")
Back to Journals » Clinical Ophthalmology » Volume 16
Reproxalap Improves Signs and Symptoms of Allergic Conjunctivitis in an Allergen Chamber: A Real-World Model of Allergen Exposure
Authors Clark D, Karpecki P , Salapatek AM, Sheppard JD, Brady TC
Received 2 November 2021
Accepted for publication 14 December 2021
Published 4 January 2022 Volume 2022:16 Pages 15—23
DOI https://doi.org/10.2147/OPTH.S345324
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
David Clark,1 Paul Karpecki,2 Anne Marie Salapatek,3 John D Sheppard,4 Todd C Brady1
1Aldeyra Therapeutics, Lexington, MA, USA; 2Kentucky Eye Institute, Lexington, KY, USA; 3Cliantha Research, Mississauga, ON, Canada; 4Virginia Eye Consultants, Norfolk, VA, USA
Correspondence: Todd C Brady
Aldeyra Therapeutics, Inc., 131 Hartwell Avenue, Suite 320, Lexington, MA, 02421, USA
Tel +1 781 761-4904
Email [email protected]
Purpose: To assess the prophylactic and treatment activity of reproxalap, a novel reactive aldehyde species inhibitor, in a real-world model of allergen exposure.
Methods: In a randomized, double-masked, vehicle-controlled, crossover Phase 2 trial, 70 adult patients with ≥ 2 years of moderate to severe allergic conjunctivitis history, a positive skin test to ragweed pollen, and allergen chamber-induced ocular itching and redness scores of ≥ 2.5 and ≥ 2 (both scales range from 0 to 4), respectively, were randomized 1:1:1 to one of three sequences: 0.25% reproxalap, 0.5% reproxalap, and placebo; 0.5% reproxalap, placebo, and 0.25% reproxalap; or placebo, 0.25% reproxalap, and 0.5% reproxalap. Symptoms and conjunctival redness were assessed over 3.5 hours in an allergen chamber of aerosolized ragweed pollen (3500 grains/m3). Test article was administered bilaterally just before chamber entry and at 90 minutes after chamber entry.
Results: Reproxalap was safe and well tolerated; 66 of 70 enrolled patients completed all visits. Relative to vehicle, both concentrations of reproxalap demonstrated statistically significant and clinically relevant improvements in ocular itching, tearing, and redness over the duration of exposure in the chamber (P < 0.001 for all assessments). Prophylactic and treatment activity of drug were demonstrated.
Conclusion: In an allergen chamber, reproxalap, a novel reactive aldehyde species inhibitor, was statistically superior to vehicle across the typical symptoms and signs of allergic conjunctivitis. These data are among the first rigorous clinical results demonstrating drug improvement in allergic conjunctivitis in an allergen chamber, a real-world model of allergen exposure.
Keywords: RASP inhibitor, allergic conjunctivitis, allergen chamber, reproxalap, inflammation
Plain Language Summary
Allergic conjunctivitis is widespread, negatively impacts patients’ quality of life, and is inadequately controlled by existing therapeutics. Reproxalap is a novel, topical therapeutic that has shown efficacy in mitigating signs and symptoms of multiple inflammatory eye diseases. This trial examined the activity of reproxalap in patients with allergic conjunctivitis by using controlled exposure to allergens in an allergen chamber over 3.5 hours. Allergen chamber testing offers precise control over the amount of allergen as well as continuous airborne exposure, allowing researchers to more closely approximate real-world exposure conditions than methods used in prior allergen exposure studies. Two concentrations of reproxalap were tested, 0.5% and 0.25%. Both concentrations of reproxalap were found to be well-tolerated and exhibited significant improvements over vehicle in reducing the signs and symptoms of allergic conjunctivitis, including ocular itching, redness, and tearing. These improvements were observed generally across all time points studied, including after chamber exit, suggesting that reproxalap is active before, during, and after allergen exposure. The activity of reproxalap established in this trial could potentially address real-world clinical challenges faced by patients with allergic conjunctivitis.
Introduction
Allergic conjunctivitis affects more than 20% of the US population1 and up to 60% of patients require medication other than topical antihistamines,2 but a new mechanistic pharmacologic treatment approach has not been available for decades. Given that the symptoms and signs of allergic conjunctivitis, including ocular itching and redness, are persistently disturbing to patients and negatively affect quality of life,3 the development of new pharmacotherapeutic modalities is warranted.
Reproxalap is a novel, topically administered reactive aldehyde species (RASP) inhibitor that has demonstrated clinical activity in noninfectious anterior uveitis,4 dry eye disease,5,6 and allergic conjunctivitis.7 RASP potentiates inflammation via covalent protein signaling by increasing the activity of a variety of inflammatory mediators, including nuclear factor kappa B and inflammasomes.8–10 Posthistaminic factors, including cellular infiltrate, cytokines, and other RASP-mediated inflammatory mediators, perpetuate the signs and symptoms of allergic conjunctivitis after allergen-induced histamine levels have declined.11 Recent clinical trials in allergic conjunctivitis have typically employed conjunctival allergen challenge,12 which consists of drug administration followed by topical administration of solubilized pollen and subsequent assessment of ocular signs and symptoms, generally for 10 minutes or less.13 The clinical relevance of conjunctival challenge is limited by the finding that the signs and symptoms of allergic conjunctivitis diminish rapidly, thus hampering the ability to distinguish treatment efficacy in the later posthistaminic time points.13 In addition, topical ocular exposure to a concentrated pollen solution is unlikely to occur outside clinical trials, whereas clinical protocols that incorporate prolonged and ambient exposure to an allergen more accurately reflect real-world experience. Field trials of drugs during allergy season have been performed,14 but uncontrolled exposure to allergens in these trials limits interpretation of the data.
To simulate real-world allergen exposure in a controlled environment, the prophylactic and treatment activity of reproxalap were tested for 3.5 hours in an allergen chamber: an enclosed room with ambient exposure to regulated levels of aerosolized pollen, which has been used previously to assess drug activity in allergic conjunctivitis patients.15 Responder-based analyses were used to confirm the clinical relevance of the findings.
Methods
Trial Design
Patients with seasonal allergic conjunctivitis were enrolled in a single-center, three-way crossover, placebo-controlled, randomized sequence, double-masked phase 2 trial (ClinicalTrials.gov: NCT03709121) that began on September 9, 2018 and concluded on December 20, 2018. The trial was designed to evaluate the activity and clinical utility of two concentrations (0.25% and 0.5%) of topical ocular reproxalap relative to vehicle during exposure to ambient aerosolized ragweed pollen in an allergen chamber for 3.5 hours, which approximates the average maximum duration of allergens that patients are generally willing to withstand. As described previously,16–18 the allergen chamber consisted of an enclosed room into which commercially obtained air-dried, nondefatted short ragweed pollen (Ambrosia artemesiifolia; Greer Laboratories, Lenoir, NC, USA) was introduced to HEPA-filtered fresh air and maintained at 3500 ± 500 grains/m3 with rigorous temperature and humidity controls. Forced visual tasking was implemented to maintain largely uninterrupted exposure of allergen to the ocular surface. Up to 20 patients were tested in the chamber simultaneously, with no more than 3 technicians present at any one time.
The trial consisted of five visits: a medical screening visit that included ragweed pollen skin testing; an allergen chamber exposure qualification visit to elicit conjunctival redness and itching; and three treatment visits during which patients were treated topically with one drop of test article in each eye approximately 1 minute prior to chamber entry and again 90 minutes after chamber entry, when peak symptoms are typically apparent. The second dose was designed to recapitulate a typical patient-driven scenario during prolonged symptomatic antigen exposure. All allergen chamber visits were separated by 2 weeks ± 3 days. Patients were randomly assigned 1:1:1 to one of three sequences for the test article visits: 0.25% reproxalap, 0.5% reproxalap, and placebo (sequence A); 0.5% reproxalap, placebo, and 0.25% reproxalap (sequence B); or placebo, 0.25% reproxalap, and 0.5% reproxalap (sequence C). Patients, investigators, and the sponsor were masked to treatment assignment throughout the trial.
Patient Selection
Adult patients aged ≥18 years with ≥2 years of moderate to severe allergic conjunctivitis history, a positive skin test (≥3 mm) to ragweed pollen, and allergen chamber-induced ocular itching and redness scores of ≥2.5 and ≥2 (both scales range from 0 to 4), respectively, were eligible. Patients were excluded for any clinically significant slit-lamp findings or a history of inflammatory or infectious diseases that may have interfered with the conduct of the trial. Other exclusions included the use of antihistamines within 7 days prior to screening and the use of corticosteroid or immunotherapeutic agents within 14 days prior to screening. Patients were excluded or deferred to a later visit if ocular itching and redness scores were >0.5 or >1, respectively, in either eye before any allergen chamber visit. Subjects with moderate or severe asthma were excluded.
Study Assessments and Endpoints
Patient-reported ocular itching and tearing scores were recorded by patients using an electronic tablet at approximately 2, 7, 12, 17, 22, 32, 42, 52, 72, 92, 97, 102, 107, 112, 122, 132, 142, 152, 172, 192, and 212 minutes after chamber entry on a scale ranging from 0 (no itching) to 4 (severe), allowing half-unit increments, for itching and from 0 (no tearing) to 3 (severe) for tearing.12 Trained technicians visually assessed conjunctival redness without a slit lamp using a lit magnifier, based on a validated descriptive and photographic redness scale from 0 (none) – 4 (extremely severe) with 0.5 increments,19 for each eye on a similar schedule offset by at least 3 minutes. Similar assessments of ocular itching, tearing, and redness were performed at approximately 2, 7, 12, 17, 22, 32, 42, and 62 minutes after chamber exit. Safety assessments included visual acuity, slit-lamp biomicroscopy, undilated fundoscopy, intraocular pressure, and adverse events (AEs). Patients were monitored for symptoms and signs of asthma or other conditions that may have affected study results or conduct.
Statistical Analysis
A sample size of 60 completed patients was expected to detect a 0.5-unit treatment difference from placebo in ocular itching, with an estimated standard deviation of 1.35 units and a power of 80%. Given that reproxalap had not been previously tested in an allergen chamber, no primary or secondary endpoints were designated. Mixed effect models for repeated measures (MMRM) were used to assess changes from baseline in ocular itching and tearing scores over all time points in aggregate, with sequence, visit, treatment group, time after chamber entry, and the interaction of treatment group and time as factors. Baseline was defined as the average of scores just prior to chamber entry. A similar MMRM analysis was used to assess conjunctival redness score averaged across both eyes. Time to ocular itching and redness scores of ≥2 in the allergen chamber was evaluated using the Kaplan–Meier method and log-rank comparisons. Safety assessments were evaluated using summary statistics.
Results
Patient Disposition and Characteristics
Patient disposition is diagrammed in Figure 1. A total of 423 patients with allergic conjunctivitis were screened, and 70 were randomized and treated between October 2, 2018, and April 9, 2019, at a single Canadian site. Most screen failures were due to screening allergen chamber itching and redness requirements. There were four discontinuations: two patients were discontinued due to scheduling conflicts (one each in sequences A [after the second visit] and C [after the first visit]), and two patients voluntarily withdrew from the trial (after the first visit of sequence B). Sixty-six patients (22 per sequence) completed all treatment periods. Baseline demographic characteristics were generally comparable across sequence groups (Table 1). Whereas all subjects were positive by skin prick test to ragweed, the percentages of subjects with allergy to dust mites (26%), cat (47%), dog (7%), tree pollen (54%), fungus (16%), and grass (27%) were lower. Only one enrolled subject reported active asthma, classified as mild, at screening.
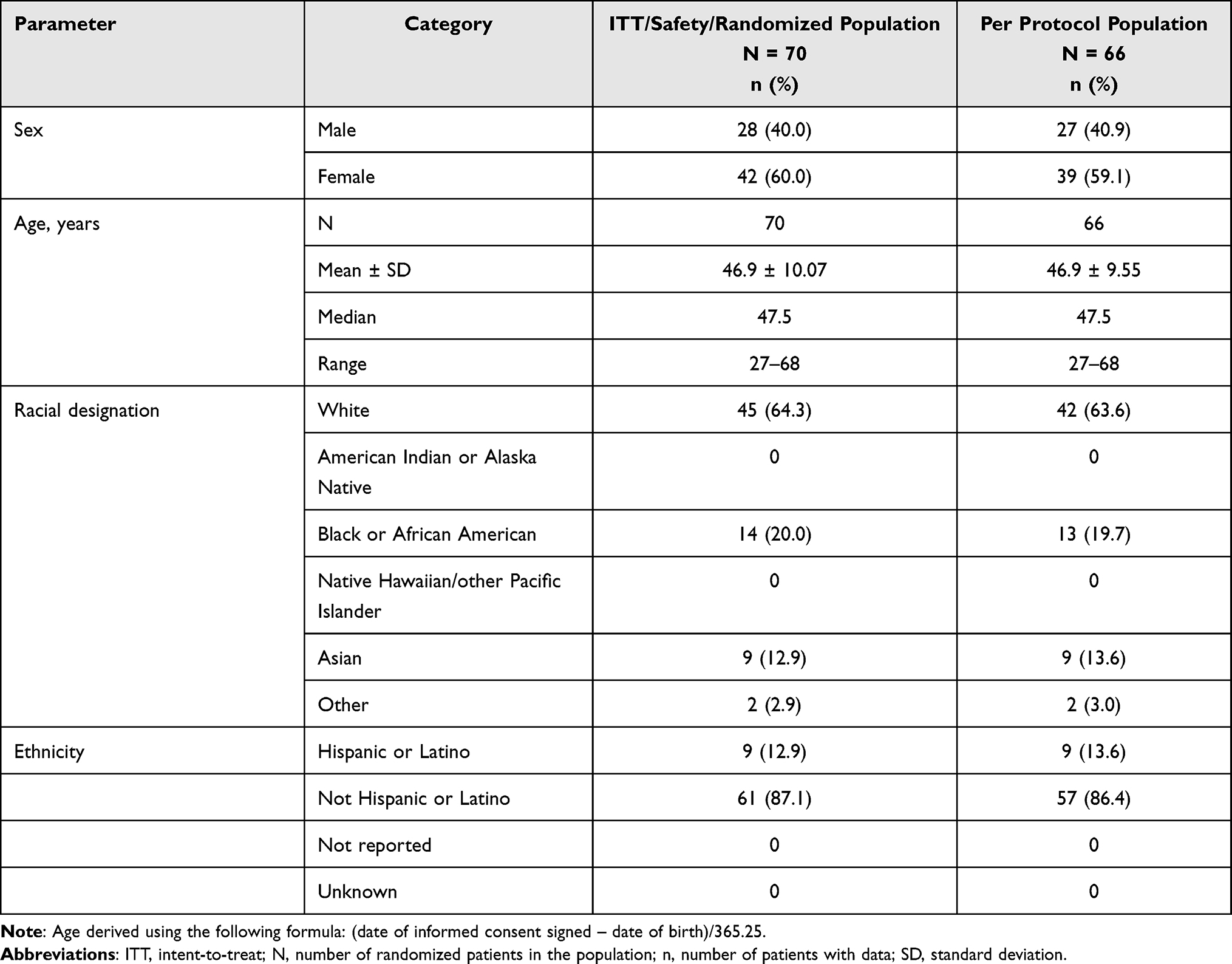 |
Table 1 Baseline Demographic Characteristics |
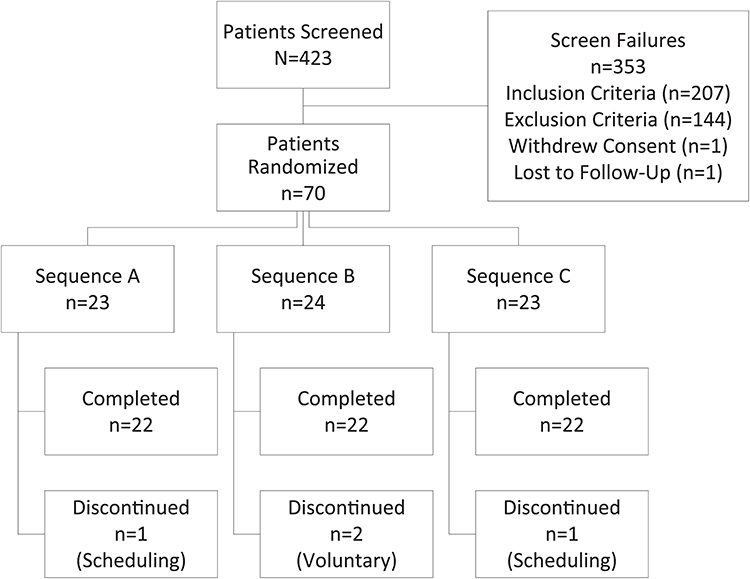 |
Figure 1 Patient disposition. Sequence A = 0.25% reproxalap, 0.5% reproxalap, and vehicle; sequence B = 0.5% reproxalap, vehicle, and 0.25% reproxalap; sequence C = vehicle, 0.25% reproxalap, and 0.5% reproxalap. |
Efficacy
Prophylactic (pre-chamber) treatment with single doses of reproxalap diminished the rate of development of patient-reported ocular itching (Figure 2) and tearing (Figure 3), as well as investigator-assessed conjunctival redness scores (Figure 4), across most time points. In addition, treatment with reproxalap near peak symptomatology led to reductions in symptom scores and conjunctival redness that were maintained through the end of the chamber. Acute and transient increases in tearing were observed with the administration of 0.25% reproxalap and 0.5% reproxalap, and an acute and transient increase in redness was observed with the administration of 0.5% reproxalap. Symptom scores and conjunctival redness diminished in all groups following chamber exit, although scores in the reproxalap groups remained below those of the vehicle group 1 hour after exit, the last time point assessed in the trial. The differences between both reproxalap concentrations and vehicle over all time points assessed were statistically significant for symptoms and conjunctival redness (P<0.0001 for all comparisons). Although a modest dose response was evident for symptom scores, post hoc testing indicated that there were no statistical differences between reproxalap groups, and therefore the lowest effective dose was deemed to be 0.25% reproxalap.
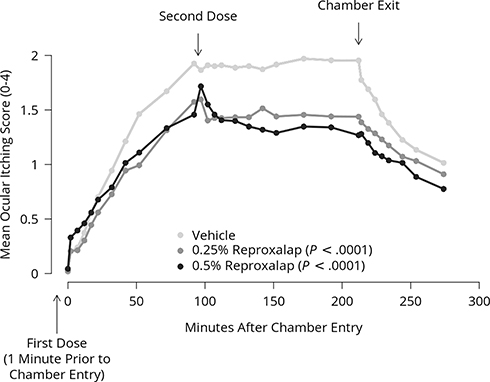 |
Figure 2 Patient-reported ocular itching score. P values derived from mixed effect models for repeated measures analysis of change from baseline (just prior to chamber entry) over all time points in aggregate. |
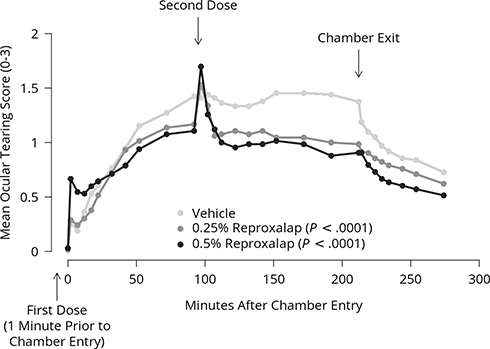 |
Figure 3 Patient-reported ocular tearing score. P values derived from mixed effect models for repeated measures analysis of change from baseline (just prior to chamber entry) over all time points in aggregate. |
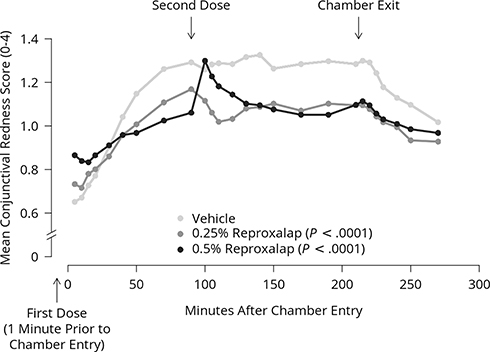 |
Figure 4 Investigator-assessed conjunctival redness score. P values derived from mixed effect models for repeated measures analysis of change from baseline (just prior to chamber entry) over all time points in aggregate. |
For 0.25% reproxalap, the clinical relevance of the symptom score and conjunctival redness findings was confirmed with responder analyses of time to ≥2-point increases (50% of the scale range) for ocular itching (Figure 5) and conjunctival redness (Figure 6) scores in the allergen chamber. Time to worsening of itching and redness was slower, and the percentage of patients with scores of ≥2 was lower (hazard ratios [95% confidence interval] of 0.67 [1.0, 2.2] and 0.51 [1.0, 3.7] for itching and redness, respectively) in patients treated with 0.25% reproxalap than in patients treated with vehicle (P<0.05 for both assessments).
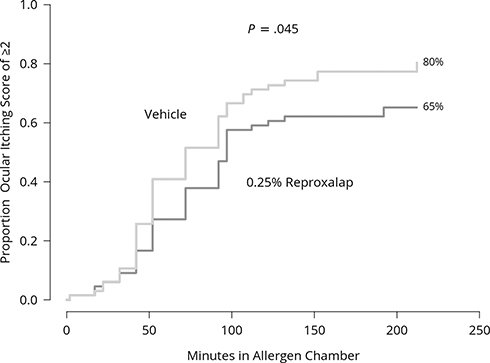 |
Figure 5 Time to patient-reported ocular itching score of ≥2 for 0.25% reproxalap versus vehicle. P value derived from log-rank analysis. |
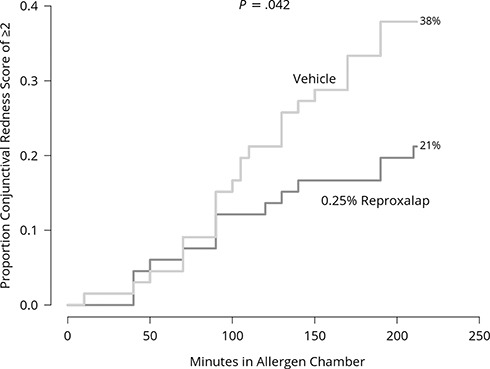 |
Figure 6 Time to investigator-assessed conjunctival redness score of ≥2 for 0.25% reproxalap versus vehicle. P value derived from log-rank analysis. |
Safety and Tolerability
Both concentrations of reproxalap were deemed to be safe and well tolerated. Treatment-emergent AEs related to test article were observed in 47 patients (70%) following exposure to 0.25% reproxalap, 54 patients (78%) following exposure to 0.5% reproxalap, and six patients (9%) following exposure to vehicle. Treatment-emergent AEs most commonly consisted of transient irritation upon instillation. No patient experienced a serious AE and no patient was withdrawn from the trial due to an AE. Best-corrected visual acuity, slit-lamp biomicroscopy, dilated fundoscopy, and intraocular pressure assessments did not reveal any clinically significant findings.
Discussion
The allergen chamber combines the controlled allergen levels of conjunctival challenge with the real-world continuous airborne exposure of field trials, and thus represents a compelling modality for assessment of the prophylactic and treatment drug activity in patients with allergic conjunctivitis. Relative to vehicle, reproxalap reduced the rate of development of patient-reported ocular itching and tearing and investigator-assessed conjunctival redness in an allergen chamber. Similarly, administration of reproxalap near peak symptomatology led to improvements in signs and symptoms greater than that observed with vehicle. The prophylactic and treatment activity of reproxalap were evident within minutes of administration, and reproxalap was generally superior to vehicle throughout the duration of the chamber exposure period and over all time points assessed after chamber exit (Figures 2–4). These results imply that reproxalap is active before, during, and after allergen exposure, potentially addressing real-world clinical challenges faced by patients with allergic conjunctivitis.
The acute but self-limiting increases in symptom scores and redness observed following the mid-chamber administration, particularly evident with 0.5% reproxalap, were likely due to instillation site discomfort, which resolves rapidly, as was evident by improvements in symptom scores and redness at adjacent time points. For 0.25% reproxalap, redness and symptom score increases above the vehicle were minimal at the initial instillation, indicating acute tolerability, and that irritated conjunctival tissues at 90-minutes post-entry may have accentuated any transient instillation response. Instillation site discomfort is common among topical ocular medications and may lead to discontinuation of drugs that, in contrast to reproxalap, require weeks or months to demonstrate activity. Treatment discontinuation is particularly apparent with regard to the current topical therapies available for dry eye disease,20–22 a condition that likely shares approximately 50% overlap with allergic conjunctivitis.23
According to US Food and Drug Administration and European Medicines Agency guidelines,24,25 responder analyses are a critical approach to assess clinical utility. Responder analyses of the lowest effective reproxalap concentration (0.25%) confirmed the clinical relevance of the improvement of ocular itching and conjunctival redness over that of vehicle (Figures 5 and 6). A 2-point escalation in itching and redness scores, equivalent to 50% of the scale range in each case, exceeds the absolute percentage of scale changes (ranging from 8% to 40%) that typically represent clinically important changes in patients with acute discomfort26 and thus delineate conservative thresholds for clinical relevance. Consistent with the time required to exacerbate itching and redness in the allergen chamber, and similar to the itching and redness scores in Figures 2 and 4, responder curves begin to separate as scores approach peak levels, an effect that is maintained or increased following the second dose of test article. Future work is needed to empirically derive meaningful within-patient changes that can be used to assess the clinical relevance of allergic conjunctivitis symptom and sign improvement in subsequent clinical trials.
Conclusions
The present results are among the first data from a controlled trial of a novel drug in an allergen chamber and indicate the prophylactic and treatment activity of reproxalap ophthalmic solution. Larger allergen chamber trials of 0.25% reproxalap, the lowest effective dose in the present trial, are warranted to confirm the onset and duration of improvement in the symptoms and signs of allergic conjunctivitis following treatment.
Abbreviations
AE, adverse event; HEPA, high efficiency particulate air; MMRM, mixed effect models for repeated measures; RASP, reactive aldehyde species; SD, standard deviation.
Data Sharing Statement
The authors do not intend to share participant-level data. Queries or requests should be directed to the corresponding author (T. C. Brady).
Ethics Approval and Informed Consent
The trial (ClinicalTrials.gov: NCT03709121) was performed in Canada in accordance with the Declaration of Helsinki on Ethical Principles for Medical Research Involving Human Patients, the International Council for Harmonisation Guideline on Good Clinical Practice, and all applicable local regulatory requirements and laws. The trial was carried out with approval from the Institutional Review Board (Advarra, Inc., Columbia, MD, USA), informed consent was obtained from the patients, and the research followed Health Insurance Portability and Accountability Act and Personal Information Protection and Electronic Documents Act regulations.
Acknowledgments
Editorial/medical writing support under the guidance of the authors was provided by Christopher Goodwin, PhD (ApotheCom, Yardley, PA, USA), and funded by Aldeyra Therapeutics, Inc., in accordance with Good Publication Practice (GPP3) guidelines (Ann Intern Med 2015; 163:461–464). The data from this study were presented at the American Academy of Ophthalmology Annual Meeting (Virtual); November 13–15, 2020.
Author Contributions
All authors made significant contributions to the work in the areas of study conception and design, data acquisition, or data analysis and interpretation; took part in drafting, revising, or critically reviewing the manuscript; gave final approval for the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
Aldeyra Therapeutics, Inc., funded and participated in the design and implementation of the study, the analysis and interpretation of the data, and the preparation, review, and approval of the manuscript.
Disclosure
D. Clark reports employment with and stock ownership in Aldeyra Therapeutics. P. Karpecki reports consulting for Aerie Pharmaceuticals, Akorn, Alcon Labs, Aldeyra Therapeutics, Allergan/AbbVie, Allysta, Aurinia, Azura Pharmaceuticals, Bausch & Lomb, BioTissue, BlephEx, Bruder Healthcare, Cambium, Dompe, Eyedetec, EyeGate, Eyevance, Imprimis, Kala Pharmaceuticals, Mallinckrodt, Novartis, Oasis Medical, Oyster Point, Regener-Eyes, ScienceBased Health, Sight Sciences, Silk Technologies, Sun Pharmaceutical Industries, Surface Pharmaceuticals, Tarsus Pharmaceuticals, Visant Medical, and Vital Tears. A. M. Salapatek reports employment with Cliantha Research. J.D. Sheppard reports consulting for Allergan, AbbVie, Alcon, Aldeyra Therapeutics, Bausch & Lomb, NovaBay, Novartis, Fidia, Clarios, Visus, Topivert, Noveome, Oyster Point, Santen, Sun Pharmaceutical Industries, Eyevance, ScienceBased Health, and Quidel; and ownership interest in Noveome, Eyedetec, Oyster Point, RPS, TearLab, EyeGate, EyeRx, Clarios, and CVP Partners. T. C. Brady reports employment with and patent interests and stock ownership in Aldeyra Therapeutics and stock ownership in F-star Therapeutics and Evoke Pharma. The authors report no other conflicts of interest in this work.
References
1. Singh K, Axelrod S, Bielory L. The epidemiology of ocular and nasal allergy in the United States, 1988–1994. J Allergy Clin Immunol. 2010;126(4):778–783. doi:10.1016/j.jaci.2010.06.050
2. Leonardi A, Piliego F, Castegnaro A, et al. Allergic conjunctivitis: a cross-sectional study. Clin Exp Allergy. 2015;45(6):1118–1125. doi:10.1111/cea.12536
3. Palmares J, Delgado L, Cidade M, Quadrado MJ, Filipe HP; Season Study Group. Allergic conjunctivitis: a national cross-sectional study of clinical characteristics and quality of life. Eur J Ophthalmol. 2010;20(2):257–264. doi:10.1177/112067211002000201
4. Mandell KJ, Clark D, Chu DS, Foster CS, Sheppard J, Brady TC. Randomized phase 2 trial of reproxalap, a novel reactive aldehyde species inhibitor, in patients with noninfectious anterior uveitis: model for corticosteroid replacement. J Ocul Pharmacol Ther. 2020;36(10):732–739. doi:10.1089/jop.2020.0056
5. Clark D, Sheppard J, Brady TC. A randomized double-masked phase 2a trial to evaluate activity and safety of topical ocular reproxalap, a novel RASP inhibitor, in dry eye disease. J Ocul Pharmacol Ther. 2021;37(4):193–199. doi:10.1089/jop.2020.0087
6. Clark D, Tauber J, Sheppard J, Brady TC. Early onset and broad activity of reproxalap in a randomized, double-masked, vehicle-controlled phase 2b trial in dry eye disease. Am J Ophthalmol. 2021;226:22–31. doi:10.1016/j.ajo.2021.01.011
7. Clark D, Cavanagh C, Shields A, Karpecki P, Sheppard J, Brady TC. Clinically relevant activity of the novel RASP inhibitor reproxalap in allergic conjunctivitis: the Phase 3 ALLEVIATE trial. Am J Ophthalmol. 2021;230:60–67. doi:10.1016/j.ajo.2021.04.023
8. Higdon A, Diers AR, Oh JY, Landar A, Darley-Usmar VM. Cell signalling by reactive lipid species: new concepts and molecular mechanisms. Biochem J. 2012;442(3):453–464. doi:10.1042/BJ20111752
9. Kalariya NM, Ramana KV, Srivastava SK, van Kuijk FJGM. Carotenoid derived aldehydes-induced oxidative stress causes apoptotic cell death in human retinal pigment epithelial cells. Exp Eye Res. 2008;86(1):70–80. doi:10.1016/j.exer.2007.09.010
10. Kauppinen A, Niskanen H, Suuronen T, Kinnunen K, Salminen A, Kaarniranta K. Oxidative stress activates NLRP3 inflammasomes in ARPE-19 cells–implications for age-related macular degeneration (AMD). Immunol Lett. 2012;147(1–2):29–33. doi:10.1016/j.imlet.2012.05.005
11. Ackerman S, Smith LM, Gomes PJ. Ocular itch associated with allergic conjunctivitis: latest evidence and clinical management. Ther Adv Chronic Dis. 2016;7(1):52–67. doi:10.1177/2040622315612745
12. Abelson MB, Chambers WA, Smith LM. Conjunctival allergen challenge: a clinical approach to studying allergic conjunctivitis. Arch Ophthalmol. 1990;108(1):84–88. doi:10.1001/archopht.1990.01070030090035
13. Torkildsen G, Narvekar A, Bergmann M. Efficacy and safety of olopatadine hydrochloride 0.77% in patients with allergic conjunctivitis using a conjunctival allergen-challenge model. Clin Ophthalmol. 2015;9:1703–1713. doi:10.2147/OPTH.S83263
14. Abelson MB, Gomes PJ, Vogelson CT, et al. Clinical efficacy of olopatadine hydrochloride ophthalmic solution 0.2% compared with placebo in patients with allergic conjunctivitis or rhinoconjunctivitis: a randomized, double-masked environmental study. Clin Ther. 2004;26(8):1237–1248. doi:10.1016/S0149-2918(04)80065-1
15. Goldstein MH, Tubridy KL, Agahigian J, et al. A Phase 2 Exploratory Study of a novel interleukin-1 receptor inhibitor (EBI-005) in the treatment of moderate-to-severe allergic conjunctivitis. Eye Contact Lens. 2015;41(3):145–155. doi:10.1097/ICL.0000000000000152
16. Rønborg SM, Mosbech H, Johnsen CR, Poulsen LK. Exposure chamber for allergen challenge. The development and validation of a new concept. Allergy. 1996;51(2):82–88. doi:10.1111/j.1398-9995.1996.tb04562.x
17. Barchuk WT, Salapatek AM, Ge T, D’Angelo P, Liu X. A proof-of-concept study of the effect of a novel H3-receptor antagonist in allergen-induced nasal congestion. J Allergy Clin Immunol. 2013;132(4):838–846. doi:10.1016/j.jaci.2013.05.001
18. Patel P, Salapatek AM, Tantry SK. Effect of olopatadine-mometasone combination nasal spray on seasonal allergic rhinitis symptoms in an environmental exposure chamber study. Ann Allergy Asthma Immunol. 2019;122(2):160–166.e1. doi:10.1016/j.anai.2018.10.011
19. Schulze MM, Jones DA, Simpson TL. The development of validated bulbar redness grading scales. Optom Vis Sci. 2007;84(10):976–983. doi:10.1097/OPX.0b013e318157ac9e
20. White DE, Zhao Y, Ogundele A, et al. Real-world treatment patterns of cyclosporine ophthalmic emulsion and lifitegrast ophthalmic solution among patients with dry eye. Clin Ophthalmol. 2019;13:2285–2292. doi:10.2147/OPTH.S226168
21. White DE, Zhao Y, Jayapalan H, Machiraju P, Periyasamy R, Ogundele A. Treatment satisfaction among patients using anti-inflammatory topical medications for dry eye disease. Clin Ophthalmol. 2020;14:875–883. doi:10.2147/OPTH.S233194
22. White DE, Zhao Y, Jayapalan H, Machiraju P, Periyasamy R, Ogundele A. Physician satisfaction with anti-inflammatory topical medications for the treatment of dry eye disease. Clin Ophthalmol. 2020;14:931–938. doi:10.2147/OPTH.S237832
23. Hom MM, Nguyen AL, Bielory L. Allergic conjunctivitis and dry eye syndrome. Ann Allergy Asthma Immunol. 2012;108(3):163–166. doi:10.1016/j.anai.2012.01.006
24. US Food and Drug Administration. Guidance for industry: patient-reported outcome measures: use in medical product development to support labeling claims; 2009. Available from: www.fda.gov/regulatory-information/search-fda-guidance-documents/patient-reported-outcome-measures-use-medical-product-development-support-labeling-claims.
25. European Medicines Agency. Appendix 2 to the guideline on the evaluation of anticancer medicinal products in man: the use of patient-reported outcome (PRO) measures in oncology studies; 2016. Available from: www.ema.europa.eu/en/documents/other/appendix-2-guideline-evaluation-anticancer-medicinal-products-man_en.pdf.
26. Olsen MF, Bjerre E, Hansen MD, et al. Pain relief that matters to patients: systematic review of empirical studies assessing the minimum clinically important difference in acute pain. BMC Med. 2017;15(1):35. doi:10.1186/s12916-016-0775-3
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.