudall W, Teng Y. Autophagy blockade sensitizes human head and neck squamous cell carcinoma towards CYT997 through enhancing excessively high reactive oxygen species-induced apoptosis. J Mol Med (Berl). 2018;96(9):929–938. doi:10.1007/s00109-018-1670-5
30. Englisch C, Königsbrügge O, Nopp S, et al. Antithrombin activity and association with risk of thrombosis and mortality in patients with cancer. Int J Mol Sci. 2022;23(24):15770. doi:10.3390/ijms232415770
31. Natorska J, Corral J, de la Morena-Barrio ME, et al. Antithrombin deficiency is associated with prothrombotic plasma fibrin clot phenotype. Thromb Haemost. 2023;123(9):880–891. doi:10.1055/s-0043-1768712
32. Ikezoe T. Advances in the diagnosis and treatment of disseminated intravascular coagulation in haematological malignancies. Int J Hematol. 2021;113(1):34–44. doi:10.1007/s12185-020-02992-w
33. Falanga A, Marchetti M. Cancer-associated thrombosis: enhanced awareness and pathophysiologic complexity. J Thromb Haemost. 2023;21(6):1397–1408. doi:10.1016/j.jtha.2023.02.029
34. Falco L, Tessitore V, Ciccarelli G, et al. Antioxidant properties of oral antithrombotic therapies in atherosclerotic disease and atrial fibrillation. Antioxidants. 2023;12(6):1185. doi:10.3390/antiox12061185
35. Paidas MJ, Triche EW, James AH, et al. Recombinant human antithrombin in pregnant patients with hereditary antithrombin deficiency: integrated analysis of clinical data. Am J Perinatol. 2016;33(4):343–349. doi:10.1055/s-0035-1564423
36. Teng YN. The Potential therapeutic applications of natural products in the oxidative stress-related MVA pathway: focus on HMGCR. Antioxidants. 2025;14(8):1001. doi:10.3390/antiox14081001
37. Xiao Q, Xia M, Tang W, Zhao H, Chen Y, Zhong J. The lipid metabolism remodeling: a hurdle in breast cancer therapy. Cancer Lett. 2024;582:216512. doi:10.1016/j.canlet.2023.216512
38. Strickland M, Stoll EA. Metabolic reprogramming in glioma. Front Cell Dev Biol. 2017;5:43. doi:10.3389/fcell.2017.00043
39. Desbats MA, Giacomini I, Prayer-Galetti T, Montopoli M. Metabolic plasticity in chemotherapy resistance. Front Oncol. 2020;10:281. doi:10.3389/fonc.2020.00281
40. Zhang Z, Yang J, Liu R, et al. Inhibiting HMGCR represses stemness and metastasis of hepatocellular carcinoma via Hedgehog signaling. Genes Dis. 2024;11(5):101285. doi:10.1016/j.gendis.2024.101285
41. Li Y, Amrutkar M, Finstadsveen AV, Dalen KT, Verbeke CS, Gladhaug IP. Fatty acids abrogate the growth-suppressive effects induced by inhibition of cholesterol flux in pancreatic cancer cells. Cancer Cell Int. 2023;23(1):276. doi:10.1186/s12935-023-03138-8
42. Ma S, Sun W, Gao L, Liu S. Therapeutic targets of hypercholesterolemia: HMGCR and LDLR. Diabetes Metab Syndr Obes. 2019;12:1543–1553. doi:10.2147/DMSO.S219013
43. Grujić-Milanović J, Rajković J, Milanović S, et al. Natural substances vs. approved drugs in the treatment of main cardiovascular disorders-Is there a breakthrough? Antioxidants. 2023;12(12):2088. doi:10.3390/antiox12122088
44. Ibrahim AB, Zaki HF, Wadie W, Omran MM, Shouman SA. Simvastatin evokes an unpredicted antagonism for tamoxifen in MCF-7 breast cancer cells. Cancer Manag Res. 2019;11:10011–10028. doi:10.2147/CMAR.S218668
45. Kim GH, Kan SY, Kang H, et al. Ursolic acid suppresses cholesterol biosynthesis and exerts anti-cancer effects in hepatocellular carcinoma cells. Int J Mol Sci. 2019;20(19):4767. doi:10.3390/ijms20194767
46. Göbel A, Pählig S, Motz A, et al. Overcoming statin resistance in prostate cancer cells by targeting the 3-hydroxy-3-methylglutaryl-CoA-reductase. Biochem Biophys Res Commun. 2024;710:149841. doi:10.1016/j.bbrc.2024.149841
47. Zhang Z, Zhang D. Circulating lipids, lipid-lowering drug targets, and breast cancer risk: comprehensive evidence from Mendelian randomization and summary data-based Mendelian randomization. Cancer Causes Control. 2024;35(6):983–994. doi:10.1007/s10552-024-01857-5
48. Saint A, Van Obberghen-Schilling E. The role of the tumor matrix environment in progression of head and neck cancer. Curr Opin Oncol. 2021;33(3):168–174. doi:10.1097/CCO.0000000000000730
49. Perurena N, Situ L, Cichowski K. Combinatorial strategies to target RAS-driven cancers. Nat Rev Cancer. 2024;24(5):316–337. doi:10.1038/s41568-024-00679-6
50. Wu J, Liu C, Tsui ST, Liu D. Second-generation inhibitors of Bruton tyrosine kinase. J Hematol Oncol. 2016;9(1):80. doi:10.1186/s13045-016-0313-y
51. Quan T, Cockburn J, Dhesy-Thind S, et al. The significance of thyroid hormone receptors in breast cancer: a hypothesis-generating narrative review. Curr Oncol. 2024;31(5):2364–2375. doi:10.3390/curroncol31050176
52. Chen X, Ma Z, Yi Z, et al. The effects of metabolism on the immune microenvironment in colorectal cancer. Cell Death Discov. 2024;10(1):118. doi:10.1038/s41420-024-01865-z
53. Shukla N, Shah K, Rathore D, et al. Androgen receptor: structure, signaling, function and potential drug discovery biomarker in different breast cancer subtypes. Life Sci. 2024;348:122697. doi:10.1016/j.lfs.2024.122697
54. Araki K, Miyoshi Y. Mechanism of resistance to endocrine therapy in breast cancer: the important role of PI3K/Akt/mTOR in estrogen receptor-positive, HER2-negative breast cancer. Breast Cancer. 2018;25(4):392–401. doi:10.1007/s12282-017-0812-x
55. Kawada K, Toda K, Sakai Y. Targeting metabolic reprogramming in KRAS-driven cancers. Int J Clin Oncol. 2017;22(4):651–659. doi:10.1007/s10147-017-1156-4
56. Zhang L. Oncogenic KRAS drives metabolic vulnerabilities by directly regulating metabolic enzymes in cancer. Glob Med Genet. 2020;7(1):1–2. doi:10.1055/s-0040-1712456
57. Ren J, Ren B, Liu X, et al. Crosstalk between metabolic remodeling and epigenetic reprogramming: a new perspective on pancreatic cancer. Cancer Lett. 2024;587:216649. doi:10.1016/j.canlet.2024.216649
58. Park JH, Pyun WY, Park HW. Cancer metabolism: phenotype, signaling and therapeutic targets. Cells. 2020;9(10):2308. doi:10.3390/cells9102308
59. Wu P, Oren O, Gertz MA, Yang EH. Proteasome inhibitor-related cardiotoxicity: mechanisms, diagnosis, and management. Curr Oncol Rep. 2020;22(7):66. doi:10.1007/s11912-020-00931-w
60. Storey RF, Valgimigli M, Cuisset T, Capodanno D, Wijns W, Knuuti J. Intolerance to aspirin in patients undergoing percutaneous coronary intervention in the setting of chronic coronary syndromes: perspectives from the ESC 2019 Chronic Coronary Syndromes guidelines. Eur Heart J. 2020;41(3):483–484. doi:10.1093/eurheartj/ehz894
61. Hussain S, Mursal M, Verma G, Hasan SM, Khan MF. Targeting oncogenic kinases: insights on FDA approved tyrosine kinase inhibitors. Eur J Pharmacol. 2024;970:176484. doi:10.1016/j.ejphar.2024.176484
62. Falchi L, Baron JM, Orlikowski CA, Ferrajoli A. BCR signaling inhibitors: an overview of toxicities associated with ibrutinib and idelalisib in patients with chronic lymphocytic leukemia. Mediterr J Hematol Infect Dis. 2016;8(1):e2016011. doi:10.4084/mjhid.2016.011
63. Rihackova E, Rihacek M, Vyskocilova M, Valik D, Elbl L. Revisiting treatment-related cardiotoxicity in patients with malignant lymphoma-A review and prospects for the future. Front Cardiovasc Med. 2023;10:1243531. doi:10.3389/fcvm.2023.1243531
64. Jain N, Singh S, Laliotis G, et al. Targeting phosphatidylinositol 3 kinase-β and -δ for Bruton tyrosine kinase resistance in diffuse large B-cell lymphoma. Blood Adv. 2020;4(18):4382–4392. doi:10.1182/bloodadvances.2020001685
65. Li Y, Wang W, Xu D, et al. PIWIL2/PDK1 axis promotes the progression of cervical epithelial lesions via metabolic reprogramming to maintain tumor-initiating cell stemness. Adv Sci. 2024;11(48):e2410756. doi:10.1002/advs.202410756
66. Mazurakova A, Koklesova L, Csizmár SH, et al. Significance of flavonoids targeting PI3K/Akt/HIF-1α signaling pathway in therapy-resistant cancer cells-A potential contribution to the predictive, preventive, and personalized medicine. J Adv Res. 2024;55:103–118. doi:10.1016/j.jare.2023.02.015
67. Klener P. Advances in molecular biology and targeted therapy of mantle cell lymphoma. Int J Mol Sci. 2019;20(18):4417. doi:10.3390/ijms20184417
68. Abdel-Hafiz HA. Epigenetic mechanisms of tamoxifen resistance in luminal breast cancer. Diseases. 2017;5(3):16. doi:10.3390/diseases5030016
69. Raffo C, Di Leo G, Capodanno D. Factor XI inhibitors and atrial fibrillation: imminent breakthrough or false start? Eur Heart J Suppl. 2025;27(Suppl 3):iii46–iii53. doi:10.1093/eurheartjsupp/suaf015
70. Pacher P, Liaudet L, Bai P, et al. Activation of poly(ADP-ribose) polymerase contributes to development of doxorubicin-induced heart failure. J Pharmacol Exp Ther. 2002;300(3):862–867. doi:10.1124/jpet.300.3.862
71. Li J, Fu T, Wen Z, et al. Advances in the Use of Immune Checkpoint Inhibitors for Colorectal Cancer Treatment. Onco Targets Ther. 2025;18:1159–1168. doi:10.2147/OTT.S551204
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.