Back to Journals » Research and Reports in Urology » Volume 12
Renal Artery Embolization for Acute Renal Hemorrhage: A Single-Center Experience
Authors Limtrakul T ![]() , Rompsaithong U
, Rompsaithong U ![]() , Ahooja A, Kiatsopit P, Lumbiganon S, Pachirat K, Sirithanaphol W
, Ahooja A, Kiatsopit P, Lumbiganon S, Pachirat K, Sirithanaphol W
Received 19 May 2020
Accepted for publication 28 July 2020
Published 5 August 2020 Volume 2020:12 Pages 315—319
DOI https://doi.org/10.2147/RRU.S263012
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jan Colli
Tanapoom Limtrakul,1 Ukrit Rompsaithong,1 Anucha Ahooja,2 Pakorn Kiatsopit,1 Supanut Lumbiganon,1 Kachit Pachirat,1 Wichien Sirithanaphol1
1Department of Surgery, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand; 2Department of Radiology, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand
Correspondence: Wichien Sirithanaphol
Department of Surgery, Faculty of Medicine, Khon Kaen University, Khon Kaen 40002, Thailand
Tel +66-43-363664
Fax +66-43-202491
Email [email protected]
Background: Emergency renal artery embolization (RAE) is a useful method in treating renal trauma and bleeding renal tumors. The aim of this study was to evaluate the clinical efficacy and safety of emergency RAE, and factors associated with RAE failure.
Methods: This retrospective study included patients treated with emergency RAE for acute renal hemorrhage between 1 January 2009 and 31 October 2019 in Srinagarind Hospital. The embolization was performed using coils, glues, and/or gel foams. Factors associated with unsuccessful outcomes were analyzed using univariate and multivariate regression analyses.
Results: A total of 94 patients were treated at the center during the study period with the clinical success rate of 91.5%. The most common cause of acute renal hemorrhage was iatrogenic injury (76.5%). Factors associated with unsuccessful RAE according to multivariate analyses were hypertension (adjusted odds ratio [AOR] 24.2) and ruptured tumor/aneurysm (AOR 26.8).
Conclusion: RAE is an effective procedure for acute renal hemorrhage. Hypertension and ruptured tumor/aneurysm were negative predictors for success.
Keywords: renal artery embolization, renal trauma, renal hemorrhage, PCNL, kidney biopsy, renal tumor
Background
Acute renal hemorrhage is an urgent condition that can lead to a severe and life-threatening outcome. It is the complication of many urological procedures including but not limited to kidney biopsy, percutaneous nephrostomy, and nephrolithotomy.1–3 Moreover, a ruptured tumor or aneurysm as well as blunt and penetrating trauma can also result in acute renal hemorrhage.1,4
Therapeutic renal artery embolization (RAE) is a minimally invasive procedure and has been the standard treatment for acute renal hemorrhage in recent years. The procedure is associated with less morbidity and complications comparing to conventional emergency nephrectomy.5,6
However, there is limiting large scale data to demonstrate the clinical efficacy and safety for emergency embolization. Herein, we report our data regarding therapeutic RAE for a variety of urological conditions.
Materials and Methods
Patients
This was a retrospective study conducted in Srinagarind Hospital, Khon Kaen University, Thailand. Patients were included if they were 1) 18 years old or over, 2) diagnosed with acute renal hemorrhage, and 3) treated with emergency RAE between 2009 and 2019. Baseline clinical data, operative details, and perioperative complications were reviewed.
Definitions
The technical success rate was defined by a successful embolization without contrast extravasation after RAE. The clinical success rate was the technical success rate and clinical improvement without the second intervention or procedure. Post embolization syndrome (PES) was defined by fever > 38 °c and/or flank pain without infection.
Glomerular filtration rate (GFR) was calculated from Cockroft-Gault formula. Postoperative GFR change was defined as the difference between baseline GFR and GFR at 24 hours after the procedure.
Procedure
The embolization was performed by the interventionists from the department of interventional radiology at Srinagarind Hospital. The technical details were as described: an angiographic catheter was introduced into the renal artery through a femoral approach and selective renal angiograms were performed to identify the lesions. Embolization was done by using coils, glues, and/or gel foams.
After the procedure, all patients were closely observed by urologists.
Vital signs, physical symptoms, urinalysis, and hematocrit levels were monitored serially during the first 24 hours. Serum creatinine was checked thereafter to assess the deterioration of renal function. If there was a sign of new bleeding, an emergency CT scan was performed.
Statistical Analysis
Descriptive statistics for baseline data were presented as percentages, mean, and standard deviation. If the distribution was not normal, the median and inter-quartile range were used instead. The effects of factors associated with clinical unsuccessful embolization were evaluated using univariate and multivariate regression analyses. Crude odds ratios (ORs) and 95% confidence intervals (CIs) were used to show the association of the factors examined with unsuccessful embolization. Factors with a p-value of <0.20 were then entered into a multiple logistic regression model. A p-value of <0.05 was considered statistically significant differences, and adjusted ORs (AORs) and 95% CIs were used to determine the strength of association. All data analyses were performed using STATA software (StataCorp LP, College Station, TX, USA).
Ethical approval was provided by the Khon Kaen University Faculty of Medicine Ethics Committee as instituted by the Declaration of Helsinki (HE631033). The patient’s consent to review the medical record was not required by the committee due to the retrospective nature of the study. All the data was anonymized and maintained with confidentiality.
Results
Success Rate
During the study period, a total of 94 patients were included. The clinical success rate of RAE for acute renal hemorrhage was 91.5% (86 cases) and the technical success rate was 98%. The baseline characteristics are shown in Table 1. In the unsuccessful group, two patients underwent emergency nephrectomy without postoperative complications.
 |
Table 1 Baseline Characteristics of the Studied Population and a Comparison of Successful and Unsuccessful Subjects Using Univariate Analyses |
Etiology of Acute Renal Hemorrhage
The most common cause of acute renal hemorrhage was iatrogenic injury (76.5%) as a result of complications from a kidney biopsy, percutaneous nephrolithotomy (PCNL), anatrophic nephrolithotomy, percutaneous nephrostomy, and partial nephrectomy, respectively. All traumatic cases were successfully treated with RAE. Eight patients suffered from blunt trauma, while the other two patients were penetrating injuries.
Complications of RAE
The median length of hospital stay in a successful group was significantly shorter than the failure group, 8 vs 23 days (p=0.02). Post-operative declination of glomerular filtration rate (GFR) was comparable in both groups; the median GFR changes were 0 vs 1.45 (p=0.8) in the success and the failure group respectively. Post embolization syndrome was observed in 12 patients (12.7%). Two patients developed septic complications and there was a massive blood transfusion complication in one patient.
Factors Associated with Unsuccessful Embolization
Following the univariate analysis (Table 1), BMI, flank pain, hypertension, and ruptured tumor/aneurysm were entered into the multiple regression models, as they are significant factors in univariate analysis (p<0.2). There was a significantly higher proportion of female patients with a ruptured tumor/aneurysm compared to male patients, therefore, sex was not entered into the model. Hypertension and ruptured tumor/aneurysm were two independent factors for unsuccessful embolization (Table 2). Multicollinearity was checked.
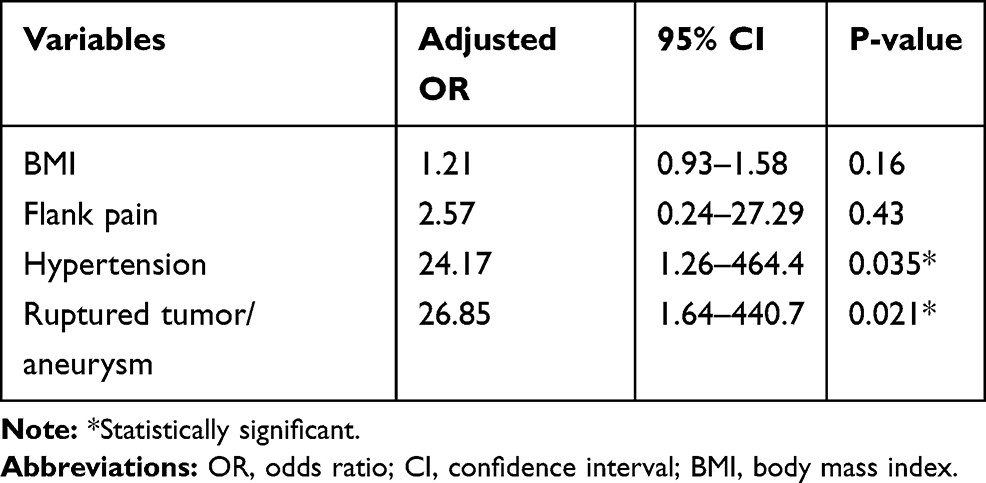 |
Table 2 Factors Associated with Unsuccessful Embolization Using Multivariate Analysis |
Discussion
In this study, the clinical success rate of renal artery embolism for acute renal hemorrhage was 91.5%, and factors associated with failure were hypertension and ruptured tumor/aneurysm.
The successful rate was consistent with prior studies as shown in Table 3. Most of the studies reported were done in post-PCNL bleeding complications, and the success rate varied between 73–100%.7–9 To be noted, most of the reported studies were conducted by experienced interventionists and high-volume centers.
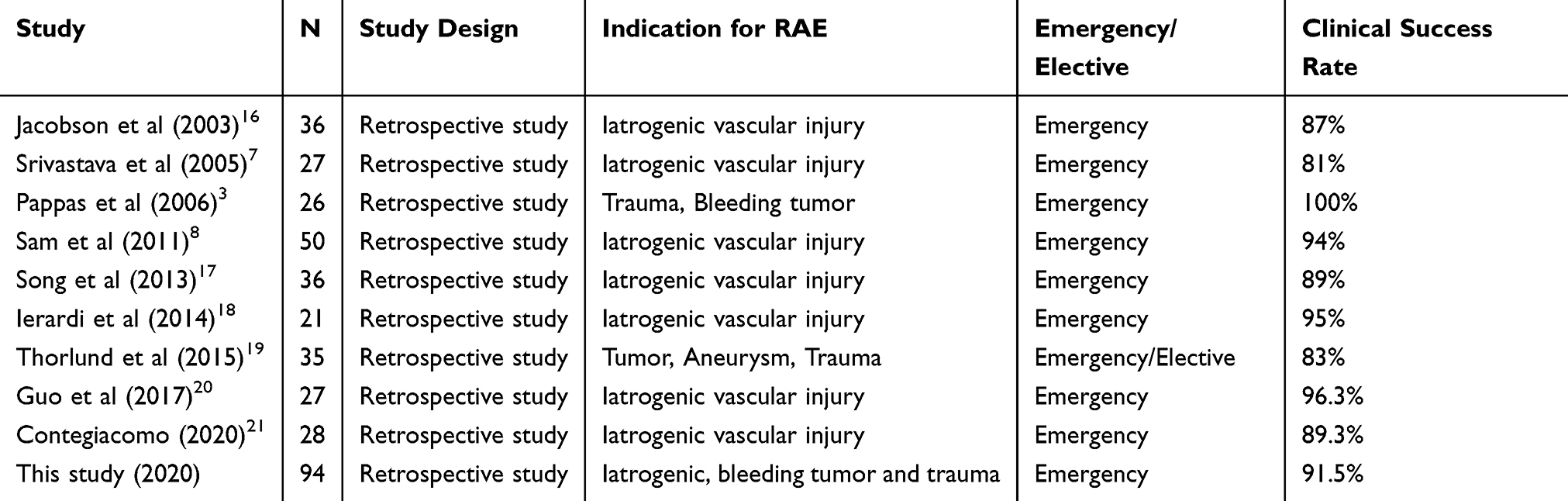 |
Table 3 Comparison of Indication for RAE, Settings, and Outcomes of This Series with That Previous Reported |
Hypertension is the main risk factor for failure RAE. Previous studies have also shown that hypertension increases the risk of unsuccessful RAE due to the presence of arteriosclerosis resulting in abnormal anatomical variants in the renal arteries.10,11 Diabetes mellitus, which is another important risk factor for arteriosclerosis, was not associated with failure rate in our cohort.9 Since the number of diabetes patients was low (only 12%), we could not draw a definite conclusion on this.
In the present study, bleeding tumor/aneurysm was also a significant factor for RAE failure. Renal vascular aberration, high vascularization, and complexity from the tumor could complicate the procedures and result in an unsuccessful outcome.2 For symptom control of bleeding tumor, the reported outcomes of successful RAE were 70–87%,12,13 similar to this cohort.
Even though obesity was found to be associated with postoperative complications and bleeding, it is not associated with unsuccessful RAE.14,15 In this study, we found that for each 1 kg/m2 BMI increase, risk factors for failure rate increased by 1.2 times but it was not an independent factor in this study. This is also consistent with prior studies.
There was no procedure-related complication, but post embolization syndrome was observed in 12 patients (12.7%). There was no treatment-related death in this cohort.
The main limitation of this study was the fact that this was a retrospective study which has biases due to its nature. Second, the follow up was short, thus the long-term morbidity of RAE cannot be evaluated. Lastly, the results of this study could be applied only to specialized centers with experienced interventionists and urologist teams.
Conclusion
Emergency renal artery embolization is safe and effective for renal hemorrhage. Hypertension and bleeding tumor/aneurysm were negative predictors for success.
Disclosure
The authors report no conflicts of interest for this work.
References
1. Breyer BN, McAninch JW, Elliott SP, Master VA. Minimally invasive endovascular techniques to treat acute renal hemorrhage. J Urol. 2008;179(6):
2. Li D, Pua BB, Madoff DC. Role of embolization in the treatment of renal masses. Semin Intervent Radiol. 2014;31(1):70–81. doi:10.1055/s-0033-1363845
3. Pappas P, Leonardou P, Papadoukakis S, et al. Urgent superselective segmental renal artery embolization in the treatment of life-threatening renal hemorrhage. Urol Int. 2006;77(1):34–41. doi:10.1159/000092932
4. Du N, Ma JQ, Luo JJ, et al. The efficacy and safety of transcatheter arterial embolization to treat renal hemorrhage after percutaneous nephrolithotomy. Biomed Res Int. 2019;2019:6265183. doi:10.1155/2019/6265183
5. Muller A, Rouviere O. Renal artery embolization-indications, technical approaches and outcomes. Nat Rev Nephrol. 2015;11(5):288–301. doi:10.1038/nrneph.2014.231
6. Schwartz MJ, Smith EB, Trost DW, Vaughan ED
7. Srivastava A, Singh KJ, Suri A, et al. Vascular complications after percutaneous nephrolithotomy: are there any predictive factors? Urology. 2005;66(1):38–40. doi:10.1016/j.urology.2005.02.010
8. Sam K, Gahide G, Soulez G, et al. Percutaneous embolization of iatrogenic arterial kidney injuries: safety, efficacy, and impact on blood pressure and renal function. J Vasc Interv Radiol. 2011;22(11):1563–1568. doi:10.1016/j.jvir.2011.06.020
9. Mao Q, Wang C, Chen G, Tan F, Shen B. Failure of initial superselective renal arterial embolization in the treatment of renal hemorrhage after percutaneous nephrolithotomy: A respective analysis of risk factors. Exp Ther Med. 2019;18(5):4151–4156. doi:10.3892/etm.2019.8033
10. Akman T, Binbay M, Sari E, et al. Factors affecting bleeding during percutaneous nephrolithotomy: single surgeon experience. J Endourol. 2011;25(2):327–333. doi:10.1089/end.2010.0302
11. Kukreja R, Desai M, Patel S, Bapat S, Desai M. Factors affecting blood loss during percutaneous nephrolithotomy: prospective study. J Endourol. 2004;18(8):715–722. doi:10.1089/end.2004.18.715
12. Mukund A, Gamanagatti S. Ethanol ablation of renal cell carcinoma for palliation of symptoms in advanced disease. J Palliat Med. 2010;13(2):117–120. doi:10.1089/jpm.2009.0243
13. Onishi T, Oishi Y, Suzuki Y, Asano K. Prognostic evaluation of transcatheter arterial embolization for unresectable renal cell carcinoma with distant metastasis. BJU Int. 2001;87(4):312–315. doi:10.1046/j.1464-410x.2001.00070.x
14. Ri M, Aikou S, Seto Y. Obesity as a surgical risk factor. Ann Gastroenterol Surg. 2018;2(1):13–21. doi:10.1002/ags3.12049
15. Tjeertes EK, Hoeks SE, Beks SB, Valentijn TM, Hoofwijk AG, Stolker RJ. Obesity–a risk factor for postoperative complications in general surgery? BMC Anesthesiol. 2015;15:112. doi:10.1186/s12871-015-0096-7
16. Jacobson AI, Amukele SA, Marcovich R, et al. Efficacy and morbidity of therapeutic renal embolization in the spectrum of urologic disease. J Endourol. 2003;17(6):385–391. doi:10.1089/089277903767923164
17. Song P, Wang MQ, Liu FY, Duan F, Wang Y. Iatrogenic renovascular injuries treated by transarterial embolization. Eur Rev Med Pharmacol Sci. 2013;17(24):3398–3404.
18. Ierardi AM, Floridi C, Foontana F, et al. Transcatheter embolisation of iatrogenic renal vascular injuries. Radiol Med. 2014;119(4):261–268. doi:10.1007/211547-013-0343-2
19. Thorlund MG, Wennevik GE, Andersen M, Andersen PE, Lund L. High success rate after arterial renal embolisation. Dan Med J. 2015;62:5.
20. Guo H, Wang C, Yang M, et al. Management of iatrogenic renal arteriovenous fistula and renal arterial pseudoaneurysm by transarterial embolization: A single center analysis and outcomes. Medicine. 2017;96(40):e8187. doi:10.1097/MD.0000000000008187
21. Contegiacomo A, Amodeo EM, Cina A, et al. Renal artery embolization for iatrogenic renal vascular injuries management: 5 years’ experience. Br J Radiol. 2020;93(1106):20190256. doi:10.1259/bjr.20190256
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.