")
Back to Journals » Clinical Ophthalmology » Volume 17
Repositioning Rates of Toric IOLs Implanted in Cataract Surgery Patients: A Retrospective Chart Review
Authors Hu EH
Received 22 September 2023
Accepted for publication 14 December 2023
Published 23 December 2023 Volume 2023:17 Pages 4001—4007
DOI https://doi.org/10.2147/OPTH.S441524
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Edward H Hu
Wolfe Eye Clinic, Hiawatha, IA, USA
Correspondence: Edward H Hu, Wolfe Eye Clinic, 1195, Boyson Road, Suite 200, Hiawatha, IA, 52233, USA, Email [email protected]
Purpose: To determine the incidence of postoperative repositioning of toric intraocular lenses (IOLs) due to clinically significant rotation.
Patients and Methods: This study included consecutive cataract patients with pre-existing astigmatism who had undergone cataract surgery with toric IOL implantation by a single experienced surgeon. Case records of patients who were recommended to undergo toric IOL repositioning surgery due to clinically significant postoperative IOL rotation from the implanted axis were identified. The need for a secondary intervention to manage residual astigmatism was based upon postoperative residual astigmatic error ≥ 0.75 D, the patient’s qualitative dissatisfaction with the level of postoperative distance vision, dilated post-op examination, and confirmation of the significant potential for astigmatism reduction.
Results: Case records of 993 eyes implanted with AcrySof toric (N = 362), Tecnis Toric I (N = 53), Tecnis Toric II (N = 308), or enVista Toric IOLs (N = 270) were included. Postoperative toric IOL repositioning was recommended in 16 eyes (1.6%). The repositioning rate was highest in the eyes implanted with Tecnis Toric I (5.7%), followed by AcrySof Toric (2.2%), enVista Toric IOLs (1.1%), and Tecnis Toric II (0.6%).
Conclusion: This real-world analysis of eyes implanted with toric IOLs revealed that the rate of surgical IOL repositioning due to clinically significant IOL rotation was lower than 2% for enVista and Tecnis Toric II IOLs. When needed and with appropriate planning, toric IOL repositioning can be very successful.
Keywords: Toric IOLs, astigmatism, IOL rotation, IOL repositioning, rotational stability
Introduction
Implantation of a toric intraocular lens (IOL) is a well-established method for correcting astigmatism at the time of cataract surgery. To achieve the desired postoperative visual acuity, the axis of astigmatism must be accurately determined preoperatively, the toric IOL must be precisely aligned intraoperatively, and it must remain on the intended axis postoperatively. For every degree of toric IOL misalignment, there is an approximately 3.3% loss of astigmatism correction; a toric IOL misalignment of 10° causes ~33% loss of the toric correction, and a 30° misalignment can result in a complete loss of the astigmatic correction.1
Among various factors, postoperative rotation is the most important contributor to toric IOL misalignment.2 Maximum rotation of toric IOLs occurs in the early postoperative period, usually within the first few hours of cataract surgery, and very little rotation occurs after 1 week postoperatively.2,3 Various modifiable and non-modifiable risk factors, including incomplete removal of ophthalmic viscosurgical devices; decentered, non-circular, or unusually large capsulorhexis; longer axial length/high myopia; larger capsular bag size; and fluctuations in intraocular pressure, have been found to be associated with an increased likelihood of toric IOL rotation.4–7 IOL manufacturers have introduced a variety of innovations in IOL material and design to improve postoperative IOL stability and prevent IOL rotation even in the presence of risk factors.
Significant toric IOL rotation may still occur and result in residual astigmatism postoperatively, unsatisfactory visual acuity outcomes, and patient dissatisfaction, necessitating surgical intervention to reposition the toric IOL. The aim of this real-world retrospective study was to determine the repositioning rates of contemporary toric IOLs due to clinically significant rotation.
Materials and Methods
This retrospective study included consecutive cataract patients with pre-existing astigmatism who had undergone toric IOL implantation between January 2018 and December 2022. The study was performed in accordance with the tenets of the Declaration of Helsinki and its amendments and was approved by Salus IRB (Austin, Texas, United States) with a waiver of informed consent as the data were recorded in patient charts as a part of routine clinical practice, and only de-identified patient data were analyzed.
As a part of routine clinical practice, the decision to implant toric IOLs in patients with regular astigmatism was based on biometry measurements obtained from four different devices: iTrace (Tracey Technologies Corp., Houston, TX, USA); TMS-2N corneal topography instrument (Tomey Technology, Nagoya, Japan); Pentacam Scheimpflug imaging system (Oculus Optikgeräte GmbH, Wetzlar, Germany) and Lenstar LS 900 (Haag-Streit AG, Switzerland). In patients with pre-existing dry eye disease (DED), appropriate treatment was administered to optimize the ocular surface and biometric measurements were repeated until minimal fluctuation in keratometry was detected to ensure the stability of measurements.
The toric IOL power and the axis of implantation were calculated using the Barrett toric calculator tool provided by the American Society of Cataract and Refractive Surgery. The intended axis was marked carefully using corneal ink marks and, when needed on occasion, re-marked to ensure accuracy. At the end of the surgery, after wound hydration, the patient was asked to look into the microscope, and toric IOL alignment on the intended axis was reconfirmed.
All toric IOL procedures performed by a single, experienced surgeon (EH) during the study period at Illinois Eye Center in Peoria, IL, and Wolfe Eye Clinic in Cedar Rapids, IA, were evaluated. The operating surgeon had over a decade of experience in toric IOL implantations before the initiation of the study period. The need for a secondary intervention to manage residual astigmatism was based upon postoperative residual astigmatic error ≥0.75 D, the patient’s qualitative dissatisfaction with their postoperative distance vision, dilated post-op examination, and confirmation of significant potential for visual improvement based on the toric enhancement software integrated with iTrace ray-tracing aberrometry and/or www.AstigmatismFix.com analysis. The iTrace system determines the orientation of the toric IOL based on internal ocular aberrations. Its toric IOL enhancement software provides the degree of misalignment of the toric IOL and the direction and magnitude of suggested repositioning to achieve optimal results.8 The www.Astigmatismfix.com website uses the patient’s postoperative manifest refraction and IOL cylinder power and orientation to determine the ideal location for the IOL and estimated refraction when the IOL axis is repositioned to that location.9
Case records of patients for whom toric IOL repositioning surgery was recommended were retrospectively reviewed.
Outcome measures included the percentage of eyes in which IOL repositioning surgery was recommended and/or performed for residual astigmatism due to toric IOL rotation; repositioning rates stratified by IOL type; and comparison of visual and refractive outcomes before and after repositioning surgery.
Statistical Analysis
Data analysis was performed using Microsoft Excel and SPSS software (version 27.0) for Windows (IBM SPSS Statistics 27, IBM Inc., Armonk, NY). Descriptive statistics on categorical data included frequencies and percentages and mean and standard deviation (SD) for continuous data. All p-values were two-sided and were considered statistically significant when less than 0.05.
Results
This retrospective study evaluated 993 eyes that underwent cataract surgery with the implantation of toric IOLs from various lens platforms including AcrySof Toric (Alcon Laboratories, Fort Worth, TX, USA; N = 362); Tecnis Toric I (Johnson & Johnson Vision, Irvine, CA, USA; N = 53); Tecnis Toric II (Johnson & Johnson Vision, Irvine, CA, USA; N = 308) and enVista Toric (Bausch + Lomb, Rochester, NY, USA; N = 270). Of the 993 cases, toric IOL repositioning due to toric IOL rotation was recommended in 16 eyes (1.61%). None of the eyes had misalignment due to incorrect selection of toric IOL. The mean preoperative manifest refraction spherical equivalent in these 16 eyes was −2.99 ± 2.78 D (range −10.38 to 1.50).
Among these 16 eyes, the IOL repositioning rate was highest among eyes implanted with the Tecnis Toric I IOL (5.7%), followed by AcrySof Toric IOL (2.2%), enVista (1.1%) and Tecnis Toric II (0.6%) (Figure 1). Of the 16 eyes requiring surgical reintervention, there was one eye in which IOL repositioning was not possible due to capsular fibrosis, and the patient declined to undergo laser vision enhancement to correct the residual astigmatism. No eye needed an IOL exchange.
 |
Figure 1 Proportion of eyes that underwent toric IOL repositioning due to clinically significant IOL rotation postoperatively (Statistically significant p-values are displayed; other comparisons had p>0.05 and are not displayed). |
Among the 15 eyes that underwent IOL repositioning, mean refractive astigmatism improved from 1.53 ± 0.71 D prior to rotation to 0.21 ± 0.24 D at week 1 after repositioning, with 93% of the eyes achieving visual acuity of 20/25 or better postoperatively. Detailed case-by-case results are presented in Table 1.
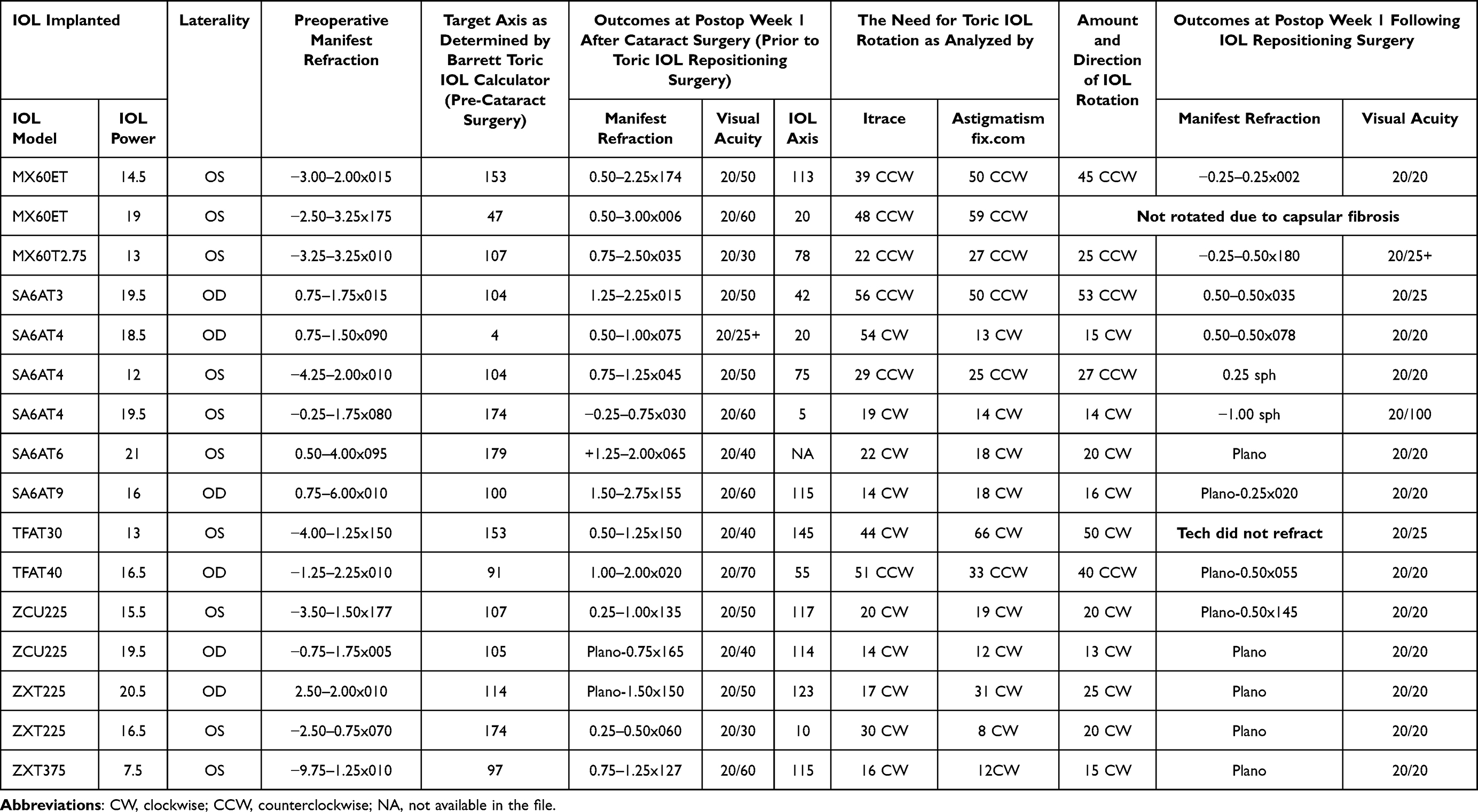 |
Table 1 Relevant Pre-Cataract Surgery, Pre- and Post- IOL Rotation Characteristics of the 16 Eyes That Had Clinically Significant IOL Rotation |
Discussion
This study evaluated the repositioning rates of toric IOLs in a real-world clinical practice setting. It demonstrates that, among all contemporary toric IOLs, clinically significant rotation is uncommon, with Tecnis Toric II and enVista Toric platforms yielding the lowest rates of repositioning.
The risk of IOL rotation for the studied lens platforms has been compared previously.10,11 Garzon et al compared the rotational stability of enVista and AcrySof toric IOLs and reported better rotational stability with enVista toric IOLs (with 90.5% eyes showing IOL rotation ≤5° versus 64.3% of those implanted with AcrySof toric IOL).11 Schartmuller et al compared the non-toric IOLs from these platforms and reported better rotational stability with AcrySof (95.2% of AcrySof eyes had IOL rotation ≤5° compared to 92.5% of Tecnis Toric I and 86.1% of enVista MX60 lenses).10 In a large series, Lee and Chang reported that 91.9% of AcrySof eyes had IOL rotation ≤5° compared to 81.8% of Tecnis Toric I eyes, although visual acuity results were equivalent between the two groups.12
While measurement of mean postoperative IOL rotation is a vital piece of information, the risk of clinically significant IOL rotation necessitating postoperative IOL repositioning may be more valuable for surgeons. In previous studies, the original Tecnis Toric I platform was found to have higher repositioning rates than the AcrySof platform.12–14 Our study also found higher repositioning rates with Tecnis Toric I (5.7%) than the AcrySof (2.2%). High myopia is considered to be one of the risk factors for toric IOL rotation. In the present study, only one patient who underwent Tecnis toric I IOL implantation had high myopia of −10.38 D prior to cataract surgery. Patients who underwent implantation of other IOL types had mild to moderate myopia. There are no previous reports in the literature of risk of IOL repositioning due to clinically significant IOL rotation with Tecnis Toric II or enVista IOL platforms; in the present study, we found that both these IOL have very low repositioning rates of 0.6% and 1.1%, respectively.
Toric IOL manufacturers have taken a variety of approaches to minimize the postoperative rotation of their lenses. The enVista IOL is designed to provide a large contact angle between its haptics and the capsular bag. This broad 110° contact angle is complemented by a high haptic compression force, which increases the stability of the IOL within the capsular bag.15 AcrySof IOLs are known to be made of a very “tacky” material that contributes to their good rotational stability.12,16–20
The Tecnis Toric II platform was designed to improve upon its predecessor with frosted haptics, which offers more surface texture and friction between the lens haptics and the capsular bag. IOL haptics with more surface texture has been documented to offer better rotational stability, probably due to the higher frictional coefficient.21–23 The frosted haptics may also expedite IOL unfolding, with earlier and greater contact between the haptics and the capsular bag equator reducing the risk of the incomplete unfolding of the haptics at the end of surgery.23 A recent prospective study validated that mean absolute lens rotation was 0.94° ± 0.71° and that postoperative rotation was ≤5° in 100% of eyes 3 months after implantation of IOLs with the newer toric design.24 The statistically significantly lower repositioning rate of the Tecnis Toric II vs the Tecnis Toric I IOLs in the present study corroborates this and other findings of a very low rate of rotation with the newer lens platform.3,23,24
While it is important to choose a toric IOL with a low risk of rotation, clinically significant IOL rotation may occur with any IOL. It is important to be prepared to reposition the lens when required. Both methods used by the author to plan for repositioning, the iTrace toric enhancement software and www.AstigmatismFix.com, have been documented to improve outcomes after IOL repositioning. In the present study, if the magnitude of required postoperative repositioning was different between the two methods, the surgeon used the middle value and achieved good results. In the author’s opinion, both www.AstigmatismFix.com and iTrace toric enhancement software work well to determine the degree and direction of IOL repositioning needed.
This retrospective study provides insights into the real-world probability of clinically significant IOL rotation requiring repositioning. The retrospective data also have some inherent disadvantages. While all care was taken to ensure precise alignment of the IOL on the intended axis, some IOL misalignment due to incorrect intraoperative alignment may have occurred. Inoue et al have demonstrated that IOL misalignment due to postoperative IOL rotation is a much larger (2.6 times higher) contributor to misalignment than incorrect intraoperative alignment. Although not studied separately, clinically significant toric IOL misalignment necessitating IOL repositioning is more likely due to postoperative IOL rotation than incorrect alignment.
Conclusion
In conclusion, the rate of clinically significant toric IOL rotation requiring IOL repositioning is low for all IOL platforms. However, in the present study, toric IOL of Tecnis II platform showed the least IOL rotation rates corresponding to only 0.6%. Both www.AstigmatismFix.com and iTrace toric enhancement software work well to determine the degree and direction of IOL repositioning when needed to correct residual astigmatism.
Abbreviations
IOLs, intraocular lenses; SD, standard deviation; DED, dry eye disease.
Data Sharing Statement
The data used to support the findings of this study are included within the article. Clarifications or additional data used to support the findings of this study may be requested from the corresponding author.
Acknowledgments
Jan Beiting (Wordsmith Consulting) and Raman Bedi, MD (IrisARC – Analytics, Research & Consulting) assisted with statistical analysis and preparation of this manuscript.
Partial results of this paper were presented at the 2022 ASCRS Annual Meeting.
Funding
Funding for this study was provided by Johnson & Johnson Vision.
Disclosure
EH is a consultant for Alcon, Bausch + Lomb, and Johnson & Johnson Vision.
References
1. Ma JJ, Tseng SS. Simple method for accurate alignment in toric phakic and aphakic intraocular lens implantation. J Cataract Refract Surg. 2008;34(10):1631–1636. doi:10.1016/j.jcrs.2008.04.041
2. Inoue Y, Takehara H, Oshika T. Axis misalignment of toric intraocular lens: placement error and postoperative rotation. Ophthalmology. 2017;124(9):1424–1425. doi:10.1016/j.ophtha.2017.05.025
3. Quesada GA, Quesada RA, Jones JJ, et al. Reproducibility of the magnitude of lens rotation following implantation of a toric intraocular lens with modified haptics. Clin Ophthalmol. 2022;16:3213–3224. doi:10.2147/OPTH.S373976
4. Emesz M, Dexl AK, Krall EM, et al. Randomized controlled clinical trial to evaluate different intraocular lenses for the surgical compensation of low to moderate-to-high regular corneal astigmatism during cataract surgery. J Cataract Refract Surg. 2015;41(12):2683–2694. doi:10.1016/j.jcrs.2015.07.036
5. Miyake T, Kamiya K, Amano R, Iida Y, Tsunehiro S, Shimizu K. Long-term clinical outcomes of toric intraocular lens implantation in cataract cases with preexisting astigmatism. J Cataract Refract Surg. 2014;40(10):1654–1660. doi:10.1016/j.jcrs.2014.01.044
6. Shah GD, Praveen MR, Vasavada AR, Vasavada VA, Rampal G, Shastry LR. Rotational stability of a toric intraocular lens: influence of axial length and alignment in the capsular bag. J Cataract Refract Surg. 2012;38(1):54–59. doi:10.1016/j.jcrs.2011.08.028
7. Zhu X, He W, Zhang K, Lu Y. Factors influencing 1-year rotational stability of AcrySof toric intraocular lenses. Br J Ophthalmol. 2016;100(2):263–268. doi:10.1136/bjophthalmol-2015-306656
8. Kaur M, Shaikh F, Falera R, Titiyal JS. Optimizing outcomes with toric intraocular lenses. Indian J Ophthalmol. 2017;65(12):1301–1313. doi:10.4103/ijo.IJO_810_17
9. Patnaik JL, Kahook MY, Berdahl JP, et al. Association between axial length and toric intraocular lens rotation according to an online toric back-calculator. Int J Ophthalmol. 2022;15(3):420–425. doi:10.18240/ijo.2022.03.08
10. Schartmuller D, Schwarzenbacher L, Meyer EL, Schriefl S, Leydolt C, Menapace R. Comparison of long-term rotational stability of three commonly implanted intraocular lenses. Am J Ophthalmol. 2020;220:72–81. doi:10.1016/j.ajo.2020.07.019
11. Garzon N, Poyales F, de Zarate BO, Ruiz-Garcia JL, Quiroga JA. Evaluation of rotation and visual outcomes after implantation of monofocal and multifocal toric intraocular lenses. J Refract Surg. 2015;31(2):90–97. doi:10.3928/1081597X-20150122-03
12. Lee BS, Chang DF. Comparison of the rotational stability of two toric intraocular lenses in 1273 consecutive eyes. Ophthalmology. 2018;125(9):1325–1331. doi:10.1016/j.ophtha.2018.02.012
13. Lee BS, Onishi AC, Chang DF. Comparison of rotational stability and repositioning rates of 2 presbyopia-correcting and 2 monofocal toric intraocular lenses. J Cataract Refract Surg. 2021;47(5):622–626. doi:10.1097/j.jcrs.0000000000000497
14. Kramer BA, Berdahl J, Gu X, Merchea M. Real-world incidence of monofocal toric intraocular lens repositioning: analysis of the American Academy of Ophthalmology IRIS Registry. J Cataract Refract Surg. 2022;48(3):298–303. doi:10.1097/j.jcrs.0000000000000748
15. Rocha KM. enVista is a great lens for the imperfect eye. Bausch+Lomb. Available from: https://www.bauschsurgical.com/resources/peer-opinions/envista-is-a-great-lens-for-the-imperfect-eye/.
16. Haripriya A, Gk S, Mani I, Chang DF. Comparison of surgical repositioning rates and outcomes for hydrophilic vs hydrophobic single-piece acrylic toric IOLs. J Cataract Refract Surg. 2021;47(2):178–183. doi:10.1097/j.jcrs.0000000000000415
17. Holland E, Lane S, Horn JD, Ernest P, Arleo R, Miller KM. The AcrySof toric intraocular lens in subjects with cataracts and corneal astigmatism: a randomized, subject-masked, parallel-group, 1-year study. Ophthalmology. 2010;117(11):2104–2111. doi:10.1016/j.ophtha.2010.07.033
18. Chang DF. Comparative rotational stability of single-piece open-loop acrylic and plate-haptic silicone toric intraocular lenses. J Cataract Refract Surg. 2008;34(11):1842–1847. doi:10.1016/j.jcrs.2008.07.012
19. Chang DF. Repositioning technique and rate for toric intraocular lenses. J Cataract Refract Surg. 2009;35(7):1315–1316. doi:10.1016/j.jcrs.2009.02.035
20. Oshika T, Fujita Y, Hirota A, et al. Comparison of incidence of repositioning surgery to correct misalignment with three toric intraocular lenses. Eur J Ophthalmol. 2020;30(4):680–684. doi:10.1177/1120672119834469
21. Vandekerckhove K. Rotational stability of monofocal and trifocal intraocular toric lenses with identical design and material but different surface treatment. J Refract Surg. 2018;34(2):84–91. doi:10.3928/1081597X-20171211-01
22. Vukich JA, Ang RE, Straker BJK, et al. Evaluation of intraocular lens rotational stability in a multicenter clinical trial. Clin Ophthalmol. 2021;15:3001–3016. doi:10.2147/OPTH.S309214
23. Takaku R, Nakano S, Iida M, Oshika T. Influence of frosted haptics on rotational stability of toric intraocular lenses. Sci Rep. 2021;11(1):15099. doi:10.1038/s41598-021-94293-3
24. Chang DH, Hu J, Miller KM, Vilupuru S, Zhao W. Post-market evaluation of rotational stability and visual performance of a new toric intraocular lens with frosted haptics. Clin Ophthalmol. 2022;16:4055–4064. doi:10.2147/OPTH.S389304
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.