")
Back to Journals » Hepatic Medicine: Evidence and Research » Volume 12
Repurposing of N-Acetylcysteine for the Treatment of Dengue Virus-Induced Acute Liver Failure
Authors Tafere GG , Wondafrash DZ , Demoz FB
Received 28 May 2020
Accepted for publication 25 August 2020
Published 3 November 2020 Volume 2020:12 Pages 173—178
DOI https://doi.org/10.2147/HMER.S263840
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gerry Lake-Bakaar
Gebrehiwot Gebremedhin Tafere, Dawit Zewdu Wondafrash, Filmon Beyenne Demoz
Department of Pharmacology and Toxicology, School of Pharmacy, Mekelle University, Mekelle, Ethiopia
Correspondence: Gebrehiwot Gebremedhin Tafere P.O. Box: 1871, Mekelle, Ethiopia
Tel +251-908822323
Email [email protected]
Abstract: The prevalence of dengue infection-induced acute liver damage is increasing from time to time. Since it has no specific antiviral treatment in the world, people in endemic areas suffer more from dengue disorders. Thus, there is a need for searching options for the treatment of dengue-induced acute liver failure. N-acetylcysteine, which is used for the treatment of nasal congestion disorder and paracetamol overdose toxicity, could be used as a definitive therapy for dengue virus-induced acute liver disease. Therefore, this review discusses the therapeutic use of N-acetylcysteine for dengue-induced acute liver disease. Various case reports and case series showed that patients received NAC recovered from their clinical status. Additionally, a preclinical study showed that N-acetylcysteine has anti-dengue virus activity. Thus, N-acetylcysteine could be used as a definitive therapy in dengue virus-induced hepatitis. This might encourage researchers to further investigate the importance of N-acetylcysteine for dengue virus-induced hepatitis.
Keywords: N-acetylcysteine, dengue virus, acute liver failure
Introduction
Dengue is one of the common harmful mosquito-borne viral disease which belongs to the Flaviviridae family.1 There are different dengue virus serotypes causing dengue disorders, including, asymptomatic infection, dengue fever, undifferentiated fever, fatal and severe dengue hemorrhagic fever. Aedes aegypti mosquito (main urban vector) and Aedes albopictus female mosquitos are the known vector for transmission of dengue virus from an infected person to others by biting.2 A person exposed for a particular viral serotype develops immunity against that serotype in a secondary infection.1 For this reason, infants who are born with dengue virus-infected mothers develop secondary immunity after passing a severe form of dengue disease during the primary infection.3
The world population, particularly those who live in endemic areas are 40% at risk of developing dengue infection. It is estimated that the world encounters 390 million dengue infections, among which 96 million are symptomatic, and 20,000 deaths occur each year in 62.8% of the world countries.4 The global burden of the disease doubles three times in its prevalence within five decades. This is due to the occurrence of the disease in previously sterilized countries from the dengue virus.5 These countries are found in the Americas, the Eastern Mediterranean, South-East Asia, Western Pacific, and Africa.1 Moreover, the virus was identified in Ethiopia in 2013, in the Dire Dawa city, which was noted as a frequent dengue outbreak since then.6 Dengue is also expanding its domain in Ethiopia and becomes a threat in Somalia region for a few years back.7
The main clinical features of dengue virus-induced hepatitis are acute liver failure and fulminant.8 Among the other clinical features of hepatic involvement, patients may experience vomiting (49–58%), nausea, anorexia, and abdominal pain (18–63%),9 raised transaminase levels, clinical jaundice (1.7–17%). Hyperbilirubinemia has been detected to be as high as 48%, and death was highly associated with dengue virus-induced acute liver failure (ALF).10 Additionally, the virus can cause Guillian-Barre syndrome, myocarditis, encephalitis, and hemolytic uremic syndrome since it affects various tissues.11
N-acetylcysteine (NAC) is produced after acetylation reaction of the L-cysteine amino acid. It acts both as a source of reduced glutathione and directly scavenging free radicals in the body.12 Thus, NAC preserves the different enzymes such as catalase, mitochondrial superoxide dismutase, and the different forms of glutathione peroxidases used in reduction and oxidation reactions to be intact thereby reducing the occurrence of oxidative. Although NAC is orally absorbable drug, it will reach the systemic circulation after it passed extensive pre-systemic metabolism.13 Besides, NAC could also be administered through the intravenous route of administration smoothly. Therefore, due to its easy way of administration and low toxicity, NAC is currently the favorite compound for the treatment of hepatotoxicity in man regardless of the cause.14 In general, these effects show NAC may be a useful agent to preserve liver function in patients with biliary obstruction, which was the path for glutathione production.15
Life Cycle of Dengue Virus
The mature dengue virus has three different structural and functional proteins. The proteins are the capsid protein C which forms the envelop, the membrane protein M which makes the virion to be intact in structure and the nucleotide envelope E which covers the ribonucleic acid (RNA) genome.16
The dengue virus targets the following cells in the human body during its natural course of infection. These are cells of the mononuclear phagocyte lineage macrophages, monocytes, and dendritic cells, including the skin-resident langerhans cells. Over the last years, several candidate receptors and/or attachment factors have been identified, which suggests that the dengue virus (DENV) is capable of utilizing multiple molecules to enter the cell. Dengue virus and flaviviruses use clathrin-mediated endocytosis for cell entry.17,18 This approach is based on a single particle lay down and rolls in the surface of the cell. This can be supported after it has been revealed that DENV-2 strain S1 particles land on the cell surface and travels in a diffusive manner toward a pre-existing clathrin-coated pit.19 This suggests that DENV particles move along the cell surface by rolling over different receptors, or migrate as virus–receptor complexes, which enables the virus to use different possible receptors for entrance.1
After the virus enters into the cell, it will have free RNA uncoated of a nucleo-capsid, which enables it to be translated as a single polyprotein.20 Then, the signal- and stop-transfer sequences of the polyprotein direct its back-and-forth translocation across the endoplasmic reticulum membrane. The polyprotein will be processed co- and post-translationally by cellular and virus-derived proteases into three structural proteins (C, M, and E) and seven nonstructural (NS) proteins (NS1-NS7). The E protein is glycosylated at amino acid residue Asn67 and Asn153 to assure proper folding of the protein.1
Since dengue-infected mosquito and mammalian cells secrete large numbers (up to 30%) of prM-containing particles, dengue virus maturation appears to be inefficient. Numerous studies have shown that fully immature particles cannot infect cells remarkably; however, this time the virus is resistant for prM antibodies developed by the body and becomes mature to infect other cells.21
Pathogenic Mechanism of Dengue Virus-Induced Acute Liver Failure
The exact pathogenesis of dengue virus-induced acute liver damage is complex and poorly understood.22 Dengue virus causes a disorder of the liver ranging from direct viral injury, hypoxic, ischemic to dysregulated immune response which ultimately results in apoptosis and necrosis.23 The dengue viremia mainly affects the liver with viral toxicity or immunological injury. During acute dengue virus infection, the level of antioxidants such as glutathione peroxidase and glutathione reductase reduced, whereas liver enzymes, including, aspartate transferase (AST) and alanine transferase (ALT) are elevated suggesting of oxidative stress induced by dengue virus.24 Additionally, as investigated in the mouse model, dengue-induced acute liver failure could occur due to the release of inflammatory cytokines, particularly interleukin-22 (IL-22) and interleukin-17 (IL-17).25 Tumor necrosis factor (TNF) alpha, interleukin −2 (IL-2), interleukin-6 (IL-6) and interleukin-8 (IL-8) levels are also elevated in early dengue virus infection whereas interleukin-5 (IL-5) and interleukin-10 (IL-10) were increased subsequently.26
Various histologic changes were observed in dengue-induced liver failure, including, fatty change, hepatocyte necrosis, hyperplasia, and destruction of Kupffer cells, Councilman bodies and mononuclear cell infiltrates at the portal tract.23 According to a recent report, acetaminophen overdose can play a crucial role in causing acute liver failure in dengue-infected patients.27
Current Management of Dengue Virus-Induced Hepatitis
Though there are no specific treatments for dengue-induced acute hepatic failure, different management modalities have been used to reduce its fatality rate. Dengvaxia is the first dengue vaccine, which has a significant effect in patients with the age group of 19–45 years.28 Paracetamol can be taken to control the symptoms of muscle aches and pains, and fever, whereas non-steroidal anti-inflammatory drugs, such as ibuprofen and aspirin should be avoided. This is because anti-inflammatory drugs are associated with severe bleeding. The most common treatment is maintenance of the patient’s body fluid volume particularly for patients with critical infection.29 Artificial liver support has also been recently suggested for the treatment of dengue patients with liver failure. This is used to support the liver in the elimination of waste materials from the body and acts as a liver while its transplantation.30
Many drugs (chloroquine, balapiravir, celgosivir, and lovastatin) have been tried to be repurposed for severe dengue infection, which primarily affects the liver a major part of its replication. But, they are not effective in treating the infection.31 Since the treatment for dengue virus-induced acute liver failure is non-specific, and many of the more experienced clinicians described the guidelines as only making sense in the light of clinical experience.32 Currently, the concurrent needs of an effective dengue vaccine and an urgent need for an effective antiviral agent against dengue is continuing.33 Therefore, this review aims to discuss the therapeutic use of NAC for dengue virus-associated acute liver failure as definitive therapy.
Use of N-Acetylcysteine for the Treatment of Dengue Virus-Induced Acute Liver Failure
N-acetylcysteine was used clinically for around 30 years as a mucolytic agent. Nowadays, various studies showed that NAC has an activity against dengue virus-induced acute liver failure as indicated in the table below (Table 1). Various online sources like Google Scholar, PubMed/MEDLINE, ResearchGate, and Science Direct were used to search the articles used for this study.
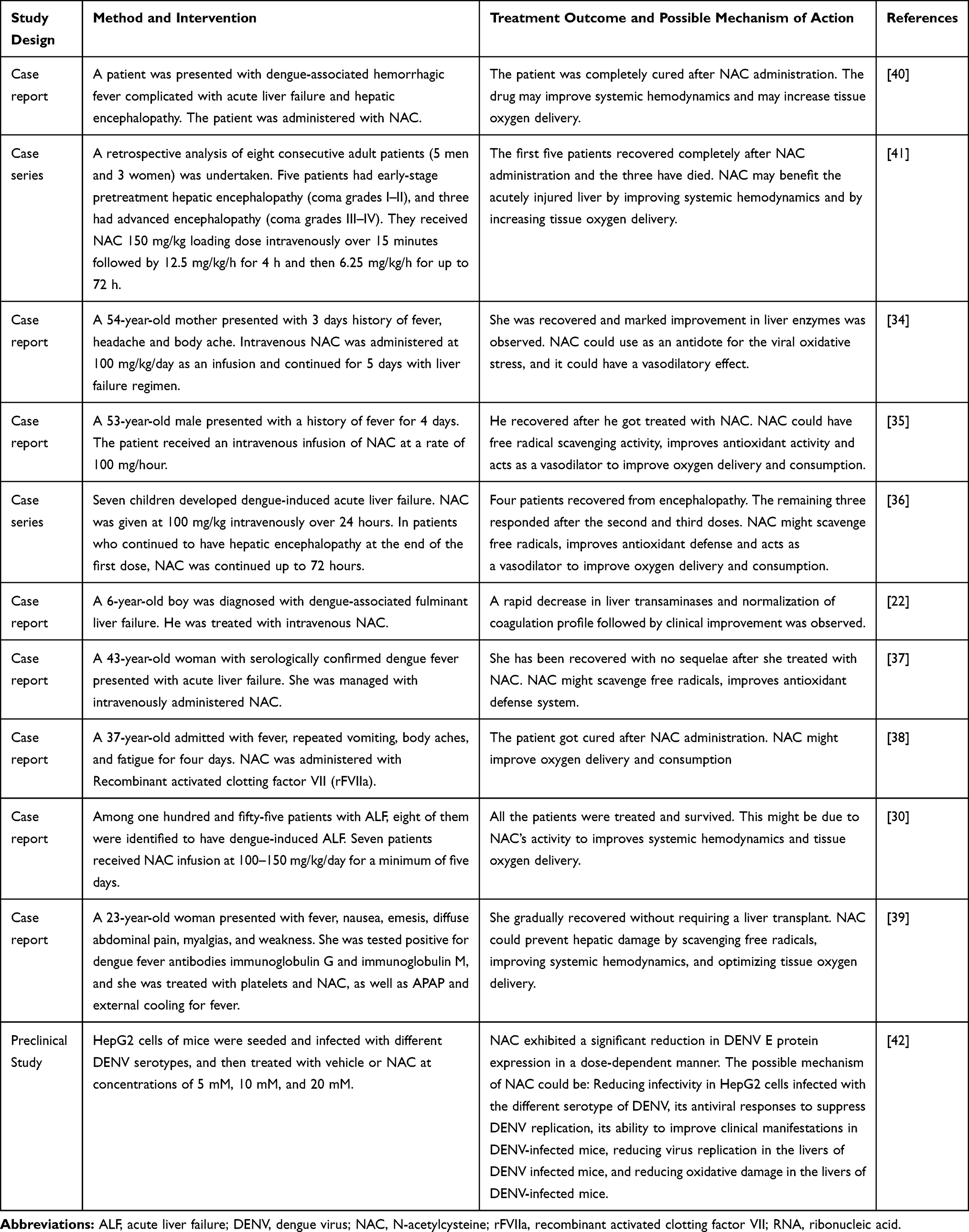 |
Table 1 Clinical and Preclinical Studies of N-Acetylcysteine in Dengue Virus-Induced Hepatitis |
Potential Benefit of N-Acetylcysteine in Dengue Virus-Induced Acute Liver Failure
Most of the patients receiving NAC during their clinical status showed a positive response to the drug which could encourage the use of NAC for dengue-induced acute liver failure. As indicated in the table, the mechanism of action of NAC in patients who recovered from dengue-induced ALF could be associated with its ability to increase antioxidant defense system, its free radical scavenging activity, and its vasodilatory activity that increases blood flow to the liver.40,41
As reported by Chandrasena et al (2019), the antioxidant enzymes such as glutathione peroxidase and glutathione reductase have been reduced during acute dengue infection. Thus, the antioxidant activity of NAC could be due to increasing plasma antioxidant levels such as glutathione peroxidase and glutathione reductase which results in reducing oxidative stress.24
A mechanistic study was done on mice to assure how NAC completely cures ALF with no sequelae. NAC showed antiviral activity by reducing infectivity in HepG2 cells infected DENV, suppressing DENV replication, and reducing oxidative damage. NAC could also reduce the infectivity of dengue virus at its entry, replication, post translation, RNA synthesis and exocytosis in a dose-dependent manner. Additionally, the drug up-regulates the expressions of pattern recognition receptors including, retinoic acid-inducible gene I and melanoma differentiation-associated gene 5 in DENV-infected mice.42
Conclusion and Future Perspective
Generally, dengue virus infection and its associated complications are now becoming a global burden; and it does not have a specific treatment modality. To prevent dengue virus-associated complications and mortality, searching for promising therapeutic options is important. N-acetylcysteine has crucial importance in the treatment of dengue-induced acute liver disease possibly by reducing oxidative stress, by its direct antiviral activity and by increasing blood flow to the liver. It has the potential to be used as a definitive therapy for dengue-associated liver failure.
Various case reports and series; and one animal study showed that NAC has an important role in the treatment of dengue-induced acute liver failure. Large randomized clinical trials and several animal studies are required to confirm the efficacy of NAC in dengue virus-induced acute liver failure. Additionally, further investigations are in need to decide the mechanism of action of NAC in dengue-induced acute liver disease.
Abbreviations
ALT, Alanine Transferase; AST, Aspartate Transferase; DENV, Dengue Virus; IL, Interleukin; NAC, N-acetylcysteine; TNF, Tumor Necrosis Factor; WHO, World Health Organization.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rodenhuis-Zybert IA, Wilschut J, Smit JM. Dengue virus life cycle: viral and host factors modulating infectivity. Cell Mol Life Sci. 2010;67(16):2773–2786.
2. Rege S, Swaminathan S. Management of Dengue. Association of physicians of India. 2017.
3. Rothman AL. Immunity to dengue virus: a tale of original antigenic sin and tropical cytokine storms. Nat Rev Microbiol. 2011;11(8):532–543.
4. Ferreira GL. Global dengue epidemiology trends. Rev Inst Med Trop Sao Paulo. 2012;54:5–6. doi:10.1590/S0036-46652012000700003
5. WHO. Global Strategy for Dengue Prevention and Control 2012–2020; 2020.
6. Degife LH, Worku Y, Belay D, Bekele A, Hailemariam Z. Factors associated with dengue fever outbreak in Dire Dawa administration city, Ethiopia-case control study. BMC Public Health. 2019;19(1):650. doi:10.1186/s12889-019-7015-7
7. Ahmed YM, Salah AA. Epidemiology of dengue fever in Ethiopian Somali region: retrospective health facility based study. Cent Afr J Public Health. 2016;2:51–56.
8. Westaway E, Brinton M, Gaidamovich SY, et al. Flaviviridae. Intervirology. 1985;24(4):183–192. doi:10.1159/000149642
9. Parkash O, Almas A, Jafri SW, Hamid S, Akhtar J, Alishah H. Severity of acute hepatitis and its outcome in patients with dengue fever in a tertiary care hospital Karachi, Pakistan (South Asia). BMC Gastroenterol. 2010;10(1):43. doi:10.1186/1471-230X-10-43
10. Souza L, Coelho J, Silva E, et al. Acute hepatitis due to dengue virus in a chronic hepatitis patient. Braz J Infect Dis. 2008;12(5):456–459. doi:10.1590/S1413-86702008000500021
11. Mourão MPG, Lacerda M, Bastos M, Albuquerque B, Alecrim WD. Dengue hemorrhagic fever and acute hepatitis: a case report. Braz J Infect Dis. 2004;8(6):461–464. doi:10.1590/S1413-86702004000600011
12. Zafarullah M, Li W, Sylvester J, Ahmad M. Molecular mechanisms of N-acetylcysteine actions. Cell Mol Life Sci. 2003;60(1):6–20. doi:10.1007/s000180300001
13. D’Amico F, Vitale A, Piovan D, et al. Use of N-acetylcysteine during liver procurement: a prospective randomized controlled study. Liver Transplant. 2013;19(2):135–144. doi:10.1002/lt.23527
14. Gray A, Dear J, Thanacoody R, et al. Reducing adverse effects from intravenous n-acetylecysteine treatment of paracetomol poisoning: principal results of the Scottish and Newcastle antemetic ore_treatment for paracetamol poisoning (snap) randomised controlled trial. J Emerg Med. 2013;30(10):867–868. doi:10.1136/emermed-2013-203113.5
15. Patel T, Tarun T, Hudhud D, Krvavac A. Novel use of N-acetylcysteine in management of tyrosine kinase inhibitor induced acute liver injury. Cureus. 2019;11(11).
16. Ma L, Jones CT, Groesch TD, Kuhn RJ, Post CB. Solution structure of dengue virus capsid protein reveals another fold. Proc Natl Acad Sci. 2004;101(10):3414–3419. doi:10.1073/pnas.0305892101
17. Acosta EG, Castilla V, Damonte EB. Functional entry of dengue virus into Aedes albopictus mosquito cells is dependent on clathrin-mediated endocytosis. J Gen Virol. 2008;89(2):474–484. doi:10.1099/vir.0.83357-0
18. Chu J, Ng M. Infectious entry of West Nile virus occurs through a clathrin-mediated endocytic pathway. J Virol. 2004;78(19):10543–10555. doi:10.1128/JVI.78.19.10543-10555.2004
19. Van Der Schaar HM, Rust MJ, Chen C, et al. Dissecting the cell entry pathway of dengue virus by single-particle tracking in living cells. PLoS Pathog. 2008;4(12). doi:10.1371/journal.ppat.1000244.
20. Clyde K, Kyle JL, Harris E. Recent advances in deciphering viral and host determinants of dengue virus replication and pathogenesis. J Virol. 2006;80(23):11418–11431. doi:10.1128/JVI.01257-06
21. Rodenhuis-Zybert IA, van der Schaar HM, da Silva Voorham JM, et al. Immature dengue virus: a veiled pathogen? PLoS Pathog. 2010;6(1). doi:10.1371/journal.ppat.1000718.
22. Lim G, Lee JH. N-acetylcysteine in children with dengue-associated liver failure: a case report. J Trop Pediatr. 2012;58(5):409–413. doi:10.1093/tropej/fmr108
23. Samanta J, Sharma V. Dengue and its effects on liver. World J Clin Cases. 2015;3(2):125. doi:10.12998/wjcc.v3.i2.125
24. Chandrasena L, De Silva A, De Mel C, et al. Glutathione enzymes and liver injury in acute dengue viral infection. J Biosci Med. 2019;7(10):61.
25. Guabiraba R, Besnard AG, Marques RE, et al. IL‐22 modulates IL‐17A production and controls inflammation and tissue damage in experimental dengue infection. Eur J Immunol. 2013;43(6):1529–1544. doi:10.1002/eji.201243229
26. Chia PY, Thein T-L, Ong SWX, Lye DC, Leo YS. Severe dengue and liver involvement: an overview and review of the literature. Expert Rev Anti Infect Ther. 2020;18(3):181–189. doi:10.1080/14787210.2020.1720652
27. WHO. Global Strategy for Dengue Prevention and Control 2012–2020; 2012.
28. WHO. Immunization, Vaccines and Biologicals. WHO; 2019.
29. WHO. Dengue and Severe Dengue; 2019.
30. Tan -S-S, Bujang MA. The clinical features and outcomes of acute liver failure associated with dengue infection in adults: a case series. Braz J Infect Dis. 2013;17(2):164–169. doi:10.1016/j.bjid.2012.09.007
31. Lee TH, Lee LK, Lye DC, Leo YS. Current management of severe dengue infection. Expert Rev Anti Infect Ther. 2017;15(1):67–78. doi:10.1080/14787210.2017.1248405
32. Wharton-Smith A, Green J, Loh EC, et al. Using clinical practice guidelines to manage dengue: a qualitative study in a Malaysian hospital. BMC Infect Dis. 2019;19(1):1–10. doi:10.1186/s12879-019-3680-5
33. Laughlin CA, Morens DM, Cassetti MC, et al. Dengue research opportunities in the Americas. J Infect Dis. 2012;206(7):1121–1127. doi:10.1093/infdis/jis351
34. Habaragamuwa BWP, Dissanayaka P. N-acetylcystein in dengue associated severe hepatitis: peer-reviewed, official publication of Indian Society of Critical Care Medicine. Indian J Crit Care Med. 2014;18(3):181. doi:10.4103/0972-5229.128712
35. Dalugama C, Gawarammana IB. Dengue hemorrhagic fever complicated with acute liver failure: a case report. J Med Case Rep. 2017;11(1):341. doi:10.1186/s13256-017-1510-1
36. Senanayake M, Jayamanne M, Kankananarachchi I. N-acetylcysteine in children with acute liver failure complicating dengue viral infection. Ceylon Med J. 2013;58(2):80. doi:10.4038/cmj.v58i2.5684
37. Dalugama C, Gawarammana IB. Lessons learnt from managing a case of dengue hemorrhagic fever complicated with acute liver failure and acute kidney injury: a case report. J Med Case Rep. 2018;12(1):215. doi:10.1186/s13256-018-1766-0
38. Manoj EM, Ranasinghe G, Ragunathan M. Successful use of N-acetyl cysteine and activated recombinant factor VII in fulminant hepatic failure and massive bleeding secondary to dengue hemorrhagic fever. J Emerg Trauma Shock. 2014;7(4):313. doi:10.4103/0974-2700.142771
39. Lewis J, Mitra A, Chang M. Acute liver failure in a patient with dengue shock syndrome. ACG Case Rep J. 2020;7(4):e00371. doi:10.14309/crj.0000000000000371
40. Abeysekera R, Illangasekera U, Jayalath T, Sandeepana A, Kularatne S. Successful use of intravenous N-acetylcysteine in dengue haemorrhagic fever with acute liver failure. Ceylon Med J. 2013;57(4):166. doi:10.4038/cmj.v57i4.5085
41. Kumarasena RS, Senanayake SM, Sivaraman K, et al. Intravenous N-acetylcysteine in dengue-associated acute liver failure. Hepatol Int. 2010;4(2):533–534. doi:10.1007/s12072-010-9176-4
42. Sreekanth GP, Panaampon J, Suttitheptumrong A, et al. Drug repurposing of N-acetyl cysteine as antiviral against dengue virus infection. Antiviral Res. 2019;166:42–55. doi:10.1016/j.antiviral.2019.03.011
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.