Back to Journals » Journal of Pain Research » Volume 13
Repeated Cesarean Delivery Predicted a Higher Risk of Inadequate Analgesia Than Primary Cesarean Delivery: A Retrospective Study with Propensity Score Match Analysis
Authors Yang G ![]() , Bao X, Peng J, Li J, Yan G, Jing S
, Bao X, Peng J, Li J, Yan G, Jing S ![]() , Li H
, Li H ![]() , Duan G
, Duan G ![]()
Received 2 September 2019
Accepted for publication 7 March 2020
Published 18 March 2020 Volume 2020:13 Pages 555—563
DOI https://doi.org/10.2147/JPR.S229566
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Guiying Yang, Xiaohang Bao, Jing Peng, Jie Li, Guangming Yan, Sheng Jing, Hong Li, Guangyou Duan
Department of Anesthesiology, Second Affiliated Hospital of Army Medical University, Chongqing 400037, People’s Republic of China
Correspondence: Hong Li; Guangyou Duan
Department of Anesthesiology, Second Affiliated Hospital of Army Medical University, Chongqing, People’s Republic of China
Tel +8618323376014
Fax +862368774997
Email [email protected]; [email protected]
Purpose: This study aimed to compare the analgesic outcomes between primary and repeated cesarean delivery.
Patients and Methods: We performed a retrospective analysis based on the medical records of a teaching hospital in China from January 2018 to March 2019. We collected data on demographic characteristics, perioperative complications, anesthesia, and surgical factors for cesarean delivery patients. We also recorded the postoperative analgesic strategy, pain intensity (assessed by the number rating scale) during the first 48 hrs after surgery, hospital cost, and hospital stay. Postoperative inadequate analgesia was defined by a score of ≥ 4 in the number rating scale. Analgesic outcomes after cesarean delivery between primiparas and multiparas were compared using propensity score matching analysis. Moreover, subgroup logistic analysis for different age groups (≥ 35 and < 35 years) was performed to investigate the effect of the maternal category on postoperative inadequate analgesia.
Results: A total of 1543 patients were included in the analysis and 571 pairs (1142 patients) were matched in the primiparas and multiparaparas group according to their propensity score. In both the non-matched and matched cohort, the incidence of inadequate analgesia in the primiparas group was lower than that in the multiparas group (16.7% vs. 24.0%, P < 0.001 and 16.1% vs. 23.5%, P = 0.002; respectively). The multiparas group was identified as being at risk of inadequate analgesia after cesarean delivery in both age groups (age ≥ 35 years, odds ratio: 2.18, 95% confidence interval: 1.20– 3.95; age < 35 years, odds ratio: 1.43, 95% confidence interval 1.08– 1.89).
Conclusion: Multiparas that undergo a repeat cesarean delivery had a significantly higher risk of inadequate postoperative pain treatment than primiparas. The maternal category should be considered when formulating the postoperative analgesia strategy after cesarean delivery.
Keywords: cesarean delivery, analgesia, primipara, multipara
Introduction
Cesarean delivery is one of the most commonly performed in-patient surgical procedures worldwide. However, despite numerous measures being taken to manage postoperative pain after cesarean delivery, inadequate pain relief remains common with a reported incidence of approximately 20–40%.1–3 Inadequate pain treatment after cesarean delivery is associated with delayed functional recovery, longer hospital stay, and long-term adverse outcomes such as postoperative persistent pain.4,5 Previous studies have suggested that exploring inter-individual variability in postoperative pain might be helpful toward accurately applying targeted treatment to women at risk of experiencing severe post-cesarean delivery pain and improve their clinical outcomes.6 Since the implementation of the new national two-child policy,7,8 an increasing number of women who have previously undergone cesarean delivery have received an another cesarean delivery. Thus, there is a novel clinical challenge regarding postoperative pain management in China. Given their scarred uterus, multiparas often face more operative difficulties and require longer surgery times, which may induce more serious noxious stimulation than primary cesarean delivery.9,10 Moreover, a previous study reported that a history of surgery was associated with a higher risk of inadequate analgesia.11 In contrast, multiparas that undergo a repeat cesarean delivery are often older, which has been associated with a lower level of postoperative pain.12–14 There has been a lack of studies that evaluate the differences in postoperative pain control between multiparas and primiparas.
Currently, there is a one-size-fits-all approach for postoperative analgesia after cesarean delivery for both multiparas and primiparas. Furthermore, in the recent Practice Guidelines for Obstetric Analgesia and Anesthesia, no specific explanation was given regarding postoperative pain treatment for multiparas and primiparas.15,16 Therefore, we investigated the potential differences in postoperative analgesia outcomes by conducting a retrospective study with propensity score match analysis on primiparas undergoing primary cesarean delivery and multiparas undergoing a repeat cesarean delivery.
Materials and Methods
Patients
This was a single-center retrospective cohort study. Study protocol was approved by the Institutional Ethics Committee of the Second Affiliated Hospital of Army Medical University, Chongqing, China (approved ID: 2019-040-1), which waived the requirement for obtaining informed consent from the participants. The participants’ names and other forms of identification were deleted before analysis. As shown in Figure 1, from January 2018 to March 2019, we enrolled a total of 1543 Chinese women who were aged from 20 to 45 years and had undergone primary or repeat cesarean delivery via a transverse incision under the subarachnoid space block anesthesia. The inclusion criteria included women with the gestational age of 37 to 40 weeks, singleton pregnancy, and an American Society of Anesthesiology physical status I–II. The exclusion criteria included women with gemellary pregnancy, fetal death, receiving epidural or general anesthesia, and with missing data (Figure 1).
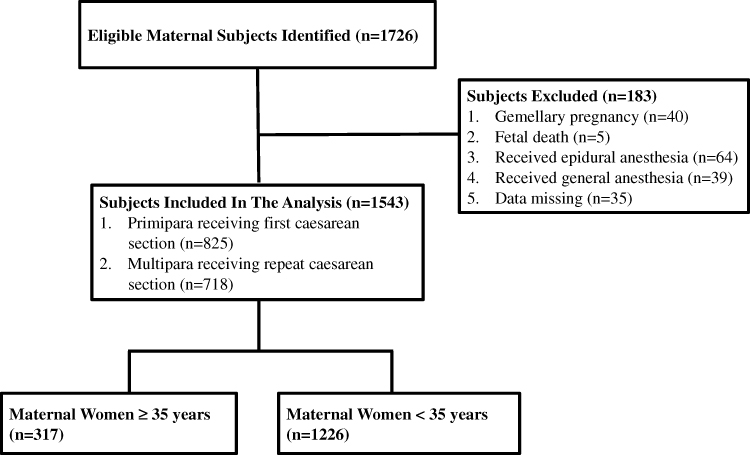 |
Figure 1 Flow diagram of patient inclusion. |
Data Source
All data were obtained from medical records from The Affiliated Hospital of Army Medical University. Preoperative demographic and baseline data were collected from the electronic medical record system and recorded by a gynecologist. Intraoperative complications and anesthesia-related data were recorded by an anesthetist. Postoperative pain assessment was followed up and recorded by a nurse anesthetist.
Anesthesia and Analgesia
All patients had received subarachnoid space anesthesia. Anesthesia was performed by an experienced anesthetist who administered ropivacaine (AstraZeneca AB,20–25 mg) to the puncture site (L3-L4 or L2-L3). Postoperative analgesia was started immediately after cesarean delivery. In the hospital, patient-controlled intravenous analgesia (PCIA) was routinely performed through a mechanical infusion pump. The background volume was 4.0 mL/h and the additional dose was 1 mL with a locking time of 15 min. Tramadol (Grunenthal) 800 mg and flurbiprofen Axetil (Beijing teide pharmaceutical co. LTD) 200 mg with 200 mL 0.9% normal saline was used for PCIA.
Patient Data and Outcomes Collection
The incidence of inadequate postoperative analgesia during the first 48 hrs after cesarean delivery was used as the primary outcome. The number rating scale (NRS, 0–10, where 0 is defined as no pain and 10 as maximum pain) was used to evaluate the postoperative pain intensity at 6, 12, 24, and 48 hrs. Inadequate analgesia was defined as an NRS score ≥ 4. In addition, cases who requested extra rescue treatment during the 48 hrs postoperative analgesia were recorded.
The following maternal preoperative complications were recorded:
- Gestational hypertension, which included emerging hypertension during pregnancy, pre-pregnancy hypertension, eclampsia, and pre-eclampsia.
- Gestational diabetes mellitus, including emerging gestational diabetes and pre-pregnancy diabetes.
- Polyhydramnios and oligoamnios, which refers to an amniotic fluid volume > 2000 mL and < 300 mL, respectively, during pregnancy.
- Fetal macrosomia, which refers to a fetus weighing ≥ 4000 g. Placental diseases including placenta previa, placenta implantation, and placenta abruption.
- Pre-diagnosed fetal diseases including fetal congenital heart disease, kidney disease and brain disease such as hydronephrosis and hydrocephalus etc. Premature membrane rupture, which is defined as membrane rupture before formal contractions.
Patients who used intrauterine balloon tamponade for uterine inertia and postpartum hemorrhage treatment were recorded. Information on synchronized surgery after cesarean section, such as simultaneous ligation, ovarian cyst surgery, and uterine fibroid surgery were recorded.
Patient demographic data such as body mass index (BMI), age, intraoperative blood loss volume, intraoperative blood transfusion volume, neonatal Apgar score, neonatal weight, and neonatal diseases at hospitalization were measured. Postoperative intestinal function recovery which referred to the recovery of anal exhaust after operation, off-bed activity at one and two days after surgery, hospital cost, and length of hospital stay were also recorded.
Statistical Analysis
In this study, the incidence of postoperative inadequate pain control was considered the primary outcome. Through propensity score-matched analysis, the basal characteristics between multiparas and primiparas group could be balanced. Based on the similar basal characteristics, the primary and other outcomes could be compared simultaneously. Thus, propensity score-matched analysis was considered as the primary analysis in the study. The PASS software version 11.0 (company name, location) was used for power analysis. Based on a two-sided group comparison, a sample size of 571 in each group for the propensity score-matched analysis achieved 97.7% power to detect a difference of 7.4% between the multiparas and primiparas group.
Continuous variables were presented as mean ± standard deviation while categorical variables were presented as percentages. Patients were classified as either multipara or primipara. Student’s t-tests or Mann–Whitney U-tests were performed to compare the differences between the multiparas and primiparas group as appropriate. The χ2 test was used to compare categorical variables between the two groups. The relative risk for the incidence of postoperative inadequate analgesia was calculated with a 95% confidence interval (CI).
Given the potential differences in the women’s baseline data between the multiparas and primiparas group, we performed a propensity score-matched analysis to further compare the intergroup differences. The propensity score was calculated for the following baseline variables: age group (< 35 years and ≥ 35 years), placenta disease (yes/no), oligoamnios or polyhydramnios (yes/no), pre-diagnosed fetal disease (yes/no), premature membrane rupture (yes/no), hypertension (yes/no), gestational diabetes mellitus (yes/no), emergency operation (yes/no), with or without intrauterine balloon tamponade, and other synchronized surgeries. Matching was carried out using the 1:1 nearest neighbor method without replacement under a logit model, which yielded 571 subjects in the multiparas group matched with 571 subjects in the primiparas group (Figure 2). We also used a non-matched cohort to compare baseline data and outcomes between the two groups.
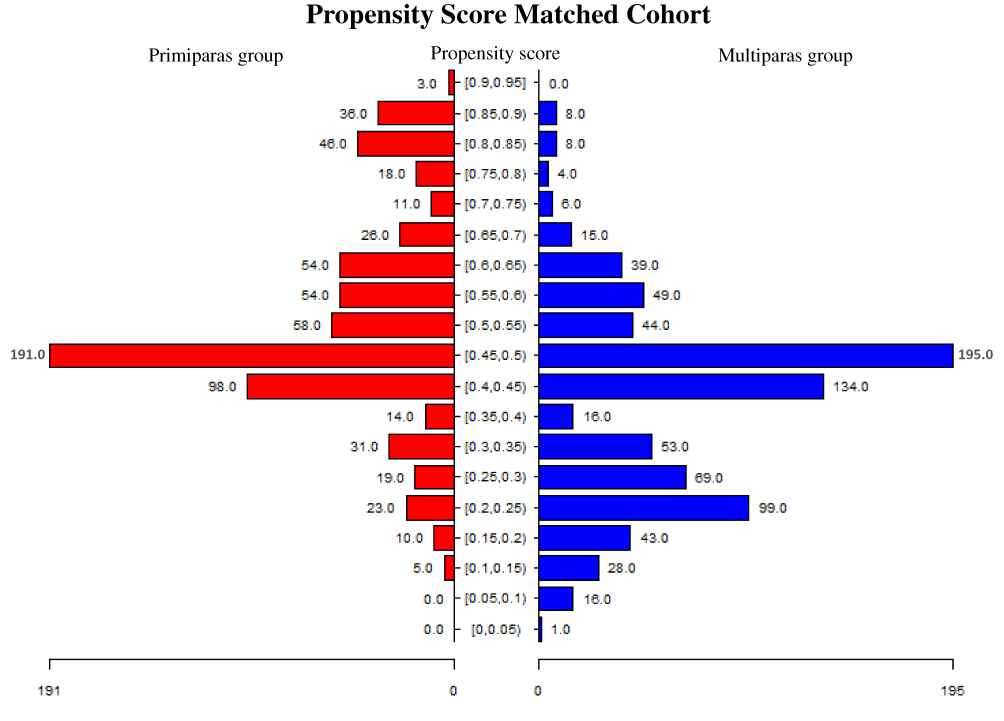 |
Figure 2 Distributions of subjects in the primiparas and multiparas group after matching of the propensity scores. The distributions of included matched pairs at different propensity scores (from [0–0.05] to [0.90–0.95]) in the multiparas and primiparas group, respectively, were presented. |
Subgroup logistic analysis was performed based on the two age groups (< 35 years and ≥ 35 years). Considering the intraoperative variables such as surgery time, blood loss, and the postoperative variables such as maternal complication at hospitalization can be affected by the patients’ basal inherent factors including maternal type, we only included baseline variables in the subgroup logistic analysis. The outcome variable was considered as the presence or absence of postoperative inadequate analgesia. A step-wise logistic regression analysis was performed, and all baseline variables were included in the model. The odds ratio with a 95% CI was calculated. All data were analyzed using SPSS 22.0 and R statistical software. A two-side P-value < 0.05 was considered statistically significant.
Results
Comparisons in Non-Matched Patients
We enrolled 1543 patients, 825 and 718 of whom underwent primary and repeat cesarean delivery, respectively. The demographic and preoperative baseline data of the two groups are shown in Table 1. The mean age of patients in the primiparas group was lower than that of those in the multiparas group (P < 0.001). There were significant between-group differences in the incidences of placental disease, oligoamnios or polyhydramnios, pre-diagnosed fetal disease, premature membrane rupture, hypertension, gestational diabetes, emergency operation, intrauterine balloon tamponade, and other synchronized surgeries (P < 0.05). There was no significant between-group difference in the other preoperative parameters (P > 0.05).
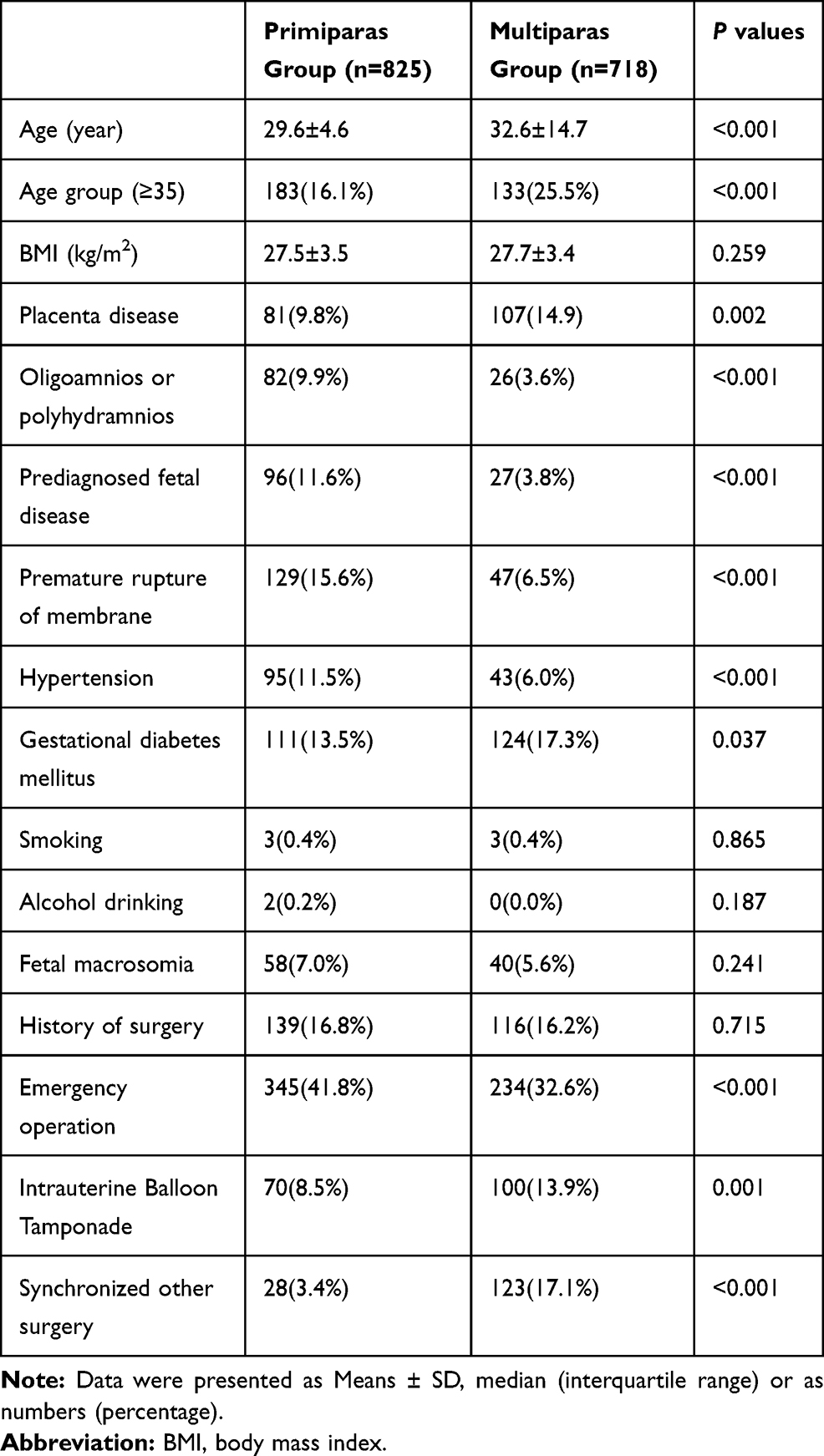 |
Table 1 Demographic and Preoperative Baseline Data for All Included Non-Matched Patients |
As shown in Table 2, the incidence of inadequate postoperative analgesia in the primiparas group was lower than that in the multiparas group (16.7% vs. 24.0%, P < 0.001). The odds ratio for the multiparas to experience inadequate analgesia was 1.57 (95% CI, 1.22–2.02). And the incidence of extra analgesia requirement for the multiparas group was higher than that in the primiparas group (9.5% vs. 6.2%, P=0.016). Intraoperative blood loss, the ratio of women with intraoperative blood loss ≥ 500 mL, and intraoperative blood transfusion volume were higher in the multiparas group than in the primiparas group (P < 0.001). The surgery duration in multiparas group was higher than that in primiparas group (83.1±26.4 vs.76.9±25.2 min, P<0.001). The incidence of presenting an Apgar score ≤ 7 at 1 and 5 min after fetal delivery was higher in the primiparas group than in the multiparas group (P < 0.05). The incidence of neonatal diseases at hospitalization was higher in the primiparas group than in the multiparas group (5.3% vs. 2.2%, P = 0.002). The incidence of intestinal function recovery at 1 day was higher in the primiparas group than in the multiparas group (25.7% vs. 21.2%, P = 0.037) while the incidence of maternal complications at hospitalization was lower in the primiparas group than in the multiparas group (4.1% vs. 7.5%, P = 0.004). The length of hospital stay was longer in the primiparas group than in the multiparas group (4.4 ± 2.4 days vs. 4.2 ± 2.5 days, P = 0.048).
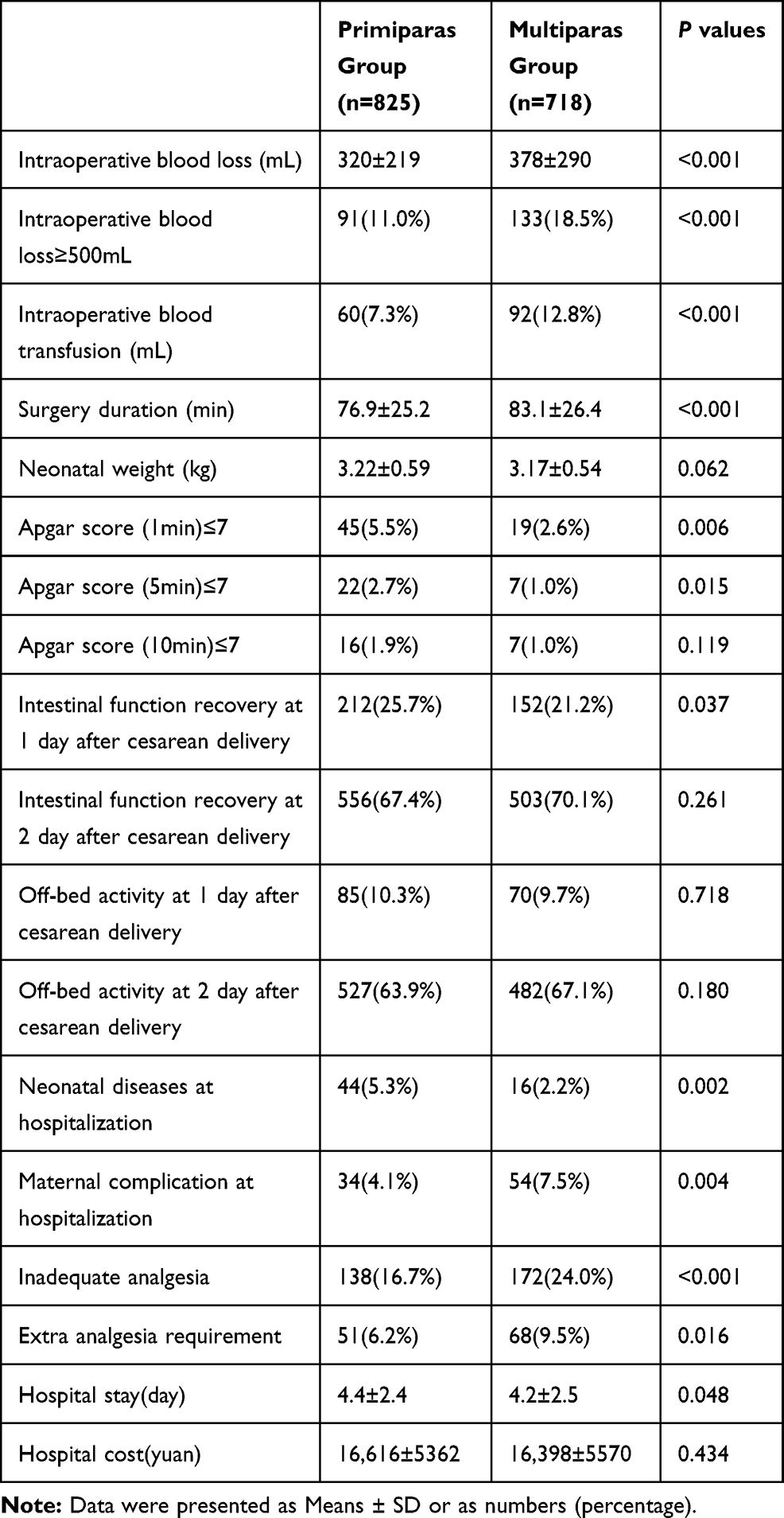 |
Table 2 Intraoperative and Postoperative Outcomes for All Included Non-Matched Patients |
Comparisons in Matched Patients
After propensity score matching, there was no significant between-group difference in the demographic and preoperative baseline data (Table 3, P > 0.05). As shown in Table 4, the surgery duration in the multiparas group was higher than that in primiparas group (82.8±25.9 vs. 74.0±21.2min, P<0.001). The incidence of inadequate analgesia was lower in the primiparas group than in the multiparas group (16.1% vs. 23.5%, P = 0.002), and the odds ratio for a multipara to experience inadequate analgesia was 1.59 (95% CI, 1.19–2.15). The incidence for the needing an extra analgesia in the multiparas group was higher than that of the primiparas group (10.1% vs. 6.5%, P=0.026). The length of hospital stay was longer in the primiparas group than in the multiparas group (4.5 ± 2.8 vs. 4.1 ± 2.5 days, P = 0.019) and the hospital cost was higher in the primiparas group than in the multiparas group (17,125 ± 5790 vs. 16,111 ± 5051 Yuan, P = 0.002). In addition, the neonatal weight was higher in the primiparas group than in the multiparas group (3.26 ± 0.55 vs. 3.18 ± 0.54 kg, P = 0.009) (Table 4).
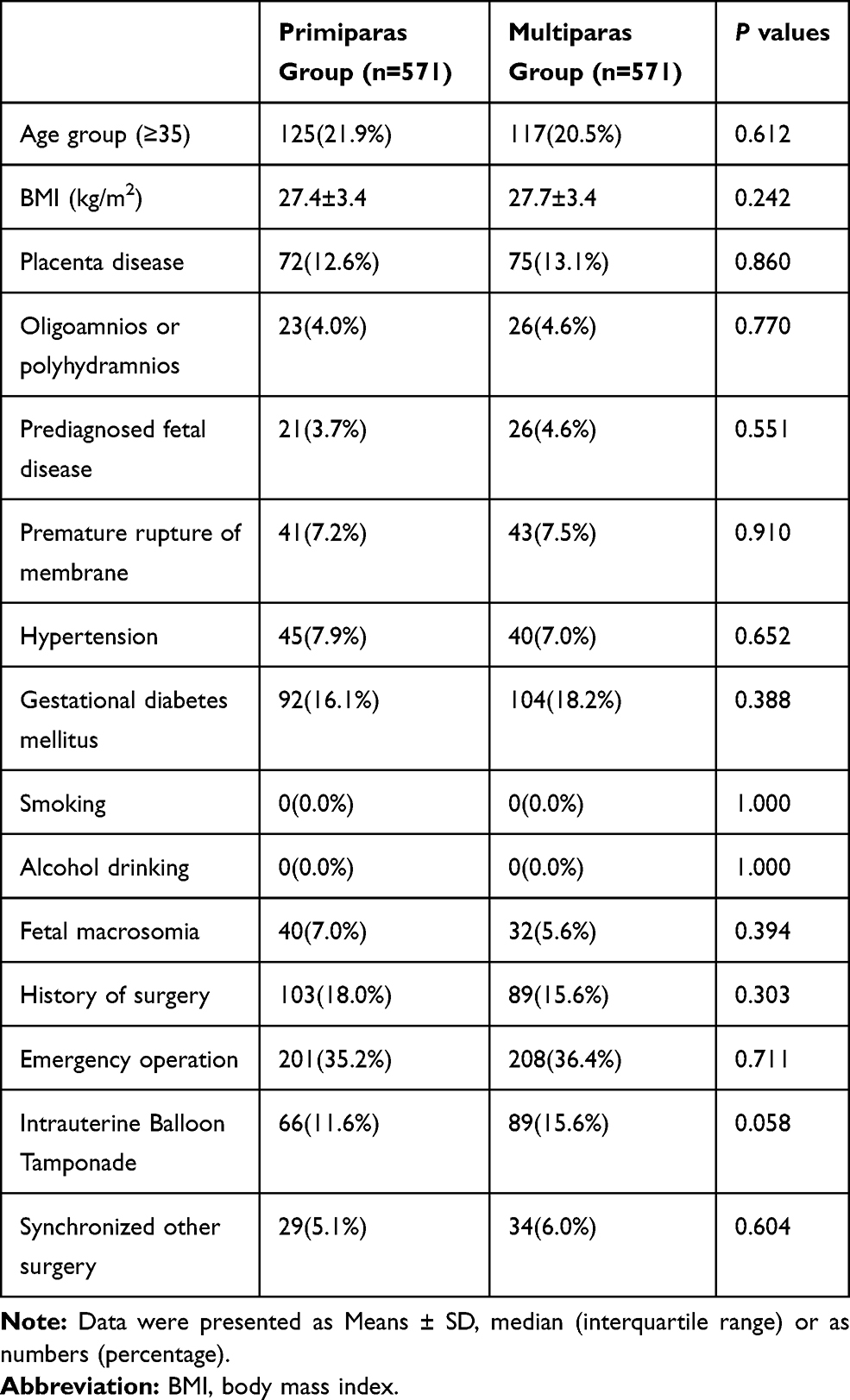 |
Table 3 Demographic and Preoperative Baseline Data for Matched Patients |
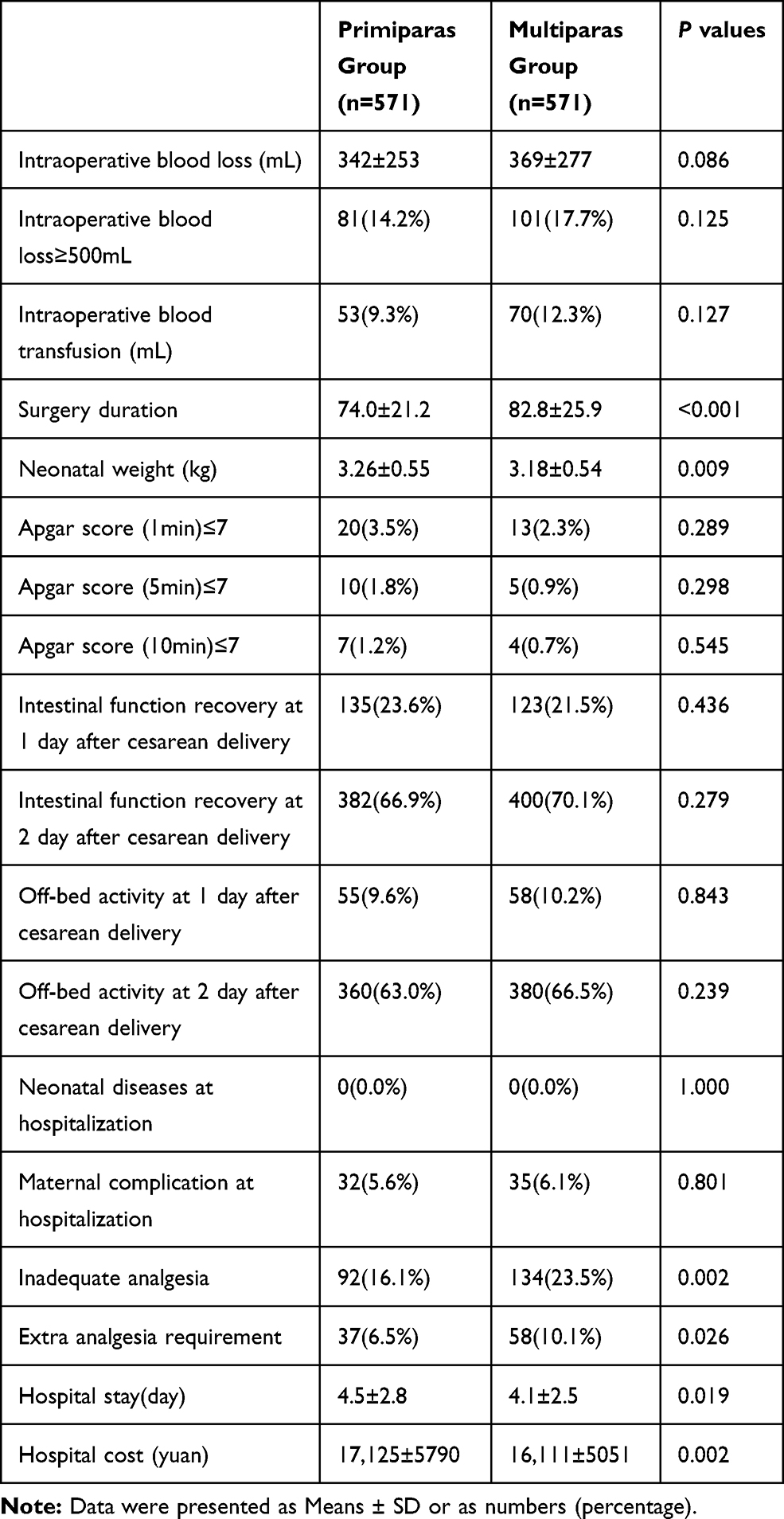 |
Table 4 Intraoperative and Postoperative Outcomes for Matched Patients |
Subgroup Analysis
For all included maternal women, the results of stepwise logistic regression analysis showed that only multiparas was identified as a risk factor of inadequate analgesia (OR = 1.53, 95% CI: 1.19–1.97, P = 0.001; Table 5). In maternal women with an age ≥ 35 years, multiparas (OR = 2.18, 95% CI: 1.20–3.95, P = 0.010) and gestational diabetes mellitus (OR = 1.96, 95% CI: 1.07–3.58, P = 0.029) were identified as risk factors of inadequate analgesia while premature membrane rupture (OR = 0.11, 95% CI: 0.02–0.83, P = 0.033) was the protective factor against inadequate analgesia. In contrast, for maternal women with an age < 35 years, multiparas was the only risk factor of inadequate analgesia (OR = 1.43, 95% CI: 1.08–1.89, P = 0.014).
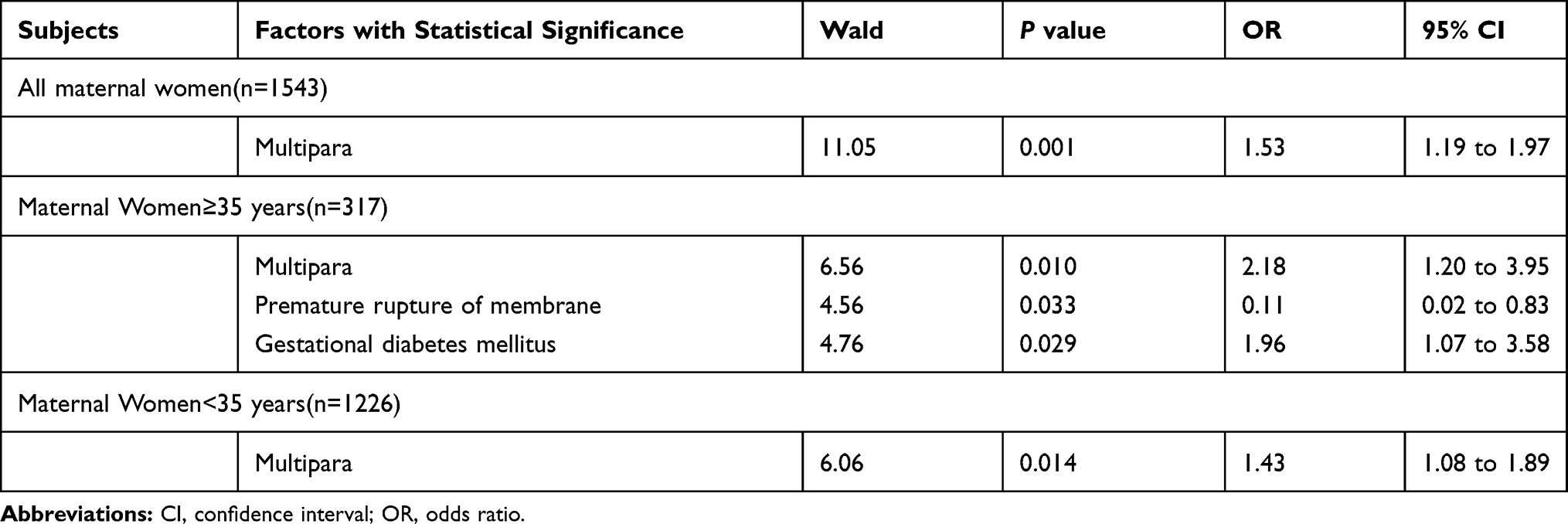 |
Table 5 Factors with Statistical Significance on Inadequate Analgesia in Stepwise Logistic Regression Analysis for Different Age Groups |
Discussion
To the best of our knowledge, this is the first study to explore the differences in postoperative analgesia between primiparas undergoing primary cesarean delivery and multiparas undergoing a repeat cesarean delivery through retrospective analysis. Our findings showed that the incidence of inadequate analgesia was significantly lower in the primiparas group than in the multiparas group. This finding was further validated in the matched cohort obtained after propensity score matching and also by a subgroup analysis of both age groups (≥ 35 and < 35 years).
In the United States, it has been reported that repeat cesarean delivery due to a previous uterine scar contributed to more than 30% of all cesarean deliveries.17,18 Therefore, it is important to understand the difference in the degree of postoperative pain between patients with primary and repeat cesarean delivery to improve postoperative analgesic management. We found that the incidence of inadequate analgesia was lower in the primiparas group than in the multiparas group in both the non-matched and matched cohorts. The results showed that the multiparas are more likely to require extra analgesia than the primiparas, which could be an indicator for postoperative analgesia requirement. In the logistic analysis, multiparas was identified as a risk factor of inadequate analgesia in all maternal women (OR = 1.53, 95% CI: 1.19–1.97) and in those in the different age groups. This further demonstrated that multiparas is a significant predictor of inadequate analgesia in women undergoing cesarean delivery and should be considered when formulating the postoperative analgesic strategy.
Based on the current and previous findings, this phenomenon could be attributed to several reasons. First, a previous history of surgery might increase patients’ pain sensitivity11,19 and has been identified as a risk factor for experiencing inadequate postoperative pain treatment.20 Second, severe adhesions induced by previous surgery are often inevitable, and thus could increase operative difficulties.21,22 The surgery duration in multiparas group was higher than that in primiparas group in both the non-matched and matched cohorts, suggesting increased operative difficulties in patients who underwent a previous cesarean delivery. Therefore, based on the above information, it can be speculated that multiparas might experience more postoperative pain than primiparas. However, the mean hospital stay was longer in the primiparas group than in the multiparas group in both non-matched and matched cohorts. This suggests that primiparas might need more care than multiparas after cesarean delivery. Moreover, the hospital cost was higher in the primiparas group than in the multiparas group in the matched cohort, which might due to the longer hospital stay.
Our results showed that gestational diabetes mellitus (OR = 1.96, 95% CI: 1.07–3.58) was a risk factor for inadequate analgesia in maternal women with an age ≥ 35 years. Since the age of the multiparas was higher than that of the primiparas, their chance of developing diabetes was higher. A previous study has reported increased pain sensitivity in diabetic patients,23,24 which could have also attributed to the inadequate analgesia. Moreover, we found that premature membrane rupture (OR = 0.11, 95% CI: 0.02–0.83), which can induce uterine contraction, was a protective factor against inadequate analgesia in maternal women with an age ≥ 35 years. We speculated that early uterine contraction may be an influencing factor in postoperative pain treatment. This interesting finding can be considered in postoperative analgesia for older parturient women; however, future studies should provide direct clinical evidence.
Several limitations should be considered when interpreting the results of the current study. First, this was a retrospective study, which limits the collection of relevant data for this investigation. Second, only Chinese women from urban areas were included; therefore, race and socioeconomic status should be considered when interpreting the current results.25,26 Thirdly, instead of neuraxial analgesic, tramadol and flurbiprofen axetil were used as PCIA after cesarean section. Therefore, the possible difference in analgesia outcomes between primiparas and multiparas when using other analgesic strategies require further validation. In addition, in our hospital mechanical pump was used for PCIA, which could not record the analgesic consumption and we were not able to report the amount of analgesic used between the two groups. Thus the analgesic consumption between primiparas and multiparas should be studied in the future.
In summary, compared to primiparas, multiparas undergoing a repeat cesarean delivery had a significantly higher risk of experiencing inadequate postoperative pain treatment. Individual differences between primiparas and multiparas should be considered when formulating the postoperative analgesia strategy after cesarean delivery in the future.
Abbreviations
OR, Odds ratio; CI, Confidence interval; BMI, body mass index; PCIA, patient-controlled intravenous analgesia.
Ethics and Consent Statement
The study protocol was approved by the Institutional Ethics Committee of Second Affiliated Hospital of Army Medical University, Chongqing, China (approved ID: 2019-040-1)
Data Sharing Statement
All data can be acquired from the corresponding author (HL) by request.
Author Contributions
All authors contributed to data analysis, drafting and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
The study was supported by National Key Research and Development Project (2018YFC0117200) and Clinical Research Project of Second Affiliated Hospital of Army Medical University (No. 2016YLC10).
Disclosure
The authors declare no competing interests.
References
1. Gerbershagen HJ, Aduckathil S, van Wijck AJ, Peelen LM, Kalkman CJ, Meissner W. Pain intensity on the first day after surgery: a prospective cohort study comparing 179 surgical procedures. Anesthesiology. 2013;118(4):934–944. doi:10.1097/ALN.0b013e31828866b3
2. Patel R, Carvalho JC, Downey K, Kanczuk M, Bernstein P, Siddiqui N. Intraperitoneal instillation of lidocaine improves postoperative analgesia at cesarean delivery: a randomized, double-blind, placebo-controlled trial. Anesth Analg. 2017;124(2):554–559. doi:10.1213/ANE.0000000000001799
3. Ortner CM, Granot M, Richebe P, Cardoso M, Bollag L, Landau R. Preoperative scar hyperalgesia is associated with post-operative pain in women undergoing a repeat caesarean delivery. Eur J Pain. 2013;17(1):111–123. doi:10.1002/j.1532-2149.2012.00171.x
4. Eisenach JC, Pan PH, Smiley R, Lavand’Homme P, Landau R, Houle TT. Severity of acute pain after childbirth, but not type of delivery, predicts persistent pain and postpartum depression. Pain. 2008;140(1):87–94. doi:10.1016/j.pain.2008.07.011
5. Lavand’homme P. Chronic pain after vaginal and cesarean delivery: a reality questioning our daily practice of obstetric anesthesia. Int J Obstet Anesth. 2010;19(1):1–2. doi:10.1016/j.ijoa.2009.09.003
6. Pan PH, Tonidandel AM, Aschenbrenner CA, Houle TT, Harris LC, Eisenach JC. Predicting acute pain after cesarean delivery using three simple questions. Anesthesiology. 2013;118(5):1170–1179. doi:10.1097/ALN.0b013e31828e156f
7. Zeng Y, Hesketh T. The effects of China’s universal two-child policy. Lancet. 2016;388(10054):1930–1938. doi:10.1016/S0140-6736(16)31405-2
8. Wang L, Xu X, Baker P, et al. Patterns and associated factors of caesarean delivery intention among expectant Mothers in China: implications from the Implementation of China’s New National Two-Child Policy. Int J Environ Res Public Health. 2016;13(7):E686. doi:10.3390/ijerph13070686
9. Gasim T, Al JF, Rahman MS, Rahman J. Multiple repeat cesarean sections: operative difficulties, maternal complications and outcome. J Reprod Med. 2013;58(7–8):312–318.
10. Elbohoty AE, Gomaa MF, Abdelaleim M, Abd-el-gawad M, Elmarakby M. Diathermy versus scalpel in transverse abdominal incision in women undergoing repeated cesarean section: a randomized controlled trial. J Obstet Gynaecol Res. 2015;41(10):1541–1546. doi:10.1111/jog.12776
11. Duan G, Guo S, Zhang Y, et al. Effects of epidemiological factors and pressure pain measurements in predicting postoperative pain: a prospective survey of 1002 Chinese patients. Pain Physician. 2017;20(6):E903–E914.
12. Hartwig M, Allvin R, Backstrom R, Stenberg E. Factors associated with increased experience of postoperative pain after laparoscopic gastric bypass surgery. Obes Surg. 2017;27(7):1854–1858. doi:10.1007/s11695-017-2570-4
13. Berglund L, Stalman A, Dungner E, Qureshi AR, Kumlin M, Fellander-Tsai L. Younger patients and smokers report a higher level of pain after knee arthroscopy: a clinical and experimental study including synovial metabolism. Knee Surg Sports Traumatol Arthrosc. 2019;27(2):471–477. doi:10.1007/s00167-018-5125-x
14. Gagliese L, Gauthier LR, Macpherson AK, Jovellanos M, Chan VW. Correlates of postoperative pain and intravenous patient-controlled analgesia use in younger and older surgical patients. Pain Med. 2008;9(3):299–314. doi:10.1111/j.1526-4637.2008.00426.x
15. Practice Guidelines for Obstetric Anesthesia. An updated report by the American Society of Anesthesiologists Task Force on obstetric anesthesia and the society for obstetric anesthesia and perinatology. Anesthesiology. 2016;124(2):270–300. doi:10.1097/ALN.0000000000000935
16. Committee on Practice Bulletins—Obstetrics. Practice bulletin No. 177: obstetric analgesia and anesthesia. Obstet Gynecol. 2017;129(4):e73–e89. doi:10.1097/AOG.0000000000002018
17. Molina G, Weiser TG, Lipsitz SR, et al. Relationship between cesarean delivery rate and maternal and neonatal mortality. JAMA. 2015;314(21):2263–2270. doi:10.1001/jama.2015.15553
18. Zhang J, Troendle J, Reddy UM, et al. Contemporary cesarean delivery practice in the United States. Am J Obstet Gynecol. 2010;203(4):
19. Valdes AM, Suokas AK, Doherty SA, Jenkins W, Doherty M. History of knee surgery is associated with higher prevalence of neuropathic pain-like symptoms in patients with severe osteoarthritis of the knee. Semin Arthritis Rheum. 2014;43(5):588–592.
20. Rath W. Prevention of postpartum haemorrhage with the oxytocin analogue carbetocin. Eur J Obstet Gynecol Reprod Biol. 2009;147(1):15–20.
21. Tulandi T, Agdi M, Zarei A, Miner L, Sikirica V. Adhesion development and morbidity after repeat cesarean delivery. Am J Obstet Gynecol. 2009;201(1):
22. Arlier S, Seyfettinoğlu S, Yilmaz E, et al. Incidence of adhesions and maternal and neonatal morbidity after repeat cesarean section. Arch Gynecol Obstet. 2017;295(2):303–311. doi:10.1007/s00404-016-4221-8
23. Holthusen H, Kojda G. Nitric oxide (NO) and pain. The role of NO in the origin and treatment of pain. Med Monatsschr Pharm. 2000;23(10):323–328.
24. Saini AK, Arun KH, Kaul CL, Sharma SS. Acute hyperglycemia attenuates nerve conduction velocity and nerve blood flow in male Sprague-Dawley rats: reversal by adenosine. Pharmacol Res. 2004;50(6):593–599. doi:10.1016/j.phrs.2004.04.004
25. Ng B, Dimsdale JE, Rollnik JD, Shapiro H. The effect of ethnicity on prescriptions for patient-controlled analgesia for post-operative pain. Pain. 1996;66(1):9–12. doi:10.1016/0304-3959(96)02955-7
26. Dorner TE, Muckenhuber J, Stronegger WJ, Rasky E, Gustorff B, Freidl W. The impact of socio-economic status on pain and the perception of disability due to pain. Eur J Pain. 2011;15(1):103–109. doi:10.1016/j.ejpain.2010.05.013
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.